
Abstract
Research has demonstrated that Parkinson’s disease can have adverse psychological effects on caregivers. Very few studies have focused on the experiences of spouses who are not primary caregivers or who do not identify as primary caregivers. The aim of this study was to explore the experiences of spouses who are not primary caregivers or do not identify as primary caregivers. Twelve Israeli women, spouses of men with Parkinson’s disease, were interviewed using a semi-structured in-depth approach. Thematic analysis revealed five themes: before diagnosis, at diagnosis, after diagnosis, interpersonal ways of coping, and intrapersonal ways of coping. A dynamic of oscillation between confronting and avoiding losses was indicated. Non-death losses were mostly unacknowledged among spouses’ social circles. Results were interpreted in the context of grieving processes after diagnosis. Findings suggest a need for psychological interventions aimed at creating safe spaces for spouses to engage in a grieving process after diagnosis.
Parkinson’s disease (PD) is a progressive neurodegenerative disorder. It is diagnosed based on clinical features, which mainly manifest through the development of motor symptoms, such as bradykinesia, rigidity, and tremor at rest (Davie, 2008; Sveinbjornsdottir, 2016). As the disease progresses, non-motor symptoms such as sleep disorders, cognitive impairment, mood disturbance, and even psychosis, may also occur (Jankovic, 2008; Sveinbjornsdottir, 2016). PD can have different onsets—juvenile, young, intermediate, and late (Ferguson etal., 2016; Mehanna etal., 2014).
PD affects an estimated 30,000 people in Israel alone, and millions worldwide. It is more prevalent in men than in women and mostly diagnosed at age 60 or older (Knesset Research and Information Center, 2018). A recent study found clusters of similar symptoms and care demands among caregivers, across disease diagnoses, including PD, Alzheimer’s disease (AD), and Parkinson’s with Dementia (PDD), suggesting a need to go beyond disease diagnosis when examining the experiences of spouses of people with PD (Roland and Chappell, 2019). The manifestation of physical and mental symptoms as well as subsequent hindered interpersonal, social, and occupational functioning, may compound strain in patients with PD and their spouses (Balash etal., 2019; Carter etal., 2012). The experiences of female spouses of men diagnosed with PD who are not primary caregivers or who do not identify as primary caregivers, are the focus of this investigation.
A review of recent literature reveals that most of the research conducted in the interest of exploring the experiences of spouses of people with PD has focused specifically on the experience of the spouse as a caregiver (Carter etal., 2012; Johansson and Grimby, 2014; Lee etal., 2019; McLaughlin etal., 2011; Tan etal., 2012; Vatter etal., 2018). Findings observed through quantitative studies revealed a significant relationship between disease stage and level of caregiver strain (Hand etal., 2019).
Another recent study, using the Multidimensional Caregiver Strain Index (MCSI) found that female caregivers report greater social constraints compared to male caregivers (Balash etal., 2019). Findings also showed evidence of psychiatric disorders, including major depression, anxiety disorder, and insomnia disorder (Lee etal., 2021). Several studies found evidence of grief for non-death losses and anticipatory grief among caregiving spouses of individuals with PD (Carter etal., 2012; Johansson and Grimby, 2014). That is, grief that may develop due to prolonged periods of witnessing a loved one’s struggle with illness, even if the illness culminates in death that occurs at an expected life stage (Boerner etal., 2015; Doka, 2010).
Studies from a qualitative perspective also focused primarily on the caregiving experiences of spouses and highlight widespread emotional and physical strain due to the burden of providing prolonged care as well as a need for better caregiver support (McLaughlin etal., 2011; Tan etal., 2012). A recent study revealed that female caregiver spouses of people with PD, of all levels of cognitive decline, described a reduction in communication, intimacy, and relationship satisfaction, but increasing feelings of anger, sadness, resentment, frustration, and a worry for the future (Vatter etal., 2018).
While most of the studies to date focused on the experiences of caregiving spouses of people with PD, very few studies explored the experiences of female spouses who are not currently or have not yet become informal caregivers to their respective spouses with PD (see Lyons etal., 2021). Preliminary findings showing evidence of grief processes (Carter etal., 2012; Johansson and Grimby, 2014) suggest that research on the experiences of spouses of people with PD has not yet encompassed the experience in its entirety.
Furthermore, since both the quantitative and the qualitative investigations thus far have mainly focused on uncovering factors that contribute to pathology, there may still be potential gaps in our understanding of the experiences of spouses. When more and more studies in the field of psychology emerge that shift the focus from pathology toward theories and models that normalize coping and grief reactions (Boerner etal., 2015; Granek, 2010; Yehene etal., 2021), it seems essential that these experiences are given another observation.
A qualitative examination was chosen for the current study as it is generally considered to be an appropriate method for exploring complex subjective experiences (Walliman, 2017). The sample consisted of spouses of different ages and varying lengths of coping periods, because the progressive and dynamic nature of PD suggested potential changeability in the experiences of spouses, which warranted exploration.
