
Abstract
Oppositional Defiant Disorder (ODD) often occurs with or without Conduct Disorder (CD) symptoms, yet it is unclear whether these presentations differ meaningfully in parenting, parent mental health, or co-occurring child difficulties. Using parent-report data from a cross-sectional, nationally representative sample of 1,000 children aged 5–12 years, this study compared those who screened positive for both ODD and CD, ODD only, or neither condition across measures of child and parent psychopathology and parenting practices and knowledge. Children with both ODD and CD showed broad elevations in anxiety, depression, and attention problems, along with higher rates of parent anxiety and depression. Their parents also reported poorer supervision, less positive parenting, and more inconsistent and harsh discipline. In contrast, children with ODD alone displayed moderate elevations in symptoms but largely normative parenting knowledge and discipline practices, differing little from those without disruptive behaviors. Findings highlight distinct symptom patterns associated with ODD with and without CD and underscore the importance of assessing these disorders separately. Clinicians should evaluate both child and parent mental health when ODD is present and tailor interventions accordingly. Moving beyond a “one-size-fits-all” approach may improve outcomes by aligning treatment strategies with each family’s unique constellation of symptoms and functioning.
Plain Language Summary
Children who often argue, refuse to follow rules, or show anger toward adults may have Oppositional Defiant Disorder (ODD). Some children with ODD also show more serious behaviors, such as aggression or rule-breaking, which are symptoms of Conduct Disorder (CD). It is not well understood whether children with ODD alone differ from those who have both ODD and CD, especially in terms of parenting and family mental health. In this study, parents of 1,000 children aged 5 to 12 across the United States reported on their child’s behavior, their own mental health, and their parenting practices. We compared three groups of families: those whose children screened positive for ODD only, ODD with CD, or neither condition. Children with both ODD and CD had much higher levels of anxiety, depression, and attention problems, and their parents also reported higher levels of anxiety and depression. These parents described more challenges with parenting, such as less supervision and more inconsistent or harsh discipline. In contrast, children with ODD alone showed only modest emotional and behavioral difficulties, and their parents reported largely healthy parenting. Children with both ODD and CD may need more intensive, combined support for both parent and child mental health, while children with ODD alone may benefit from more targeted, focused interventions.
Oppositional Defiant Disorder
Oppositional defiant disorder (ODD) is among the most common childhood disruptive behavior disorders, characterized by a persistent pattern of angry, defiant, and argumentative behavior toward authority figures (American Psychiatric Association, 2013). In clinical practice, diagnosis and treatment planning for ODD rely heavily on the criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders−5 (DSM-5, American Psychiatric Association, 2013). The most common evidence-based treatment for ODD is parent management training (PMT), a family-focused intervention designed to strengthen parenting practices by reducing harsh or inconsistent discipline and increasing positive, supportive parent-child interactions (National Institute for Health and Clinical Excellence, 2013). Multiple randomized controlled trials and meta-analyses have demonstrated that PMT is effective in reducing oppositional and disruptive behaviors (Fossum et al., 2008; Kaur et al., 2022; Leijten et al., 2018, 2019; Lundahl et al., 2006). The approach is grounded in Patterson’s Coercion Model, which posits that ODD symptoms arise, at least in part, from patterns of harsh, inconsistent, or otherwise ineffective parenting that inadvertently reinforce oppositional behavior and impede the development of adaptive self-regulation in children (Fisher & Gilliam, 2012; Patterson, 2002).
Careful Assessment of ODD and Treatment Implications
Although substantial evidence supports the efficacy of PMT for the treatment of ODD, outcomes are variable, and a third to half of children in treatment do not show adequate improvement, particularly in the long-term (Colalillo & Johnston, 2016; Hawes et al., 2014; Ollendick et al., 2016). Part of the variability in PMT outcomes may stem from incomplete or inconsistent assessment. Comprehensive assessment plays a critical role not only in diagnostic clarification but also in determining the type and intensity of intervention most appropriate for a given child and family. In some cases, children presenting with oppositional behaviors are evaluated only for ODD, without consideration of co-occurring conditions such as conduct disorder (CD), attention-deficit/hyperactivity disorder (ADHD), anxiety, or depression (Chase & Eyberg, 2008; Frick & Nigg, 2012). In other instances, clinicians may aggregate ODD and CD symptoms into a broader “disruptive behavior” category (Epstein et al., 2015). Such approaches may obscure meaningful differences in symptom profiles and family characteristics.
Comorbid child psychopathology and parent mental health difficulties are common among youth with disruptive behaviors (Drabick et al., 2008; Helander et al., 2023). These comorbidities may shape both the expression of oppositional behavior and the types of interventions that are most appropriate. For example, children with elevated anxiety may be more avoidant or emotionally dysregulated, while children with elevated depression may demonstrate reduced motivation and engagement in treatment, suggesting the need for interventions that incorporate emotion regulation or cognitive-behavioral components alongside parent-focused strategies (Drabick et al., 2008; Jacobs et al., 2010). Similarly, ADHD-related difficulties in attention and impulse control may necessitate adaptations that account for executive functioning challenges (Paiva et al., 2024). Comorbid CD may further may further alter treatment planning, as children with CD often present with more severe and pervasive behavioral problems that may warrant more intensive or multi-systemic approaches (Frick & Nigg, 2012).
