
Abstract
The effectiveness of cognitive behaviour therapy for paediatric functional abdominal pain leaves room for improvement. We studied which factors addressed in cognitive behaviour therapy relate most strongly to the physical and psychological functioning of children with functional abdominal pain and are thus most important to target. Questionnaires were filled out by 117 children with functional abdominal pain and their parents. Multiple regression analyses showed that children’s passive coping and parental and children’s positive cognitions relate to child functioning. Negative cognitions and parental solicitous behaviour were unrelated to child functioning. Cognitive behaviour therapy for functional abdominal pain may benefit most from changing children’s passive coping and promoting positive cognitions.
Introduction
Chronic abdominal pain (AP) affects more than 10 per cent of school-aged children in Western countries (Korterink et al., 2015). Most children presenting with chronic AP suffer from ‘functional’ AP (FAP), which refers to pain that is not caused by any organic diseases. Still, FAP affects children’s quality of life just as much as organic gastrointestinal disorders like Crohn’s disease do (Varni et al., 2006). Moreover, suffering from FAP at a young age predicts continued functional gastrointestinal problems as an adult (Howell et al., 2005) and increases the risk of other functional somatic complaints and psychiatric problems in adulthood (Shelby et al., 2013). Treating these complaints successfully at an early age is therefore of utmost importance. As the aetiology of FAP is most often viewed from a biopsychosocial perspective, psychological therapies like cognitive behaviour therapy (CBT) are often recommended. A number of randomized controlled trials (RCTs) show that CBT indeed significantly reduces pain complaints (Eccleston et al., 2014). However, treatment effectiveness for CBT is usually about 60 per cent (e.g. Eccleston et al., 2014; Lackner et al., 2004; Van der Veek et al., 2013), which leaves room for improvement. To improve the effectiveness of CBT for FAP, it is necessary to critically evaluate its content. This study therefore investigates which factors targeted in CBT relate most strongly to the psychological and physical functioning of children with FAP.
CBT targets multiple potential causes or maintaining factors for FAP. It focuses on (1) teaching children to cope with their complaints, (2) teaching parents to react adequately to their children’s complaints and reduce ‘rewarding’ or solicitous reactions (e.g. no longer allowing the child to stay home from school) and (3) teaching both parents and children to reduce negative thinking patterns about the condition and think more positively about the coping potential of the child (e.g. Levy et al., 2010; Robins et al., 2005; Van der Veek et al., 2013). Previous studies showed that these cognitive and behavioural factors relate to pain intensity and/or the physical and psychological functioning of children with FAP (e.g. Compas et al., 2012; Evans et al., 2016; Langer et al., 2009; Shirkey et al., 2011; Van der Veek et al., 2012). But is it necessary that CBT focuses on all of them, or are some more important than others? During the past 5 years, studies have begun to experimentally test whether a change in these factors indeed results in positive treatment outcome (i.e. mediation of treatment effectiveness). These studies find that some hypothesized mechanisms do mediate treatment effects, whereas others do not. For example, Levy et al. (2014) found that although parental solicitousness changed after CBT, this did not relate to the changes in child pain, while the changes in negative cognitions did. Similarly, Wicksell et al. (2011) found that in acceptance and commitment therapy for paediatric chronic pain, beliefs about pain impairment and pain reactivity mediated treatment effects, but not self-efficacy or catastrophizing. This seems to suggest that when it comes to the factors addressed in CBT, some may be more important to target than others.
A straightforward first step to investigate which factors addressed in CBT may be most important to target is to simultaneously investigate the relationship between all factors that are targeted in CBT and the physical and psychological functioning of children with FAP. Up till now, many studies have been conducted on each of these factors separately, but no single study has combined them all. As such, it is unknown which factors show the strongest relation with the functioning of the child and are thus most important to target in CBT. Therefore, this study investigated which of the following factors targeted in CBT relate most strongly to the physical and psychological functioning of children with FAP: children’s coping with AP, children’s and parental negative cognitions concerning the condition, children’s and parental positive cognitions about the coping potential of the child and parental solicitous behaviour.
