
Abstract
Background
ADHD is a prevalent neurodevelopmental disorder frequently accompanied by psychiatric comorbidities. While international evidence is well-established, data from South Africa — particularly in younger children — remain limited.
Aim
To describe psychiatric comorbidities and associated factors in children aged 7–12 years with primary ADHD at the Child, Adolescent, and Family Unit (CAFU), Charlotte Maxeke Johannesburg Academic Hospital (CMJAH).
Methods
A retrospective cross-sectional record review of children aged 7–12 years with primary ADHD at CAFU between January 2020 and December 2022. Data were analysed using SPSS version 26.
Results
Of 573 records screened, 108 were included. The combined subtype was most prevalent (72.2%). Almost all children (95.5%) had at least one comorbidity. The most frequent were generalised anxiety disorder (52.8%), intellectual disability (38.9%), and oppositional defiant disorder (29.6%). Females were more likely to present with oppositional defiant disorder (p = .007) and males with autism spectrum disorder (p = .032). High rates of domestic violence (29.6%), parental substance abuse (33.3%), and parental psychiatric history (30.6%) were documented.
Conclusion
Psychiatric comorbidities are highly prevalent in South African children with ADHD, exceeding international estimates, and reflect the broader psychosocial context of the setting. Comprehensive, multidisciplinary, and trauma-informed assessments are essential.
Plain Language Summary
Attention Deficit Hyperactivity Disorder (ADHD) is one of the most common conditions affecting children. Children with ADHD often struggle with attention, impulsivity, and hyperactivity — but many also have other mental health or developmental conditions at the same time. We wanted to find out how common this is among younger children in South Africa, where very little research on this topic has been done. We looked at the medical records of 108 children aged 7 to 12 years who were diagnosed with ADHD at Charlotte Maxeke Johannesburg Academic Hospital between 2020 and 2022. We found that almost all of the children (95%) had at least one additional condition alongside their ADHD. The most common were anxiety (found in more than half the children), intellectual disability (affecting about 4 in 10), and oppositional defiant disorder — a condition where children persistently argue, defy rules, or act angrily. Interestingly, girls were more likely to have oppositional defiant disorder, while boys were more likely to have autism, which is different from what many international studies have found. We also found that many families in our study were dealing with difficult circumstances, including domestic violence (nearly 1 in 3 families) and parental mental illness or substance use — all of which can affect a child’s mental health. These findings show that children with ADHD in South Africa are dealing with a heavy load of challenges, many of which may be missed if doctors only focus on the ADHD diagnosis. Children need thorough assessments that look at the whole picture. Schools, families, and health services all have a role to play in identifying these additional difficulties early and getting children the right support before problems become harder to treat.
Introduction
Attention Deficit Hyperactivity Disorder (ADHD) is a common neurodevelopmental disorder of childhood that frequently presents with psychiatric comorbidities. Globally, it is estimated that more than 60% of children with ADHD have at least one comorbid psychiatric condition, significantly complicating diagnosis, treatment, and long-term outcomes (Gnanavel et al., 2019; Reale et al., 2017). Despite a growing international evidence base, the psychiatric comorbidity profile of children with ADHD in sub-Saharan Africa, and specifically in South Africa, remains poorly characterised.
South Africa presents a unique and complex sociocultural context that distinguishes it from high-income countries where most ADHD research has been conducted. The country is characterised by significant socioeconomic inequality, a high burden of psychosocial adversity (including elevated rates of domestic violence, parental substance use, and poverty), and a pluralistic cultural landscape in which beliefs about mental illness vary widely across communities. Stigma towards ADHD and mental illness more broadly has been identified as a substantial barrier to help-seeking, diagnosis, and treatment adherence in South Africa (Rajcumar & Paruk, 2020; Schoeman & Voges, 2022).
A study at a specialist child psychiatry clinic in KwaZulu-Natal found that nearly a third of parents (32.9%) had consulted a traditional healer before seeking medical care for their child’s ADHD, and the majority held significant misconceptions about the disorder’s causes and treatment (Rajcumar & Paruk, 2020). This contrasts starkly with patterns in high-income countries, where parental knowledge of ADHD, while imperfect, is more often shaped by engagement with biomedical health systems and access to online health information. Similarly, while ADHD diagnosis in South Africa is further complicated by limited specialist services, unequal access to psychometric assessment, and staff shortages particularly in the public sector, countries such as the United States benefit from a well-resourced diagnostic infrastructure and robust insurance coverage for mental health services. These structural and sociocultural differences have direct implications for how ADHD and its comorbidities present and are identified in South African children.
A further distinguishing feature of the South African context is the educational system. Research indicates that the majority of children requiring special educational support in South African mainstream schools present with neurodevelopmental conditions including ADHD and learning disorders; yet formal identification and support remain inconsistent, particularly in under-resourced public schools (Stark et al., 2022). This is in contrast to countries such as the United Kingdom or Australia, where structured school-based identification pathways and learning support systems provide a more systematic safety net for children with neurodevelopmental difficulties.
Thus, this retrospective study aimed to describe psychiatric comorbidities and associated factors in children aged 7 to 12 with primary ADHD at Charlotte Maxeke Johannesburg Academic Hospital (CMJAH), Child and Adolescent Family Unit (CAFU), between January 2020 and December 2022. Understanding the psychiatric comorbidity profile of this population, within its specific sociocultural context, is critical for improving clinical practice, service planning, and policy development in South Africa.
Literature Review
Introduction
ADHD is a neurodevelopmental disorder, with significant heritability, affecting children, adolescents, and adults with symptoms typically presenting in early childhood and often persisting into adulthood (Posner et al., 2020). According to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), the condition is characterised by pervasive symptoms of inattention, hyperactivity, and impulsivity which must be present for at least 6 months before the age of 12 years with impairment in academic, occupational, or social functioning (American Psychiatric Association, 2013).
There are three distinct presentation subtypes of ADHD (American Psychiatric Association, 2013): • Predominantly inattentive subtype when symptoms of inattentiveness are present. • Predominantly hyperactive/impulsive subtype in which symptoms of hyperactivity and/or impulsivity are present. • A combined subtype is diagnosed when both criteria for inattentiveness and hyperactivity/impulsivity are met.
Prevalence
The global prevalence of ADHD is 7.6% in children aged 3 to 12 years and 5.6% in teenagers aged 12 to 18 years (Salari et al., 2023). An umbrella review of 13 meta-analyses comprising over 3.2 million participants found a pooled global prevalence of 8.0% (95% CI 6.0–10%) in children and adolescents, with boys (10%) twice as likely to be affected as girls (5%). Notably, the inattentive subtype (ADHD-I) was the most prevalent globally, followed by the hyperactive/impulsive (ADHD-HI) and combined (ADHD-C) subtypes (Ayano et al., 2023). Studies evaluating the prevalence of ADHD in African countries estimated the prevalence values to range between 5–7% (Ayano et al., 2020; Bakare, 2012; Davidovitch et al., 2017; Mphahlele et al., 2020; Mulat et al., 2021; Regnart et al., 2019; Walker, 2011). The prevalence rates in South Africa range between 8–10% according to the Attention Deficit and Hyperactivity Support Group of Southern Africa (ADHASA; Louw et al., 2009; Mahomedy et al., 2007; Meyer et al., 2004; Muthukrishna, 2013).
The prevalence of ADHD subtypes in children varies due to geographic location, diagnostic criteria, and population (Nazeer et al., 2022). A population-based study in Chile found that most children who met the criteria for ADHD could be classified in the hyperactive/impulsive subtype (de la Barra et al., 2013). However, a clinic-based study from Iran indicated that 42.7% of children with ADHD were classified in the combined subtype, 31.0% hyperactive and 26.3% inattentive (Ghanizadeh, 2009).
