
Abstract
This study aimed to evaluate the work ability and its associated factors in patients with glioma (II, III) and breast cancer after 6 (T0) and 12 (T1) months from surgery. A total of 99 patients were evaluated with self-reported questionnaires at T0 and T1. Correlation and Mann–Whitney tests were used to investigate the association between work ability and sociodemographic, clinical, and psychosocial factors. The Wilcoxon test was used to investigate the longitudinal change in work ability. Our sample showed a decrease in work ability level between T0 and T1. Work ability was associated with emotional distress, disability, resilience, and social support in glioma III patients at T0, and with fatigue, disability, and clinical treatments in patients with breast cancer at T0 and T1. Work ability levels decreased in patients with glioma and breast cancer and were associated with different psychosocial factors after surgery. Their investigation is suggested to facilitate the return to work.
Introduction
This study is part of a larger project funded by the Lombardy Region (Italy) aimed at identifying the way patients with cancer are followed-up after surgery with curative intent. Glioma and breast cancers were chosen as the best case models since they are similar with respect to the lacking of a well-defined follow-up strategy (Moschetti et al., 2016; Weller et al., 2017). Glioma is a type of brain tumor arising from glial or precursor cells and including from benign grade I, predominant in children and young adults, to grade IV, whose incidence increases in older age (McNeill, 2016). On the contrary, breast cancer is the most common cancer among women. In Italy, an estimated 55 million new cases of breast cancer were diagnosed last year, accounting for 30.3% of all tumor frequently diagnosed (AIOM, 2021). Together with the identification of the patients’ follow-up (Silvaggi et al., 2022), this project included also a study on work ability and its associated factors during the post-surgical period.
Work ability is defined as the balance between the job demand and the individual physical and cognitive resources. It is a dimension evaluating whether an employee is able to do his/her job in the present and the future, in relation to the job demands, the work environment, and his/her own mental and physical resources (Ilmarinen, 2009). Work ability is also determined by professional knowledge and competence (skills), values, attitudes, motivation, the type of work, and the working environment (Van Den Berg et al., 2008). We are interested in exploring patients’ work ability because it is one of the main factors affecting the return to work process among cancer survivors (Feuerstein et al., 2007; Harrington et al., 2010). In recent years the number of people who recover from cancer has significantly increased thanks to advances in diagnosis and treatment (Aaronson et al., 2011). Furthermore, the evaluation of work ability is promoted by the recent EU Joint Action with the development of the Chrodis Plus toolkit for workplaces, a training tool for managers to improve inclusion and work ability in all workers with chronic health conditions including patients with cancers. In addition to work ability, other factors that can play a role in return to work include age, gender, income, employment type as well as supervisor and co-worker relationships, availability of work adjustments and perceived workplace support (Berry, 1993; Blinder et al., 2013), type and severity of cancer, treatment type, and other disease-related factors and symptoms such as fatigue, pain, and concentration problems (Baqutayan, 2012; Hoofien et al., 2011).
Glioma and breast cancer are suitable for the study of work ability: the first one mainly for the impact of disease and treatment on the cognitive status; the second one because the breast cancer mainly affects women increasing their difficulties in maintaining the balance between work and family life.
Among the various types of cancer, patients with glioma II and III are less likely to return to work due to the side-effects of treatments, clinical deterioration for tumor progression, fatigue, seizures, and cognitive complaints (Bouknight et al., 2006; Bradley and Bednarek, 2002). In addition, patients with glioma experience more disabling symptoms due to poor prognosis and lower survival despite increased treatment options (Batash et al., 2017). The most commonly experienced symptoms reported by glioma patients that impact daily life include tiredness, loss of autonomy, cognitive, and neuropsychiatric symptoms (Halkett et al., 2010; Molassiotis et al., 2010; Schubart et al., 2008; Sherwood et al., 2006). Few studies specifically explored the return to work process in glioma patients. Patients with glioma who cannot manage the return to work often experience an increase in anxiety, depression and social isolation, a reduction in physical health, and a loss of identity (Campagna et al., 2020; Chen et al., 2021). However, to our knowledge, no studies exist on work ability in patients with glioma.
On the other hand, among potential factors associated with work ability in patients with breast cancer, some studies have found low income, fatigue, poor support from a supervisor, anxiety, and depression (Carlsen et al., 2013; Cheung et al., 2017). Specifically, depression was associated with lower work ability in approximately one-third of patients, who reported a change in their working conditions after cancer treatments (Kim et al., 2022). Regarding resilience, a study suggested that it could be a protective factor of work ability in a sample of patients with breast cancer: a high level of total resilience allowed them to perceive their illness in an adaptive way (Gómez-Molinero et al., 2019). Breast cancer survivors who experienced or perceived more physical or cognitive disability following treatments were more likely to have work difficulties with an impact on their productivity (Oberst et al., 2010). Schallig et al. (2021) analyzed the association between social support and work functioning founding that the supervisor’s social support was associated with better work functioning in patients with cancer who returned to work.
