
Abstract
This study examined the association of organisational justice with pain among employees of a large organisation. Employees (n = 1829) completed measures of pain, fair pay, organisational justice, job satisfaction and stress. Logistic regression analyses found that organisational justice was unrelated to pain among women, but men with higher perceptions of fair pay were more likely to report chronic pain as were men with lower perceptions of distributive justice. This is the first study indicating that fair pay and distributive justice are both unique predictors of chronic pain in men. The findings have implications for supporting employees with chronic pain.
Introduction
Pain is a major public health issue that is a burden on health and social care systems across the world. Chronic primary pain, defined as pain in at least one anatomical region that persists or recurs for longer than 3 months (Nicholas et al., 2019) affects up to half of the UK population (Fayaz et al., 2016), a pattern that is mimicked globally. Moderate or severe chronic pain can have a significant impact on an individual’s daily activities, including their working lives (Breivik et al., 2013). Chronic pain is a significant burden within the workplace, due to its effect on sickness absence, employment status and productivity (Patel et al., 2012; Philips, 2009).
While some people with chronic pain cannot work, many employees remain at work with pain (Pain Alliance Europe, 2018), although they may require workplace accommodations and have poorer wellbeing and less functional capacity to complete tasks than employees without pain (Rodrigues et al., 2017; Soer et al., 2012). Pain can be affected not only by the physical work environment but also by other, psychosocial work factors. This is consistent with the biopsychosocial formulation of pain which suggests that psychosocial factors can contribute to pain and suffering (Gatchel et al., 2007). Psychosocial factors are a central part of the work experience. They involve the workplace characteristics individuals are exposed to at work as well as employee beliefs about the workplace and are known risk factors for poor health and sickness absence (White et al., 2013). Much research has found numerous psychosocial work factors and work attitudes to be associated with chronic pain, including work demands, job control and social support (Buruck et al., 2019; Lang et al., 2012).
One specific work attitude that has implication for health and wellbeing and is a determinant of other workplace factors, is organisational justice (Van Dijke and De Cremer, 2016). Organisational justice is characterised by perceived fairness in relation to different work domains, including interpersonal treatment (e.g. dignity, respect), the distribution of outputs such as rewards and benefits and procedures for making decisions about the allocation of outputs. These types of organisational justice have had differential effects on the physical and mental health of employees (Ndjaboue et al., 2012; Robbins et al., 2012) with repercussions for sickness absence (Tenhiälä et al., 2013). Explanations for this association consider organisational justice as a stressor that adversely affects health through psychophysiological and/or behavioural mechanisms (Kompier and Taris, 2011; Robbins et al., 2012), although alternative plausible explanations suggest health status can affect perceptions of injustice because they triggers negative work attitudes and/or behaviour that elicits a change in the work environment (Eib et al., 2018).
Despite evidence of a clear association between organisational justice and health, relatively little is known about the role of organisational justice in the experience of pain. A small number of studies have reported a negative association between perceived organisational justice and pain (Freimann et al., 2016; Heponiemi et al., 2013; Herr et al., 2015; Manville et al., 2016; Pekkarinen et al., 2013; Saastamoinen et al., 2009), but beyond this virtually nothing is known about injustice in the context of pain and work, particularly which type or types of organisational justice are most relevant to the pain experience.
The aim of the present study was to examine the association of procedural, interpersonal and distributive justice with acute and chronic pain among male and female employees, compared to employees without pain. Fair pay is a component of distributive justice but was distinguished from this as distributive justice encompasses broader outcomes such as promotion, recognition and access to physical facilities, and we sought to examine the association of fair pay as a unique component of the workplace experience. Since organisational justice is part of a complex psychosocial work environment with direct implications for work stress (Matta et al., 2017) and job satisfaction (Herr et al., 2020) that are both risk factors for pain (Ariens et al., 2001; Bonzini et al., 2015), we included these variables to investigate the associations between each type of organisational justice and acute and chronic pain independently of these other important aspects of the psychosocial work environment.
Materials and methods
Study setting and participants
This study is part of a larger employee wellbeing study examining the health and pain status of employees of a large public sector organisation in Scotland. Ethical approval for the study was granted by the Department of Psychology, Social Work and Allied Health Sciences at Glasgow Caledonian University. Employees were emailed a web link to the study questionnaire by their employer through their work email address and hard copies were distributed within the organisation. Written or online consent was obtained prior to data collection. The total number of respondents was 1829 (approximate 10% response rate).