Sex
ADHD affects children differently depending on their sex and age (Kaplan & Sadock, 2007). It is, however, more prevalent in males than females, with a male-to-female ratio of 2:1 (American Psychiatric Association, 2013). It has been proposed that sex differences could be attributed to males presenting earlier than females (Reale et al., 2017).
Comorbidities
The bidirectional relationship between ADHD and comorbid conditions is well documented in the literature (Mulat et al., 2021; Seo et al., 2022; Shaaban et al., 2020). ADHD has been reported to present with other comorbid psychiatric disorders, contributing to the clinical heterogeneity of this condition (Jogia et al., 2022; Seo et al., 2022). It is estimated that over 60% of children with ADHD present with at least one comorbidity (Gnanavel et al., 2019; Jogia et al., 2022). Comorbidity rates vary markedly across countries and healthcare settings, influenced not only by true epidemiological differences but also by factors such as stigma, access to specialist services, diagnostic capacity, and cultural frameworks for understanding mental illness. In South Africa, where mental health stigma has been identified as a significant barrier to care (Schoeman & Voges, 2022), and where access to comprehensive psychological assessments is limited in the public sector, comorbidities may be systematically under-identified. The following section reviews comorbidities grouped by clinical theme, to facilitate integrated clinical understanding.
Neurodevelopmental Conditions
Generalised Anxiety Disorder (GAD)
International studies confirm the strong association between ADHD and GAD in children (Gümüş et al., 2015; Rimal & Pokharel, 2016; Seo et al., 2022). The presence of GAD could influence the course and treatment response of ADHD (Gnanavel et al., 2019). A study in Nepal indicated GAD as the second most common comorbidity (24.4%), while a study done in Korea indicated GAD as the third most common comorbidity (9.9%) in children and adolescents diagnosed with ADHD (Rimal & Pokharel, 2016; Seo et al., 2022). Turkish children showed a 27.6% comorbidity rate between GAD and ADHD (Gümüş et al., 2015). A Nigerian study found that GAD is more common with the inattentive subtype of ADHD in a multi-ethnic and multicultural sample (Adewuya & Famuyiwa, 2007). A local South African study conducted in Limpopo found higher rates of GAD among children with ADHD than in controls, with equal prevalence among both sexes (Mphahlele et al., 2020).
Intellectual Disability (ID)
A study in Denmark found comorbid ID in 7.9% of ADHD children and adolescents. ID was also further found to be the second most common comorbidity in ADHD children (Jensen & Steinhausen, 2015; Jogia et al., 2022).
Learning Disorders (LD)
Children diagnosed with ADHD face an elevated susceptibility to the development of LD and encounter challenges in the academic domain (Pondé et al., 2012). A systematic review demonstrated that the co-occurrence of LD in children with ADHD ranges between 27% to 31% (Doyle et al., 2005). This substantial comorbidity of LD in children with ADHD can be attributed to the shared neuropsychological manifestations in terms of executive function, attention, learning and processing speed (Doyle et al., 2005; Martinussen et al., 2005; Mayes & Calhoun, 2006). In a South African private practice study, 38.6% of learners presented with co-occurring ADHD and developmental dyslexia, highlighting the importance of comprehensive assessment beyond a single neurodevelopmental diagnosis (Stark et al., 2022).
Autism Spectrum Disorders (ASD)
Numerous international publications have indicated the growing prevalence of ASD in children with primary ADHD which can be attributed to similarities in the symptom presentation of both disorders (Gadow et al., 2009). Beyond the similarities in symptom presentation, genetic links as well as environmental risk factor links have been found between ADHD and ASD (Nijmeijer et al., 2009; Taurines et al., 2012). Prevalence in a United States-based study found that the prevalence of ASD among children with ADHD was 25%. Children with ASD and ADHD were more likely to be diagnosed with the combined subtype (Zablotsky et al., 2017). Despite the significant similarities between the two disorders, there is still a deficiency of data and population-based studies of ASD among children with primary ADHD.
Internalising and Mood Disorders
Depressive Disorders
ADHD presentation with comorbid depressive disorders has been associated with poorer prognosis, earlier commencement of treatment, and decreased success of medical intervention, along with increased rates of suicidality (Shaker et al., 2021). Prevalence rates of primary ADHD diagnosis with major depressive disorder (MDD) show great variation with ranges between 1% and 76% (Gorlin et al., 2016; Jaideep et al., 2006; Propper et al., 2015; Vannucchi et al., 2019). These large discrepancies may be due to the use of small sample sizes, indicating the gap in research on the primary diagnosis of ADHD with comorbid depressive disorders both globally and locally (Sandstrom et al., 2021).
Externalising and Behavioural Disorders
Oppositional Defiant Disorder (ODD)
International research suggests that 22–32% of children with ADHD have comorbid ODD (Adewuya & Famuyiwa, 2007; Olashore et al., 2020; Rimal & Pokharel, 2016). Other studies found that male patients with ADHD are more likely to display externalising disorders such as ODD, compared to females (Cuffe et al., 2020; Romano et al., 2005; Seo et al., 2022).
Conduct Disorder (CD)
A meta-analysis has shown that the prevalence of CD among individuals with ADHD ranges between 3.1% to 41.0% (Erskine et al., 2016). However, there are conflicting reports regarding sex differences in ODD/CD and children with ADHD. Some studies found no sex differences in comorbidity symptoms of CD amongst children with ADHD (Nock et al., 2007). However, others report more symptoms of ODD and CD in girls with ADHD compared to boys (Levy et al., 2005). More recent studies report CD to be two times more common in males with ADHD than females (Cuffe et al., 2020; Eskander, 2020; Mohammadi et al., 2021). Childhood ADHD has been described to progress to ODD and further into CD resulting in poor outcomes in adulthood (Eskander, 2020; Mphahlele et al., 2023). There is limited research to date, regarding the prevalence and co-existence of CD and ODD in South African children with ADHD.
Attachment and Trauma-Related Disorders
Reactive Attachment Disorder (RAD)
The prevalence of RAD in the general population is 1–2% (Irfan et al., 2022). However, the prevalence of RAD in children, specifically those with ADHD is not widely reported. Research has shown that there can be some overlap in symptoms between RAD and ADHD, however, they often occur together (Follan et al., 2011). Children who were removed from their homes and placed in foster care homes were more likely to experience RAD (Ellis et al., 2025).
Rationale for Research
ADHD in children is a globally prevalent neurodevelopmental disorder that is consistently accompanied by high rates of psychiatric comorbidity across diverse settings. However, the vast majority of the existing evidence base is drawn from high-income countries with well-resourced health systems, established diagnostic infrastructure, and relatively homogeneous sociocultural contexts. South Africa, as a middle-income country characterised by profound socioeconomic inequality, a pluralistic cultural landscape, significant mental health stigma, and limited specialist child psychiatric services, presents a context in which the presentation and recognition of ADHD comorbidities may differ substantially from international patterns.
Key contextual factors that set the South African setting apart include the role of traditional healing practices in mental health care-seeking (Rajcumar & Paruk, 2020), the impact of stigma as a barrier to diagnosis and treatment (Schoeman & Voges, 2022), structural inequities in access to specialist services and psychometric assessment, and the high burden of psychosocial adversity experienced by children and families in this context. These factors are likely to influence both the types of comorbidities that present clinically and the degree to which they are identified.
There is, therefore, a shortage of research both globally and within South Africa examining psychiatric comorbidities specifically in younger children diagnosed with ADHD. Early recognition and treatment of these comorbidities are important to ensure better long-term outcomes. This study addresses this gap by describing the psychiatric comorbidity profile of children aged 7–12 with primary ADHD at CAFU, CMJAH, situated within the South African public healthcare context.
Research Questions
1. What is the prevalence of psychiatric comorbidities in children with primary ADHD presenting to CAFU at CMJAH, and how does this compare with international data? 2. Which demographic and family-related factors are associated with specific psychiatric comorbidities in this sample, and do these reflect the sociocontextual risks prevalent in the South African setting?
