
Abstract
Individuals living with chronic physical health conditions are more likely to be out-of-work than other groups. Often framed as a ‘response’ to these statistics, many countries have introduced policy instruments for promoting the employment of individuals with chronic conditions. This qualitative study sought to explore the impact of welfare reforms on UK individuals. Employing a phenomenological approach, semi-structured interviews were conducted with five participants living with chronic conditions. Three themes were generated using Interpretative Phenomenological Analysis: ‘intersubjective sense making of the condition’; ‘battles for control’ and ‘the fluidity and strengthening of identity’. Implications for further, holistic, policy reform are explored.
Keywords
Introduction
The work capability assessment (WCA)
Within the past century, the world has witnessed dramatic epidemiological change. The largest challenges facing healthcare systems in the 21st century now include the increasing prevalence of chronic illness (Murray, 2012). As of 2012, 15 million people within England (approximately 30% of the population) had one or more long-term chronic physical conditions (Naylor et al., 2012).
These growing numbers have impacted upon welfare systems: many countries have introduced a policy instrument for assessing working capability and promoting the employment of individuals with chronic illness (Gjersø, 2016). Within the UK, the WCA was introduced in 2007, used to determine an individual’s eligibility for the Employment and Support Allowance (ESA) benefit.
The WCA involves an assessment of the individual’s physical and mental limitations against 17 specific activities, known as descriptors (Gjersø, 2016). Each descriptor carries a number of points, with the sum total determining whether ESA should be awarded. ESA is a two-tier system, with potential claimants being assigned to one of two groups. The Work Related Activity Group (WRAG) is for those who are expected to engage in paid work, with payment of the benefit dependent upon attendance of mandatory employment training schemes. Those placed with the Support Group (SG) receive a higher level of benefit and are not expected to engage in work-related activity. As of February 2020, there are currently 1.9 million ESA claimants (DWP, 2020). ESA is now one of the six components that form Universal Credit (Dwyer & Wright, 2014).
Claimants initially complete a questionnaire before a ‘medical test’, conducted by an outsourced private healthcare company. Both the questionnaire and completed medical report are used by non-medically trained civil servants within the Department of Work and Pensions (DWP) to make a decision on ESA eligibility. The decision is time-limited with claimants being reassessed after a period of years, determined within the report. When comparing the UK’s WCA process with the assessment procedures of Norway, it becomes possible to see fundamental differences in intended outcomes; informed by ideological conceptualisations of welfare. In essence, the UK WCA aims to decrease the inflow into the benefit system whilst the Norwegian approach seeks to increase the outflow away from welfare (Gjersø, 2016).
The WCA has been subject to increasing levels of public and academic criticism. Using aggregate routine population and survey data for 149 local authorities within England, Barr et al. (2016) found that for each additional 10,000 people reassessed an association exists with 6 additional suicides, 2700 cases of reported mental health issues and the prescribing of an additional 7020 anti-depressant items; independent of baseline measures in the area, and following (rather than preceding) the process of reassessment. Data from the Adult Psychiatric Morbidity Survey (McManus et al., 2016) suggest that two thirds (66.4%) of people in receipt of ESA had thought about taking their life, with 43.2% having made a suicide attempt. However, these studies cannot support claims of a direct casualty between the WCA and significant mental health problems.
Utilising thematic analysis following interviews with 25 long-term sickness benefits recipients, Garthwaite (2014) saw themes of fear and trepidation over ongoing welfare reforms; with media coverage of benefit ‘scroungers’ leading to greater stigma and struggles with personal identifications of ‘disability’ for those within the welfare system. At a public level, the dissatisfaction with the WCA is especially related to the medical test. The test, outsourced to a private healthcare company (ATOS between the years 2008 and 2014 and Maximus from 2014 onwards), is perceived as too technically driven with little human interaction, and claimants reporting feelings of a lack of respect and empathetic understanding (Harrington, 2010). Both the ‘scrounger’ discourse and the logistical over-reliance on technology have the effect of dehumanising the categorisation of ‘work capability’.
The controversy around reassessments have been addressed by the UK’s governing Conservative Party. Reforms initially proposed at the 2016 Conservative Party conference, positioned as a ‘common sense’ approach to reassessment, suggested that ESA allowance will continue automatically for those living with ‘lifelong, severe health conditions’ (Grierson, 2016). Table 1 details the criteria that must be met to ‘avoid’ further reassessments:
Criteria for ‘switching off’ ESA reassessments (Kennedy & Gheera, 2017).
