
Abstract
Background
The Assessment Checklist for Adolescents Plus (ACA+) is a 30-item caregiver-report mental health and relational strengths measure, containing items that are the converse of maltreatment-related mental health and relational difficulties measured by the Assessment Checklist for Adolescents (ACA) and its short form (ACA-SF). The present study is the first to investigate the ACA+’s content validity and factor structure.
Methods
ACA+ and ACA-SF scores were obtained for 220 adolescents (50.9% boys), aged 12-18 years, living in residential out-of-home care (OOHC) in the UK. Item validity was estimated from item score distributions (item means and prevalence), and correlations with ACA+ total and ACA-SF scale scores. Factor structure was investigated using principal components factor analysis.
Results
As anticipated, all item-rest correlations were positive (r = .20 to .58), while correlations with the ACA-SF total score were all negative. However, items measuring emotion sharing and relational intimacy were positively correlated with several ACA-SF sub-scale scores, suggesting that among some adolescents these items measure maladaptive dysregulated emotion and relational difficulties. To maximise clinical utility, two sets of factor analyses were performed, yielding: a 21-item four-factor solution that can be safely interpreted by children’s agencies; and a 29-item six-factor solution that requires skilled interpretation by mental health clinicians. Factor analyses explained 53.9% and 75.1% of the score variance respectively.
Conclusions
The present analyses suggest the ACA+ has strong content and factorial validity for assessment of adolescents in residential OOHC. Further research is needed to establish its validity for use with adolescents in foster and kinship care.
Plain language summary
Background Adolescents in residential out-of-home care (OOHC) have high relationship and mental health difficulties. Clinical assessments mainly focus on symptoms rather than mental health strengths. But measuring young people’s mental health strengths can increase understanding of their treatment needs. The Assessment Checklist for Adolescents Plus (ACA+) is a list of 30 statements describing adaptive behaviours and mental health strengths that is completed by young people’s caregivers. The statements describe positive alternatives to mental health problems experienced by youth in OOHC, as measured by the Assessment Checklist for Adolescents (ACA) and its short form (ACA-SF). This study explored how well the ACA+ measures mental health strengths of adolescents in residential OOHC. Methods ACA+ and ACA-SF checklists were completed for 220 adolescents living in residential OOHC in the United Kingdom. The study investigated statistical relationships between mental health strengths and problems, and which strengths tend to co-occur with each other. Results The young people had high levels of mental health strengths, as well as difficulties. Individual strengths tended to co-occur with similar types of strengths. We found that some of the behaviours measured by the ACA+ were positive and adaptive for some young people but were possibly problematic for others. Conclusion The ACA+ checklists appear to accurately measure mental health strengths in this population. A shorter version with 21 questions and four scales (measuring ‘regulated emotion’, ‘relational security’, ‘empathy’, and ‘sociability’) can be safely used by children’s agencies without clinical oversight. A longer version with 29 questions (measuring ‘regulated emotion’, ‘relational security / contentment’, ‘empathy’, ‘relational closeness’, ‘emotional sharing/help-seeking’, and ‘sociability’) requires skilled interpretation by mental health clinicians.
Keywords
Introduction
Children and adolescents residing in statutory out-of-home care (OOHC, including family-based foster care and kinship care, and residential care) constitute a highly disadvantaged and vulnerable population. Their early and chronic exposure to child maltreatment and other biopsychosocial adversities accounts for high levels and rates of mental health difficulties. Roughly half of such children have clinical-level mental health difficulties, and another quarter have difficulties approaching clinical significance (Engler et al., 2022; Oswald et al., 2010). Many manifest complex attachment- and trauma-related mental health and relational difficulties that are not well conceptualized within standard diagnostic classifications (DeJong, 2010; Tarren-Sweeney, 2021). These difficulties typically follow a long-term developmental course and have trait-like durability, such that children’s recovery tends to occur over much longer time periods than does recovery from more discrete, state-like disorders (Tarren-Sweeney & Goemans, 2019).
Identifying Early Signs of Mental Health Recovery
Most clinical and epidemiological studies carried out with this population measure their mental health using symptom checklists, notably the Achenbach Child Behavior Checklist (CBCL) and Youth Self Report (YSR) (Achenbach & Rescorla, 2001), and the Strengths and Difficulties Questionnaire (SDQ) (Goodman, 2001). These checklists measure numbers of symptoms and how often they are manifested, but not individual symptom severity. The symptom frequency timeframes are quite long – six months for the CBCL, YSR and SDQ. The lack of symptom severity measurement, and long measurement timeframes greatly constrains their ability to detect mental health changes over shorter periods – and hence, treatment sensitivity. Furthermore, measuring mental health improvement exclusively in terms of reduced symptoms and symptom frequency only tells half of the story. Recovery from maladaptive mental health difficulties is also demonstrated by increasing manifestations of adaptive behaviours, emotions, thoughts and relational styles that indicate normative psychological functioning – which can be termed mental health and relational strengths. For example, recovery from Reactive Attachment Disorder (RAD) can be measured not just from reductions in inhibited social interactions, but also from an increase in spontaneous affection towards family members. It is important to emphasize that recovery from maltreatment-related mental health difficulties does not, at least initially, involve a net replacement of maltreatment-related difficulties (symptoms) with strengths (the opposing and desired behaviours). Instead, foster carers often describe the earliest signs of recovery as their child displaying positive ‘uncharacteristic’ behaviours that surprise their carers (e.g. spontaneous, unsolicited affection), without necessarily observing a reduction in the converse problem behaviours (Tarren-Sweeney, 2014b).
Measuring Mental Health Strengths of Children and Adolescents in OOHC
While there are several measures of general psychological strengths that are potentially suitable to include in mental health and relational assessments of children and adolescents in OOHC (Day et al., 2022), very few explicitly measure mental and/or relational health. The Child and Adolescent Strengths Assessment (CASA) is a 30-item measure of psychological strengths designed to assist mental health service planning and delivery (Lyons et al., 2000). Strengths are assessed on six dimensions (family; school/vocational; psychological; peer; moral/spiritual; extracurricular). However, the domains and items don’t appear to explicitly measure positive mental health or indications of recovery. The SDQ includes a 5-item general prosocial behaviour sub-scale (along with four mental health symptom scales). The SDQ’s prosocial sub-scale appears to be the only strengths measure that is regularly included in clinical and epidemiological studies of young people in OOHC (Goemans et al., 2018; Goodman et al., 2004). The BERRI is a caregiver-report questionnaire designed to measure the mental health and well-being of children and adolescents in OOHC across five domains: Behaviour; Emotional wellbeing; Risk (to self and others); Relationships; and Indicators (of psychiatric or neurodevelopmental conditions) (Harris, 2019; Silver, 2025). Twenty strengths items were recently added to BERRI (personal communication with the developer).
