
Abstract
We sought to establish whether two recently developed measures, the 5C scale and the Vaccination Attitudes Examination (VAX) were reliable and valid for use with older adults. A total of 372 UK-dwelling participants (65–92 years, M = 70.5 years, SD = 4.6) completed a cross-sectional survey measuring health and socio-demographic characteristics in relation to vaccine uptake for influenza, pneumococcal and shingles. The 5C and VAX scales were administered to test their reliability, validity and dimensionality. Both scales showed good internal reliability and convergent, discriminant and concurrent validity. Their factor structures were also confirmed, supporting their use with older adult populations.
Introduction
Outbreaks of vaccine-preventable diseases (VPDs) are a growing international concern particularly in the context of the COVID-19 pandemic (Suryadevara, 2021; Gallant et al., 2021). As a result of these outbreaks there is an urgent need to focus on the development and evaluation of screening tools to identity those who may be hesitant about vaccine(s) and to inform interventions to increase vaccine uptake. Vaccine hesitancy (VH) has contributed to outbreaks of VPDs across a range of socio-cultural contexts and populations (Murphy et al., 2021; Sallam, 2021; Wiysonge et al., 2021). Although there is a lack of consensus in terms of how to define VH, it can be understood as the mental state of holding back, in doubt or indecision regarding vaccination (Bedford et al., 2018). VH includes a broad spectrum of attitudes, beliefs and behaviours including vaccine refusal and intentional vaccine delay (Ryan and Malinga, 2021). While there has been a growing body of research exploring VH among children, parents and diverse adult populations and occupational groups (Alfieri et al., 2021; Noyman-Veksler et al., 2021; Quinn et al., 2019; Saied et al., 2021; Santibanez et al., 2020; Shahar et al., 2017), there is need for further work incorporating the expanding demographic of older adults (aged ⩾65 years), given that they are recognised as an ‘at risk’ group for VPDs (Bhagianadh and Arora, 2022; Nicholls et al., 2021; Privor-Dumm et al., 2021; Talbird et al., 2020).
Due to decreased immunity and greater likelihood of existing chronic health conditions, older adults are more susceptible to infectious diseases and have altered immune response to vaccinations (Coll et al., 2020; Russell et al., 2018). Vaccination can support healthy ageing and efforts to increase uptake among older adults seek to reduce morbidity, mortality and loss of quality of life associated with VPDs (Ozawa et al., 2016). Vaccination uptake varies by vaccine (Klett-Tammen et al., 2016); despite the availability of effective vaccines, many countries fail to reach recommended coverage levels (Doherty et al., 2018). Within the UK, older adults (aged ⩾65 years) are freely offered an annual influenza vaccine, a single-dose pneumococcal vaccine and a single-dose shingles (aged 70–79 years) vaccine. However, uptake has been found to fall below the World Health Organisation’s (WHO’s) target of 75% (Dios-Guerra et al., 2017; Sheikh et al., 2018). For influenza vaccination, between 2004–05 and 2019–20, uptake has fluctuated between 71% and 75% among older adults (Health Protection Scotland, 2021b). Pneumococcal vaccination uptake is typically around 51%–69% (Briggs et al., 2019; Frank et al., 2020), and shingles uptake rates can be lower than 50% (Health Protection Scotland, 2021a).
Given these uptake rates, it is important to understand the reasons for low uptake and/or VH. A recent population-level cohort study of UK adults (aged ⩾65 years) found that uptake for influenza, shingles and pneumococcal vaccination are patterned by ethnicity, deprivation, household size and comorbidities (Tan et al., 2021). In addition, psychosocial factors are increasingly being recognised as providing important insights into the determinants of vaccination behaviour (Betsch et al., 2018, 2020; Schmid et al., 2017). Measuring vaccination-related psychosocial factors is necessary to identify target populations, determine potential reasons for under-vaccination and inform the design of tailored and cost-effective interventions (Butler and MacDonald, 2015; Eitze et al., 2021). Recently, two self-report measures, the 5C scale (Betsch et al., 2018) and the Vaccination Attitudes Examination (VAX) Scale (Martin and Petrie, 2017), have been developed to help identify reasons why people do or do not vaccinate. The 5C scale is a novel measure of five psychological antecedents, or precursors, of vaccination behaviour: confidence, complacency, constraints, calculation and collective responsibility. The VAX scale assesses attitudes that may underlie VH across four domains: mistrust of vaccine benefit, worries about unforeseen future effects, concerns about commercial profiteering, and preference for natural immunity. These measures are useful for predicting vaccination behaviour; however, to date, their reliability and validity have yet to be confirmed in older adults aged ⩾65 years. While the 5C scale has been tested once with slightly older adults, this sample was middle aged (M = 48 years). The VAX scale has been tested with young adults only (typically those in their 20s and 30s) and, therefore, it is not known if it can distinguish between vaccinating and non-vaccinating older adults.
