
Abstract
Psychiatric admission for youth can be a highly stressful experience for caregivers. Groups are one form of caregiver support in the inpatient setting, though evidence is limited. We conducted a needs assessment survey of caregivers of psychiatrically hospitalized children and adolescents to better understand caregiver support needs and their interest in participating in groups. Of 78 caregivers, individualized care plan information was the most frequently received and desired support. 51% reported being extremely likely to attend a caregiver group on parenting skills. Groups were also rated the most helpful among other evidence-based forms of caregiver supports (n = 22; 50%). Most frequently reported barriers to group include travel, work, and time. In conclusion, while their child’s individualized care plan information remains the priority, many caregivers still identify groups as an important form of inpatient support though may face various logistical barriers.
Plain Language Summary
Having one’s child be hospitalized for a mental illness can be a highly stressful experience for caregivers. Caregiver groups are one way to support caregivers while their child is admitted, although this type of support has not been well-tested for this type of situation. We conducted a needs assessment survey with caregivers whose child was admitted to a psychiatric hospital, to better understand what their perceived needs are and how to support them. We also asked about their interest in participating in caregiver groups. Of 78 caregivers, at least 80% reported receiving individualized care plan information, which was also the most frequently desired support. Still, 51% reported being extremely likely to attend a caregiver group to learn parenting skills. Among other tested interventions to support caregivers such as groups, 1:1 support, website of shared experiences, and a parenting handbook, groups were rated the most helpful ( n = 22; 50%). Most frequently reported barriers to attending groups included travel, work, and time. In conclusion, while their child’s individualized care plan information remains the priority, many caregivers still find groups as a valuable form of support while their child is hospitalized, although they may face various logistical barriers to participating.
Introduction
Caregivers of children and adolescents with mental illness play a crucial role in their child’s treatment and recovery. They also face significant caregiver burden, particularly during an acute mental health crisis necessitating psychiatric hospitalization. Psychiatric admission for a child or adolescent can be a highly stressful experience for caregivers, marked by embarrassment, guilt and shame, helplessness, and exhaustion (D’Angelo et al., 2023; Merayo-Sereno et al., 2023). Research suggests caregivers may benefit from their own resources and support when their child is in acute psychiatric care (D’Angelo et al., 2023).
Few robust evidence-based interventions have been tested to support caregivers during their child’s psychiatric hospitalization (Hsiung et al., 2025). While some inpatient interventions for caregivers have been explored, including individualized peer support, personalized assessments, groups, and websites with shared experiences, studies have largely consisted of small, non-randomized samples, with significant variations in goals and structure (Hsiung et al., 2025; Sternbeck-Rutter et al., 2025). Further, limited research gives voice to caregivers to understand their support preferences during this challenging time.
One tested inpatient intervention is caregiver groups. Groups offer a space for both emotional and practical support and may more efficiently reach multiple caregivers at once. Inpatient caregiver groups have shown to support paternal self-efficacy, increase understanding of sibling impacts, and decrease anxiety and stress (Mestermann et al., 2023; Rubin et al., 2018; Sharma et al., 2022). Yet, these studies include only those caregivers willing to participate in a group and cannot be generalized to all caregivers of psychiatrically hospitalized youth.
The purpose of this exploratory study was to conduct a needs assessment survey with caregivers to better understand their support needs during their child’s psychiatric hospitalization. This study also aimed to understand caregivers’ interest in participating in groups while their child was hospitalized, including preferences for group timing, focus, and structure.
Methods
Setting
This study took place on the child (ages 4–12) and adolescent units (ages 13–17) in a psychiatric hospital of an academic medical center in the Southeastern United States. The units total 30 beds, with an average hospital stay of 7 days. On admission, nursing staff orient caregivers to unit procedures. On the first full hospital day, patients are assigned a treatment team consisting of a social worker, an attending child and adolescent psychiatrist, and often a psychiatry resident or fellow, who contact caregivers for an intake assessment and discussing treatment goals. Family visitation is permitted during scheduled one-hour times every midday and evening. A family meeting with the child and their caregiver(s) is typically held on the day of discharge to review treatment, safety plan, and next steps post-discharge.