Research Hypotheses
We predict that most children aged 7–12 with primary ADHD will have at least one comorbid psychiatric condition, in line with international research. Among these comorbidities, we hypothesise that ODD, GAD, LD, ID, and depressive disorders will be among the most common in our study. We also hypothesise that the sex distribution will be similar to international research, with more boys than girls presenting with ADHD. Given the high psychosocial burden and limited access to psychological assessment in the South African public healthcare context, we further hypothesise that rates of anxiety-related comorbidities may be elevated, while comorbidities requiring formal psychometric diagnosis (such as LD and ASD) may be under-represented relative to international norms.
Aim
To describe the psychiatric comorbidities and associated factors in children aged 7–12 years diagnosed with ADHD at CAFU, based at CMJAH, within the South African public healthcare context.
Objectives
• To describe the demographic profile, family structure, and school setting of all participants. • To estimate the overall prevalence of psychiatric comorbid conditions in children aged 7–12 years with a primary diagnosis of ADHD. • To estimate the prevalence of specific psychiatric comorbidities in ADHD children aged 7–12 years at their first visit to the unit. • To contextualise findings within the South African sociocultural and healthcare setting.
Methodology
Research Design
A retrospective, cross-sectional observational study design was used. All patient records at CAFU who fulfilled the study’s inclusion criteria were assessed.
Study Site
The study was conducted at CAFU, based at CMJAH. CAFU is an Outpatient Department which forms part of the Division of Child and Adolescent Psychiatry at the Department of Psychiatry, University of Witwatersrand Medical School. CAFU functions as a tertiary referral unit, receiving cases from community health centres, district hospitals, and general practitioners. The unit is staffed by specialist child and adolescent psychiatrists, registrars rotating through the unit, and allied health professionals including psychologists and social workers. Patients are seen for comprehensive multidisciplinary assessments, and diagnoses are made by qualified clinicians based on DSM-5 criteria.
Study Population
The study population consisted of children aged 7–12 years, with a primary diagnosis of ADHD. The children were from all sexes and ethnic groups, and all school settings were considered. Files with fully completed consent, assent forms, and information on admission between the first of January 2020 and the 31st of December 2022 to the unit were included in the study. Only comorbidities meeting the independent DSM-5 criteria were recorded. Comorbid diagnoses were established during the initial assessment at CAFU based on clinical interview, collateral information from caregivers and schools, and where indicated, formal psychometric evaluation by a registered psychologist. Pre-existing diagnoses from other facilities were verified against available documentation and clinical assessment at CAFU before being recorded.
Sampling
This was a convenience sample where the researchers accessed the clinic files of all patients, with a primary diagnosis of ADHD, aged 7 to 12 years accepted to the unit between the first of January 2020 and the 31st of December 2022. The files in which ADHD did not appear as a primary diagnosis were excluded from the study. Permission to access the records was acquired from the head of CAFU and the head of the health establishment at CMJAH. Ethics approval was obtained from the Human Research Ethics Committee (HREC), University of the Witwatersrand (Protocol No. M210601).
Data Collection Tool/Instrument
Data was collected from the records at CAFU at CMJAH by the researchers involved in the study and recorded on a data sheet using Microsoft Excel.
Data Collection Process
Hospital files were accessed, and all information was documented on the data sheet; no individual identifiers were included. All data was collected by the researchers. To ensure patient confidentiality, each patient received a study number. Information was transferred into an Excel datasheet. All the collected data was accessible only to the researchers and the supervisor.
Sources of Bias
Retrospective studies using hospital records, such as this one, can fall subject to several biases, including: • Selection bias: this was a convenience sample which is not a statistically balanced sample of the population, hence prone to selection bias. As a tertiary referral centre, CAFU may attract more complex cases; therefore, comorbidity rates observed may not reflect those at primary or secondary healthcare levels. • Information bias (reporting bias): individuals completing patient records lends itself to variation in the completeness of information. Mental health care professionals rotate regularly at CAFU, which may affect the consistency of records. However, documentation is guided by structured intake forms and patient charts, providing some degree of standardisation. • Confounding bias: there could have been a presence of variables outside the scope of this review that may have impacted on the findings. • COVID-19 pandemic impact: The study period (January 2020–December 2022) overlapped with the COVID-19 pandemic and associated lockdowns in South Africa. During lockdown periods, CAFU only saw emergency cases, which may have resulted in a smaller and potentially more severely affected sample. The pandemic may also have worsened mental health outcomes for children generally. A formal sub-analysis by pandemic period was not conducted due to the small sample size.
Acknowledging and minimising these potential biases is crucial for strengthening the validity and reliability of our study.
Ethics
• Informed consent: due to the study being retrospective, obtaining informed consent from every patient was not feasible. All patients complete consent and assent forms upon intake into CAFU, which includes consent for use of hospital records for retrospective reviews. • Confidentiality and privacy: patient’s personal information was kept safe and patients were anonymised using a study number. • Data security: the data sheets were placed on a secure Google Drive only accessible to the researchers. • Institutional review board (IRB) approval: ethical approval from the Human Research Ethics Committee (HREC), University of the Witwatersrand (Protocol No. M210601) was successfully obtained. • Equity and representation: the demographics of the psychiatric facility need to be considered to alleviate any risks of health disparity perpetuation from the study’s results. • Conflict of interest: these are all made evident and accounted for in the potential biases within the study. • Transparency in reporting: the reporting of methods and results in this study are in no way altered for the benefit of those involved in the research.
Data Analysis
Data was analysed using SPSS (Statistical Package for Social Sciences) version 26. Continuous variables like the age were summarised and presented as mean and standard deviation meanwhile categorical variables like sex and ADHD subtypes were presented as proportions. Chi-square test was used to determine the association between sex and psychiatric comorbidity. Fisher’s exact test was used to correct Chi-square where more than 20% of expected counts were less than 5. Level of statistical significance was at p < .05.
Results
Description of the Study Population
A total of 573 files were screened, and 108 files were included based on the inclusion criteria of the study.
