
Abstract
Applying the Common Sense Model, this cross-sectional study examines associations between illness perceptions and quality of life and the mediating role of coping in 243 adults with alopecia areata, a chronic dermatological condition. At least some QoL impairment was reported by 84 percent of participants, with 31 percent reporting very to extremely large impairment. Stronger perceptions of consequences, emotional representations, identity, and lower attribution to chance were related to more impairment, with avoidant coping acting as (partial) mediator. Illness perceptions and avoidant coping seem to play an important role in QoL and are relevant intervention targets in alopecia areata.
Introduction
Alopecia areata (AA) is a chronic dermatological condition that is characterized by sudden and unpredictable hair loss, ranging from minor patches to loss of all scalp and body hair. About 2 percent of the population is affected by this condition. No clear cause or effective treatment is currently available. Although AA is medically a benign condition, due to accompanying appearance changes, persons often experience a lowered self-esteem, self-confidence, and heightened self-consciousness (Hunt and McHale, 2005), which negatively impacts their social lives (Dubois et al., 2010). Even though most people with AA hide their condition (e.g. wear a wig), they often do experience disease-related distress (Wiggins et al., 2014). Specifically, higher anxiety and depression levels (Sellami et al., 2014) and more social life disturbances (Dubois et al., 2010) have been found compared to persons without hair loss. As such, particularly the psychosocial quality-of-life (QoL) aspects, generally consisting of emotional well-being (e.g. negative mood) and social functioning (e.g. social support), seem adversely affected in AA (e.g. Tucker, 2009). Thus far, there is limited insight into the variables associated with QoL in this group (Cartwright et al., 2009). Based on the Common Sense Model (CSM) of Self-Regulation of health and illness (Leventhal et al., 2001), this study aims to examine the role of illness perceptions and coping in relation to QoL, in order to provide further direction for interventions to improve QoL in persons with AA.
According to the CSM, health outcomes of patients with chronic conditions are influenced by their cognitive and emotional illness perceptions. These enable patients to make sense of their symptoms and may impact on health outcomes directly or through their influence on coping actions (Leventhal et al., 2001). Illness perceptions reveal persons’ implicit illness representations, derived from multiple sources such as medical advice, bodily sensations, and others’ reactions (Henderson et al., 2009). Distinguished are beliefs about identity (the description or view of symptoms involved with having the condition), timeline (how long the person believes the condition will last), consequences (the expected effects and outcome of the condition), control (the amount of control the patient feels he/she has over the illness and the extent to which he/she considers the medical treatment to help), coherence (the extent to which the person has a clear understanding of the condition), and cause (personal ideas about the cause of the condition). Additionally, two emotional components include the degree of concern (level of concern experienced regarding the condition) and emotional representation (personal perception of the influence the condition has on experiencing emotions such as fear and anger) (Broadbent et al., 2006).
Illness perceptions have shown to play a predictive role in health outcomes in many illnesses (e.g. Hagger and Orbell, 2003). Only limited research has been conducted in dermatological conditions that show similarity in the visibility of the signs and symptoms, chronicity, and unpredictable nature, being contact dermatitis, atopic dermatitis, and psoriasis. Studies in these populations have shown similar associations as in other illnesses, with stronger identity perceptions, perceiving a longer timeline, and a stronger perception of the disease as having negative consequences being mostly associated with more psychological distress and stronger controllability/curability beliefs with better psychological well-being (Benyamini et al., 2012; Hagger and Orbell, 2003; Scharloo et al., 2000; Wittkowski et al., 2007). In the single study on illness perceptions in alopecia, beliefs about more serious consequences, strong emotional representations regarding the perceived influence on well-being, and stronger identity perceptions were cross-sectionally related to poorer QoL (Cartwright et al., 2009). Causal attributions were not significantly related to QoL in this study, but strong beliefs of blaming oneself for developing a condition were related to psychological distress in other dermatological samples (Fortune et al., 2000; Wittkowski et al., 2007).