Method
Sample and procedure
The design of this study was cross-sectional. Children with FAP aged 7–18 years were recruited from the general paediatric and paediatric gastroenterology outpatient clinics at a university hospital. Children participated in an RCT investigating the efficacy of CBT versus medical care (Van der Veek et al., 2013). Ethical approval for this RCT was obtained from the Medical Ethical Committee of the university hospital. The data presented are derived from questionnaires children and (one of) their parents filled out before entering treatment. Children were eligible if they fulfilled Rome III criteria for FAP (Rasquin et al., 2006). Of the 201 children screened for eligibility, 117 (58.2%) fulfilled inclusion and exclusion criteria and filled out the questionnaires. For 59.8 per cent of the children, mothers filled out the questionnaires, for 4.3 per cent fathers did and for 33.3 per cent both parents filled out the questionnaires together. For three children, no parental data were available.
Instruments
Cronbach’s alpha reliability is presented in Table 2. All questionnaires were filled out by children, except the parental Pain Beliefs Questionnaire (PBQ).
Outcome measures
AP was measured using the Abdominal Pain Index (API; Walker et al., 1997). The API consists of five questions and taps on the frequency, duration and intensity of the AP the child experienced in the past 2 weeks. Two questions make use of a 6-point scale, one of a 9-point scale and another two of an 11-point scale. A total score for the API was computed by recoding each item to reflect a scale ranging from 0 to 10 and summing all items (Van der Veek et al., 2010). The API has been shown to be a reliable instrument, with a Cronbach’s alpha ranging from .80 to .93 (Walker et al., 1997).
Functional disability was measured using the Functional Disability Inventory (FDI; Walker and Greene, 1991), which consists of 15 items scored on a 5-point scale, ranging from (0) no trouble at all to (4) impossible. The scores on the items are summed to a total score, with higher scores indicating more disabilities. The FDI has been validated for children with recurrent AP with Cronbach’s alpha ranging from .86 to .91 (Claar and Walker, 2006).
Symptoms of anxiety and depression were measured using the Revised Anxiety and Depression Scale – short version (RCADS-25; Muris et al., 2002). The shortened version of the RCADS has been shown to be a valid and reliable instrument to measure symptoms of generalized anxiety disorder, separation anxiety disorder, social phobia, panic disorder and major depressive disorder (Muris et al., 2002). Each of the five scales consists of five items that are scored on a 4-point scale, ranging from (0) never to (3) always. Cronbach’s alphas of the separate scales were satisfactory in previous research (Kösters et al., 2015). For this study, the four scales of the different anxiety disorders were summed to compute one score for anxiety symptoms. A separate score was calculated for depression symptoms.
Quality of life was measured using the physical well-being subscale of the KIDSCREEN-27 (Jervaeus et al., 2013). The KIDSCREEN-27 was developed across different countries and consists of 27 items, to be scored on a 5-point Likert scale. Several items are reverse-scored. Scores for each scale are calculated using Rasch analysis and then transformed into t-values. Higher scores reflect a better quality of life. The KIDSCREEN-27 has been shown to be a reliable and valid instrument, with a Cronbach’s alpha for the physical well-being subscale of .80 and good test–retest reliability (Jervaeus et al., 2013).
Independent variables
Pain coping strategies were measured using the Pain Response Inventory (PRI; Walker et al., 1997), a 60-item questionnaire. Answers can be given on a 5-point Likert scale, with higher scores reflecting a greater use of these coping strategies. As no Dutch version was available, the PRI was translated by our research group and back-translated by a native speaker. Any discrepancies in the back-translation were discussed with the head of the research group that developed the PRI, Dr L.S. Walker. The PRI consists of three higher order scales, measuring active, passive and accommodative coping. A confirmatory factor analysis performed on data derived from a large group of school children (see Van der Veek et al., 2010, for characteristics of this sample) showed that the factor structure as described by Walker et al. fitted the data well (model-fit unweighted least squares model χ2(131) = 10405.67; p < .001; goodness of fit index (GFI) = .92; adjusted GFI (AGFI) = .91).