ADHD Subtypes (Figure 1)
The combined subtype of ADHD was most prevalent (72.2%), followed by the inattentive subtype (19.4%) and lastly the hyperactive/impulsive subtype (1.9%). The subtype of ADHD was not recorded in 7 files (6.5%). ADHD subtypes (n = 108)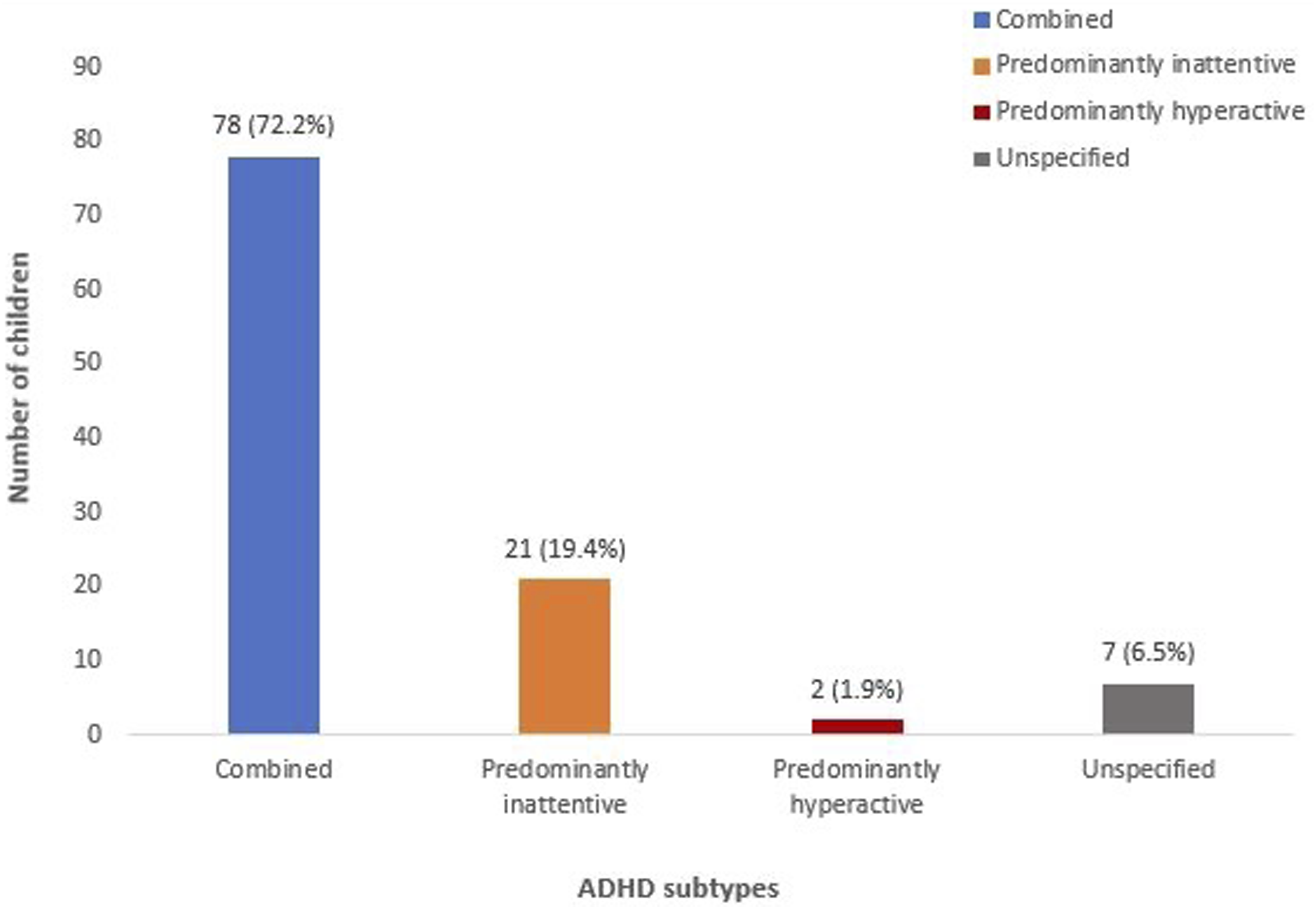
Demographic Variables (Table 1)
Demographics, Family Structure and School Settings of the Children With Diagnosis of ADHD
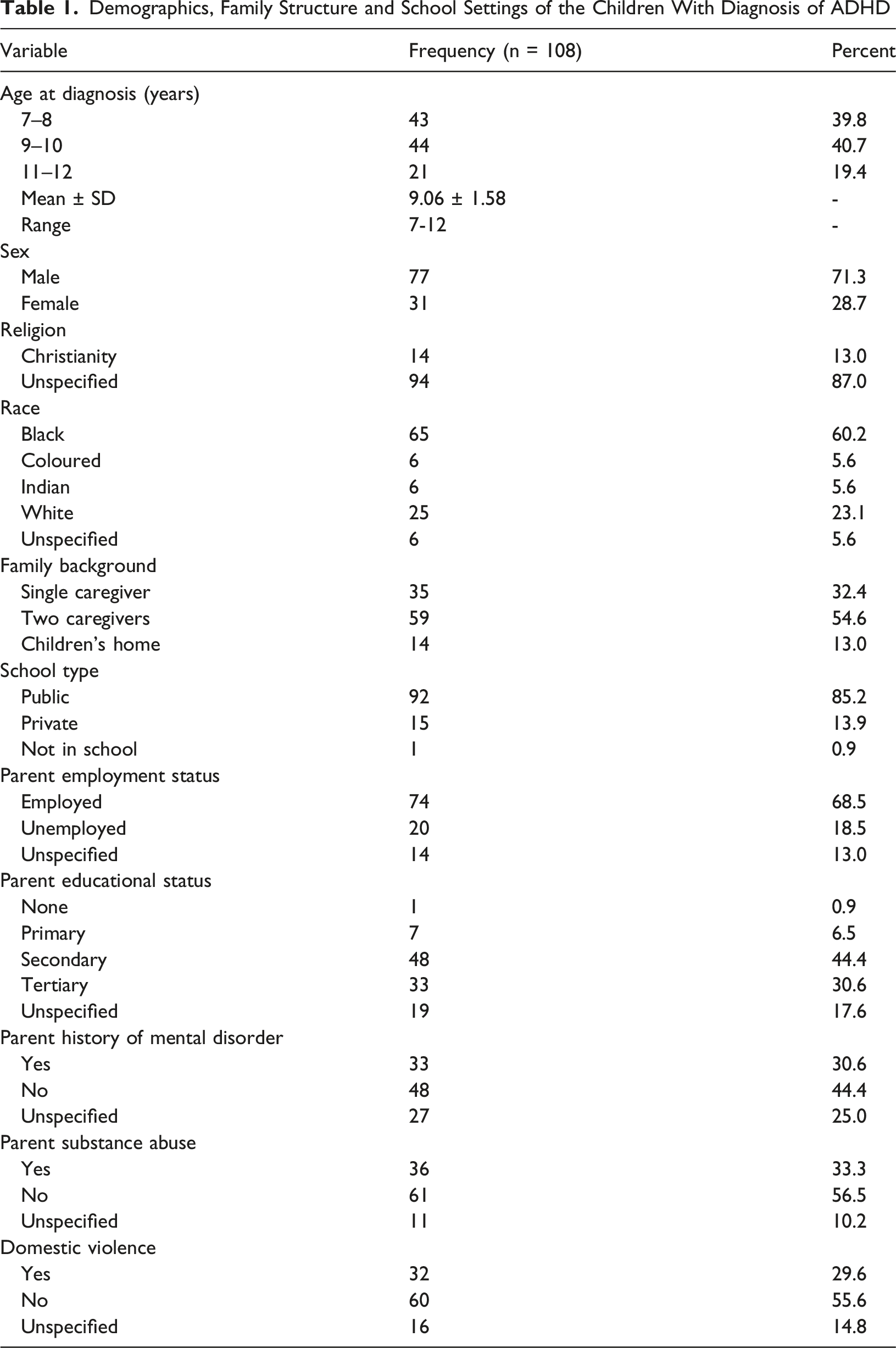
More than two-thirds of the parents were employed (n = 74, 68.5%); however, less than half had secondary education (n = 48, 44.4%). Among participants for whom parental mental health history was specified (n = 81), 40.7% (n = 33) had a known parental history of mental illness. Although a quarter of the sample had not specified the presence or absence of mental illness, only 30.6% (n = 33) of our sample had a known parental history of mental illness. Most parents in our sample did not abuse substances (n = 61, 56.5%) and 55.6% (n = 60) of families did not report domestic violence (Table 1).