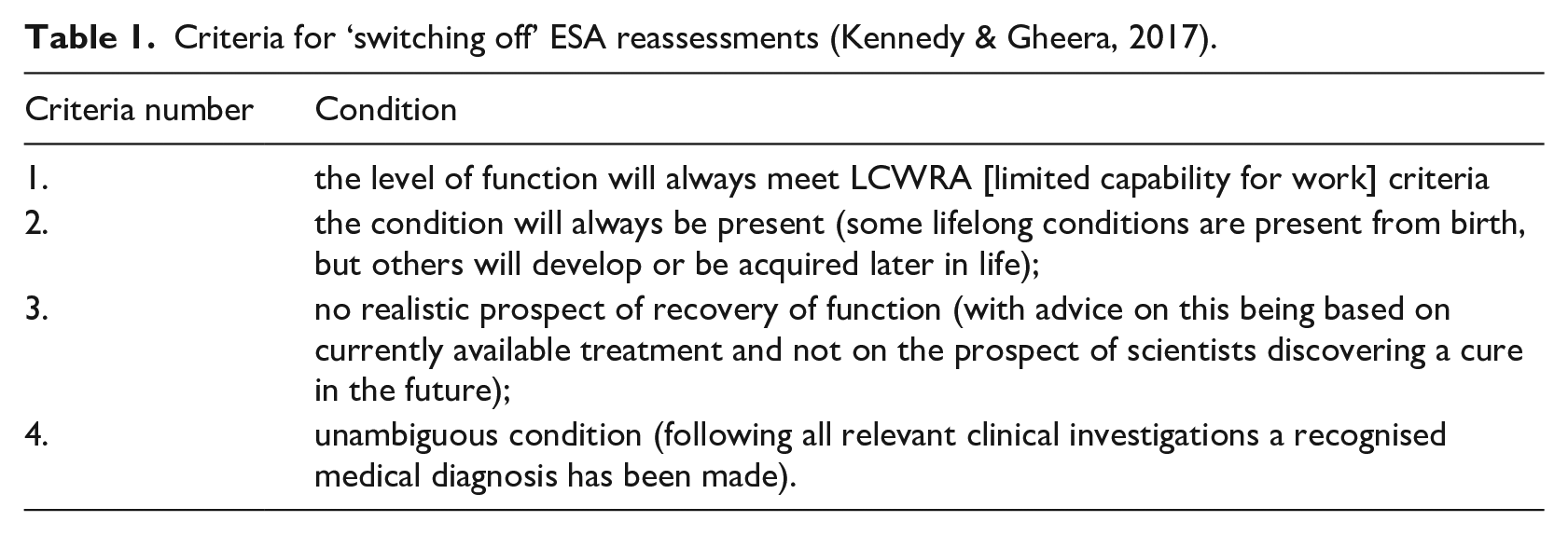
Only a minority of ESA claimants satisfy these criteria, the continual process of reassessments remaining for the majority (Grover, 2017). The Labour Party’s 2019 election manifesto proposed to ‘stop’ the WCA, yet retain some form of ‘in-house’ assessment (The Labour Party, 2019). But questions remain about how such a test may work in practise.
The medical model and patient-led care
The operationalisation of the WCA process in the UK could be interpreted as an extension of the medical model, beyond the usual context of patient healthcare. Within the medical model, the physician is seen as the ‘expert’, with an expectation that patients should comply with their advice. Disability rights campaigners believe that a consequence of the model is its grounding in a false notion of ‘normality’ with those outside of these expectations considered a ‘problem’: providing justification for patronising and dismissive attitudes to those with long term conditions (Shah and Mountain, 2007).
The emergence of patient-led care, whereby healthcare policy aims to give patients greater choice and voice within their own care, can be considered as a direct response to critiques of the medical model. NHS guidelines for patient-led care stress the need to respect patients’ understanding of their own experiences and ensuring a sense of value, facilitated through ‘respectful and compassionate treatment’ (Department of Health, 2005). With these changes in NHS policy, towards a more ‘patient-led approach’ (Department of Health, 2012), there now exists a dichotomy for those living with chronic illness within the UK. Individuals receive greater autonomy in their own care, with the caveat of being responsible for their own healthcare. However this attempt at ‘re-humanising’ the process of caring for chronic illness is potentially undermined by the dehumanising effect of the WCA: the impact of intersecting policies.
Despite a call to action on WCA reform from the British Psychology Society (BPS, 2016), the majority of research looking at the impact of welfare reforms has come from sociology and social policy (e.g. Baumberg, 2016; Dwyer et al., 2020; Patrick, 2014; Patrick, 2016; Patrick, 2017); human geography (e.g. Garthwaite, 2014; Garthwaite et al., 2014); and independent researchers with lived experience (e.g. Stewart, 2018). Through the WCA’s reliance on descriptors, attempts to quantify illness and disability run the risk of dehumanising at both an individual level and also within the wider embodied world, through changes in cultural perception: what are the lived experiences of those living within this intersection between health and welfare policies?
Methods
Design
Beginning from a pragmatic paradigm, as the research question sought to investigate the experiences of the individual, the study employed interpretative phenomenological analysis (IPA; Smith, 1996) as a way to explore how individuals made sense of their world (Smith et al., 2009). IPA as methodological approach allows the researcher to look in detail at how a phenomenon is made sense of by someone who is currently experiencing, or making sense of, the experience. Using a purposive sample, the aim of an IPA approach is to develop detailed descriptions of the experiences of a small number of individuals who all share this experience.
Data collection
The data set of this study consists of audio recorded and transcribed semi-structured interviews. The research team devised an interview schedule which outlined topics of discussion relevant to answering the study’s aims. The progression of the questioning was structured to move chronologically through the experiences of the interviewee: beginning first with biographical information and the contexts within which they live their life, towards a focussing on their experiences of chronic illness and perceptions of their WCA process. The schedule was not prescriptive, instead it acted as a guide to facilitate the interview.