Self-report measures
Pain Consistent with previous work (Elliot et al., 2014) pain was measured by asking participants whether they were currently troubled by pain or discomfort, either all the time, or on and off (Yes/No). Those who responded ‘Yes’ were asked whether they had experienced pain or discomfort for more than 3 months (Yes/No). Those who reported currently experiencing pain but not for 3 months or longer were categorised as having acute pain, while those who reported experiencing pain for at least three months were categorised as having chronic pain (International Association for the Study of Pain, 1986). All others were categorised as having no pain.
Organisational justice was measured using single item measures based on a modified version of items developed previously (Jordan and Turner, 2008). Distributive justice was measured with: ‘I feel the rewards I receive from working for my employer are fair. Pay, recognition and physical facilities are examples of rewards’. Procedural justice was measured with: ‘I feel the formal policies and procedures used by my employer to make decisions are fair’. Interpersonal justice was measured with: ‘In all aspects of my work environment, I feel that my primary supervisor treats me in a fair manner’. Fair pay was measured with: ‘I feel the pay I receive from working for my employer is fair’. Each item was measured on a 1–7 scale, from 1 (Strongly disagree) to 7 (Strongly agree). The reliability and concurrent validity of the scales has been established (Jordan and Turner, 2008).
Job satisfaction was measured using the four-item job satisfaction scale from the Copenhagen Psychosocial Questionnaire (COPSOQ) (version 2), a measure of the psychosocial work environment (Pejtersen et al., 2010). The scale measures satisfaction with work prospects, physical working conditions, the way one’s abilities are used and general job satisfaction. Each item was scored on a scale with the response options: ‘Very unsatisfied’, ‘Unsatisfied’, ‘Satisfied’ and ‘Very satisfied’. The optional fifth option, ‘Not relevant’ was excluded. Each item was scored on a 0–100 scale (i.e. 100, 66.7, 33.3 and 0, for a four-item category scale). If fewer than half of the scale questions were answered, then the scale score was set to missing. A total score was created as an average of the individual scores. A higher score indicated greater job satisfaction. The COPSOQ has been widely used and the scales have been found to be reliable and valid (Bjorner and Pejtersen, 2010; Thorsen and Bjorner, 2010). Within the present study, the internal consistency of the scale was 0.80 (Cronbach’s Alpha).
Job stress was measured using the four-item job stress scale from the COPSOQ (Version 2) (Pejtersen et al., 2010). The scale items measure stress in the past 4 weeks, in relation to the frequency of having a problem relaxing, irritability, tension and general stress. Each question was scored on a scale with the response options: ‘All the time’, ‘A large part of the time’, ‘Part of the time’, ‘A small part of the time’ and ‘Not at all’. Each item was scored on a 0–100 scale (i.e. 100, 75, 50, 25, 0 for a five-item response category scale). If fewer than half of the questions in the scale were answered, then the scale score was set to missing. A total score was created as an average of the individual scores. A higher score indicated greater stress. Within the present study, the internal consistency of the scale was 0.92 (Cronbach’s Alpha).
Data sharing statement
The statistical data file corresponding to our analysis is available from the first author on request.
Data analysis
Descriptive statistics for the sample were reported. Bivariate correlations to test for the presence of multicollinearity between organisational justice, psychological stress and job satisfaction variables produced correlations ranging in value from ‒0.19 to 0.69. The strongest correlation was between fair pay and distributive justice. Colquitt and Shaw (2005) indicate that correlations between organisational justice variables below 0.70 can be tolerated. Therefore, these variables were not aggregated.
