
Abstract
This study explores the views of advance care planning in caregivers of older hospitalised patients following an emergency admission. Semi-structured interviews were conducted with eight carers, mostly with a personal relationship to the older patient. Thematic analysis generated three themes: (1) working with uncertainty – it all sounds very fine. . . what is the reality?, (2) supporting the older person – you have to look at it on an individual basis and (3) enabling the process – when you do it properly. The belief that advance care planning can support older individuals and scepticism whether advance care planning can be enabled among social and healthcare challenges are discussed.
Introduction
Advance care planning (ACP) is described as a process that helps to determine how people wish to be cared for with regards to future medical care ‘during serious and chronic illness’, in a manner which is ‘consistent with their values, goals and preferences’ (Sudore et al., 2017). ACP can involve (1) making an advance statement for preferences for care, (2) an advance decision to refuse treatment in pre-defined future circumstances and (3) nomination of a surrogate decision maker in case of loss of mental capacity (Conroy et al., 2009).
Discussing future wishes with caregivers can be a valuable part of the process of ACP; this activity ensures that an individual’s wishes are heard and understood, together with carers that an individual may choose to involve (Bakitas et al., 2017; Zwakman et al., 2018). ACP can be seen as a spectrum with three potential stages: first, future care planning (with several years prognosis, patient-centred planning focussing on understanding illness, health, well-being and social care); second, urgent care planning (mostly with a limited, 1- to 2-year prognosis, focussing on medical options for care, including understanding disease trajectory and limitation of interventions, and may include resuscitation decisions) and third, end-of-life planning (focussing on preferred choices of care and death at the end-of-life, including discussions on resuscitation).
A systematic review of the literature has shown that ACP with appropriate urgent and end-of-life care planning improves the quality of care at the end of life, with better concordance of medical care with the end-of-life wishes of individuals and reduced unplanned hospital admissions (Brinkman-Stoppelenburg et al., 2014). Similarly, in older hospitalised patients (aged 80 years and above), ACP has shown to improve end-of-life care, ensuring that older adults’ wishes are known and followed, and improving patient satisfaction (Detering et al., 2010).
There is substantial evidence that the success of ACP depends on carers as well as patients (Hall et al., 2019), with family carers mediating between patients and healthcare professionals during decision-making (Mignani et al., 2017; Sharp et al., 2013; Skinner et al., 2014). It has also been posited that ACP might positively impact on the emotional well-being of carers with fewer signs of post-traumatic stress, anxiety and depression after the death of a loved one, potentially due to better satisfaction with the quality of death, compared to usual care (Detering et al., 2010). This is particularly relevant since care-giving responsibilities can be associated with significant psychological burden in carers (Liu et al., 2017; Malhotra et al., 2012; Podgorski, 2018), even following bereavement of the older person they care for (Detering et al., 2010). Supporting carers is not only important on a compassionate basis but is also crucial to health economics, as unpaid informal carers are a ‘hidden workforce’ (Grande, 2017; Rowland et al., 2017), on which the National Health Service (NHS) currently depends (Buckner & Yeandle, 2015).
The relevance of acute hospitalisation to ACP is also apparent. An emergency hospital admission in later life may be a time which triggers a reflection on an older person’s needs or deteriorating health as an impetus to starting an ACP discussion or updating an existing care plan (Bielinska et al., 2017b; Moore et al., 2018). This is crucial for both older adults and their loved ones, since an estimated 20–30 per cent of hospitalised adults are in their last year of life, with mortality rising with age (Bielinska et al., 2017b; Clark et al., 2014). Indeed, research suggests that the last year of life can be a time punctuated with unplanned hospital admissions, highlighting the relevance of ACP in acute hospital practice (Gill et al., 2015; Quinn and Thomas, 2017). As such, there is a need to provide medical care concordant with the patient’s wishes and to support carers.
Despite the growing need to understand the interplay between acute hospitalisation, older patients and carers in order to facilitate ACP, there has been no research investigating the views towards ACP of carers of older adults who have been hospitalised following an emergency. To address this gap, the aim of this study was to explore the views of ACP in caregivers from this cohort, including their preferences in the language of ACP, perceptions of the significance of ACP, preferred content of advance care plans and preferences on sharing advance care plans.