Participants
Seventy-eight adult caregivers (ages 18+) of psychiatrically hospitalized child and adolescent patients were recruited for the survey. Caregivers were considered those with an active caregiving role in the patient’s life as identified by the treatment team, often the primary point of contact during hospitalization, and must live in the residence(s) to which the patient would discharge. Caregivers were excluded if (1) their child was discharging to another inpatient or residential facility, (2) their child discharged against medical advice, (3) they were designated by the Department of Children’s Services, or (4) they had insufficient English literacy for survey participation.
Caregiver and Child/Adolescent Demographics
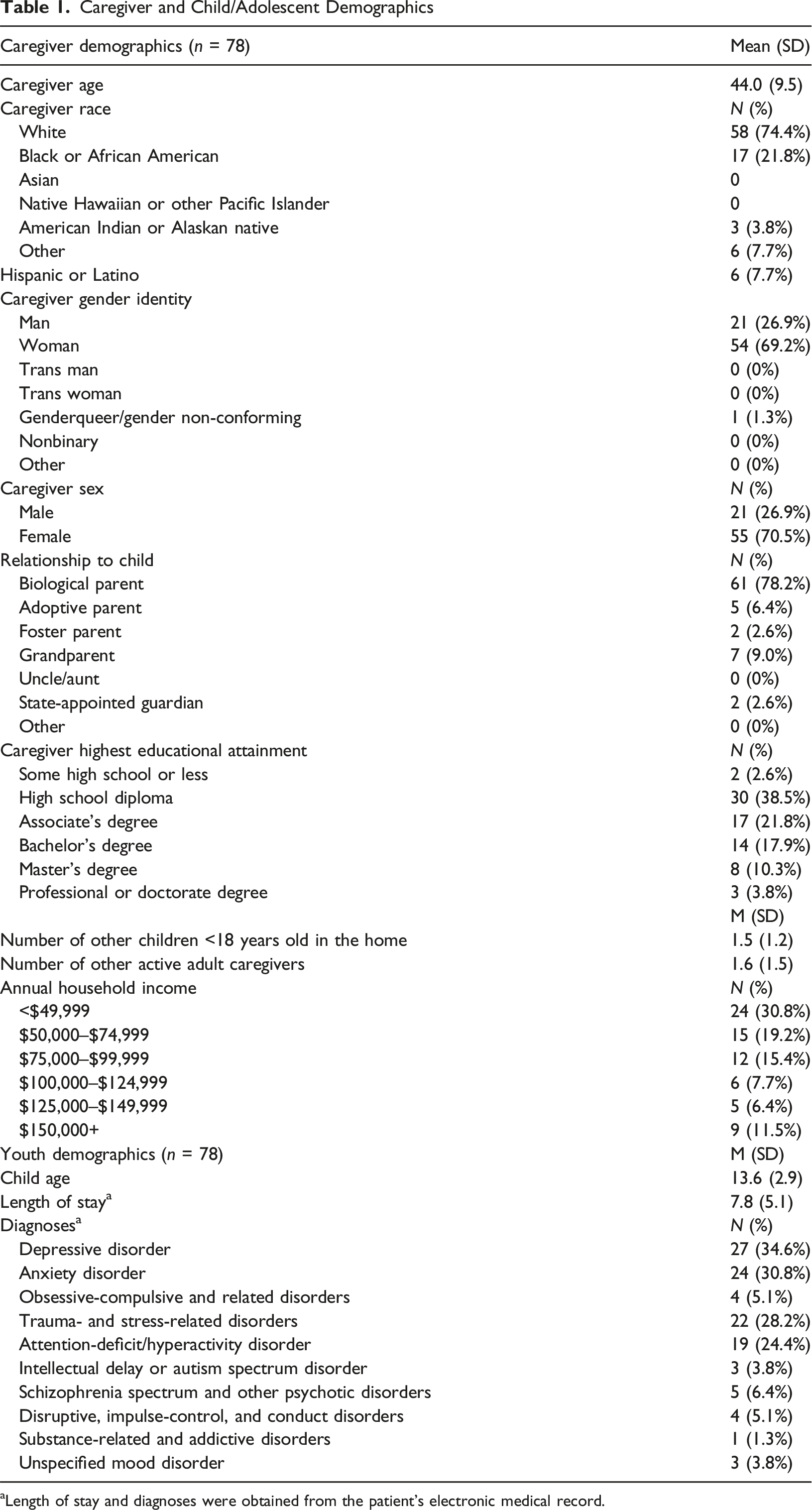
aLength of stay and diagnoses were obtained from the patient’s electronic medical record.