Statistics show that most of the people who are diagnosed with PD in Israel are men, most of whom are married to women (Knesset Research and Information Center, 2018). The target population of this study, female spouses of individuals with PD in non-primary caregiving roles, is indeed an understudied minority within a majority of female spouses. Thus, the aim of this study was to conduct a qualitative investigation of the experiences of women who are spouses of men with PD. The research question was “What is the experience of female spouses, in a non-primary caregiving role, of men with PD?”
Method
Sample
The inclusion criteria were female spouses of men with PD who were not or did not identify themselves in a primary caregiving role. The sample included 12 women ranged in age from 34 to 74. They also varied with respect to the time that had elapsed since their spouse’s diagnosis, ranging from less than 6 months to 16 years (see Table 1 for details). Most participants’ husbands had either full or near full Activities of Daily Living (ADL) functioning, with mostly mild emotional and behavioral impairment, which meant they did not have, nor did they require a full-time caregiver. A few participants’ husbands did have limited ADL functioning, in which case they had a paid part-time non-family member assistant or nurse in a formal caregiving role.
Participant characteristics.
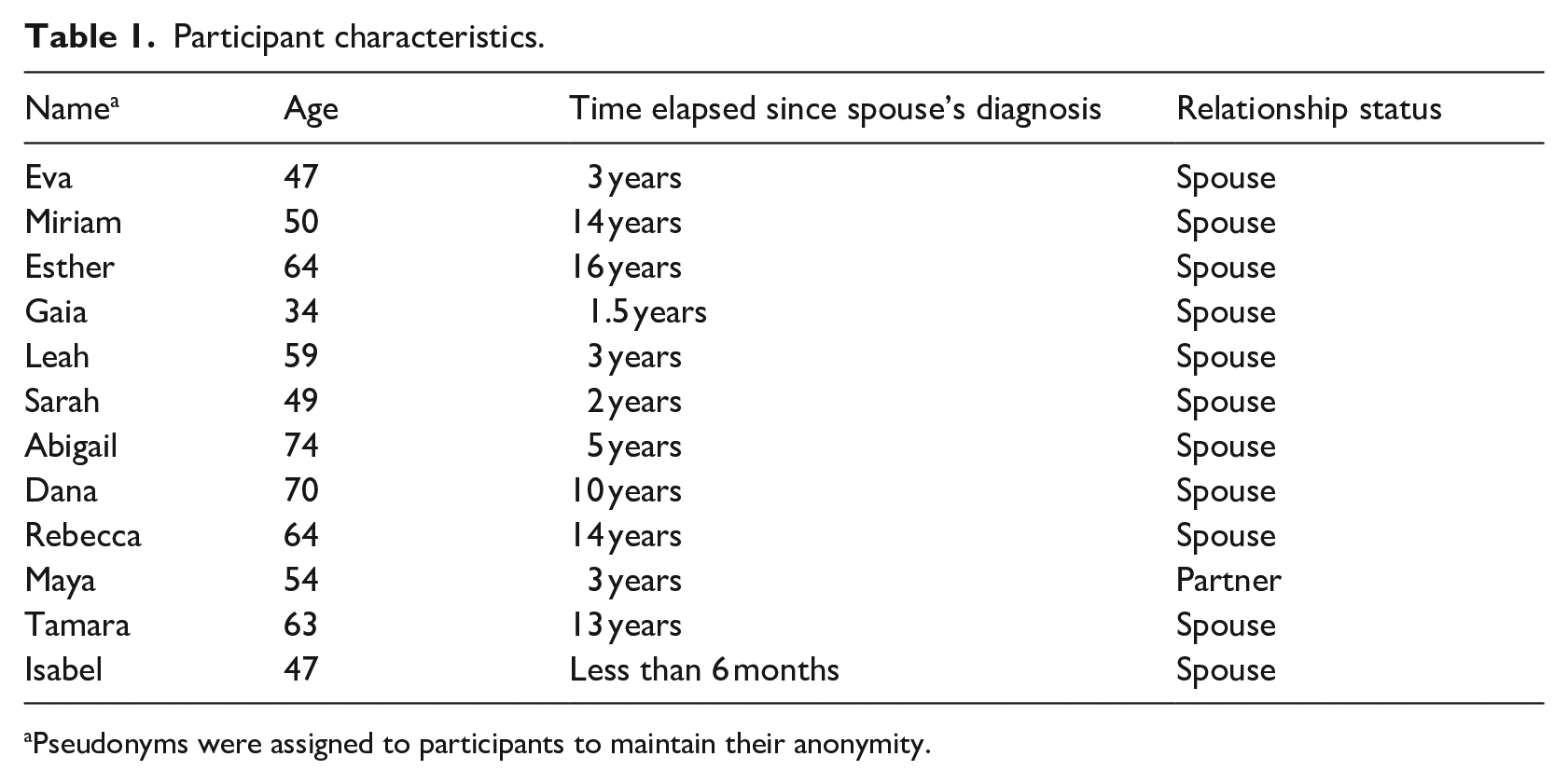
Pseudonyms were assigned to participants to maintain their anonymity.