Ethical considerations
Ethical approval was gained from the university’s ethics committee. Due to the potential impact of chronic illness on mobility and energy levels, great consideration was paid to offering a comprehensive selection of interview methods (face-to-face at any convenient location, via telephone or over internet messaging applications). The choice of which method would be most appropriate was made entirely by the participant: interviews were either conducted face-to-face, by telephone or Skype.
Participants
Participants were living with chronic health condition(s) and had all been through the WCA process. Participants were recruited following their response to advertisement material. Online charitable and disability rights organisations were contacted and assisted with the promotion of the study via social media posts. Poster advertisements were displayed in local public spaces, such as supermarkets, post office notice boards and libraries. The study excluded individuals who were living with chronic illnesses but had not been through the WCA process and those whose conditions were related solely to mobility or mental illness.
Analysis
Analysis initially began with the first author reading and re-reading each interview transcript. After familiarisation with the data was achieved, each transcript was annotated into a series of small handwritten summaries, succinctly describing the participants’ accounts. These explanatory comments were analysed to identify emergent themes, reflecting both the participant’s original words and the analyst’s interpretation. Identified themes were further explored with the second author and organised into tentative superordinate themes. This process was then repeated for each transcript. Themes from the transcripts were compared and recurrent superordinate themes identified. These reoccurring superordinate themes form the basis of the findings of this study.
Through the process of double hermeneutic interpretation (the researchers attempting to make sense of how participants are making sense of their experiences) and the desire of the IPA researcher to empathise and understand the participants’ experiences but from a critical and questioning standpoint, IPA allows the researcher to play an active role within the data collection and analysis (Smiths et al., 2009). As the first author has been living with a chronic condition, but not been through the WCA process, the need for reflexivity was of uttermost importance and can be accommodated by the IPA approach. Through the strategies of introspection, impression management and monitoring one’s own reactions (recorded within a reflexive log before discussing these written reflections within the research team), the first author was able to make sense of their own presuppositions, minimising their affect through these processes of active monitoring: reflexivity as a tool enabling hermeneutic reflection (Shaw, 2010). Insights gained from this engagement with reflexivity are explored within the study’s discussion section.
Results
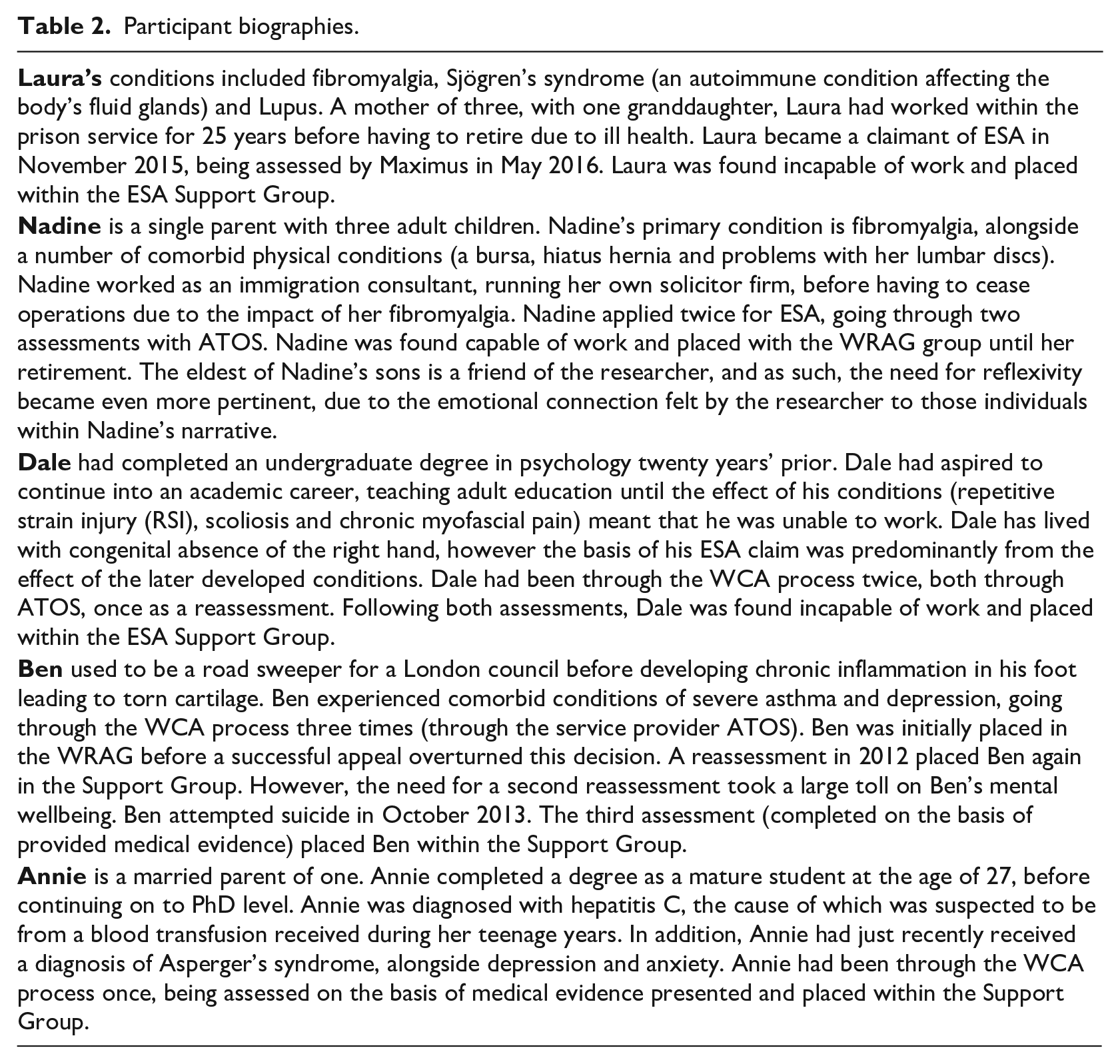
Participants (n = 5) had a varied range of chronic conditions and had all been through the WCA process. The final sample consisted of three women and two men. Participant ages ranged from 35 to 58. Further biographical details are included within table 2: pseudonyms have been used as a way to preserve participants’ anonymity. Interviews lasted between 50 to 118 minutes. Three themes were generated from the transcripts: ‘intersubjective sense making of the condition’; ‘battles for control’ and ‘the fluidity and strengthening of identity’.