Presently, we aimed to test the reliability, validity and dimensionality of the 5C (Betsch et al., 2018) and VAX (Martin and Petrie, 2017) scales with UK-dwelling older adults (aged ⩾65 years) in relation to VH for influenza, pneumococcal and shingles. We sought to test the psychometric properties of these scales and use confirmatory factor analysis to elucidate their underlying factor structures, thereby supporting their generalisability with an older adult population. Further, we aimed to establish their internal consistency and discriminant and convergent validity. Building upon earlier work assessing independent predictors of older adults’ vaccination uptake (Nicholls et al., 2021), the concurrent validity of the 5C and VAX was also examined.
Methods
Participants
Participants were 372 older adults aged 65–92 years (M = 70.5 years, SD = 4.6). Participants were living in the UK, generally in good health, not diagnosed with a neurological condition and living independently in the community (see Table 1 for socio-demographic characteristics).
Participants’ socio-demographic data.
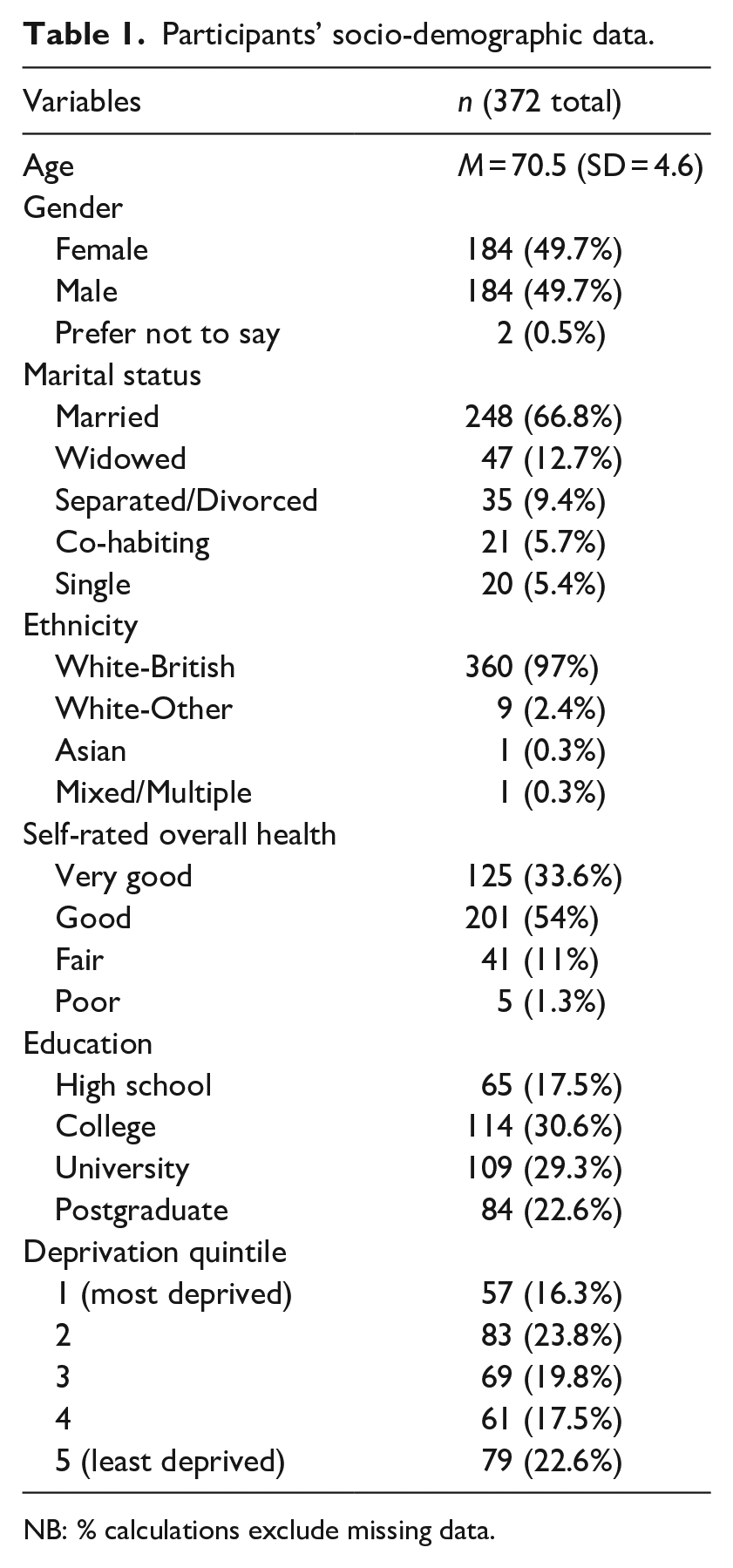
NB: % calculations exclude missing data.
Procedure
An online, cross-sectional survey was administered using Qualtrics. Data collection took place between 8th February and 17th March 2020, prior to the first COVID-19 lockdown in the UK. Participants were recruited through university participation panels and social media (e.g. Twitter and Facebook).
Measures
The online survey included the 5C (Betsch et al., 2018) and the VAX (Martin and Petrie, 2017). We included other measures related to VH; the Beliefs About Medicines Questionnaire (BMQ; Horne et al., 1999), the Perceived Sensitivity to Medicines scale (PSM; Horne et al., 2013) and the Medical Mistrust Index (MMI; LaVeist et al., 2009). We also included measures that we considered theoretically not to be highly related to VH; the Perceived Stress Scale (PSS; Cohen et al., 1994) and the Interpersonal Support Evaluation List (ISEL-12; Cohen et al., 1985) (see Supplemental Table for description of measures). Participants were asked their age, gender, marital status, ethnicity, self-reported overall health, education and socio-economic status. Participants were also asked whether