
Abstract
The purpose of this study is to characterize contemporary Canadian health psychology through an environmental scan by identifying faculty, research productivity and strengths, and collaborator interconnectivity. Profiles at Canadian universities were reviewed for faculty with psychology doctorates and health psychology research programs. Publications were obtained through Google Scholar and PubMed (Jan/18–Mar/21). A total of 284 faculty were identified. Cancer, pain, and sleep were key research topics. The collaborator network analysis revealed that most were linked through a common network, with clusters organized around geography, topic, and trainee relationships. Canada is a unique and productive contributor to health psychology.
Introduction
Health psychology is a sub-discipline that studies topics at the intersection of the psychological and the health sciences (Johnson and Acabchuk, 2018). Approximately 40 years old, it is one of the fastest growing disciplines in psychology (Adair et al., 1996; Hadjistavropoulos, 2009; Murray, 2014; Quinn et al., 2020). Health psychology is, however, difficult to characterize, with implications for developing collaborator networks, attracting trainees, and supporting continued growth and development. First, due to its youth and with health psychology-specific training programs only developing in the late 1990s and early 2000s, many health psychology researchers were trained in other disciplines (e.g. clinical, developmental, or social psychology) before moving into health psychology research. As such, many primarily identify with their origin discipline and searches for “health psychologists” miss many experts in the field. Second, due to the broad and interdisciplinary nature of their research, health psychologists are potentially housed in a range of academic departments, including Psychology, Health Sciences, Social Work, Medicine, and Kinesiology. Limiting searches to Psychology Departments risks missing many experts in the field. Collectively, this makes identifying health psychology researchers a challenge.
Characterizing health psychology in Canada is even more problematic. Psychology in Canada is challenged to define and organize itself separately from the U.S. (Murray, 2014). Canada “punches above its weight” on the global psychology stage owing to a number of unique strengths (Brock, 2013), including Canada’s small population relative to the U.S., its ties to Britain and France, bilingualism and a high proportion of immigrants, all of which make Canada an ideal cross-roads and cross-pollinator for psychology theory and practice (Brock, 2013; Hadjistavropoulos, 2009). Canada’s unique historical, geographical, healthcare and cultural perspectives are further differentiators, with an emphasis on culture and multi-culturalism, collective and social values, influences from a large Indigenous population, and the challenges of a large landmass with a relatively small population (Brock, 2013; Hadjistavropoulos, 2009). Nonetheless, owing to its larger size and influence, U.S. psychology has a strong influence on Canada, and specific efforts are required to ensure that Canadian psychologists and their work are not lost in the overwhelming context of U.S. psychology.
Characterizing health psychology in general, and in Canada in particular, is problematic for a number of reasons. Although a growing field that is focused on topics of interest in both the psychological and health sciences, Canadian medical and public health practitioners and policy makers are largely unaware of the existing and potential contributions of health psychology to health and healthcare, beyond non-pharmaceutical treatment of mental health disorders (Arnett, 2001; Korecky, 2020). There is also evidence of a lack of awareness of the scope of health psychology within Canadian psychology itself. Although two reviews of psychology in Canada specifically mention health psychology (Adair et al., 1996; Hadjistavropoulos, 2009), not all strengths of health psychology in Canada were discussed. For example, Canada’s contribution to cardio-metabolic and cancer-related health psychology research was not included. Not only are health psychologists and their expertise an under-recognized and under-utilized resource, both in Canada and internationally, but the scope, contributions, and potential of the field is not fully recognized within the Canadian psychology and health psychology academic communities. In short, there is appears to be an important knowledge translation gap and opportunity.
The purpose of this study was to conduct an environmental scan of university-affiliated health psychology faculty in Canada to (1) characterize health psychology faculty with respect to career stage, academic affiliations, and geographic locations; (2) describe research productivity; (3) examine faculty profiles and research outputs to determine areas of expertise; and (4) examine the inter-connectedness of the field through a collaborator network analysis (Fonseca Bde et al., 2016).
Methods
The environmental scan approach was modeled on Nagi et al. (2020). A passive approach was used in that all data were obtained from publicly available sources (Graham et al., 2008). Sources included faculty profiles on university websites, personal webpages, and information available through databases.
Canadian university-affiliated health psychology faculty
A list of Canadian universities was compiled using several sources (e.g. Wikipedia, universitystudy.ca; N = 102, Supplemental Table 1). Colleges or hospitals affiliated with a university (e.g. Luther College, University of Regina; SickKids, University of Toronto) were included separately in the search, but were listed in the database by the university’s name. Non-university affiliated colleges (e.g. Bow Valley College) were not included in the search.
For each university, all profiles were searched for faculty that met inclusion criteria for the environmental scan. All health- or psychology-related departments that could potentially house health psychology faculty were searched, including Psychology, Health Sciences, Medicine, Kinesiology, Psychiatry, Nursing and Social Work. Faculty had to (1) be active, (2) have a doctorate in psychology or psychology-related fields (e.g. neurosciences), and (3) have a faculty profile that demonstrated evidence of health psychology-related research. “Faculty” was defined as anyone affiliated with a university with any professor status, including assistant, associate, full, or adjunct. “Active” was defined as anyone who was hired, employed or not retired between June and August 2020. “Health psychology research” was defined as listing any work that included a psychological component and a health, physical disease, and/or well-being component. This could include the study of psychological disorders in specific medical populations (e.g. depression in cardiac patients); interconnections between psychology and biological processes (e.g. social support and immune activity); links between psychology and risk for disease (e.g. personality and cancer); health or health-risk behaviors (e.g. exercise, smoking cessation); and predictors of psychological well-being (e.g. purpose, quality of life). Research programs that focused on psychological, social or mental health phenomenon only without a specific patient population or physical disease component (e.g. general anxiety etiology, depression risk over the lifespan) were excluded. Preliminary searches erred on the side of inclusivity. The initial list was reviewed by the authors; researchers who did not meet inclusion criteria were trimmed, and those who were missed were added. The term “health psychologist” here is used to refer to any faculty who engages in health psychology work; it does not indicate clinical training or registration with an accreditation college.
