
Abstract
The aim of this study was to describe the experiences of post-sedation COVID-19 patients in rehabilitation. Eleven Israeli men and women were interviewed in semi-structured interviews. They were patients recovering in a neurological rehabilitation unit from severe COVID-19 post-mechanical ventilation and sedation. Five themes were generated through thematic analysis: “an unexpected turn of events,” “filling the gaps,” “emotional reactions,” “ambiguity regarding medical condition,” and “sense and meaning-making.” Findings suggest a need for improved communication between patients and medical staff to enhance a sense of control and coherence. Psychological support should be considered to facilitate sense and meaning-making processes during hospitalization.
COVID-19 is caused by a strain of the coronavirus, the severe acute respiratory syndrome coronavirus 2, universally known as SARS-CoV-2 (Sanche et al., 2020). As of February 2022, there have been over 392 million confirmed cases cumulatively and over 5 million deaths worldwide (World Health Organization, 2022). In Israel, there have been close to 3 million confirmed cases cumulatively, over 1100 severe cases of hospitalization, and 9000 deaths (COVID-19 National Information and Knowledge Center, 2022).
Since its announcement as a global pandemic, information regarding the ramifications of contracting the disease accumulated steadily thanks to the quick response of the scientific and medical communities. Records show that 20% of COVID-19 patients follow a severe course which requires hospitalization (Tzotzos et al., 2020). Research has indicated that the most critically ill patients experience acute respiratory distress syndrome (ARDS) and require sedation, mechanical ventilation, and even the use of extracorporeal membrane oxygenation (ECMO) (Hosey and Needham, 2020; Namendys-Silva, 2020). A growing number of studies have reported longer term post COVID-19 neurological effects in association with a severe course of COVID-19, which is recognized as PCNS (Post COVID-19 Neurological Syndrome) (Heneka et al., 2020; Serrano-Castro et al., 2020; Wijeratne and Crewther, 2021).
Research on the use of sedation, mechanical ventilation, and ECMO, to treat other medical conditions, such as heart and lung disease, has indicated that these treatments can involve enduring effects of psychological distress and trauma (Tramm et al., 2016; Worsham et al., 2021; Zhang et al., 2021). Studies reported that patients who had undergone treatment with ECMO experience patchy factual memories, detailed delirious memories, paranoid ideations (Tramm et al., 2016), and often also experience depression, anxiety, and PTSD, post-hospitalization (Zhang et al., 2021).
It is well-documented that severe COVID-19 can also involve extensive psychological complications, such as cognitive disorders, mood and anxiety disorders, hallucinations, and even psychosis (Paterson et al., 2020; Rogers et al., 2020; Wijeratne et al., 2021). The discovery of pervasive mental health effects, in combination with the high incidence of patients hospitalized with severe COVID-19, generated research exploring the experiences of patients during hospitalization (Hao et al., 2020; Sun et al., 2020).
Research specifically focusing on the mental health experiences of patients hospitalized with COVID-19 is also extensive (Pistarini et al., 2021; Son et al., 2021; Sun et al., 2021; Zhang et al., 2022). In an exploratory survey study, researchers assessed and compared the neuropsychological deficits and emotional disturbances of patients in the subacute phase of COVID-19 and of patients who were in rehabilitation post-hospitalization. Post-hospitalization patients in the study experienced significantly higher levels of distress in comparison to patients in the subacute phase (Pistarini et al., 2021). Studies on hospitalized COVID-19 patients have also identified high levels of anxiety and depression symptoms as well as feelings of social disconnection and an increased risk for the development of post-traumatic stress post-hospitalization (Matalon et al., 2021; Sun et al., 2020). Another study found high levels of anxiety specifically associated with feelings of isolation during hospitalization (Dorman-Ilan et al., 2020).
