
Abstract
The use of generic “you” (GY) in writing samples fosters psychological distancing and functions as a linguistic mechanism to facilitate emotion regulation. This method of creating psychological distance from the traumatic experience of cancer may be used by patients processing emotions. We used behavioral coding to analyze expressive writing samples collected from 138 cancer patients to examine the association between the use of “you” and cancer-related symptoms and psychological outcomes. Occurrences of GY were low, but our qualitative results showed how the use of GY could create a universal experience of cancer. The use of GY was not associated with cancer-related symptoms and depressive symptoms, but longitudinal analyses revealed that those using GY had fewer intrusive thoughts and avoidance behaviors across the follow-up period of 1, 4, and 10 months after the intervention. The development of psychological self-distancing prompts to use in writing interventions or as a clinical tool for cancer patients should be explored.
Background
The diagnosis and treatment of cancer is typically perceived as a stressful, unpleasant experience during which patients must employ strategies to increase resilience and decrease distress. Extensive research shows that people with cancer tend to have higher rates of psychological distress, such as anxiety and depressive symptoms, as well as other nonspecific psychosocial stress (Draeger et al., 2018; Kendall et al., 2011; Linden et al., 2012; Orvell et al., 2017).Psychological distress and other aspects of mental health lead to a reduced quality of life (QoL), reduced treatment compliance, and elevated mortality (Conley et al., 2016; DiMatteo et al., 2000; Pinquart and Duberstein, 2010; Satin et al., 2009), which illustrates the need to better understand aspects of coping and resilience in patients with cancer and to develop strategies to help patients manage their distress.
One technique for managing distress in patients with cancer is appropriate emotion regulation (Conley et al., 2016; Peh et al., 2017; Vaughan et al., 2019). Emotion regulation is the process by which individuals manage and respond to emotional experiences (Gross, 1998), such as a cancer diagnosis and treatment. Accessible emotion regulation strategies have been shown to help people with cancer manage distress (Vaughan et al., 2019). One of these helpful strategies is psychological distancing, a form of cognitive reappraisal that changes the meaning of a stimulus to alter its effect. A method of increasing psychological distance is self-distancing, a process by which a person detaches from a distressing experience through shifting one’s perspective from a self-focused to a third person/observer view point (Kross and Ayduk, 2017). Clinically, studies have indicated that the beneficial effects of self-distancing, such as reduction of emotional reactivity, extend to disorders such as major depressive disorder and bipolar disorder (Kross and Ayduk, 2017). Theoretically, psychological distance may create the feeling of space or distance between the cancer patient and the intense emotional experience of a cancer diagnosis and treatment.
Psychological distancing has been shown to be an effective emotional regulation coping technique that can be learned over time through repeated practice. In a longitudinal study (Denny and Ochsner, 2014), over the course of four sessions, a group that received training in psychological distancing showed lower negative affect and perceived stress levels in their daily lives than a group that learned another cognitive reappraisal technique–reinterpretation, as well as a control group. The accessibility of psychological distancing may be attributed to the habitual nature of distancing because, once the strategy has been learned, it is easy to apply it to new situations without instruction (Denny and Ochsner, 2014). If psychological distancing is an easily learned technique that cancer patients can use when experiencing distress, interventions using this method should be further explored and used.
Linguistic mechanisms that facilitate psychological distancing could be easily learned in an intervention that is accessible to many. In expressive writing exercises, linguistic mechanisms that promote psychological distancing facilitate emotional regulation (Nook et al., 2017) and have a positive effect on health and wellness (Shahane and Denny, 2019). An experiment in which pictures are used as stimuli to induce negative affect showed that participants who were instructed to reappraise these negative stimuli reported less negative affect than those who were instructed to simply write about the images. When regulating emotion, participants naturally increased their use of words expressing psychological distance, such as words that were impersonal, not focused on the personal present, and abstract (Nook et al., 2017). In another study, participants were instructed to manipulate their writing to portray psychological distance (e.g. by writing objectively or using words that create physical distance), and this practice was linked to a positive effect on the participants’ health and wellness scores (Shahane and Denny, 2019). These findings demonstrate that through expressive writing exercises, a psychological distancing approach to emotion regulation may help patients process and adjust to their cancer experience.