The Assessment Checklist for Adolescents – Plus (ACA+) and the Assessment Checklist for Children – Plus (ACC+), are corresponding 30-item caregiver-report strengths measures for ages (12-18) and (ages 4-11) respectively. Their items were derived deductively, with a view to measuring adaptive behaviours, thoughts, emotions and relational styles that are the direct converse to maltreatment-related mental health and relational difficulties – as measured by the caregiver-report Assessment Checklist for Adolescents (ACA) and Assessment Checklist for Children (ACC) (Tarren-Sweeney, 2014a). The ACA+ and ACC+ share 27 items, with each checklist having only three unique items. The checklists employ a 4-point response scale (Never = 0; Rarely = 1; Sometimes = 2; Often = 3). The ACA+ and ACC+ have been distributed with the ACA and ACC checklists to licensed clinicians since 2016. To date however, neither the ACA+ or ACC + has been formally developed or validated.
While no research data have been published for the ACA+, two studies have published data for the ACC+. The first is a longitudinal study of mental health, attachment security and psychological strengths among children and adolescents in a therapeutic foster care programme in Ontario, Canada (N = 555) (Smith et al., 2022, 2024). The study commenced prior to development of a separate ACA+ measure, and the ACC+ was therefore used for both children and adolescents. Children in permanent foster placements had significantly higher ACC+ strengths scores than children in non-permanent placements, while there was no significant difference in ACC+ scores between adolescents in permanent versus non-permanent placements (Browne et al., 2019). Using growth curve and random intercepts cross-lagged panel models, the study found that: (1) whilst girls’ attachment security improved and boys’ attachment security worsened over time, both boys and girls ACC+ strengths increased over time; and (2) fewer insecure attachment behaviours predicted higher ACC+ strengths six months later (Smith et al., 2024).
The second study evaluated a group-based parenting programme for adoptive parents of UK children aged 2 to 8 years, who had been adopted from OOHC (Harold et al., 2017). The study measured 2-year pre-post changes in children’s mental health strengths and difficulties among an evaluation sample (N = 93), and a subsequent pilot sample (N = 157), using the ACC+, the Assessment Checklist for Children – Short Form (ACC-SF) (Tarren-Sweeney, 2014a) and the SDQ (Goodman, 2001). The study measured significant reductions in ACC-SF and SDQ total mental health difficulties scores (Cohen’s d = .43 and .21 respectively), and a significant improvement in ACC+ mental health strengths scores (d = .22) (Harold et al., 2017).
Background to the Present Study
The present study was conducted by the psychology service of the Keys Group, which is a large private provider of residential out-of-home care (OOHC) in England and Wales, in collaboration with two university researchers. Prior to this, the psychology service conducted a systematic review of strengths-based mental health measures appropriate for assessment of young people in residential OOHC (Day et al., 2022). The review concluded that the most suitable measures for routine assessment of this population were the ACA+ and the ACA/ACA-SF. Whereas the ACA and ACA-SF are formally developed measures with evidence of good content, construct and criterion-related validity, and high internal reliability (Tarren-Sweeney, 2014a), the review noted that the ACA+ “… is yet to be psychometrically researched. Further research is needed to assess the psychometric properties of the strengths-based supplementary checklist and to understand if this can be used as a standalone measure, or only in conjunction with the ACA” (Day et al., 2022). Following on from the systematic review, the provider’s psychology service included the ACA-SF and ACA+ in their standard assessment protocol, with a plan to evaluate their utility and accuracy with respect to their client group.
Given the need for validated mental health strengths measures suitable for routine assessment and monitoring of mental health recovery in adolescents living in OOHC, and the unique access to data from a large sample of adolescents living in residential OOHC in England and Wales, the current study therefore aimed to: (1) investigate the content validity and factor structure of the ACA+ strengths items among adolescents in residential OOHC; and (2) learn more about the levels of, and relationship between, mental health/relational problems and strengths in adolescents living in residential OOHC.
Method
Participants and Setting
Caregiver-reported ACA-SF and ACA+ checklist scores were routinely collected over an 8-month period (December 2022 to July 2023) for all adolescents (age 12 to 17) residing in 105 group homes in England and Wales, as part of their standard psychological assessments. Residents were young people accommodated by the statutory social care authorities and considered “children looked after”. Homes accommodated one to six young people. All young people had experienced maltreatment and other social adversity prior to entering care.
ACA+ and ACA-SF data were collected for 220 adolescents; 112 boys (50.9%) and 96 girls (43.6%), with gender not reported for 12 participants. Their mean age was 14.8 years (range 11.9 to 17.8 years), with boys’ and girls’ having similar mean ages (14.7 and 15.0 years respectively). Mean age at entry into the current OOHC event (i.e. excluding previous entries into OOHC) was 13.0 years (range 6.5 to 17.8 years).
Procedure
In accordance with the service assessment protocol, assessments of newly placed young people were carried out after they had spent at least 10 weeks in their new placement; to ensure carers had adequate time to gain enough knowledge and understanding of the child to reliably respond to the checklist items. Checklists were administered verbally by assistant psychologists in face-to-face or video interviews with the young person’s care team. The care team included those staff who routinely supported the young person within the home on a daily basis and were well known to them. The assistant psychologists entered checklist item scores on a central data spreadsheet, as well as the young person’s date of birth, date of entry into care (present care event), and gender.