Research method
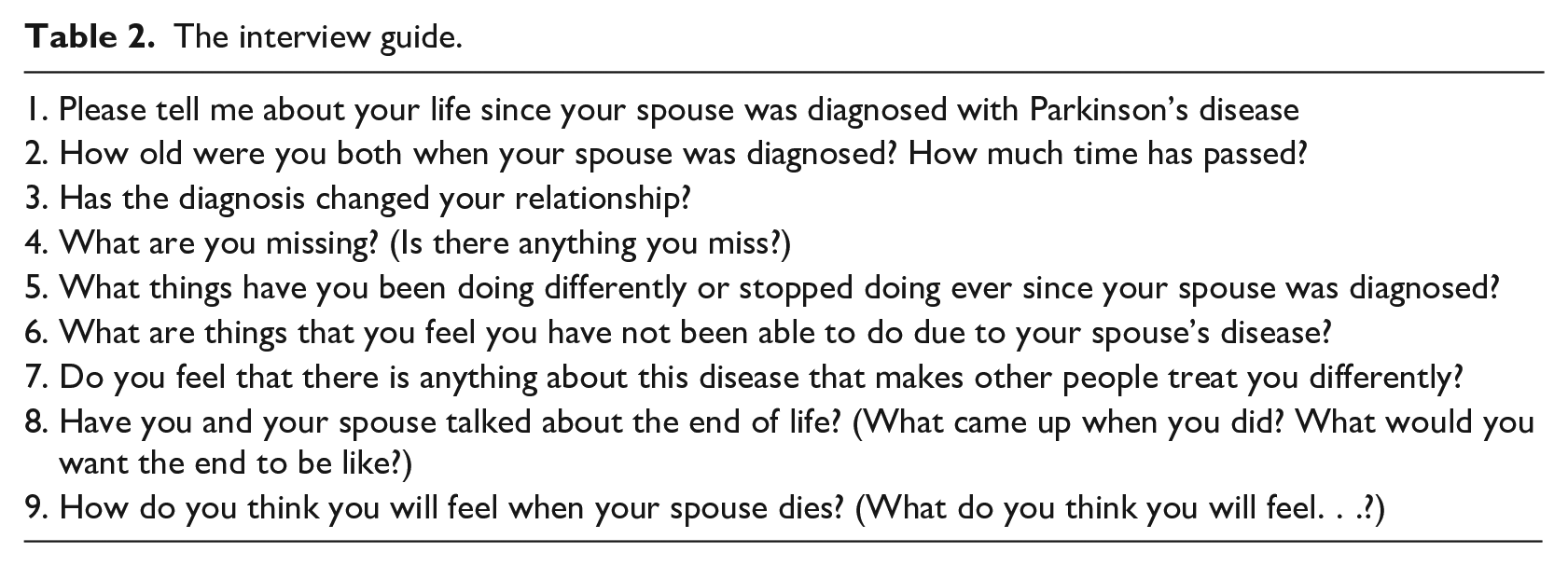
This study received ethical approval from the institutional review board of the Academic College of Tel Aviv-Yaffo, Israel (number: 2020051). Advertisements were posted on internet forums, whose members consisted of patients and their relatives. A phone call conversation was conducted with each candidate to ascertain their compatibility with the inclusion criteria. We asked each candidate to share the exact diagnosis their spouses received, their spouse’s level of physical and cognitive functioning, whether their spouse lived at home or in a care facility, and whether they had an identified caregiver. Spouses who met the inclusion criteria and expressed interest signed an informed consent form. Data were collected through in-depth semi-structured interviews (see Table 2 for interview guide). Interviews took place in the period between April and July of 2020, during the first wave of the COVID-19 pandemic, in pre-closure Israel. Participants were interviewed by a graduate student who has extensive experience with semi-structured interviewing (experience gained during their medical psychology studies and practicum). Interviews were held via Zoom due to pandemic-related social distancing measures and lasted between 40 and 90 minutes. They were recorded and transcribed verbatim by the interviewer, in their original Hebrew. Data analysis was conducted on the Hebrew transcripts, and any utilized quotes were only translated into English after the analysis was completed. The analysis was conducted by both authors, both are researchers with experience in conducting qualitative research, who have worked with patients diagnosed with neurodegenerative conditions.
The interview guide.
Data analysis
An inductive thematic analysis of the data was conducted. The analysis was conducted simultaneously with interviewing. The purpose of this analysis was to extract the most vivid details of spouses’ subjective experiences and craft them into refined themes that would reflect the entirety of their experiences. The researchers followed six phases suggested by Braun and Clarke’s (2006) step-by-step guide for thematic analysis.
Verbatim transcripts were read and re-read several times to allow familiarization with each woman’s tone and messaging. At this point, preliminary ideas were written down. Initial codes and categories were generated from each individual transcript. Transcripts were systematically coded, and codes were then grouped together into elevated categories, based on either being too similar or by virtue of conceptually belonging to the same area.