Needs Assessment Survey
The survey was developed in collaboration with authors KH, KG, JE, AB, and BR, all of whom have diverse expertise in the inpatient setting and/or working with caregivers. All inpatient child and adolescent clinical social workers then reviewed the survey for additional feedback and revision.
Informed consent was obtained by all participants before survey administration. The survey first assessed supports that caregivers received during their child’s current hospitalization (“received supports”) and their level of satisfaction with each on a 6-point Likert scale. The survey also assessed supports caregivers would have additionally liked to receive (“desired supports”), by allowing up to four selections from a list. The survey also assessed likelihood of attending caregiver-specific groups during their child’s hospitalization and preferences on how it would be offered (i.e., timing, frequency, topics). This section included one open-ended item regarding barriers to attendance. Halfway through the study, an item was added asking caregivers to select up to two interventions they thought may be most helpful from a list, based on a newly published scoping review of caregiver interventions in the psychiatric inpatient setting (Hsiung et al., 2025). See Appendix 1 for the complete needs assessment survey.
Procedures
The study was approved by the Institutional Review Board at Vanderbilt University. Recruitment took place from August 2024 to June 2025. After obtaining permission from the treating social worker, study personnel approached eligible caregivers on the day of their child’s discharge to obtain informed consent for the survey. While as many caregivers as eligible were allowed to complete surveys to capture communal caregiving approaches, caregivers instead designated one caregiver to complete the survey or completed the survey together. Both the consent form and survey were administered electronically via REDCap (Harris et al., 2009, 2019).
Data Analytic Plan