Therefore, a better understanding of which factors are associated with work ability could help to develop appropriate interventions to facilitate the return to work of patients with cancer.
Our study aimed to evaluate the work ability in patients with a diagnosis of glioma (II, III) and breast cancer at 6 and 12 months after surgery and to analyze the association between psychosocial factors and the work ability level during the postoperative course. As concerning the timing of evaluation of factors associated with work ability in the postoperative period, few studies reported that 44% of patients with cancer return to work after treatments between 6 and 12 months following diagnosis (Chen et al., 2021; Mehnert, 2011). In line with these studies, we hypothesized that 6 months was a good time to make sure that most patients returned to work.
Materials and methods
In this prospective observational study, we approached 54 patients with glioma and 79 patients with breast cancer undergoing tumor resection between March 2019 and July 2020 at the Neurological Institute C. Besta IRCCS Foundation and the Fondazione IRCCS Istituto Nazionale dei Tumori, in Italy. Among patients with glioma, 13 refused to participate or did not complete the questionnaires, 1 died and 2 were unemployed. Among patients with breast cancer, 17 refused to participate or did not complete the questionnaires and 1 had to undergo a second surgery. So a total of 99 patients were included in our study: 38 operated for glioma II or III, 18 women (mean age = 44; SD = ±9.59) and 20 men (mean age = 42; SD = ±10.16), and 61 women operated for breast cancer (mean age = 47; SD = ±9.94). For the aim of our study we included working-aged patients (18–65 years) who were employees (N = 56), workers (N = 16), freelancers (N = 21), occasional collaborators (N = 5), and entrepreneurs (N = 1). All patients were enrolled on a voluntary basis and they were evaluated at 6 months (T0) and 12 months (T1) after surgery. We excluded patients with psychiatric illnesses and/or taking psychotropic drugs reported in the medical records, patients with cognitive decline not related to the brain cancer, and patients with other cancer diagnoses. This study complied with the ethical standards of the Declaration of Helsinki and received approval from the Ethical Committees of both institutions. Written informed consent was obtained from all patients before their inclusion in the study.
Assessment protocol
Patients included in this study were contacted by phone and completed an online assessment protocol at T0 and T1. The protocol was composed of a section on socio-demographic data (gender, age, educational level, working situation, treatments) and the following self-reported questionnaires:
The HADS (Hospital Anxiety and Depression Scale) is a 14 items instrument on a 4-point Likert scale for the evaluation of emotional distress and is composed of two subscales evaluating anxiety and depression symptoms. The total score ranges from 0 to 42 with higher scores indicative of higher anxiety levels and depressive symptoms (Zigmond and Snaith, 1983).
The Oslo-3 Social Support Scale (OSS-3) is a tool for the evaluation of social support perceived by patients. It consists of three items that refer to the support that a patient could receive from close people. The score ranges from 3 to 14: scores below 9 indicate poor social support (Meltzer, 2003).
The Work Ability Index (WAI) is a questionnaire based on the self-assessment of present work capacity concerning seven elements: (1) self-assessment of present work capacity compared to the best period of life; (2) self-assessment of work capacity with the demands of the work task; (3) a number of current diseases diagnosed by a doctor; (4) estimate of the reduction in working capacity due to diseases; (5) absence due to illness; (6) forecast of the working capacity in the next 2 years; and (7) personal resources (feeling able to carry out the usual daily activities with satisfaction; feeling active and alert; feeling full of hope for the future). High values correspond to high levels of work ability (the scores range from 7 to 47 points: 7–27 poor work ability; 28–36 moderate work ability; 37–43 good work ability; and 44–47 excellent work ability) (Tuomi et al., 1998).
EORTC QLQ-FA12 (FA-12) is a module developed by the European Organization for Research and Treatment of Cancer for the assessment of fatigue in patients with cancer. It consists of 12 items that measure specific forms of fatigue (physical, emotional, and cognitive) and the interference of fatigue with the activities of daily life and social life. The score ranges from 0 to 100: higher scores indicate more fatigue (Weis et al., 2017).
The 14-item Resilience Scale (RS-14) is a scale evaluating resilience. The responses to the items are expressed on a Likert scale ranging from 1 (strongly disagree) to 7 (fully agree). Higher scores correspond to higher resilience levels: <56 very low, from 57 to 64 low resilience, from 65 to 73 medium, from 74 to 81 moderate, from 82 to 90 moderately high, and >91 high (Callegari et al., 2016).
The Cognitive Failures Questionnaire (CFQ) is composed of 25 items on deficits in cognitive processes that can occur in daily life. The request is to estimate the frequency of the cognitive failures by indicating the most adequate response for each item on a 5-point scale that varies from “very often” to “never.” High values correspond to high levels of cognitive deficits (Broadbent et al., 1982; Salmaso et al., 1988).