ACA+ Item Pool
Unpublished ACA+ Item Pool With Corresponding ACC/ACA Mental Health Difficulties Scales
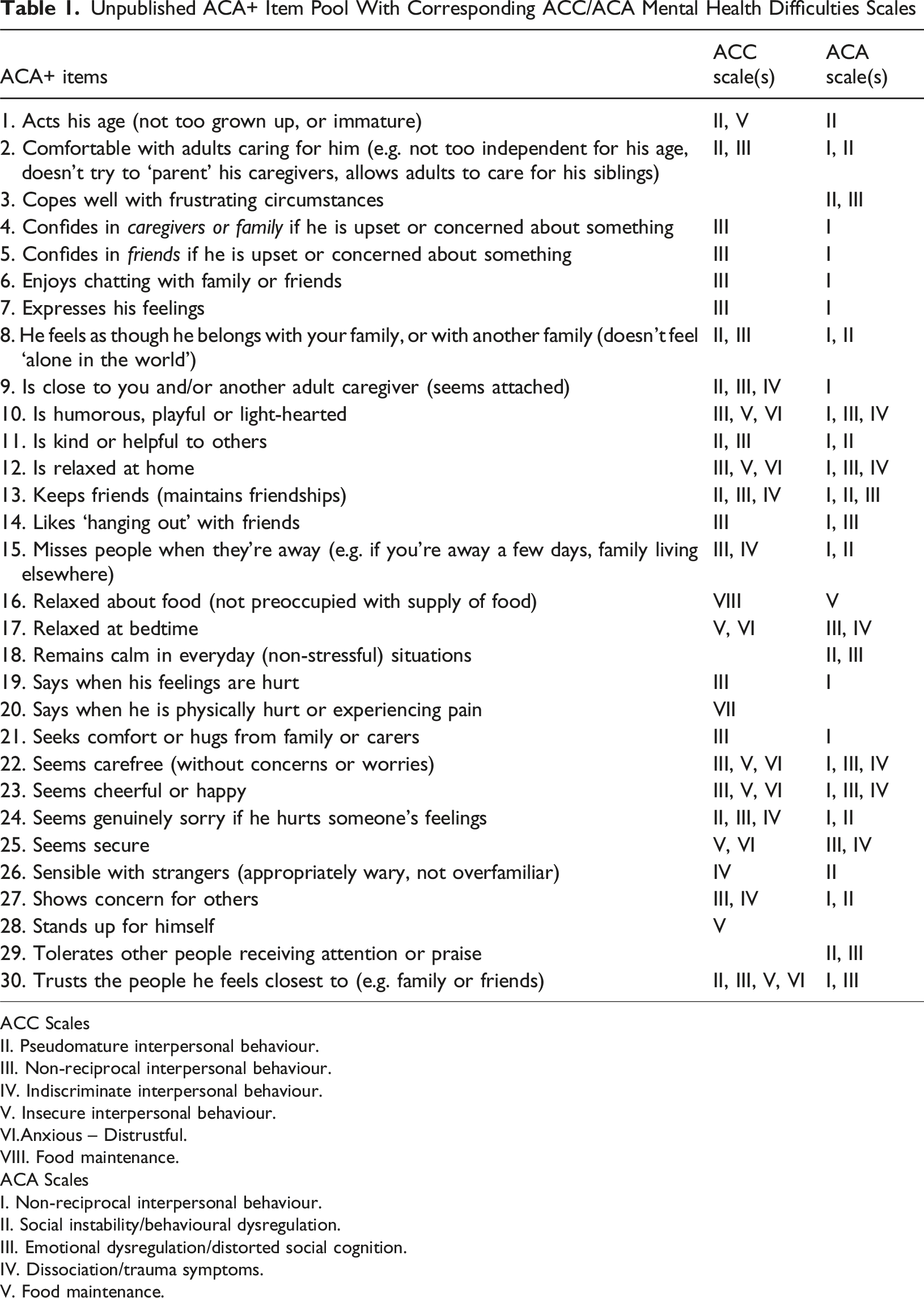
ACC Scales
II. Pseudomature interpersonal behaviour.
III. Non-reciprocal interpersonal behaviour.
IV. Indiscriminate interpersonal behaviour.
V. Insecure interpersonal behaviour.
VI.Anxious – Distrustful.
VIII. Food maintenance.
ACA Scales
I. Non-reciprocal interpersonal behaviour.
II. Social instability/behavioural dysregulation.
III. Emotional dysregulation/distorted social cognition.
IV. Dissociation/trauma symptoms.
V. Food maintenance.
ACA-SF
The 37-item ACA-SF and 105-item ACA are caregiver-report mental health rating scales that measure problem behaviours, emotional states, traits, and manners of relating to others, as manifested by adolescents (ages 12 to 17) residing in various types of alternate care, as well as those adopted from care (Tarren-Sweeney, 2014a). They were designed to measure a range of maltreatment-related mental health and relational difficulties experienced by adolescents in OOHC that are not measured by generic checklists such as the CBCL and SDQ. Whereas the ACA is designed for comprehensive mental health assessments, the ACA-SF was designed for use as a brief assessment and monitoring tool. In addition to a total clinical score, the ACA-SF has six clinical sub-scales derived through factor analysis, labelled: Non-reciprocal (NR); Social Instability (SI); Emotional Dysregulation/Distorted Social Cognition (ED/DSC); Dissociation/Trauma Symptoms (D/TS); Food Maintenance (FM); and Sexual Behaviour (SB). The ACA-SF was employed in two recent studies of young people in residential OOHC (Eadie et al., 2020; Maneiro et al., 2025).
Statistical Analysis
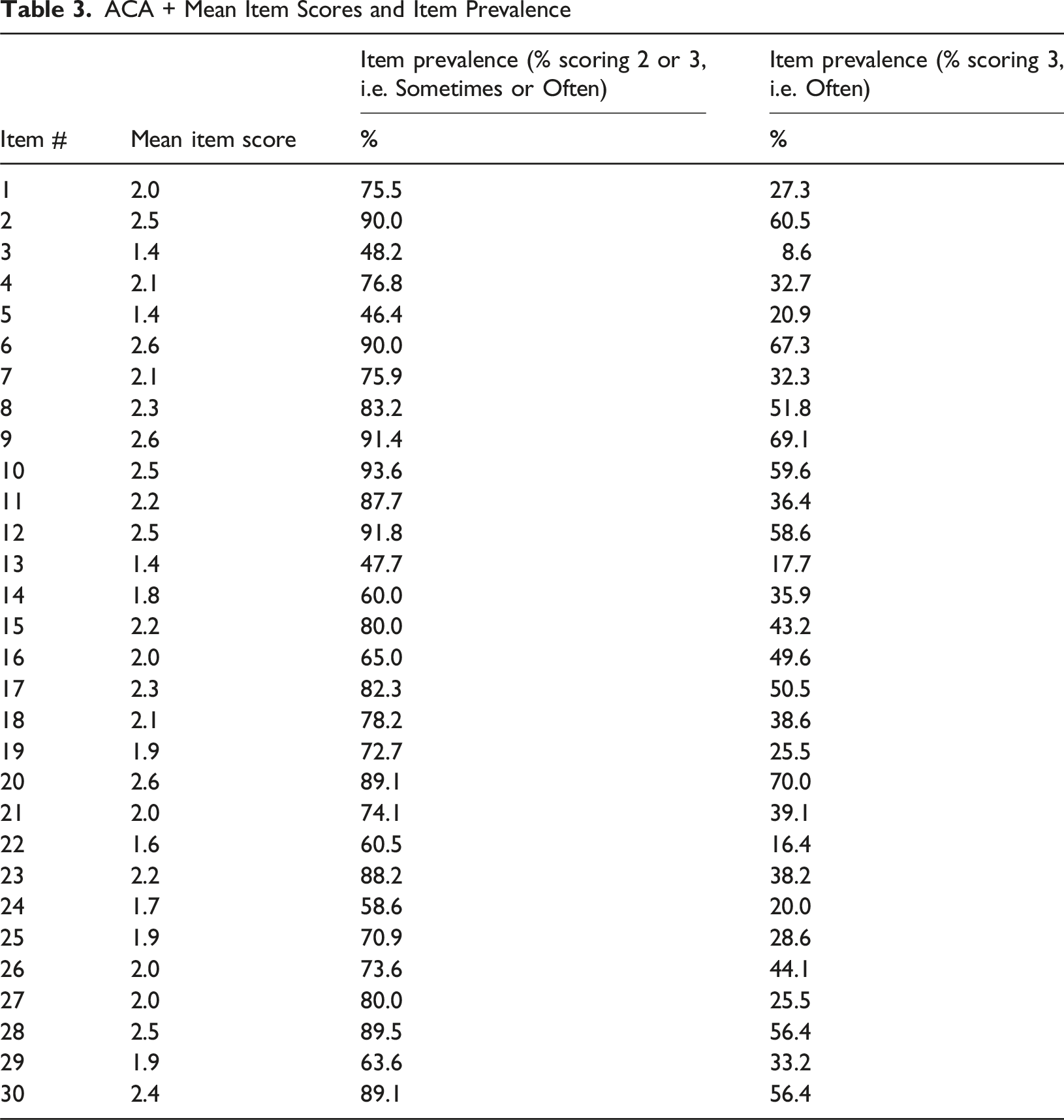
Item prevalence rates were calculated for two dichotomous variables: item prevalence defined by a score of 3 (occurs ‘often’); and item prevalence defined by a score of 2 or 3 (occurs ‘sometimes’ or ‘often’). Item-rest correlations (Pearsons r) were calculated, with rest scores being nominal total scores (sum of 30 item scores) minus