In the CSM, illness representations are assumed to guide individual’s coping actions and impact on QoL (partly) through that route (Leventhal et al., 2001). With regard to coping, three main dimensions are distinguished: avoidant (e.g. self-blame), problem-focused (e.g. planning), and active emotional coping (e.g. humor) (Lazarus and Folkman, 1984). Across illnesses, more avoidant coping is generally considered to be maladaptive and problem-focused coping adaptive in terms of psychological health (e.g. Hesselink et al., 2004; Lazarus and Folkman, 1984). Yet, illness characteristics and perceptions may determine how a coping strategy is related to QoL. In uncontrollable conditions, such as AA, both avoidant and problem-focused coping were associated with impaired QoL (Cartwright et al., 2009), while in conditions with more (perceived) control options, problem-focused coping was related to good QoL (e.g. Lazarus and Folkman, 1984). The adaptiveness of emotion-focused coping strategies is unclear; a lack of controllability could increase a focus on the health threat, subsequently creating anxiety (Bolger, 1990), which could be dealt with by emotion-focused strategies. An association between emotion-focused coping and better psychological functioning was found in psoriasis (Hill and Kennedy, 2002), but not in alopecia (Cartwright et al., 2009).
In various populations, illness perceptions were found to be associated with coping. For example, more personal control perceptions have been related to adaptive coping and perceiving more consequences to maladaptive coping (e.g. Hallas et al., 2011). Also, support has been found for the postulated mediating role of coping between illness perceptions and health outcomes. For instance, the association between more negative illness perceptions and poorer QoL was mediated by emotional coping in people with hepatocellular carcinoma (Fan et al., 2013). Also, avoidant coping partly mediated the relation between a stronger illness identity and psychiatric morbidity in women with rheumatoid arthritis (Carlisle et al., 2005). However, some studies failed to support the mediating role of coping (e.g. Graham et al., 2014).
Since research on the role of illness perceptions and the mediating role of coping is limited in dermatological conditions, and non-existent in AA, this study aims to examine the associations between illness perceptions and QoL and to explore the mediating role of coping in this association in persons with AA. It was hypothesized that more negative illness perceptions (perceiving AA with a greater identity, longer duration, more consequences, more negative emotional representations, and more internal causal attributions) will be related to lower QoL and more positive illness perceptions (perceiving AA as a controllable condition and understanding the condition) with better QoL. Given the uncontrollability of AA, avoidant and problem-focused coping were hypothesized to be related to worse QoL and emotion-focused coping to better QoL. Finally, coping was hypothesized to (partially) mediate the association between illness perceptions and QoL.
Method
Participants and procedure
An (English or Dutch) online survey on QoL and its potential determinants was completed by 243 persons with AA. Inclusion criteria were being ≥16 years and reporting to be diagnosed with AA by a dermatologist or general practitioner. Participants were recruited through a link on social media pages/websites of (inter)national alopecia support groups and gave informed consent. The study was approved by the Ethics Committee Psychology of the Faculty of Social and Behavioural Sciences of Leiden University.
Of 351 people starting the survey, 243 (69%) completed the questionnaires included in this article. Dropouts and completers did not differ significantly with regard to gender, QoL, AA duration, and AA clinical severity. The final sample includes participants from 25 countries, with the most prevalent countries of residence being the United States (N = 60), United Kingdom (N = 60), The Netherlands (N = 38), Canada (N = 28), and Australia (N = 15).
Measures
QoL
The Dermatology Life Quality Index (DLQI) is a QoL measure for persons with a dermatological condition, consisting of 10 items on daily activities, symptoms and feelings, leisure, work/school, treatment, and personal relationships (Finlay and Khan, 1994). An example item is Over the last week, how much has your skin (replace by “alopecia” for this study) affected any social or leisure activities? In this study, the word “skin” was replaced by “alopecia.” The items are scored using a 4-point Likert scale (from 0—not at all/not relevant to 3—very much). The effect of AA on QoL was categorized into five categories, from no effect (0–1) to an extremely large effect (21–30; Hongbo et al., 2005). Internal consistency was high in this sample (Cronbach’s alpha = .87).