Logistic regression analyses were conducted to examine the associations between these variables and each of three groups (no pain, acute pain, chronic pain), with ‘no pain’ as the reference group in the analysis. Logistic regression models relate the log odds of a binary outcome measure to explanatory variables, which may be categorical or continuous. In our analyses, 0 indicates the ‘no pain’ reference category while 1 indicates either acute or chronic pain. Logistic regression coefficients give the change in the log odds or percentage change in the odds for a successful outcome (i.e. that the dependent variable equals 1) associated with a unit change in an independent variable. Job-related, demographic and health-related variables were controlled for in the analyses. These variables included UK Standard Occupational Classifications (Professional, Associate Professional or Technical staff, Administrative and Secretarial staff), gross weekly earnings, employment status (full-time, part-time), age (categories 35–44, 45+, compared to 16–34 category), marital status (Cohabiting partner/No current partner), highest educational qualification (post-graduate, degree, Further Education or Highers, compared to low qualifications), self-reported general health (0–100, higher scores indicate better health) (Bowling, 2005), whether currently a cigarette smoker (Yes/No), the number of days per month a minimum of 30 minutes exercise has been completed (1–11 days, 12–19 days, 20+ days) (Milton et al., 2011) and total frequency and amount of alcohol consumed (scored 0–12; 5+ indicates higher risk drinking). Alcohol consumption was modelled in quadratic form (with a squared term) to reflect the likely non-linear relationship between chronic pain and alcohol consumption found within the literature (Skillgate et al., 2009). The organisational justice, job satisfaction and psychological stress variables were adjusted for confounders and simultaneously for each other (fully adjusted model). The results of the logistic regression are presented as odds ratios (OR) with their 95% confidence intervals (CI). Pseudo R2 values were included to provide an approximation of goodness of fit for the regression models. The tables report the regression models for pain for all the sample, and then separately for males and females.
Results
Descriptive statistics
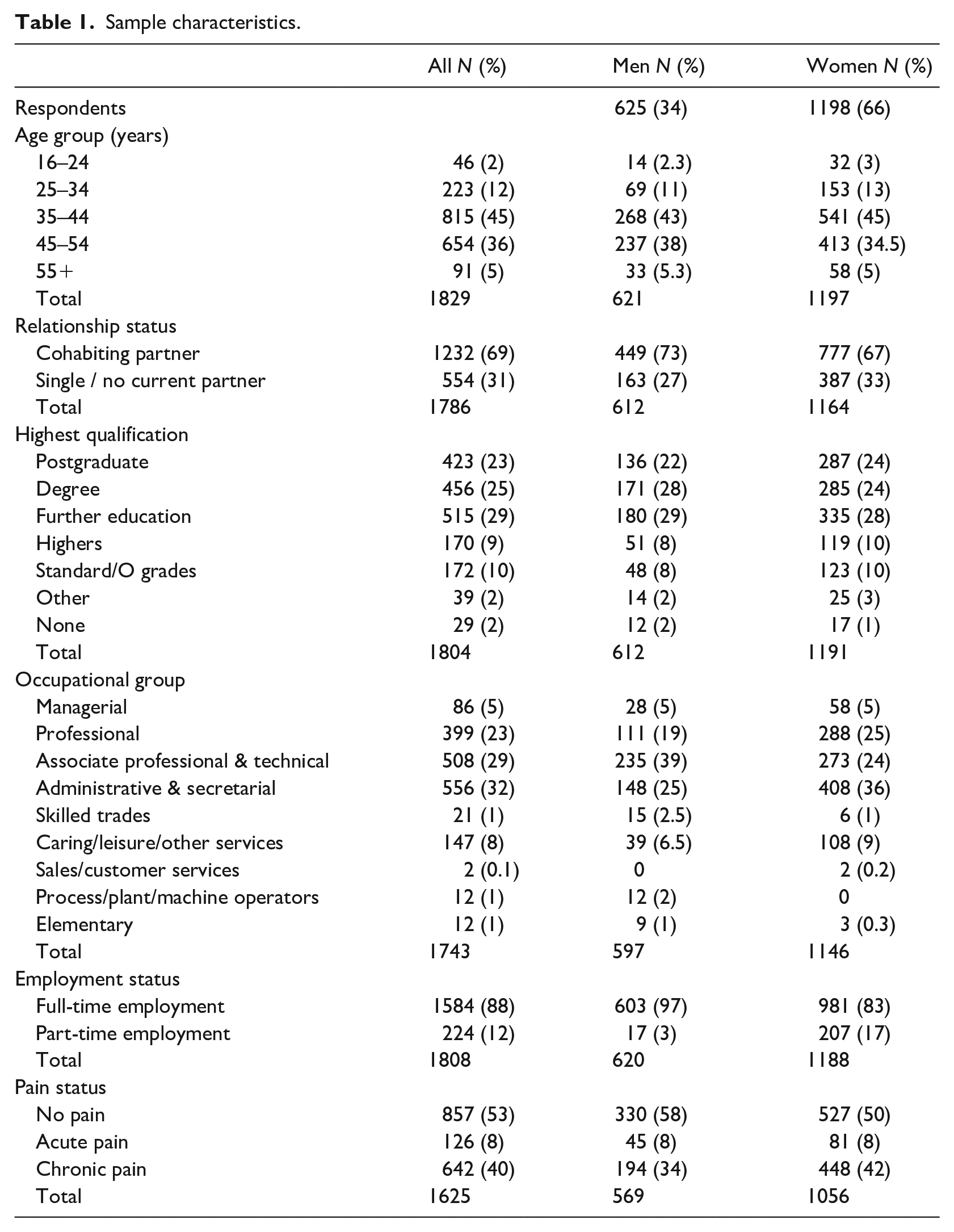
Table 1 shows the descriptive statistics of the sample. Most of the sample was female (66%), in the age range 35–44 (45%) and either married or living with a partner (69%). Most employees had Further Education (29%) or Degree/Postgraduate qualifications (48%) and were employed full-time (88%), mainly in Administrative/Secretarial (32%), Associate Professional and Technical (29%) and Professional (23%) occupations. Of the 48% of employees reporting pain, most experienced chronic pain (40%), 70% of whom were female. Of those reporting chronic pain, 92% had at least one musculoskeletal pain condition, commonly back pain, joint pain and/or neck pain, or a musculoskeletal condition accompanied by another type of pain condition (headache, toothache, abdominal pain). The remaining 8% of those with chronic pain reported one or more of these other pain conditions.
