
Abstract
A decade of ongoing armed conflict in Syria has damaged the physical and mental health of millions of adults and children. This study aimed to systematically review the prevalence of post-traumatic stress disorder among youth exposed to the Syrian conflict, and understand its individual and contextual determinants. The screening procedure resulted in 26 studies, with a total of 11,400 Syrian children and adolescents. The prevalence was 36% (95% CI (0.29–0.43), p < 0.001). Loss of family members or acquaintances, witnessing violence, and social withdrawal increased the risk of post-traumatic stress disorder, while social trust and social support were protective factors.
Introduction
The Syrian crisis has entered its 10th year, with an—ongoing—armed conflict exposing Syrians to violence and deprivation, and damaging their physical and mental health. Since 2011 over 5.5 million people have fled the country and 6 million have been internally displaced, leading Syria from the third-largest refugee-hosting country in the world to the largest refugee-producing country (UNHCR, 2018). In 2019, the total number of Syrian children in need of humanitarian aid exceeded 8 million; 2.6 million were internally displaced, and over 2.5 million were registered as refugees in host countries (UNICEF, 2019).
According to the World Health Organization (WHO), more than 20% of those living in conflict-affected areas suffer from mental illness, and about 10% from moderate to severe illness (World Health Organization, 2019). Conflict-related emotional trauma can occur not only as a result of direct exposure to violence, but also as a result of indirect stressors such as disruption of daily life, displacement, and economic hardship (Giordano et al., 2019). Even after reaching host countries, many of those difficulties remain and acculturation-related mental health issues emerge, like those related to clashing of native and host cultural values (Karadag et al., 2018; Killian et al., 2018; Tabur et al., 2019).
Children and adolescents are especially vulnerable to the physical and psychological consequences of armed conflicts, commonly affected by mental disorders such as depression, anxiety, and post-traumatic stress disorder (PTSD) (Attanayake et al., 2009). A month after exposure to a traumatic event, about 70% of children may develop stress reaction behaviors and, within the first year, 20%–30% may have full diagnostic criteria for PTSD (Attanayake et al., 2009).
PTSD’s definition by the ICD-11 includes re-experiencing the traumatic event, perceiving being under threat, and avoiding reminders (Bryant, 2019). The DMS-5 definition is more detailed, comprising four symptom clusters: (1) psychological distress at exposure to trauma reminders, distressing dreams, intrusive memories, dissociative reactions, (2) avoidance of reminders, either external (e.g. situations, conversations) or internal (e.g. thoughts, memories), (3) two or more cognitive or mood changes (as the inability to remember aspects of the event, lack of interest and detachment, inability to experience positive emotions), and (4) two or more arousal symptoms (as hypervigilance, sleep disturbance, loss of concentration, irritable behavior and angry outbursts, and reckless or self-destructive behavior) (Bryant, 2019). These symptoms must manifest after experiencing or witnessing a major traumatic event and persist for at least a month (Bryant, 2019). Without support and treatment, PTSD hinders children’s psychosocial development and has serious effects on their academic and social performance, putting them into further deprivation (Attanayake et al., 2009; Killian et al., 2018).
During the last decade, Syrian children and adolescents have been exposed to traumatic events and daily life struggles, with a significant effect on their psychological well-being (Tabur et al., 2019). Indeed, one study conducted in 2016 showed that PTSD was the most prevalent mental health disorder among 8–15-year-olds studying in Syrian public schools (Tabur et al., 2019). However, recent psychosocial studies have discovered that children have the potential for resilience, allowing them to become functional individuals despite their childhood traumas (Karadag et al., 2018). Though, their limited access to mental health care services, due to the shortage of adequately trained professionals and facilities, language barriers in the new post-emergency contexts (Hassan et al., 2016), and denial, misunderstanding, and stigma associated with mental illness, may have hindered their recovery (Hassan et al., 2016; Hedar, 2017).
Some studies have assessed the prevalence of PTSD among children and adolescent refugees (Attanayake et al., 2009; Killian et al., 2018). However, a systematic approach and meta-analysis focusing on the children and adolescents exposed to the Syrian conflict are much needed to grasp its magnitude in this group and identify its risk and protective factors, while considering the very specific characteristics of this population, as the specificities of their life paths, contexts, and culture (Giordano et al., 2019; Karadag et al., 2018). This knowledge can feed policymakers and organizations to better address PTSD, and promote their present and future mental health, well-being, and professional growth. Thus, this systematic review and meta-analysis aim to fill in this gap and assess the prevalence of PTSD among youth exposed to the Syrian conflict and identify its risk and protective, individual and contextual, determinants.