The following were obtained from faculty profiles: First and last name, institution and geographic location; faculty, department and/or area; professional rank or role, doctorate area, doctorate institution, and profile research description. If information on doctorate area and/or doctorate institution was not available, the dissertation was found online (e.g. ProQuest) and information obtained from there. Information on sociodemographic characteristics that are typically self-reported (e.g. race/ethnicity, sex/gender, and sexuality) were not inferred from information in faculty profiles.
Research product search
A search was conducted for all research products produced by each identified faculty (January 2018–March 2021). Author searches were completed in Google Scholar and PubMed. (APA PsycInfo was initially included but discontinued due to returning fewer and the same products as Google Scholar and PubMed). For each product, information on title, authors, author order, publication year, type of publication (e.g. original contribution, review), publication or outlet name, keywords, and total citations were extracted.
Analytic approach
All analyses were conducted using SPSS 26.0 (IBM Corp, 2018). Summary statistics were generated from faculty profile information, including institution affiliation and geographic location; faculty, department and/or area; professional rank or role, doctorate area, and institution where doctorate was completed. With respect to research products, averages or frequencies were calculated for total number of research products, type of research product, product outlet, citations, and place in author order. One-way ANOVAs were used to test differences in researcher productivity by geography and professional rank or role.
Two approaches were used to examine areas of expertise. First, a thematic analysis of faculty research profiles was completed using NVivo 12 (QSR International, 1999). Three coders separately reviewed a random selection of 30 profiles and generated a coding scheme. The coders then met to discuss and agree upon a final coding scheme. One coder finished coding the remaining profiles. Second, keywords were extracted from each journal article and were examined. Keywords were first cleaned and aggregated with respect to differences in spelling (e.g. behaviour vs behavior) and specific construct terms (e.g. domestic violence vs intimate partner violence). Keywords were categorized based on common themes (e.g. all pain-related keywords). All percentages refer to total codes or keywords.
To determine the extent of health psychology research interconnection across Canada, a collaborator network analysis was completed using journal article co-authorship information (Fonseca Bde et al., 2016). For each researcher identified, journal article co-author information was extracted and translated into university-affiliated health psychologist-collaborator dyads. Data were first cleaned by aggregating different approaches to author naming (e.g. Marjorie A. Smith, M. A. Smith; efforts were made to aggregate married and pre-married publications if names were changed) and double-checking for spelling errors.
The network was generated and analyzed using Gephi 0.9.2 (Bastian et al., 2009). Information on number of nodes and links, density, clustering, and presence of communities were extracted (Fonseca Bde et al., 2016). Density, a measure of connectivity, was captured by examining average path length (average shortest difference between two nodes) and network diameter (longest path length). The clustering coefficient is a measure of the extent to which a node’s neighbors are connected to each other. The range of clustering coefficients is from 0 to 1, with higher values indicating a better-connected neighborhood. Presence of communities within the network was determined by inspecting the modularity coefficient (Newman, 2004), such that values that are >|0.3| indicate presence of communities. If the modularity coefficient indicated likely presence of communities, the network was examined for sub-networks. Each sub-network was examined for common themes, for example with respect to area of research, geographic location, or mentor-mentee connections.
Results
Health psychology faculty
The profile review produced a list of 325 faculty. The list was reviewed, and two faculty were added (recent hires), 11 were removed for not meeting inclusion criteria (two had no faculty appointment; nine did not have a psychology or related doctorate), and 31 were removed for not meeting health psychology research program criteria. Most of the faculty trimmed for non-psychology doctorates were housed in the Health Psychology and Behavioural Medicine Area in the Faculty of Kinesiology at the University of Alberta.
A total of 284 university-affiliated professors with health psychology research programs were identified from 55 Canadian universities (54% of total Canadian universities). The largest single concentration of health psychologists were located in a unique department, the Department of Clinical Health Psychology in the Faculty of Health Sciences at the University of Manitoba (16% of total health psychology faculty in Canada), which was also the only department specifically dedicated to health psychology. The department consisted mostly of clinicians with primary appointments in medical settings or private practices; the majority of faculty also obtained their doctorates from the University of Manitoba (50% of department faculty) and the department consisted primarily of Assistant Professors (87% of department faculty). Given the unique, primarily clinical focus of this department, it was treated as its own entity. Health psychology researchers from other institutions tended to be housed within conventional teaching/research departments (“conventionally-housed,” N = 238).
Of the remaining conventionally-housed health psychologists, the majority had the title of Professor (42%), followed by Associate Professor (31%), or Assistant Professor (24%). Other titles were Clinical Associate Professor, Research Professor, and Adjunct Professor. Universities with the highest number of health psychology faculty were the Université de Montreal (6%), Carleton University (5%), Concordia University (5%), the University of Calgary (5%), and York University (5%). All 10 Canadian provinces were represented, although there were no university-affiliated health psychologists identified in the three territories (specifically, none at Yukon University, the only territorial university). The largest geographic concentration of health psychologists was in Montreal, QC (16%), encompassing four universities; and the second largest concentration was in the Greater Toronto Area (11%), also encompassing four universities.
The majority of health psychologists were in Psychology Departments (72%), faculties of Health Sciences (3%) or Medical Schools (4%; Psychiatry, Pediatrics, Anesthesiology and Pain, and Oncology). Remaining faculty were housed in Kinesiology, Education, Applied Disability Studies and Public Health departments or faculties. It was possible to have health psychology faculty housed in different faculties and departments at a single institution. For example, health psychologists at the University of Calgary were housed in Anesthesiology, Pediatrics, Education, Kinesiology, and Psychology departments.
Among Psychology Departments, eight had health psychology-specific concentrations that housed 22% of the conventionally-housed health psychologists: McGill University (Health Psychology), Concordia University (Clinical and Health), Ryerson University (Community and Health), University of Toronto Mississauga (Health, Adaptation and Well-being Cluster), Université Laval (Clinique de la Santé; QC), Bishop’s University (Psychology, Health and Well-being Cluster; QC), 1 Carleton University (Health Psychology; ON), and the University of British Columbia (Health Psychology; BC). Notably, not only did health and clinical areas overlap at some institutions, but many faculty members were housed in health and clinical areas or clinical-specific areas (18%). Speaking to the diversity of the field, some faculty were not housed in health or clinical areas at all, but instead in cognitive, behavioral, developmental, or neuropsychology areas.