Of particular interest is a seminal work in which distanced self-talk (DY) and the generic “you” (GY) were given as examples of linguistic mechanisms that facilitate emotional regulation through self-distancing to create psychological distance, in a naturally occurring, easy manner (Orvell et al., 2017). DY involves using one’s own name with non-first-person pronouns to promote self-reflection from an outside perspective, and GY is the use of the word “you” in a way that broadly refers to people in general (Orvell, 2019). Orvell proposed that these two linguistic mechanisms can function as self-distancing techniques, and help people change perspective when they reflect on a negative experience by enabling them to “step back” to shift their perspective and extend the experience beyond themselves (Orvell et al., 2017). For example, the second-person statements “You have to be strong to get through cancer treatment” (GY) or “[your name], you have to be strong to get through cancer treatment” (DY) create the feeling of a universal, shared experience, whereas the first-person statement “I have to be strong to get through cancer treatment” creates the feeling of an isolated experience. Essentially, GY and DY can represent an imagined spatial distance from an emotionally salient experience such as cancer diagnosis and treatment. Whereas first-person singular pronoun use among inpatients with clinical depression has been shown to be predictive of increased depressive symptoms and negative emotionality (Tackman et al., 2019; Zimmermann et al., 2017), GY usage is a newer linguistic mechanism, and to the best of our knowledge, the role of psychological distancing mechanisms to facilitate patients’ adjustment to the diagnosis and treatment of cancer has not yet been examined in the cancer setting.
To address this knowledge gap, we applied Orvell’s conceptualization of psychological distancing (i.e. GY and DY) to guide a secondary data analysis of a large expressive writing study involving patients with renal cell carcinoma (RCC). Psychological distancing is promoted through the practice of expressive writing (Nook et al., 2017; Park et al., 2016; Shahane and Denny, 2019), and use of the GY and DY linguistic mechanisms may materialize naturally within expressive writing samples. In the original expressive writing study, relative to those in a neutral writing comparison arm, participants in the expressive writing arm reported significantly reduced cancer-related symptoms via reduced cognitive intrusions and avoidance behaviors. In the present study, we explored whether these improvements were a function of the psychological distancing mechanisms displayed in the writing samples of the participants who were randomized to the expressive writing arm of the original study. More specifically, we hypothesized that the more frequently participants naturally use the linguistic mechanisms of GY and DY when emotionally processing their cancer experiences, the better their outcomes regarding cancer-related symptoms and psychological measures will be throughout a 10-month follow-up.
Methods
Participants and procedures
At the time of the original study, participants were diagnosed with stage I-IV RCC; had a Zubrod performance status of two or less (ambulatory at least 50% of the time); were at least 18 years old; and were able to read, write, and speak English. They were randomly assigned to either an expressive writing or a neutral writing group after completion of a baseline questionnaire (timepoint [T]1). Three additional assessments were completed 1 (T2), 4 (T3), and 10 (T4) months later. Following the procedures outlined in a prior study (Pennebaker and Beall, 1986), expressive writing samples were collected over a 10-day period on four separate occasions, after completion of the baseline questionnaire.. The participants were instructed to write about their deepest thoughts and feelings regarding their cancer diagnosis and treatment. Participants were given no instructions to use psychological distancing or other reappraisal methods. All procedures were approved by the Institutional Review Board, and written informed consent was obtained prior to data collection. The current study only reports on participants who were randomized to the expressive writing group (N = 138).
