
Abstract
Background
Parents of children with emotional or behavioural disorders (EBD) experience challenges with their own wellbeing. Parenting practices are impacted by parent wellbeing and are vital to supporting children with EBD. Programs with peer-led components, aimed at developing healthy parenting skills have been developed. While peer-led parenting interventions for parents of children with EBD have led to positive outcomes for children, outcomes related to parent wellbeing are not known. This systematic review examines the impact of peer-led parenting programs on the wellbeing of parents of children with EBD.
Methods
A systematic review across 7 databases was conducted. 1009 articles were screened, and 13 met criteria for inclusion.
Results
This study identified 8 peer-led parenting interventions. 11 outcome measures of parent wellbeing were used across the 13 studies. 7 studies reported statistically significant improvement in parent wellbeing outcomes. The 6 studies that did not report statistically significant improvement showed a trend toward improved parent wellbeing on outcome measure scores.
Conclusions
Findings indicate the potential for peer-led parenting interventions to have a positive impact on parent wellbeing. Future research is needed to determine how to meaningfully measure parent wellbeing and what aspects of peer-led parenting interventions positively impact parent wellbeing.
Plain Language Summary
Emotional or Behavioural Disorders (EBD) are conditions that impact on children’s abilities to manage their emotions, behaviours or social interactions. Parents of children with these difficulties often struggle with their own wellbeing, which can affect how they care for their child. Parenting support programs led by other parents (peers) exist, but their impact on parent wellbeing is unclear. This study reviewed 13 research articles on peer-led parenting programs. Findings indicate the potential for peer-led parenting interventions to have a positive impact on parent well-being. In the articles included, parent wellbeing was measured in different ways and many different peer-led parenting interventions were described. Future research is needed to determine meaningful ways to measure parent wellbeing and to better understand what aspects of peer-led parenting interventions positively impact parent wellbeing.
Keywords
Introduction
It is estimated that 20% of Canadian children and youth will experience challenges with their mental health and that 70% of mental health concerns begin in childhood or adolescence (Canadian Mental Health Association, 2025a). Signs of mental health concerns in children and youth can take the form of emotional or behavioural challenges such as avoiding friends or family, changes in sleeping or eating habits, persistent worrying, outbursts of anger, rebelling against authority, engaging in risk-taking behaviours or experiencing regular mood swings (Canadian Mental Health Association, 2025b). In the United States, approximately 21% of children aged 3-17 are diagnosed with an emotional or behavioural disorder (Centers for Disease Control and Prevention, 2025). According to data from 2022-2023, 11% of American children have diagnosed anxiety, 8% are diagnosed with a behavioural condition and 4% are diagnosed with depression (Centers for Disease Control and Prevention, 2025).
The term emotional and behavioral disorders or difficulties (EBD) represents mental health conditions that are not well-defined in the literature. There is a lack of consistent terminology and agreed upon acceptance for what diagnoses fit under the EBD umbrella, which also leads to challenges with obtaining accurate prevalence estimates (Boydell Brauner & Bowers Stephens, 2006; Forness & Kavale, 2000). Although there is notable inconsistency in how EBD are defined and prevalence is reported, there is consensus that untreated childhood EBD can have negative effects on school performance, peer relationships, sleep patterns, and employment prospects (Ogundele, 2018). For the purpose of this review, EBD is conceptualized as an emotional or behavioural disorder, challenge or difficulty that negatively impacts a child or youths’ day-to-day function and participation (Ringeisen et al., 2020). Some conditions commonly described as EBD include mood disorders such as depression, anxiety disorders such as obsessive-compulsive disorders (OCD) and behaviour disorders such as oppositional defiant disorder (ODD) (Ringeisen et al., 2020). EBD prevalence estimates are further complicated by underreporting linked to the underuse of supports available to families of children with an EBD (Ringeisen et al., 2020). Barriers such as stigma for seeking mental health treatment and parent uncertainty about what types of emotional disturbances or behaviours constitute as atypical may make it challenging for families to access available supports, contributing to underuse (Ringeisen et al., 2020). Though reported prevalence of EBD varies greatly within the literature, it is estimated that 20% children in the United States will experience an EBD before the age of 18 (Ringeisen et al., 2020).