Doctoral training
Information on training was available for 274 (96%) of the identified faculty, representing training at 80 institutions. The majority obtained their doctorate from Canadian (76%) or American (20%) institutions, with the remaining from Germany, the United Kingdom, France and the Netherlands. Canadian-awarded doctorates were granted by 31 institutions. Excluding the Department of Clinical Health Psychology at the University of Manitoba, whose faculty predominantly had doctorates from the University of Manitoba, most had doctorate training from McGill University (6%), the University of British Columbia (5%), Dalhousie University (5%), the University of Toronto (5%), Université de Montreal (4%), and the University of Waterloo (4%). The largest proportion of doctorate degrees were obtained at universities in either Montreal, QC (15%) or the Greater Toronto Area, ON (8%).
Whether faculty members were also hired at the institution at which they received their doctorates was also examined. A total of 28 faculty (10%) were employed at the same institution where they had completed their doctorate. The Université de Montreal accounted for the largest number of faculty that remained at their institution of training. However, health psychologists trained in the Greater Toronto Area were most likely to stay in the same area post-graduation, with 11 of 19 (58%) of area graduates also employed in the area. A large proportion of Montreal graduates also stayed in the same geographic location (41% of Montreal graduates). No other regions were identified where large proportions of health psychologists were likely to be both trained and employed in the same area.
Information on doctoral degree field was extracted from available dissertations. The majority of faculty had a degree in Psychology with no sub-area specification (48%). Specializations were most likely to be Clinical Psychology (20%) or Neuroscience (9%). Others listed included Cognitive, Community, Counselling, Developmental, Education, Experimental, Industrial/Organizational, Medical, Social, and Sport Psychology. Of note, only 1% specifically identified “Health Psychology” as their dissertation field.
Research outputs
Research products produced from January 2018 to March 2021 were examined. A total of 3898 unique research products were identified. The majority of these were journal articles (84%), conference abstracts (10%), book chapters (3%), or pre-preprints (2%), but also included books, perspective pieces (letters to editors, editorials, commentaries, and viewpoints), and reports. Conference output were limited to those that publish abstracts in journals, suggesting that this number is likely an under representation.
Health psychologists published in 1058 different journals. The top five journals were Sleep, Psychoneuroendocrinology, Pain, PLOS ONE, and BMJ Open. Number of journal articles published was higher in 2020 (37%) compared to 2018 (27%) and 2019 (30%). Citation information was available for 2808 articles (86%). Average citations were 8.8 ± 31 citations (Median = 3, range 0 –1036).
The majority of faculty (80%) produced at least one research product over the last 3 years (“active researchers”). Those who produced none were primarily in clinically-focused departments or smaller teaching-focused universities. On average, those who did produce research products produced 19 ± 19 products (or 6 per year; range 1–99 over 3 years; Figure 1a). Significant differences in number of research products produced per researcher emerged when comparing by city, F(4, 279) = 11.3, p < 0.001. Researchers in Montreal (Mn = 27, SD = 24), the Greater Toronto Area (Mn = 22, SD = 22), Ottawa (Mn = 22, SD = 18) and Calgary (Mn = 32, SD = 27) did not significantly differ from each other with respect to research products produced, but researchers in these areas produced significantly more research products compared to all other regions in Canada (Mn = 11, SD = 15).
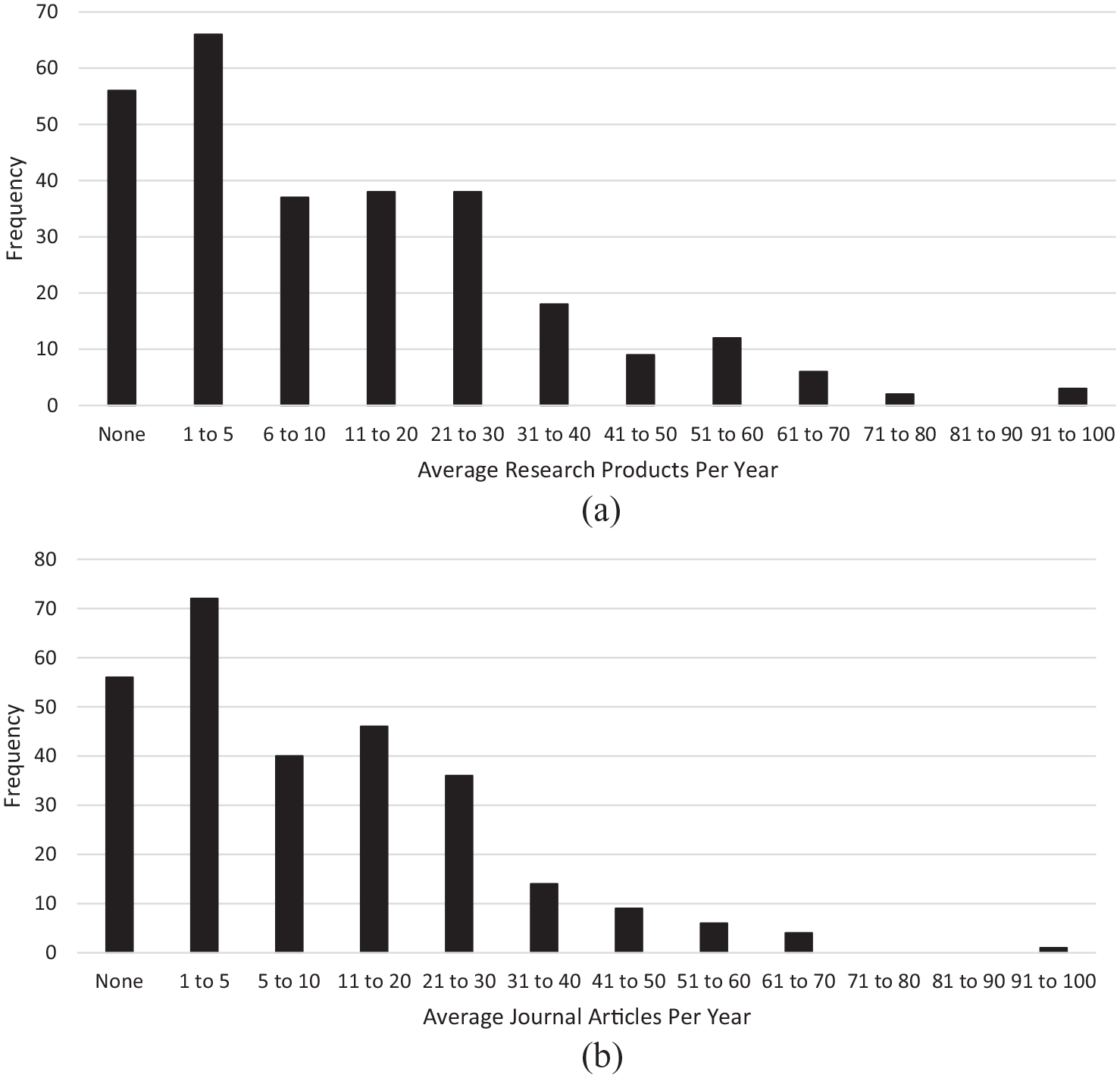
(a) Frequency of average number of research products produced per year by all identified university-affiliated health psychologists between Jan 2018 and Mar 2021. (b) Frequency of average number of peer-reviewed journal articles produced each year by all identified university-affiliated health psychologists between Jan 2018 and Mar 2021.