Parent-level factors may further contribute to this heterogeneity. Depression and anxiety in parents have been shown to interfere with the implementation of parenting strategies, as symptoms such as low energy, heightened irritability, or excessive worry can undermine consistency, reduce positive engagement, and escalate family conflict (Moghaddam et al., 2016; Ollendick et al., 2016). Clarifying the distinctions between children with ODD alone, and those with co-occurring disorders is therefore important for refining assessment and guiding the selection and intensity of interventions within heterogeneous ODD presentations.
Parenting and ODD
Less attention has been devoted to examining whether impairments in parenting are uniformly present among families of children with ODD, or whether such impairments vary across clinically meaningful subgroups. Much of the existing work presumes that harsh, inconsistent, or negative parenting is a core feature of ODD, yet this assumption is not commonly tested (Kaur et al., 2022; Lindhiem et al., 2023). It remains unclear whether parenting difficulties represent a universal risk factor, or whether they are more characteristic of particular subgroups, such as children with comorbid conduct disorder or greater severity of externalizing symptoms (Azeredo et al., 2018; Lindhiem et al., 2023). Clarifying the extent and variability of parenting difficulties across ODD presentations is therefore critical for refining theoretical models and ensuring that interventions are appropriately targeted.
Moreover, research has not consistently integrated parental mental health difficulties or children’s internalizing symptoms into models of ODD, leaving important gaps in understanding how these factors may shape treatment needs and outcomes. The current study addresses these limitations by evaluating child anxiety, depression, and attention-deficit/hyperactivity disorder (ADHD), parent depression and anxiety, and parenting knowledge and behavior across three groups: children screening positive for ODD only, children screening positive for comorbid ODD and CD, and children screening negative for either diagnosis. This design clarifies whether the presence of ODD is consistently associated with parenting and both parent and child mental health impairments or whether such associations vary depending on comorbidity patterns in the child.
Method
Participants
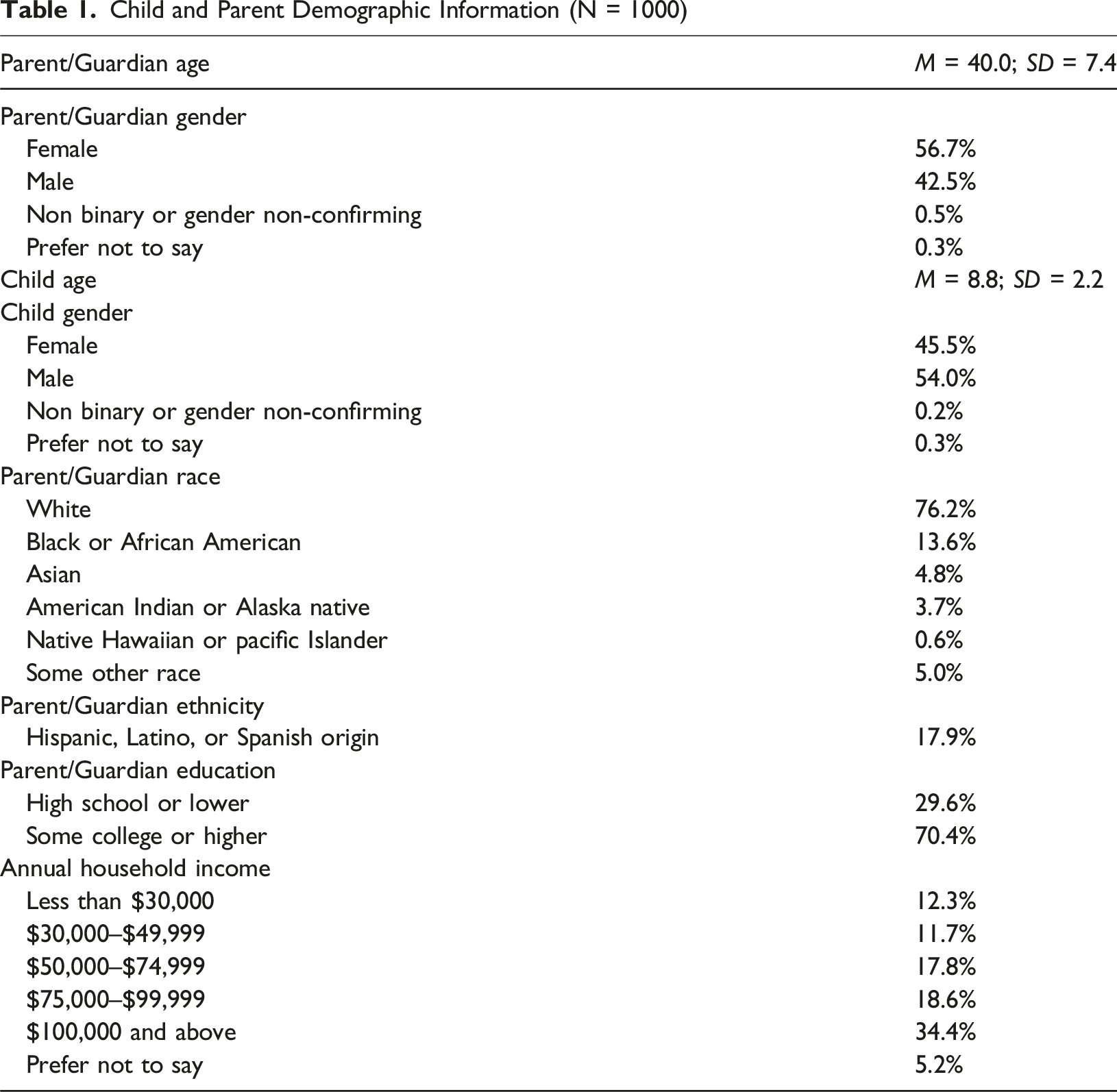
Child and Parent Demographic Information (N = 1000)
Procedures
Over two million U.S. residents participate in YouGov panels and have been recruited through web advertising, permission-based email campaigns, partner contacts, random digit dialing, and postal mail. YouGov surveyed 1,102 parents of children ages 5–12, who were then used to create the final sample of 1,000. The eligibility rate for the survey was 66.7% and the response rate was 57.8%. The sampling frame was constructed by mirroring stratified sampling from a parents-only subset of the 2022 American Community Survey (ACS) sample. The YouGov matched cases were weighted to the sampling frame using propensity scores. The propensity score function included age, gender, race/ethnicity, years of education, marital status, employment status, and region. The YouGov matched cases and the ACS subsample were combined, and a logistic regression was estimated for inclusion in the frame. The propensity scores were grouped into deciles, and post-stratified according to these deciles. Participants were compensated with a $25 gift card for completing the full survey.