Psychiatric Comorbidities
The prevalence rate of children with at least one psychiatric comorbidity is 95.5% (n = 103; Figure 2). Presence of psychiatric comorbidity among children with diagnosis of ADHD (n = 108)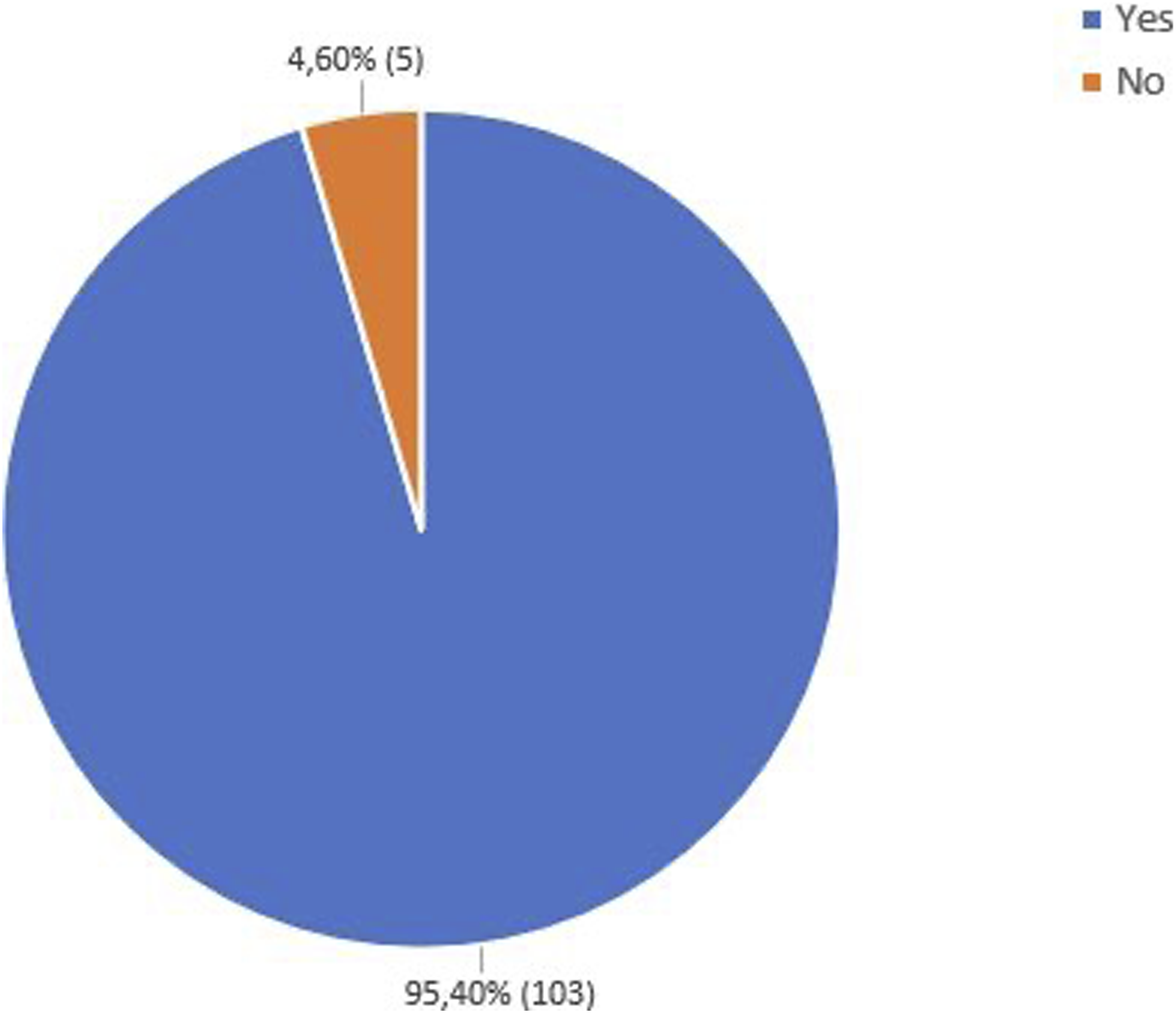
Most children presented with one or more comorbidity (n = 103, 95.5%) with a third of children having two comorbidities (n = 36, 33.3%), 30.6% (n = 33) having one comorbidity and 24.1% (n = 26) having three comorbidities (Figure 3). Number of comorbidities among children with a diagnosis of ADHD (n = 108)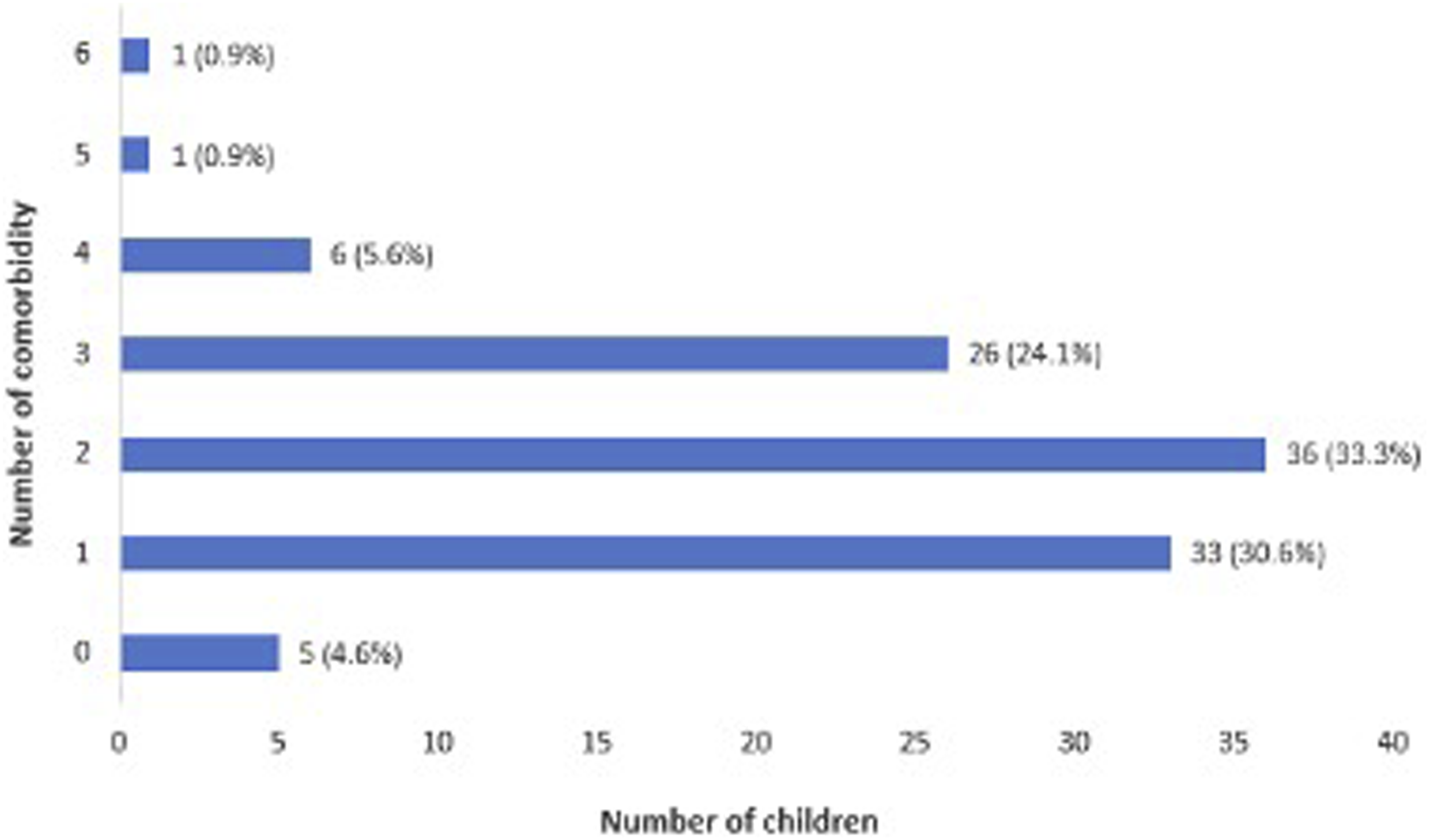
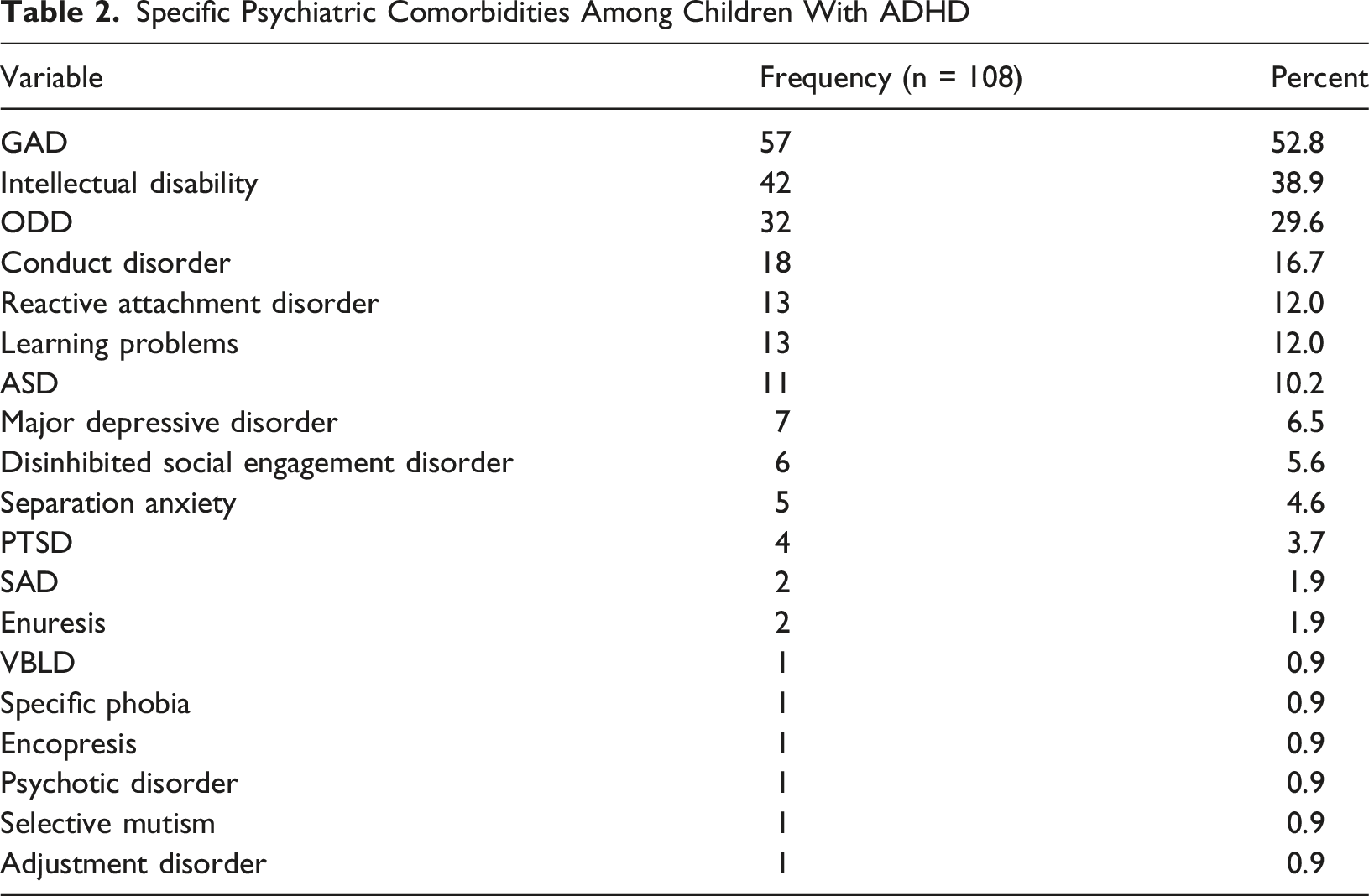
Prevalence of Comorbidities
Specific Psychiatric Comorbidities Among Children With ADHD
Association Between Sex and Presence of Specific Psychiatric Comorbidities