There is a growing body of qualitative studies on hospitalized COVID-19 patients. In one qualitative study, researchers interviewed COVID-19 patients during hospitalization and found that they expressed emotional responses dependent on the stage of the disease; negative emotions dominated early stages, then gave way to mixed positive and negative emotions (Sun et al., 2021). In another qualitative study, researchers interviewed COVID-19 patients who had been discharged from hospitals following treatment in isolation. These patients expressed shock and dissatisfaction due to an excessive invasion of privacy during quarantine and described experiencing social stigma and feelings of guilt (Son et al., 2021). Interviews with hospitalized COVID-19 patients, age- and gender-matched psychiatric patients, and healthy controls, revealed that COVID-19 patients were significantly more worried about their health than healthy controls (Hao et al., 2020). These patients also reported feelings of shock, fear, despair, boredom, and hope.
To date, the mental health experiences of post sedation and mechanical ventilation COVID-19 patients in rehabilitation remain under-researched. The present study addresses this research gap and explores the psychological experiences of these COVID-19 patients.
Methods
Study design and participants
Participants were recruited through purposive sampling from the inpatient unit in the Department of Neurological Rehabilitation at Sheba Medical Center in Israel. Inclusion criteria for patients were: (1) 18 years old and older; (2) COVID-19 diagnosis; (3) initial admission to the ICU with ARDS; (4) sedation and invasive mechanical ventilation during ICU stay; (5) having suffered from Post-COVID-19 Neurological Syndrome (PCNS); (6) hospitalized at the time of recruitment in the neurological rehabilitation inpatient unit for multidisciplinary rehabilitation.
All patients in the department at the time who met the inclusion criteria were approached by Avital Gershfeld-Litvin, a senior psychologist in the department, regarding participation in the study. As the senior psychologist in the department, she did not treat any of the patients who were approached. Other psychologists working in the department provided psychological treatments to these patients upon request. It was made clear to all patients who were approached that the study was not linked to nor going to affect the medical and psychological treatment they receive during their stay in the department.