Methodology
Inclusion and exclusion criteria
The studies included in this systematic review and meta-analysis followed several selection criteria. First, we included all studies published between March 15th, 2011 (the start of the Syrian conflict) and January 1st, 2021. Second, we included studies assessing the prevalence of PTSD among Syrian children and adolescents (up to 18 years old), regardless of their country of placement, or visa legal status. Third, we only considered studies with primary data on the prevalence of PTSD among children and adolescents; as such, qualitative studies, case reports, or others without these data were excluded. Fourth, the diagnosis of PTSD could have been given by clinical psychiatric interviews or by self-report questionnaires done by trained professionals. Fifth, there were no limits for the sample size. Sixth, there were no language restrictions.
Search strategy
We undertook a systematic search strategy during November and December 2020 in MEDLINE (via PubMed), Scopus, and PsycINFO databases. We used a combination of Medical Subject Headings (MeSH terms) with related search keywords to widen the search records scope and minimize the fallout of missed studies. We included Post-Traumatic Stress Disorder (or other potential equivalents as PTSD, Posttraumatic Stress Disorders, Stress Disorder, Post Traumatic, Stress Disorders, Posttraumatic, Acute Post-Traumatic Stress Disorder, Chronic Post-Traumatic Stress Disorder, Delayed Onset Post-Traumatic Stress Disorder, Moral Injury, Neuroses, Post-Traumatic, Neuroses, Posttraumatic), child (or child*, preschool, infant) and adolescent (or adolescen*, teen*, youth), Syria (or Syrian). The search strategy was adapted for each database.
We further examined each article’s reference list to find further eligible studies. Gray literature was also included, both from references’ scan and from Google Scholar, searching reports from nongovernment international organizations such as United Nations High Commissioner for Refugees (UNHCR), United Nations International Children’s Emergency Fund (UNICEF), and WHO that could provide data on the prevalence and determinants of PTSD in Syrian children and adolescents.
One author screened titles and abstracts. When abstract or title screening was not enough to opt for inclusion or exclusion of the article, a full-text review was done to verify if the studies met the inclusion and exclusion criteria (namely if they presented primary data on the prevalence of PTSD among children or adolescents). If there were hesitations over the eligibility of particular studies, those were resolved by a second author. Only when consensus was reached, these studies were retained. Articles not written in English (n = 1) were translated (from Turkish to English) using an online translation website (https://www.translate.com/).
Data extraction
We extracted the prevalence of PTSD, method of assessment (self-report questionnaire vs personal psychiatric interview), sample size, participants characteristics as age and gender, country and duration of stay, citizenship status, traumatic events type, and risk or protective factors. Factors were characterized as “risk” or “protective” if statistical analyses showed statistically significant positive or negative associations with PTSD, or “no association” when the association was not statistically significant. These data were assessed by both authors independently.
Risk-of-bias appraisal
The quality of the included studies was assessed by both authors using a study assessment tool provided by the U.S. National Health Institute (available online at https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools). Items related to study quality such as internal and external validity, reporting bias, confounding, and conflict of interest were assessed by the first author, and doubts were discussed with a second author (see Supplementary File).
Meta-analysis
We performed a meta-analysis to estimate the PTSD prevalence of the pooled included studies using STATA software (Stata 13.1 for mac) with Metaprop command (Nyaga et al., 2014) and a random-effects model.
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, and this study protocol was registered in PROSPERO (CRD42021226619).
Results
Description of the studies included
A flowchart outlines the three databases search results (PubMed, Scopus, and Psych INFO) and the grey literature selection of studies (Figure 1).