the relevant item score. Correlations were also calculated for the ACA+ items with the ACA-SF total and sub-scale scores (excluding the ‘sexual behaviour’ scale, since no ACA+ items align with it). For the purpose of item analysis, well-performing strength items should be at least moderately, negatively correlated with mental health difficulties items. Principal components factor analyses of retained ACA+ items were performed in STATA 16 (StataCorp, 2019), using the same factor analysis procedure used to develop the Assessment Checklist measures (Tarren-Sweeney, 2014a).
Ethics Approval
The study data were routinely collected within standard psychological assessments of young people residing in the Keys Group residential homes. Use of anonymised data for the current research study was approved by the Keys Group’s internal ethics committee. All procedures performed were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Results
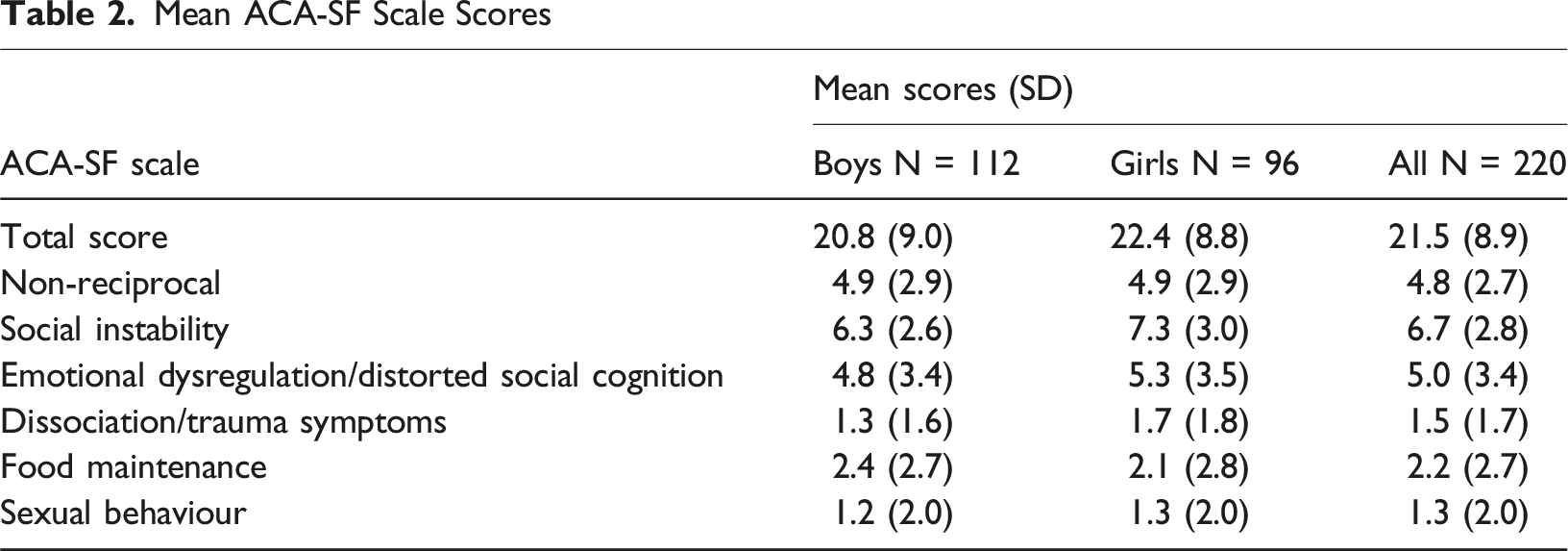
Level of Mental Health Difficulties
Mean ACA-SF Scale Scores
Item Analysis
Item Means and Prevalence
ACA + Mean Item Scores and Item Prevalence
Item Correlations
Item Correlations (Pearsons r) With ACA+ Rest Scores, and With ACA-SF Total and Sub-scale Scores
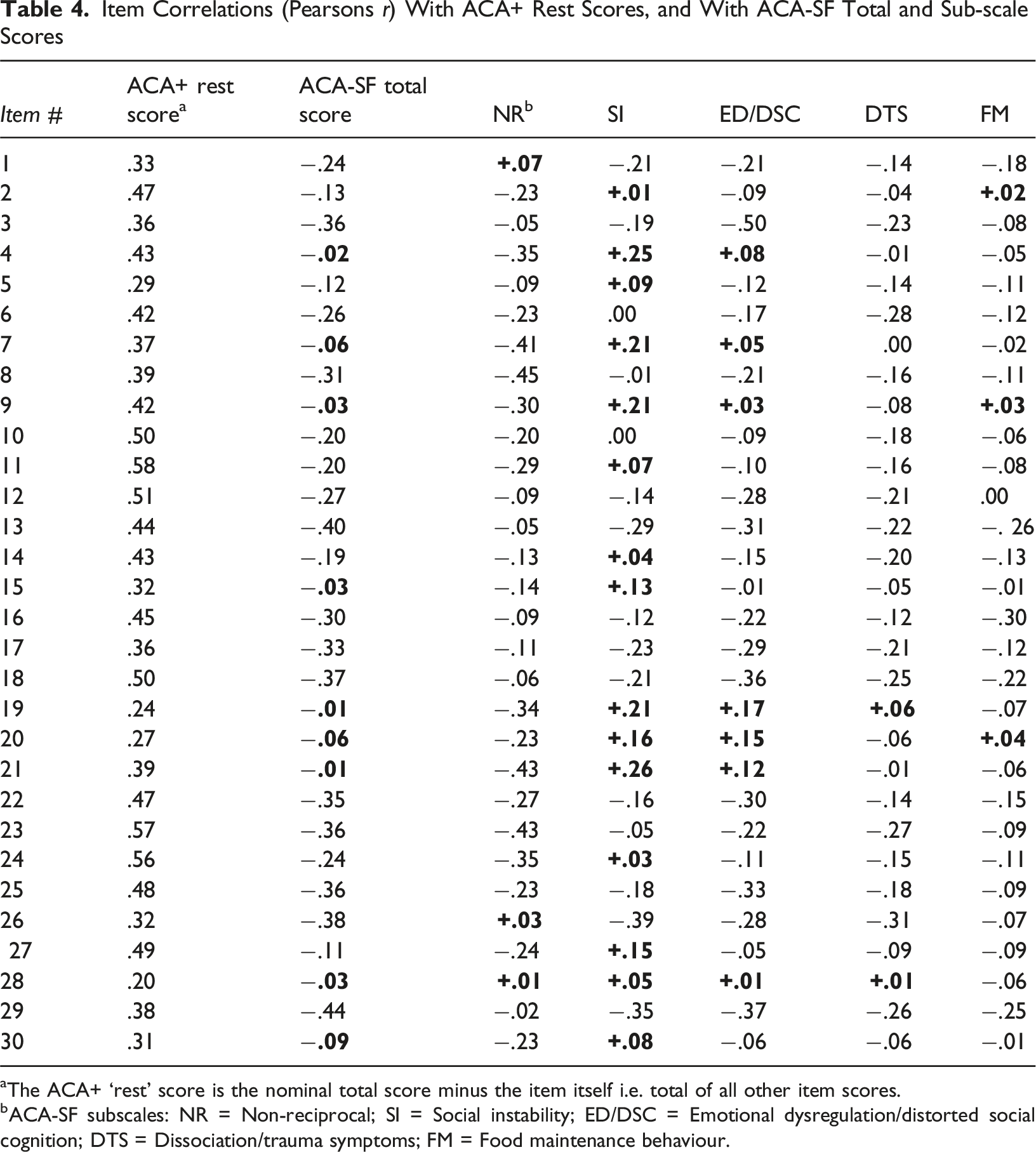
aThe ACA+ ‘rest’ score is the nominal total score minus the item itself i.e. total of all other item scores.
bACA-SF subscales: NR = Non-reciprocal; SI = Social instability; ED/DSC = Emotional dysregulation/distorted social cognition; DTS = Dissociation/trauma symptoms; FM = Food maintenance behaviour.
Item Retention for Factor Analyses
Item 28 ‘Stands up for him/herself’ had the lowest item-rest correlation and was positively correlated with most ACA-SF sub-scales. While this behaviour can suggest mental health recovery or adaptive coping in a residential setting for some youth, it can also measure maladaptive aggression among others. The item was therefore excluded from further analysis. Item 16 ‘relaxed about food (not preoccupied with supply of food)’ is the only item designed to measure recovery from ‘Food Maintenance’ difficulties and was therefore withheld from the factor analyses.