Children’s and parents’ negative and positive cognitions were measured using the PBQ (Walker et al., 2005). The PBQ is a 32-item questionnaire, with 20 items assessing beliefs about five specific characteristics of FAP: condition frequency, condition duration, condition seriousness, episode specific intensity and episode specific duration. The other 12 items make up the problem-focused and emotion-focused coping potential (PFCP and EFCP) scales, which measure whether children and parents believe the child can cope with their pain. Participants respond to each item of the PBQ on a 5-point Likert scale; higher scores reflect that the participant has such cognitions more often. The PBQ was translated into Dutch by the present research group, back-translated by a native speaker and any discrepancies were discussed with Dr L.S. Walker. A confirmatory factor analysis on data from the same group of Dutch school children as used for the PRI showed that the 20 items assessing cognitions about the condition could be construed under one higher order scale, but the five lower order scales could also be preserved (model-fit unweighted least squares model χ2(165) = 536.97; p < .001; GFI = .97; AGFI = .97). For this study, it was decided to use the condition seriousness scale only, as this scale incorporates the type of cognitions explicitly addressed in cognitive therapy (e.g. ‘my stomach aches mean I have a serious illness’) and the other scales show large conceptual overlap with the items included in the API. The PFCP and EFCP scales were calculated by averaging the six items of each scale.
Parental solicitous behaviour was measured using the child-reported Illness Behavior Encouragement Scale (IBES; Walker & Zeman, 1992). The IBES consists of 12 items which are answered on a 5-point scale. Higher scores reflect more parental solicitous behaviour. The IBES has been shown to be a reliable instrument, with Cronbach’s alphas of .75–.85 (Walker & Zeman, 1992).
Statistical analyses
To answer the research question, five multiple regression analyses (MRAs) were performed, one for each measure of child functioning (i.e. level of AP, functional disability, depression symptoms, anxiety symptoms and quality of life). As it has been found that younger children and girls report FAP more often (Rasquin et al., 2006), age and gender were entered as control variables in a first block in each analysis. Child variables were then entered as a second block and parent variables as a third block.
Results
Preliminary analyses
Table 1 shows descriptive statistics for every variable used in the analyses. For 21 children (17.9%), no parental PBQ data were available because this questionnaire was added to the instrument battery at a later time. The reason for the missing values in these cases was ‘missing at random’ (MAR; Rubin, 1976). For the other variables, 2.6–10.3 per cent of values were missing. Inspection of the missing value patterns did not show any signs of ‘not at random’ missing values. Therefore, we assumed all missing values to be MAR. It has been shown that in the case of MAR, it is better to impute data than do a complete-case analysis (Schafer and Graham, 2002). Therefore, we imputed the PBQ and other missing data using the multiple imputations subroutine in SPSS 18.0. All variables were used to impute the missing data five times. To calculate the mean R2 across the five imputed datasets, Harel’s method was used (Harel, 2009).
Cronbach’s alpha and descriptive statistics of all variables used in the analyses.