The WHO Disability Assessment Schedule 2.0, second version (WHODAS 12 to 12 items) is a disability assessment tool providing a global disability score taking into account the difficulties patients meet in carrying out a series of activities due to their health state. Each item is rated on a scale of 1–5 (no difficulty–complete difficulty). High scores correspond to greater disability (Ustun et al., 2010).
The RS-14 questionnaire was not administered at T1 because it evaluates a stable construct over time; consequently, we do not expect a change from T0.
Statistical analysis
Descriptive statistics were used to illustrate the sample characteristics (socio-demographic, clinical data) and questionnaires scores at T0 and T1 (number and percentage for categorical variables and mean ± standard deviation for quantitative variables). We investigated the change in the WAI scores between T0 and T1 using the Wilcoxon test in the glioma II and glioma III samples and t-test in the breast cancer sample. Regarding the association between WAI and the psychosocial variables, specifically emotional distress (HADS), resilience level (RS-14), disability level (WHODAS-12), fatigue (EORTC QLQ-FA12), and cognitive deficits (CFQ), we used Spearman or Pearson’s correlation coefficient. Correlations were considered weak with coefficient values <.29, moderate with values between .30 and .59, and strong with values >.60 (Fisk et al., 2005). The association between WAI, clinical treatment, and job classification was also investigated using Mann–Whitney test and t-test. We did not analyze the correlation between WAI and clinical treatments in the sample of patients with glioma III since all patients underwent oral chemotherapy and/or radiotherapy. For these analyses, a two-tailed significance level of α = .003 was adopted since Bonferroni adjustment was applied to reduce type 1 error due to multiple comparisons.
All statistical analyses were performed using SPSS (version 24.0; SPSS Inc., Chicago, IL, USA) and the normality of data distribution was tested using the kurtosis and skewness values.
Results
We reported socio-demographic, clinical, and work-related variables in Table 1. On the total sample (N = 99), 22 patients (N = 13 breast cancer; N = 1 glioma II; N = 8 glioma III) were lost at follow-up for the following reasons: death, second surgery, COVID-19 emergency or because they were unreachable. In addition, 84% received adjuvant treatment at 6 months after surgery and 77% at 12 months after surgery.
Socio-demographic and clinical data in Glioma II, III, and breast cancer patients.
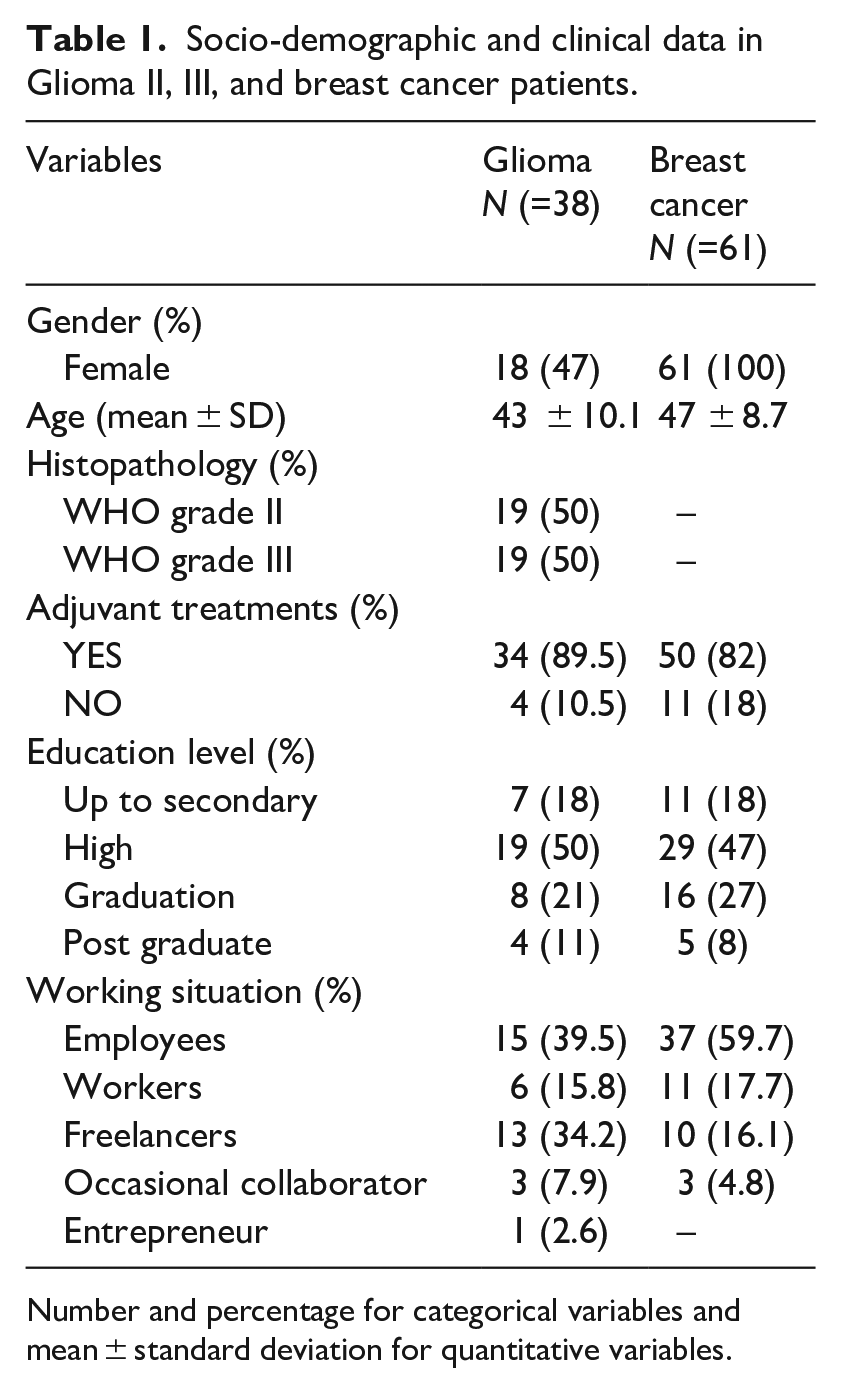
Number and percentage for categorical variables and mean ± standard deviation for quantitative variables.