Participant biographies.
Intersubjective sense making of the condition
Being diagnosed with a chronic illness may change how an individual perceives themselves within the context of their lived life. A person needs to redefine their understanding of their own body. However, this redressing of ‘knowing the self’ cannot be done in isolation and is instead a process that plays out within the context of their lived life. Participants demonstrated a variety of differing complex coping strategies, in an attempt to make sense of the impact their condition was having on their lives.
For Laura this sense making was underpinned by the ‘unseen’ qualities of her condition. The lack of visible affect went further than an omission of symptoms, but rather that as a consequence of Lupus she presented with a ‘healthy glow’ on her face. Within the context of work, this led to a surrendering of her private interpretations of her conditions. An open dialogue with colleagues and immediate management can be perceived as serving a function for Laura, to gain their acceptance of her experiences:
I was always very open right from the beginning I was very open with my colleagues about my condition and how it impacted on my my life because I think that if you try and hide it and just get on with it people are not so understanding
However there exists a contrast between her openness at work with her family life, in which the effect of her conditions took on more private and personal qualities. Struggles with steep stairs at her daughter’s house were a private act, not observed by her family members. This created a dichotomy between the shared and unshared-unseen. When the consequences of her condition were unable to be publicly avoided, feelings of vulnerable appeared to exist, suggesting a link between openness about her condition and which role (either as co-worker or parent) she presently occupied:
Maybe when I’m playing with my granddaughter that’s when it’s quite noticeable because I can’t get up and down off the floor and when you’re playing with a small child you need to be able to get down to their level don’t you? (.) So that’s difficult
Dale’s account of sense making was closely linked to the physical effects of his conditions. For Dale the body was understood in mechanical terms: the body as a malfunctioning machine:
It doesn’t mean how far you push it your body will just say no just which is what happened because you are arguing with your own muscle system and that then inflames the tendons
This interpretation of the body as a machine led to feelings of inevitability and futility for Dale. Coupled with a very strong sense of perceived lack of organisational support, sense of his life was made through the conclusions of these mechanical failings: the laws of physics, alongside physiological understandings of muscle structure were evoked to present a resigned sense of acceptance of the impact of his conditions.
Dale expanded these mechanical analogies to the context of his treatment by the WCA. In his account of both the assessment and discussions with ATOS staff, the mechanical extended beyond the merely physical. In contrast to his self-perceptions, whereby he was at the mercy of his physiology, employees of the WCA process acted purely as machines, devoid of any sense of human compassion:
When I finally got through which took 20 minutes on call waiting a guy completely monotonous voice just what they said was you give your national insurance number details to identify yourself as soon as I did that no conversation like a drone
The DWP was portrayed by Dale as being a tangible, oppressive physical being, able to physically act upon those within the system. He and other claimants were subjected to metaphorical physicality: ‘kicked’, ‘thrown’, ‘pushed’. These interpretations of the embodied world in which Dale finds himself, give further meaning to his feelings of inevitability.
Related to the understanding of their condition within the context of the WCA, all participants expressed a level of dismay at the categorisation process of ‘capability’. In the below example we see how the qualitative aspects of experience are reduced to a simply either/or response by the WCA assessor:
He said oh well can you drink a cup of tea I said yeah sometimes with both hands there are days when I can’t lift a cup of tea didn’t make a note of that but yes I can drink a cup of tea so it was a tick so it was basically just a tick tick area nothing I didn’t see him write anything it was a tick box um and I don’t think it really should be done that way
With no consideration of the effects of an action (i.e. potential for future pain) or the unusual methods developed to combat illness limitations; instead an emphasis on an individual’s potential to complete the action (capability), many participants felt their experiences reduced to an oversimplified and unrepresentative recorded response. The use of ‘tick boxes’ was a reoccurring symbol for most participants; representing a tangible, dehumanising, representation of their experiences.
Battles for control
In our second theme we see the need and desire for control over participants’ own lives. Participants perceived themselves at the mercy of many systems; the DWP (representing the state), healthcare services and the WCA process. Some relished the challenge, with the perpetual state of battle adding sense of purpose to their life. However, for others, the constant fight and uncertainty created an unwelcome and challenging additional worry.