they had received the influenza vaccination in the past 12 months and if they had ever received the pneumococcal vaccination. Those aged 70 and older were asked about previous uptake of the shingles vaccination. Self-reported vaccine status has been found to be a sensitive and fairly specific indicator of actual vaccine status (Irving et al., 2009).
Data analyses
Analyses were performed using SPSS version 23. First, internal consistency using MIIC rather than Cronbach’s α was used due to the low number of items in each subscale. Next, to verify the structural validity of the 5C and VAX scales, confirmatory factor analysis (CFA) was performed. The following indices of model fit were considered: comparative fit index (CFI), the Tucker Lewis Index (TLI), root mean square error of approximation (RMSEA) and standardised root mean square error of approximation and MIIC. CFI and TLI values between 0.90 and 0.95 and RMSEA values between 0.05 and 0.08 are indicative of acceptable model fit (Chen, 2007; Hu and Bentler, 1999; Kline, 2005). Convergent validity was examined using the correlations between the 5C and VAX with the BMQ, PSM and MMI. Discriminant validity was assessed by examining the correlations between the 5C and VAX with the PSS and IESL-12. Finally, concurrent validity was assessed using logistic regressions (correct classification rates) within each scale, to determine if they successfully predicted vaccination behaviour (dependent variable: vaccinated yes/no for influenza, pneumococcal and shingles). All tests were two-tailed, and p < 0.05 was considered statistically significant.
Results
Internal reliability
For the 5C, good internal consistency was found across all subscales (with MIIC > 0.15): confidence, MIIC = 0.74; complacency, MIIC = 0.30; constraints, MIIC = 0.47, calculation MIIC = 0.58 and collective responsibility MIIC = 0.32. For the VAX, a total mean score MIIC = 0.45 was obtained with subscales: mistrust of vaccine benefits, MIIC = 0.74; worries over unforeseen future effects, MIIC = 0.49; concerns about commercial profiteering, MIIC = 0.73; and preference for natural immunity, MIIC = 0.67; all demonstrated good internal consistency. The 5C and VAX were found to be reliable measures for use with an older adult population.