On average active researchers produced 16 ± 16 journal articles (5 per year, range 1 to 93; Figure 1b). Productivity varied by professional rank, F(3, 227) = 4.62, p = 0.004, with Assistant Professors having lowest (Mn = 11.3, SD = 11.8), Associate Professors intermediate (Mn = 15.4, SD = 14.7), and Professors highest (Mn = 20.3, SD = 12.5) total journal articles published. With respect to author order, active researchers produced on average 2.35 ± 2.79 (range 0–14) first-author, 2.00 ± 2.72 (range 0–14) second-author, 6.55 ± 8.11 (range 0–44) middle-author, and 5.28 ± 6.88 (range 0–54) last-author papers. Total number of middle-author, F(3, 227) = 3.68, p = 0.013, and last-author publications, F(3, 227) = 10.5, p < 0.001, varied by rank. Specifically, higher rank was associated with higher middle-author (MnProf = 8.51, SD = 9.91 vs MnAsst Prof = 4.38, SD = 5.35) and last-author publications (MnProf = 7.71, SD = 8.64 vs MnAsst Prof = 2.01, SD = 3.17). In contrast, number of first- and second-authorships did not differ by rank, p’s > 0.322. This suggests that differences in total journal productivity by rank could be driven more by increases in supervised trainee-written papers and inclusion on multi-author or research group papers, and not change in total main-author paper outputs.
Research topics
Findings from faculty profile and journal article keyword thematic analyses were complementary, and so are presented together here. A total of 72 themes were identified from faculty profiles, with a total of 695 codes assigned (Supplemental Table 2). A total of 12,987 keywords were extracted from journal articles, consisting of 4531 unique keywords. Approximately 75% of keywords were categorized into broader topics; the remaining 25% could not be categorized either due to use of vague acronyms or terms (e.g. PD, predictors), or because keywords did not fit into any category (e.g. authorship, celebrity, predator odor, public safety personnel). Only major themes are discussed here.
Psychological research topics related to stress and well-being were represented in both faculty profiles and journal keywords. Pain, sleep and close relationships and social support topics were highly represented in both faculty profiles and journal keywords. The study of specific mental health disorders was also common, particularly anxiety and depression-related topics. Health behavior topics were also evident, with a broad focus on addiction, sports and exercise, and eating, nutrition and body image-related topics. Biomarker and disease-specific topics were also well-represented, particularly brain-related topics, for example, structure and imaging, and hormones, for example, sex hormones, and hypothalamic-pituitary-adrenal (HPA) axis-related hormones. Cardio-metabolic disease, including heart disease, stroke and diabetes, and cancer were also well-represented. Although not present in faculty profiles, COVID-19 pandemic-related topics were also fairly well-represented in journal article keywords. This is particularly noteworthy given that the pandemic was active for only 10 months at the time of the research product search. Reproductive health also emerged as an important research topic, specifically with respect to maternal-child health, pregnancy and sexual health.
Specific contexts also emerged. Although developmental origins of health and disease was a mentioned in faculty profiles (1.4%), no journal article keywords specific to developmental origins or fetal origins of health and disease were identified. It is possible this is because other keywords (e.g. development) were used instead. Lifespan topics also emerged as key research topics, particularly with respect to pediatrics, adolescence and young adulthood. Other specific populations emerged, including sexual minorities and gender/sex. Of note, although several faculty profiles indicated caregivers as a research topic, caregiver-specific research was relatively underrepresented in journal article keywords. Similarly, the proportion of faculty who stated a research focus on racial/ethnic minorities, and Indigenous populations specifically, in profiles was higher than prevalence of these topics in journal keywords. Finally, public health topics emerged. Intervention research was mentioned in both faculty profiles and journal article keywords. A focus on healthcare and treatments emerged in journal article keywords, but not in faculty profiles.
Although not mentioned in faculty profiles, journal article keywords related to research methods were also evident. This included topics related to design (3.5%), statistical approaches (2.0%), online or technological modalities (0.6%), and implementation science (0.5%). Topics related to policy were relatively under-represented (0.1%).
Finally, several faculty profiles specifically identified with a psychology discipline. Health psychology was evident (1.7%), but faculty also identified as clinical, developmental or social psychologists. Of note, a large proportion of faculty profiles (6.5%) specifically stated a primarily clinical or practitioner focus.
Collaborator network
Between January 2018 and March 2021, the 228 research active, university-affiliated health psychologists produced work that amounted to >28,000 collaborator dyads, with >11,000 unique collaborators. When the list was trimmed of collaborators that only appeared once in the network, a total of 5090 unique collaborators (nodes) remained, linked by 8749 connections (edges). The average path length was 4.36. The network diameter, or the longest graph distance between any two collaborators in the network, was 12.0.
The network is shown in Figure 2. The average clustering coefficient was 0.515, indicating moderate level of connections between node neighbors. Although there were prominent nodes that were well integrated across the network, there was evidence of communities (modularity = 0.848). Most researchers were integrated into a sub-network or bubble. Six distinct networks emerged: Montreal Network, Sexual Health Network, Pain Network, Campbell Network University of Manitoba Network and University of British Columbia Network or “bubble.”