Codes were sorted into themes and overarching themes. This involved grouping some of the categories and generating new themes to better define and accommodate the scope of the categories. The themes were then reviewed to check whether any could be combined, refined, or discarded. The most vivid, compelling, and descriptive extracts were selected from each transcript upon unanimous agreement among the researchers regarding each theme. As the analysis was conducted as a constant comparison at the same time as ongoing interviewing, it was determined that data saturation had been achieved when no new information emerged.
Findings
The experiences can be outlined by two axes: disease progression and coping. These axes lend structure, context, and narrative to the experiences. Five overarching themes and eleven sub-themes emerged. The first three themes correspond to the disease progression axis (see Figure 1), whereas the fourth and fifth themes correspond to the coping axis (see Figure 2).The main themes were: (i) before diagnosis, (ii) at diagnosis, (iii) after diagnosis, (iv) interpersonal ways of coping, and (v) intrapersonal ways of coping.
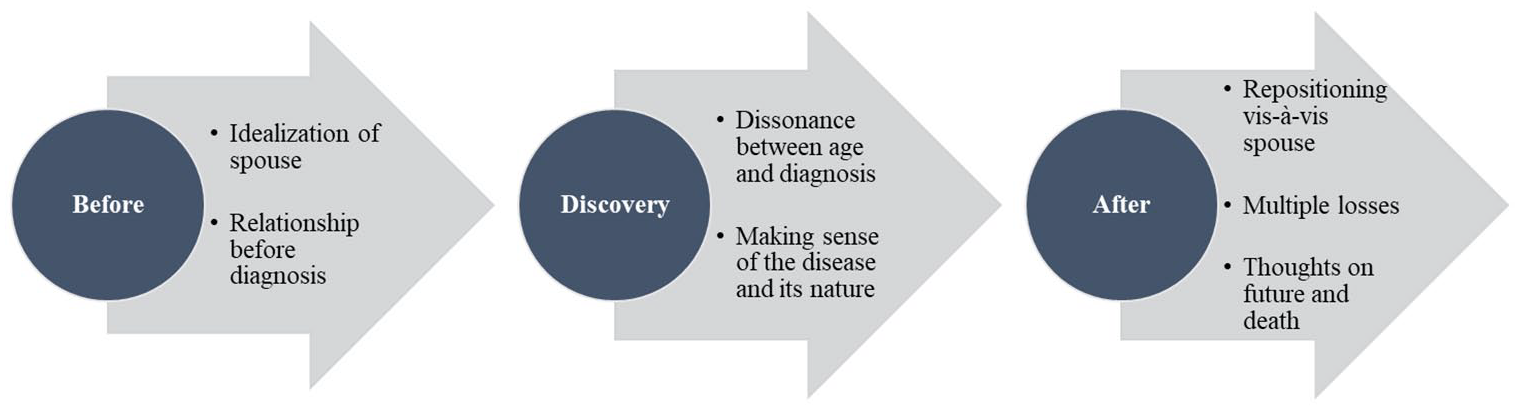
Disease progression axis.
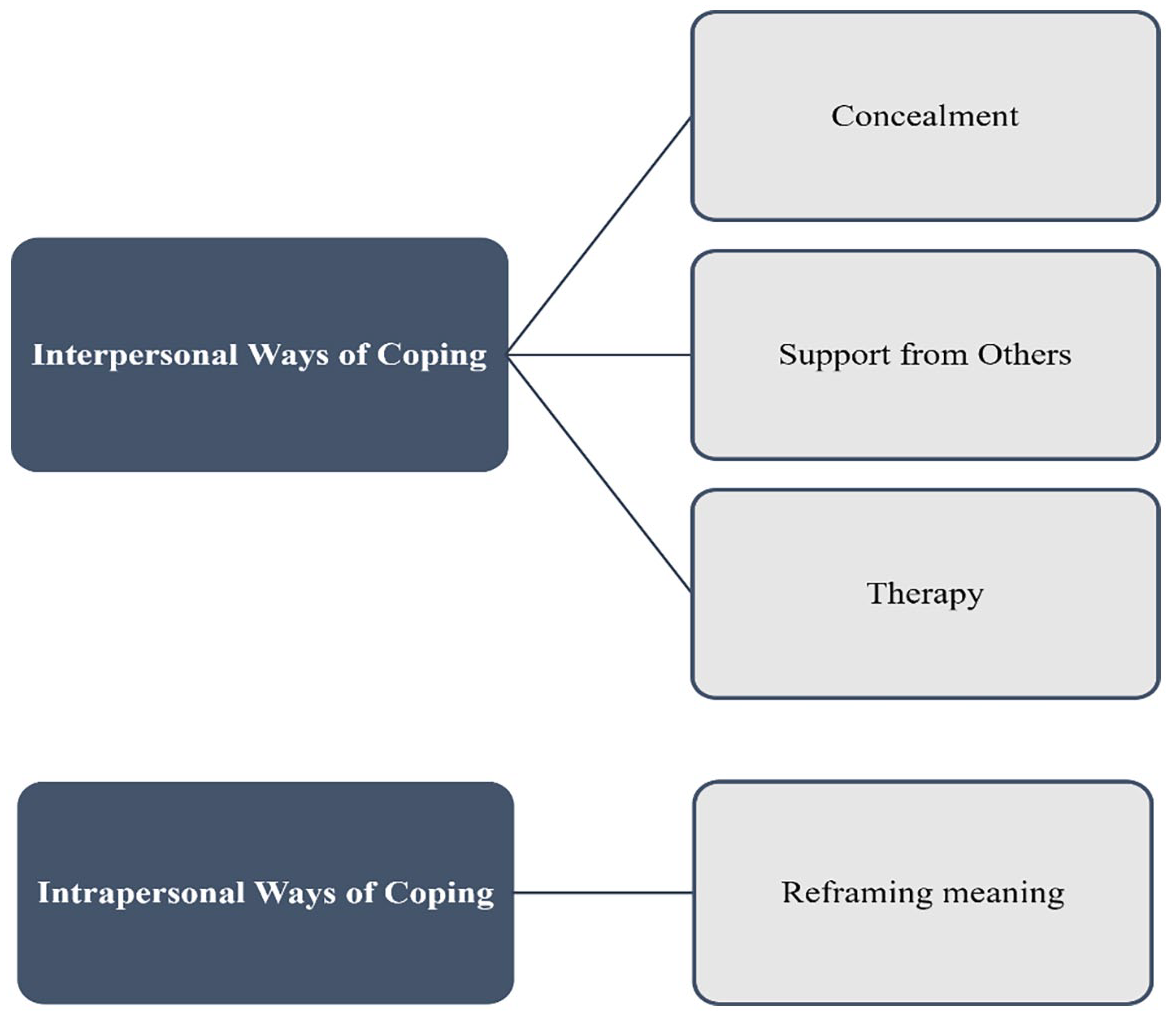
Coping axis.
First theme: Before diagnosis
The sub-themes of “before diagnosis” were idealization of spouse and relationship before diagnosis. It was apparent that the spouses tended to focus on how they perceived their spouses prior to the diagnosis and on their relationship before diagnosis.
Idealization of spouse
All participants described their spouses in favorable terms whenever references to times prior to the diagnosis had been made. Considering the disease, several participants described their spouses in terms that alluded to a hero’s fall. In their view, their spouses were more than ordinary, and the disease changed that for the worse. “He was a very strong man, very healthy. . .a radiant, cheerful fellow. . . .A decade later, he wasn’t the man I knew at all. It manifested in speech. It manifested in facial expressions. . . .His personality remained the same, but something changed there” (Maya). Up to the moment of diagnosis, spouses were perceived as being invincible. A perception predicated on real experiences. No matter how unwavering it was, this perception either cracked or fully shattered upon diagnosis.
Relationship before diagnosis
Spouses described their relationship before diagnosis in idealized terms. “He used to be my anchor, the one I could talk to about arguments I had had with friends, and all types of emotional stuff. Now the emotional stuff is with and about him” (Eva). Several participants described experiences that reflected merging and symbiosis between them and their spouse. For example: “I don’t think he understands how much I miss this. . .the symbiosis we used to have.” (Esther)