Eleven patients who met all criteria were interviewed for the study: nine men and two women, aged 44–64 (M = 52.9, SD = 6.37) (see Table 1 for demographic and medical characteristics). All participants were Jewish Israelis. Almost all participants identified as observant or religious. Interviews were conducted in Hebrew and lasted 45 minutes on average (between 30 and 60 minutes). Identifying information was removed from all transcripts to ensure anonymity, and all recordings and transcripts were saved under password protection to ensure confidentiality. Participant quotes were translated into English by Itay Ressler, a native speaker of Hebrew with bilingual proficiency in English, in agreement with Avital Gershfeld-Litvin.
Participant demographic and medical characteristics.
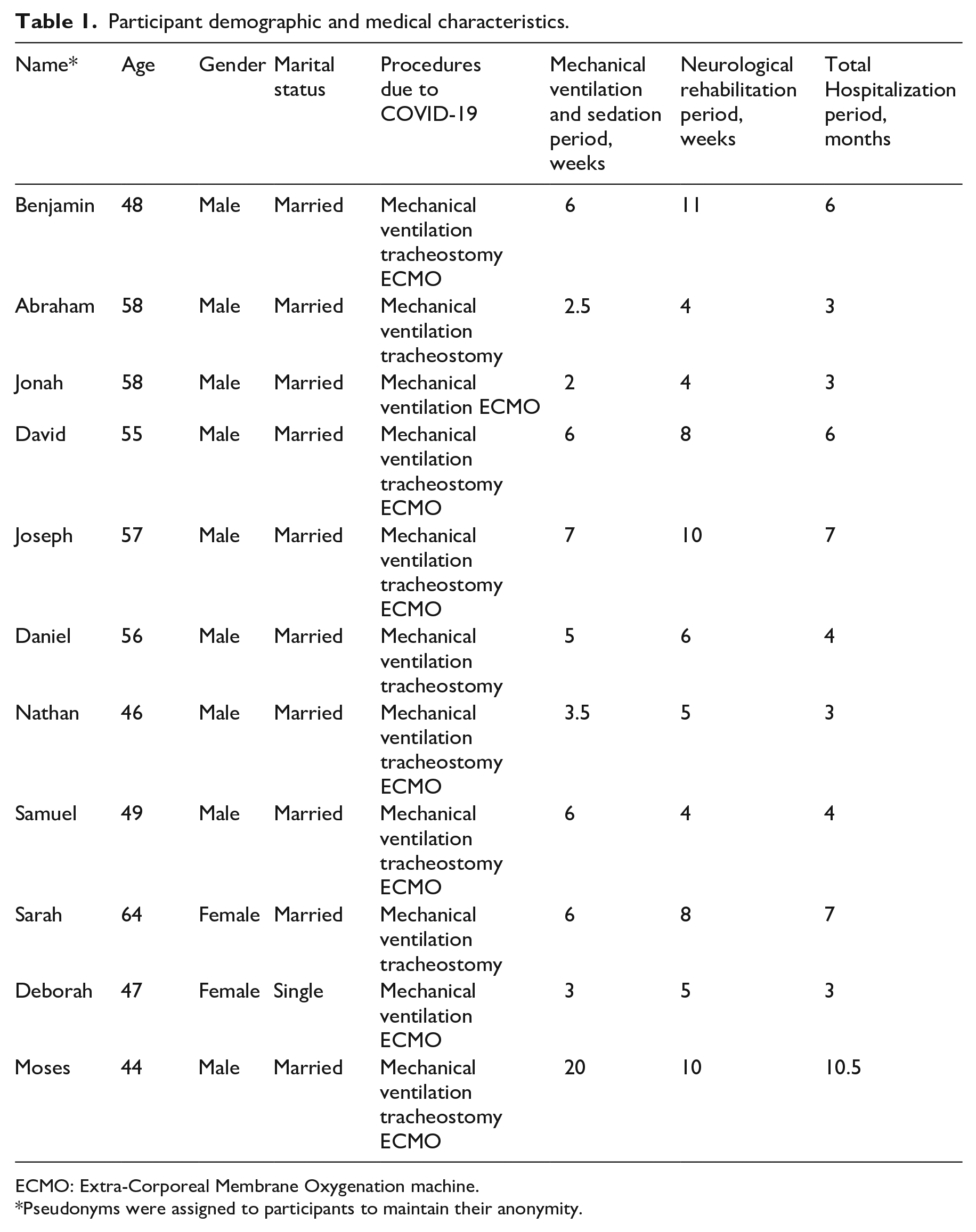
ECMO: Extra-Corporeal Membrane Oxygenation machine.
Pseudonyms were assigned to participants to maintain their anonymity.
Procedure
This study received ethical approval by the institutional review board at Sheba Medical Center (SMC-7558-20). Oral and written informed consent was obtained from all patients prior to their participation. Participants were interviewed by Avital Gershfeld-Litvin, a senior psychologist in the department of neurological rehabilitation, who did not treat any of the patients who were approached or participated in the study. In case of distress, professional mental health support was available to participants, free of charge, from other psychologists in the department. Interviews were semi-structured and conducted between March 7 and September 30, 2021. All interviews were conducted face-to-face in the participants’ rooms and audio-recorded with their permission. The following information was gathered at the start of each interview: age, marital status, date of hospitalization with severe COVID-19, procedures undergone, discharge status, neurological symptoms upon admission to neurological rehabilitation, and total hospitalization duration.
A general question was used as an opener: “Please tell me about your experience from the moment of diagnosis and until now.” The ensuing questions were a mix of open-ended, follow-up, and exploratory questions, including: “What is it like to be a COVID-19 patient?”; “What did you feel throughout the various stages of the disease, and how are you feeling right now?”; “How did you cope with the various stages of the disease?”; “What was the most difficult moment for you, and what has been the most difficult aspect to cope with?”; “Could you describe the responses you received from your close social circle (family, friends)? Have they changed over time?”; and “What is your greatest fear when you think about the future?”