All data were exported from REDCap to Microsoft Excel for analyses and summarized using descriptive statistics. The open-ended item on barriers to groups was analyzed using qualitative coding methods; two raters KH and KG independently coded responses using inductive coding and content analysis, then reconciled discrepancies through consensus. Data are available upon request from the corresponding author.
Results
Supports Caregivers Received
80–90% of participants reported receiving care plan information about diagnoses, medications, treatment updates, aftercare, and safety planning (Figure 1(A)). Sixty-eight (87.2%) participants reported being extremely or very satisfied with the care plan information they received. The majority (>50%) of caregivers reported receiving resources regarding returning to school, making the home safe, and/or parenting (Figure 1(B)); 65 (83.3%) were very or extremely satisfied with these. Regarding support for communication around mental health, around 65% of participants reported receiving caregiver-only or family meetings (Figure 1(C)), with 56 (71.9%) being very or extremely satisfied. Most participants (80.8%) reported feeling extremely or very competent in their ability to communicate with their child about their child’s mental health (Figure 1(E)). Supports caregivers received and desired to receive. MH, mental health.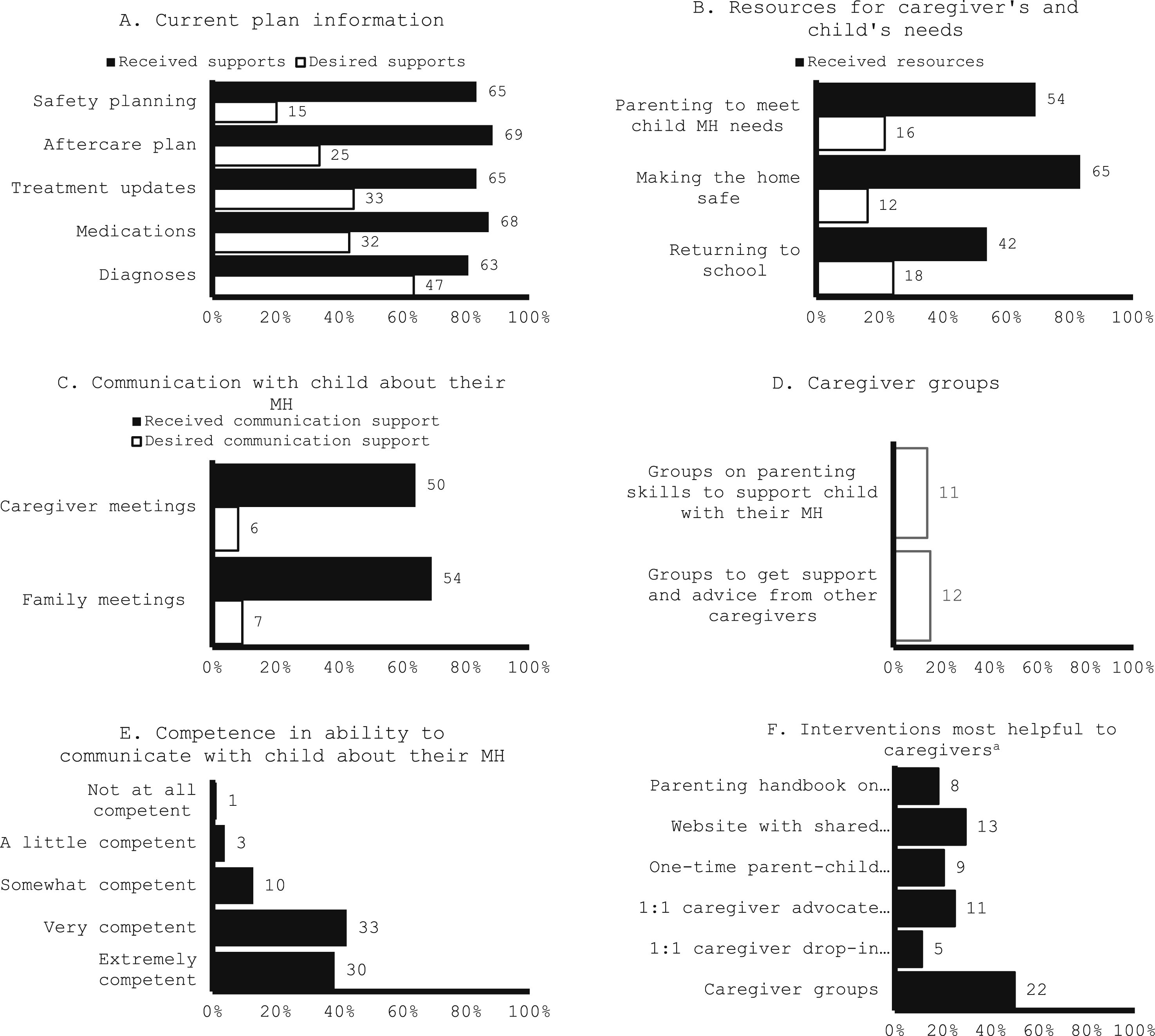
Supports Caregivers Desired
Over half of caregivers wanted additional support with care plan information regarding diagnoses (63.5%), medications (43.2%), and treatment updates (44.6%) (Figure 1(A)). Fewer caregivers reported wanting additional resources for parenting (21.6%) and returning to school (24.3%) (Figure 1(B)). Around 15% of caregivers reported interest in groups, either for support and advice from other caregivers (15.4%) or for learning parenting skills (14.1%) (Figure 1(D)). Of 44 caregivers, groups were the most desired form of support (50.0%), followed by a website of shared experiences (29.5%) (Figure 1(F)).