Emotion Expression/Emotion Sharing/Relational Intimacy Items
Of the remaining 28 items, several that measure adolescents’ expressed emotions, emotion sharing, or relational intimacy were: (1) moderately, negatively correlated with the ACA-SF NR sub-scale; (2) positively correlated with the SI and (to a lesser extent) the ED/DSC sub-scales of the ACA-SF; and (3) weakly, negatively correlated (r < −.1) with the ACA-SF total score. This suggests those items measure behaviours that reflect mental and relational health for some young people in residential care, notably those with high non-reciprocal scores. Paradoxically, they may constitute mental and relational difficulties for others, particularly those with high SI and ED/DSC scores. We considered the potential clinical significance of each of these items and decided that item 27 (‘shows concern for others’) and item 30 (‘trusts the people he/she feels closest to’) are unlikely to represent maladaptive behaviour for adolescents with high SI and/or ED/DSC scores – whereas items 4, 5, 7, 9, 15, 19, 20 and 21 may do. We considered excluding the latter eight items from the factor analysis, to ensure any derived sub-scales measure unambiguous and easy-to-interpret strengths. However, there is clinical utility in retaining items that measure mental health recovery for socially withdrawn, relationally non-reciprocal youth in OOHC. Doing so would necessitate a more complex scoring and interpretation system, and restricted licensing to skilled clinicians (as is the case for the ACA). On the other hand, excluding those items from the factor analysis would ensure sub-scales that are relatively easy to score and interpret, and that could be safely used by agencies and caseworkers without clinical training or clinical oversight. We therefore conducted two exploratory factor analyses with a view to identifying two potential versions of the ACA+: a longer version that includes the emotion expression-sharing, and relational intimacy items; and a shorter version that excludes those items.