Data analysis
Data analysis began while data collection was still on going. Braun and Clarke’s (2006) method for thematic analysis was used to analyze the data. Transcripts were read and re-read several times, allowing for familiarization with participants’ tone and messaging. Initial codes were then generated from each transcript. Codes were then grouped together into elevated categories on the basis of belonging to the same conceptual plain. Categories were subsequently sorted into themes, and full theme descriptions were created. Themes were then reviewed to identify whether they could be better defined or refined. Upon unanimous agreement among the researchers, the most descriptive extracts were selected from the transcripts to complement relevant themes.
The integrity of the data was ensured through several steps. First, Braun and Clarke’s (2006) six-step method for thematic analysis was followed from beginning to end. Additionally, the researchers, both of whom are psychologists who have worked in hospital settings, analyzed the transcripts independently and then compared and debated them until unanimous agreement was reached on both themes and extracts. The generalizability of the data was considered, as evinced by the relative heterogeneity of the sample and the demographic and disease-related data collected.
Researcher reflexivity
The researchers are experienced in the field of medical psychology. Both researchers have worked in hospital settings with patients suffering from neurological disorders. The researchers have extensive experience in the collection and interpretation of qualitative data; experience gained through conducting multiple qualitative studies in their field. Taking potential biases into consideration, the researchers discussed their analyses with each other throughout the study. Any disagreements on themes and excerpts were resolved through discussion and exploration of alternative explanations for both data and conclusions. Unanimous agreement on themes and extracts served as a prerequisite for them to be included in the final manuscript.
Findings
Five themes were generated (see Figure 1): “an unexpected turn of events,” “filling the gaps,” “emotional reactions,” “ambiguity regarding medical condition,” and “sense and meaning-making.”
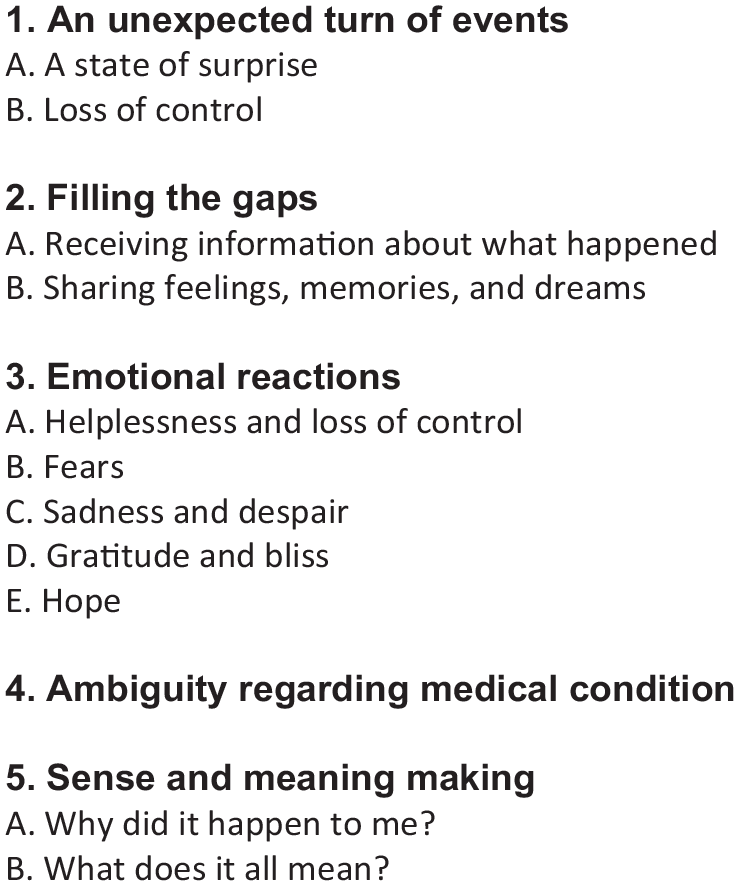
Themes and sub-themes.