Factor structure of 5C and VAX
The factor structure of the 5C and VAX was assessed using CFA. CFA was run on all 5C subscales and the 12 VAX items grouped into four subscales (three items per subscale). For the tested models, RMSEA values were reasonable (values near to 0.08). The CFI and TLI were above the acceptable value of 0.90 (5C: CFI = 0.959, TLI = 0.946; VAX: CFI = 0.978, TLI = 0.970) suggesting good fit and verifies the structural validity of the scales when tested with an older adult population. The 5C and VAX were found to have sound factor structures, when tested with an older adult population.
Convergent and discriminant validity
Table 2 shows the correlations measuring associations between the mean 5C subscale scores, VAX total score and MMI, BMQ and PSM total means for the sample. Mean 5C subscale scores and VAX total scores correlated positively with MMI, BMQ and PSM, showing good convergent validity. Discriminant validity was assessed by examining the correlations between the mean 5C subscale scores and VAX total score with PSS and IESL-12. As expected, these correlations were found to be weaker than those observed with the BMQ, PSM and MMI. Both the 5C and VAX showed good convergent and discriminant validity, supporting their use with older adult populations.
Correlation matrix of associations between mean VAX total and 5C scores and relevant questionnaires to test convergent and discriminant validity.
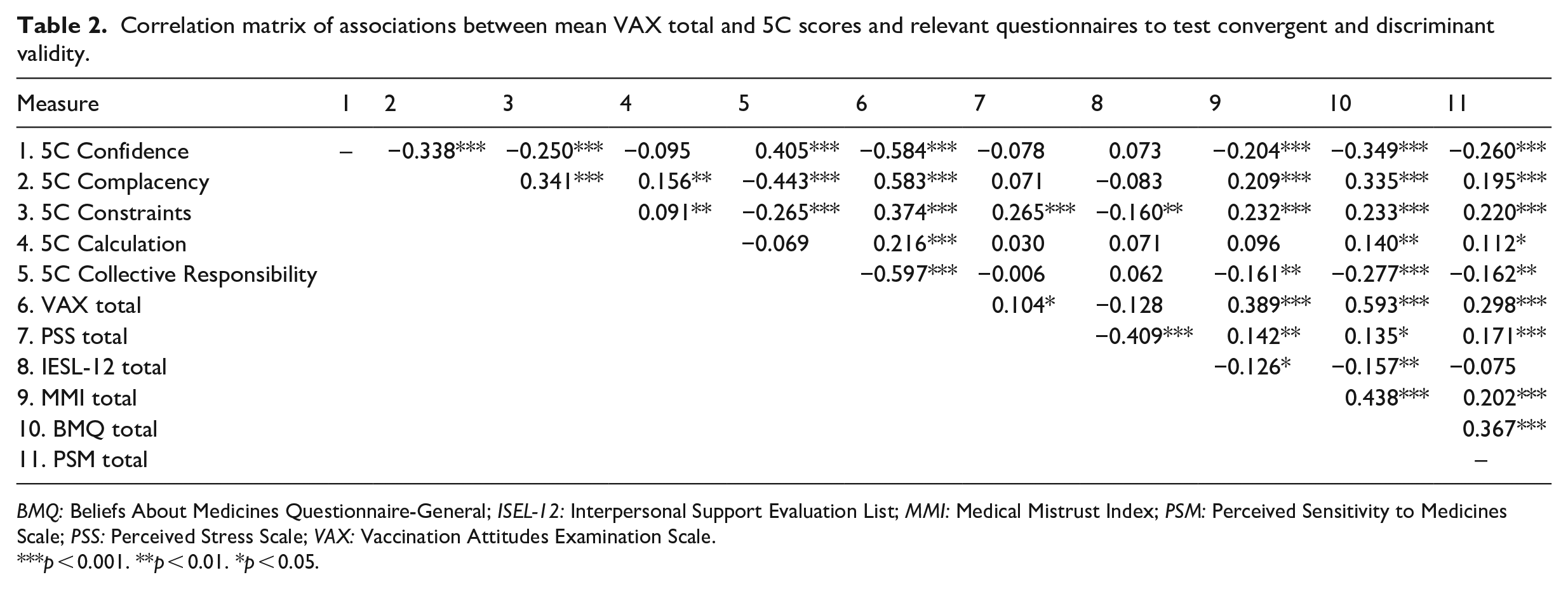
BMQ: Beliefs About Medicines Questionnaire-General; ISEL-12: Interpersonal Support Evaluation List; MMI: Medical Mistrust Index; PSM: Perceived Sensitivity to Medicines Scale; PSS: Perceived Stress Scale; VAX: Vaccination Attitudes Examination Scale.