Illness perceptions
The eight-item Brief Illness Perception Questionnaire (Brief-IPQ), measures eight cognitive and emotional representation dimensions regarding one’s condition: consequences, timeline, personal control, treatment control, identity, coherence (understanding), emotional representation, and concern. Items are scored on a Likert scale from 0 to 10. Conforming to earlier studies, “your illness” was replaced with the disease/condition (“alopecia areata”). Higher scores on the dimensions personal control, treatment control, and coherence indicate more positive illness perceptions; for the other dimensions, higher scores indicate more negative illness perceptions (Broadbent et al., 2006).
To study the illness dimension Cause, an item from the original IPQ with 16 possible causes of the condition from the patient’s perspective was included (Moss-Morris et al., 2002). The participants indicated the extent to which they (dis)agree that these are causes for their AA, using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Principal component analysis (PCA) with Varimax rotation on the 16 causes led to removal of four items that loaded ≤.45, leaving three factors with eigenvalues above 1.0, explaining 61.7 percent of the variance: (1) internal causes (eight causes, e.g. family problems or worries, own behavior; α = .89), (2) external causes/immunity (three causes, germ/virus, pollution/environment, and altered immunity; α = .74), and (3) chance/bad luck (1 item).
Coping strategies
The Brief-COPE covers 14 coping dimensions, each assessed by two items (Cartwright et al., 2009; Carver, 1997) and was introduced asking participants how they coped with stress since their AA diagnosis. Items were scored on a 4-point Likert scale (from 1—“I have not been doing this at all” to 4—“I have been doing this a lot”). Based on previous research (Cartwright et al., 2009), three main coping strategies were distinguished: problem-focused (including active coping, planning, religion, and instrumental support), active emotional coping (including venting, positive reframing, emotional support, humor, and acceptance), and avoidant coping (including self-distraction, denial, behavioral engagement, self-blame, and substance use). Cronbach’s alphas varied between .80 and .82.
Demographic/clinical data
Questions were included about (1) demographics: gender, age, living situation, work situation, and country of residence and (2) duration and perceived clinical characteristics of AA: first onset, percentage of hair loss, periods of remission, stability, texture–color change, and perceived severity. The extent of AA was measured according to Olsen et al.’s (1999) investigational guidelines. As loss of eyebrows and/or eyelashes combined with hair loss on the scalp can be seen as progression of the condition, this was added to the general category of scalp. The severity of the condition was rated as extensive (>50% hair loss), moderate (20%–50% hair loss), or mild (<20% hair loss).
Statistical analysis
Scale scores were normally distributed with the exception of timeline (kurtosis = 5.16). To examine the relationship between illness perceptions and QoL, and the mediating role of coping in the illness perceptions–QoL association, a series of regression analyses were conducted. Mediation was tested by the following steps: (1) the illness perceptions (predictor) are significantly related to QoL (outcome), (2) the illness perceptions are significantly related to coping (mediator), (3) coping is significantly related to QoL, controlling for illness perceptions, and (4) the relation between illness perceptions and QoL is significantly reduced after the inclusion of coping as a predictor. In all regressions, demographic/clinical characteristics that were significantly related to both predictor(s) and outcome were controlled. The data were analyzed using SPSS (version 22.0; IBM Corp., 2013). The significance of the indirect effect of illness perceptions on QoL through coping was determined by the Sobel test and by a bootstrapping method, using the program MEDIATE for SPSS (Preacher and Hayes, 2004).
Results
Demographic and clinical characteristics in relation to QoL
Participants were mostly female (89%) and living together with a partner, family, or friend(s) (83%); had a mean age of 37.9 years (standard deviation (SD) = 13.0 years); and were employed (69%). Average disease duration was 15.3 years (SD = 12.9 years), with 68 and 53 percent reporting >50 percent hair loss of the scalp and eyebrows/eyelashes, respectively. No significant QoL differences were found between men and women (p = .33), living alone versus together (p = .34), and different amounts of hair loss (p = .10). More QoL impairment was found in participants not working (t(241) = −3.59, p < .001), being younger (r = −.19, p = .002), and with a shorter AA duration (r = −.14, p =. 03).