First theme: “An unexpected turn of events”
This theme consists of sub-themes that correspond to a chronological timeline of unexpected events. All participants went through several stages during their experience with COVID-19: diagnosis, ICU, sedation, ventilation, waking up, physical and neurological dysfunction, and rehabilitation. The first sub-theme was labeled “a state of surprise.” Every stage was experienced as unexpected and riddled with doubt and confusion. Patients felt unprepared and found it difficult to reorient themselves thereafter: “I was very surprised. I wasn’t ready for this [contracting COVID-19]. I wasn’t hanging out outside; I was careful” (Sarah).
The second sub-theme was “loss of control.” Feelings of surprise, confusion, and uncertainty as well as physical constraints led to an increasing feeling of losing control. Patients felt under extreme duress and completely reliant on medical staff for both information and comfort: “I felt I was suffocating. It was a very stressful feeling. You feel real distress. . .I asked the doctor, ‘Will I wake up later?’” (Benjamin). Concerns for the future were expressed, with the prospect of full recovery unclear throughout most of the hospitalization period: “I don’t know if I will ever return to being who I used to be” (Daniel).
Second theme: “Filling the gaps”
This theme reflected patients beginning to fill in the gaps of their experience after waking up from sedation. The first sub-theme was “receiving information about what happened.” Patients were engaged in gradually learning details about their physical and mental condition and about the experience of their close relatives and caregivers: “After [I woke up] they told me what had happened. My family was told I had a 5% chance [of survival]. My relatives cried” (Joseph); “A friend from work came to visit me and told me that someone from work had died. I was in shock, started crying and trembling. . ..I called my boss and asked why I hadn’t been told sooner. He said he didn’t want to add to my sorrows” (Daniel); “I was told by my family and my doctor that I had died. They did not expect me to come back [from the dead]” (Benjamin).
The second sub-theme was “sharing feelings, memories, and dreams.” After waking up from sedation, patients began to recognize feelings, memories, and sometimes dreams they had had during and after the sedation and ventilation period. A significant psychological aspect of this stage was whether they could remember anything and, if they could, whether they were willing to share it with others or not: “After I woke up, I asked people if they had been present in certain situations. They said, ‘What are you talking about?’, which is when I realized I had been dreaming” (Abraham); “I was told I had been shouting, ‘Go away, leave me alone’” (Jonah); “I feel pain for the people around me, my wife, my parents. They thought I had been closer to death than life” (Nathan).
Third theme: “Emotional reactions”
Patients described experiencing different emotions and frequent changes in emotional intensity throughout their hospitalization. The first sub-theme was “helplessness and loss of control.” Patients felt helpless, realizing they had no control over their own bodies. Helplessness manifested in a need to be told about actions and procedures they were supposed to undergo. Confusion and lack of knowledge particularly contributed to this feeling. In essence, patients felt they needed medical staff to be more attentive to these feelings: “I felt like I had been kidnapped and taken somewhere, all tied up, without being able to move. . .I didn’t understand. I needed someone to tell me, ‘You are in the ICU now’” (Jonah); “That’s when I started to feel limited. . ..I couldn’t raise my arm, it felt like a heavy load. I couldn’t move. It was horrible. The feeling was hard [to bear]. You want to get up but can’t” (Nathan).
The second sub-theme was “fear.” Patients experienced fear in various stages of their coping experience and were mostly afraid of death. For some, fear manifested in nightmares. For others, fear was more prominent when they reached the rehabilitation stage. Fear was inherent to the experience, an almost constant companion, and affected decision-making and the ability to cope: “I was afraid I wouldn’t make it. I immediately asked for a notary [and] had my eldest child and my wife sign [papers] to become my legal guardians. I was afraid I would die. I didn’t know what complications awaited me” (Daniel); “There was one night when I thought I was going to die. . .I was afraid I might have [suffered] heart damage” (Deborah); “I’m afraid of something that didn’t use to scare me – what if it [COVID-19] happens to my family? It’s been bothering me recently” (Moses).