Measures
Oppositional Defiant Disorder and Conduct Disorder
Vanderbilt Assessment Scale-Parent Report (VAS-P)
The VAS-P is a 22-item parent-report that screens for oppositional defiant disorder (ODD) and conduct disorder (CD) among other behavioral concerns. Symptom items are rated using a four-point scale (“never” to “very often”), with total subscale score ranges of 0 to 24 for ODD and 0 to 42 for CD. The measure has current study Cronbach’s alphas of .89, and .97, respectively, and strong evidence of construct validity (Anderson et al., 2022; Wolraich et al., 1998). Children were classified as screening positive for ODD if parents scored them a two “often” or three “very often” on at least four of eight items and as screening positive for CD if parents scored them as a two “often” or three “very often” on at least three of 14 items.
Mental Health Measures
Child Anxiety: Screen for Child Anxiety Related Disorders (SCARED) Parent Report
The SCARED is a 41-item measure of parent-reported symptoms of child generalized anxiety, separation anxiety, social phobia, panic disorder, and school phobia. Items are rated using a 3-point Likert scale (range 0 - 82; 0 = ‘not true or hardly ever true’, 1 = ‘somewhat or sometimes true’, 2 = ‘very or often true’). The internal consistency of the SCARED is high, with a current study Cronbach’s alpha of .95. The measure has strong convergent and divergent validity (Birmaher et al., 1997; Sequeira et al., 2020). Tests of criterion validity suggest a cut-off score of 25 for optimal prediction consistent with an anxiety disorder (Birmaher et al., 1997).
Child Depression: Mood and Feelings Questionnaire (MFQ) Parent Report
The MFQ is a 34-item measure of parent-reported depression symptoms in children (Costello & Angold, 1988). Items are rated using a 3-point scale (range, 0 - 68; 0 = “not true”; 1 = “sometimes”; 2 = “true”). The measure has high internal consistency (current study Cronbach’s alpha = .96) and strong construct validity. The 90th percentile is commonly used to identify clinically elevated symptoms across measures (Craighead et al., 1998); in the current sample, this corresponds to a cutoff score of 23 (Lindhiem et al., 2025).
Attention Deficit Disorder: Vanderbilt Assessment Scale-Parent Report (VAS-P)
The VAS-P is an 18-item parent-report screen for attention-deficit/hyperactivity disorder (ADHD). Symptom items are rated using a 4-point scale (“never” to “very often”), with total scores ranging from 0 to 54. The measure has a current study Cronbach’s alpha of .94, and strong evidence of construct validity (Anderson et al., 2022; Wolraich et al., 1998). Children were classified as screening positive for ADHD if they scored two or three (“often” or “very often”) on at least six of nine items for either inattentive or hyperactive/impulsive symptoms. These subtypes were combined into an omnibus ADHD variable (yes/no).
Parent Depression: Patient Health Questionnaire-8
The PHQ-8 is an eight-item self-report measure for assessing symptoms of depression using a four-point scale ranging from “not at all” to “nearly every day”. Scores range from 0 to 24, with 10 or higher belonging to the clinical range of moderate (10–14) or severe (15+) symptoms. The measure has a current study Cronbach’s alpha of 0.91 and has satisfactory construct validity (Kroenke et al., 2009; Pressler et al., 2011).
Parent Anxiety: Generalized Anxiety Disorder-7
The GAD-7 is a seven-item self-report screening measure for assessing the severity of generalized anxiety disorder. Items are rated using a four-point scale from “not at all” to “nearly every day’” Scores range from 0 to 21, with 10 or higher being in the clinical range of moderate (10–14) or severe (15+) symptoms. The measure has excellent internal consistency (current study Cronbach’s alpha of 0.88), with strong test-retest reliability and evidence for convergent validity (Spitzer et al., 2006).