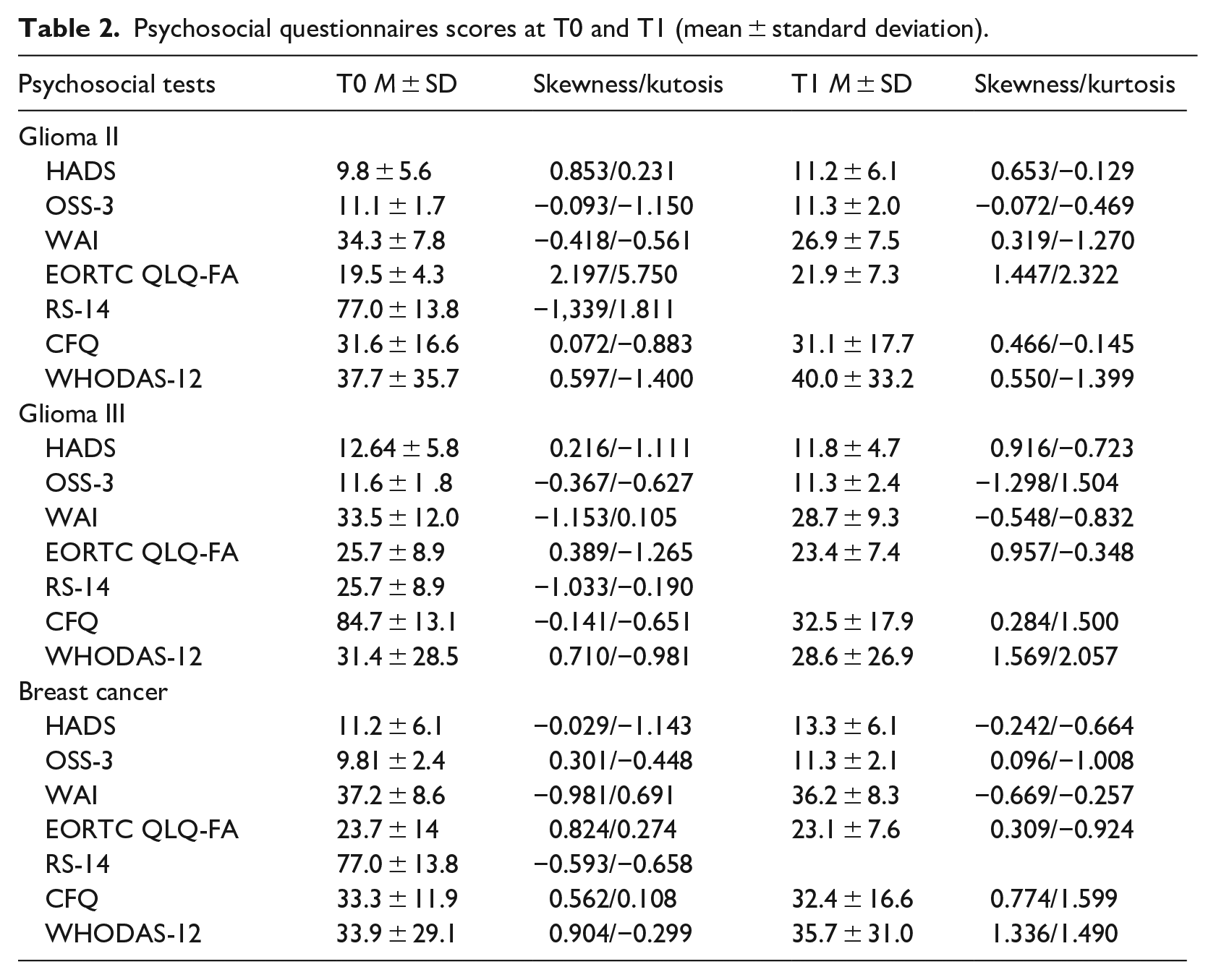
Table 2 reports the mean scores at the psychosocial questionnaires in patients with glioma and breast cancer at T0 and T1: in both groups, the mean scores of HADS indicated the presence of anxiety and depressive symptoms, the RS-14 scores indicated a moderate to moderately high resilience level, the mean scores of OSS-3, EORTC QLQ-FA 12, and CFQ were in line with the normative values, while the WHODAS 12 mean score was higher, meaning an increase in disability.