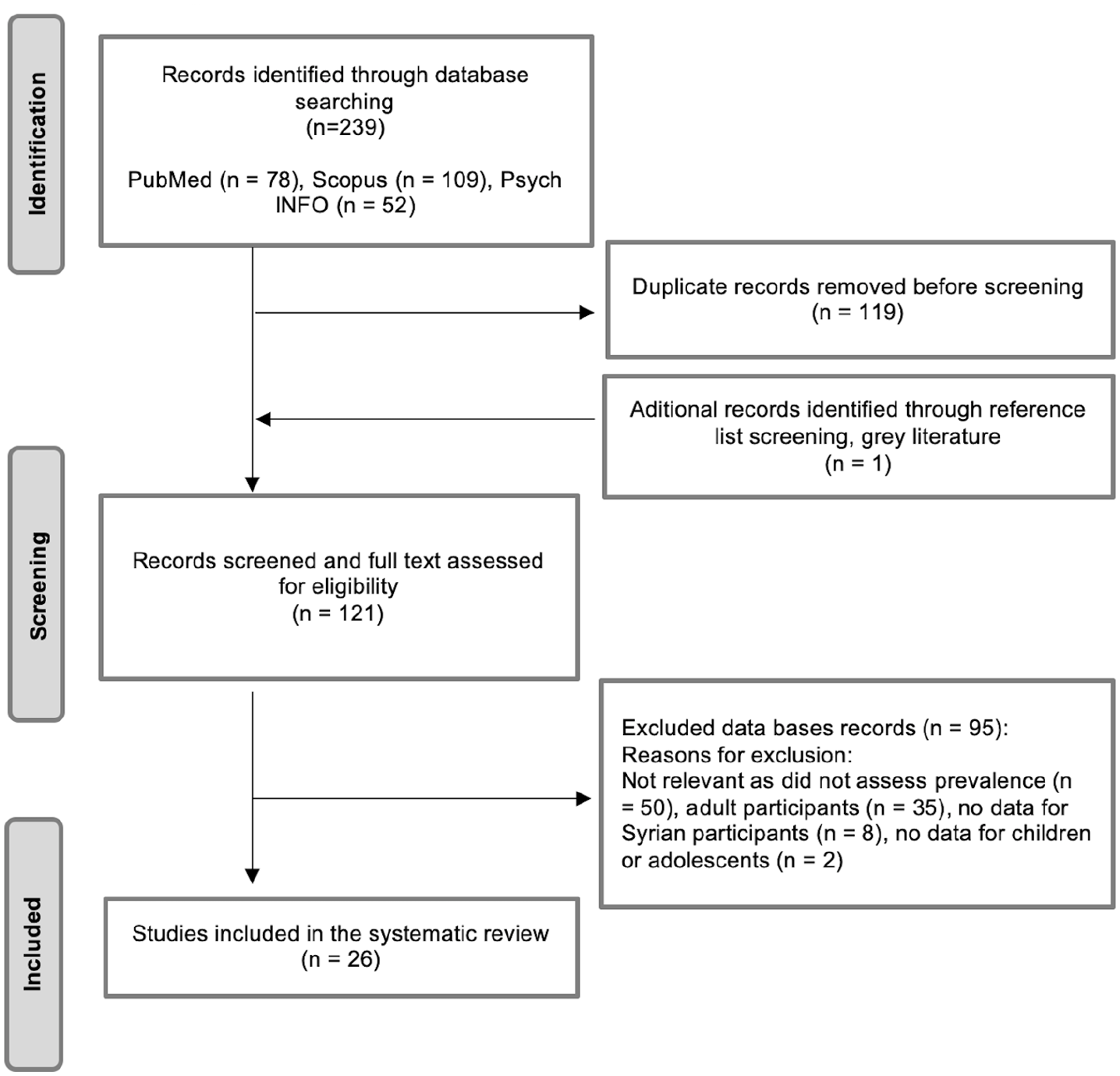
Flow diagram of data sources included.
The search of electronic databases yielded a total of 239 publications, to each one gray literature publication was added. After removing 119 duplicates, 121 documents were screened based on title and abstract and, when the information there included was not sufficient, full-text assessment. Out of 121 records, 95 records were excluded as they did not mention prevalence (n = 50), only included adults or did not show data stratified by age group (n = 37), or did not provide data relative to Syrian refugees (n = 8).
A total of 26 studies about Syrian child and adolescent populations fulfilled the inclusion criteria, with a total of 11,401 observations. Most studies were performed in the Middle-east: 14 studies were conducted in Turkey, three in Jordan, one in Lebanon, one study included participants from Lebanon and Jordan, and two in Syria. There were six studies in Europe—four in Germany, one in Sweden, and one in Italy; and one study referred to the United States.
Sample sizes ranged between 31 and 1773 participants: four studies with less than 50 participants, three with 50–100 participants, three with 100–200 participants, and 16 with 200 or over. Studies included participants from both genders, most with a balance between female and male proportions.
