
Abstract
Active components of psychological intervention for RAP remain unclear. This study involved completing interviews about parental experience of psychological intervention for RAP to ascertain how and why psychological intervention can be effective. Difficulty making sense of RAP and barriers to treatment were identified as struggles. Acceptance and containment were key overlapping mechanisms, which allowed families to develop a changed relationship with the pain and manage the impact of pain. To further develop interventions, the role of containment should be considered and acceptance-based interventions explored, given the growing evidence base in this area. Practical implications of this research are also discussed.
Recurrent abdominal pain (RAP) is a condition frequently seen in paediatric settings and is associated with impairment in the everyday life of children and their families (Abbott et al., 2017). To diagnose RAP, the abdominal pain must be present for at least 2 months and occur at least four times per month. It must also not meet criteria for medical conditions or physiological events (Schmulson and Drossman, 2017). RAP tends to impede the child’s ability to continue activities of daily living (ADLs) and has significant impact upon life in the family and peer relationships (Asmundson et al., 2012).
Children experiencing RAP are found to show greater levels of emotional distress and have poorer coping strategies compared to control groups (Youssef et al., 2008). If not treated, RAP can persist into adulthood, which can lead to chronic pain, anxiety, depression and other significant impacts upon quality of life (QOL) (Abbott et al., 2017). It is imperative for RAP to be effectively treated in childhood, to minimise long-term implications.
Although causes of RAP are often unknown and can remain unclear even after treatment, a number of dietary, pharmacological and psychosocial interventions have been investigated and indeed studies show a role of physiological processes, personality traits and temperaments in the development of RAP (Martin et al., 2017). Other hypotheses point towards underlying anxiety, stress in the family and parental anxiety (Newton et al., 2019). Currently, RAP is viewed within a bio-psycho-social model, with physical, emotional and environmental factors contributing towards the presentation (McOmber and Shulman, 2007).
First-line treatment involves diagnostic work-ups and providing reassurance that there are no underlying diseases. Following potential medical causes being investigated, a diagnosis of RAP is frequently given where no physical explanation for the pain has been identified (Paul and Candy, 2013). Some families continue to seek medical explanations and find it difficult to accept that one has not been found (Masia-Warner et al., 2009). Caregivers can experience significant anxiety, overwhelming fear of underlying diseases, and helplessness as they feel unable to relieve their child’s symptoms (Paul and Candy, 2013). While the pain may not have a named physical cause, it is a very real experience for children and families. Families can view referrals to psychology as ‘failure’ to find explanation for the pain, which in turn can be interpreted as determining physical versus psychological causes or a pain being real or imaginary (Masia-Warner et al., 2009).
There are a variety of therapeutic approaches to treating RAP, including Cognitive Behavioural Therapy (CBT) approaches, family approaches and online interventions. Common factors across these are aims to improve coping strategies, support families to recognise and manage symptoms and reduce anxiety and impact of pain on ADLs (Abbott et al., 2017). However, the mechanisms of how these interventions work are largely unknown. A recent Cochrane review found some evidence for benefits of CBT and hypnotherapy in reducing pain in the short term and recommended the need to identify active components of the interventions and to decipher if benefits are maintained long term (Abbott et al., 2017).
As family is the most central element of social context, family factors should be considered when investigating RAP (Logan and Scharff, 2005). Systemic influences can impact a child’s experience of pain, and parental modelling can also influence how children respond to pain (Stone et al., 2018). Parental anxiety and/or depression, preoccupation with health concerns and family stressors have also been detailed as potential precipitating factors to RAP (Stone et al., 2018). By interviewing parents, researchers can increase understanding into the family experience of RAP.
There is currently a lack of research on the experience of children and families in relation to RAP and psychological interventions. Recent studies involved interviewing children and parents about their experience, but both these studies were specific to evaluating a particular online intervention (Nieto et al., 2019, 2020). Both studies highlighted that education about pain; relaxation and distraction techniques, communication skills, emotional regulation and changing negative thoughts about pain were helpful. However, neither of these studies looked at families’ understanding of RAP, or the experience of completing in-person interventions or the experience of psychological intervention as a whole.
The recent Cochrane review also highlighted a lack of congruence in how treatment success with RAP is measured. Some studies reported on number of children being completely pain free, others reporting pain intensity, frequency and duration, and others using scales to assess QOL or functional impairment (Abbott et al., 2017). Again, there is a gap in the research on the experience of service users on the impact of the intervention. Qualitative studies in this area will provide information about complex, multidimensional and subjective factors of RAP that is difficult to obtain from self-report questionnaires (Morse, 2015).