The third sub-theme was “sadness and despair.” Some patients were overcome with feelings of desperation due to both a long isolation period and, partially, feelings of helplessness and loss of control: “They said I once yelled out for my son, ‘Save me!’ I don’t know if and how he could hear because of the mask, but I turned wild, and eventually they said that he had come [to visit]” (Jonah); “When I woke up, I felt broken. Like the world had turned upside down. . ..They lifted me with a crane onto a chair. It was embarrassing and really got me down. I felt discouraged and didn’t want to do anything” (David).
The fourth sub-theme was “gratitude and bliss.” Such feelings were less common but were, nonetheless, profound and elaborate. While patients were grateful to be alive, it was not necessarily the most pronounced aspect of their experience for which they felt most grateful. Rather, they expressed renewed or newfound appreciation for the “little things” in life: “[First shower after two and a half months] Bliss. When I came out of the shower and sat down on the bed, I said: ‘God, I’m in heaven.’ I forgot about all the numbness. It was incomprehensible” (Abraham). Facing and vanquishing the challenge of COVID-19 led to feelings of gratitude and joy, even when reflecting on the prospect of rehabilitation: “If the challenge is ahead of you, it [only stands to] increase the joy. Mending comes out of hardship. Hardship occurs, a rupture, and out of it comes the mending. It lets you into the club of those who feel they have purpose in life. I hope to use it [in future]” (Nathan).
The fifth sub-theme was “hope.” Hope was, in a sense, both a feeling and a coping mechanism. In the rehabilitative stages of the experience, hope was renewed when patients noticed improvements in their condition. It worked as a coping mechanism when lingering effects of sedation and ventilation suddenly became more bearable: “Do I feel like a convalescent from COVID-19 – Yes. Because my breathing is regular. When I arrived at the [rehabilitation] ward, I couldn’t get out of bed, I was lowered onto it with a crane. . ..I’ve been trying not to focus on the limiting factors, but to look onward with hope, to move on” (Benjamin); “I can see the progress all the time. When I arrived [at the rehabilitation ward], I couldn’t walk. Today I [can] walk. I was home on Saturday, and I walked down the stairs. When you see progress, there is hope” (Nathan).
Fourth theme: “Ambiguity regarding medical condition”
Upon arriving at the rehabilitation ward, all patients were diagnosed with critical illness polyneuropathy, required oxygen, and were physically impaired in movement and sensation after waking up from sedation. Some had a tracheostomy. While they did not feel physically sick with COVID-19, they did feel disabled due to a prolonged period of requiring the use of either a wheelchair or a walker, being assisted with feeding and bathing, and being unable to use the toilet on their own. Patients described their day-to-day coping as painful and characterized mostly by dependence on others. These aspects of their experience contributed to a sense of ambiguity regarding their medical condition: “[It’s] the disability that remained. I try to make peace with it, but it’s not exactly [what I want], because I do want to improve. . .Maybe I’m repressing the situation, I keep telling myself I’ll make it when I leave here” (Sarah); “I feel like I’ve recovered from COVID-19, but my body isn’t the same as it used to be. I used to be an athlete, a working man” (Daniel); “When I’m off the oxygen I’ll feel that I’m through with it. The oxygen reminds me the most [of COVID-19]. Only then will I feel back in shape, a convalescent” (Jonah).
Fifth theme: “Sense and meaning-making”
This theme comprised several ways in which patients attempted to make sense of their condition and explain why they got sick in the first place. They also found meaning in their experiences. The first sub-theme was “why did it happen to me?” Non-religious participants focused on personal lifestyle choices as an explanation: “Before COVID-19, I had been working very hard and I’ve [now] lost my patience. . .I learned that I need to choose life anew. . .I was worn out and tired; I needed a restart” (Deborah). Religious participants contextualized their condition through faith. For some, it manifested as a spiritual crisis: “I feel a spiritual decline. I hardly pray. . .[it’s] like a barrier. I don’t understand why. I should be more grateful and devout. . .I’m angry at myself [for it]” (Sarah).
For others, their survival strengthened their faith: “It is enlightening that God intervened and with His grace brought me back to life. I don’t know why I deserve it, [but] I got another chance” (Benjamin).