Regarding interest in caregiver groups, 40 (51.3%) caregivers reported being extremely likely to attend a group to learn parenting skills. Of the 68 who felt neutral, somewhat, or extremely likely (87.2%), caregivers preferred a heterogeneous array of topics, attending once weekly (75.0%), evening hours (44.1%), and either virtual only (40%) or hybrid attendance (38.2%) (Figure 2(A)–(D) and (F)). Of the 42 caregivers who responded to the open-ended question about barriers to attending groups, the most common barrier was work (52.4%), followed by distance (16.7%) (Figure 2(E)). Caregiver perceptions on inpatient caregiver groups. aParticipants may check all that apply. bPercentages were taken from a sample size of 68 (those who responded neutral, somewhat likely, or extremely likely to A.) cPercentages were taken from a sample size of 42 total responses *Those who chose “other” provided a free-text response. Responses largely consisted of evening times after 4:00 p.m.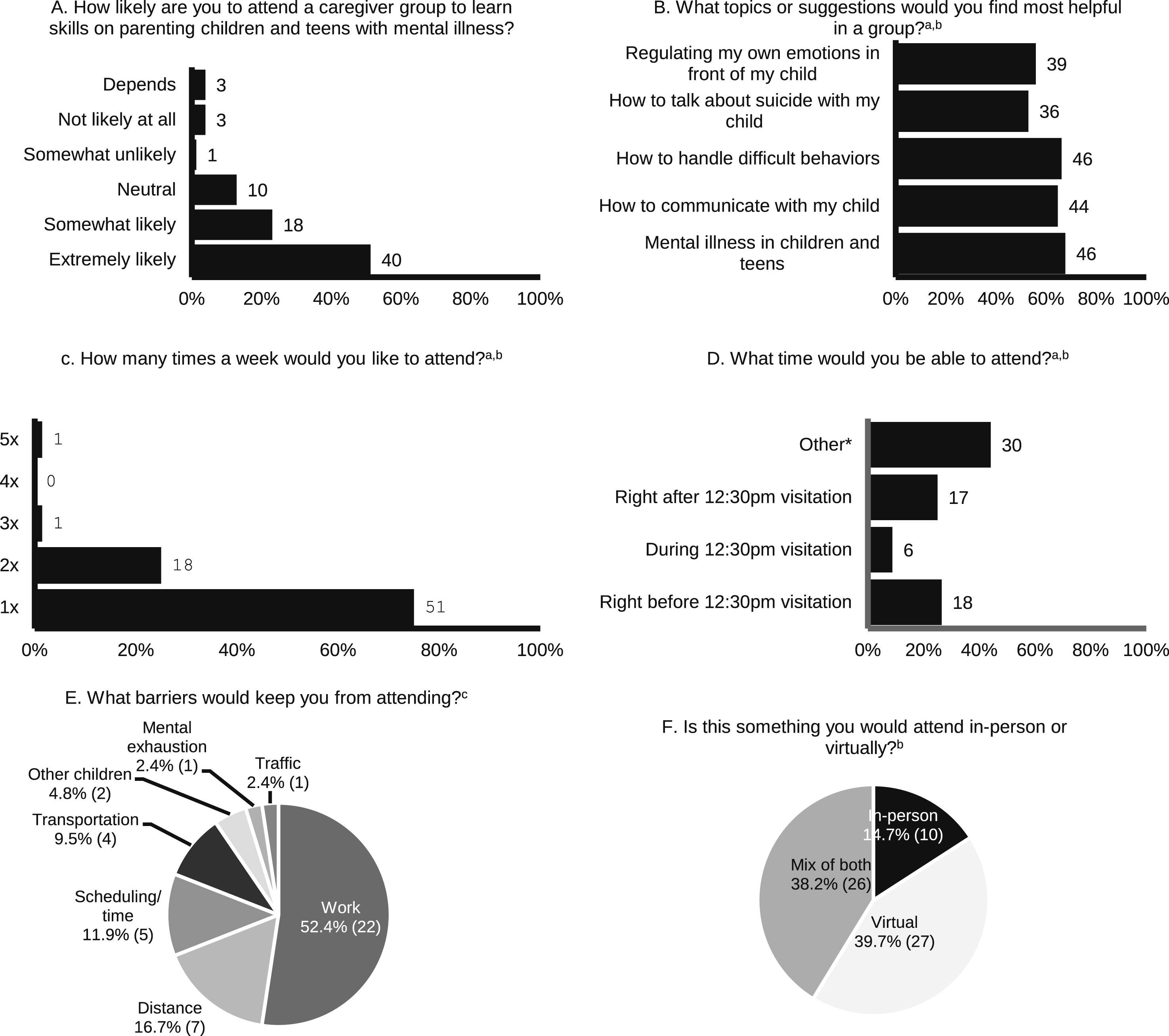
Discussion
We conducted a needs assessment survey to understand caregivers’ perceived needs during their child’s acute psychiatric hospitalization. Results showed that while individualized care plans remain the priority, caregivers remain interested in caregiver groups though face barriers to feasibility.
Overall, caregivers reported high satisfaction with inpatient care. Consistent with prior literature, caregivers most frequently reported receiving informational support pertaining to diagnoses, medications, and aftercare, which was also the most desired support, suggesting that the caregiver’s priority remains their child’s individualized care plan with the treatment team (Rodríguez-Meirinhos et al., 2018; Sternbeck-Rutter et al., 2025). Considering most caregivers reported feeling competent in communicating with their child about mental health, the informational support they seek may relate more to understanding their child’s psychopathology rather than their own communication skills.