Parenting Measures
Parenting Knowledge: Knowledge of Effective Parenting Test – Externalizing (KEPT – E)
The KEPT-E (Lindhiem et al., 2019) is a 21-item measure of parental knowledge of effective parenting skills. The measure was developed as a potential treatment target for evidence-based psychosocial treatments of disruptive behaviors in children. The KEPT-E assesses parental knowledge of domains including praise, rewards/point systems, attending and ignoring, commands/expectations, consequences, and time-outs. Parents are presented with video and text-based parenting scenarios and four potential responses, with the correct response scored 1 and the other three alternatives scored 0. Thus, raw scores range from 0 to 21. The measure has good internal consistency (current study Cronbach’s alpha = .83). The measure also demonstrated convergent validity with other measures of parenting knowledge and parenting related constructs (e.g., child behavior, child psychopathology).
Parenting Practices: The Alabama Parenting Questionnaire (APQ)
The APQ (Frick, 1991; Shelton et al., 1996) is a 42-item measure that assesses five dimensions of parenting, each on a 5-point scale ranging from 1, “never” to 5, “always”: (1) involvement (score range, 10–50), (2) positive parenting (score range, 6–30), (3) poor supervision (score range, 10–50), (4) inconsistent discipline (score range 6–30), and (5) corporal punishment (score range, 3–15). The internal consistency of the scale is acceptable with alphas in the current study for the five domains ranging from .76 to .91. The measure has well-established construct validity.
Statistical Analyses
For measures with established clinical cutoffs (child anxiety, depression, ADHD, and parent anxiety and depression), participants were classified as above or below the threshold to facilitate clinically meaningful interpretation. Descriptive statistics, including means, standard deviations, and percentages above clinical cutoffs, were calculated for each group: children screening negative for ODD and CD, those screening positive for ODD only, and those screening positive for both ODD and CD.
Differences on continuous measures were examined using one-way analyses of variance (ANOVAs), with group (neither, ODD only, ODD and CD) as the between-subjects factor. When omnibus tests were significant, pairwise comparisons were conducted using Bonferroni-corrected p-values. Separate Bonferroni corrections were applied for each set of analyses (overall omnibus tests, pairwise comparisons) to control the family-wise error rate within each domain. Cohen’s d effect sizes were calculated for all pairwise comparisons to aid interpretation of group differences. All analyses were conducted using SPSS version 29.0, with an alpha level of 0.05 applied prior to correction. Missing data were minimal (<0.05%) and were handled through listwise deletion.
Results
Sample Characteristics
Positive screens for comorbid ODD and CD were prevalent. Of the 117 children who screened positive for ODD, 50.4% (n = 59) screened positive for CD. Of the 75 children who screened positive for CD, 78.7% (again n = 59) also screened positive for ODD. Only 16 children screened positive for CD alone. ODD symptom severity differed across groups. Children with ODD only had a mean ODD score of 14.2 (SD = 3.5), whereas children with comorbid ODD + CD had higher ODD scores, with a mean of 16.3 (SD = 3.7). In contrast, children with no ODD or CD had much lower mean ODD scores (M = 4.4, SD = 3.1).
Mental Health Differences
Child Mental Health
Descriptives and Omnibus ANOVA Results of Oppositional Defiant Disorder and Conduct Disorder by Measure: Mental Health
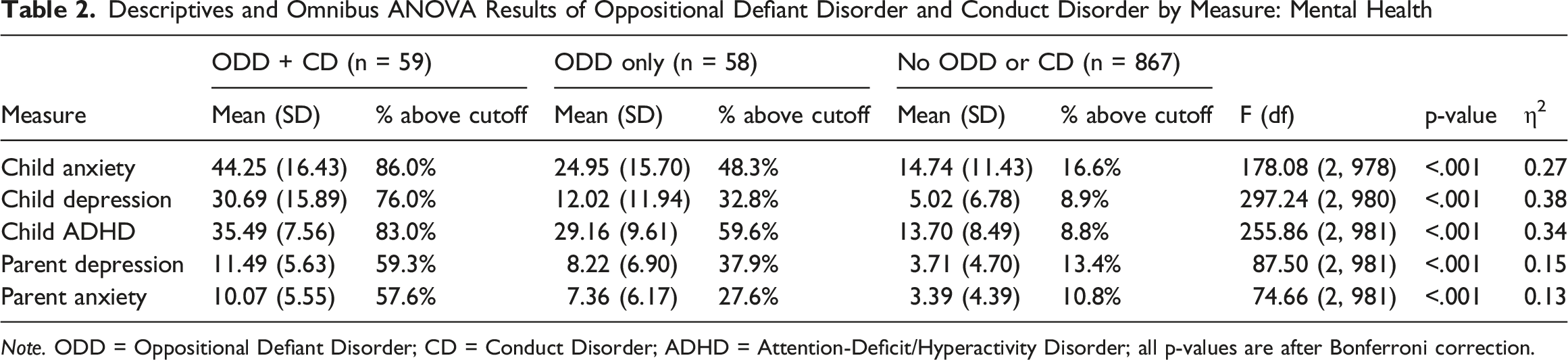
Note. ODD = Oppositional Defiant Disorder; CD = Conduct Disorder; ADHD = Attention-Deficit/Hyperactivity Disorder; all p-values are after Bonferroni correction.