Psychological distancing coding
Psychological distancing language was defined by the presence of GY and/or DY use in participants’ writing samples. We used Language Inquiry Word Count (Pennebaker et al., 2007) software to identify writing samples that contained the pronoun “you.” Then, two independent raters coded these expressive writing samples for the frequency of GY and DY use. We followed previously published procedures for coding GY and DY use (Orvell et al., 2017). Phrases that involved the present tense, without aspect, and included “you,” “your,” and “you” within contractions (e.g. y’all) were coded as GY. GY is used in a generic way, so we did not include a “you” that was part of a quote (e.g. “The doctor told me, ‛You must start to exercise’”) or a “you” that was directed towards the reader (e.g. “I’m so thankful for the research you are doing”). Coding rules for DY were identical to those for GY, with the additional usage of the writer’s name. Two coders rated all samples, and a high degree of interrater reliability was reached (intra-class correlation coefficients = 0.99). All discrepancies between the coders were discussed with an additional reviewer until rater agreement was achieved. Each GY and DY occurrence was counted, aggregated across writing samples, and then converted into proportions by dividing the total count for GY and DY by the total word count of the writing samples. To account for the overall word length of participants’ writing samples, we used the proportion scores rather than the raw frequencies scores in the analyses described below.
Self-report measures
Baseline questionnaires asked for relevant demographic details, including age, education, marital status, and income. Medical variables were extracted from the medical record and included the cancer stage, time since diagnosis, and tumor type.
Cancer-related symptoms were assessed with the MD Anderson Symptom Inventory (MDASI; Cleeland et al., 2000). The MDASI measures the 13 core symptoms found in the highest frequencies across various types of cancer diagnoses and treatments. Patients rate symptom severity and the extent to which their daily activities are affected by symptom burden on a scale of 0 to 10. Here, we present the subscales of cancer symptom severity (Cronbach’s alpha = 0.87) and cancer symptom interference (Cronbach’s alpha = 0.93). Higher scores denote a greater likelihood that cancer symptoms interfered with daily activities.
Depressive symptoms were assessed using the Center for Epidemiologic Studies Depression Scale (Radloff, 1977), a self-reported measure of 20 items focusing on the affective components of depression (Cronbach’s alpha = 0.89). A score of 16 or higher is considered the cut-off for a depressive disorder.
Intrusive thoughts and avoidance behaviors were measured with the Impact of Events Scale (IES), a 15-item, self-reported scale assessing thought intrusion and avoidance during the past week (Horowitz et al., 1979; Cronbach’s alpha = 0.97). Higher scores represent a greater prevalence of intrusive thoughts and avoidance behaviors.
Statistical methods
We first performed descriptive analyses (e.g. calculating frequencies, means, and correlations) of the psychological distancing variables (i.e. GY and DY codes) and self-reported baseline measures. To test the study hypotheses that the more frequently participants naturally use the linguistic mechanism of GY and DY when emotionally processing their cancer experiences, the better their outcomes regarding cancer-related symptoms and psychological measures will be throughout a 10-month follow-up, we performed multilevel modeling analyses using PROC MIXED (SAS, 9.4 version) accounting for the nested data structure of the repeated measures. Unlike the general linear model using listwise deletion, PROC MIXED uses a likelihood-based estimation method to minimize the impact of attrition and missing data in the analysis (Wolfer and Sang, 1995). We specified a random intercept and an unstructured covariance matrix and treated the assessment time as a categorical covariate. p-Values less than 0.05 were considered significant. We also included the baseline level of the outcome of interest as a covariate in all the multilevel modeling analyses. Because age, sex, and stage at diagnosis are important prognostic factors in RCC (Downs et al., 2009; Parker et al., 2012; Poulakis et al., 2003; Stark et al., 2002), we also included these variables as a priori covariates.
Results
Baseline sample characteristics
Of the 138 participants assigned to the expressive writing group, 117 initiated the intervention, and follow-up assessments were available for 87 participants at T2, 84 at T3, and 72 at T4. Attrition occurred because of passive or active withdrawal (n = 37; 82%) and participants’ death (n = 8; 18%). Of the 138 participants in these analyses, 60% were men, 76% were non-Hispanic White, 71% were married, 73% had completed at least some college, and 59% were employed full time. The patients’ mean age was 58 years (standard deviation = 10 years). Almost half (48%) of the patients had advanced disease (stage III or IV RCC). Please see Table 1 for baseline characteristics of the sample.
Participant demographics and clinical characteristics for the EW group.