Second theme: At diagnosis
The sub-themes of “at diagnosis” were dissonance between age and diagnosis and making sense of the disease and its nature. Diagnosis was a focal point with enduring effects. It might be the point where the stories began but, in most cases, it is not when signs of the disease began to show. Thus, narratives slid in and out of the past, in what seemed like an attempt to make sense of the disease and the experience.
Dissonance between age and diagnosis
Participants emphasized age as a prominent factor. The younger they were, the harder it was to reconcile the manifestation of the disease. Younger participants seemed to have mentioned age by way of expressing their difficulty to accept that such a disease could befall a young person like their spouse. “So, what I’m saying is that we are too young to cope with such changes, and it’s like we still have miles and miles more to go” (Eva). Older participants seemed to have the inverse reaction, essentially expressing acceptance of the idea that it is not uncommon for a person of their spouse’s age to cope with disease. “At our age, it’s a topic, you know. We meet up and start off discussing who had gone to see the doctor and how many tests and medications they were prescribed.” (Dana)
Making sense of the disease and its nature
This manifested in diverse ways. Epidemiology, for one, received prominent focus. “We went to a specialist doctor at the hospital, and he checked and determined that his condition was caused by a specific contributing factor from his past” (Leah). This was primarily done out of expressed fear that PD may be hereditary.
Several participants focused on disease optics. This helped them to contextualize physical symptoms and, in some cases, to recognize their priorities. “He looks really old for his age. He looks very old in general. So, now with the disease, wow, old age seems to have settled on him.” (Isabel). All participants formed illness perception despite the effects of ambiguity and the suddenness of the disease. “. . .the most important thing to learn, suddenly you have someone new that entered your life, something new, it’s very dominant, it’s very present, you cannot ignore it. You have to live with it to the best of your ability.” (Abigail).
Participants also expressed a sense of ambiguity. “The rate of progression isn’t clear, to anyone, none can tell us.” (Miriam). Ambiguity did not only apply to pace, but also to the dynamics of the disease. “You can never know. . .It’s a disease that can go in any direction, you can’t ever know where it’ll take you” (Leah). Essentially, participants expressed that PD was a disease one could not encapsulate right away, that it requires learning and time to “get used to.”