Given that research has outlined a need to determine the active components of interventions, it is important to look at the experience of families, in what they view as useful components of interventions, how they understand and interpret pain, and what are successful outcomes from their perspective. This study aims to increase understanding of the experience of RAP and useful components of clinical interventions. This will help guide the development of interventions and aid effective delivery of services.
Method
Participants
Inclusion criteria for the study were parents of children age 6 to 16 who had completed psychological intervention for diagnosed RAP within the 12 months prior to data collection. Exclusion criteria were participants who had not yet completed input with psychology or who had identified risk issues around self-harm/ suicidal ideation. Recruitment of participants took place between November 2020 and February 2021. Fifteen participants were contacted via telephone by the research team and asked if they would like to participate. Fourteen participants had expressed interest and were sent information sheets and consent forms via post and advised to return completed consent forms. Ten consent forms were received during the period of recruitment. Participants were parents of children age 6-16 who had completed psychological intervention for RAP within the previous 12 months with Children’s Health Ireland at Temple Street.
Materials
Due to the Covid-19 pandemic, it was agreed by the ethics committees that telephone interviews would be the most appropriate means for collecting data. Interviews took place via telephone in a confidential space using an encrypted audio recorder. Recordings were coded so they remained anonymous. Audio recordings were then transcribed verbatim by the researcher, with all identifying information removed upon transcription. Recordings were then deleted in order to protect patient confidentiality.
Procedure
Participants completed individual semi-structured interviews about their experience of their child’s psychological intervention for RAP. In creating the interview schedule, the researchers were curious about the impact of RAP, how families felt about referrals to psychology and what was helpful/unhelpful. This was guided by previous literature where there were hypotheses about family stressors as precipitators to RAP, or parental worries about RAP (Masia-Warner et al., 2009). This was also guided by curiosity about helpful aspects of psychological interventions for this population given the gap in this area of research. The researcher used a semi-structured interview schedule as a guide to the conversation. The focus of each question remained the participant’s experience. Prompts were given, such as ‘what was that like for you?’ or ‘how did you feel about that?’ in order to keep the focus on the participant’s experience. Participants were recruited from Children’s Health Ireland at Temple Street. Study advertisements were completed and given to Psychologists in the Child and Adolescent Mental Health Team. Informed written consent forms were sent to those who expressed interest. Once completed consent forms were received, interviews were scheduled with the researcher. Interviews took place via telephone call and were audio recorded using an encrypted audio recorder and transcribed by the researcher. Interviews took approximately 50 minutes (ranging 35 minutes–1 hour). Transcripts were then analysed using Interpretive Phenomenological Analysis (IPA).
Ethics
Ethical approval was provided from The Research and Ethics Committee at Children’s Health Ireland at Temple Street (Reference number: 19.064) and from the School of Psychology Research Ethics Committee at Trinity College Dublin (Approval ID: SPREC022020-09).
Analysis
Interviews were transcribed verbatim. Transcripts were analysed using IPA whereby the focus in interviews was the lived experience of participants and relating this to bio-psycho-social models. The relatively small sample size allowed for deeper exploration and analysis of the data (Biggerstaff and Thompson, 2008). Transcripts were read by the researcher multiple times. In early readings, initial thoughts in response to the text were coded. Preliminary ideas were then coded on the texts into experiential themes. Codes and initial themes were discussed with the research team. Through re-reading and organising into a number of subthemes, the primary researcher then identified themes and clustered themes which were then organised in a table and analysed. The analysis was grounded in the participants own accounts of their experiences and how they made sense of this. In addition to this, the researchers attempted to make sense of the participant’s sense making in order to make meaning from the codes and themes identified.
Positionality
The research team is made up of female psychologists with clinical experience working therapeutically with children and families. The research team were a mixture of parents and non-parents, with varied levels of experience in working with RAP. The primary researcher, who conducted all interviews and coding of themes, had no direct experience in working with RAP, which decreased likelihood of bias as the researcher was able to maintain objectivity. The research team bracketed their personal experiences by ensuring interview questions were open-ended and interviews were guided by participants with the focus sustained on the participant’s lived experience. The Authors declare that there are no conflicts of interest.
Data
The raw dataset is not to be shared as participant consent forms indicated that only excerpts (ie. relevant quotes) from interviews would be used for analysis and used in the write up of the article. Should relevant studies wish to request data, an application can be made to the author which can then undergo ethical committee consideration.
Results
Five main themes were developed from the data, which are illustrated in the model below in Figure 1.