Methods
Participants and recruitment
The study was set in a large teaching hospital in North West London with an emergency department. To identify carers of older adults, patients aged 70 years and above admitted as an emergency with any diagnosis were identified randomly from a daily computer-generated list. A member of the inpatient clinical team, namely the ward manager (nurse in charge or deputy) or ward doctor, sought permission from medically stable patients as to whether they agreed to be approached by a researcher to nominate a carer for interview. Carers visiting the older person during the hospital stay who had sufficient English language proficiency for interview were eligible to participate. Patients were excluded if they were less than 24 hours into their hospital admission, were in a terminal stage of illness or were critically unwell in a high dependency or intensive care setting. Participants were also excluded if they lacked capacity (as defined by the Mental Capacity Act, 2005).
Patients were offered a participant information sheet by the researcher and gave their verbal consent for their nominated carer to be invited for interview. Carer participants provided written informed consent for interview, obtained by the researcher (A-M.B.). Carers were asked to reflect on the concept of ACP and were not required to discuss their individual situation.
Materials and procedure
Face-to-face semi-structured interviews were conducted in the hospital environment by A-M.B., a doctor outside the patient’s clinical care team, with a background in hospital medicine and research interest in ACP. The semi-structured interview was based on a topic guide co-designed and pilot tested in an earlier study with a separate sample of patients and carers who had a specific interest in ACP (Bielinska et al., 2017a).
The interview explored carers’ views of ACP, including (1) attitudes towards language used in ACP discussions, (2) the preferred content of an advance care plan using a list of potential topics (modified from Boyd et al., 2010) and (3) the significance of ACP relating to the perceived benefits and risks and attitudes towards sharing information within advance care plans. To facilitate discussion, a case study was presented to participants, using a leaflet from Coordinate My Care (CMC – an electronic palliative care coordination system (EPaCCS)), of an older patient with advanced cancer admitted to hospital as an emergency with a CMC plan. Interviews (lasting on average 30 minutes) were audio-recorded digitally and transcribed verbatim, using pseudonyms (that were chosen by the carer) throughout. In addition to field notes, the Caregiver Burden Inventory (CBI) was performed to screen for caregiver stress. Interviews were conducted until data saturation was reached.
Ethical approval
Ethical approval was granted by the Hampstead Research Ethics Committee (REC; Reference no. 16/LO/1798).
Data analysis
All transcripts were analysed using the six-phase process of thematic analysis (Braun and Clarke, 2006), a rigorous approach which has been used elsewhere in qualitative analysis of views ACP practices (Jack et al., 2018; Moore et al., 2019; Sævareid et al., 2019). Transcripts were repeatedly read, and notes were created about possible codes (by A-M.B.). Formal manual line-by-line coding followed and further notes were written to support data patterns (by A-M.B.). A random sample of transcripts was independently coded line-by-line by a second researcher (G.S.) and discussed with A-M.B., revealing high convergence. Codes were extracted and were drawn together as sub-themes and themes which represented the overall data (by A-M.B.). Sub-themes and themes were reviewed and refined with the construction of a thematic map displaying the relationship between themes and sub-themes (by A-M.B., reviewed together with S.A. and C.U.). Examples from the dataset were used to demonstrate each theme and help understanding. Throughout the process, authors discussed the evolving analysis to resolve any discrepancies; this process was aided by the multi-disciplinary nature of the team.
Results
Carer characteristics
Eight carers were recruited into the study; seven were female. Participants were aged between 21 and 82 years. The majority were informal carers (7/8) and were first-degree relatives or spouses (6/8); only one carer was employed professionally. Five carers agreed to complete the CBI; two carers reported ‘little or no burden’, two reported ‘mild to moderate burden’ and one reported ‘moderate to severe burden’ as shown in Table 1.
Carer participant characteristics.