Still, caregivers showed high interest in groups to support their parenting. Groups were also rated the most helpful form of caregiver support, followed by a website of shared experiences, both uniquely providing lived experiences that other forms of support lack. Caregivers can feel isolated when their child is admitted to the psychiatric hospital (Merayo-Sereno et al., 2023), and therefore the caregiver’s socioemotional needs are an important consideration (Rodríguez-Meirinhos et al., 2018). As seen in other settings, groups provide real-time connection and mutual knowledge exchange that a treatment team alone cannot provide. Studies on parent support groups for children with eating disorders, other mental disorders, and complex needs showed improved caregiver confidence and self-efficacy, decreased caregiver isolation and burden, and appreciation for the emotional support (Nicula et al., 2023; Sartore et al., 2021; Yen & Valentine, 2023). However, evidence for inpatient groups is limited (Hsiung et al., 2025).
That most caregivers felt competent in their ability to communicate with their child about their mental health seemingly contradicts their interest in attending a caregiver group on parenting and the prevailing evidence of caregiver influence on child mental health symptoms (Yap et al., 2014; Yap & Jorm, 2015). This suggests a gap in caregiver psychoeducation and argues for caregiver interventions to be a routine part of child mental health treatment despite caregiver-reported competence and preference. Understanding effects of inpatient caregiver support on youth outcomes is worth further study.
Our study provides practical guidance for developing an inpatient caregiver group. Caregivers preferred groups once per week, which averages to once per inpatient stay. Thus, flexible, standalone sessions may be more feasible than multiple-session programming. While caregivers in our study did not favor any one topic, basic psychoeducation on psychiatric diagnoses and medications in children, and on caregiver mental health in child psychopathology, may be of interest. Evening hours may better accommodate standard work schedules; virtual groups may address travel barriers, though in-person groups may bypass technological barriers and offer needed socioemotional connection. In measuring effectiveness, one should consider caregiver socioemotional outcomes, such as social support, feelings of isolation, and perceived stress, as these are potentially modifiable risk factors during a child’s mental health crisis.
Our study has several limitations. Due to study personnel availability, some surveys were gathered before discharge family meetings, where substantial support is provided, potentially leading caregivers to underreport received supports. Most surveys were administered after meetings to minimize this concern. Caregivers from family meetings that were emotionally challenging were less likely to consent; those attending by phone and lacking English proficiency were also excluded, limiting sample diversity. The voluntary nature of the surveys risks selection bias. Finally, the small sample size may not represent all caregiver experiences in this setting. Notably, the hospital experienced increased turnover among social work staff during this time, contributing challenges to study recruitment.
Conclusion
While the need of caregivers for individualized care plan information for their child during their acute inpatient stay remains the priority, caregivers still identify groups as an important form of support. Creating inpatient groups should account for caregiver limitations including work, travel, and other responsibilities. Higher-powered studies with feasible caregiver and youth outcomes may broaden understanding of the benefits of inpatient caregiver groups.
Supplemental Material
Supplemental Material - Supporting Caregivers During Their Child’s Acute Psychiatric Hospitalization: A Needs Assessment Survey
Supplemental Material Supporting Caregivers During Their Child’s Acute Psychiatric Hospitalization: A Needs Assessment Survey by Kimberly S. Hsiung, Kelly Geelan, Daisy Sornabala, Jon S. Ebert, Alexandra H. Bettis, Bavani Rajah in Clinical Child Psychology and Psychiatry
Footnotes
Author Note
Since the completion of this research, Kimberly Hsiung, MD, MS has moved to a new institution and is currently affiliated with Nationwide Children’s Hospital, Department of Psychiatry and Behavioral Health, Columbus, OH at the time of this manuscript submission.
Acknowledgements
The authors would like to acknowledge the following social workers who played an instrumental role in coordinating with the research team to determine eligible participants for the survey and to have caregivers be available after discharge meetings: Alexandra Keller, LMSW, Alexis Vatterott, LMSW, and Rebecca Winstead, LMSW. We would also like to acknowledge Caroline Castleman, BA, who provided substantial help in recruitment by administering surveys to eligible caregivers after discharge meetings.
Ethical Considerations
This study was approved by the Institutional Review Board at Vanderbilt University Medical Center.
Consent to Participate
Written informed consent was obtained by all participants before participation in the survey.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors’ use of REDCap was supported through grant UL1 TR000445 from National Center for Advancing Translational Sciences/National Institute of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data related to the findings of this study are available upon request from the corresponding author.
Supplemental Material
Supplemental Material for this article is available online
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.