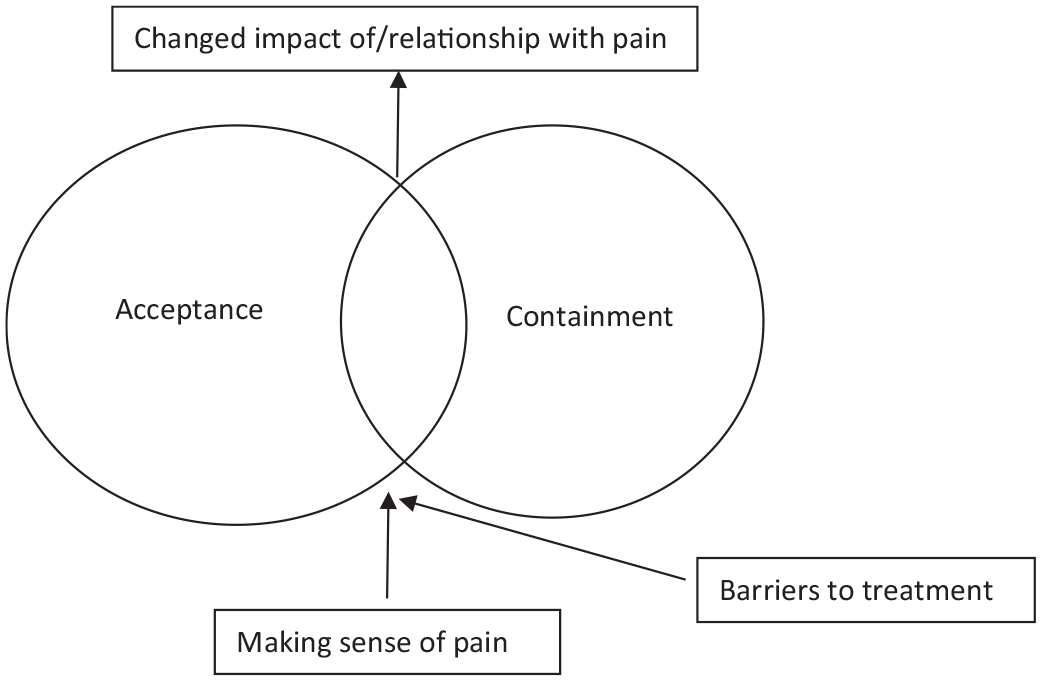
Overarching themes in parental experience of psychological intervention for children’s RAP.
Difficulty in making sense of pain
Levels of impact of pain
Participants described evocatively how RAP impacted multiple aspects of their lives, such as the child’s physical and mental health, the parent’s lives, impact on school and impact on functioning. When describing the impact of pain on the child’s functioning one father said, ‘His energy levels were very low. It wasn’t really feasible for us to send him to school and that obviously caused a lot of difficulty for us, just managing the household’. Other parents discussed ‘It was just taking over her life for a while’ and, ‘it was just difficult to get her up, to get her dressed, to get her to do school work’. This impact exacerbated participants’ sense of helplessness in the face of their child’s pain, and with the uncertainty inherent in living with unexplained pain. These experiences led to futile attempts to make sense of pain, usually by a focus on removing the pain or identifying a physical cause. Participants explained that prior to psychology involvement they struggled to make sense of the pain, and how this caused distress and frustration. Parents explained ‘I didn’t understand it and I didn’t know how to treat it’ denoting feelings of helplessness in how to manage their child’s pain. In describing the experience of pain, one participant said ‘In terms of stomach pain, you physically cannot see outside the outer layer of the stomach and when you don’t know what is going on it is just a completely different story’. Participants reported feeling upset, frustrated and stressed related to difficulties making sense of the pain.
Understanding that the pain is real
Coinciding with difficulties making sense of pain, were assumptions that there was a physical or medical explanation, and a focus on this, ‘when your child has something like a pain. . .initially you just think of medical’. Some participants appeared to equate referral to psychology as meaning the pain was not ‘real’ and struggled initially with this referral option. One parent reflected her thoughts when psychology was first mentioned as ‘We knew that this wasn’t pretending to be in pain. It was a most definite in pain’. Parents appeared to struggle with accepting RAP as a diagnosis. One parent reported, ‘I was heartbroken, like at least if I have a most definite answer, like coeliac, I can go educate myself and then when it was put down to the RAP, I wasn’t satisfied. . .I didn’t feel comfortable, because that didn’t make sense’. Parents reported a lack of understanding around psychological aspects of pain, as stated by one participant, ‘You just wanted the GP to say it was an appendix problem or there’s reflux there. . .because I didn’t understand the psychological part of it’. Parents could also perceive that where no medical explanation could be found that there was a misconception around the existence of pain, ‘They said there was nothing wrong with him, but he is complaining about pain so he is obviously in pain’, highlighting an important distinction between RAP as unexplained pain, rather than this being misconstrued as meaning non-existent. Difficulties around making sense of the pain, and focussing on causes appeared to add to feelings of distress in parents.