Four out of five participants went through a lengthy perceived ‘battle’ for diagnosis. The role of general practitioners (GPs) became paramount, with the search for ‘good’ and supportive practitioners apparent as a common and shared experience. Nadine’s battles to be considered ‘unwell’, both for herself and for her youngest child (Ed), placed her own understanding of her conditions against healthcare professionals:
If I accepted everything that’s been said to me about me and I accepted everything that’s been said about Ed (.) I sometimes think well where would we be? [. . .] I sometimes think GPs and consultants think (.) they’re gods and whatever they say patients have to accept no they don’t (.) we don’t have to accept I’ve seen it too often with people outside accepting whatever the consultant and GPs are saying to them and then what happens to them 5 or 10 years down the road? (.) No I don’t want to end up like that
Through her process of self-knowledge (progressing from the ‘early days’ to the present), Nadine achieved a sense of justification that enabled her to step outside the perceived medical model. The opinion and treatment regimens of doctors were merely suggestions, options that needed to fit with her own worldview as a necessity. However, this willingness to challenge those in positions of authority also gave Nadine a sense of unease, despite her outward confidence in her self-understanding. Regarding her difficulties in getting diagnoses and the inconsistent levels of care received, Nadine questioned if her challenging approach may be the reason why; if she was being punished (perhaps consciously) by healthcare professionals for her resistance:
(.) I don’t know I really still can’t understand why they sort of even after all this they think um is it because I challenge them?
This perception of punishment was felt in an embodiment sense through the treatment received by Nadine. However by forging her own version of patient-led care, through her challenging approach to healthcare professionals, Nadine saw and felt potentiality, in opposition to the more definitive and restrictive conclusions of the medical model. In the below short extract we are able to see the hope greater autonomy can provide for people with chronic illness:
I’m not gonna let someone else dictate to me and say you know x y and z when it isn’t it’s a b c (.) it’s the beginning not the end right?
Battles for control were similarly present within the WCA process. For Laura this manifested as taking proactive responses in the face of opaque processes. As a first time applicant of ESA, Laura found herself within the ‘mysterious’ and worrying environment of the job centre:
So it was like you go to the job centre and it’s a horrific experience [. . .] I just kind of wandered in there and stood there and nobody tells you the queuing system I didn’t understand the queuing system! It seems that you just sit on a chair and move along and they all know who is next but you don’t
Here we are able to see how Laura’s perception of the unspoken rules of the job centre positioned her as an outsider, neglected by staff. With this outsider status came a loss of control, Laura finding herself unable to master her immediate environment. When attending her WCA medical assessment, these feelings of horror merged with a sense of paranoia. Laura perceived the whole environment in which the assessment took place, from the armless chairs she sat in, inaccessible ‘accessible’ toilet and questions asked by staff, as all part of a wider attempt to uncover a fraudulent claim (‘constantly looking to shut you up’). However, through her manipulation of the physical environment surrounding her (pulling her chair up to a desk for arm support), Laura was able to regain a level of autonomy. Laura told of similar experiences within the workplace, of her proactively seeking out and making changes to her working environment which enabled her to continue in employment for a longer period of time. However, she did consider herself ‘lucky’ in her ability to persist with and actualise her need for control.
In contrast Ben’s loss of employment in addition to the inconsistency and uncertainty created by the WCA process (specifically the DWP’s dismissal of medical evidence) had a devastating effect on his sense of control over his own life: Ben interpreting these stresses as causally leading to a suicide attempt. For Ben this loss of control had a physical manifestation, an ever-looming fear of receiving a third reassessment letter from the DWP:
There’s always in like the back of my mind every day the postman comes is there gonna be another form er or another like letter for another appointment so (.) in a way the last result I’m happy about but to be honest I don’t think if someone has got severe mental health like um issues they shouldn’t keep calling him back in
Ben’s loss of control appeared to be linked with a loss of faith with the benefit system (explored further within the theme ‘the fluidity and strengthening of identity’). A sense of bewilderment was apparent; Ben was unable to fully come to terms with this loss of control. Appeals to superstitions (‘touch wood’) and hope were present throughout his narrative, acting as illustrations of his perceived external locus of control. Happiness was fleeting, undermined by the extended periods of uncertainty cultivated by the WCA process. However, for Ben, a return to work was something he desired. Due to his most recent assessment placing him in the Support Group, this was an element of his life he was able to regain control back from the DWP:
I do want to try and go back to work but I wanna do it when I’m I feel ready to you know? Not when they say oh you will like go out tomorrow and get a job
The fluidity and strengthening of identity
In our final theme, the impact of chronic illness and the WCA process upon participants’ identity is considered. For most participants the life processes of illness altered their notions of identity and their previous perceptions of the self. For others, living with chronic conditions strengthened and reaffirmed held beliefs about their own identity.