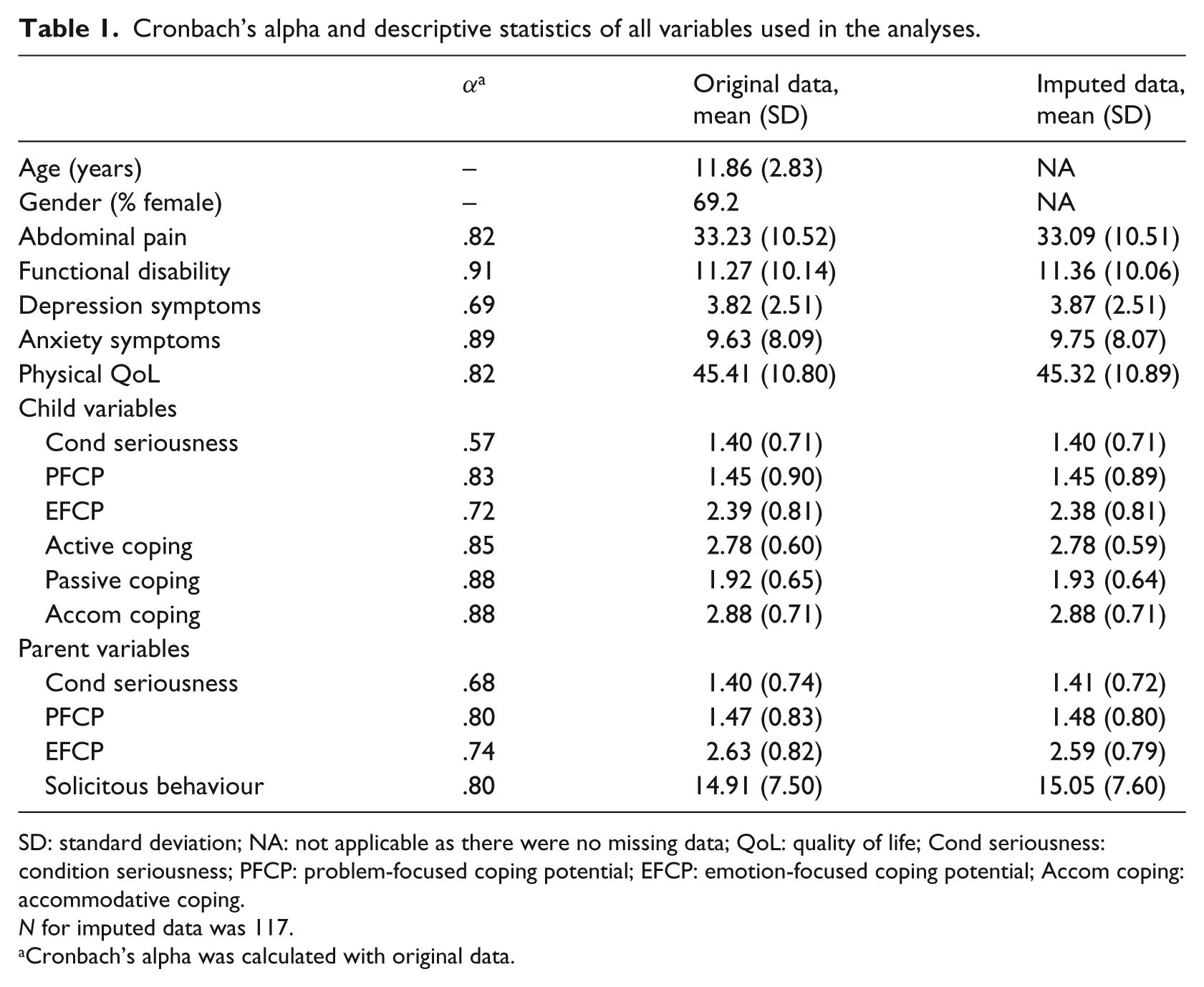
SD: standard deviation; NA: not applicable as there were no missing data; QoL: quality of life; Cond seriousness: condition seriousness; PFCP: problem-focused coping potential; EFCP: emotion-focused coping potential; Accom coping: accommodative coping.
N for imputed data was 117.
Cronbach’s alpha was calculated with original data.
Assumptions relevant to MRAs were checked (Tabachnick and Fidell, 2001). No multi-collinearity was present (see Table 2); however, scatter plots of the residuals showed heteroscedasticity for the MRAs with AP, functional disability and anxiety. Boxplots showed that these outcomes had skewed distributions. A reflected square root transformation for AP and a logarithmic transformation for functional disability and anxiety resolved both the skewed distributions and the heteroscedasticity. The MRAs for AP and functional disability also showed a multivariate outlier, which was deleted.
Pearson’s correlations between all variables used in analyses (N = 117).