A focus on pain explanations or pain elimination
Parents appeared to focus on medical explanations for pain, and on removing or eliminating pain, and equated this to a sense of parental responsibility. One mother explained ‘your instinct is to protect them and I suppose, to get rid of the pain’. Parents appeared to seek containment from health professionals by seeking medical answers. When no underlying cause could be found, this felt very uncontained and added to parental feelings of distress. One mother expressed ‘to come away with no answer – we were still taking a child away who was still in pain and so it didn’t make sense. . .it was physically something she was experiencing so it had to be a physical problem’. Participants reported distress at being unable to get answers or solutions to the pain, and while they felt this parental responsibility, they also felt there was a responsibility on health professionals to find resolution to the pain. Another parent described this as ‘We wanted answers now – like what is wrong with her, fix it now sort of thing’.
Helplessness and uncertainty
The overwhelming response to seeing their child in distress was a feeling of helplessness as parents were unable to alleviate the child’s pain and yet felt responsible for doing so: ‘I felt a little bit heartbroken, that I couldn’t or that I wasn’t able to help him’. Many participants compared their experience as being in a ‘dark tunnel’ with ‘no light at the end’, in relation to feeling helpless around difficulties making sense of the pain. Parents experienced uncertainty about how long their child’s pain would last alongside uncertainty about how to manage it. One parent reflected that ‘it isn’t standard. . .it isn’t like a broken leg and you just go to the hospital and fix it’. Another parent reflected ‘I just was like, is she ever going to get better’. Many parents used the words ‘unknown’ and referred to ‘not knowing what to expect’ discussing how unpredictable RAP appeared to be. Parents appeared to carry worries about what RAP might mean in terms of their child’s long term QOL, and worries that RAP may persist throughout their life. When discussing this, one mother explained ‘When we did find out what it was, it was still scary because she was thinking that she was going to have this for life’. Uncertainty for parents increased their sense of responsibility, made them feel uncontained and uncontaining, and led to significant personal distress, suggesting inter-relationships between these constructs.
Facing barriers to treatment
Numerous barriers were identified in accessing psychological treatment. Participants discussed their distress in facing the lengths of various waiting lists and having to attend numerous appointments prior to psychology. Parents felt there was a lack of awareness of psychological treatments for RAP. It emerged that difficulty accepting a psychological explanation of the pain also acted as a barrier to treatment, as families were reluctant to pursue psychology if they are unaware of how this intervention can be helpful for RAP.
Difficulty accessing treatment
Participants discussed that the process of getting a referral to psychology involved numerous previous appointments with different professionals. This acted as a barrier to accessing treatment as the process felt ‘fraught’ and ‘took a long time’. Parents explained while they understood some things had to be ruled out, that this process was frustrating while their child was still suffering symptoms, adding to both theirs and their child’s distress. One mother explained ‘That [test] came back as negative, and it took months for that to come back. And all the while, the whole time, she was still having the pains, the sickness, the weakness’. Parents struggled when they sought help from medical professionals and were sent home, which added to their experience of distress and feelings of helplessness. Parents explained that their difficulties ‘didn’t seem to get prioritised because there wasn’t an immediate physical issue’. Parents identified what they thought were gaps in their support, such as doctors reporting that pain was psychological but there being no direct follow up for this; ‘well if it is psychological, where is the follow up for that? Why are we being sent home?’ Parents reported feeling dejected and disheartened and feeling like their child’s condition was not being prioritised or taken seriously, and there was no containment for their distress. Some parents appeared frustrated with health system related issues reporting ‘it is just a systemic issue. . .the amount of times that we struggled to get referrals and diagnoses’. This, combined with difficulty in making sense of the pain exacerbated parental distress.
Difficulty accessing timely appointments
Parents also identified length of time to be seen by professionals as a source of frustration, and report that their distress would have been alleviated should they have been referred for psychological intervention at an earlier point, as explained by one participant ‘If we had have seen a psychologist sooner it would have saved us a lot of anxiety and time as well’. Participants felt that there were considerable waits for appointments to be seen by various professionals, which again added to feelings of helplessness. For example, parents explained ‘the waiting time was very long for um – any kind of resolution so you just felt like completely left, like, you know, helpless’ and ‘a letter to say that your appointment is in 15 months time. What am I going to do? Keep him off school for 15 months?’ Parents referenced feeling that there was frequently no sense of urgency to support them and their child and they were ‘shouting into the void’.