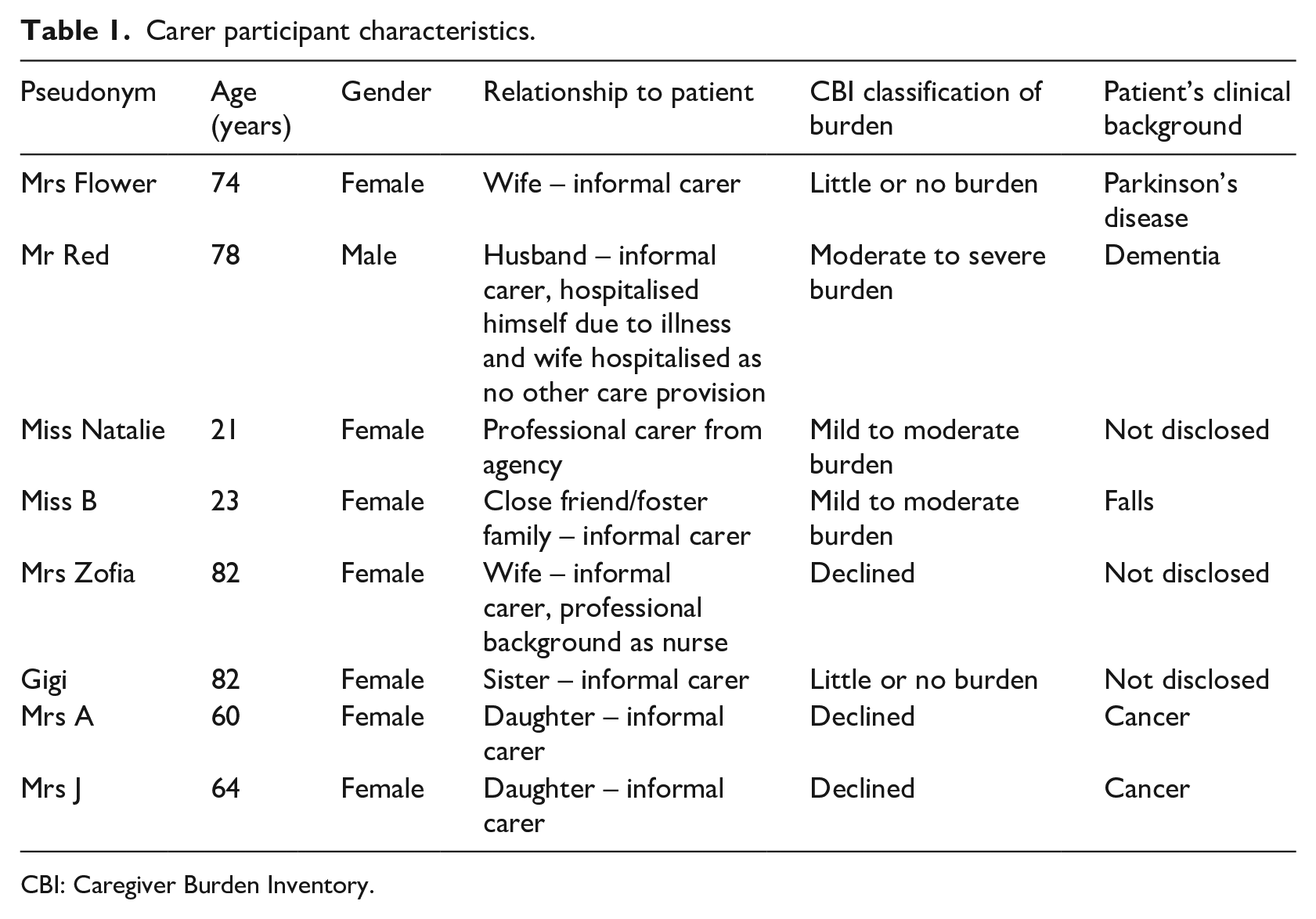
CBI: Caregiver Burden Inventory.
Data analysis
Data saturation was reached after eight interviews. The thematic analysis generated three themes: (1) working with uncertainty – it all sounds very fine. . . what is the reality?, (2) supporting the older person – you have to look at it on an individual basis and (3) enabling the process – when you do it properly as shown in Figure 1.