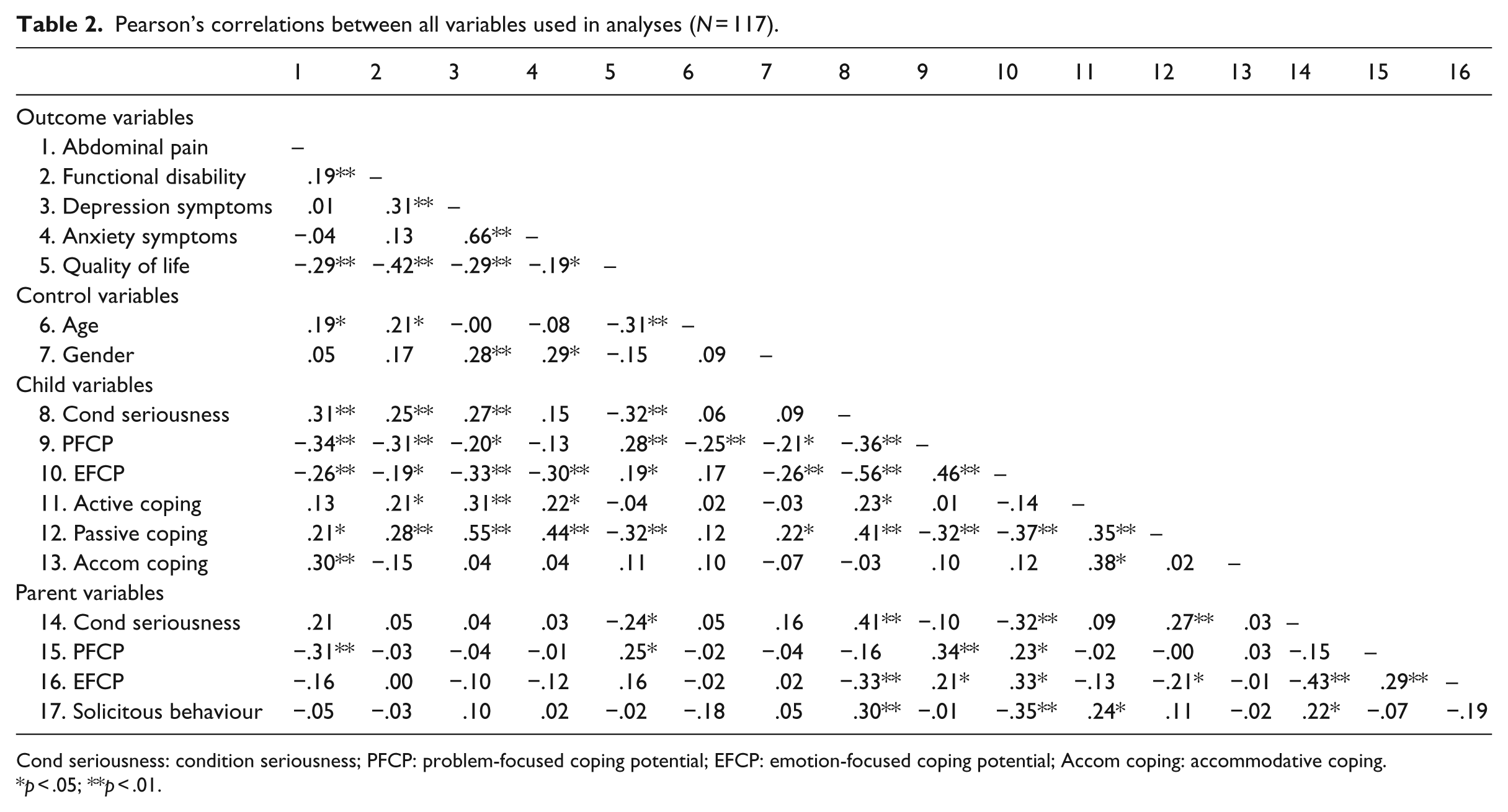
Cond seriousness: condition seriousness; PFCP: problem-focused coping potential; EFCP: emotion-focused coping potential; Accom coping: accommodative coping.
p < .05; **p < .01.