Regarding the studies’ quality assessment, all studies’ populations were clearly specified, and exposure measures and outcomes were clearly defined, valid, and reliable (Supplementary File). All inclusion and exclusion criteria were prespecified. Nonetheless, most studies did not provide sample sizes justification nor information about power description or effect estimates. As expected, none of the outcome assessors were blinded to the exposure status of participants to the conflict in Syria.
PTSD prevalence estimates
PTSD prevalence estimates ranged between 6.3% and 65.3%. Most studies (n = 22) used self-report questionnaires as assessment tools of PTSD, namely the Children’s Revised Impact of Event Scale-8 (CRIES-8) (n = 7) and the UCLA PTSD Reaction Index for the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) (n = 5). Four studies used clinical psychiatric interview assessment.
The meta-analysis estimated a 36% pooled prevalence (95% CI (0.29–0.43), p < 0.001) (Figure 2). Studies assessed using questionnaires had a pooled prevalence of 38% (95% CI (0.30–0.46), p < 0.001), while those that used interviews had a pooled prevalence of 25% (95% CI (0.05–0.45), p < 0.001). As shown in Figure 2, estimates are substantially heterogeneous, with about half of the studies with prevalences ranging from 10.5% to 35.1% and the other half from 40% to 65.2%. I2 was 98.56%, which means that most of the variance of the results reflects variance in true prevalences estimates instead of sampling error.
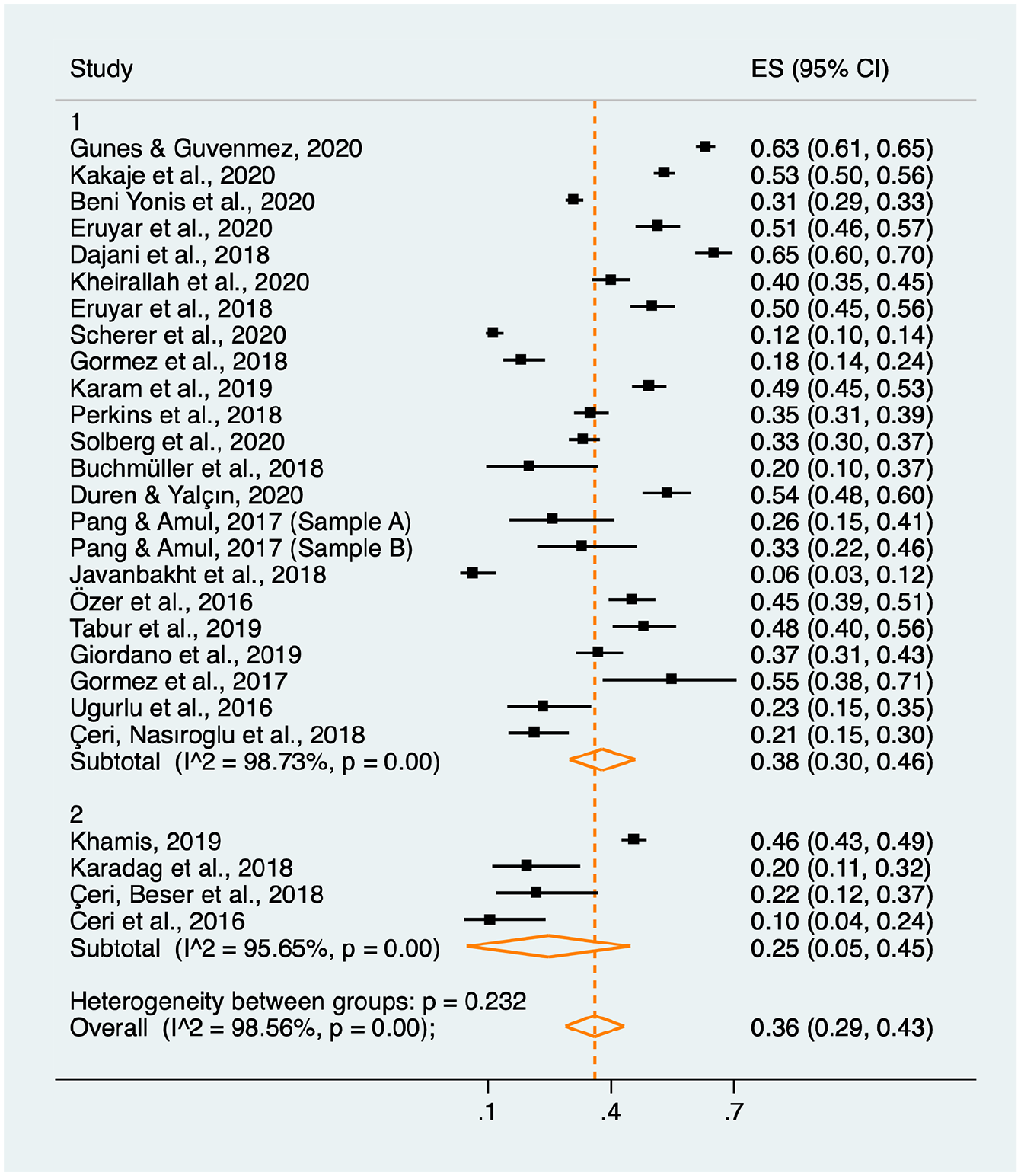
Forest plot with meta-analysis results.