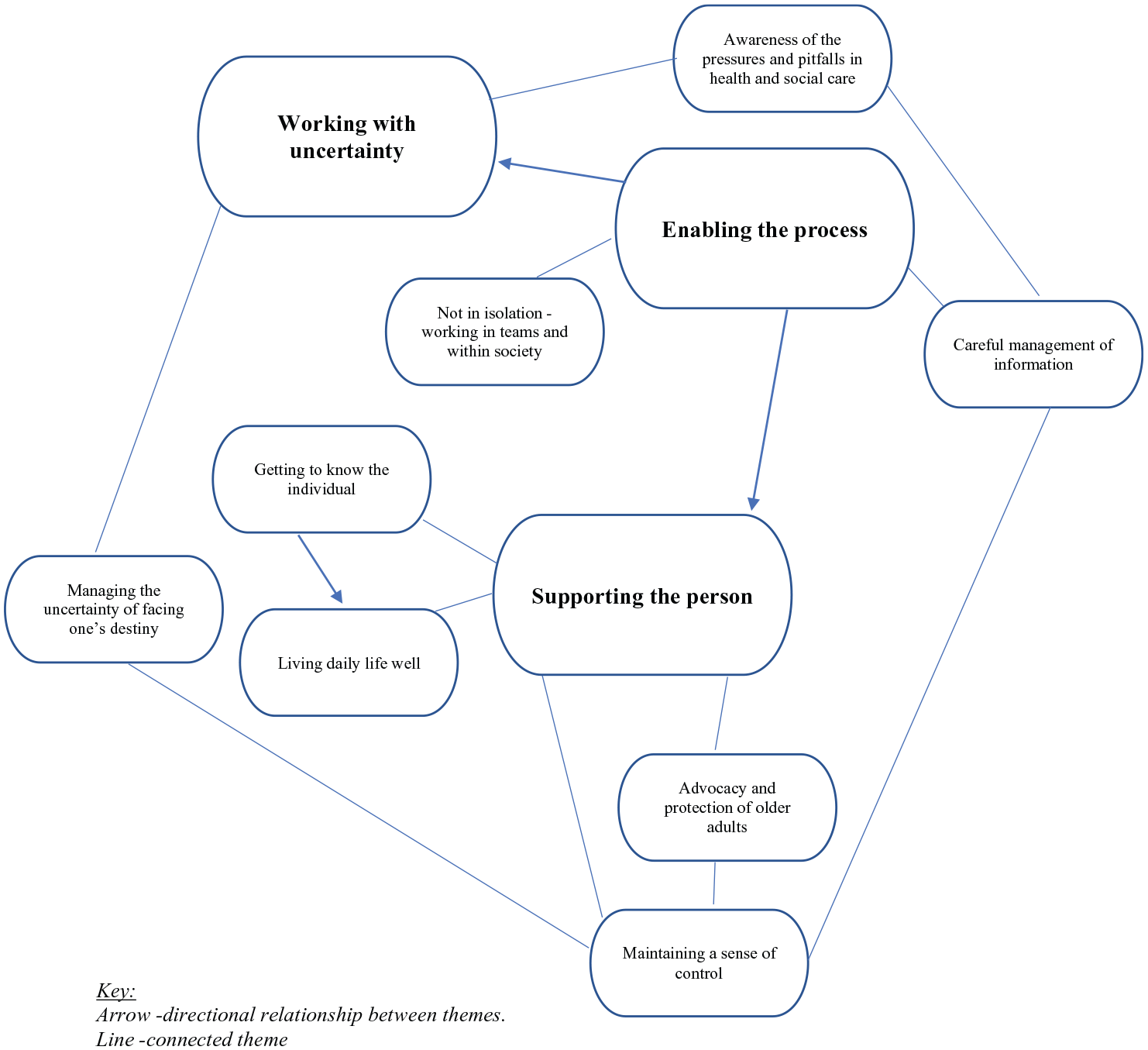
Thematic map of views of ACP in carers.
Theme 1: working with uncertainty – ‘it all sounds very fine. . . what is the reality?’
Carers expressed that ACP was fraught with uncertainty and acknowledging this was crucial to actualise plans. Carers expressed uncertainty in two main areas: first, the pitfalls in health and social care systems that could impact ACP, and second, the existential problem of facing an uncertain destiny in older age, particularly how a physical condition may progress, prognosis and deal with unforeseen emergencies.