Sample characteristics.
Logistic regression modelling for males and females
The acute pain regression model identified no significant predictors of acute pain among men and women and is not reported. The model for chronic pain was significant, for both sexes (Table 2). Women were 64% more likely to report chronic pain than men (inverted OR: 0.60; 95% confidence interval: 0.44–0.81). Among men, age, highest educational qualification, general health, fair pay and distributive justice were associated with chronic pain. Men with higher perceptions of fair pay (compared to lower perceptions of fair pay) were 25% more likely to report chronic pain (OR: 1.25; 95% confidence interval: 1.03–1.53). Men with higher perceptions of distributive justice were less likely to report chronic pain than those with lower perceptions of distributive justice (OR: 0.76; 95% confidence interval: 0.59–0.98). Compared to younger male employees (16–34 years), males aged 35–44 were almost three times as likely to report chronic pain (OR: 3.00; 95% confidence interval: 1.25–7.21), while those over 45 years of age were almost four times as likely to report chronic pain (OR: 3.89; 95% confidence interval: 1.61–9.41). Male employees with a postgraduate qualification (OR: 3.06; 95% confidence interval: 1.24–7.57), a degree (OR: 2.54; 95% confidence interval: 1.09–5.91) or a further education qualification (OR: 3.58; 95% confidence interval: 1.57–8.16) were up to three times as likely to report chronic pain than employees with only school level or no qualifications. In terms of self-reported general health, for every additional one-unit increase in a man’s health, he was 3% less likely to report chronic pain than those who reported poorer health (OR: 0.97; 95% confidence interval: 0.96–0.98).
Logistic regression analysis for chronic pain.
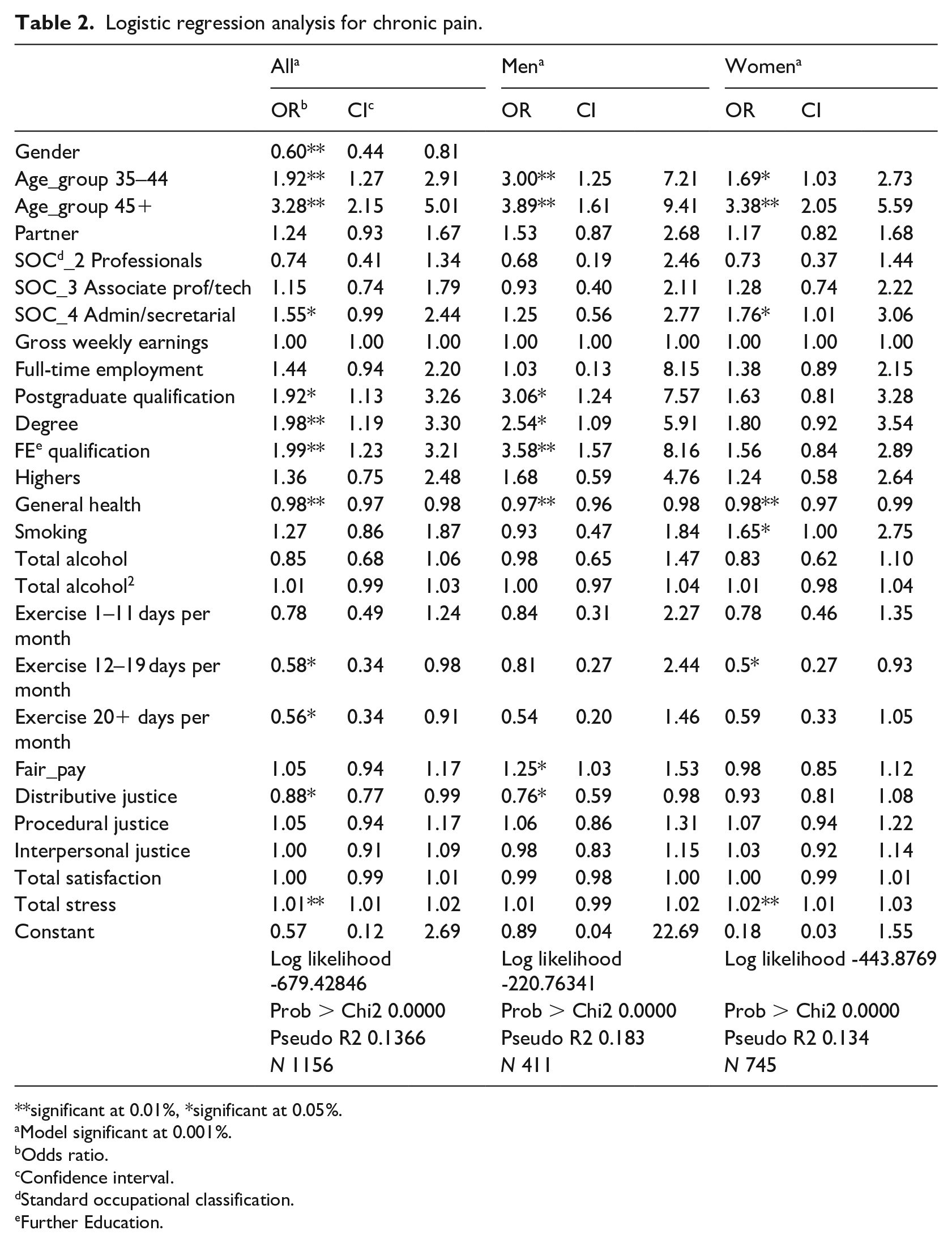
**significant at 0.01%, *significant at 0.05%.
Model significant at 0.001%.
Odds ratio.
Confidence interval.
Standard occupational classification.
Further Education.