Psychosocial questionnaires scores at T0 and T1 (mean ± standard deviation).
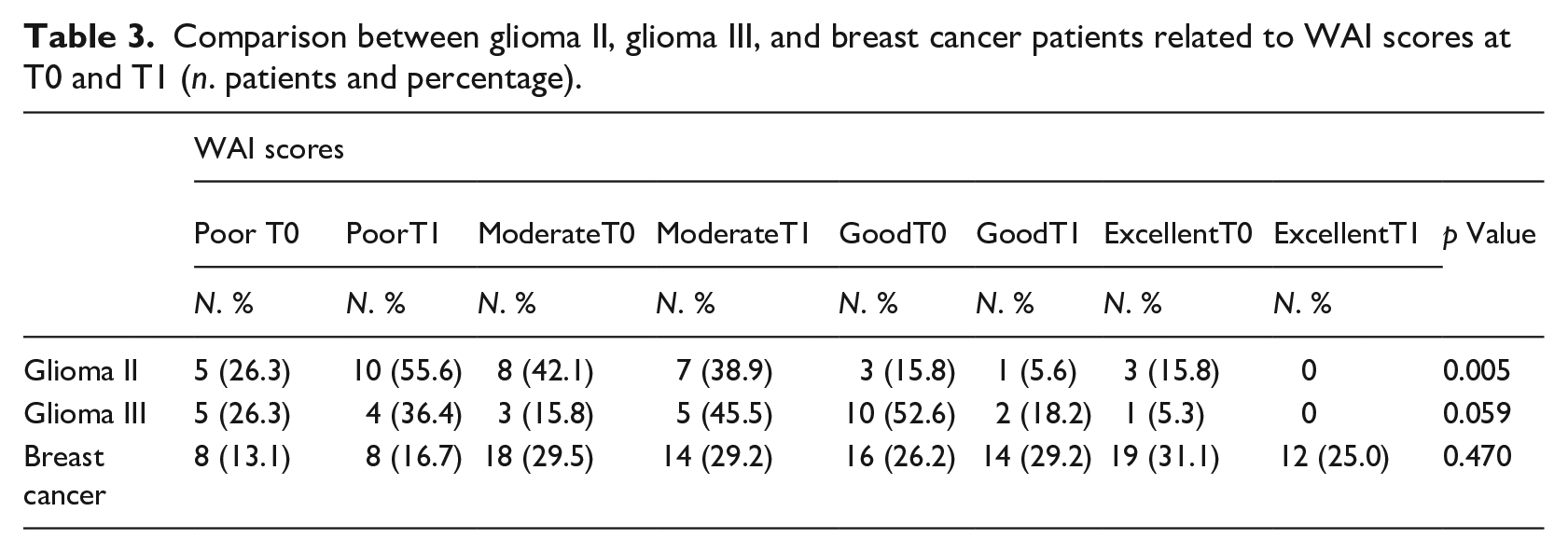
The longitudinal analyses showed a decrease in the WAI between T0 and T1 that was statistically significant in patients with glioma II (glioma II: z = −2.790, p = 0.005; glioma 3: z = −1.891, p = 0.059; breast cancer: t = 0.796, p = 0.470). Table 3 reports the details on the levels of work ability: the majority of patients with glioma II had moderate scores at T0 (42.1%) and poor scores at T1 (55.6%); most of the patients with glioma III had good scores at T0 (52.6%) and moderate at T1 (45.5%); most of the patients with breast cancer had excellent scores at T0 (31.1%), moderate (29.2%) and good (29.2%) at T1 (Table 4).
Comparison between glioma II, glioma III, and breast cancer patients related to WAI scores at T0 and T1 (n. patients and percentage).
Correlations between WAI and psychosocial questionnaires, sociodemographic and clinical data in glioma and breast cancer patients.