Factor Analysis of the Larger Item Pool (27 Items)
ACA + Factors/Sub-scales Derived From 27-Item Principal Components Factor Analysis: Sub-scale Internal Consistency and Sample Mean Scores, and Item Factor Loadings
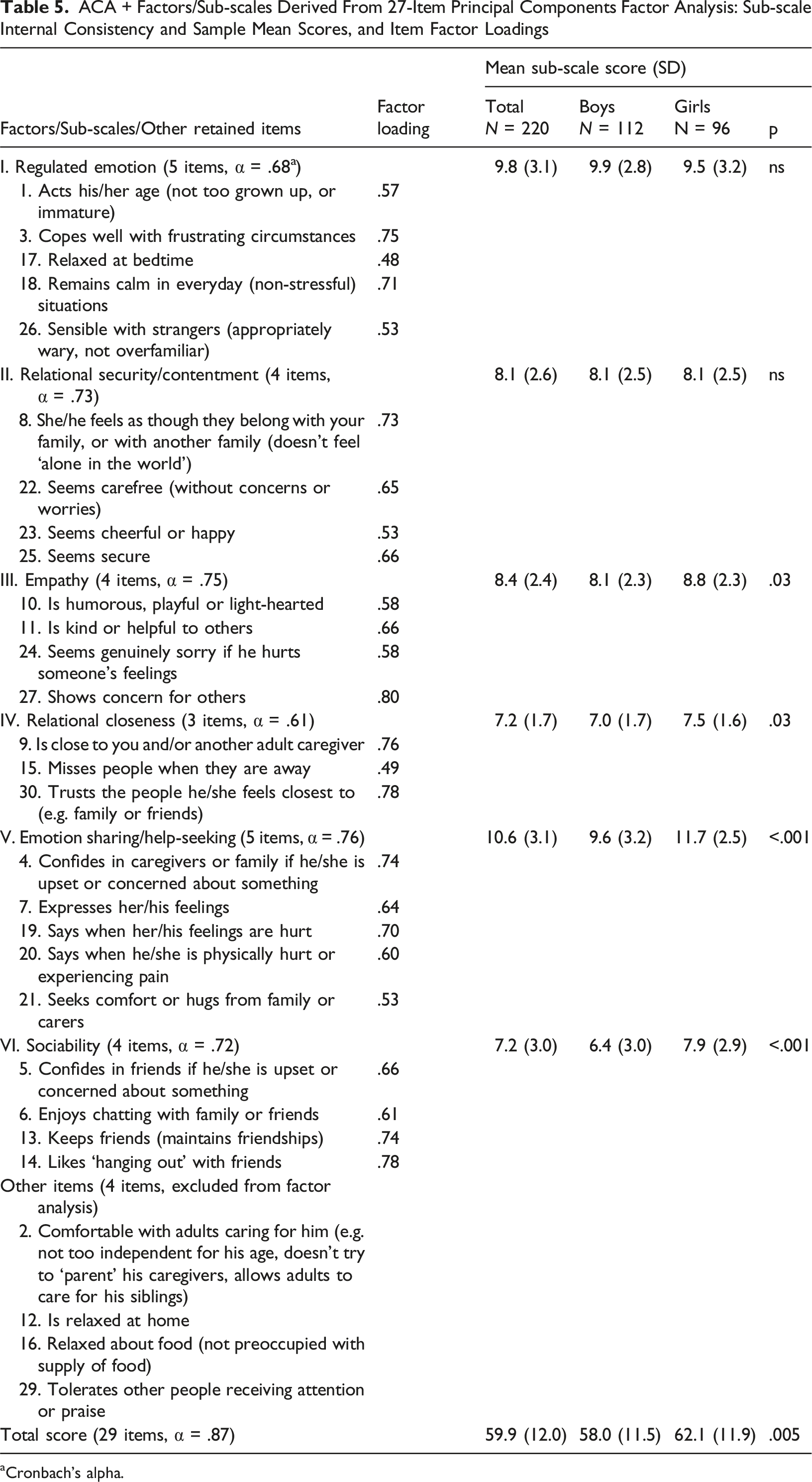
aCronbach’s alpha.
Factor Analysis of the Smaller Item Pool (19 Items)
ACA+ Factors/Sub-scales Derived From 19-Item Principal Components Factor Analysis (N = 220): Sub-scale Internal Consistency and Sample Mean Scores, and Item Factor Loadings
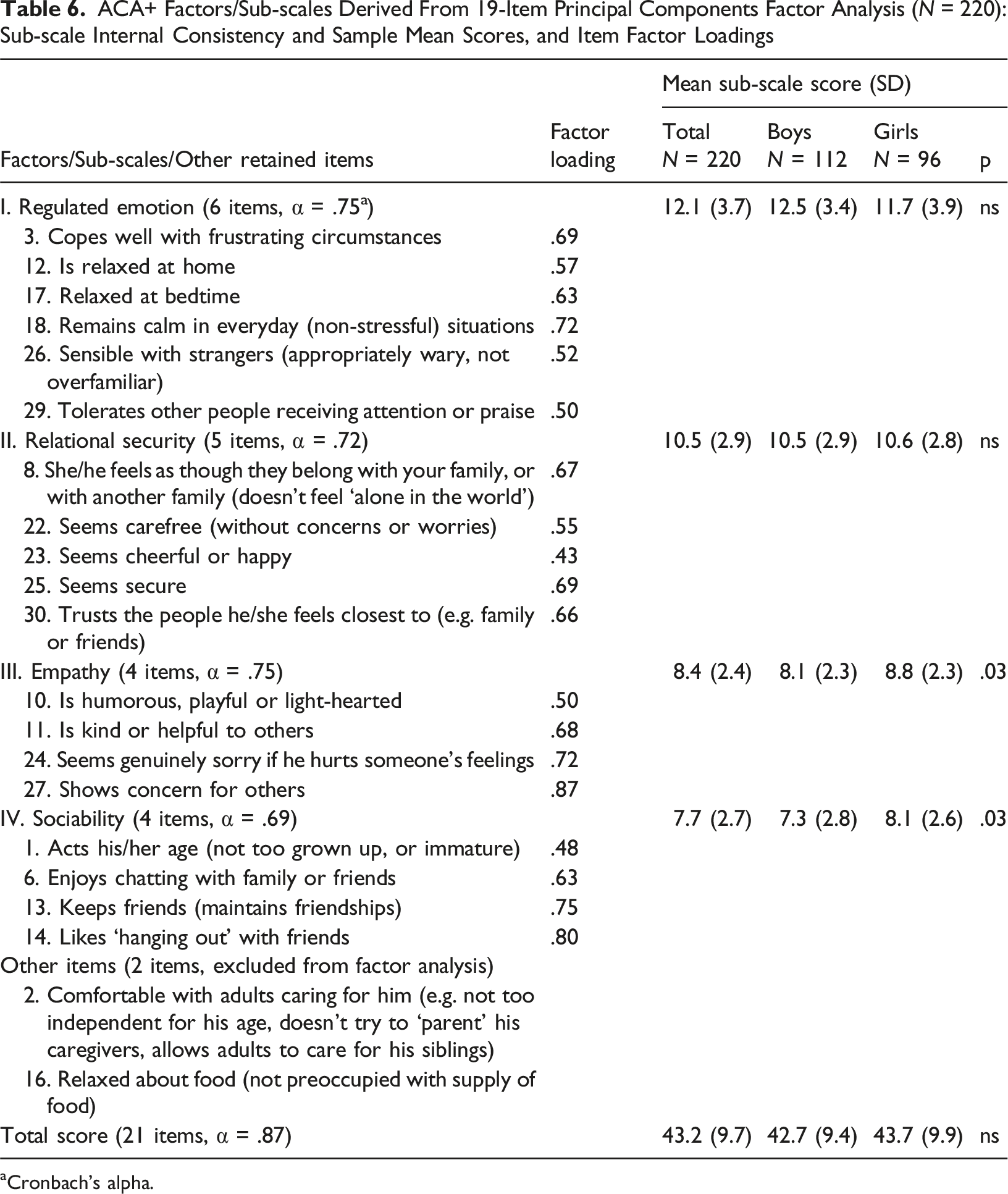
aCronbach’s alpha.