Using cutoff scores for the DLQI indicated that 84 percent of the sample had at least some QoL impairment, with 29 percent (n = 71) reporting a small effect, 24 percent (n = 58) a moderate effect, 26 percent (n = 62) a very large effect, and 5 percent (n = 13) an extremely large effect. The remaining 15 percent (n = 37) reported no effect of alopecia on QoL.
Associations between illness perceptions and QoL
Descriptive characteristics and zero-order correlations of QoL, illness perceptions, and coping are presented in Table 1. The high mean and limited variance in the illness perceptions dimension timeline indicates that most persons considered their AA to be chronic. More QoL impairment was related to beliefs about AA having more consequences, a stronger illness identity, more concern about AA, higher scores on emotional representations (all p values < .001), experiencing less personal control (p = .003), and less coherence (p = .002). Illness perceptions regarding timeline and treatment control were unrelated to QoL. More QoL impairment was associated with attributing AA to external and internal causes (p values < .001), but not to chance/bad luck (p = .73).
Means (M), standard deviations (SDs), and Pearson correlation coefficients for quality of life (QoL), illness perceptions (IP), and coping strategies.
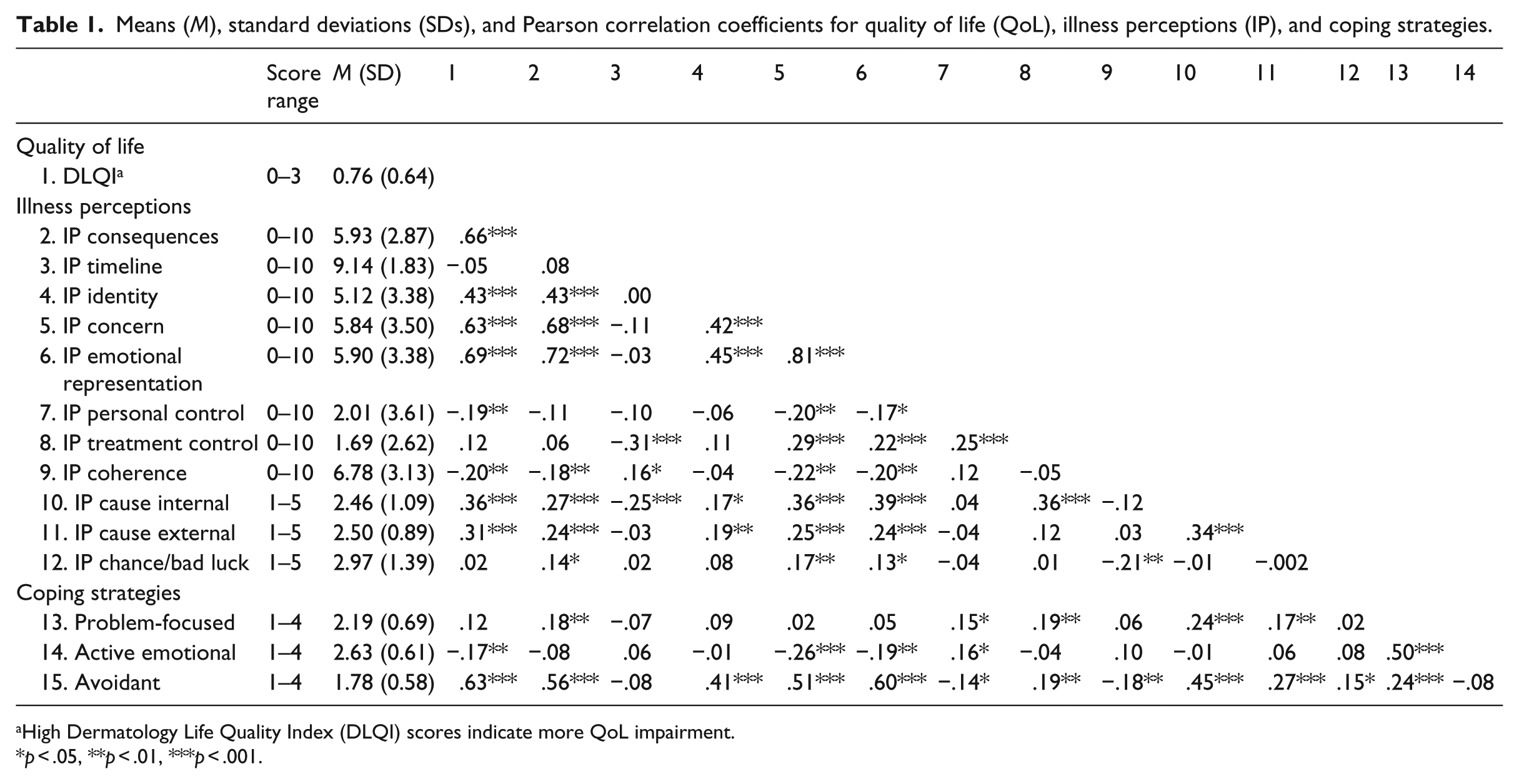
High Dermatology Life Quality Index (DLQI) scores indicate more QoL impairment.