p < 0.001. **p < 0.01. *p < 0.05.
Concurrent validity
Concurrent validity was assessed using logistic regression to determine if the 5C and VAX scales successfully predicted vaccination behaviour (vaccinated yes/no) for influenza, pneumococcal and shingles. Multivariate logistic models were constructed to determine the independent predictors of lack of vaccine uptake for each vaccine. Results (see Table 3) showed that both the 5C and VAX scales were able to correctly classify vaccinators and non-vaccinators across each of the vaccines, thus showing good concurrent validity.
Multivariate logistic regression analyses within the 5C and VAX Scales for predicting older adults’ non-uptake of influenza, pneumococcal, and shingles vaccines.
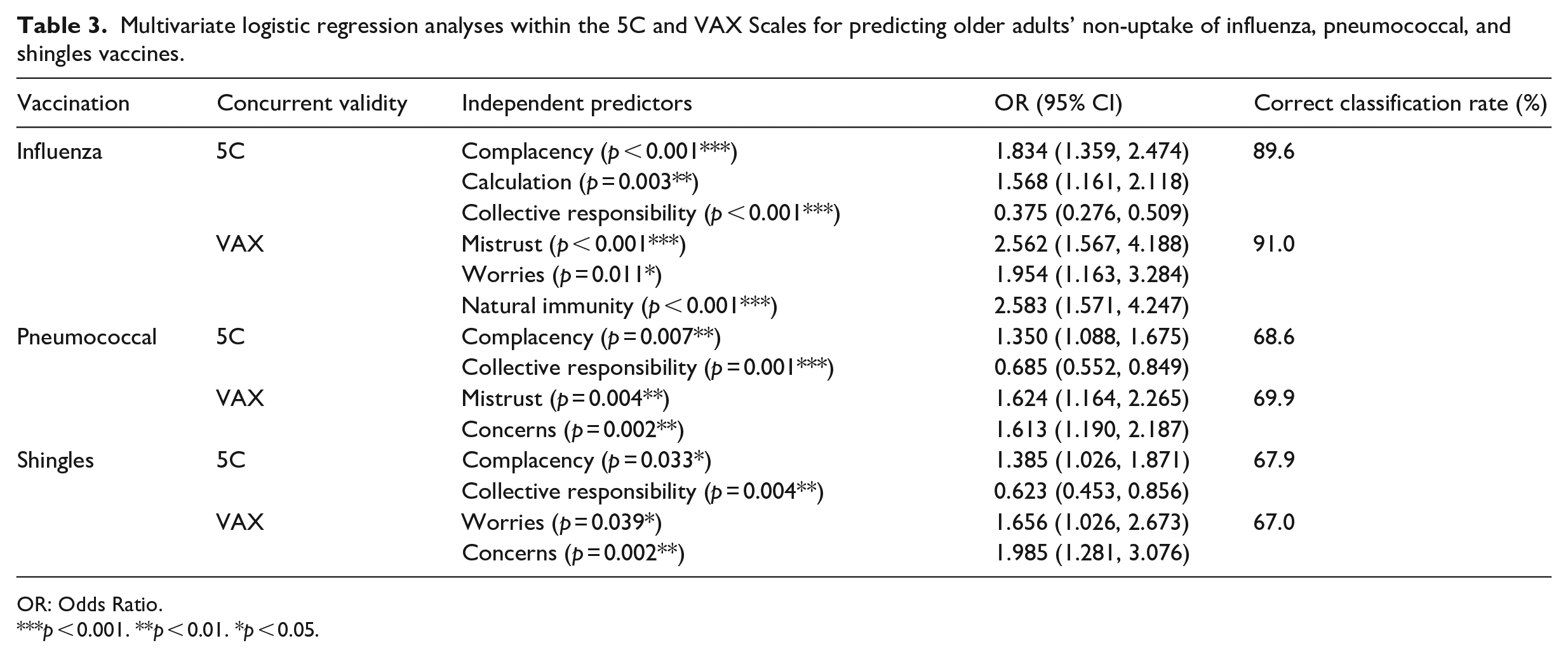
OR: Odds Ratio.
p < 0.001. **p < 0.01. *p < 0.05.