Main analyses
Table 3 shows the results of the MRAs. It should be noted that as the measure for AP was reflected for transformation purposes, a higher score on the API in the MRA means that children experienced less AP.
Hierarchical multiple regression analyses, method enter.
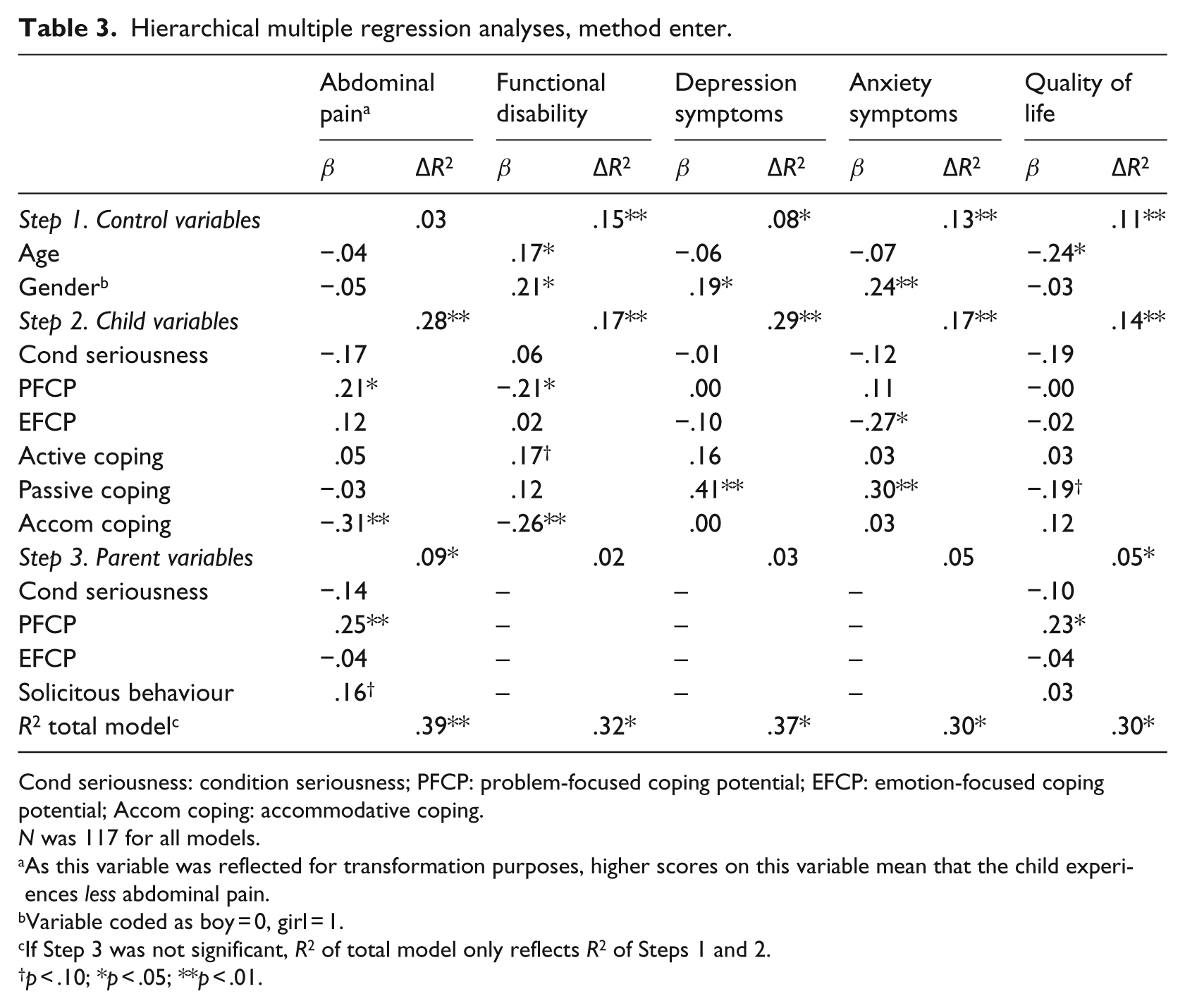
Cond seriousness: condition seriousness; PFCP: problem-focused coping potential; EFCP: emotion-focused coping potential; Accom coping: accommodative coping.