EBD in children and youth have been associated with increased parental strain including higher stress levels (Bode et al., 2016; Bögels et al., 2014). High levels of parental stress persist across demographic domains including the child’s age, the child’s gender, and family socio-economic status (Bode et al., 2016). Strain of parenting a child experiencing emotional or behavioural challenges may be increased when parents themselves experience challenges with their mental health (Bögels et al., 2014). In a study examining the psychological distress in parents of children with psychiatric disorders, 54.5% of parents reported experiencing severe psychological distress (Saed O’leimat et al., 2019). Findings of a 2021 scoping review indicate that 1 in 3 parents of children receiving mental health services report experiencing a mental illness (Campbell et al., 2021). Parent mental health challenges can lead to poorer outcomes related to child behavioural and emotional development and mental health interventions (Campbell et al., 2021; Smith, 2004). Further, parenting a child with an EBD can impact how a parent feels they perform in other areas of their lives such as at work and in social relationships (Campbell et al., 2021). In families where both the child and parent experience mental health challenges, capacity for parenting and the parent-child relationship can be impacted (Campbell et al., 2021). Although parents experiencing mental health challenges will often seek support for their children, they less frequently seek support for themselves (Campbell et al., 2021). Given the impact of mental health on parenting practices, screening parent wellbeing and addressing identified concerns has been recommended in the child mental health field (Campbell et al., 2021). Although individual concepts such as parent mental health (Duncombe et al., 2012), psychological distress (Saed O’leimat et al., 2019) and caregiver strain (Mayberry & Heflinger, 2013) have been explored in the EBD literature; parent wellbeing as a general construct has not been clearly defined.
The Conceptual Model of the Factors that Influence Parent Wellbeing is a dynamic process model that provides a framework for explaining factors influencing parent wellbeing by simultaneously considering the impact of personal factors (e.g., family demographics, parent mental health) and environmental factors (e.g., social supports, access to information) (Resch et al., 2012). The model theorizes that outcomes of parent wellbeing are impacted by a parent’s mental/emotional health, physical health, personal life satisfaction and family satisfaction (Resch et al., 2012). In this model, parent wellbeing is influenced by whether parents appraise their environmental/social characteristics (e.g., access to services) and parent and child characteristics (e.g., disability severity) as an opportunity for growth or as a threat (Resch et al., 2012). Although developed for use with parents of children with disabilities, this conceptual model provides a holistic framework for parent wellbeing that can be applied to parents of children with EBD and informed how we defined this construct.
The link between parent mental health (or more broadly positioned as parent wellbeing) and associated parenting practices is of the upmost importance as some parenting practices such as inconsistent discipline have been linked to the development of problematic child behaviours and emotional difficulties (Berg-nielsen et al., 2003; Duncombe et al., 2012). By contrast, parenting practices that are consistent, empathic, and validating of emotions have been demonstrated to have positive outcomes for children (Duncombe et al., 2012). As a result of the impact of parenting practices on outcomes for children with EBD, interventions focusing on parenting practices, beliefs, feelings and the overall child-parent relationship (Scott and Gardner, 2015) are common in a multi-faceted approach to the treatment of EBD. Parenting programs aim to positively impact the parent-child relationship by improving the quality of parenting provided to a child and have been demonstrated to be effective at reducing behavioural challenges in children, decreasing parent stress levels, improving parent mental health outcomes and increasing parents’ feeling of competence (Högström et al., 2017; Scott and Gardner, 2015; Stattin et al., 2015). Two systematic reviews examining the effectiveness of parenting interventions in the EBD population indicated that they had the potential to positively influence outcomes related to behavior and emotional functioning in both younger and older children (Barlow et al., 2005, 2016).