Having had to leave plans for academia behind due to the impact of his chronic illness, a sense of haunting existed within Dale’s account: loss of the live imagined (Ahlström, 2007). ‘Ghosts’ of his past self that might have been, or future selves that could not now be, were present throughout, either as lost potentials or unrealisable goals:
There was a sense of resignation er when I was diagnosed oh good but so what it was (laughs) there was nowhere else I could go with it well ok it would have been really good to go back in time 20 years because I might have been able to stay fully functional [. . .] I would have been able to fight for an academic career because even if I couldn’t type um I wouldn’t have um been out of action for so long I could possibly have er forced through things that didn’t exist
These feelings of loss channelled into a myriad of different emotions for Dale: anger and frustration at the WCA process and his treatment by the NHS, but also the positive. Despite removing himself from anti-WCA activism, and guided by a strong sense of empathy for those perceived to have had ‘a lot worse’ than himself, Dale positioned himself as a potential educator for those interested in continuing ‘the fight’:
I don’t care [about] activism anymore although I would support anybody else who is doing it completely if they needed information or they didn’t know or they didn’t the background that I know they don’t know where the links are [. . .] you know if somebody asked for that and they can’t find it I would ah I’ll give it to them in a second
Annie’s identity as a pragmatic realist appeared to have been strengthened in response to the perceived illogical approach taken by the DWP. Annie showed a great understanding of the long-term progressive effects of her condition, discussing the possibility of death and further mental deterioration in a considered and accepted manner. However due to her understanding of the progression her condition will take, Annie questioned the process of reassessment required as part of the WCA:
I have a constant progressive disease that isn’t getting better um so and I think for a lot of people it’s the idea that you still have to be reassessed again and again every couple of years is surely a waste of the DWP’s own budget because you know if people have incurable conditions then nothing you know they don’t need to be constantly reassessed their situation isn’t going to change
Through her pragmatic approach to the collection of medical information, Annie’s WCA was completed without a face-to-face assessment. As such, Annie positioned herself outside of those who experienced the full assessment. In contrast to the ‘fortunate’ feeling associated with finding a supportive GP, Annie ascribed her successful WCA process solely to her own considered approach: her avoidance attributed to her own efforts of collecting information and ‘sufficient’ filling in of the initial questionnaire.
Although not reflectively acknowledged, Ben’s experiences of the WCA tell a story of him as an experiential learner. In his first assessment, Ben trusted that the information he had given about his chronic inflammation would be sufficient.
I didn’t really mention the depression because I thought having a problem with the foot would be enough to get get me through the assessment
However due to his need to appeal, and the vindication received following the success of this appeal, Ben began on a process of discovery, dismantling his trusting faith in the welfare system and building a new identity of problem solver through action. His own experiences informed by a lived understanding of the bureaucratic processes, led him to gather further medical evidence and complete further reassessments with the sought help of different assisting professionals (solicitor, benefit support officer and a more supportive GP).
The history of Nadine’s identity as a single mother became deeply intertwined with her experiences of chronic illness. Her love for her children drives and informs all of her decisions around medical treatment and work. However due to the debilitating effects of her conditions, the traditional care provider component of motherhood became merged between Nadine and her children.
Um even silly things like washing up in the sink it’ll just get pilled and the youngest will come home and go [. . .] into the kitchen and if the washing’s still there to be done because I haven’t got up to do it (.) it’s not because I’m lazy [. . .] he just does it so if I didn’t have him as I said to a lot of people I couldn’t manage (.) I really couldn’t manage without him being in the house with me he helps me so much
Here despite the ‘silliness’ of simple household chores, Nadine was unable to attain her own expectations. Aware of how this may be perceived by others, Nadine shows a keenness to distance herself from potential accusations of ‘laziness’. This unconditional support from her children was understood by Nadine in terms of a closeness to her own illness that takes on a metaphorical-physical connection between mother and child:
When I have a flare-up and my body is burning literally my body burns with pain and the kids can feel it
Here the symptomatic pain she feels transcends physical possibilities. Due to the way in which her children have grown-up learning the effects of their mother’s fibromyalgia, a connection is felt that extended beyond the normal capacity of empathy.