N was 117 for all models.
As this variable was reflected for transformation purposes, higher scores on this variable mean that the child experiences less abdominal pain.
Variable coded as boy = 0, girl = 1.
If Step 3 was not significant, R2 of total model only reflects R2 of Steps 1 and 2.
p < .10; *p < .05; **p < .01.
The MRAs showed that if children reported to think more positively about their PFCP, this was related to experiencing less AP, whereas using accommodative coping was related to more AP. Also, if parents thought more positively about the PFCP of their child, this was related to less pain. For functional disability, when children experienced less positive cognitions about their own PFCP and used accommodative coping less often, this was related to more disability. It should be noted, however, that there was no significant Pearson’s correlation between accommodative coping and functional disability, which signals a suppressor effect (Tabachnick and Fidell, 2001). Female gender and using passive coping more often were related to symptoms of depression and anxiety. If children had more confidence in their own EFCP, this was related to less anxiety. For quality of life, the total block of child variables added a significant percentage of variance to the model, but no single predictor reached significance. There was a trend for passive coping being related to a lower sense of quality of life. If parents were more confident about the PFCP of their children, this was related to an increased quality of life.
Discussion
This study aimed to determine which factors targeted in CBT for paediatric FAP relate most strongly to the physical and psychological functioning of children with FAP. Two specific coping strategies – passive and accommodative coping – were related to various aspects of the child’s functioning. In addition, children’s and parents’ confidence in the child’s potential to cope with their AP was related to better functioning. Finally, parental solicitous behaviour was unrelated to the physical or psychological functioning of the child. Below, the results of this study are discussed in light of their implications for psychological therapies for FAP.
Children’s coping strategies
In line with previous research (e.g. Shirkey et al., 2011; Walker et al., 2005), we found that passive coping strategies (i.e. self-isolation, catastrophizing and disengagement) were related to more symptoms of anxiety and depression. Thus, it seems important that psychological therapies like CBT continue to try and alter these counterproductive ways of coping. Also in line with these studies, active coping was not related to any of the measures of functioning of the child. Although active coping is generally considered adaptive, the findings with regard to chronically ill children are mixed (Compas et al., 2012). Active coping is usually most adaptive when applied in situations that can be controlled, which may explain the mixed findings for chronically ill children, as only some aspects of their illness (e.g. school absence) can be brought under control, whereas others cannot (e.g. feeling different from peers; Compas et al., 2012). Note, however, that as this study only investigated coping strategies spontaneously used by untreated children, these findings do not apply to the active coping strategies that are part of CBT. More experimental research is needed to ascertain which specific active coping strategies taught in CBT positively affect the physical and psychological functioning of children with FAP (Compas et al., 2012).
Accommodative coping was related to both more AP and less disability, although the latter finding may be due to a statistical suppression effect and should thus be interpreted with care (Tabachnick and Fidell, 2001). In general, the literature on accommodative coping is mixed about its effectiveness. In samples of children with chronic illness, it is usually found to be an adaptive strategy, but the literature on children with FAP shows diverse findings: from no relationship between accommodative coping and children’s well-being, to better physical and psychological functioning, to worse physical functioning (Compas et al., 2012). These differences in results may be explained by how accommodative coping is measured throughout the literature. For example, studies using the Responses to Stress Questionnaire (RSQ; Connor-Smith et al., 2000) more often find a beneficial effect for accommodative coping than studies like the present using the PRI (Walker et al., 1997). Unlike the PRI, the RSQ includes cognitive reappraisal in the accommodative coping scale, a strategy that may particularly be helpful in chronic pain (Compas et al., 2012). This study used the PRI, as this instrument was specifically designed to measure coping with FAP and is the most often used instrument in children with FAP. However, future research might do well to investigate the accommodative coping concept with other instruments like the RSQ.