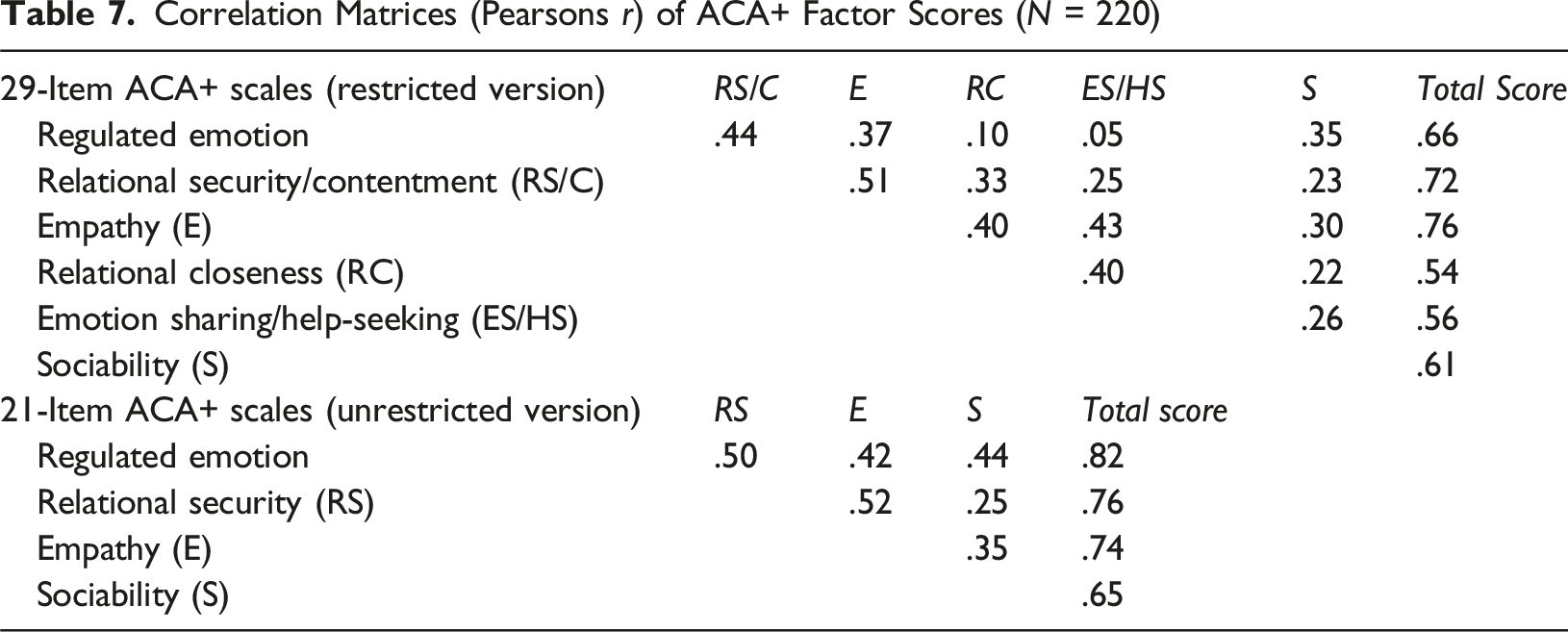
Inter-scale Correlations
Correlation Matrices (Pearsons r) of ACA+ Factor Scores (N = 220)
Correlation Matrix (Pearsons r) of ACA+ and ACA-SF Scale Scores (N = 220)
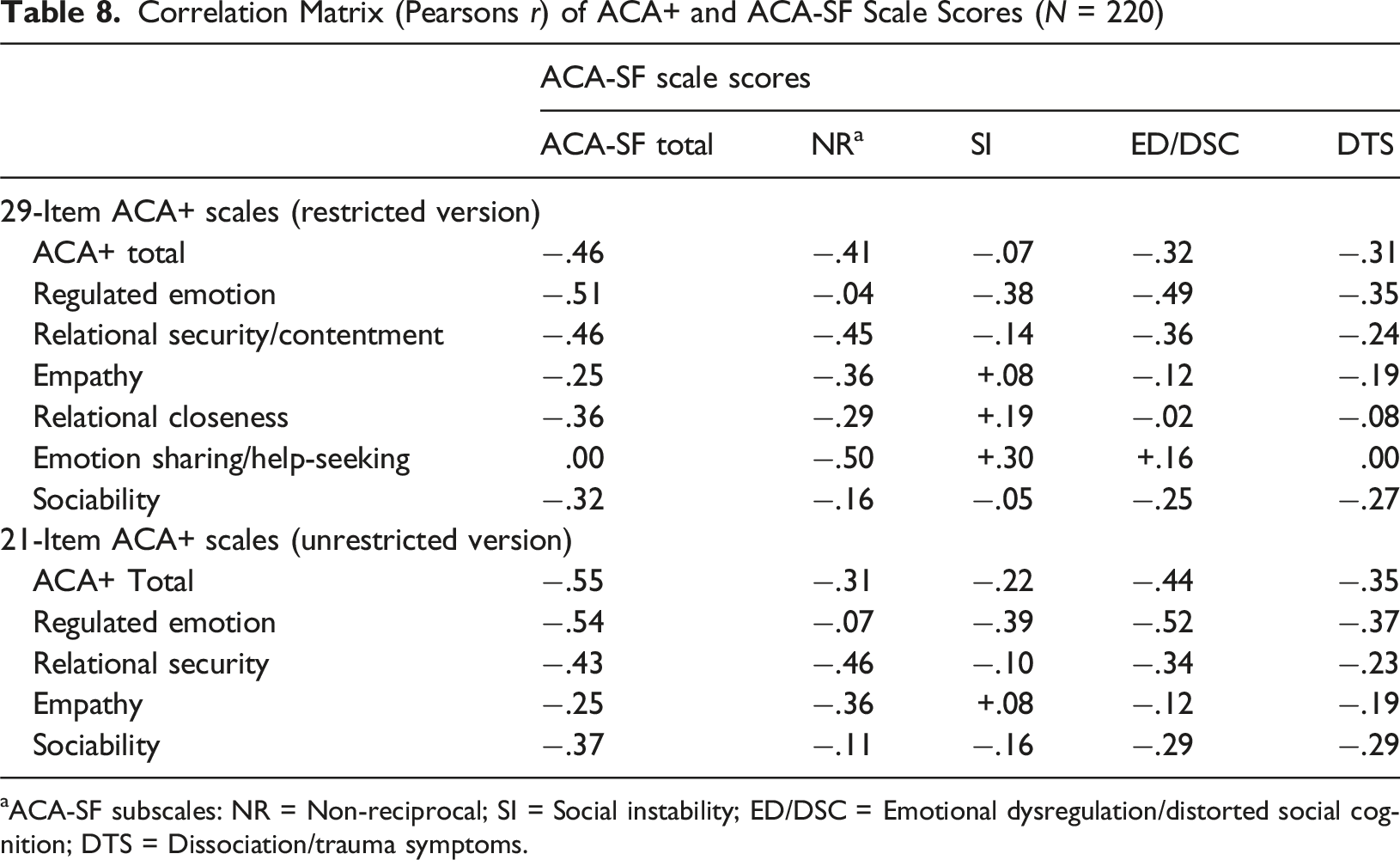
aACA-SF subscales: NR = Non-reciprocal; SI = Social instability; ED/DSC = Emotional dysregulation/distorted social cognition; DTS = Dissociation/trauma symptoms.