Lack of awareness of RAP
As well as length of time to be seen, parents also reported feeling there was a general lack of awareness in society in relation to RAP and children’s psychological health, which also acted as a contributing factor towards barriers in treatment. As discussed by one participant ‘you don’t really think about, oh, there’s psychologists for children. . .it is not something that comes under your radar unless you’re actually in the situation’. Participants suggested that being informed about the possibility of RAP earlier in their journey may have been helpful to prevent catastrophising. Parents felt there should be ‘something that informs people that these things can happen so that you’re not thinking that it is a life threatening or physical piece’. Parents also felt that further clarity on the process would have been useful at the outset to support them to manage their expectations. For example, one participant suggested ‘one thing that I would think would be helpful was if there was a way for parents to understand what the journey is going to be and the expectations of what they need to do’.
Difficulty understanding RAP as a barrier itself
Difficulty making sense of the pain, and difficulty accepting a psychological explanation for the pain was also highlighted as a subtheme in relation to barriers to accessing psychological treatment. Parents reported a lack of understanding in relation to psychological pain. For example, one mother explained, ‘I wanted the GP to say, yeah, there is something actually wrong there, because I didn’t understand the psychological part of it’. Parents reported that a physical explanation to the pain would have been easier to accept and due to having difficulty making sense of the pain, that ‘it took a bit of persuading’ that it was not a physical cause, leaving them feeling sceptical about psychology involvement. This is conveyed when parents reported ‘it was just disheartening. . .and when they said it was RAP and the psychologist was popped in as well’. As there was so much focus on physical investigations and ruling out certain diagnoses, parents then had difficulty accepting psychological explanations of the pain, leading to feeling they were ‘fobbed off’ to psychology when this referral option was presented.
Acceptance
Accept that pain is there
Prior to psychology involvement, the majority of parents were focussed dually upon finding a medical explanation of the pain and upon eliminating the pain. When families were involved with psychology, the focus shifted from removing pain, or finding a cause, to accepting the pain, and learning to manage it. In discussing the process of accepting the pain, parents explained ‘we’ve just come to accept that and that it is part of him. . .but it is how you deal with it then going forward’. Validating the child’s experience of pain, despite no medical explanation, was also key to acceptance, as one parent described ‘you need to accept that the pain is real as far as the child is concerned. . .you need to accept that even if you can’t find an objective measurable meaning for it’.
How parents approach pain
Families learned to treat the pain less like an enemy that they must fight off, and more like a companion that they must learn to co-exist with. This acceptance was the other side of the coin of containment; when pain was accepted it was more easily contained, and more contained pain was more easily accepted. Parents learned that their own approach to pain was important for accepting, and thus containing, the pain. For example, ‘We’ve all accepted that we just have to manage if it comes up and just be calmer in our approach and not to panic’ and ‘he still gets it an odd time, but now we know what to do and we know why he has the pain, and we’re not worrying, ‘oh, is it an ulcer’’. Instead of focussing on a medical explanation, families appeared to make sense of RAP through mind-body connections or understanding anxiety or stress components in the presentation. As explained by participants ‘both he and myself kind of figured out that when he gets stressed, it is his stomach that reacts, he gets the physical symptoms’ and ‘when people sometimes get anxious or stressed, some people might get a headache, other people get a pain in their stomach and that’s normal’. This sits in stark contrast to difficulties making sense of pain prior to psychological intervention which was repeatedly frustrated as physical investigations failed to come up with an answer or diagnosis. As parents began to be able to receive psychological formulations in relation to RAP, this helped them to accept the pain, and in turn, they were better able to focus upon managing the pain.