Pairwise comparisons showed that children screening positive for ODD + CD scored significantly higher than both the ODD-only and negative ODD/CD groups on all three measures, with large effect sizes (d’s = 0.73−2.59, p’s < .001). Children screening positive for ODD only also scored significantly higher than those screening negative for ODD/CD, but with smaller effects (d’s = 0.63-1.75, p’s < .001). Percentages above clinical cutoffs followed this same graded pattern, with the highest elevations observed among children screening positive for ODD + CD (86.0% for anxiety, 76.0% for depression, 83.0% for ADHD), followed by those screening positive for ODD only (48.3%, 32.8%, and 59.6%), and with the lowest percentages among children screening negative for ODD/CD (16.6%, 8.9%, and 8.8%).
Parent Mental Health
Significant group differences also emerged for parent anxiety and depression (all p < .001; see Table 2). Parents of children screening positive for ODD + CD reported the highest levels of anxiety and depression, followed by those screening positive for ODD only, and with the lowest levels among parents of children screening negative for ODD/CD. Pairwise comparisons indicated that parents of children screening positive for ODD + CD reported significantly higher symptoms than both those screening positive for ODD only (d’s = 0.48–0.52, p’s < .01) and those screening negative for ODD/CD (d’s = 1.18−1.38, p’s < .001). Parents of children screening positive for ODD only also reported higher symptoms than those screening negative for ODD/CD (d’s = 0.69−0.70, p’s < .001). Percentages above clinical cutoffs reflected this pattern, with the highest percentages among parents of children screening positive for ODD + CD (57.6% for anxiety, 59.3% for depression), followed by those screening positive for ODD only (27.6%, 37.9%), and with the lowest rates among parents of children screening negative for ODD/CD (10.8%, 13.4%).
Parenting Differences
Descriptives and Omnibus ANOVA Results of Oppositional Defiant Disorder and Conduct Disorder by Measure: Parenting
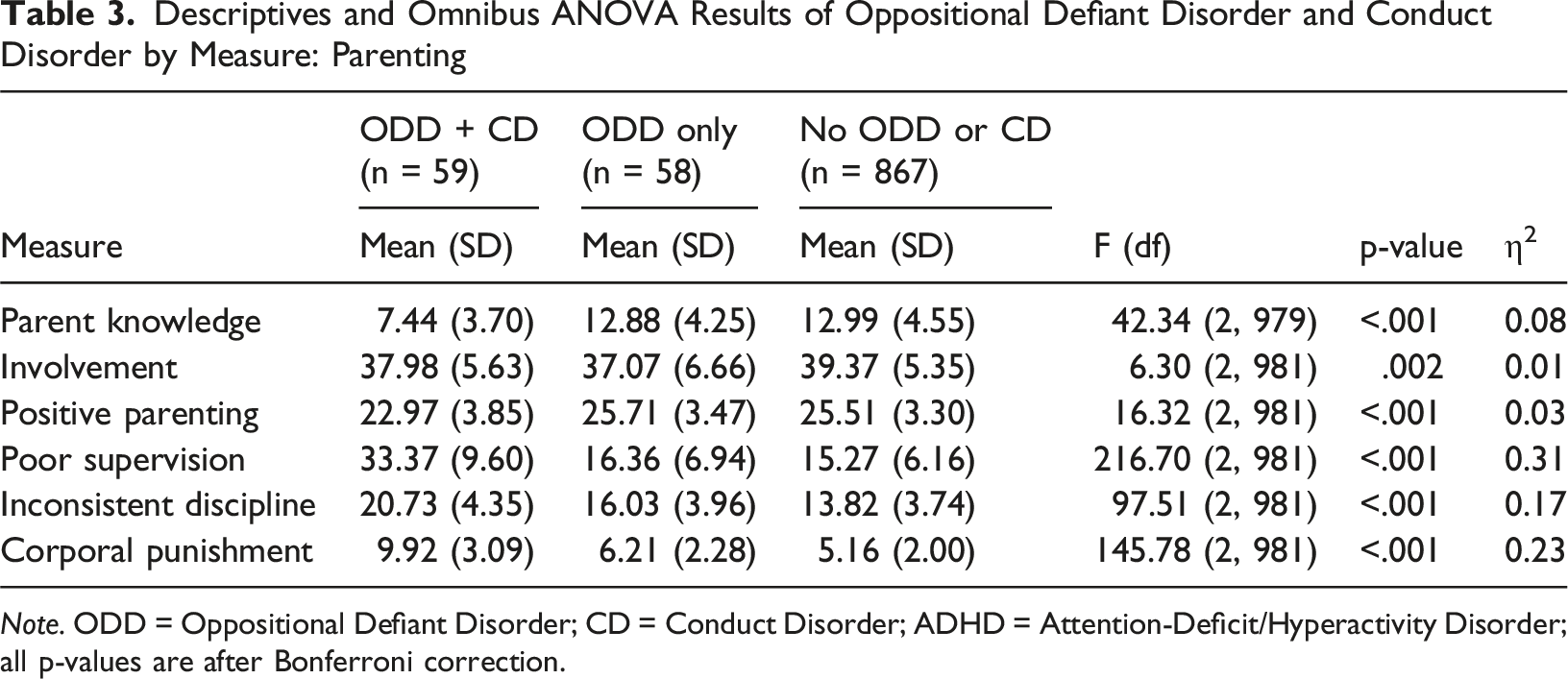
Note. ODD = Oppositional Defiant Disorder; CD = Conduct Disorder; ADHD = Attention-Deficit/Hyperactivity Disorder; all p-values are after Bonferroni correction.