Carers experienced a disconnection between the current problems within health and social care and the aspirations of ACP. Participants referred to cuts within frontline acute services and described how this prevented ‘the dream’ of personalised care: As much as I really would love for there to be catered plans, with the current resources that the NHS have that’s not feasible. (Miss B)
Concerns regarding low levels of staffing and the impact of low pay also contributed to doubts around the feasibility of ACP: It all sounds very fine. . . what is the reality? We know there aren’t enough carers and we know they get paid disgustingly poorly and you probably don’t get the right people because of the bad pay. (Gigi)
Some believed that ACP could improve the use of resources, reducing emergency service use and hospitalisation: We could have cut down the stress of my father going to A&E and knowing that there is a care plan. . . alleviate the beds that we’re using. (Mrs A)
Carers highlighted the time pressures faced by healthcare professionals as a barrier to conducting ACP discussions with older patients. Drawing from her experience as a patient, rather than a carer, Gigi recalled a discussion about resuscitation preferences when she was previously in hospital: Well, something happened, and he went away, and the conversation was never finished so I didn’t sign anything, and I hadn’t filled one of those forms in saying that I don’t want to be. Yes, he got called away and then we didn’t have, or I went home, or something happened, it was never finished. (Gigi)
Although many carers acknowledged the positive role of ACP, some participants believed that advance care plans might result in the neglect of older persons, where patients and family carers believed that appropriate actions have been taken to put a medical care plan into place, later discovering nothing had been done: . . .sometimes we feel that we could be let down, or my father slipped through the net. (Mrs A)
Carers had an awareness of the unpredictability of life and insight into how this may affect ACP. Carers either believed ACP should take life’s changeability into account and be frequently reviewed to succeed, or that the intrinsic unpredictability of life would prevent ACP from working altogether: You can’t really plan to what will happen, a week ago he was alright and yesterday he was here because it wasn’t planned. (Mrs Zofia)
The participants highlighted the need to adopt a flexible approach to ACP, accounting for varying experiences and attitudes: I think having, yeah, someone taking into account your actual circumstances not kind of saying this is, you know, dogma and the way it has to be, like regimented because that sometimes just doesn’t work. Everyone has different lifestyles. (Miss B)
Some carers noted that engagement with ACP was often determined by the patient’s preference for information on their prognosis. Avoiding consideration of the future in older age was described as maladaptive if it prevented consideration of care needs due to a false sense of security: You think you’re going to live forever and you’re not going to need care, this is the trouble, you tend to leave it until it’s possibly too late. (Gigi)
Carers felt that ACP would prepare older persons for the experience of illness and encourage someone to develop strategies on how to manage their disease, including in urgent situations: Your wishes are taken account. . . you can’t choose when you get ill but with the plan you can choose how. It’s kind of preplanning for everything that you’d need. (Miss B)
Control over the initiation of ACP was essential for patient ‘buy-in’. Mandatory imposition of a care plan was described as a potential source of unnecessary stress for older persons: I think when looking at a care plan one needs to look at the actual circumstances of the family, oh, and the patient themselves. There may be cases where a care plan is not needed at all and having it kind of discussed may just cause the patient stress. (Miss B)
A further limiting factor to the completion of ACP was the risk of disagreements between patient and family carers. The use of power of attorney within ACP was also potentially contentious, with anxiety of making the wrong decisions or poor communication during decision-making exacerbating this problem: The difficulty is that at the moment we have a different view and there’s a bit of a clash. . . So, it’s very tricky, very tricky. (Mrs J)
In summary, carers recognised that there were real-world challenges to the delivery of ACP, primarily focussed around the pressures of the health and social care structures and life itself presenting unforeseen challenges, centred around illness and ageing.
Theme 2: supporting the older person – ‘you have to look at it on an individual basis’
ACP was described as a beneficial process that would help to support the older person in terms of advocacy for their well-being and rights, independence, quality of life and supporting them as an individual. Carers believed that ACP had a role in the protection and well-being of older adults, particularly frail, isolated or otherwise vulnerable persons.