Managing expectations
Many participants commented that psychology did not promise to remove the pain, but instead focussed on the family using proactive strategies to manage RAP. Parents felt that psychologists ‘weren’t making promises that they couldn’t fulfil’. This sits in contrast to many families prior experiences where there was a focus on identifying cause and removing the pain. Parents explained ‘like they had said, we can’t fix this pain, but we can give him tools to cope and we can put a plan in place to get him back to school’. As there had been such focus on finding an explanation to the pain in the time prior to psychology involvement, this could feel like the experience of failure as they searched for answers that they couldn’t find, and led to increased experiences of feeling disheartened and distress, but when this focus was shifted from removing pain, to pain management, those feelings of failure turn towards success. Parents acknowledged the importance of managing expectations, and psychology appeared supportive with this. As explained by one participant ‘the psychological intervention isn’t going to make the pain go away, what it will do is give you mechanisms to try and cope with it. . .expectation management is important’. Parents began to accept that while psychology could help, that abdominal pain could still arise, and they would have to learn to live with this pain. Therefore, once families learned to accept the pain, the pain became easier to manage and the families felt more contained. And vice versa, once the pain became contained and easier to manage, families were in a better position to accept the pain.
A need to accept the pain?
Interestingly, one participant found there was no improvement following psychological intervention. This parent noted they ‘refused to take that as an answer’ when clinicians gave a diagnosis of RAP. Perhaps a barrier in treatment was not being able to accept RAP as a diagnosis, however, other factors may have been present here. For the other participants, while it was initially difficult to accept a psychological formulation of the pain, this appeared to be a key mechanism of change in reflections following interventions, combined with strategies for living with pain. This can be summarised by the following quote, ‘he is who he is. . .he has his own way of dealing with things, and this pain is going to be something that is going to be there throughout his life on and off, but now he has techniques of what to do’. RAP becomes a companion families learn to live with, rather than an enemy to resist.
Containment
Psychological intervention was experienced as containing on multiple levels; parents felt contained, children felt contained and pain itself was contained through proactive strategies.
Containing parents
Parents reported feeling validated, supported and listened to by the psychologist they were involved with which led to the feelings of containment. Parents reported that there was an ‘understanding of how hard it was for me and for the family and how much stress it had put on us’. Parents appreciated how with psychology involvement, there was validation that it was not parents’ responsibility to remove pain. As one parent explained ‘the psychologist said to me was that it wasn’t up to me to fix it and that there was a name for it and that was a massive relief for me to know that I didn’t have to be able to fix this for him’. This not only explains how much responsibility parents were undertaking in trying to remove something outside of their control, but highlights how their experience of psychology was containing as this responsibility was shifted. Parents valued the proactive and collaborative nature of the therapeutic work, as described by one participant ‘one aspect that was great about that it was them who put the plan in place. . .it would have been difficult for us to do that without the support of the psychologist’, which appeared to help with the parental experience of feeling contained as the psychologist took responsibility for helping their child to manage RAP.
Psycho-education of the role of parent’s worry or parental catastrophising was highlighted as important for parents to make sense of the pain. One mother described ‘bouncing off each other thinking about ‘yeah, when you worry I worry’, so it was a bit like she would be worried because I would be worried, and I would be worried because she was sick’. Parents reported feeling contained through ‘reassurance that [psychologist] knows what she is talking about, and she has seen other children with similar experiences’. By changing how parents made sense of RAP, this helped shift their experience from uncontained to contained.
Containing children
Parents also experienced feelings of containment when they could see that their child was responding well to psychological intervention. Parents referenced the sessions going well, ‘which had a calming effect in terms of saying well, look, it is something that she is comfortable with and it is working for her’, and their child’s relationship with the psychologist as aspects of what was helpful in psychological intervention. Parents were able to reach containment through their child taking control of RAP and managing the impact the pain had on their lives and how psychology supported this development. As one parent explained how the psychologist ‘gave [her] the words for it. . .that you have to boss the pain back and you’re telling the pain now that you are in control and the pain won’t tell you what to do’.
Containing pain
When parents felt contained, they were then able to change their approach to the pain. Parents discussed saying ‘how can I help you to use your tools’, as opposed to trying to make the pain go away. Taking a proactive approach to the pain and managing this through strategies also supported parents, and children, to feel contained. With feeling contained, parents were more able to accept the presence of pain. Parents noted how the focus changed to ‘coping techniques that he could try himself’, where the focus shifts from pain elimination to pain management. Participants reflected upon this change in how pain was being managed using ‘something concrete we can work with rather than ‘it is a pain, where is this coming from?’’ Parents reflected on how their goals changed from removing pain, to managing the impact the pain had on their lives. One parent explained ‘the goal of this exercise, is to help you go about the normal functions of everyday life’ and referred to psychology as helpful for ‘pragmatic, breaking down the problem’ as an important mechanism for making RAP easier to live with: ‘instead of thinking, my God, my kid has got this massive existential thing he’s going to have to deal with for the next 50 years of his life or whatever, instead it is like, okay, what do we need to do to get him to school by 9 o’clock tomorrow. It is a much easier thing to cope with’.