Pairwise Statistical Comparisons of Symptom Groupings: Mental Health
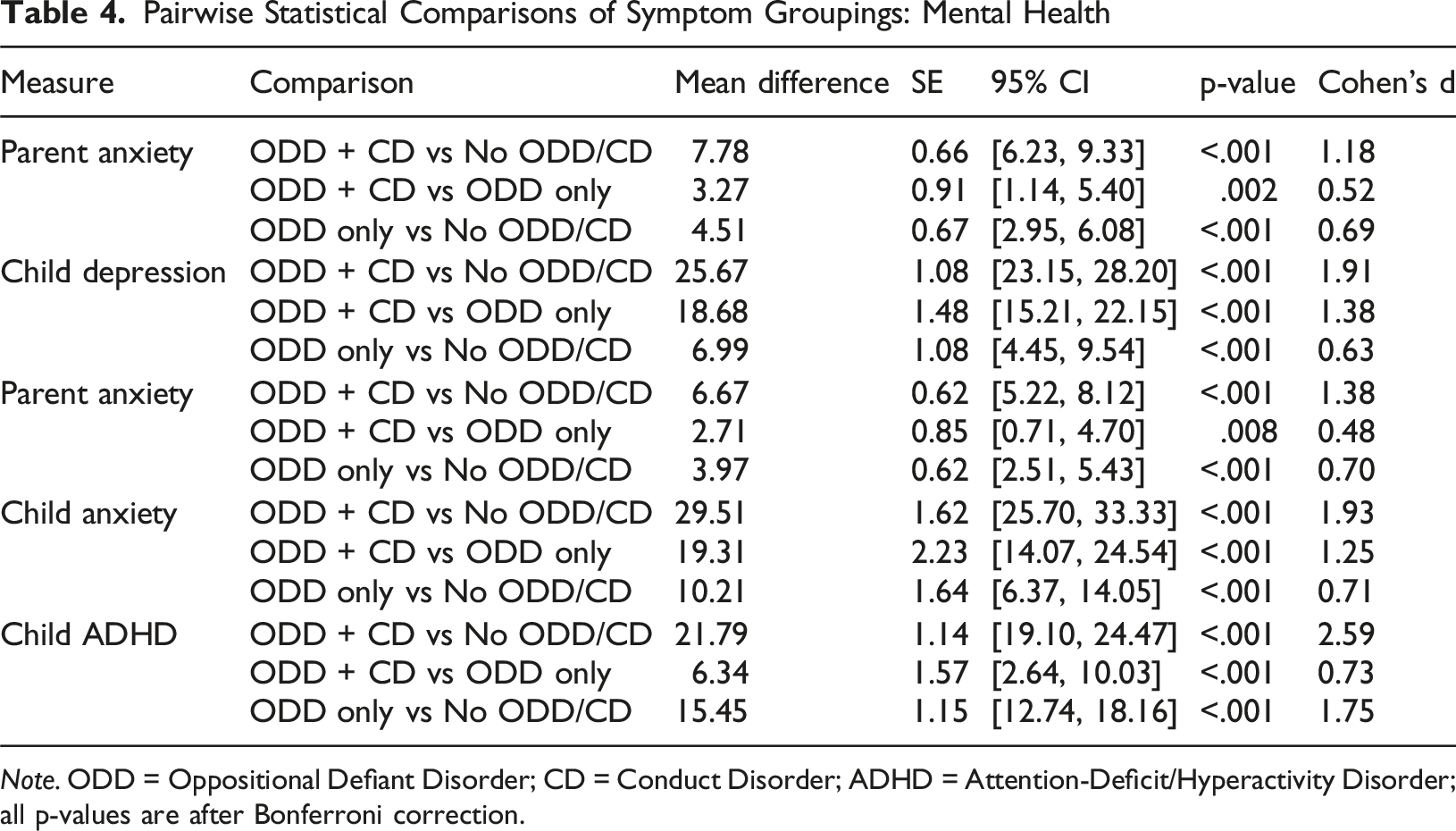
Note. ODD = Oppositional Defiant Disorder; CD = Conduct Disorder; ADHD = Attention-Deficit/Hyperactivity Disorder; all p-values are after Bonferroni correction.