For women, age, administrative/secretarial occupation, general health, smoking, exercise and stress were associated with chronic pain but no organisational justice variables were significant predictors. Like the men, older women, particularly those aged 45 years and over, were over three times as likely to report chronic pain compared to their younger female counterparts (OR: 3.38; 95% confidence interval: 2.05–5.59) (Table 2). Female employees in administrative/secretarial occupations were 76% more likely to report experiencing chronic pain than those in other occupations (OR: 1.76; 95% confidence interval: 1.01–3.06). In terms of general health status, like men, women who reported better health were less likely to report chronic pain than those who reported poorer health (OR: 0.98; 95% confidence interval: 0.97–0.99), and women who smoked were 65% more likely to report chronic pain compared to female non-smokers. (OR: 1.65, 95% confidence interval: 1.00–2.75). Additionally, for each one-unit increase in a woman’s total stress score, they were 2% more likely to report chronic pain (OR: 1.02; 95% confidence interval: 1.01–1.03). Finally, women who exercised for between 12 and 19 days per month were only half as likely to report chronic pain compared to those who reported less exercise (OR: 0.5; 95% confidence interval: 0.27–0.93).
Discussion
This study examined the association of organisational justice with acute and chronic pain among male and female employees. Work, health and demographic variables were controlled for in the analysis, and job satisfaction and psychological stress were included.
Among men only, perceptions of fair pay and distributive justice were unique predictors of chronic pain. Specifically, men with a higher perception of fair pay compared to a lower perception were more likely to report chronic pain, as were men who reported a low level of distributive justice. We are uncertain about the meaning of the positive interaction between fair pay and pain among men. It is possible this is a chance finding but we suggest the finding aligns with research showing that pay equity is an important concern of male employees, as a symbol of how their work is evaluated and a measure of their status at work (Khoreva and Tenhiala, 2016; Tata, 2000). Although not found in this study, research indicates women may have other priorities linked to procedural justice to achieve desired outcomes through fair decision-making processes at work (Khoreva and Tenhiala, 2016). This interpretation, however, remains speculative until further research is conducted examining the implications of perceptions of fair pay among employees with chronic pain.