Risk and protective factors
Twelve studies identified conflict-related traumatic events (Beni Yonis et al., 2020; Çeri et al., 2018a, 2018b; Eruyar et al., 2018; Giordano et al., 2019; Gormez et al., 2018; Gunes and Guvenmez, 2020; Kakaje et al., 2022; Karam et al., 2019; Khamis, 2019; Perkins et al., 2018; Tabur et al., 2019), namely death of parents, family members, or acquaintances, having witnessed violence against someone, clashes, or blasts, or having seen injured people or dead bodies. Being internally displaced, living in Damascus (Syria) compared to Latakia (Syria), and in Lebanon compared to Jordan, showed an increased risk for PTSD in two studies (Khamis, 2019; Perkins et al., 2018), while longer stays in host countries was found as a protective factor in one (Khamis, 2019).
Childhood adversities, as abuse and neglect were identified by Karam et al. (2019) as risk factors for PTSD in Syrian children and adolescents, and Giordano et al. (2019) identified socioeconomic deprivation as a risk factor, but these factors were not found significant by others (Beni Yonis et al., 2020; Kakaje et al., 2022; Perkins et al., 2018; Scherer et al., 2020). Coping through social withdrawal, self-criticism, and resignation were assessed as risk factors by Khamis (2019). Differently, social trust and social support were found to be protective factors (Duren and Yalçın, 2021; Khamis, 2019), alongside cognitive restructuring, expressing feelings inside the family (Khamis, 2019), and emotionally warm parenting (Eruyar et al., 2020).
Being a female was a risk factor in five studies (Beni Yonis et al., 2020; Kakaje et al., 2022; Perkins et al., 2018; Scherer et al., 2020; Tabur et al., 2019) while being a male was a risk factor in a study by Kheirallah et al. (2020). Considering age, it was associated with a higher risk of PTSD in the Scherer et al. (2020) study. Living with eight or more family members was a protective factor in one study (Scherer et al., 2020), but Perkins et al. (2018) did not find any association between family size and PTSD. Khamis (2019) did not find any association with the school environment, nor did Gormez et al. (2018) with speaking the host countries’ language or satisfaction with living conditions.
The detailed results can be found in Table 1.
Summary of the characteristics and data extracted from the included studies.
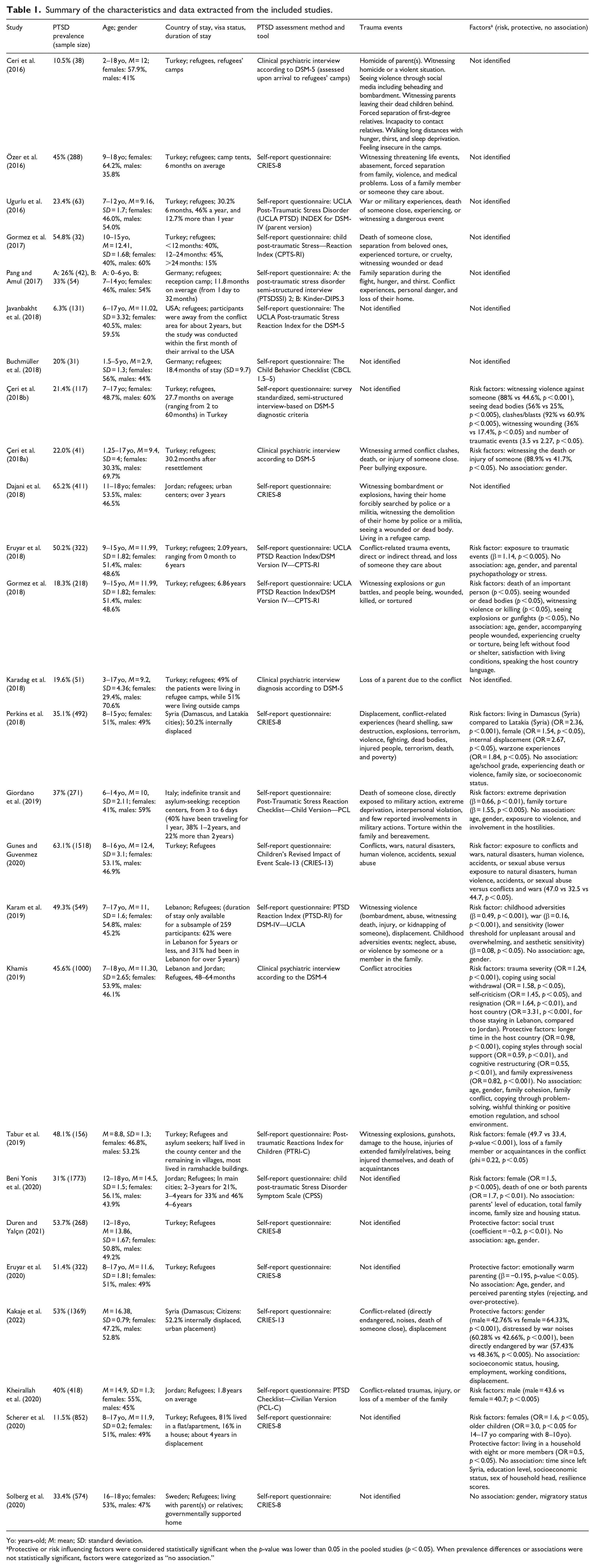
Yo: years-old; M: mean; SD: standard deviation.
Protective or risk influencing factors were considered statistically significant when the p-value was lower than 0.05 in the pooled studies (p < 0.05). When prevalence differences or associations were not statistically significant, factors were categorized as “no association.”
Discussion