Sharing information within advance care plans across health and social care was deemed to have the potential to improve the safety of care. Miss B favoured sharing information within care plans with relevant professionals to benefit the safety of service users with mental health problems and carers: One lady we look after she has schizophrenia and social services are quite involved in that because, you know, she’s leaving her door open in the middle of the night and she’s 90, and you know, anyone can walk in. Absolutely safety and it’s also safety for the workers themselves. (Miss B)
Some carers advocated for increased sensitivity to the psychological preparedness of an older person to discuss ACP. Mrs J emphasised the need to occasionally slow down discussions to protect the emotional well-being of the older person: Sometimes you need to drip feed information, so it doesn’t come as a complete shock because it’s how you handle it. (Mrs J)
Although advance care plans were generally seen to help others advocate for older persons, some carers emphasised the need to be vigilant whether an older person was making a decision due to external pressure or fear of being a burden to others: It’s very difficult because when you’re an elderly person you don’t want to be a burden to anybody and this is what everybody says, so you may come round to doing something that you really don’t want to do because you’ve been persuaded to. (Gigi)
Carers also recognised that it was important for older persons to maintain a sense of control over their own lives as they plan their future care. Control included independence, self-expression and empowerment through gaining knowledge through ACP. Determining activities important to an older person was felt to promote independence: . . . a lot of people think that they’re unable to do certain things and tasks, and that can be really depressing for the patient, so to put a positive light on and say, ‘Yes, continue doing this’. That is important. (Mrs J)
It was believed that ACP discussions could empower older persons: If somebody has knowledge of what’s going on then they’re better able to sort of have control over what needs to be done. (Mrs J)
Carers also described the need to overcome obstacles to self-determination, including healthcare professionals with opposing views to older patients who may persuade against their wishes. Gigi discussed a doctor trying to persuade against a do-not-resuscitate decision she had made when she was a patient: I’d had a heart problem and they did ask me then did I want to be resuscitated and I said no and then the doctor. . . wasn’t prepared to accept that I didn’t want to be resuscitated which I thought was quite funny. (Gigi)
Carers also believed that quality of life could be promoted through ACP by achieving the tasks of daily living and enabling preferred choices. It was hoped that appropriate ACP could help older persons continue to live in their home: Well, if you’ve got the right care plan then you wouldn’t have to leave home. I think everybody wants to stay home as long as they possibly can. (Gigi)
ACP was also felt to prioritise quality of life during chronic illness and enable person-centred care. For some carers, maximising quality of life meant making an advance decision to refuse treatment or planning fulfilling activities during medical treatment. Miss Natalie described the potential of social care plans to improve an older person’s quality of life by improving their mental well-being: . . .and the social care plan. . . it’s to do more with the mentally, mentally, the whole, you know, his body and everything or how he feel and like his family, or how he wants you to contact him, what he would like to do, go out or meet people, which people he wants you to contact when he’s sad or happy. (Miss Natalie)
Carers also emphasised the need to build up a picture of the individual for whom the advance care plan is being created, to remember the older person’s identity before they were affected by illness. For example, Mrs J stated that knowing the views of the individual is important: It really depends on each different situation, and some people are more demanding and want more information than other people, so I think you have to look at it on an individual basis. (Mrs J)
Overall, the carers acknowledged that conversation and familiar faces were advantageous to ACP, preferring this over the anonymity of digital plans. Some believed that ACP might encourage human interaction. Others felt that candid discussions were crucial, particularly for discussing life-prolonging treatment and resuscitation with older persons: I know a lot of elderly people. . . and they’ve turned around and went, ‘Oh if I go, I go, don’t resuscitate me, if anything I’m just a drain on the NHS, I’ve lived my life’. Then again, I know on the other hand there are so many other relatives who would be like, ‘No, keep me alive, I want to be alive’ so I think you really need to have these discussions. (Miss B)
Carers recognised that despite the adversities of life and challenges facing the health and social care service, ACP could provide opportunities to support individuals holistically in later life, boosting their well-being and quality of life through promoting person-centred care.
Theme 3: enabling the process – ‘when you do it properly’
Carers identified the need for ACP to be practically enabled as a process by a wider supportive network, which allowed for diligent management of information. Enabling the process of ACP as a theme was conceptually linked to supporting the older person in their needs and a means to manage working with uncertainty. Carers rooted ACP within an enabling societal network from the closer ties of family to team working with health and social care professionals, to the awareness of influence of media, legal frameworks and society as a whole.