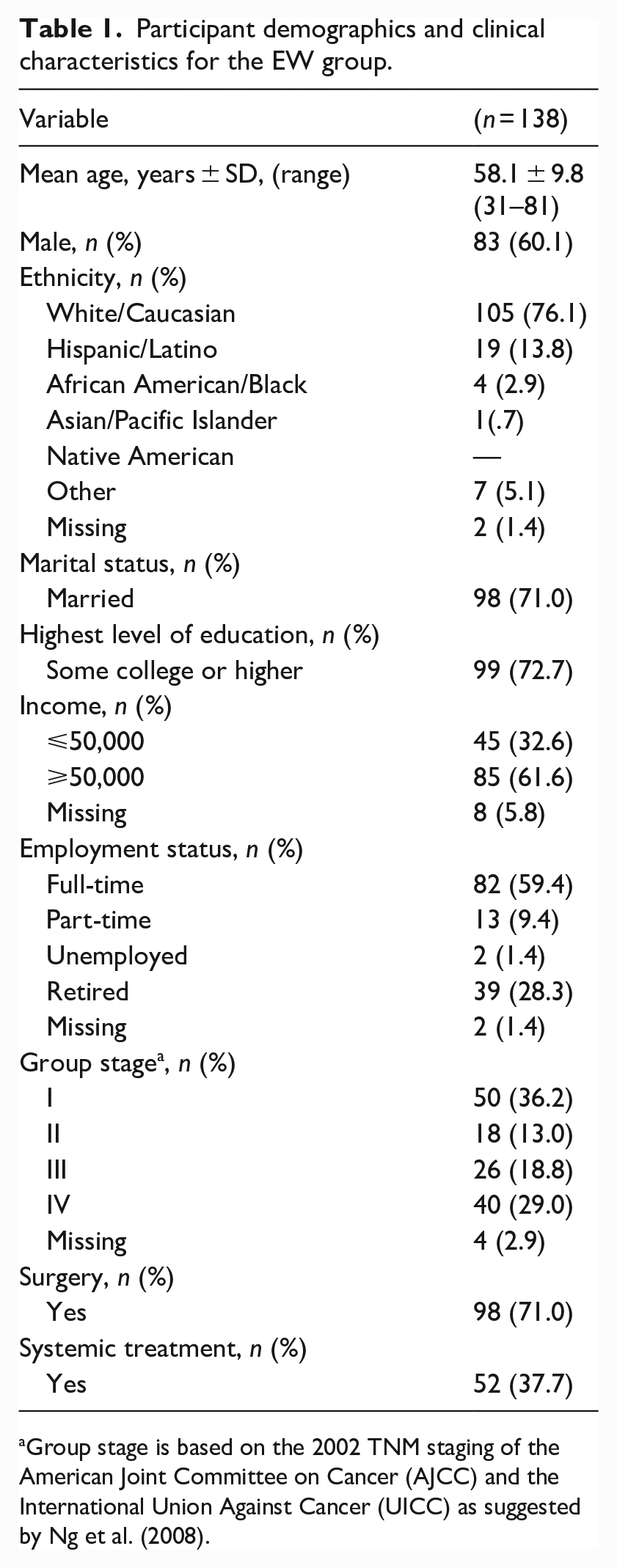
Group stage is based on the 2002 TNM staging of the American Joint Committee on Cancer (AJCC) and the International Union Against Cancer (UICC) as suggested by Ng et al. (2008).
Descriptive analyses of psychological distancing in the writing samples
Of the 117 participants who completed baseline assessments, all completed at least one writing sample, and 102 completed all four writing sessions. Based on the Language Inquiry Word Count analyses, of the 425 writing samples, 38.1% (n = 162) contained references in the “you” category, which were then coded as GY and DY use as described above. Participants used GY a mean of 3.81 times (SD = 7.14 times; range = 0–45 times). This translated into a mean proportion of 0.0031 (SD = 0.006; range = 0–0.04), meaning that only 0.3% of all language contained GY use. We did not find a single incidence of DY use across participants and writing samples. None of the sociomedical factors (e.g. age, gender, education, race/ethnicity, and stage of disease) were significantly associated with GY use (see the Supplemental Table for the results regarding the null associations).