Changed impact of/relationship with pain
Managing impacts of pain
With successful psychological intervention came a changed relationship with their child’s pain. Parents reported the pain going from ‘unpredictable’ to ‘predictable’. Alongside this changed relationship was the changed impact of the pain on their children’s lives such as ‘it is not really stopping her in her tracks anymore’. Parents also spoke of the impact of the decreased pain on their own lives, stating this as ‘less stress in the house and there was less worry’. Some parents discussed that while the impact has decreased, the pain still has somewhat of an impact, but the relationship has changed, as parents and their children no longer catastrophise the pain. For example, ‘while you know it will pass it is just like a cloud over the house’. Thereby, the pain goes from uncontained to contained and manageable.
Improving relationships with children
Parents discussed changes in their relationships with their children as a result of the intervention, and how this opened up different ways to communicate with their child, which supported management of RAP. Parents described ‘just checking in with each other and just checking in with how he is feeling about different things’ and ‘talking more to my daughter one-to-one and trying to understand more about her’. Thereby, while the impact and relationship with pain is changed, the relationship with their child was also positively impacted.
Improving relationship with pain
Parents reflected upon their changed relationship with the pain, which can be seen in terms of the process of accepting the pain. For example, one parent described, ‘those types of episodes, we know that after they start they will finish, you know, and she can get back to normal again’, highlighting acceptance of the pain and knowing they can manage it. This sits in huge contrast to before treatment where parents reported panicking, distress and frustration. There appeared to be a shift in responsibility in how the pain was managed. Parents had discussed feeling sense of responsibility to alleviate their child’s pain, but in discussing the impact the pain currently had on their lives parents reported ‘I can’t get rid of the pain. . .so now the tools are back on her’. Use of proactive strategies in helping children to manage supports parents to feel contained and accept the pain, and have a changed relationship to the pain.
Changing reactions to child’s pain
Through a changed approach to the pain, there was a changed impact of RAP and changed relationship with the pain. Parents reflected on the changes to their child reactions prior to intervention and after intervention, such as ‘before it was just ‘I have pains in my belly’ and now it is ‘I think I’m just worried’’. Parents also reflected on changes in their own reactions, such as ‘the pain was the focus, like ‘did you eat something? Did you hurt something?’ and now different questions are asked’. Parents acknowledged the role of their own reactions, how this can impact their child’s reaction and how this changed after psychological intervention. Parents reflected ‘I realised how much I was panicking and how that can’t be good either. Like I’m worrying, and then she is panicking because I am panicking’ and how they were more mindful of their own reactions. Taking a proactive strategy using tools to manage the pain appeared important in changing the impact of the pain. Therefore, a changed approach to the pain is important in order to change the impact of the pain and the relationship with the pain, and the processes of acceptance and containment are crucial in order to achieve this.
Discussion
The aim in this study was to increase understanding of parental experiences of RAP and begin to ascertain active components in this intervention. What can be seen from the data is that acceptance and containment were key mechanisms of change that allowed for a changed relationship with pain and a changed impact of pain on family life. These themes sat in huge contrast from parental experiences prior to psychological intervention where they found it difficult to make sense of the pain, and faced numerous barriers to treatment.
Three of the five overarching themes reinforce findings from earlier studies on RAP. Previous research has discussed how parents can struggle with accepting a primarily psychological explanation to their child’s pain (Masia-Warner et al., 2009). This was clearly evident in this study as parents struggled to make sense of their child’s pain and appeared focussed towards finding medical explanations so that the pain could be eliminated. When a cause could not be found, this increased uncertainty and heightened parental stress and anxiety. As parental stress and anxiety has been highlighted as a potential precipitator to RAP, it appears that difficulty making sense of RAP can perpetuate the occurrence of pain, and as discussed, a focus on finding medical explanations can lead to barriers in seeking and accessing psychological intervention (Newton et al., 2019). Limited access and long waits for treatment were further highlighted as barriers to psychological interventions again reinforcing previous research around difficulties accessing psychological interventions in this population, and again reinforcing how long waits for treatment can heighten distress, and in turn increase the presence of RAP (Robins et al., 2005),
One of the aims of the paper was to increase understanding of how psychological intervention supports management of RAP. There is a lack of previous research in this area, however Nieto et al. (2019) found that psychological intervention leads to reduced pain severity and improved QOL, and use of more adaptive coping strategies. This can be compared to the findings of this research whereby participants reported improvements in school attendance, increased ADLs, and decreased pain severity or pain occurrence, which in turn lead to a changed impact of the pain, and changed relationship with the pain. (Nieto et al., 2019).