Association Between Gender and Presence of Specific Psychiatric Comorbidity Among the Children With Diagnosis of ADHD
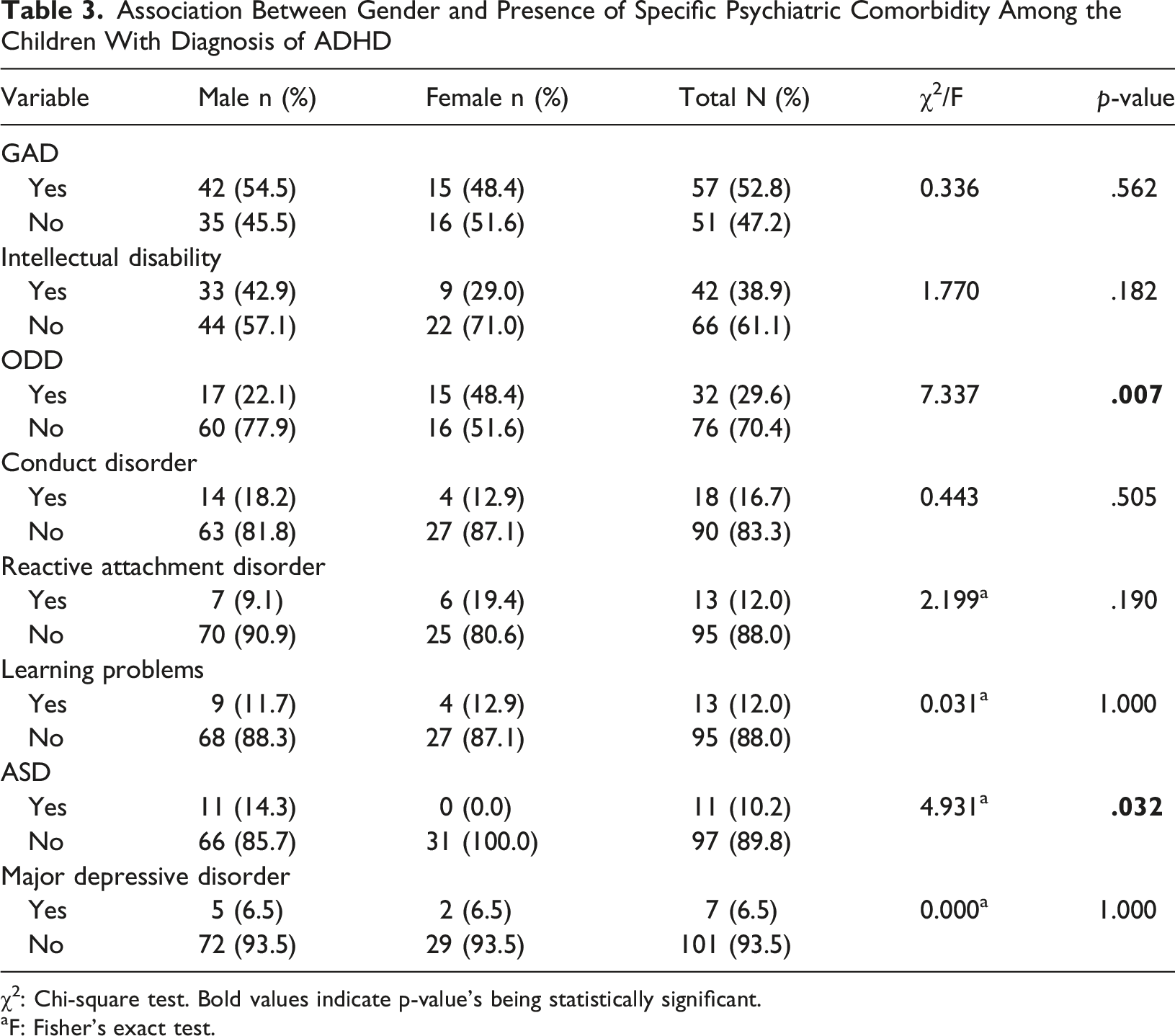
χ2: Chi-square test. Bold values indicate p-value's being statistically significant.
aF: Fisher’s exact test.
Discussion of Findings
ADHD Subtypes
Although our findings regarding the combined subtype of ADHD being most prevalent in clinical settings were consistent with previous research, our sample had higher rates (72.2%) than the studies conducted in Iran (42.7%). The predominantly hyperactive subtype (1.9%) was significantly lower compared to international research (31.0%; Ghanizadeh, 2009). These comparisons emphasize the variety in presentation which can be influenced by geographical location and the population characteristics (Nazeer et al., 2022).