Peer-led programs (i.e. programs run by parents for other parents) have been utilized in many fields including chronic disease self-management (Funnell, 2010), smoking cessation (Apata et al., 2019) and caregiver support (Han et al., 2022). In some health-related fields, the use of peer-led interventions has been found to be effective in knowledge sharing and supporting changes in behaviour, however more evidence is needed to generalize the effectiveness of this intervention approach more broadly (Topping, 2022). In parents of children with disabilities, peer-led interventions aimed at health promoting behaviours in parents have been found to be feasible in community settings (Bjornstad et al., 2021). This model of intervention has been used to support parents of children with emotional and behavioural challenges gain parenting practices that promote positive outcomes for the child and the family (January et al., 2016; Michelson et al., 2014). Further, a peer-led approach to parenting intervention was found to be an acceptable format for parents with self-identified difficulties related to parenting (Bradley et al., 2020). In a peer to peer support program for parents of children with a neurodisability, parents felt understood by their peer supporters and that shared elements of their lived experience helped with developing a genuine connection (McCrossin & Lach, 2022). Further, opportunities to connect with peer supporters, allowed parents to envision a hopeful future for their children (McCrossin & Lach, 2022). This hopeful state, may positively impact overall family satisfaction, a factor described as influencing parent wellbeing in the Conceptual Model of the Factors that Influence Parent Wellbeing (Resch et al., 2012).
Parenting has been demonstrated to impact outcomes for children with EBD and a parent’s sense of wellbeing has been shown to influence parenting practices. It is important to understand if participating in a peer-led parenting intervention has positive outcomes for parents because parenting interventions are a common approach to the treatment of EBD in children. Currently, the impact of participating in peer-led parenting interventions on parent wellbeing is not known in the EBD literature. This systematic review examines the question: For parents of children or youth with emotional and behavioural disorders or difficulties, does participation in peer-led parenting interventions result in improved parent wellbeing?
The objectives of this systematic review are to. 1. Describe the types of peer-led parenting interventions identified in the literature. 2. Describe the range of outcomes measured in the literature related to parent wellbeing when peer-led parenting interventions are delivered. 3. Identify if participation in peer-led parenting interventions is beneficial for the wellbeing of parents of children or youth with EBD. 4. Make recommendations about the use of peer-led parenting interventions in the population of parents of children and youth with EBD and areas for future research.
Methods
This systematic review was completed in alignment with the protocol registered with the National Institute for Health Research international prospective register of systematic reviews (PROSPERO CRD42022300596) (Reitzel et al., 2022) and is reported according to the updated Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement (Page et al., 2021) and the Synthesis Without Meta-Analysis (SWIM) reporting guidelines (Campbell et al., 2020). Deviations from the protocol are reported in the methods section of this paper.
Development of the Research Question and Objectives
After reviewing the pediatric EBD literature, our research question and objectives for this systematic review were developed by an interdisciplinary team. Our team includes rehabilitation science researchers with clinical backgrounds in occupational therapy and speech and language pathology and two parent partners with lived experience of having a child with an EBD. The team is located at McMaster University in Ontario, Canada. Based on feedback from our parent partners about the research question and objectives, the word “difficulty” was used in addition to disorder to be inclusive of children and youth who may experience emotional and behavioural challenges but who do not have a diagnosed disorder.
Identification and Selection of Studies
The search strategy was developed in consultation with an experienced health sciences librarian. Electronic searches of the Web of Science, Education Resources Information Centre (ERIC), Cumulative Index to Nursing and Allied Health Literature (CINAHL) and MEDLINE, EMBASE, EMCare and PsychINFO via OVID were completed in December 2021 and updated in September 2024. No limits were placed on language, publication period or publication type for all databases with the exception of CINAHL. Under advisement from the research librarian, the search in CINAHL was restricted to peer reviewed literature. Grey literature and unpublished studies were not searched. The search strategy was developed using synonyms of four core concepts of the review: parents (e.g., mother, father), parenting intervention (e.g., parenting program), peer-led (e.g., peer-facilitated) and EBD (e.g., depression). A comprehensive list of search terms is provided in the Supplementary Material. Covidence was used to collate and deduplicate search yields (Veritas Health Innovation, n.d). Duplicates removed by Covidence were reviewed for accuracy and additional duplicates were removed and tracked manually during title and abstract screening. The references of articles included after full-text screening were searched for additional relevant primary studies.
Review of the literature and discussions with the review team guided development of the inclusion and exclusion criteria. Parent partners provided feedback on the inclusion and exclusion criteria which helped to establish an inclusive definition of the construct of parent and finalize the EBD to be included. The inclusion and exclusion criteria were piloted by two reviewers (Reviewer 1, Reviewer 2) through independently screening a small sample of articles, comparing decisions, discussing disagreements and making adjustments to the criteria accordingly.