p < .05, **p < .01, ***p < .001.
The relative contribution of illness perceptions on QoL is reported in Table 2. After controlling for demographic/clinical characteristics that were significantly related to both predictor(s) and outcome (i.e. age, work situation, and AA duration), the illness perceptions accounted for a significant 49.7 percent additional explained variance in QoL. More QoL impairment was predicted by higher perceived AA consequences (p < .001), more emotional representations (p = .004), a stronger illness identity (p = .04), and attributing AA to a lesser extent to chance or bad luck (p = .04). Because the correlation between chance/bad luck attribution and QoL was non-significant, this suppressor effect was further examined: at higher levels of concern, bad luck/chance attribution was associated with lower QoL impairment, whereas at low concern, no significant association was found.
Results regression analyses on the relationship between illness perceptions, coping strategies, and quality of life, examining the mediating role of coping strategies. Controlled for age, work status, and alopecia areata (AA) duration (results not reported).
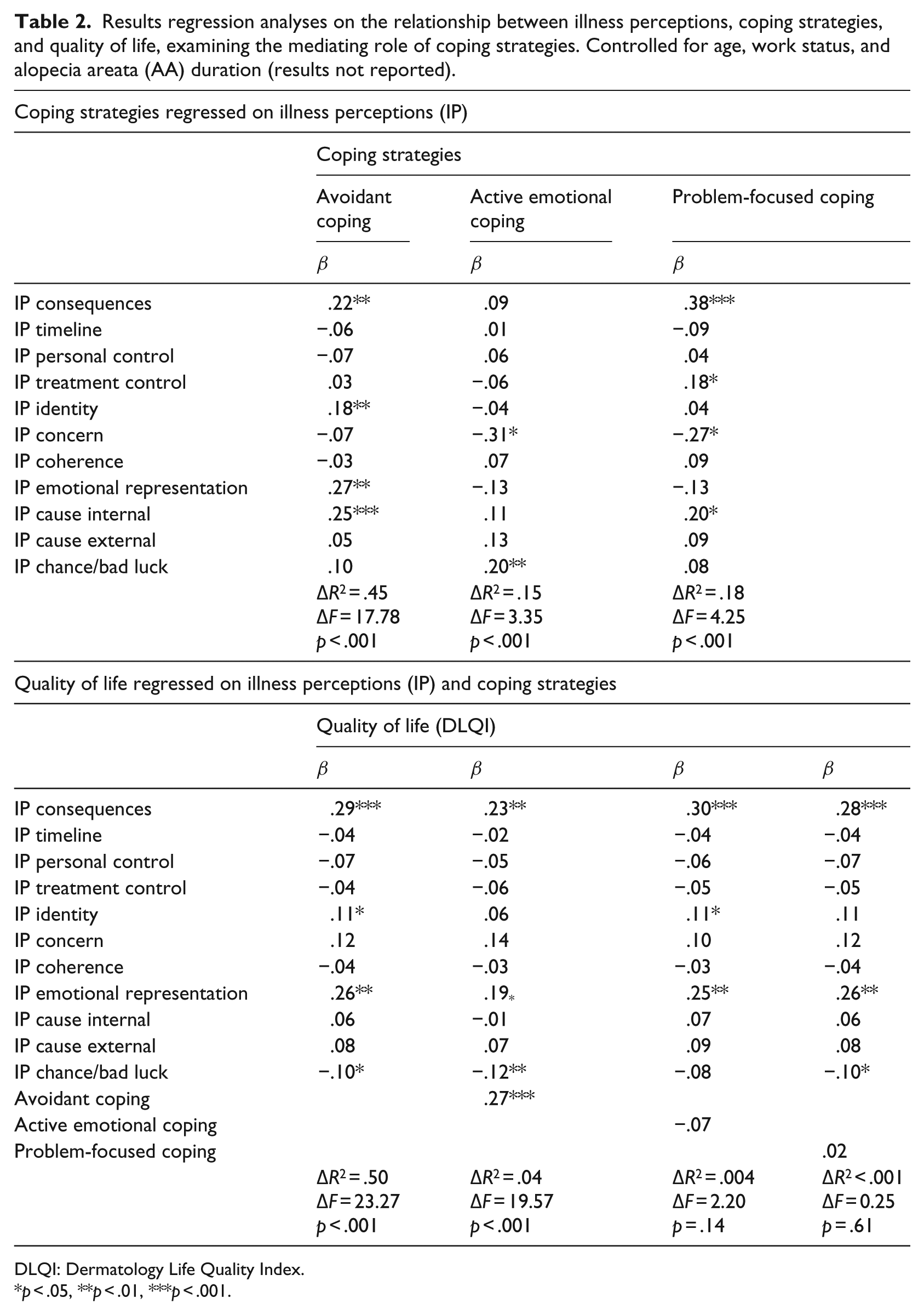
DLQI: Dermatology Life Quality Index.
p < .05, **p < .01, ***p < .001.
The mediating role of coping in the illness perceptions—QoL association
Univariately (see Table 1), more avoidant coping (p < .001) and less active emotional coping (p = .007) were associated with more QoL impairment, whereas problem-focused coping was unrelated. All illness perceptions, except timeline, were significantly related to at least one coping strategy.
To examine the direct and mediating effect of coping, first, the relative contribution of illness perceptions on coping, after controlling for age, work situation, and AA duration, was assessed (see Table 2). Together, the illness perceptions significantly explained 45.3 percent of the variance in avoidant coping, 18 percent in problem-focused coping, and 15 percent in active emotional coping. More