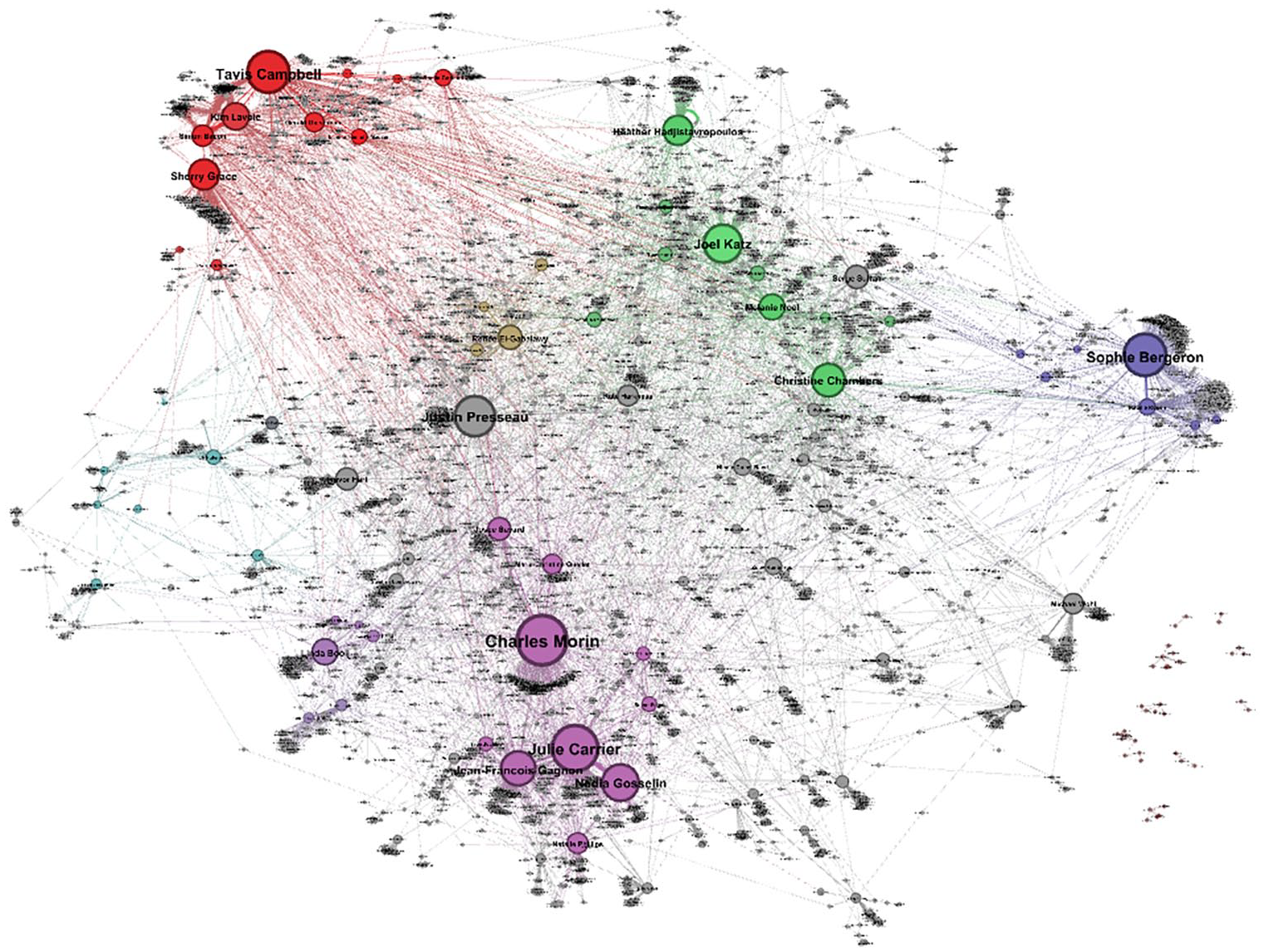
Collaborator network of university affiliated health psychologists, based on research products produced from 2018 to 2021. Different colors capture the different identified networks, with gray circles indicating individuals who do not belong to a major network. Individuals not at all connected to the network appear on the lower right side. Purple is the Montreal Network; Blue is the Sexual Health Network; Green is the Pain Network; Red is the Campbell Network; Yellow is the University of Manitoba Network, and Teal is the University of British Columbia “Bubble.”
The most prominent network is the Montreal Network, consisting of a large network that contains smaller sub-networks. It consists primarily of researchers at universities in the Montreal area (Université de Montreal, Concordia University, UQAM, and McGill University) and the Université Laval. The Montreal Network consists of four smaller networks: Montreal-Sleep, Concordia, McGill-Cancer and Montreal-Neuroscience. The Montreal-Sleep sub-network is the largest, primarily arranged around Charles Morin (Université Laval) and Julie Carrier (Université de Montreal), but also Jean Francois Gagnon (UQAM), Natalie Gosselin (Université de Montreal), Natalie Phillips (Concordia University), Josée Savard (Université Laval), and Marie-Christine Ouellet (Université Laval). Faculty in this network not currently in the Montreal area, for example, Rebecca Robillard and Stuart Fogel (University of Ottawa), completed doctoral or post-doctoral training at the Université de Montreal. In addition to common geography, this network is primarily organized sleep research (although not all sleep researchers in Canada are part of this network). There was also a Concordia sub-network organized around common geography (Concordia University), primarily arranged around Linda Booij, and includes Carsten Wrosch, Jean-Phillippe Gouin, and Jennifer McGrath; and a Montreal-Neuroscience sub-network housed at the Université de Montreal organized around neuroscience and psychoneuroendocrinology, consisting primarily of Sonia Lupien and Robert-Paul Juster.