Whilst satisfied that they were paid fairly, the findings indicated that male employees with chronic pain had lower perceptions of distributive justice in relation to rewards such as recognition, promotion or benefits. It is possible that, while some outcomes may be set, in terms of pay, employees with chronic pain perceive that other, more flexible outcomes and opportunities are withheld from them or are out of their reach due to their pain condition, such as the opportunity for promotion (Beatty, 2012). This interpretation is consistent with research showing that individuals with chronic illness can feel under threat of being stigmatised at work (McGonagle and Barnes-Farrell, 2013), in relation to productivity and the ability to maintain regular working hours (Beatty and Joffe, 2006). It is also possible that, for the employee with chronic pain, weaker perceptions of distributive justice reflect issues associated with work accommodations such as flexible working hours or adjustment to type of work or working hours that are needed to manage pain at work (Grant et al., 2019). However, further investigation is needed to understand the nature of the perceptions of distributive justice in this group.
The finding with respect to distributive justice supports that of previous research (Freimann et al., 2016; Pekkarinen et al., 2013), including those of Saastamoinen et al. (2009) who found organisational justice was associated with chronic pain among male but not female employees. Although organisational justice was unrelated to chronic pain among females, it is possible that men and women experience justice-related issues differently from each other. For example, research suggests that organisational justice is associated with different work-related outcomes for male and female employees in general (Jepsen and Rodwell, 2010; Ramamoorthy and Flood, 2004). This is worthy of future investigation among employees with pain.
In other findings, consistent with previous research, women, older employees and those with poorer health were more likely to report chronic pain among men and women (Fillingim, 2017; Saastamoinen et al., 2006). Among women only, working in administrative or clerical occupations, higher self-reported stress and smoking behaviour were predictors of self-reported chronic pain, while moderate exercise (exercising for between 12 and 19 days per month) was associated with less likelihood of reporting chronic pain. These findings support the patterning of previous research (Ditre et al., 2011; Landmark et al., 2011; Widanarko et al., 2012). However, adding to the mixed results of previous work (McNamara et al., 2017) a higher rather than a lower level of education was associated with an increased likelihood of reporting chronic pain among male employees.
The results contribute to research on psychosocial and behavioural factors associated with pain among employees, particularly with respect to the growing body of research indicating the importance of organisational justice to employees with chronic pain. These perceptions of work have potential implications for clinical decision -makers who recognise work attitudes as potential ‘blue flags’ to be addressed as part of treatment to support the employee with chronic pain (Shaw et al., 2009). There are also implications for the employer, in relation to their processes for supporting the employee with chronic pain to offset or minimise the potential negative repercussions of weak organisational justice beliefs in relation to, for example, job satisfaction, commitment and work performance (Van Dijke and De Cremer, 2016). Evidence suggests training employers in organisational justice techniques can improve perceptions of fairness and occupational functioning among employees (Nakamura et al., 2016).
A strength of the study is that we sought to recruit all employees, regardless of pain status, thus reducing the potential for bias had we actively recruited only employees with chronic pain. A study limitation is that causality cannot be established from the data. Future research should examine the bi-directional relationship between organisational justice and chronic pain to determine the direction of intervention work. Additionally, caution is needed with the generalisation of the findings, as the sample were predominantly middle-aged, co-habiting, educated females from a range of professions, among whom musculoskeletal pain was more commonly reported. Although there was an approximate 10% response rate, there was a large variance in all key phenomena that enabled these analyses to be performed with good internal validity for this sample. A third limitation is that, while single item measures can provide useful information in the context of organisational research (Fisher et al., 2016), multiple item measures tend to have stronger psychometric properties and should be considered in future research.
Notwithstanding these limitations, this is the first study to find that fair pay and distributive justice are both unique predictors of chronic pain. Future research is needed to investigate these findings further and consider gender differences in justice-related reasoning within the workplace, and the implications of justice-related reasoning for the employee with pain.
Footnotes
Acknowledgements
The authors thank Dr Richard Graveling for assistance in planning the research.
Author’s Note
Manuscript note for end of paper: Dr Anne Gasteen is now based in the Division of Economics, University of Stirling.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scottish Economic Society and the Glasgow School for Business and Society, Glasgow Caledonian University.