Some participants emphasised the primacy of family in ACP, including discussions regarding prognosis and resuscitation status. Mrs A stated that the whole family should be involved when discussing resuscitation to prevent communication breakdown: The whole family is put in the picture. I think that’s really important because there could be a breakdown in communication, especially when the whole family is involved in the care. (Mrs A)
The partnership between an older person and a professional, such as a doctor or nurse specialist, to assist with ACP was also emphasised: Certainly, the GP should have insight into what’s going on because that way there can be intervention if there is anything that needs to be done. (Mrs J)
ACP was also viewed within the context of a supportive multi-professional team by carers, with individual professionals providing unique expertise: When you do it properly, you need to have all these little pieces to put them together to make a good care plan, and you need them properly from all the different people, they’ve got different experience and different things, different brain. (Miss Natalie)
Carers valued good medical record keeping and sensitively handling information within an advance care plan. This included an awareness of how information may be perceived by lay people and creating a secure record for use by health and social care professionals. Carers felt that ACP should be limited to focus on direct care thereby avoiding information overload: Too many questions, I think. It needs to be very, very specific. (Mrs A)
Participants described confusion in care planning jargon as an obstacle to ACP, with some lacking awareness of the definitions of living will or power of attorney. For example, one carer, for whom English was not their first language, felt that the CMC leaflet was difficult to read: It’s not very inviting, you know, you have to take it home if you have time and read it carefully and then discuss it. . . What’s this?. . . Too much text. (Mrs Zofia)
Carers described that the ability to update care plans was essential; some participants felt that digitalising plans would enable them to be contemporaneous. While updating was important for safety (e.g. to communicate information relevant in an emergency to carers), several carers emphasised that updated care plans were required to provide care consistent with the needs of the older person which may change over time: That’s a really difficult one, it really is, because sometimes people may say, ‘Oh, yes, resuscitate’, but as an illness progresses, they may change their opinions and views. (Mrs J)
Carers described one of the benefits of digital care plans for healthcare professionals as providing instant access to key information to healthcare professionals in acute healthcare. Mrs A supported CMC because they believed that it prevented communication breakdown between professionals: Because it keeps everyone in the picture. And I think for me, I would be quite happy knowing that different people who are accessing my father’s wellbeing have got access to that. (Mrs A)
However, digitalisation of advance care plans was sometimes viewed as being a risk to information security and some feared it may lead to digital exclusion of older adults: That’s not going to work, I don’t think. . . not everyone is computer-literature. (Mrs A)
In summary, carers identified the support of a collaborative network and careful handling of information within advance care plans as key to enabling the process of ACP, potentially overcoming some of the practical challenges within current health and social care systems.
Discussion
Participants in this study are experts in care and advocates through their active caring role, bringing first-hand experience of health systems across different settings. This analysis suggests that there was a level of uncertainty as to whether the benefits of ACP could be translated into real-world settings. This was influenced by the unpredictability of the future and multiple pressures facing health and social care systems hindering the actualisation of advance care plans. Carers highlighted that ACP can have an empowering effect on older adults, through advocacy, promoting self-determination, personalised care and improving the quality of life. However, for ACP to be enabled, carers believed that a coordinated team approach and diligent management of information were critical. These themes demonstrate the equipoise between the carer’s positive beliefs that ACP can support their role as carers and the scepticism as to whether it can truly work in the context of current health and social care infrastructures.
The carers demonstrated an awareness of the uncertainties that may negatively impact ACP, both through health and social care systems and the inherent uncertainties of life. The strong emphasis on setbacks in health and social services and how this may impact on the quality of care supports evidence from the literature on the perceived barriers to ACP (Risk et al., 2019), including limited consultation time and lack of continuity in healthcare (Howard et al., 2018). Carers described the potential problems associated with the implementation of ACP, in a similar way to frontline clinicians (Lewis et al., 2016). Carers were also cognisant of the uncertainties of planning for the future, since it was unpredictable, supportive of studies reflecting on the practical challenges of supporting those with an uncertain prognosis (Sharp et al., 2018), including in the hospital environment (Bristowe et al., 2015; Koffman et al., 2019) and the personal psychological ramifications of coping with uncertainty during serious illness (Carlson, 2016; Pietilä et al., 2018).