In addition to these well-established findings, the current study offers an explanation for the helpfulness of psychological interventions for childhood RAP. The themes of acceptance and containment are new findings in this area of research. In relation to research of both child and adult chronic pain, there is growing evidence for the practice of acceptance and acceptance-based interventions (Coakley and Wihak, 2017). Given this, perhaps acceptance-based interventions should be considered as a potential option for treating RAP. Further research into acceptance-based interventions and childhood RAP would increase our understanding in the role of acceptance. Containment is a core concept in psychology, yet there is a lack of research into the role of containment in psychological interventions for childhood RAP. Given how this study highlighted containment happening on multiple levels, further research into childhood RAP and containment would increase understanding of this construct as both containing the pain and containing parents and children were evident as key mechanisms of change. Further research using IPA approach around containment in psychological interventions for pain would be beneficial to extend this research.
A strength of this study is that it was guided by what participants viewed as supportive. While it is useful to look at treatment protocols and outcomes, it is difficult to compare this to how families themselves experience the intervention. It is imperative that the voices of service users are heard when developing interventions. Through use of IPA, the researchers made sense of how participants make sense of their experiences, giving an in depth insight into parents’ understanding of RAP and psychological interventions. The researcher was able to use their knowledge of literature and psychological theory and participants’ experiences and combine these to give a deeper understanding of parental experiences. Thus, this study provides a unique insight into the experience of families in this context, and use of IPA in this study allowed for a combination of idiographic and interpretative components to understand parental experience. Participants were given the opportunity to speak about their experiences both good and bad, which allows for services to be developed based on the honest experiences of individuals who use services. This study was also the first study to directly focus on parental experiences for psychological intervention for RAP, and as outlined, this is a key area to look at when developing interventions given the important role of parents in the presentation of RAP and psychological interventions for children.
Limitations of this study include that participants were recruited from one particular hospital in a secondary care setting. However, given that Rome Criteria indicates RAP as a diagnosis whereby physical health investigations must precede psychological investigations in order to ensure no underlying medical explanation for the pain, it is unlikely that these participants would be currently accessible in other healthcare settings. This study also used a small sample with participants all recruited from urban and suburban areas of Ireland. In order to increase generalisability, it would be worthwhile to complete further research in other areas, perhaps with a larger sample. However, many of the overarching themes appear to fit with previous research, so it would be expected that participants may report similar experiences. While this study looked specifically at parental experiences, young people’s experience remains unclear. Another avenue of future research should look specifically at child and adolescent experience, to support our understanding of mechanisms of change in psychological interventions for RAP.
In relation to practical implications, interventions could be developed that focus on supporting parents to accept that their child has RAP, yet with that acceptance, pain can be contained and managed through proactive and behavioural strategies, such as relaxation strategies, distraction techniques or exposure-based tasks. Further research into acceptance-based interventions and childhood RAP would also be beneficial. Practitioners should also be aware of the role of containment, and how it is imperative for families to feel contained throughout therapeutic intervention. Additionally, this research indicated how families experience distress related to difficulties making sense of the pain, including increased focus on possible medical explanations in order to attempt to eliminate the pain, which can in turn act as a barrier to pain management. Families also faced barriers to treatment including long waiting times for appointments, and as these participants had described, psychology was only explored after many medical investigations. The family experience of distress related to RAP could be alleviated at a primary care level, if RAP and possible psychological explanations of pain are mentioned at earlier stages in care, to minimise the impact of catastrophising, increase family understanding of RAP and improve family containment. Referrals could be made to psychology at an earlier stage in treatment to support families with their experience of distress around pain, or perhaps joined initial assessments with Paediatricians and Psychologists, which would address barriers to treatment. In relation to the themes of acceptance and containment, this research has wider implications than psychological intervention. Given that families indicated acceptance and containment as active components, these findings are useful for other healthcare professionals to consider when working with families experiencing RAP.
Conclusion
As research indicates how parents play an important role when it comes to their children’s experience of pain, looking at the experience of parents in their involvement in interventions can give us an insight to how they experience pain, the impact this has on their lives and the mechanisms of change that lead to improved outcomes. Acceptance and containment were overlapping mechanisms of change in parents’ experiences of psychological intervention. As a result of acceptance and containment, there were positive outcomes in relation to a changed relationship with pain, which allowed for a changed impact of pain on families. These findings support understanding of how psychological intervention for RAP supports parents and allows us to further research important mechanisms of change in interventions, which should target acceptance and containment of RAP.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.