Pairwise Statistical Comparisons of Symptom Groupings: Parenting
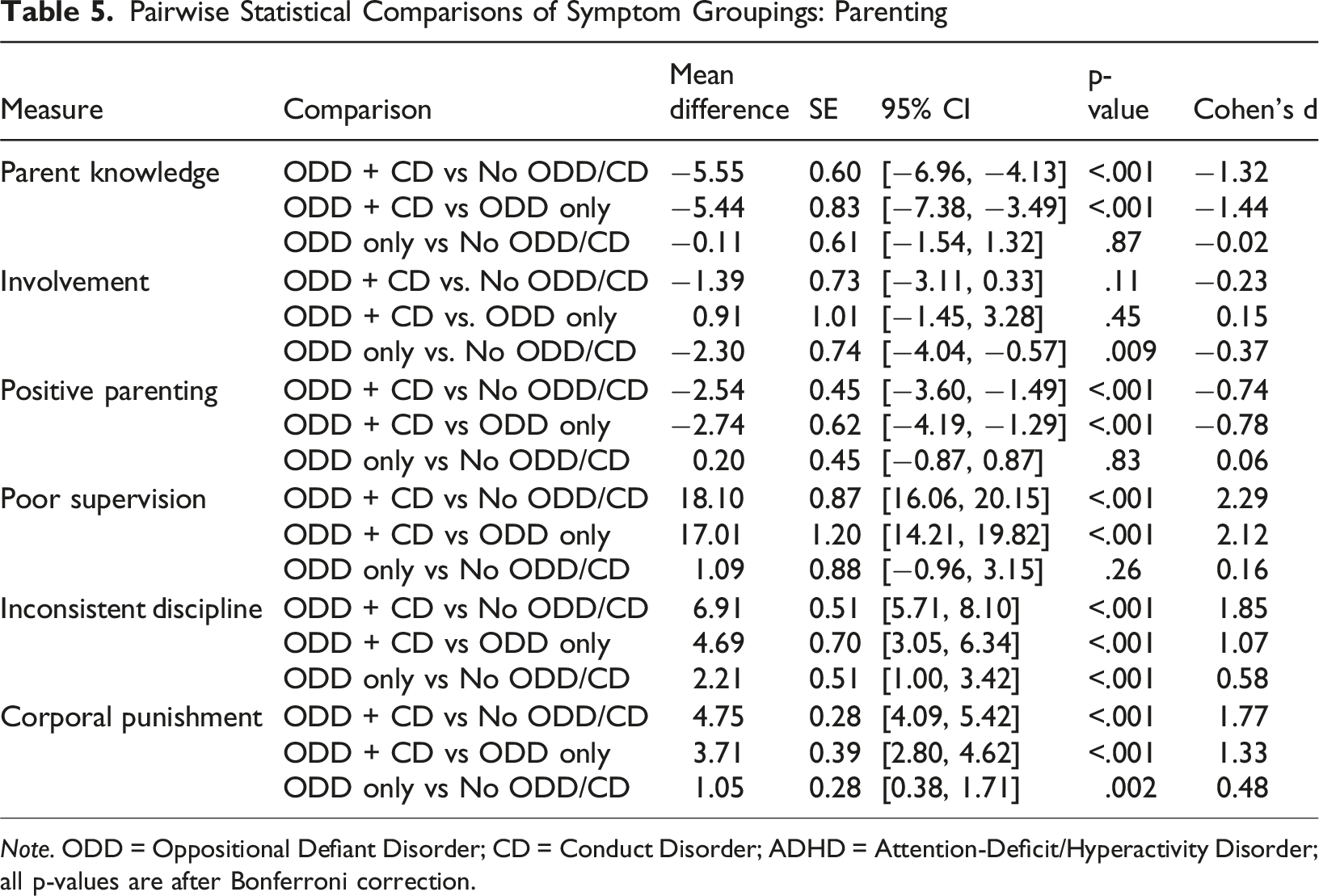
Note. ODD = Oppositional Defiant Disorder; CD = Conduct Disorder; ADHD = Attention-Deficit/Hyperactivity Disorder; all p-values are after Bonferroni correction.
Differences were pronounced for negative parenting practices. Parents of children screening positive for ODD + CD reported markedly higher poor supervision, inconsistent discipline, and corporal punishment compared to the other groups, with large effect sizes (d’s = 1.07−2.29, p’s < .001). Parents of children screening positive for ODD only also reported higher inconsistent discipline and corporal punishment than those screening negative for ODD/CD (d’s = 0.48−0.58, ps < .01); however, these effects were more modest in magnitude than those observed for comparisons involving the ODD + CD group versus the other groups. Poor supervision did not differ significantly between the ODD-only and negative ODD/CD groups.
Discussion
In the present study, distinct patterns of child internalizing and externalizing symptoms, parenting behaviors, and parenting knowledge emerged across groups of children with positive screens for ODD and CD. First, the proportion of children screening positive for ODD and ODD + CD in this community sample was broadly consistent with epidemiological prevalence estimates, supporting the validity of the screening procedures used (Bitsko, 2022). Parents of children with positive screens for both ODD and CD consistently reported higher symptoms of anxiety and depression in their children and in themselves. Parents of children with positive screens for ODD only reported elevated rates of anxiety, depression, and ADHD symptoms for their children, as well as elevated depressive and anxiety symptoms for themselves, though levels were consistently lower than those observed in the ODD + CD group. Rates of anxiety and depressive symptoms in the group screening negative for ODD and CD were consistent with population-based estimates for school-aged children, indicating that elevations in the ODD and ODD + CD groups reflect meaningful increases above expected community levels (Bitsko, 2022). ADHD symptoms were most pronounced among children screened positive for both ODD and CD but were less severe in the other two groups.
Parenting patterns showed a similar divergence: parents of children with positive screens for ODD and CD reported greater deficits in knowledge of effective parenting strategies, supervision behaviors, positive parenting, and consistency in discipline, compared to parents of children with negative ODD and CD screens. Parents of children with positive screens for ODD only reported largely comparable parenting knowledge and parenting behaviors to the parents of children with negative screens for ODD or CD, with the exception of higher inconsistent discipline and higher corporal punishment reported by parents of children with positive ODD screens.