emotional AA representations (p = .006), more perceived consequences (p = .006), a stronger illness identity (p = .002), and perceiving internal causes (p < .001) were predictive of more avoidant coping. Lower concern (p = .01) and stronger attribution of AA to chance/bad luck (p = .004) were predictive of more active emotional coping. Finally, experiencing more AA consequences (p < .001), lower concern (p = .02), higher perceived treatment control (p = .02), and stronger attribution of AA to internal causes (p = .01) were predictive of more problem-focused coping.
Regressing QoL on both illness perceptions and coping, controlling for demographic and clinical AA variables (Table 2), showed that only avoidant coping significantly predicted QoL beyond the illness perceptions (p < .001), accounting for an additional 3.5 percent of the variance in QoL. The illness perceptions consequences, emotional representations, and the causal chance/bad luck attribution remained significant QoL predictors, indicating no full mediation by avoidant coping. Identity was no longer significant, suggesting a full mediating effect. The Sobel test confirmed avoidant coping as a significant mediator in the association of consequences (z = 3.63, p < .001), emotional representations (z = 3.71, p = .001), chance/bad luck attribution (z = 3.05, p = .001), and identity (z = 2.77, p < .001) with QoL, which were all confirmed using a bootstrapping method (consequences: bootstrapped point estimate = 0.0126 (standard error (SE) = 0.0054), 95% confidence interval (CI) lower–upper = 0.0042–0.0263; emotional representations: estimate = 0.0137 (SE = 0.0064), 95% CI lower–upper = 0.0042–0.0300; bad luck/chance attribution: estimate = 0.0120 (SE = 0.0067), 95% CI lower–upper = 0.0014–0.0287; identity: estimate = 0.0094 (SE = 0.0038), 95% CI lower–upper = 0.0035–0.0188). This analysis also indicated a significant indirect effect of internal causal attribution (estimate = 0.0441 (SE = 0.0158), 95% CI lower–upper = 0.0193–0.0830) on QoL through avoidant coping.