This systematic review showed that 6.3%–65.3% of Syrian children and adolescents exposed to the 2011 Syrian conflict were affected by PTSD, with a pooled estimate of 36% (95% CI (0.29–0.43), p < 0.001). Trauma events were mostly related to the conflict, as witnessing physical aggressions, seeing clashes, blasts, injured people or corpses, and the loss of parents, family members, or acquaintances. Childhood adversities and the use of coping mechanisms based on social withdrawal, resignation, and self-criticism were associated with PTSD. Coping mechanisms based on social trust and social support, emotionally warm parenting and expression of feelings and cognitive restructuring were protective factors.
Our estimates of prevalence are higher than those estimated by Alisic et al. (2014) or Blackmore et al. (2020) meta-analysis. However, the first included children and adolescents exposed to interpersonal and non-interpersonal trauma, assessing 25.2% and 9.7% prevalence of PTSD in these subgroups, respectively, and Blackmore et al. (2020) meta-analysis was on refugees and asylum seekers overall, estimating 22.7% prevalence of PTSD. If the estimates of the prevalence of PTSD among Syrian children and adolescents exposed to the conflict were also higher these found in these meta-analyses and higher than those estimated among Lebanese peers after conflict (8.5%–32.5%) (Shaar, 2013), they were similar to the estimates of 34.1% of prevalence among Palestinian children (Khamis, 2005).
We hypothesize that the higher prevalence of PTSD among these children and adolescents may be due to the extreme levels of violence they were—and continue to be—exposed to during the conflicts in these two countries, as well as the extreme deprivation lived in certain areas, and forced displacement. As Alisic et al. (2014) had shown, children and adolescents exposed to interpersonal violence had higher risks of PTSD, and the studies here-analyzed repeatedly reported traumatic exposures as violence and death of loved ones, and several showed associations between these factors and PTSD (Beni Yonis et al., 2020; Gormez et al., 2018; Tabur et al., 2019). Several authors have also discussed the devastating effect of the loss of parents or beloved persons in the life of a child, increasing their short- and long-term risk of mental health disorders, including PTSD (Boelen and Spuij, 2013; Boelen et al., 2017; Luecken and Roubinov, 2012). Alongside witnessing death, seeing a corpse, and/or injury of someone (Ceri et al., 2016, 2018a, 2018b), witnessing violence, clashes, and blasts, experiencing extreme deprivation, internal and external displacement experience, or family abuse were factors that increased the risk of PTSD (Çeri et al., 2018b; Eruyar et al., 2018; Giordano et al., 2019; Gunes and Guvenmez, 2020; Perkins et al., 2018).