The second sub-theme was “what does it all mean?” Patients found themselves reflecting on their experiences, pondering the meaning behind them. These reflections allowed them to move on while remaining in some contact with their experience and the changes and losses it incurred. Patients focused on ways to move forward that would constitute an improvement in various aspects of their lives prior to COVID-19. They felt a need to make changes, to avoid a repeat of this experience and to feel that they had earned the “second chance” they had received: “By now I’ve learned my lesson, to take it easy” (Deborah); “I will appreciate the little things in life. . .Like getting out of bed, putting on shoes. . .making myself a cup of coffee” (Moses); “I was given a great auxiliary tool for life – the realization that I’m not the master of my own life, [yet] there is purpose to it. . .It emphasizes that time is limited and there is so much to do” (Nathan).
Discussion
This study explored the psychological experiences of patients rehabilitating from a severe course of COVID-19 which involved sedation and mechanical ventilation. The first encounter of patients with COVID-19 was felt as a sudden shock. Surprised by the realization that the disease could still be contracted despite careful maintenance of socially-distanced and highly hygienic behavior, a sense of disillusionment was the first sign of what was to come in terms of both the perceived and actual ability to control their condition. From diagnosis to recovery, feelings of uncertainty and loss of control dominated. Patients primarily attributed these feelings to their dependence on medical staff for information regarding their condition. Other studies have also reported that people who had been hospitalized with COVID-19 felt uncertainty about their health status as well as loss of control, which led to increased levels of stress (Matalon et al., 2021; Son et al., 2021).
COVID-19 patients who had been diagnosed with ARDS were sedated and mechanically-ventilated for a period of several weeks at the least. This period acted as a gap in their memory of the experience. On waking up from sedation, patients engaged themselves in attempts to fill this gap by acquiring information about what had transpired. However, this proved challenging as the information was not always clearly organized and communicated to them and the content itself was often difficult to access, contain, and process. This created a dynamic where patients did not feel they could share their remembered experience with close relatives and friends. Searching for information about the sedation period and finding it difficult to share once recalled or discovered seem to be novel aspects of the experience of hospitalized COVID-19 patients. It emphasizes patients’ reliance on medical staff for information which, in turn, calls for better communication between staff and patients during hospitalization to help shape the narrative of their experience.
The volatile nature of COVID-19, particularly during hospitalization, fostered a sense of ambiguity among patients regarding their health status. They felt a dissonance between their formal status as convalescents and the fact they were still coping with long-lasting effects of the disease, namely, physical disabilities and cognitive impairments. These aspects coincide with literature on physical and psychological trauma, particularly regarding the experience of acquired physical conditions. It has been found that the physical trauma experienced by severe COVID-19 patients is interrelated with psychological trauma (Kaseda and Levine, 2020; Nagarajan et al., 2022; Tarsitani et al., 2021). People who experience abrupt and fundamental changes to their bodily experience, following an acquired medical condition, may also experience psychological disruption to the foundations of their self-knowledge, self-constitution, and core beliefs (Negri et al., 2023; Segal, 2018).
Several studies exploring the experiences of patients hospitalized with COVID-19 found that patients described the disease as confusing and ambiguous (Khoshnood et al., 2021; Ladds et al., 2020). However, the present study seems to be the first to report a sense of dissonance among COVID-19 patients in rehabilitation. Resolving the dissonance in the rehabilitation stage is probably not a realistic expectation as patients are only beginning to grapple with it at that point. Patients could, nonetheless, benefit from psychological support during rehabilitation to facilitate the emotional and cognitive processing of the ramifications of their condition.