Discussion
This study, including a large sample of people with AA, confirmed the previously found QoL impairment in persons with alopecia (e.g. Tucker, 2009). In the current sample, 84 percent experienced at least some QoL impairment and 31 percent experienced a very or extremely large QoL impairment. These percentages are comparable to, or even higher than, QoL impairments of persons with visible vitiligo and psoriasis (Chung et al., 2014; Ingordo et al., 2013). The main findings of this study are that both illness perceptions and coping strategies are associated with QoL outcomes among AA persons and that avoidant coping (partially) mediates the association between illness perceptions and QoL.
With the exception of timeline and treatment control, all illness perceptions were univariately related to QoL. Controlling for relevant demographic and clinical characteristics, especially the illness perceptions, consequences, identity, and emotional representations were found to be important for QoL in AA. These results are in line with the previous alopecia study in which the same illness perceptions were related to QoL (Cartwright et al., 2009). Also in samples of people with other chronic conditions, identity and consequences have been associated with psychological distress (e.g. Benyamini et al., 2012; Hagger and Orbell, 2003; Scharloo et al., 2000; Wittkowski et al., 2007). The illness cognition of emotional representations has been examined less often than the other illness perceptions, simply due to the fact that this illness perception was more recently added to the questionnaire (Moss-Morris et al., 2002). However, the results for emotional representation found are in line with previous studies showing that a chronic condition affects the experience of negative emotions (e.g. anger, anxiety, and depression) and thus contributes to impaired psychosocial QoL (Cartwright et al., 2009).
Regarding causal attributions, attributing the condition to chance or bad luck was found to be predictive of less QoL impairment, especially among persons with a high score on concern. An explanation could be that ascribing a condition to chance or bad luck which not only eliminates possible feelings of regret, frustration, or sorrow of past actions that might have caused the condition but also eliminates thinking of having to make lifestyle adjustments. Thus, when attributing AA to chance or bad luck, worrying about past actions that might have caused the condition or overthinking present and future actions that might control the condition, seem irrelevant. The finding that chance attributions, which were reported by 45 percent of the sample, were related to QoL could indicate an AA-specific relevant causal attribution, since this has not been found in other dermatological conditions, such as eczema (e.g. Wittkowski et al., 2007). However, more research is needed to elucidate this issue.
To summarize the findings on illness perceptions, the dimensions consequences, identity, emotional representations, and causal attribution to chance/bad luck have been identified as relevant predictors of QoL in AA and consequently seem to be an important intervention target to improve QoL in people with this condition.
Of the coping strategies examined, only avoidant coping was predictive of QoL beyond the effect of illness perceptions. The finding that avoidant coping was related to worse QoL is consistent with previous studies in (chronic) disease populations (e.g. Hesselink et al., 2004). It might be explained by the finding of thought suppression increasing frequency of these thoughts and associated moods (Wenzlaff et al., 1991). Active emotional coping was significantly correlated with QoL, in line with the notion that it would be a beneficial coping strategy given the uncontrollability of the condition of AA. However, its lack of predictive value beyond the effect of illness perceptions suggests that this coping strategy need not be the primary aim of interventions to improve QoL in AA. Also, problem-focused coping was not related to QoL in our sample, in contrast to the single previous study on QoL in alopecia that found that more problem-focused coping was related to poorer QoL (Cartwright et al., 2009). However, it is in line with research indicating that in conditions that cannot be brought under control by treatment or personal behavioral changes, problem-focused coping may not be effective (Affleck et al., 1987; Hagger and Orbell, 2003). Thus, mainly avoidant coping seems to be of relevance for impaired QoL in people with AA, warranting further investigation into this association.