Participants described emotional effects the disease has had on them. Some found it difficult to name emotions they felt and could only tell that they had felt something. “It’s nudgy, and pisses you off, it’s always there.” (Rebecca). For some, there were times where emotional detachment served as a better coping mechanism. For example, when asked to think about their spouse’s life expectancy. “I don’t know how I will feel, I can’t know how I will feel. Obviously, it will be hard” (Gaia). It was most likely quite scary to think about it, and emotional detachment was protective in that instance.
Third theme: After diagnosis
The sub-themes of “after diagnosis” were repositioning vis-à-vis spouse, multiple losses, and thoughts on future and death. At this point in their stories, the participants tended to go back and forth between the brief period just after diagnosis and the present day.
Repositioning vis-à-vis spouse
Participants described the disease as dynamic, ambiguous, and unstable. The progressive nature of the disease and changes in family dynamics triggered a need to reposition vis-à-vis their spouses. Some reported increased splitting and distance in their relationship. “You can’t talk about us as a couple. Because my needs and my interests are entirely different” (Rebecca).
Several participants described an increased sensitivity to their spouses. “We have to be very, very careful of one another all the time” (Sarah). Note that it was a mutual need to avoid hurting one another. There were also expressed needs for empathy and containment.
Participants also spoke about their roles post-diagnosis, describing shifts in their role as well as their respective spouse’s role. For the most part, spouses who were breadwinners passed the role on to their wives or partners, who then inevitably became the mainstay of the family. “The division of labor between us. Nowadays, I do a lot more. Because it’s harder for him. . .a whole lot has been transferred to me” (Isabel).
Several participants did describe views on the prospect of caregiving. “When my parents were a couple, with one stroke of a so-called knife. . .they turned into patient and caregiver. Spouses should be spouses. . . .keeping the balance between being a spouse and a caregiver is a fine line one should know to implement” (Sarah). There seems to be general acknowledgement that the nature of PD could necessitate some level of caregiving down the line, but it is accompanied by the hope that one will be able to balance one’s roles as a spouse and a caregiver.
Some reported changes in their intimacy with their spouses. “Physically he is more tired. . ..He suffers from physical pain here and there. He has all sorts of things. Our togetherness has changed. There are days. . .[I am] more alone, he is more withdrawn, in his own space” (Miriam). Intensifying physical symptoms hindered the men’s ability and sometimes willingness to be intimate, to the manifest chagrin of spouses.
Multiple losses
Participants described losses that occurred in the time that has passed since diagnosis. They described losses related to their spouses. “Even if he is not disabled, there is still something that feels like a loss. It’s like a ticking clock, sitting in the corner. Sitting on the side there is a ticking clock. And we don’t know when that happens.” (Eva). There is a common theme of impending doom, a loss that is bound to happen, with no way to anticipate its exact timing. Like an hourglass metaphor, it conveys a sense that time is running out. Though not necessarily central to all participants’ experience of coping, there was general awareness of this feeling.
Participants spoke about losses related to their relationship or nuclear family. “I remember when we first got married, I said: ‘Wow, we are going to have, we are going to start a family together’. It’s like. . .it has been hindered to some extent” (Esther). It speaks to some form of derailment of plans. The dynamics of the disease forced changes of plans as well as routines. In some cases, these dynamics served as a catalyst, to realize plans that had already been in place.
Thoughts of future and death
Thoughts of the future and of death emerged before, right after the diagnosis, and remained afterwards. As the disease progressed, thoughts of future and death intensified among the participants. Several spouses described how the ambiguous nature of the disease led them to think about their spouse’s life expectancy. “It’s his right to choose whether to end his life or not. So, yes, it does come up from time to time” (Gaia). Some expressed concern about a future of dependence. “We want to it to end in a “good place,” not to be dependent and not to experience hardship.” (Eva)
Fourth theme: Interpersonal ways of coping
The sub-themes of “interpersonal ways of coping” were concealment, support from others, and therapy. All participants shared diverse and complex ways of coping with the impact of the disease on their well-being.
Concealment
Opting to conceal the disease was either a step that was meant to protect others from the news or a decision based on the men’s feelings about having the disease. The ambiguous nature of this disease elicited several approaches to breaking the news, a decision that often involved and affected the spouses. Some participants adhered to their spouse’s preference. “In this regard, I really went along with him. No, I don’t recall that it bothered me. Concealment from me maybe was difficult. His denial toward me was difficult. But not toward others” (Esther). Several women preferred to share the news with family from the get-go. “I brought them over for a conversation, because I realized I could not hide it from them” (Miriam). For some, concealment often led to feelings of loneliness and stagnation that contributed to a growing need to refocus on self-care. “We had to cope and reinvent ourselves. We didn’t have any organized help around” (Miriam). Several participants expressed a need for their own space, essentially room for themselves. “I think dealing with the affairs of the house and my business, that was something that protected me. Pretty much shielded me.” (Eva)
Support from others
Participants expressed varying levels of support from their surroundings. Some expressed solidarity with people who have gone through similar experiences. “I discovered I was not truly alone. . .That what I am experiencing and what I feel, I can say out loud, and that would be like everybody saying: ‘Wow, that’s true, wow, how can you say that? That’s so true’.” (Miriam).