Of note, not all Montreal-based researchers were placed in this network. Another major network also based primarily in Montreal is the Sexual Health Network, which is primarily formed around Sophie Bergeron (Université de Montreal), but also Natalie Rosen (Dalhousie University), Emily Impett (University of Toronto Mississauga), Rebecca Cobb (Simon Fraser University), Caroline Pukall (Queen’s University), and Isabelle Daigneault (Université de Montreal). In addition to having a common focus on sexual health, there could also be training connections: The majority completed graduate work in Montreal (McGill University: Bergeron, Rosen, and Pukal; Université de Montreal: Daugneault); the remaining members completed doctorates at the University of California: Los Angeles (Impett and Cobb).
The next largest network is the Pain Network. It is primarily organized around Joel Katz (York University), Heather Hadjistravopoulos (University of Regina), Christine Chambers (Dalhousie University), and Melanie Noel (University of Calgary), but also Thomas Hadjistravopoulos (University of Regina), Kathryn Birnie (University of Calgary), C. Meghan McMurtry (University of Guelph), Gabrielle Page (Universite de Montreal), Gordon Asmundson (University of Regina), and Loren Martin (University of Toronto Mississauga). Although all of these researchers have a strong pain research program many are also connected by training experiences. For example, both H. Hadjistravopolous and Chambers completed doctoral training with Kenneth Craig at the University of British Columbia; Noel, Birnie and McMurtry completed doctoral training with Chambers; Page completed doctoral training with Katz; Paulette Hunter and Michelle Gagnon (University of Saskatchewan) completed doctoral training with T. Hadjistravopolous.
Another network is the Campbell Network, and is unique in that it seems to be less organized around a common geography or research theme and more around a central collaborator: Tavis Campbell (University of Calgary). Campbell, Kim Lavoie (UQAM) and Simon Bacon (Concordia University) completed graduate or post-doctoral training with Blaine Ditto (McGill University), and share a focus on cardio-metabolic research. Campbell supervised Sheila Garland (Memorial University), and through her and Linda Carlson (University of Calgary) is involved in cancer research. Campbell also supervised Josh Rash (Memorial University), and through him is also connected to cancer and pain research. Campbell also supervised Kharah Ross (Athabasca University) and Gerald Giesbrecht (University of Calgary), and all three share a common geographic location (Calgary, AB), research focus (maternal-child health) and connection to a collaborative study [Alberta Pregnancy Outcomes and Nutrition (APrON) Study] with Lianne Tomfohr-Madsen (University of Calgary).
The last major network is the University of Manitoba Network. It is primarily formed around Renee El-Gabalawy (University of Manitoba, Department of Clinical Health Psychology), and includes Gordon Asmundson (University of Regina), Corey MacKenzie (University of Manitoba), Natalie Mota (University of Manitoba, Department of Clinical Health Psychology), and Lesley Graff (University of Manitoba, Department of Clinical Health Psychology). In addition to predominantly sharing a common geographic location (Asmundson completed doctoral training at the University of Manitoba), researchers in this network also focus on mental health and trauma research topics.
Finally, University of British Columbia (UBC) Network emerged as a loosely integrated network or “bubble.” Although UBC has one of the larger Health Psychology programs in Canada, the faculty at UBC are only generally connected with each other. The largest and most integrated node is Eli Puterman, but also includes Anita DeLongis, Nancy Sin, Christiane Hoppmann, and Eric Kim. Of note, other UBC faculty (Frances Chen and Wolfgang Linden) are primarily connected elsewhere in the network.
Although the network is largely interconnected, there are several researchers that are only narrowly-associated with the main network or are completely unconnected satellite networks (Figure 2). It is not clear why these individuals are not more integrated into the network, and it is possible that several reasons are at play. For example, research interests could be more closely allied with other fields (e.g. developmental psychology, biology), despite doing health psychology-related research; some are housed at smaller and/or undergraduate-focused universities (e.g. Lakehead University, Mount Allison University). There are also no clear patterns with respect to where a researcher trained (in or out of Canada), rank/role (range from Assistant to Full Professor) or research topics, which also include pain, aging, sexual health, and cancer.
Discussion
The purpose of this environmental scan was to characterize the state of university-affiliated health psychologists and their activities in Canada, including characteristics, affiliation and geography; scholarly productivity; areas of expertise derived from university profiles and research products; and interconnections examined using a collaboration network analysis. The environmental scan revealed a large number of university-affiliated health psychologists and health-specific concentrations in Canada, which speaks to the strength of the field given the relatively small population of Canada and relative youth of health psychology as a discipline. There were some surprising gaps and growth opportunities noted. Although Canada’s position as an international “cross-roads” is cited as a strength (Brock, 2013; Hadjistavropoulos, 2009), the majority of academics were trained in Canada or the US, with little representation from Europe, and no representation from Asia, Africa, Central America or South America. It is possible that this is because most Canadian universities prioritize hiring Canadian citizens in order to prevent “brain drain” to the U.S. and protect jobs for Canadians and Permanent Residents. Another cause could be regional differences in academic structure and culture, making it difficult for trainees from outside the Canadian or U.S. systems to re-integrate post-graduation. Another cited differentiator is Canada’s cultural diversity and the challenges of being a large country with a small population (Brock, 2013; Hadjistavropoulos, 2009), and yet research related to culture, race, ethnicity, discrimination, or prejudice—particularly for Indigenous and immigrant populations—was not strongly represented, and even less research was related to rural or geographic-related health or healthcare challenges. Regardless, Canadian health psychologists are a highly productive group, representing a range of research interests, training locations, and background disciplines.
The number of university-affiliated health psychologists identified is large (N = 284). Speaking to the relative newness of the field, however, many academics did not specifically identify “health psychology” as their field of study on dissertations, or identify themselves as “health psychologists” in faculty profiles. Moreover, there is reason to believe that there are more university-affiliated health psychologists than were identified here. A key challenge was that not all departments maintain online profiles for all faculty. After Psychology Departments, health psychologists were most likely to be housed in Medicine and Health Science faculties, which were also less likely to provide detailed online faculty profiles. Although adjunct faculty were included in search criteria, few were identified because most universities did not maintain online profiles for adjunct faculty. It is also possible that, given the interdisciplinary nature of health psychology, some faculty are housed in non-psychology and non-health/medicine departments, and could have been missed by our search. To address these challenges, future research could adopt a more active approach, reaching out to departments, contacting faculty and/or professional colleges directly, or through maintenance of a “living” database where health psychologists self-identify and opt-in. Identifying university-affiliated health psychologists in Canada (and elsewhere) will continue to be a challenge that could be made more difficult by a possible tendency for the term “health psychology” to be appropriated by non-psychology disciplines. For example, the Health Psychology and Behavioural Medicine area at the University of Alberta is housed in the Faculty of Kinesiology, yet had no psychology-trained academics affiliated with the program. Additional research should explore the extent to which “health psychology” topics, research products, or grant applications are generated by professionals in psychology versus in other fields.