The carers’ beliefs that ACP can support older persons in later life are consistent with a wider body of literature demonstrating the potential benefits. For example, ACP with end-of-life care planning has been shown to improve patient satisfaction, self-determination and autonomy in end-of-life care, in addition to benefiting the psychological well-being of their relatives (Detering et al., 2010). Other studies have highlighted the improved quality of end-of-life care with ACP (Bischoff et al., 2013) and improved shared decision-making (Brinkman-Stoppelenburg et al., 2014). The personal accounts of carers in this study support the notion of ACP valuing individualised information and improving the day-to-day life valued by patients and carers, supporting the national drive for person-centred care in the NHS (Redding, 2013). The enthusiasm the carers display for preserving the identity of older persons and recognising their individual emotional and psychological needs also supports the overarching recommendation for ACP to help individuals to achieve their life goals and preferences at any stage of health (Rietjens et al., 2017).
Drawing upon their first-hand experiences, carers expressed the need to enable the process of ACP, through appropriate management of information and teamwork. This reflection may have been further stimulated within the interview by their reading of the leaflet describing CMC (EPaCCS), which explained the potential benefits of sharing information within care plans with multiple health and social care professionals across different care boundaries. The carers’ accounts reflect on the benefits of an interdisciplinary approach to ACP, which is investigated in several studies and consistent with the EPaCCS literature, regarding improving the transfer of information through electronic healthcare records (Petrova et al., 2018) and the wider national narrative regarding the drive towards achieving a ‘paperless NHS’ (Macaulay, 2016). There was also concern for the management of information, in the wake of the well-publicised NHS cyber attack of 2017 and heightened awareness of data security issues of information technology systems (O’Dowd, 2017).
This study contributes previously unheard views of ACP from carers who have experienced an emergency hospitalisation of person they care for. Both patients and carers were involved in the co-design of the semi-structured interview topic guide (Bielinska et al., 2017a) to facilitate the careful exploration of a sensitive issue (Borgstrom and Barclay, 2019). A further merit of the study is that the patients who nominated carers for interview were subsequently admitted through the emergency department to both medical and surgical specialties and not excluded on the basis of any diagnosis, making the findings relevant to a broad population. However, limitations should be recognised, since the study under-represents the views and experiences of carers of those affected by dementia, as patients needed full mental capacity to nominate a carer for interview. While this study provides in-depth insight into carers’ experiences, it would be useful to expand the research by collecting data from a wider group of caregivers, potentially through a questionnaire. The participants were interviewed by a researcher who was also a hospital doctor outside their usual care team, which may have influenced responses biasing a more medicalised view of ACP. In addition, the time-pressured environment of acute hospital environment may have limited the depth of interviews. Three carers did not complete the CBI questionnaire because they perceived it to be too burdensome to complete at the time of the study.
From the analysis, several recommendations for ACP strategies arise for both clinicians and commissioners. ACP should be normalised and embedded in healthcare and society. Carers question whether the current healthcare processes and infrastructures would allow advance care plans to be adequately actualised to meet the needs of older adults. Therefore, the implementation of ACP should continue to be a high priority in health services and research (James Lind Alliance, 2015; Marie Curie, 2018). Furthermore, ACP would likely benefit from robust information systems to support health and social care staff to have meaningful ACP discussions with older persons and their carers (O’Riordan et al., 2019) and update and share care plans across healthcare settings (Petrova et al., 2018). Further research into co-designing an approach to facilitate ACP in later life for carers and healthcare professionals would contribute to a better understanding of how to initiate and re-visit ACP discussions in a manner which is acceptable to older persons and carers, overcoming barriers and scepticism (Borgstrom and Barclay, 2019).
Conclusion
Encouragingly, ACP is positively viewed by carers of older persons as helping to support individuals’ self-determination, daily life and emotional well-being, in addition to empowering those caring for them in their role. However, there is a duality between the perceived beneficial role of ACP and their belief as to whether it will work due to challenges facing it: navigating pressures in health and social care, the existential problem coping with uncertainties in older age and chronic disease and creating reliable information and staffing systems that would enable future planning. As such, to develop, implement and sustain ACP for older persons, the social and operational aspects must be considered simultaneously.
Footnotes
Author contributions
A-M.B., S.A., J.R. and C.U. contributed to the study design. A-M.B. wrote the article, under supervision from S.A. and C.U. All authors contributed to interpretation, further revisions and to the final draft.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: J.R. is the clinical lead for ‘Coordinate My Care’.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Department of Surgery and Cancer receives infrastructural support from the Imperial NIHR Biomedical Research Centre (BRC).