Most participants, however, described a lack of either support or understanding from their social circles, some even described experiences that conveyed social disenfranchisement. “There is a lack of understanding that we also experience this, that we also suffer from this disease.” (Sarah). Several participants exhibited self-disenfranchisement as well. That is, where they felt that their own feelings and actions did not have legitimacy, a form of internalized social-disenfranchisement. “One shouldn’t withdraw into oneself, into depression, to withdraw. . .into oneself, and to think and ruminate. On the contrary, banish the thought. Life is all scary. It’s not just this disease. One should walk with their head held high. . .” (Maya)
Therapy
Several participants turned to self-help and therapy. They found it useful, a space to begin a process that would eventually allow them and their spouses to speak to one another about their experiences. “I also think that anyone who copes with something like this. . .they must have some way to vent. . . .Because I’ve been a therapist for some years, I know how to manage that. But I suppose if I weren’t, I would go. . .to seek help” (Leah). For some, it was also a means to reaffirm their perceptions regarding their experience. “I once spoke to our therapist alone, and the therapist confirmed to me that there’s some denial. . .Not of the disease, but of the effects of the disease on our [intimate] physicality.” (Esther)
Fifth theme: Intrapersonal ways of coping
The sub-theme of “intrapersonal ways of coping” was reframing and downplaying meaning. Feelings of stagnation and loneliness contributed to a need to refocus on self-growth.
Reframing and downplaying meaning
This was a process utilized by most participants to cope and make sense of the disease. This manifested through comparison between PD and other progressive diseases. “Okay, fine. It’s not Alzheimer’s. . . .We will cope. We will fight it together. We will cope” (Esther). Some compared it to terminal diseases. “I don’t believe anyone can cope on their own with a diagnosis, though it isn’t cancer, it’s not. . .but it’s a disease that is in the background. And you have to be aware and know how to manage your feelings” (Leah).
Participants expressed retrospection and meaning reconstruction, alluding to retrospection that had occurred over time throughout their experiences. “I remember planning for the future. . .and my mind ran ahead, how old our child would be if it lasted longer than several years. . .These days I think about that less and less, it’s a disease that you roll with, you live with” (Miriam). Participants engaged in active reconstruction while interviewing for this study. “I have never actually sat down to. . .deconstruct this period. I’m talking to you now and I am thinking about how much we have gone through simultaneously. It is simply crazy” (Eva). Participants felt that they were asked questions that allowed them to focus their thoughts and reflect on their experiences.
Discussion
In the present study, participants were women married to husbands who are diagnosed with PD, living in Israel (except for one woman who was in a common-law marriage). The progressive nature of PD directly contributed to the formation of a progressive structure whereby spouses organized their narratives. This revealed a dynamic nature to the participants’ experiences; as the disease progressed, it intensified in their experience.
Participants experienced the progressive nature of their spouses’ disease as increasingly more pronounced. However, in a similar fashion to the “on-off” phenomenon experienced by levodopa-treated PD patients, where patients go through cycles of fluctuating symptoms, spouses experienced a seesaw dynamic where the disease took up more (off) or less (on) space in their lives. It was experienced as a dichotomy between absence and presence that compounded the challenge of grieving for losses that had occurred along the way. Whenever individuals experienced “off” phases and symptoms were present, the feeling of loss intensified among spouses, and vice-versa. Thus, the experience of loss of a fully present spouse mirrored the different phases of the disease.
These dynamics coincide with recent literature on ambiguous loss. Such losses occur when a loved one is physically present, but psychologically absent, or vice-versa. Ambiguity complicates the process of grief, prevents cognition and coping, and could result in fractures in or entire loss of relationships with friends, as they are left uncertain as per how to support (Boss, 2010). Ambiguity may fracture meaning reconstruction of loss, and without any sense of meaning, hope for reprieve or closure is scarce at best (Boss, 1999, 2006, 2007, 2010; Fuchs, 2018; Yehene etal., 2021). Spouses attempted to grieve for and find meaning in the multiple non-death losses they had witnessed and experienced after diagnosis, even as they were interviewing for the current study.
The duality of the “on” and “off” dynamic can also be interpreted in the context of the dual-process model of coping (Schut, 1999; Stroebe and Schut, 2010). It reflects a dual-process dynamic, where grievers either concentrate on the loss of a love object or on distracting themselves from the loss and participating in the world. Grievers either confront the loss or avoid it. Except that the processes are not mutually exclusive. Grieving demands work, but it also requires respite. This model declares them both legitimate and necessary (Schut, 1999).