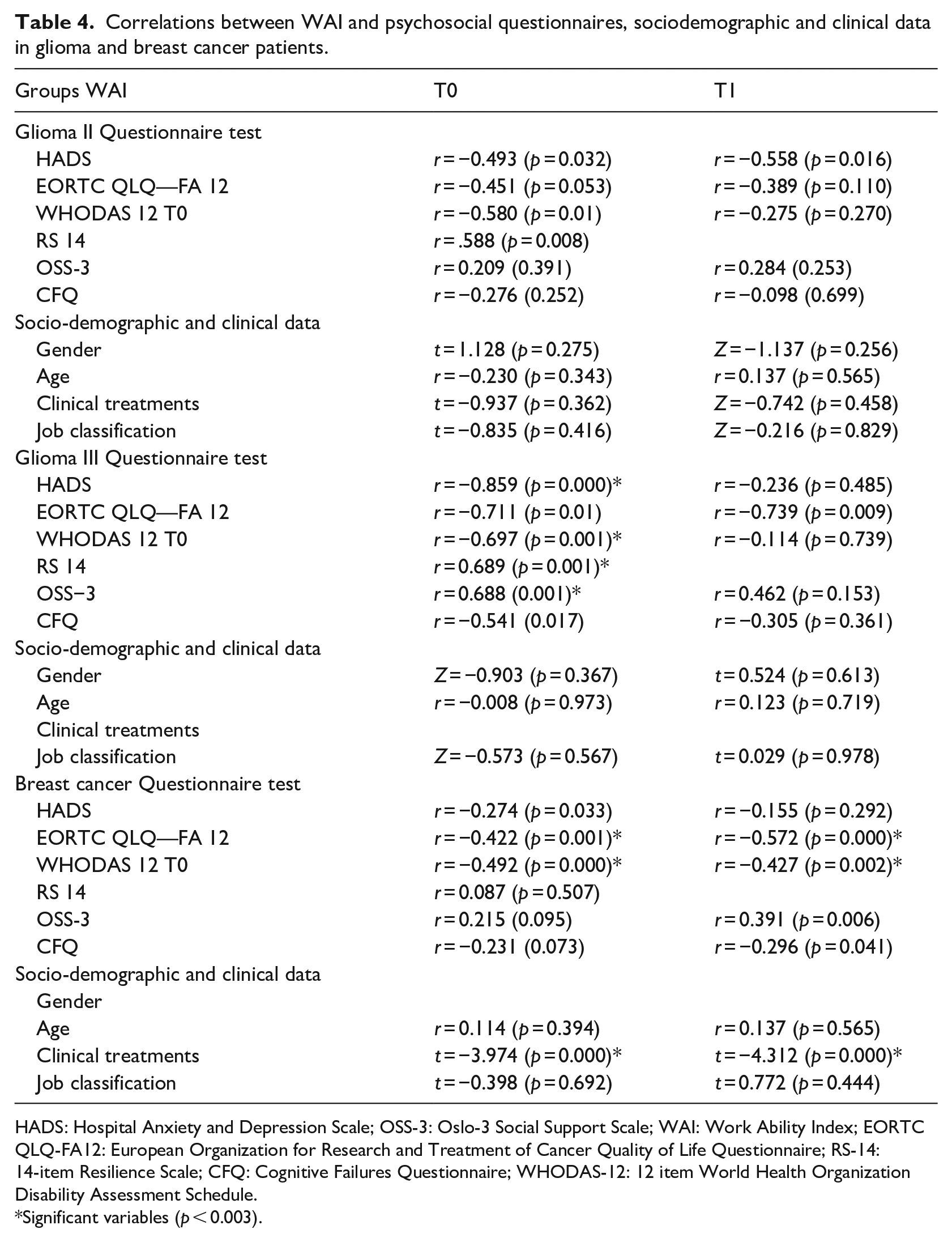
HADS: Hospital Anxiety and Depression Scale; OSS-3: Oslo-3 Social Support Scale; WAI: Work Ability Index; EORTC QLQ-FA12: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire; RS-14: 14-item Resilience Scale; CFQ: Cognitive Failures Questionnaire; WHODAS-12: 12 item World Health Organization Disability Assessment Schedule.
Significant variables (p < 0.003).
Correlations between WAI and questionnaires, socio-demographic, and clinical data
Glioma II and III patients
In the sample of patients with glioma III, HADS (r = −0.859; p = 0.000), WHODAS 12 (r = −0.697; p = 0.001), RS14 (r = 0.689; p = 0.001), and OSS-3 (r = 0.688; p = 0.001) scores at T0 were significantly and strongly correlated with the WAI at T0. We did not find statistically significant correlations between WAI and the questionnaires, socio-demographic, and clinical variables in the sample of patients with glioma II.
Breast cancer
The EORTC QLQ-FA 12 and WHODAS-12 scores and the clinical treatments had a significant and moderate correlation with the WAI both at T0 (EORTC QLQ-FA 12: r = −0.422; p = 0.001: WHODAS-12: r = −0.492; p = 0.000; clinical treatments: t = −3.974; p = 0.000) and T1 (EORTC QLQ-FA 12: r = −0.572; p = 0.000; WHODAS-12: r = −0.427; p = 0.002; clinical treatments: t = −4.312; p = 0.000).