Associations between psychological distancing and baseline self-report measures
Bivariate correlation analyses revealed that GY was significantly associated with cancer symptom interference (r = 0.28; p < 0.01), meaning that greater GY use was associated with a greater probability that cancer symptoms were interfering with patients’ daily activities. The associations between GY and cancer symptom severity, depressive symptoms, and cognitive intrusion and avoidance were not significant. See Table 2 for the descriptive results of all study variables.
Means, standard deviations, and correlation coefficients of study variables at baseline.
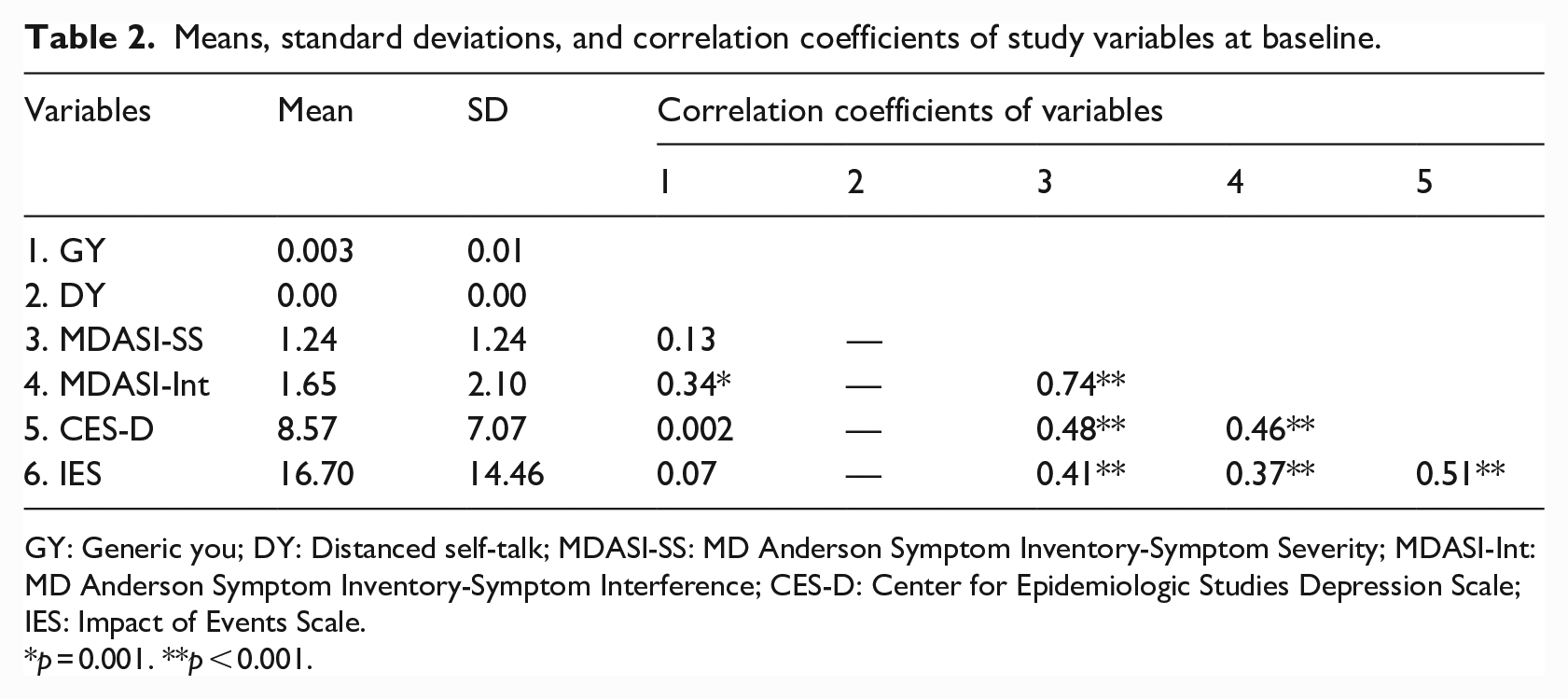
GY: Generic you; DY: Distanced self-talk; MDASI-SS: MD Anderson Symptom Inventory-Symptom Severity; MDASI-Int: MD Anderson Symptom Inventory-Symptom Interference; CES-D: Center for Epidemiologic Studies Depression Scale; IES: Impact of Events Scale.
p = 0.001. **p < 0.001.