Children’s and parents’ negative and positive cognitions
Although reducing negative cognitions is an important target of CBT, this study found no relation between children’s or parental negative cognitions about the seriousness of the AP and the child’s physical and psychological functioning. However, a recent experimental study showed that this variable was an important treatment mechanism of CBT for children with FAP (Levy et al., 2014). A possible explanation for this discrepant finding may be that in this study both negative and positive cognitions and coping and parental solicitous behaviour were simultaneously studied, while in the experimental study only negative cognitions and solicitous behaviour were included. Indeed, in our single Pearson’s correlations, negative cognitions were related to the child’s functioning, but relative to the other factors the concept of negative cognitions lost its significance.
In contrast, children’s and parental positive cognitions about the child’s ability to cope with his or her complaints were related to less AP, less functional disability, less anxiety and a better quality of life. Future studies should investigate whether increases in these positive cognitions relate to treatment effectiveness in CBT for children with FAP.
Parental solicitous behaviour
Finally, parental solicitous behaviour did not relate to the physical or psychological functioning of children with FAP. This held true not only in MRAs but also in single Pearson’s correlations. Although multiple empirical studies show relations between solicitous behaviour and child pain (e.g. Evans et al., 2016; Welkom et al., 2013), other studies find no relations (Langer et al., 2009; Rousseau et al., 2014). Solicitous behaviour is often described as a key element in the occurrence and maintenance of FAP (Levy, 2011); as such, most CBT protocols try to alter this behaviour. However, a recent intervention study provided preliminary experimental evidence that this actually may not be a mechanism of change for CBT. Levy et al. (2014) investigated CBT for FAP and while they were successful in reducing solicitous behaviour in parents and reducing pain in children, these changes in solicitous behaviour could not account for the reductions in pain. This study is in line with the results from Levy et al. as it shows that compared to other factors that are tackled within CBT, parental solicitousness seemed least related to child well-being. Future studies are encouraged to replicate the study by Levy et al. (2014) and sort out whether CBT should continue focusing on these explicit parental solicitous behaviours, or perhaps shift focus to other, more covert parental behaviours like nonverbal communications of concern (Dunford et al., 2014). Also, this study suggests that it does seem relevant to keep involving parents in the coping skills training for children, as this might improve parental beliefs about whether their child can cope with their pain.
Limitations and directions for future studies
This study has a number of limitations. First, all data were gathered by self-report, which may have caused some bias. Second, as the design of this study was cross-sectional, the implications the study holds for CBT are preliminary. Future experimental studies investigating mediating factors of CBT for paediatric FAP are needed to test whether the factors found in this study are indeed mechanisms of action for CBT. Finally, we would like to stress that in this study, about 30–40 per cent of the variance in physical and psychological functioning of children with FAP could be explained by the factors that are usually targeted in psychological therapies. Although this is no small amount, it also means that a considerable percentage of variance is still unaccounted for. As psychological therapies at present are still ineffective for up to 40 per cent of patients (Lackner et al., 2004), psychological therapies may benefit from targeting other factors than the ones investigated in this study, like attentional biases (Van der Veek et al., 2014) or parental (non)verbal communications of concern (Levy et al., 2014).
Conclusion
This study showed that children’s passive coping and parental and children’s positive cognitions about the ability of the child to cope with FAP relate most strongly to the physical and psychological functioning of children with FAP. By simultaneously investigating the key factors that are targeted in CBT, we were able to show which of these factors were most strongly related to the functioning of children with FAP, and thus seem most important to target during CBT. Future studies investigating mechanisms of action of CBT are necessary to show whether the factors identified in this study indeed are essential to the treatment effectiveness of CBT for paediatric FAP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dutch Digestive Foundation (SWO 05-09).