Importantly, our finding of an overwhelmingly predominant combined subtype and a notably low inattentive subtype diverges substantially from global epidemiological data. The umbrella review by Ayano et al. (2023) found that the inattentive subtype was the most common globally (3%), followed by the hyperactive (2.95%) and combined types (2.44%). This discrepancy is unlikely to reflect a true epidemiological difference and is more plausibly explained by referral bias to a tertiary clinic. Children with predominantly inattentive ADHD, who may present with quieter, less disruptive symptoms, may go unrecognised in the South African public sector setting where hyperactivity and behavioural disturbance are primary drivers of referral. This is consistent with broader literature suggesting that inattentive presentations are consistently underidentified, particularly in girls and in lower-resource contexts. Future population-based studies in South Africa are needed to clarify this pattern.
Unfortunately, the subtype of ADHD was not recorded in 6.5% of files. This emphasises the importance of comprehensive assessment, accurate subtype identification, and record keeping and limits our findings due to reporting bias.
Demographics
The majority of children were male (71.3%), compared to only 28.7% being female, having a ratio of ∼2.5:1, which is slightly higher than the global average ratio of 2:1 (American Psychiatric Association, 2013). Most children were diagnosed before the age of 11, with 39.8% presenting between the ages of 7–8 years and 40.7% between 9–10 years. Most of our study population was Black (60.2%) followed by White (23.1%), Indian and Coloured (both 5.6%), and unspecified (5.6%).
The racial distribution in our sample is not proportionally reflective of South Africa’s general population, where approximately 81% are Black, 9% White, 9% Coloured, and 2% Indian/Asian. Our sample over-represents White children (23.1%) and under-represents Coloured children (5.6%), likely reflecting differential access to specialist psychiatric services at an urban academic hospital. This raises important concerns about healthcare equity: communities with lower socioeconomic status or those located further from urban tertiary centres may face significant barriers to specialist ADHD diagnosis and treatment. These access disparities have direct implications for resource allocation and the development of community-level mental health services in South Africa.
Most of the children in our study resided with two caregivers (54.6%). The distribution according to schooling was in line with the overall South African population, with most children attending public schools (85.2%; Statisa, 2018). Our study showed adequate demographical distribution, although our results are not generalisable to the greater South African population due to it being a convenience sample.
Although less than half of parents achieved secondary schooling (44.4%), employment rates (68.5%) were higher than the national reported employment rate (56.3–58.3%) for the period investigated (Statistics South Africa, 2021, 2023).
Parental psychiatric disorders were not specified in a quarter of the sample (25.0%); however, only 30.6% reported a history of parental psychiatric disorder. When restricting the analysis to participants with specified parental mental health status (n = 81), 40.7% had a known parental history of psychiatric disorder. This is clinically significant given the well-established heritability of ADHD and the broader impact of parental mental illness on child development and family functioning. The reason for collecting parental psychiatric disorder data specifically (rather than broader family history) relates to the direct genetic and environmental relevance of parental mental illness to the child’s clinical presentation. Parental psychiatric history directly informs risk stratification and treatment planning, and families where a parent has a psychiatric disorder may benefit from targeted psychoeducation and family-based interventions. Unspecified parental psychiatric disorders could partly be explained by the 13% of children residing in children’s homes.
Parental substance abuse was reported in a third of our sample (33.3%). Domestic violence was reported in 29.6% of our sample. This rate is markedly higher than the 5% reported in Canadian self-report studies, and is consistent with South Africa’s recognised burden of domestic violence (Statista, 2023). The elevated domestic violence rate in this sample is of considerable clinical significance: domestic violence is a well-established risk factor for childhood psychiatric disorders, including both ADHD and anxiety disorders. The high rates in our sample likely reflect the socioeconomic challenges prevalent in the communities served by CMJAH and may partly account for the high comorbidity burden observed, including the elevated rates of GAD and RAD. Clinicians working with children with ADHD in this context should routinely screen for domestic violence and substance use, and refer to appropriate support services where indicated.
Prevalence of Comorbidities
Prevalence rates of comorbidities in children with ADHD differ remarkably from population to population (Polanczyk et al., 2014; Willcutt, 2012). Almost all children with ADHD in this study presented with at least one comorbidity (95%), which is substantially higher than the international estimate of 60% (Gnanavel et al., 2019; Jogia et al., 2022). The average number of psychiatric comorbidities ranged between 1–3.
The comorbidities are discussed below by thematic cluster, to facilitate integrated clinical interpretation and support consideration of care needs.
Neurodevelopmental Conditions (ID, ASD, LD)
The second most common psychiatric comorbidity was ID (38.9%), in line with findings in a study done in the United Arab Emirates; however, it was four times higher than the 7.9% found in Denmark (Jensen & Steinhausen, 2015; Jogia et al., 2022). The elevated rate of ID in our sample warrants careful interpretation in the South African context. Limited access to early developmental screening and intervention, the legacy of educational inequity, and the tertiary referral pattern of CAFU may all contribute to the higher rates observed. Children with ADHD and co-occurring ID require adapted therapeutic approaches, modified educational support, and often benefit from multidisciplinary involvement including occupational therapy and speech-language therapy. The availability and accessibility of such services in the South African public health sector remains constrained, and clinicians should actively coordinate multidisciplinary care for this subgroup.
ASD was found to be prevalent in 10.2% of our study sample, lower than the prevalence rates (25%) in a United States-based study (Zablotsky et al., 2017). The relatively low ASD prevalence in our sample is unlikely to reflect a true epidemiological difference. ASD in South Africa is widely considered to be under-diagnosed, particularly in resource-constrained settings. Diagnostic challenges include the symptom overlap between ASD and ADHD, limited availability of specialist ASD diagnostic services, and the potential for cultural factors to influence symptom recognition. This aligns with the broader South African literature demonstrating that limited diagnostic capacity and service access significantly affect identification of neurodevelopmental conditions (Stark et al., 2022). Future research should specifically investigate ASD diagnostic rates and the factors contributing to under-identification in South African children.
Only one-eighth of children were diagnosed with LD. This was lower than the findings in another study where LD was prevalent in 27–31% of children with ADHD (DuPaul & Volpe, 2009). Learning Disorders are diagnosed using psychological assessments. In our sample, psychological assessments were not routinely completed for all children at CAFU during the study period; fewer than half are estimated to have undergone formal psychometric evaluation. This is likely a key driver of the lower LD rate and reflects a significant gap in service provision. This finding is consistent with the broader South African literature, which documents under-identification of learning disorders particularly in public sector settings where psychometric resources are scarce (Stark et al., 2022). Systematic access to psychometric testing should be part of the standard workup for children with ADHD at public tertiary facilities.
Anxiety and Internalising Disorders (GAD, Depressive Disorders)
Similar to another South African study, the most prevalent comorbidity in our study sample was GAD (52.8%; Mphahlele et al., 2020). The association between males and females was not statistically significant (Chi-square test, p = .562). However, the prevalence of GAD as a comorbidity in our study is double the rates compared to a study in Nepal (24.4%), and five times higher (9.9%) than a Korean study (Rimal & Pokharel, 2016; Seo et al., 2022). The markedly elevated GAD rates in this sample may reflect the high psychosocial burden in this population. Domestic violence, parental substance abuse, and family instability are well-recognised risk factors for anxiety disorders in children, and all three were prevalent in our sample. This is consistent with the sociocultural context of this study, where significant psychosocial adversity forms part of the lived experience of many children accessing care in the South African public sector. Clinicians should assess for anxiety as part of routine ADHD evaluation, particularly in settings with high psychosocial burden.