Several geographic trends emerged. Notably, the Clinical Health Psychology Department (University of Manitoba) emerged as a unique cluster of health psychologists. This department was the only one dedicated entirely to health psychology, and was the largest in Canada by far. It is the only department with a primarily clinical focus, as opposed to a traditional focus on research and teaching. Consistent with this, approximately a third of the department produced no research products between Jan 2018 and Mar 2021. Nonetheless, a University of Manitoba-centered community was identified in the collaboration network analysis, indicating that a proportion of academics in this department have active and integrated research programs, and collaborate with other academics primarily in Manitoba and Saskatchewan.
With respect to the more traditional research and teaching academics, Montreal, QC, emerged as the health psychology hub in Canada. After Winnipeg (and the Clinical Health Psychology Department), Montreal had the largest concentration of university-affiliated health psychologists, and two universities with health psychology-specific concentrations. The Montreal region also produced most of the conventionally-housed health psychologists, and had a tendency to retain trainees as faculty (especially the Université de Montreal). It is possible retention is due to language barriers, with the majority of primarily-French universities existing in Quebec and thus limiting opportunities for Francophones outside this province. Montreal also housed two of the largest collaborator networks in Canada. The Greater Toronto Area also emerged as a health psychology hub in Canada, with the second largest concentration of university-affiliated health psychologists (11%), and two universities with health psychology-specific concentrations. Although half that of Montreal, the Greater Toronto Areas was nonetheless responsible for producing a significant proportion of the university-affiliated health psychologists identified in this scan, and for retaining trainees in the region. The Greater Toronto Area did not emerge as a basis for a collaborator network, suggesting that this region is not as well integrated as Montreal. Although Montreal and the Greater Toronto Area are clear hubs, productivity did not significantly differ between Montreal, the Greater Toronto Area, or cities with other large concentrations of university-affiliated health psychologists (Ottawa, Calgary).
That geographic hubs do appear is noteworthy given that Canada has a small population spread over a large geography, and breaking down geographic silos and developing cross-country collaborations is difficult. However, geographic proximity is not sufficient for the development of integrated hubs. For example, neither the University of British Columbia nor the Calgary region emerged as clear or closely integrated communities in the collaborative network analysis, despite having large concentrations of university-affiliated health psychologists and/or health-specific concentrations. Similarly, although the Montreal Network and Sexual Health Network were both primarily located in Montreal, these networks are largely independent of each other. Although many networks had common research themes (e.g. pain, sleep, or sexual health), a more consistent unifying factor were trainee-rooted collaborator relationships, either due to a former mentor-mentee relationship or among members of a trainee cohort. Indeed, the Montreal-Sleep network, Pain Network, Campbell Network, University of Manitoba Network, and possibly the Sexual Health Network all had evidence of foundations in trainee-linked and maintained collaborative relationships, regardless of current location or primary research focus. In other words, although geographic proximity and common research interests are important, trainee-rooted collaborative relationships (and possibly friendships) seem to be at the heart of the most integrated and productive Canadian health psychology networks. Of note, this pattern suggests that traditional academic approaches, where trainees are “kicked out of the nest” post-graduation and expected to establish a research program independent of their former mentors, could actually penalize early career investigators by depriving them of resources available in established and productive networks. 2 Beyond this environmental scan, research into the role of trainee cohorts and maintained mentor-mentee relationships in establishing productive research programs should be more broadly explored, and could be a means to foster collaborations that cross geographic regions.
The collaborator network analysis also revealed a large number of university-affiliated health psychologists who were tenuously or not at all connected to the network. It is not clear why some individuals are well integrated and others are not. It is possible that there is not one but many reasons for why a university-affiliated health psychologists might lie at the edge or outside of the network. Nonetheless, it would be beneficial to follow-up with these researchers to understand why they are not better integrated, and to find ways to integrate them into the larger Canadian health psychology network, if possible or applicable.
This study revealed that Canadian health psychologists are addressing globally-relevant health issues with an aim to promote health and treat illness. Of note, a disconnect was observed between research topics from faculty profiles verses journal article keywords. This could be for two reasons: Faculty profiles may not be updated regularly, and so may not capture evolving research programs (e.g. COVID research) as effectively as journal article keywords. And profile analysis included faculty with active research programs and those without (e.g. primarily teaching, administrative or clinical focuses), which could account for differences in faculty profiles verses journal article keywords. Research on pain, sleep, cancer, and depression were major themes in the national health psychology research agenda, with solid contributions in sexual and reproductive health, health behaviors, healthcare, and treatment. Speaking to the impact of COVID-19 and the nimbleness of Canadian health psychologists, pandemic-related research was also identified, despite this context only affecting the last year of the research product search window. Although these were the dominant areas of research, the research profile and keyword analyses also revealed a broad range of topics across health psychology.
Environmental scans of fields by country have several potential uses. First, they provide a basis for professional organizations to reach out and intentionally develop professional and regional communities. More integrated communities foster collaborative opportunities and foundations for policy and funding advocacy. Second, mapping out expertise can be used as a resource for researchers to find potential collaborators and identify reviewers for grants and manuscripts. And third, this work can be used by trainees as a “road map” of health psychology in Canada, to identify potential supervisors and graduate programs.