Examples of psychological distancing in the writing samples
The following are examples of how unprompted participants chose to use GY as a linguistic mechanism in a way that exemplifies emotion regulation through expressive writing. These examples exhibit how the use of GY may function to create a universal, shared experience.
The following example illustrates how the use of GY may portray recovery after hitting a low point as a common, shared experience.
“I now know how a bird must feel if surviving after slamming into a reflection of him/herself in a glass window- you’re knocked off your feet, you falter & fall and possibly hit rock bottom, you finally pick yourself up and check for anything broken, you fix it as best you can, and then you go on. If you’re as fortunate as I am, you have love, support, and especially the prayers of so many who care (especially a great husband) – and that is what keeps you going.”
(A 70-year-old White woman with stage IV disease)
Next, a participant uses GY to describe their cancer-related increase in mortality awareness, which helps to create the feeling of a shared experience.
“None of us are promised tomorrow, but with knowing you have cancer, it makes you stop and think more. We know we will all die someday, but w/a disease that can ravage your body, it makes you a little more aware of this.”
(A 71-year-old White woman with stage I disease)
Finally, in the below example, a participant uses GY to frame their changing relationship with fear as a universal experience.
“Sometimes, but I did before this too, you work through your fears and when you get right down to it, we all are going to die sometime, and there is no good time to die. So when I get fearful, or depressed, I recognize that that will happen and then work to ignore it, and sometimes acting like you are not afraid becomes easier over time and you start learning not to be afraid.”
(A 59-year-old White man with stage IV disease)
Main study analyses
The results below are based on multilevel modeling analyses with adjustment for baseline levels of the given self-reported measure (i.e. MDASI, CES-D, and IES) and other aforementioned covariates.
Cancer-related symptoms
GY was not significantly associated with MDASI scores (severity: t = −0.15, p = 0.88; interference: t = −0.82; p = 0.42; b = −0.13) across the follow-up period.
Depressive symptoms
GY was not significantly associated with the CES-D scores (t = 0.18; p = 0.86) across the follow-up period.
Cognitive intrusion and avoidance behaviors
GY was significantly inversely associated with IES scores (t = −2.10; p = 0.04) across the follow-up period, suggesting that greater GY use was prospectively associated with reduced intrusion and avoidance.
Discussion
The aim of this study was to investigate whether increased use of GY statements in existing expressive writing samples from renal cancer patients are correlated with lower cancer-related symptoms and better overall psychological health outcomes. Occurrences of GY and DY in the present study were substantially fewer than anticipated, as only a small percentage of language (0.3%) included GY usage, and no DY statements were found. Our qualitative results revealed clear examples of how using GY creates a universal, shared experience of cancer, which we expected to have a direct association with improved symptom outcomes. Although GY use was not significantly associated with cancer-related symptoms and depressive symptoms, and although it was rarely found in patients’ writing samples, prospective analyses revealed that the more patients were using GY, the more likely they reported lower levels of intrusive thoughts and avoidance behaviors across the 10-month follow-up period. This finding suggests that psychological distancing may still be occurring despite the low occurrence of GY. The reduction in intrusive thoughts and avoidance behaviors is especially relevant, as it was found to mediate the beneficial effects of expressive writing on cancer-related symptoms at the 10-month follow-up in a larger sample that also included the neutral writing group (Milbury et al., 2017).