Discussion
To our knowledge, our study is the first to establish the reliability and validity of the 5C (Betsch et al., 2018) and VAX (Martin and Petrie, 2017) scales, two psychosocial measures of vaccine uptake, in an older adult population. Our study revealed satisfactory psychometric properties for both measures as the results were indicative of statistically sound factor models. The 5C and VAX were shown to have good internal consistency and good levels of convergent and discriminant validity. As reported in earlier work, psychosocial factors independently predicted older adults’ hesitancy towards the influenza, pneumococcal and shingles vaccines (Nicholls et al., 2021). Presently, these findings additionally show that the two scales have good concurrent validity.
The 5C and VAX contribute to metrics which aim to assess VH (Betsch et al., 2018; Huza, 2020; Martin and Petrie, 2017; Wood et al., 2019) through demonstrating that both these measures are reliable and valid for use with an older adult (aged 65+) population. Such measures can be used to inform targeted public health action to increase vaccine uptake with older adults, using appropriate strategies, policies and interventions to reduce VH, and during mass screening and vaccination campaigns (Frank et al., 2020; Jarrett et al., 2015; Nicholls et al., 2021). Given the pressures on healthcare systems during the COVID-19 pandemic, having sound measures of VH with older adults, who may be more vulnerable to adverse outcomes, has come into strong focus (Roller-Wirnsberger et al., 2021). This is pertinent given that recent longitudinal work suggests that the pandemic has led older adults to re-evaluate the importance of vaccination and may have increased their willingness to protect others; however, concerns about vaccine side effects were found to have significantly increased during the pandemic (Gallant et al., 2021). These findings are also consistent with previous research relating to COVID-19 vaccines among diverse populations, where participants have raised concerns about vaccine side effects (Domnich et al., 2020; Pogue et al., 2020; Williams et al., 2020). Understanding and measuring ongoing structural and psychosocial barriers to vaccination is essential (Baraniuk, 2021).
Future studies are recommended to determine the relationship between psychosocial and other factors associated with older adults’ vaccine uptake using the 5C and VAX. Given that participants in the current study were high functioning and were living independently at home with minimal assistance, the findings may not be generalisable to older adults with lower functional abilities, for example, those who are experiencing cognitive impairment or limitations in everyday functioning (Nicholls et al., 2021). Further work could therefore explore the psychometric properties and feasibility of the 5C and VAX in more diverse populations of older adults (e.g. ethnic minorities, LGBTQ+, varied functional levels) and socio-cultural contexts (e.g. low-income countries); This is essential given increasing evidence that minority and/or vulnerable populations face challenges due to inequitable access, discrimination and systemic suppression which impacts on vaccine uptake (Corbie-Smith, 2021; Garg et al., 2021). Longitudinal studies are also required to establish their ability to predict outcomes such as objective measurements of vaccination uptake relative to the total number of recommended dosages. Furthermore, it is possible that participants may report less VH face-to-face than through an anonymous online survey, which may encourage self-disclosure on sensitive items (Hollier et al., 2017). It would be useful for future work to evaluate possible differences in VH using the 5C and VAX with online surveys, telephone surveys and face-to-face assessments. Given that older adults are at increased risk of disease morbidity, including VPDs, targeting research to inform intervention programmes to increase uptake, using psychometrically validated measures of VH, is of paramount importance. This is particularly pertinent given the global challenges associated with the dynamic, complex and changing nature of COVID-19, highlighting the need for ongoing research on VH (Holeva et al., 2022; Karafillakis et al., 2022; Reno et al., 2021). Measuring and monitoring VH among older adults and using this information to inform policy (Sprengholz et al., 2021) and intervention developments to increase vaccine uptake is essential (Higgins et al., 2021; Motta et al., 2021). Developing a better understanding of older adults’ perceived risks versus benefits of vaccines not only involves measuring attitudes and beliefs concerning vaccines but also engaging with health practitioners, media, governmental bodies and community organisations to increase awareness of the burden of VPDs (Van Buynder and Woodward, 2019) and the risks associated with VH (Dube et al., 2013). Indeed, a recent longitudinal randomised controlled study conducted with older adults, who were especially vulnerable to primary and secondary diseases, recommended that interventions aiming to reduce VH might be more effective in specific contexts and locations such as doctors’ clinics (Eitze et al., 2021). Using the 5C and VAX in conjunction with other measures of VH such as the Multidimensional Vaccine Hesitancy Scale (Howard, 2021) may be particularly useful in capturing the changeable nature of VH and help inform the development of adaptive interventions. Given the heterogeneity in VH and the diversity of situations and contexts in which it can arise; screening tools and interventions aiming to address VH may benefit from being both context and problem-specific (Ryan and Malinga, 2021), as well as seeking to understand population-specific challenges (Kristensen et al., 2016; Tan et al., 2022).