Contextual factors
Living in Damascus was a risk factor compared to living in Latakia, both in Syria (Perkins et al., 2018), and living in Jordan was a protective factor compared to living in Lebanon (Khamis, 2019). A longer stay in the host country was associated with lower PTSD rates (Khamis, 2019). Participants hosted in lower-income countries seemed to present higher PTSD rates than those settled in high-income countries, such as northern European countries and the USA. This could indicate that more deprived contexts can contribute to higher PTSD rates among children’s refugees, which is consistent with the considerably higher estimates of PTSD among children and adolescents living in low- and middle-income countries than in high-income countries found in Yatham et al. (2018) literature review. Less deprived contexts may provide better access to social, educational, and health services, as well as better employment and living conditions, which may contribute to higher protection against PTSD and support individuals’ recovery. These contextual differences may explain, at least partially, the heterogeneity of the prevalence estimates observed in this meta-analysis.
Social support
Social support and social trust seem to have a protective influence on PTSD rates, as well as higher family attachment levels (Duren and Yalçın, 2021; Kakaje et al., 2021), while social withdrawal was a risk factor (Khamis, 2005; Tabur et al., 2019). These results are in line with the extensive review of the literature collected by Charuvastra and Cloitre (2008), which shows the importance of social bonds for the maintenance of mental health and/or recovery from PTSD.
Family size did not show a significant influence in most of the studies. Although larger families could indicate stronger social support and a lower risk of PTSD (Scherer et al., 2020), this influence can also be reversed by the fact that larger families can be at higher risk of deprivation, which could hinder their capacity to recover from traumatic experiences (World Bank, 2021).
Socioeconomic status
The literature shows an association between low socioeconomic status and PTSD among conflict-affected populations (Bogic et al., 2015; Chen et al., 2017). Porter and Haslam’s (2005) meta-analysis points to a linear relationship between refugees’ mental health and their socioeconomic status, including access to employment. From the studies here-analyzed, one indicated that socioeconomic deprivation was a risk factor (Giordano et al., 2019) but other studies did not find a significant association with PTSD (Beni Yonis et al., 2020; Kakaje et al., 2022; Perkins et al., 2018; Scherer et al., 2020). The difference between what the literature reports and what was assessed in the pooled studies may be due to some factors: first, most socioeconomic strata was touched by the conflict in Syria and, second, Syrian refugees in the Middle East are living under the poverty line, which may diminish the differentiation between higher and lower incomes (World Bank, 2021). Also, there are significant differences in the living standards between Syria and the surrounding countries in where these findings were reported, as Lebanon and Jordan, and as well as with other countries where many socioeconomic status questionnaires are validated. In addition, responses to questions about parents’ income may have an important response bias, as these questions may not be considered convenient in the Syrian culture (Kakaje et al., 2022).
Demographics
The role of age in aggravating or alleviating the risk of PTSD is inconsistent, as most studies found no association and one study found that older age was a risk factor (Scherer et al., 2020). Though, the small age span in the samples here included may have limited the capacity to discern the effect of age on the risk of PTSD.
As of gender, the literature suggests that female gender could be a risk factor for PTSD in children (Garza and Jovanovic, 2017), which was not clearly observed in this systematic review, as eight studies did not find any association of female gender with PTSD (Çeri et al., 2018b; Duren and Yalçın, 2021; Eruyar et al., 2018, 2020; Giordano et al., 2019; Karam et al., 2019; Khamis, 2005; Solberg et al., 2020), five studies found it to be a risk factor (Beni Yonis et al., 2020; Kakaje et al., 2021; Perkins et al., 2018; Scherer et al., 2020; Tabur et al., 2019) and one study showed female gender as a protective (Gormez et al., 2018; Kheirallah et al., 2020). These mixed results may be due to several factors: (i) the conflict affected civilians, not merely military groups (usually constituted by males), (ii) in the Syrian community females generally are more protected and less exposed to the external environments whereas males are expected to take some of the adults’ responsibilities, (Kheirallah et al., 2020), and (iii) differences in how male and female children and adolescents experienced the conflict may vary according to cultural, ethnic and socioeconomic groups, and between geographic areas.
Limitations
These results must be interpreted taking into account the following limitations. First, though the prevalence of PTSD has been analyzed by several studies, few have been concerned with its determinants—namely psychosocial, socioeconomic, cultural, and political contexts—which may limit the identification of some contextual determinants of PTSD.