Discussion
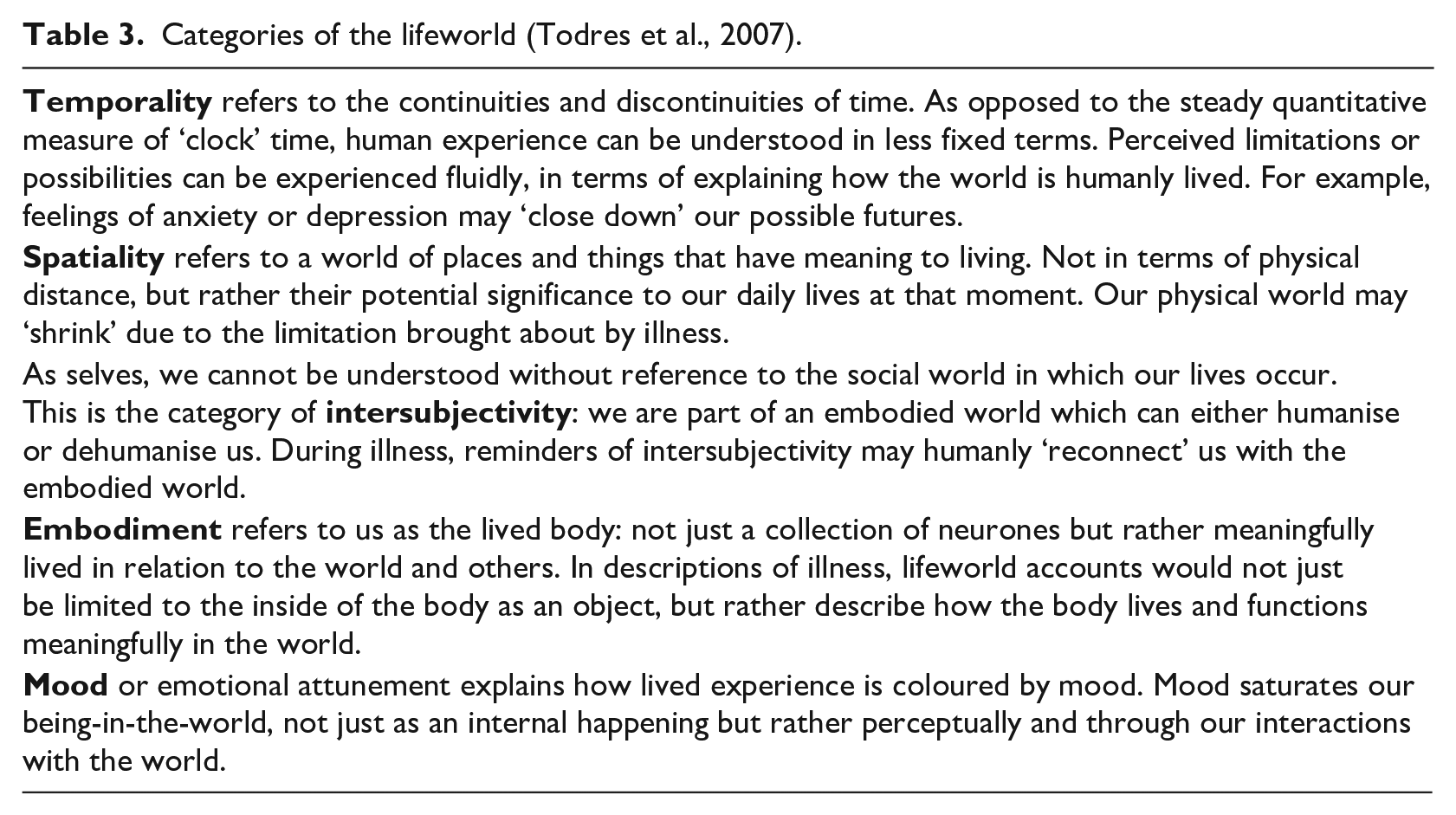
The findings reveal a number of overarching and interconnected themes within participants’ accounts. Their narratives revealed the need to ‘re-know’ the self following the onset of chronic conditions. Analysis of these processes revealed a complex array of sense making approaches. By considering our findings in relation to Todres et al.’s notion of ‘life-world led care’ (2007) we can appreciate the holistic context in which human experience makes sense. The lifeworld can be best understood as a conscious acknowledgment that all events have a qualitative dimension; that we do not exist ‘objectively’ within a universal of neutral objects, a sum of processes, attributing meaning to others and things (Todres et al., 2007). We are part of an embodied world; through the intersubjectivity and aided by language we are able to locate ourselves meaningfully in the ongoing interpersonal world (Todres et al., 2007). However, as we have seen, this meaning is found within our lived worlds, such as welfare systems and healthcare services (Table 3).
Categories of the lifeworld (Todres et al., 2007).
Elements of participants’ conditions were inherently connected to intersubjectivity: the impact of a lack of condition-visibility. Driven by perceived expectations or the judgement of others, participants sought to understand their condition as lived. Once, or whilst, sense was made participants gained a sense of confidence; an understanding of their condition in opposition to perceived prevalent cultural interpretations. However, this understanding was then undermined, or ignored, by the WCA process. The focus on ‘capability’, manifested in either/or tick box choices, ignored the qualitative dimensions of their conditions and led to feelings of dehumanisation. The physical environment of assessment clinics created acutely felt feelings of horror and paranoia through the dehumanising effects of space.
Participants also described strong feelings of a lack of autonomy. However, this loss was not due to the restrictions of their conditions, but rather through lengthy battles for diagnosis, effective treatment and recognition by the WCA process. Battles for control can be understood as attempts to distinguish themselves beyond the medical gaze (Foucault, 1973). When autonomy was possible (through authentic patient-led care and after WCA decisions), participants described emotions of relief and potentiality; directly contrasting with the anxiety and uncertainty associated with medical model approaches.
Participants’ experienced the WCA as an extension of the medical model. Habermas (1990) progressed Heidegger’s (1966) thoughts, predicting that capitalism and technological progress would eventually turn humans into commodities, with their value determined by how efficiently they fit into larger, impersonal systems (Todres et al., 2007). The WCA quantitatively categorises those with ill health into either the legitimate (thereby those individuals who are ‘excused’ from work) or illegitimate (individuals who then required to comply with workfare systems). However, unlike the ‘rational’ workplace (Vickers, 2003), participant narratives presented this process of categorisation as illogical due to its impersonal and ineffective approach; decisions that did not cohesively fit with their own gained understandings of their conditions. Due to the embodied world in which participants live, the DWP was perceived as an inescapable and physical force whose decisions cannot be easily battled, creating feelings of uncertainty, stigmatisation and frustration.