Discussion
The main results of our study are the following: (1) patients with glioma and breast cancer show a decrease in work ability between 6 and 12 months after surgery, although the change is only statistically significant for Glioma II; (2) emotional distress, disability, resilience, and social support are associated with work ability after 6 months from surgery in patients with glioma III, while fatigue, disability, and clinical treatments are associated with work ability after 6 and 12 months from surgery in patients with breast cancer. Work ability levels decreased significantly between 6 and 12 months after surgery in patients with glioma II, while the remaining groups showed a non-statistically significant decrease. This could indicate that a substantial proportion of employed patients are not sufficiently able to balance the demands of their job with their physical and mental resources. Previous studies suggested that breast cancer and brain tumor survivors reported lower work ability and work limitations compared with no cancer individuals (Feuerstein et al., 2007; Hansen et al., 2008). When we investigated the relationship between work ability and psychosocial factors, we found that the factors associated with work ability were different according to patients’ clinical conditions and timing of assessment. Patients with glioma III showed the strongest associations between psychosocial factors and work ability. Specifically, the association between work ability and social support was strong after 6 months from surgery. Since it has been shown that patients with cancer experience limitations in work ability, employment and satisfaction with work (Mehnert and Koch, 2013), our results suggest that social support from family and friends and a stable social network could facilitate patients in the return to work process. According to our results, this seems to be particularly true in the first period after surgery which is the most critical due to the ongoing adjuvant treatments and the presence of clinical symptoms. The positive effects of social support were found in previous studies on patients with cancers: Götze et al. (2015) found that individuals with cancer reported a high level of perceived social support at all times of assessment (post-therapy, 6 months and 12 months after therapy) and that the increase in social support led to a decrease in psychological distress (Götze et al., 2015); another study demonstrated that social support is essential for the development of resilience and the improvement of quality of life (Zhang et al., 2017). We believe that patients with cancer with great social support could reach their normal life and find a sense of meaning in the context of disease thanks to the integration into the daily working routine. Moreover, they could have more resources and energy to spend in their work life when they receive continuous help from close people in carrying out daily activities. The evaluation of social support in patients with cancer, especially with glioma III, is therefore suggested to identify people with a lack of social contacts in order to plan specific interventions.
After 6 months from surgery, emotional distress and disability were also strongly associated with work ability in patients with glioma III highlighting again the vulnerability of this period. Previous studies showed the influence of emotional distress reporting the impact on the productivity of depressive and anxiety symptoms (Kessler et al., 2006) and the relationship between higher levels of depression and work limitations in a sample of brain cancer survivors compared to the non-cancer group (Feuerstein et al., 2007). Regarding disability, most of the studies in the literature did not evaluate the association between work ability and this variable in patients with glioma. Despite this, it was showed that brain tumor survivors experience limitations at work due to a higher prevalence of both physical and mental deficits related to the disease itself and the received treatments (Feuerstein et al., 2007).
Patients with glioma III had also a strong association between resilience and work ability. Our result is supported by a recent study on resilience in patients with brain cancer that found an association between working status and resilience. Specifically, lower resilience was associated with not currently working, not being involved in family decisions, receiving adjuvant treatments, and mild depression and anxiety (Zahid et al., 2021). However, to our knowledge, no studies exist on the relationship between resilience and work ability in patients with brain cancer. Since resilience may play a key role in mediating return to work, further studies should investigate the impact on work functioning in patients with brain cancer who return to working life after surgery.
Contrary to patients with glioma III, patients with breast cancer showed moderate associations between psychosocial factors and work ability both after 6 and 12 months from surgery. It is possible that there is not a critical period early after surgery as in patients with glioma III, but that the difficulties in patients with breast cancer are more spread out during the first postoperative year. Among psychosocial factors, we found an association between work ability, fatigue, and disability. Our results are in line with previous studies that found an association between the reduction of general fatigue and the improvement in work ability at 6, 12, and 18 months after treatments (Wolvers et al., 2019) and that reported the role of the fatigue in determining the work difficulties in cancer survivors, especially after treatments (Calvio et al., 2010; Lavigne et al., 2008). We suggest to evaluate and monitor fatigue over time in patients with breast cancer, but also in patients with glioma since they could experience a higher level of fatigue due to the side effects of treatments (e.g., radiotherapy, chemotherapy) and disease overall. Furthermore, considering the impact of fatigue on the work functioning, personalized intervention in the workplace with reasonable accommodation could be a facilitator. Regarding disability, a confirmation of our result comes from a study by Ho et al., (2018) who investigated the association between work ability and patient-perceived physical and psychosocial outcomes. They found that 37% of employed breast cancer survivors had lower work ability levels associated with physical fatigue, more breast symptoms and poorer global health status at 1 year after diagnosis. The work-related problems among breast cancer survivors include perceived physical or cognitive disability, fatigue, and exhaustion (Lilliehorn et al., 2013; Oberst et al., 2010) leading to leave the workforce and representing barriers to the return to work (Lilliehorn et al., 2013).