Clinical Implications
Findings from this study underscore the importance of comprehensive assessment practices when evaluating disruptive behavior problems. Clinicians should carefully assess both oppositional-defiant and conduct-disordered behaviors, as their co-occurrence identifies a subgroup of youth with a more severe and clinically complex profile, marked by broader child and parent mental health difficulties (Ghosh et al., 2017; Lindhiem et al., 2015). Much of the existing literature and many clinical trials use an omnibus category of “disruptive behaviors” that combines ODD and CD (Epstein et al., 2015). While this simplifies categorization, it obscures important differences: children with ODD only typically show irritability and defiance, whereas children with CD are more likely to engage in aggression and rule-breaking (Azeredo et al., 2018). Combining them may mask differences in treatment response and comorbidities (Petty et al., 2009). Assessing ODD and CD separately, and considering their co-occurrence, is therefore critical for accurate diagnosis, tailored treatment, and clearer interpretation of outcomes (Petty et al., 2009). In addition, routine assessment of comorbid conditions, including anxiety, depression, and ADHD, is critical, given their high prevalence and differential associations across subgroups (Evans & Burke, 2024; McKinney & Morse, 2012). Such an approach not only provides a more accurate clinical picture but also facilitates more tailored treatment planning that accounts for the heterogeneity observed among children presenting with disruptive behavior.
The results also highlight the need for differentiated intervention approaches based on clinical presentation. For children screened positive for both ODD and CD, intensive parenting-only interventions remain essential but are unlikely to be sufficient. Given the young age of our sample (5–12 years), those already exhibiting CD symptoms may represent a high-risk group for life-course persistent conduct problems, consistent with evidence linking earlier onset to more severe trajectories (Moffitt, 1993). These families may benefit from multimodal approaches that integrate parent management training with interventions addressing comorbid child psychiatric symptoms, as well as parent mental health, such as cognitive-behavioral therapy (CBT) for anxiety and depression or skills training to improve emotion regulation and family functioning (Masi et al., 2014; Shaffer et al., 2013; Silverstone et al., 2016). Evidence-based treatments such as multisystemic therapy (MST) offer a model for such multimodal intervention, targeting parent-child dynamics as well as broader child-in-context factors, including peer relationships, school engagement, and community supports, and have demonstrated efficacy in reducing conduct problems and improving long-term outcomes in youth with severe disruptive behavior (Littell et al., 2021).
In contrast, children with ODD only present a different clinical profile. Although aspects of parent training may be helpful, particularly around reducing inconsistent discipline and supporting parents in applying strategies in the moment (Dedousis-Wallace, 2024; Dekkers et al., 2022), broad parenting deficits (both knowledge and behavior) were not observed in this group compare to the group of parents whose children had negative ODD/CD screens. It is possible that some parents possess adequate knowledge but struggle with consistent implementation, especially given that our study relied on the report of a single parent. Interventions for ODD only may be most effective when they extend beyond parent training to include CBT for children and parents, targeted emotion regulation skills training, and supports that address comorbid symptoms without overemphasizing generalized parenting deficits (Gouze et al., 2024).
Strengths and Limitations
This study has several strengths. First, it draws on a large, nationally representative sample, enhancing the generalizability of findings to the broader U.S. population. Second, the sample included children with sufficient variability in positive screens for ODD and combined presentations, allowing for direct comparisons across groups that are often conflated or understudied. Third, the inclusion of both child mental health symptoms and parenting knowledge and behavior provides a more comprehensive view of the family context surrounding disruptive behavior. At the same time, some limitations should be acknowledged. First, while screening tools offer valuable clinical insight, they are less comprehensive than structured diagnostic interviews, limiting the precision of diagnostic classification and nuanced exploration of symptom combinations within each ODD symptom group. Screening measures also do not capture the persistence or stability of symptoms over time, which is necessary for formal diagnosis, and may therefore be overly sensitive, potentially producing false positives. In addition, the study relied on parent-report measures; although parent report of child symptoms is common and informative for children in the study age range (5–12), parent reports may be subject to bias and may not fully capture children’s internal experiences or behaviors across settings.
Conclusions and Future Directions
Taken together, the findings provide new insight into the heterogeneity of ODD and its overlap with CD, highlighting meaningful differences in both child psychopathology and parenting across groups. These results underscore the importance of comprehensive assessment and the need for intervention approaches that move beyond a one-size-fits-all model. Future research should build on this work in several ways. Longitudinal studies have shown that early ODD predicts both later conduct problems and internalizing symptoms, and that distinct ODD symptom dimensions carry differential risk: affective/irritable symptoms are linked to later depression and anxiety, whereas defiant/oppositional behaviors predict conduct problems (Burke et al., 2005, 2010; Lavigne et al., 2014; Loeber & Burke, 2011) Building on this literature, future studies could examine how the symptom patterns identified here, particularly distinctions between ODD-only versus ODD plus CD presentations, interact with early parenting, child emotion regulation, and comorbid internalizing symptoms to shape developmental trajectories. Intervention studies should test tailored approaches that differentiate between children with ODD only and those with ODD and CD to determine whether precision in targeting leads to improved outcomes. In addition, more work is needed to understand how cultural and contextual factors shape symptom presentation, parenting practices, and treatment response, ensuring that interventions are both effective and applicable across diverse populations.
Footnotes
ORCID iDs
Ethical Considerations
University of Pittsburgh IRB study number: STUDY23100020, approval date: 10/20/2023.
Consent to Participate
The Institutional Review Board (IRB) at the University of Pittsburgh waived written informed consent due to the nature of the data used for this study (i.e., survey-based).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant to the last author from NIH / NICHD (R01HD108140).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data will be made available upon request from the corresponding author with an appropriate inter-institutional data use agreement at the conclusion of the grant award period.