Second, 15 out of 26 studies selected participants from schools. We admit this represents a more accessible way to collect data, but as there is a considerable drop in school percentage among refugee and Syrian children—according to the World Bank, more than half of school-age children in Jordan and Lebanon (World Bank, 2021)—the existing studies may be leaving outside an important part of this population. This vulnerable population may be undocumented, with no access to education, living in poor conditions, working illegally, and at a higher risk of being exposed to violence, namely to multiple forms of abuse including sexual abuse (UNHCR, 2017; UNICEF, 2015, 2017). These children and adolescents are, thus, at further risk of PTSD and our pooled prevalence may be underestimated.
Third, the majority of pooled studies (n = 22) used self-report questionnaires as an assessment tool. However, the reliance on self-report questionnaires with cut-off scores to determine PTSD diagnoses might not be validated for the population here studied (Blackmore et al., 2020; Kakaje et al., 2022; Khamis, 2005). Literal translation to the participants’ native language may not be enough, as an adaptation to the participants’ cultural background must be ensured. Moreover, the study of the association of PTSD with other different mental disorders was not done in most studies. The assessment of other mental health problems that probably occur in these populations, as anxiety and depression disorders, is needed to better understand PTSD and its interaction with other mental illnesses.
Fourth, our meta-analysis included two different assessment methods—self-report questionnaires and clinical psychiatric interview diagnoses. Despite being different in nature, and the different prevalence estimates (38% vs 25%), confidence intervals overlap (95% CI (0.30–0.46) vs 95% CI (0.05–0.45)).
Fifth, the studies analyzing this public health problem in Syria covered only two large cities (Damascus and Latakia), whereas other regions are still exposed to ongoing conflict, severe social and economic deprivation, and, nowadays, to the COVID-19 pandemic effects (Kakaje et al., 2022; Perkins et al., 2018).
Sixth, only cross-sectional studies were found in our search, which does not allow us to assess the evolution of PTSD in these groups nor the impact of some determinants in its aggravation or mitigation. Cross-sectional data do not allow for strong inferences regarding the temporal ordering, though it makes logical sense to expect PTSD to follow after a salient life disruption such as those experienced due to the Syrian crisis.
Conclusion
This study showed that PTSD occurs in 36% of children and adolescents exposed to the 2011 Syrian conflict, a higher estimate than those found in studies with children and adolescents exposed to other traumatic events or conflicts in other regions. The exposure to the conflict itself, as having experienced the death of a close family member or acquaintance or witnessed traumatic events such as clashes and violence, was associated with PTSD in these children and adolescents, but social withdrawal and low parental/maternal attachment were also risk factors. Differently, a positive social environment, with social trust and social support, protected these children and adolescents against PTSD.
This knowledge emphasizes the urgent mental health needs of conflict-affected populations, particularly Syrian children and adolescents, and encourages policymakers to ensure that social and economic safe and supportive environments are provided for a more sustainable recovery and development of these young people.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053221123141 – Supplemental material for Post-traumatic stress disorder in youth exposed to the Syrian conflict: A systematic review and meta-analysis of prevalence and determinants
Supplemental material, sj-docx-1-hpq-10.1177_13591053221123141 for Post-traumatic stress disorder in youth exposed to the Syrian conflict: A systematic review and meta-analysis of prevalence and determinants by Gabriel Kanan and Teresa Leão in Journal of Health Psychology
Research Data
sj-docx-2-hpq-10.1177_13591053221123141 – Supplemental material for Post-traumatic stress disorder in youth exposed to the Syrian conflict: A systematic review and meta-analysis of prevalence and determinants
Supplemental material, sj-docx-2-hpq-10.1177_13591053221123141 for Post-traumatic stress disorder in youth exposed to the Syrian conflict: A systematic review and meta-analysis of prevalence and determinants by Gabriel Kanan and Teresa Leão in Journal of Health Psychology
Footnotes
Acknowledgements
TL and JK conceptualized the article. JK performed data acquisition and manuscripts screening. JK and TL verified for inclusion/exclusion and quality assessment, performed data analysis and interpretation of the results, and wrote the manuscript. Both authors approved the final manuscript.
Data sharing statement
The current article includes the complete raw data-set collected in the study including the participants’ dataset, syntax file and log files for analysis. It is available in the Figshare repository and as Supplemental Material via the SAGE Journals platform.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
No ethical approval is needed for this review.
Informed consent
No informed consent was needed.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.