In addition, we found a negative correlation between clinical treatments and work ability in patients with breast cancer undergoing further clinical treatments after surgery both at 6 and 12 months. We suppose that the diagnosis and adjuvant treatments in women with breast cancer can lead to continuous emotional, physical, and psychological distress that negatively affect their work ability. This is sustained also by the evidence that women respond to the disease differently from men paying more attention to the psychological factors and manifesting more disturbances (MacIntyre et al., 1996). A previous study highlighted that at 12 months after diagnosis patients with breast cancer who did not receive chemotherapy were back to full-time work compared to women who underwent chemotherapy. Indeed, only 9% of those who had received chemotherapy improved their work ability (Lilliehorn et al., 2013). This could be related to the side-effects of treatments that lead the patients to leave their jobs (Braybrooke et al., 2015). Contrary to the literature, we did not find any association between work ability and depression and anxiety in patients with breast cancer. This could be related to the fact that the sample was enrolled during the COVID-19 pandemic and probably there were adjustments in work life for many women, including smart working and a flexible schedule, that allowed a better conciliation of personal life and work. We suggest that the identification of psychosocial features associated with work ability is essential for patients with cancer. The knowledge of factors influencing the work ability could support the health professional in planning tailored interventions and facilitating the return to work process in patients with cancer. Furthermore, our study provides potential support for a culture of reasonable accommodations in all workplaces to improve inclusion and work ability for all workers with a history of chronic health conditions.
Some limitations need to be acknowledged. First, the small sample size, the heterogeneity between groups, the different surgical strategies, post-surgical treatments, and tumor location did not allow us to have strong results. Further studies with larger samples could find more significant findings using different statistical analyses. It is also possible that patients with more severe clinical deterioration failed to continue the follow-up with the consequent loss of important cases. Second, we did not collect variables related to the work environment that might have influenced the work ability. Third, we only studied the correlation between psychosocial factors and work ability and we did not know the cause-and-effect relationship between these variables. Fourth, we considered only two time points while it could be interest to monitor the association between work ability and psychosocial factors over time. Another limitation of this study concerns the use of a self-reported questionnaire on work ability. Further studies should include also objective instruments to assess work ability. Furthermore, the use of many psychosocial measures could have been demanding for the patients although the self-reported questionnaires do not generally require a lot of time and resources for participants. Finally, the COVID-19 pandemic certainly had an impact on the ways of working influencing the results of our study.
Conclusion
Patients with glioma and breast cancer diagnoses showed a decrease in work ability levels between 6 and 12 months after surgery. Psychosocial factors associated with work ability were emotional distress, disability, resilience, and social support in patients with glioma III, while in patients with breast cancer were fatigue, disability, and clinical treatments. Our study supports the importance to investigate psychosocial factors that could have an impact on work ability in order to facilitate the return to work and to plan tailored intervention for patients with glioma and breast cancer.
Research Data
sj-doc-2-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-doc-2-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-doc-3-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-doc-3-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-doc-5-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-doc-5-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-doc-6-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-doc-6-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-doc-9-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-doc-9-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-docx-10-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-docx-10-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-rtf-1-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-rtf-1-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-rtf-4-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-rtf-4-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-rtf-7-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-rtf-7-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-rtf-8-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-rtf-8-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Research Data
sj-xlsx-11-hpq-10.1177_13591053231151286 – Supplemental material for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study
sj-xlsx-11-hpq-10.1177_13591053231151286 for Psychosocial factors associated with workability after surgery in cancer survivors: An explorative study by Fabiola Silvaggi, Arianna Mariniello, Matilde Leonardi, Antonio Silvani, Elena Lamperti, Serena Di Cosimo, Secondo Folli, Anna Trapani and Silvia Schiavolin in Journal of Health Psychology
Footnotes
Acknowledgements
Thanks to the Neuro-oncology Unit of Fondazione IRCCS Istituto Neurologico Carlo Besta and Breast Cancer Unit of Fondazione IRCCS Istituto Nazionale dei Tumori, Milano medical and nursing staff for the collaboration to sample structuring.
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the Sage Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of the larger project “I controlli periodici (follow-up) dopo la diagnosi e le terapie in pazienti liberi da malattia e asintomatici: verso una personalizzazione delle strategie di follow-up” supported by Lombardy Region Italy (Grant agreement n. RR33 to develop personalized follow-up strategies based on patient and health care professional needs and perspectives).
Silvia Schiavolin is supported by the Italian Ministry of Health (RRC).
Ethics approval
Prior to recruitment, full ethical approval was obtained from the Fondazione IRCSS Istituto Neurologico Carlo Besta and Fondazione IRCCS Istituto Nazionale dei Tumori Ethics Committee. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.