Discussion
The present study found that mental health strengths (as reported by caregivers) are highly prevalent in this high-risk sample. The present analyses provide initial empirical support for the item and factorial validity of the ACA+ mental health strengths items, yielding: a 21-item four-factor solution for general use by children’s agencies; and a 29-item six-factor solution that requires symptom-specific differential interpretation of sub-scale scores by mental health clinicians. Both versions demonstrate strong factorial validity, with the factor solutions explaining 53.9% and 75.1% of the score variance respectively.
The item analysis and inter-scale correlations identified a paradox, whereby some behaviours, thoughts and feelings likely indicate mental health and relational strengths for some young people, versus difficulties for others. In other words, some items are contextualised to the nature of a young person’s difficulties. In the present analysis, several ACA+ items measuring adolescents’ emotion expression, emotion sharing or relational intimacy were moderately, negatively correlated with the ACA-SF NR sub-scale, but positively correlated with the ACA-SF SI and (to a lesser extent) the ED/DSC sub-scales. This is borne out further in the inter-scale correlations. Three of the 29-item version sub-scale scores (empathy; relational closeness; emotion sharing/help-seeking), as well as the 21-item version ‘empathy’ sub-scale score, were positively correlated with the ACA-SF SI scale. Conversely, the ACA+ regulated emotion subscale was only weakly negatively correlated with the ACA-SF NR scores, but moderately negatively correlated with the remaining ACA-SF scale scores. Adolescents with high NR scores tend to be socially withdrawn and non-relational, and in some instances manifest signs of Reactive Attachment Disorder (RAD) (Tarren-Sweeney, 2013). For them, increased social-emotional expression and relational behaviours are unambiguously positive. However, whereas high ‘regulated emotion’ scores probably reflect a mental health strength for most young people, they are less likely to indicate recovery for those with high NR scores. Conversely, young people with high SI, and to a lesser extent ED/DSC, may manifest excessive and dysregulated emotions, an intensely insecure relational style, pseudomaturity, and/or signs of Disinhibited Social Engagement Disorder (DSED) (Tarren-Sweeney, 2014a). For these young people, high scores on ACA+ ‘relational closeness’ and ‘emotion sharing/help-seeking’ scales may partially reflect dysregulated emotion and/or relational difficulties. These results highlight why a 29-item version of ACA+ will require a detailed scoring and interpretation procedure that is restricted to qualified clinicians.
The present study results suggest that adolescents living in residential OOHC in the UK have considerable levels of mental health difficulties, with no differences between the sexes. The distribution of mental health difficulties is consistent with the type of care and child protection jurisdiction in which they reside – namely that residential care is largely reserved in the UK for those young people who are most difficult to place or retain in family-based care. They had roughly double the mean ACA-SF scores of the Australian CICS foster care sample (Tarren-Sweeney, 2014a), and of a ‘going well’ sub-sample of UK adolescents adopted from OOHC (Selwyn et al., 2014). Their mean ACA-SF scores were a little higher than those obtained for a sample of Spanish youth in residential care (Maneiro et al., 2025), which is consistent with a much greater proportion of Spanish OOHC youth being placed in residential care (44% in Spain, versus 11% in the UK) (Del Valle & Bravo, 2013). However, they had lower mean ACA-SF scores than that of an Australian clinic-referred sample (Eadie et al., 2020), and that of an ‘experiencing major difficulties’ sub-sample of UK adolescents adopted from OOHC (Selwyn et al., 2014).
A strength of the study design is that scores were obtained for all adolescents residing in the provider’s residential homes over an 8-month period. However, a limitation of the study is that the score data were collected within a single provider’s care homes, and the extent to which those young people are representative of the broader residential care population in England and Wales is not known. A second limitation is that the item validity and factor structures identified among the present sample’s ACA+ scores may not generalize to young people in family-based (foster and kinship) OOHC. Further research is needed to establish the extent to which these two proposed measures are valid for adolescents in foster care, or those adopted from OOHC.
In conclusion, the present analyses provide data for formal development of two versions of the ACA+ that are suitable for assessing the mental health and relational strengths of adolescents residing in residential care homes: an unrestricted 21-item checklist with four sub-scales that can be safely used and interpreted by care services; and a 29-item checklist with six sub-scales that will need to be administered and interpreted in conjunction with the ACA or ACA-SF by mental health clinicians.
Footnotes
Acknowledgments
The authors gratefully acknowledge the invaluable support and cooperation of Keys Group, a national provider of residential care in the UK, in facilitating their research. We are particularly indebted to the children’s residential clinical team at Keys Group and in particular, to Matilda Steele, Assistant Psychologist, for their crucial assistance in setting up the original database used in this study. Their dedication was fundamental to the data collection process and the successful completion of this study. Without their collaboration and generous access to their facilities and participants, this research would not have been possible.
Ethical Considerations
The study data were routinely collected within standard psychological assessments of young people residing in Keys Group children’s residential homes. Use of anonymised data for the current research study was approved by the Keys Group’s internal ethics committee. All procedures performed were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
There is no approval to share the study data.