Our findings support and extend the existing literature. For one, it has been shown that expressive writing participants exhibit more self-distancing and less emotional reactivity (Park et al., 2016). Our analysis showed a significant inverse association between GY and IES scores, suggesting that the use of psychological distancing leads to fewer intrusive thoughts and avoidance behaviors. This result is consistent with a recent study of breast cancer patients that found a strong positive correlation between unprocessed emotion and IES scores (Oginska-Bulik and Michalska, 2020) illustrating that GY may help lower intrusive thoughts and avoidance behaviors by allowing participants to process and regulate emotion. In another study, in which participants (who were not cancer patients) analyzed their personal anger incidents either in a self-immersed or self-distanced manner, the self-distanced group had lower IES avoidance subscale scores (Ayduk and Kross, 2009). We expect that GY usage has a similar psychological distancing effect and lessens the stress participants experience because of their cancer diagnosis and treatment. In a previous study of GY, participants who used GY more frequently in expressive writing samples showed a significantly higher degree of psychological distancing than did participants who used first-person singular pronouns more frequently (Orvell et al., 2017). This finding further illustrates that GY usage may promote psychological distancing. In an earlier analysis of these expressive writing data, lower IES scores at 1 month had a mediating relationship with lower MDASI scores at 10 months for the expressive writing group (Milbury et al., 2017). GY usage may function by creating psychological distance and helping with emotion regulation, leading to less stress from cancer and its treatment. However, with the low usage of GY found in our study, it could not be associated with other outcomes.
Of note, in one study of GY (Orvell et al., 2017), study procedures prompted participants to practice perspective taking in their writing, which we speculate yielded a higher rate of GY statements. Specifically, participants were randomized to writing exercise groups in which they were prompted to use GY or first-person singular pronouns. The GY group was prompted to “write in universal terms about the meaning of this experience for people in general,” and were given an example of using GY as the preferred pronoun (Orvell et al., 2017). In contrast, participants in the current study were not prompted to use GY statements, and the samples we assessed included only spontaneous GY use. Future research using prompted samples to elicit GY use, thereby leading to more GY usage, may find that the effects of expressive writing can be enhanced, leading to greater reductions in intrusive thoughts and avoidance behaviors and improved QoL.
An interesting direction for future research might be to explore the use of GY in patients with cancer other than RCC. Adolescent and young adult patients are notably optimistic and resilient through treatment (Greup et al., 2018) and may be more likely to recognize resources to cope with stressors to gain a positive benefit (Haase, 2004), such as GY statements. Informal caregivers of cancer patients also may benefit from using GY to assist with emotion processing because these caregivers tend to have a high distress level and need for support and to be responsive to emotion-regulation interventions (Applebaum et al., 2020).
Study limitations
Our study had some limitations. First, due to the use of secondary data, we did not use writing prompts to encourage the use of GY and instead depended on the participants’ natural inclination to use GY statements. Second, the lack of significant associations between GY usage and symptom burden may be due to a floor effect, as the spontaneous use of GY was very low. However, even with the low use of GY, the findings of one of the three main analyses were significant. We speculate that, with greater GY use, the outcomes may be more salient. Also, due to the use of secondary data analysis, our findings were limited by the lack of a diverse cancer population and the fact that our participants were mostly White (76%) and had some college education (73%). The original study showed that participants with lower levels of education were more likely to withdraw from the study, likely attributable to participants with more education feeling more proficient in or comfortable with writing. Finally, attrition rate may be considered a limitation, as only 62% of participants who initiated the intervention completed all timepoint assessments.
Clinical implications
Future studies should further investigate the linguistic use of psychological self-distancing using DY- and GY-based interventions to determine whether they can improve the psychological and physical health outcomes of cancer patients. The development of psychological self-distancing prompts to use in emotional writing interventions or as clinical tools in supportive expressive therapy for cancer patients should be explored. Such prompts could simply include instructions to write expressively using “you” statements, as well as examples of GY usage. A major advantage of this type of intervention is that linguistic mechanisms are easily learned and accessible tools that individuals can use during cancer treatment to lessen cancer-related distress.