Although the children presented with low rates of depressive disorders (6.5%), international prevalence rates range significantly (1–73%; Gorlin et al., 2016; Jaideep et al., 2006; Propper et al., 2015; Vannucchi et al., 2019). The lower rates of depressive disorders in our sample may reflect diagnostic complexity in this age group, as depressive symptoms may be masked by or attributed to ADHD or other comorbid conditions. Future longitudinal research tracking mood outcomes in South African children with ADHD would be valuable.
Externalising and Behavioural Disorders (ODD, CD)
ODD was present in 29.6% of children. The prevalence rates of ODD in children with ADHD in our study align with international research rates, which range between 22% and 32% (Adewuya & Famuyiwa, 2007; Olashore et al., 2020; Rimal & Pokharel, 2016). In South Korea and the United States there were higher rates of ODD reported among males (Cuffe et al., 2020; Seo et al., 2022). However, our findings showed ODD to be significantly higher in female children compared to male children (Chi-square test, p = .007). This is an important finding with both clinical and policy implications. Clinicians should be alert to ODD presentations in girls with ADHD, as these may be overlooked given stereotyped expectations of female behaviour. The presence of ODD in girls is associated with poorer social outcomes and may benefit from targeted behavioural interventions. School-based resources such as social skills programmes, anger management interventions, and teacher psychoeducation may be particularly valuable for this subgroup.
The conduct disorder prevalence rates (16.7%) are in line with the range of 3.1–41% described in international literature (Erskine et al., 2016; Nock et al., 2007). There was no significant difference in the prevalence of CD between males and females in our study (Chi-square test, p = .51).
Attachment and Trauma-Related Disorders (RAD)
RAD was present in 12.0% of children, remarkably higher than previously reported prevalence rates in the general population (1–2%; Irfan et al., 2022). In the literature it is suggested that RAD was more likely to occur in children who were removed from their homes (Ellis et al., 2025). This may account for higher rates of RAD in our sample, where 13.0% of children were found to be residing in children’s homes. The elevated RAD rate may also reflect the broader context of domestic violence, substance abuse, and family disruption found in this sample. The high domestic violence rate (29.6%) and the proportion of children in out-of-home care (13%) are consistent with conditions associated with disrupted attachment. These findings highlight the importance of trauma-informed approaches in the assessment and management of children presenting with ADHD in this setting.
Strengths and Limitations
This study contributes to current research and aims to address the gaps within research regarding the prevalence of comorbidities in children with ADHD in South Africa. Children presenting with ADHD require a thorough history with psychological assessment when indicated to determine possible comorbid conditions. Mental health care professionals who are responsible for completing the initial assessment at CAFU rotate regularly, thus reporting bias might have impacted the outcome of our study. However, clinical documentation at CAFU is guided by structured intake forms and patient charts, which provide some degree of standardisation despite staff rotation. Therefore, we recommend that future researchers be actively involved in the history-taking process and encourage clinicians to practise comprehensive recordkeeping. This retrospective study took place at a tertiary institution in South Africa that receives multiple specialist case referrals, and some ADHD cases might have been dealt with in community services. This referral pattern may have contributed to the high comorbidity rates observed, as more complex cases with co-occurring conditions are more likely to be referred to tertiary services. Simpler, uncomplicated ADHD cases may be underrepresented in this sample. It is also important to keep in mind that part of our study period included the COVID-19 lockdown during which time only emergency cases were seen; this could have contributed to our small sample size. There was no comparison group to be drawn upon from a local perspective; however, this study could be used as a comparison for future studies.
Conclusion
This study was a retrospective record review of children at CAFU at CMJAH. Children aged 7–12 years with a primary diagnosis of ADHD were included. Most of the children had the combined subtype of ADHD and 95.4% had comorbid conditions. The most common comorbidity was GAD, followed by ID and then ODD. ODD was more prevalent in female children than male children. The high comorbidity burden, together with the sociocultural and structural factors prevalent in this sample – including high domestic violence rates, parental psychiatric history, substance use, and children in out-of-home care – underscores the need for comprehensive, trauma-informed, and multidisciplinary assessment of children with ADHD in South Africa. The racial distribution of the sample further highlights inequities in access to specialist services that require systemic attention.
Recommendations
For Clinical Practice
Healthcare professionals should conduct thorough, structured history-taking in all children presenting with symptoms of ADHD, with the explicit aim of identifying co-occurring psychiatric conditions. Given the exceptionally high comorbidity rate observed in this study (95.5%), a single-diagnosis approach is likely to be insufficient. Multidisciplinary assessments – including psychological evaluation, developmental assessment, and speech-language and occupational therapy input where indicated – should be prioritised, particularly given the high rates of intellectual disability (38.9%) and reactive attachment disorder (12%) in this sample. Clinicians should be particularly alert to sex-specific comorbidity patterns: our findings confirm significantly higher rates of ODD in girls (p = .007) and ASD in boys (p = .032), both of which may be missed if presentations are interpreted through gender-stereotyped clinical expectations. The high rate of domestic violence exposure (29.6%) in this sample indicates that routine screening for family adversity, trauma, and attachment difficulties should be integrated into ADHD assessments, with clearly defined referral pathways to social work, trauma-informed care, and family support services. Clinicians should also routinely enquire about parental mental illness and substance use, given their established roles as risk factors for ADHD and comorbid conditions.
For Policy and Service Planning
The discrepancy between the racial distribution of our sample and national South African demographics highlights significant inequities in access to tertiary mental healthcare. Black and Coloured communities, who are underrepresented in this sample relative to their population proportions, are likely to face greater barriers to specialist ADHD diagnosis and management. Policy efforts should focus on improving referral pathways and service accessibility for underserved communities, including strengthening ADHD assessment capacity at primary and secondary healthcare levels. Given the high comorbidity burden observed in this study, integrated care models that address ADHD alongside co-occurring conditions – including anxiety, intellectual disability, and attachment difficulties – are essential. School-based mental health resources should be strengthened to support children with ADHD and comorbid learning or behavioural difficulties. Access to formal psychometric evaluation should be systematically expanded at public tertiary facilities, as the absence of routine assessment is a key driver of the under-identification of learning disorders and ASD in this population.
For Future Research
Future studies should include local, district, and regional hospitals to obtain larger and more representative sample sizes, moving beyond the constraints of a single tertiary referral sample. Population-based epidemiological studies are urgently needed to determine the true prevalence of ADHD subtypes and their comorbidities in South Africa, given that clinic-based samples such as ours are subject to referral bias. Researchers should specifically investigate the reasons for the unusually low rates of the hyperactive/impulsive subtype (1.9%) and learning disorders (12%) identified in this study. Longitudinal studies are needed to understand the developmental trajectories of South African children with ADHD and comorbidities. The relationship between domestic violence, family disruption, and ADHD comorbidity profiles warrants dedicated investigation. Future studies should also specifically examine the impact of the COVID-19 pandemic on child mental health presentations, ADHD diagnosis rates, and service utilisation patterns in South Africa.
For Education and Awareness
Healthcare professionals, educators, and parents should be educated about the signs and symptoms of ADHD to facilitate timeous referral, early diagnosis, and intervention, thereby improving long-term outcomes. Given the high rates of comorbidity demonstrated in this study, awareness initiatives should extend beyond ADHD itself to encompass the full spectrum of conditions that may co-occur – including anxiety disorders, intellectual disability, learning disorders, and behavioural difficulties. Psychoeducation programmes should be developed that are culturally appropriate and accessible across language groups, with particular attention to addressing common misconceptions about ADHD and its treatment. The role of traditional healers as community health resources should be acknowledged and engaged, given evidence that many families in South Africa consult traditional healers before accessing biomedical services (Rajcumar & Paruk, 2020). Anti-stigma campaigns informed by the South African context are needed to reduce the barriers to help-seeking that have been identified as a significant obstacle to timeous diagnosis and treatment (Schoeman & Voges, 2022).
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.