Reflexivity
As the first author is living with a chronic condition, this shared commonality between interviewer and interviewee heightened the potential for presuppositions to influence both the interview and analysis. However due to my engagement with reflexive practises, I believe these presuppositions were acknowledged and became known; a ‘bridling’ of beliefs and experience that may have overwise hastened my (mis)understandings (Dahlberg, 2006). As more interviews occurred it did, however, became more problematic to begin from a ‘neutral’ standpoint as presumptions became informed by previously heard narratives.
Nadine’s account revealed particular significant feelings for myself. In her discussion of her battles for her son’s diagnosis I saw my own past in these descriptions, and the experiences of both my parents (in particular my mother). The ‘battles’ fought on my behalf by my mother (whose lifelong profession as a nurse may have given her an ‘advantage’ in comparison to Nadine’s necessary learning process) became easier once I was under the care of a supportive consultant and his team, leading to a successful diagnosis and treatment regime.
The reflexive practice undertaken as part of this research enabled me to understand the consequences of this relationship between compassionate healthcare professionals and myself as a patient. Due to my eventual ‘positive’ experiences I now understand myself as a proponent of the medical model; a persistent and unwavering degree of respect for those working as healthcare professionals, and myself as an unquestioning and compliant patient. However, I also hold a contrasting view; believing in the importance of a deeper understanding of humanly lived experiences for those living with chronic illness, and an acknowledgement that cannot be fully accommodated by the medical model. This contradiction has been strengthened by hearing the narratives of this study’s participants, in tandem with my own reflexive understanding of the self.
Limitations
Participants recruited and included within the study had a wide and varied range of conditions, both in terms of symptoms and length of living with their illnesses. However, it is apparent that, despite these differences, participants were treated similarly by healthcare services and the WCA. The qualitative approach taken by this study allowed a deeper interpretation of individuals’ experiences of these systems, without the aim of generalising these findings to all those living with chronic illness. However, future research should not exclude the benefits of exploring illness capability by condition.
The majority of participants were recruited in response to advertisements promoted by welfare reform campaign groups. As such, it may be that participant perceptions of the WCA were always likely to be negative; a potential selection bias. However, the purpose of this study was not to provide a comprehensive evaluation of the WCA process, but rather present narratives of those who have experienced the phenomena.
Implications for practice and future research
Within battles for diagnosis and recognition, the deprivation of autonomy was a common experience. Through processes of sense making, a complex effect on personal identities occurred, in attempt to gain ‘consistency’. The need for greater autonomy can be accommodated by healthcare professionals, aided by a more respectful, thorough treatment of physical ailments, without being seen to reduce symptoms to a purely psychological cause. Experiences of patient-led care led to positive feelings of hope; occurring when participants felt as though their own (gained) knowledge and understanding were considered. Dahlberg et al. (2009) argue that the patient is often positioned as a consumer, within the wider context of ‘citizenship’, and that the developments of NHS feedback systems take for granted the meaning of health and illness, prioritising operational concerns. Authentic attempts at patient-led care, through the utilisation of lifeworld-led care concepts, may increase patient feelings of hope and autonomy.
However, the dichotomy that now exists for those living with chronic illness in the UK undermines the positive effect of authentic patient-led care. Individuals may be able to receive greater autonomy in their own care; however, they also experience the dehumanising effect of the WCA. Participants’ understandings reveal the WCA as an extreme version of the medical model, measuring conditions via a systematic refusal of the qualitative aspects of illness. When considering specific biographical accounts, it is possible to see how greater inclusion of lifeworld concepts could more accurately, and fairly, assess ‘capability’. Having the autonomy to return to work on his own terms allowed Ben to enjoy this temporality possibility; a projection of his future self. Laura’s need to spatially manipulate her immediate physical environment reveals how embodied meaning can be gained from objects, empowering her.
These positive effects were however anchored to the ebb and flow of reassessments. Participants often despaired at the need for reassessment, perceiving an illogical and fundamentally uncompassionate system. Informed by their own journeys of illness understanding, many questioned how their chronic and often progressive conditions would justify a reassessment every two years. Reassessments perpetuated anxious moods; colouring individuals’ daily lives with uncertainty and unpredictability. Individuals’ wellbeing would likely be improved were the DWP’s criteria for removal of reassessment broadened to include those living with long-term health conditions (Agerholm, 2016). However the narrative accounts explored within this study do suggest that the factors which contribute to ‘capability’ are far more complex than can be captured by the WCA process in its current form.
From a methodological standpoint, we believe that this research illustrates the value of examining the impact of social policy from a phenomenological perspective; allowing us explore, in-depth, the impact of intersecting policy approaches on those individuals entangled within bureaucratic systems. Future research should follow this thread, considering the viability of lifeworld informed measures of work capability.
This study provides a valuable contribution, presenting experiences of individuals living with chronic conditions within the wider context of modern welfare reform. The findings demonstrate the importance of individuals’ autonomy, and illustrate examples of how considerations of lifeworld concepts would provide a broader and deeper understanding of chronic illness and capability.
Footnotes
Acknowledgements
We would like to sincerely thank the participants who gave their time to take part and all those who helped promote the study – with particular thanks to Disabled People Against Cuts. Additional thanks to Dr Peter Branney for their invaluable feedback on an initial draft of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.