There are several limitations to consider. First, this environmental scan represents a snapshot in time of Canadian health psychology from 2018 to 2020. Total number of university-affiliated health psychologists, geographic concentrations, collaborative networks, and productivity will change over time. Second, it is likely that the total of university-affiliated health psychologists is an underestimation due to a variety of reasons. Moreover, many health psychologists are practicing clinicians without a research program or university affiliation (or are adjunct faculty, who are difficult to identify due to lack of university profiles). The expertise of these individuals is an important part of the health psychology landscape, but was not captured here due to a focus on university-affiliated psychologists. This scan also did not consider graduate or post-doctoral trainees who also substantially contribute; it would be useful to determine where health psychology trainees are employed post-graduation and the areas of research they ultimately pursue. Third, due to limitations in information available from faculty profiles, it was not possible to make statements about diversity amongst university-affiliated health psychologists, specifically with respect to race/ethnicity, gender identity, and nationality. This information is typically self-identified. Follow up research will be needed to obtain this information. It is also possible that some faculty profiles were out-of-date. Nonetheless, based on information obtained in this scan, the Territories (and Indigenous peoples more broadly) are likely not represented or are under-represented in Canadian health psychology. Fourth, an obstacle to doing keyword and collaborator network analyses is the range of terms and author names used. It was not uncommon to find misspelled collaborator names or researchers who published under more than one professional name. Approaches to journal article keywords also varied, with many researchers using vague terms. Although the data were cleaned as much as possible, connections and keyword classifications could have been missed. Given that Canadian health psychology is already difficult to differentiate, researchers in this field should take care to stand out as much as possible by using distinct professional names and consistent terminology in journal keywords. And fifth, although this study could speak to training origins of faculty who are currently employed at Canadian universities, it is not possible to make statements about post-graduation employment for Canadian health psychology graduates overall. Future research will need to explore career trajectories and employment opportunities for Canadian health psychology trainees specifically.
This environmental scan represents the first comprehensive assessment of health psychology faculty, research, and their interconnections. It is clear that the landscape of health psychology research in Canada is broad and vibrant, with key areas of strength and clusters of researchers. There are opportunities for institutions and national and regional health psychology organizations and societies to draw from these findings; to enhance collaboration, recruitment, and diversity of health psychology faculty; and to disseminate and showcase health psychology research in Canada.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053221124748 – Supplemental material for Health psychology and behavioral medicine researchers in Canada: An environmental scan
Supplemental material, sj-docx-1-hpq-10.1177_13591053221124748 for Health psychology and behavioral medicine researchers in Canada: An environmental scan by Kharah M Ross, Ryan Hoggan, Tavis S Campbell, Jennifer Gordon, Vincent Gosselin Boucher, Eric Kim, Kim Lavoie, Wolfgang Linden, Joshua A Rash, Codie R Rouleau, Sherry H Stewart and Justin Presseau in Journal of Health Psychology
Research Data
sj-docx-2-hpq-10.1177_13591053221124748 – Supplemental material for Health psychology and behavioral medicine researchers in Canada: An environmental scan
Supplemental material, sj-docx-2-hpq-10.1177_13591053221124748 for Health psychology and behavioral medicine researchers in Canada: An environmental scan by Kharah M Ross, Ryan Hoggan, Tavis S Campbell, Jennifer Gordon, Vincent Gosselin Boucher, Eric Kim, Kim Lavoie, Wolfgang Linden, Joshua A Rash, Codie R Rouleau, Sherry H Stewart and Justin Presseau in Journal of Health Psychology
Research Data
sj-sav-3-hpq-10.1177_13591053221124748 – Supplemental material for Health psychology and behavioral medicine researchers in Canada: An environmental scan
Supplemental material, sj-sav-3-hpq-10.1177_13591053221124748 for Health psychology and behavioral medicine researchers in Canada: An environmental scan by Kharah M Ross, Ryan Hoggan, Tavis S Campbell, Jennifer Gordon, Vincent Gosselin Boucher, Eric Kim, Kim Lavoie, Wolfgang Linden, Joshua A Rash, Codie R Rouleau, Sherry H Stewart and Justin Presseau in Journal of Health Psychology
Research Data
sj-sav-4-hpq-10.1177_13591053221124748 – Supplemental material for Health psychology and behavioral medicine researchers in Canada: An environmental scan
Supplemental material, sj-sav-4-hpq-10.1177_13591053221124748 for Health psychology and behavioral medicine researchers in Canada: An environmental scan by Kharah M Ross, Ryan Hoggan, Tavis S Campbell, Jennifer Gordon, Vincent Gosselin Boucher, Eric Kim, Kim Lavoie, Wolfgang Linden, Joshua A Rash, Codie R Rouleau, Sherry H Stewart and Justin Presseau in Journal of Health Psychology
Research Data
sj-sps-5-hpq-10.1177_13591053221124748 – Supplemental material for Health psychology and behavioral medicine researchers in Canada: An environmental scan
Supplemental material, sj-sps-5-hpq-10.1177_13591053221124748 for Health psychology and behavioral medicine researchers in Canada: An environmental scan by Kharah M Ross, Ryan Hoggan, Tavis S Campbell, Jennifer Gordon, Vincent Gosselin Boucher, Eric Kim, Kim Lavoie, Wolfgang Linden, Joshua A Rash, Codie R Rouleau, Sherry H Stewart and Justin Presseau in Journal of Health Psychology
Research Data
sj-xlsx-6-hpq-10.1177_13591053221124748 – Supplemental material for Health psychology and behavioral medicine researchers in Canada: An environmental scan
Supplemental material, sj-xlsx-6-hpq-10.1177_13591053221124748 for Health psychology and behavioral medicine researchers in Canada: An environmental scan by Kharah M Ross, Ryan Hoggan, Tavis S Campbell, Jennifer Gordon, Vincent Gosselin Boucher, Eric Kim, Kim Lavoie, Wolfgang Linden, Joshua A Rash, Codie R Rouleau, Sherry H Stewart and Justin Presseau in Journal of Health Psychology
Research Data
sj-xlsx-7-hpq-10.1177_13591053221124748 – Supplemental material for Health psychology and behavioral medicine researchers in Canada: An environmental scan
Supplemental material, sj-xlsx-7-hpq-10.1177_13591053221124748 for Health psychology and behavioral medicine researchers in Canada: An environmental scan by Kharah M Ross, Ryan Hoggan, Tavis S Campbell, Jennifer Gordon, Vincent Gosselin Boucher, Eric Kim, Kim Lavoie, Wolfgang Linden, Joshua A Rash, Codie R Rouleau, Sherry H Stewart and Justin Presseau in Journal of Health Psychology
Footnotes
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an Athabasca University Academic Research Fund grant (PI: Ross; File No. 24164).
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.