The expression of various emotional reactions documented in the present study corresponds with evidence from recent studies. A few studies have reported positive emotional reactions during hospitalization, such as gratitude toward medical staff and hope for the future (Olufadewa et al., 2020; Sun et al., 2021). However, the foundations of gratitude may differ. In the present study, patients were mostly grateful for the role of their faith in ensuring their survival and, to a much lesser extent, the medical staff. There is substantial research on the experiences of hospitalized and post-hospitalization COVID-19 patients reporting negative emotional reactions, including loneliness, despair, helplessness, fear, and confusion (Jamili et al., 2022; Rogers et al., 2020; Son et al., 2021). These feelings were associated with difficulty accepting the diagnosis but also manifested in later stages of hospitalization when ambiguity and loss of control dominated the patients’ psychological experience.
Sense and meaning-making were also found to be integral to the experience of COVID-19 patients in rehabilitation. These processes are associated with other themes, including a sense of ambiguity regarding medical condition and negative emotions (confusion and helplessness). All participants were found to engage in these processes. This finding is in line with literature on coping with physical and psychological trauma, as in the case of COVID-19. Research has emphasized the role of sense and meaning-making in reducing the risk for trauma – the more one can make sense of a traumatic event, the lesser the negative impact the event has on one’s mental health (Negri et al., 2023; Neimeyer, 2019).
Meaning-making did not exclusively revolve around the reasons one got sick, as particular attention was paid to the facts of survival and recovery. Most of the participants in the present study were religious and engaged faith or spirituality both as a coping mechanism and as an inherent part of their belief system. Research on the role of spirituality among COVID-19 patients has suggested that the impact of coping with the disease on faith is, on average, less significant than its impact on finances, work, family, and emotions (Pirutinsky et al., 2020). However, religious patients in the present study reported experiencing either a spiritual crisis or reinforcement of their faith. Non-religious patients felt that they had got sick due to their pre-disease lifestyle. Further research is needed to ascertain the role of spirituality and faith in coping with COVID-19 and the effects of the disease on faith.
The present findings should be considered within the context of some limitations. The researchers recognize that the size and uneven composition of the sample may limit one’s ability to draw conclusions regarding the roles of faith and gender in the experience of severe COVID-19 patients. The sample included predominantly observant religious Jewish men and consisted of eleven participants in total. A small sample may hinder generalizability, although this is not a goal of qualitative research and was not a stated goal for the current research. Gender differences in COVID-19 hospitalization rates have been unclear and different studies have shown various trends (Dehingia and Raj, 2021; Gomez et al., 2021; Jin et al., 2020). Since trends of hospitalization and mortality are still being analyzed and debated by the medical community, the authors primarily focused on presenting the subjective experiences of patients irrespective of their gender. Another possible limitation is that patients were interviewed following rehabilitation for neurological damage, which might have influenced the narratives they shared. While enabling a unique point of view, this requires caution in interpreting the narratives. Lastly, there was no follow-up with patients after they had been discharged from the hospital, which leaves the experience of the later stages of rehabilitation largely unexplored.
The present study suggests that severe COVID-19 patients cope not only with a life-threatening condition but also with long-lasting physical and psychological ramifications that require special consideration. Disability and loss of control warrant medical staff providing the patient and their family with detailed explanations about the patient’s condition, even during the sedation period. This helps to increase the patient’s sense of coherence and control when they most need it. Psychological support should facilitate sense and meaning-making processes during hospitalization, as it can help patients dispel ambiguity regarding their health status and regain control, which may assist in reducing the risk of COVID-19-related traumatic stressors. While several studies have found that psychological interventions can alleviate distress among COVID-19 patients (Foley et al., 2020; Rossi Ferrario et al., 2021), further research is needed to develop effective interventions aimed at restoring control and a sense of a coherent self to COVID-19 patients during and after hospitalization.
Research Data
sj-pdf-1-hpq-10.1177_13591053231174940 – Supplemental material for Psychological experiences of patients recovering from severe COVID-19 in rehabilitation: A qualitative study
Supplemental material, sj-pdf-1-hpq-10.1177_13591053231174940 for Psychological experiences of patients recovering from severe COVID-19 in rehabilitation: A qualitative study by Avital Gershfeld-Litvin and Itay Ressler in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the Sage Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the institutional review board at Sheba Medical Center (SMC-7558-20).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.