Talking about loss brought the women’s husbands’ disease into focus, making it more present in the moment. This dynamic reflected a need to be in touch with losses they experienced. Spouses were able to recall their experiences, only in a less stressful and more sheltered setting. Discussing aspects unrelated to the disease and reminiscing about times prior, made the disease less present, even absent. This was particularly manifest when participants spoke about how the interview impacted them. Several participants reported feeling cleansed, relieved, nostalgic, rattled, and happy because of the interview. Some alluded to meaning reconstruction, referring to the interview as an opportunity to deconstruct the experience.
The “on” and “off” dynamic possibly reflects the oscillation described by the dual-process model of coping (Stroebe and Schut, 2010). The ambiguous nature of multiple losses complicated the participants’ ability to grieve. It is important to note that not only did the nature of the disease incur this dynamic, but the participants also chose to cope in this manner. There was an active and conscious choice to engage in the world and focus on personal growth, to find meaning in loss.
Grief did not garner significant support from close or distant social circles. These experiences of support, or lack thereof, and views of the role of social support reflect aspects of disenfranchised grief (Doka, 1999). The coping axis and its corresponding themes may be interpreted in the context of disenfranchised grief. This type of grief is experienced by those who are subjected to loss that is not openly acknowledged, publicly mourned, or socially supported (Doka, 1999). Its effects are felt in social as well as psychological aspects. These effects are of immense influence, as they could potentially lead to a person feeling they have no right to grieve and that their emotional expressions are illegitimate (Kauffman, 2002).
Disenfranchisement may occur for one or several reasons. Some seem to resonate more with the findings of this study: the loss itself is not recognized by society since the object of the loss remains physically present or the way an individual grieves is not socially acceptable (Doka, 2010). Some tend to express their grief in ways that are more cognitive than emotive. A more cognitive style may manifest in information seeking and case managing, as it did among several participants. Society may view this kind of behavior as non-grief and invalidate it (Doka, 1999, 2008).
Participants often reported feeling that their ways of coping were not acknowledged by their friends and relatives. Several participants described scenarios where others told them they were reacting in ways that were not acceptable. In some cases, rejection was only implied, but was felt in interactions with others, which made them feel that their experiences were not accepted.
Several participants expressed self-disenfranchisement. This disenfranchisement refers to situations where a griever feels that their grief is illegitimate, because they think others may be going through worse experiences. However, these cases may not always be self-induced. Social disenfranchisement may lead to self-disenfranchisement (Kauffman, 2002). Indeed, several participants reported no change in society’s treatment of them post-diagnosis, yet there was evidence of internalized disenfranchisement.
The researchers recognize that focusing solely on female spouses may limit one’s ability to draw conclusions regarding the role of gender in the experience of coping as a spouse. However, the researchers believe that there is room for both gender-specific explorations and comparative analyses (see Balash etal., 2019). Furthermore, the fact that all participants were Jewish means they do not represent the entire population of spouses of individuals with PD in Israel. However, it should be noted that generalization of findings is not a goal of qualitative research (Polit and Beck, 2010). In addition, it may not be possible to characterize the changeability of the experiences in a time-limited study. It would be beneficial to study such experiences longitudinally.
Five major themes were outlined by the current findings: “before diagnosis,” “at diagnosis,” “after diagnosis,” “interpersonal ways of coping,” and “intrapersonal ways of coping.” The first three themes indicate that female spouses experience their husbands’ disease progressively. That is, it becomes more dominant in their own experience as their husbands’ disease progresses. These highlight the notion that there are points in time where difficulty may compound, and support may be needed more—at diagnosis and after diagnosis. The period after diagnosis is not time-limited and may be experienced with progressing levels of difficulty, in tandem with disease progression. The last two themes delineate the coping styles utilized by female spouses of men with PD. Interpersonal styles suggest that female spouses may choose to rely on other people for support and may find it helpful indeed—this includes family, friends, and therapy. Intrapersonal styles emphasize the role of meaning reconstruction and represent a way for female spouses to personally grieve for non-death losses, whether support from others is available or not, whether it is wished for or not.
The present findings may help mental health and healthcare professionals focus treatment on disenfranchised grief. They suggest a need for psychological and grief counseling aimed at creating a safe space for spouses to reconstruct the meanings of and grieve over their non-death losses (Carter etal., 2012; Fox etal., 2020; Lyons etal., 2021; Mosley etal., 2021; Park etal., 2019; Rodriguez etal., 2020; Sturm etal., 2019). The current findings add to the literature by highlighting the progressive nature of grieving for non-death losses in PD, which seems to be parallel to the disease progression. This may be useful to professionals in developing treatment plans to match the progressive nature of these grieving processes. Findings also emphasize the importance of supporting spouses as they work through their grief. As previously mentioned, a significant part of this process requires participation in the world. The least the world could do to help is to welcome them with open arms when they do. These findings suggest more research is needed to reveal and explore further instances of disenfranchised grief.
Research Data
sj-pdf-1-hpq-10.1177_13591053221134740 – Supplemental material for Living with Parkinson’s disease: A qualitative study of spousal perspectives
Supplemental material, sj-pdf-1-hpq-10.1177_13591053221134740 for Living with Parkinson’s disease: A qualitative study of spousal perspectives by Itay Ressler and Avital Gershfeld-Litvin in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.