Conclusion
This is the first exploration of the linguistic use of psychological self-distancing using DY and GY to determine associations between this linguistic mechanism and multiple aspects of QoL in patients with cancer. Within expressive writing samples, we discovered qualitative examples of how patients with RCC may use GY statements to process emotions and normalize their experiences. Furthermore, we found a significant inverse association between GY and IES scores across the follow-up period; this association indicated a reduction in intrusive thoughts and avoidance behaviors, possibly because of more effective processing of emotions. Ideally, future research will prompt patients to use GY statements in an expressive writing intervention that may lead to better psychological and physical health outcomes.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053231182218 – Supplemental material for Words matter: The use of generic “you” in expressive writing in an oncology setting
Supplemental material, sj-docx-1-hpq-10.1177_13591053231182218 for Words matter: The use of generic “you” in expressive writing in an oncology setting by Stella Snyder, Kathrin Milbury, Richard Wagner and Lorenzo Cohen in Journal of Health Psychology
Research Data
sj-docx-2-hpq-10.1177_13591053231182218 – Supplemental material for Words matter: The use of generic “you” in expressive writing in an oncology setting
Supplemental material, sj-docx-2-hpq-10.1177_13591053231182218 for Words matter: The use of generic “you” in expressive writing in an oncology setting by Stella Snyder, Kathrin Milbury, Richard Wagner and Lorenzo Cohen in Journal of Health Psychology
Supplemental Material
sj-pdf-3-hpq-10.1177_13591053231182218 – Supplemental material for Words matter: The use of generic “you” in expressive writing in an oncology setting
Supplemental material, sj-pdf-3-hpq-10.1177_13591053231182218 for Words matter: The use of generic “you” in expressive writing in an oncology setting by Stella Snyder, Kathrin Milbury, Richard Wagner and Lorenzo Cohen in Journal of Health Psychology
Research Data
sj-pdf-4-hpq-10.1177_13591053231182218 – Supplemental material for Words matter: The use of generic “you” in expressive writing in an oncology setting
Supplemental material, sj-pdf-4-hpq-10.1177_13591053231182218 for Words matter: The use of generic “you” in expressive writing in an oncology setting by Stella Snyder, Kathrin Milbury, Richard Wagner and Lorenzo Cohen in Journal of Health Psychology
Research Data
sj-sas-7-hpq-10.1177_13591053231182218 – Supplemental material for Words matter: The use of generic “you” in expressive writing in an oncology setting
Supplemental material, sj-sas-7-hpq-10.1177_13591053231182218 for Words matter: The use of generic “you” in expressive writing in an oncology setting by Stella Snyder, Kathrin Milbury, Richard Wagner and Lorenzo Cohen in Journal of Health Psychology
Research Data
sj-xlsx-5-cll-10.1177_13591053231182218 – Supplemental material for Words matter: The use of generic “you” in expressive writing in an oncology setting
Supplemental material, sj-xlsx-5-cll-10.1177_13591053231182218 for Words matter: The use of generic “you” in expressive writing in an oncology setting by Stella Snyder, Kathrin Milbury, Richard Wagner and Lorenzo Cohen in Journal of Health Psychology
Research Data
sj-xlsx-6-cll-10.1177_13591053231182218 – Supplemental material for Words matter: The use of generic “you” in expressive writing in an oncology setting
Supplemental material, sj-xlsx-6-cll-10.1177_13591053231182218 for Words matter: The use of generic “you” in expressive writing in an oncology setting by Stella Snyder, Kathrin Milbury, Richard Wagner and Lorenzo Cohen in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as ![]() via the sage Journals platform. Ethical approval, participant permissions, and all other relevant approvals were granted for this data sharing.
via the sage Journals platform. Ethical approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by the NCI grant R01CA090966 (PI, Lorenzo Cohen, PhD); the Richard E. Haynes Distinguished Professorship for Clinical Cancer Prevention at the University of Texas MD Anderson Cancer Center (L Cohen); and by the NIH/NCI through MD Anderson’s Cancer Center Support Grant (P30CA016672). ClinicalTrials.gov: NCT00505310.
Ethical approval
All procedures were approved by The University of Texas MD Anderson Cancer Center Institutional Review Board, protocol ID00-168, and written informed consent was obtained prior to data collection.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.