Conclusion
Globally, in developed and developing countries alike, a demographic shift towards an ageing population is underway. Many VPDs inflict a disproportionate burden of disease in older adults but may be prevented or attenuated by vaccination. Vaccine uptake by this population is generally low and must be substantially improved if the potential of vaccines to reduce the morbidity, mortality, loss of quality of life and health and social care costs caused by VPDs is to be realised. Importantly, the available evidence indicates that VH in older adults can be reduced. Having reliable and valid measures of VH is essential, however, in order to better understand and develop tailored and targeted interventions to address VH among this population. In our work, the 5C and VAX scales were found to be reliable and valid measures of VH with a UK-dwelling, older adult (65+) population. Future research could use these scales to evaluate the impact of psychological antecedents of vaccine uptake, and how concerns about vaccination may be challenged and reversed in older adults. Improved measurement and targeted education around VPDs, disease risk and vaccine benefits is required to increase vaccine coverage. It is hoped that these findings will influence future research and intervention development with older adults aimed at achieving this. The 5C and VAX scales are therefore useful to help understand the health and vaccination attitudes that promote and deter older adults’ vaccination behaviours. Behavioural and psychosocial research can support the design and measurement of effective vaccination interventions directed towards older adults, aiming to reduce VH and increase uptake. A multi-dimensional approach measuring VH using the 5C and VAX, along with ensuring access to vaccines, will be important. The lessons learned from the COVID-19 vaccination drive will also aid in the successful implementation of subsequent vaccinations and in efforts to reach those older adults who may be most resistant to vaccines. Further work is needed in order to design evidence-informed responses to VH appropriate to the setting, context and hesitant subgroup. Given the ageing population and corresponding increases in healthcare resource utilisation required to treat VPDs, we recommend particular attention be directed towards research focussing on ‘at risk’ older adult populations.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-docx-1-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-docx-2-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Supplemental Material
sj-docx-3-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-docx-3-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Supplemental Material
sj-docx-4-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-docx-4-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Supplemental Material
sj-docx-5-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-docx-5-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Supplemental Material
sj-docx-6-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-docx-6-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Supplemental Material
sj-spv-1-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-spv-1-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Supplemental Material
sj-spv-2-hpq-10.1177_13591053221089104 – Supplemental material for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people?
Supplemental material, sj-spv-2-hpq-10.1177_13591053221089104 for Improving older adults’ vaccination uptake: Are existing measures of vaccine hesitancy valid and reliable for older people? by Nicola Cogan, Allyson J Gallant, Louise A Brown Nicholls, Susan Rasmussen, David Young and Lynn Williams in Journal of Health Psychology
Footnotes
Data sharing statement
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Chief Scientist Office, Scottish Government [grant number CGA/19/52].
Ethical approval
Ethical approval (34/26/11/2019/Staff) was granted by the School of Psychological Sciences and Health Ethics Committee (SEC19/20: Williams et al., 2020). Approved on 8th January 2020. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.