According to the Common Sense Model, illness perceptions may determine how people cope with a condition, which consequently can improve or worsen psychological health outcomes (Leventhal et al., 2001). With regard to avoidance coping, this hypothesized mediation effect was found. Labeling AA as a condition with a greater identity, perceiving more consequences, reporting more emotional representations, and attributing AA less to chance/bad luck predicted poorer QoL, partially or totally (for identity) through increased use of adverse avoidant coping strategies. Furthermore, even though attributing AA to internal causes was not directly related to QoL, it seemed to exert an indirect effect through avoidant coping. This provides theoretical insight into the specific pathway through which illness perceptions impact on QoL in people with AA and provides indications on where to intervene on to improve QoL of people with AA.
Although longitudinal studies are needed to confirm causality, current results suggest some practical implications for QoL interventions in AA populations. First, education about the role of negative illness perceptions (e.g. stronger identity and more emotional representations) and avoidant coping strategies (e.g. denial, self-distraction, and self-blame) for QoL could be provided to persons with AA and relevant health-care professionals. Second, challenging negative illness perceptions and changing them into more positive ones could be effective in reducing QoL impairment. Previous studies on cardiac and asthma patients have shown that modification of illness perceptions is feasible and leads to enhanced outcomes (e.g. Petrie et al., 2002, 2012). Also, the causal attribution of the condition deserves attention, as the findings suggest that attribution to internal causes relates to more maladaptive avoidance coping, whereas attribution to chance may exert a direct positive influence on QoL. Third, reducing the use of avoidant coping strategies (e.g. self-blame and denial) would be a final aspect to address. On one hand, changing illness perceptions could already result in a decrease in avoidant coping. On the other hand, direct interventions to reduce avoidant coping and stimulate more positive coping strategies such as positive reframing and acceptance may also help reduce QoL impairment. The feasibility and value of such an approach has been illustrated, for instance, in a recent study examining the effects of acceptance-oriented cognitive–behavioral therapy in highly distressed patients with rheumatic diseases (Vriezekolk et al., 2013).
This study has some strengths and limitations. First, based on the Common Sense Model and using valid measures, this is the first study to examine the mediating role of coping between illness perceptions and QoL in AA persons. Second, the recruitment of AA participants was performed through online support groups, which has resulted in an international and large sample, including people with AA from 25 countries. Additionally, variability of QoL scores, AA duration, age, and AA severity was large enough to be confident about having reached an adequate sample to examine the relations between illness perceptions, coping, and QoL. However, the recruitment method could have led to an overrepresentation of people who are in need for and seek support. Those who are coping well might be less likely to be members of support groups. Yet, this recruitment process could have biased the sample in another direction as well, since positive changes in well-being in support groups have been found (Kalabokes, 2011). Additionally, given the online data collection, the diagnosis of AA could not be verified. Further studies could recruit persons through medical centers and/or general practitioners to reduce these potential biases. Another limitation concerns the cross-sectional design of the study. As a consequence, causality between illness perceptions, coping, and QoL cannot be determined. Reverse or reciprocal relationships might also be plausible. A longitudinal study could provide insight into the causality and explore whether changes over time in illness perceptions and coping are related to changes in QoL.
Conclusion
This study aimed to improve understanding of the relationships between illness perceptions, coping strategies, and QoL in persons with AA, using Leventhal’s Common Sense Model. Particularly, the illness perceptions consequences, identity, emotional representations, and avoidant coping, were found to be related to QoL. The hypothesized mediating role of coping in the association between illness perceptions and QoL was partially confirmed, with perceiving AA with a greater identity (perceiving more symptoms) being fully mediated by avoidant coping in explaining poorer QoL and perceiving more consequences, reporting greater emotional representations, and attributing AA to chance/bad luck being partially mediated by avoidant coping. These findings provide indications for the development of interventions focusing on changing illness perceptions and on reducing avoidant coping in order to improve QoL in persons with this chronic condition.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.