Studies that met inclusion criteria were peer-reviewed articles published in English and included the following criteria: (a) parents (including stepparents, adoptive parents, foster parents, mothers and fathers) of a child with an EBD aged 0-18 years; (b) focused on children or youth with depression, dysthymia, bipolar disorder, anxiety disorder, agoraphobia, separation anxiety disorder, social anxiety disorder, post-traumatic stress disorder, obsessive-compulsive disorder, specific phobia, panic disorder, attention deficit with hyperactivity disorder, attention deficit disorder, oppositional defiant disorder, conduct disorder, eating disorders or generalized emotional or behavioural disorders or difficulties. Included EBD were determined according to epidemiological literature exploring the prevalence of common EBD (Ringeisen et al., 2020; Waddell et al., 2014); (c) contained a peer-led (could be co-led with parent peer and clinician) individual intervention or group-based parenting intervention; (d) had an outcome related to parent wellbeing extending beyond measuring change in parenting skills or knowledge. Wellbeing was defined using the Conceptual Model of Factors Influencing Parent Wellbeing by Resch et al. (2012). Aligned with this model, studies needed to have an outcome measure broadly related to parent mental/emotional health, physical health, personal life satisfaction or family satisfaction to be included (Resch et al., 2012). Given the interest in intervention effectiveness, articles focusing on informal education, support or advice offered from one parent to another outside of an intervention program were excluded. Study protocols and evidence syntheses were excluded, however if the evidence synthesis matched the review population, intervention and outcome of interest, the reference list was searched for additional primary studies that fit our inclusion criteria.
For the initial search, completed in December 2021, two reviewers (Reviewer 1, Reviewer 2) independently screened a subset of articles (n = 248) from the total number of articles yielded from the search and an inter-rater reliability of 96% (ĸ = 0.80) was achieved. For the second search in September 2024, the process was repeated where two reviewers (Reviewer 3, Reviewer 4) screened a subset of 25 articles and achieved 96% inter-rater reliability (ĸ = 0.78). Given that a Cohen’s kappa score of greater than 0.60 indicates substantial agreement (Cohen, 1960), all reviewers continued to independently screen the titles and abstracts of each retrieved article. For the initial search, reviewers (Reviewer 1, Reviewer 2) independently completed full-text review of each article and reasons for exclusion were recorded. An inter-rater reliability of 97% (ĸ = 0.74) was achieved for full-text screening. Every article was screened by both reviewers (Reviewer 1, Reviewer 2) at the level of title and abstract as well as full-text review. An attempt to find consensus between reviewers (Reviewer 1, Reviewer 2) was first used to address discrepancies in decisions to include or exclude a study. If consensus could not be reached another reviewer (Reviewer 5) was available to adjudicate the decision, this was only required for one article. For the updated search in December 2024, reviewers (Reviewer 3, Reviewer 4) repeated the same process and achieved an inter-rater reliability of 92% (ĸ = 0.80) for full-text screening. Another reviewer (Reviewer 1) was once again available to resolve conflicts but was not required for any articles.
Data Extraction
The data extraction form was developed by the full research team and piloted by reviewers (Reviewer 1, Reviewer 2) by collaboratively extracting data from one of the included studies. Data from the remaining studies were independently extracted by two reviewers (Reviewer 1, Reviewer 2) in the initial search and two reviewers (Reviewer 3, Reviewer 4) in the updated search. Feedback from parent partners on the data extraction table was obtained to help ensure that meaningful content from the parent perspective was extracted from the included studies. The following data were extracted and recorded in a spreadsheet using Microsoft Excel (Microsoft Corporation, 2016): title, year, author, country, number of participants, parental role (e.g., mother, father, stepparent), number of parent participants, study design, EBD of focus, aims of intervention, intervention outcome measures, parent wellbeing outcome measures, results related to parent wellbeing outcomes. To ensure thorough and consistent extraction of data related to describing the interventions of the included studies, the reporting guidelines outlined by the template for intervention description and replication (TIDieR) checklist was followed (Hoffmann et al., 2014).
Risk of Bias Assessment
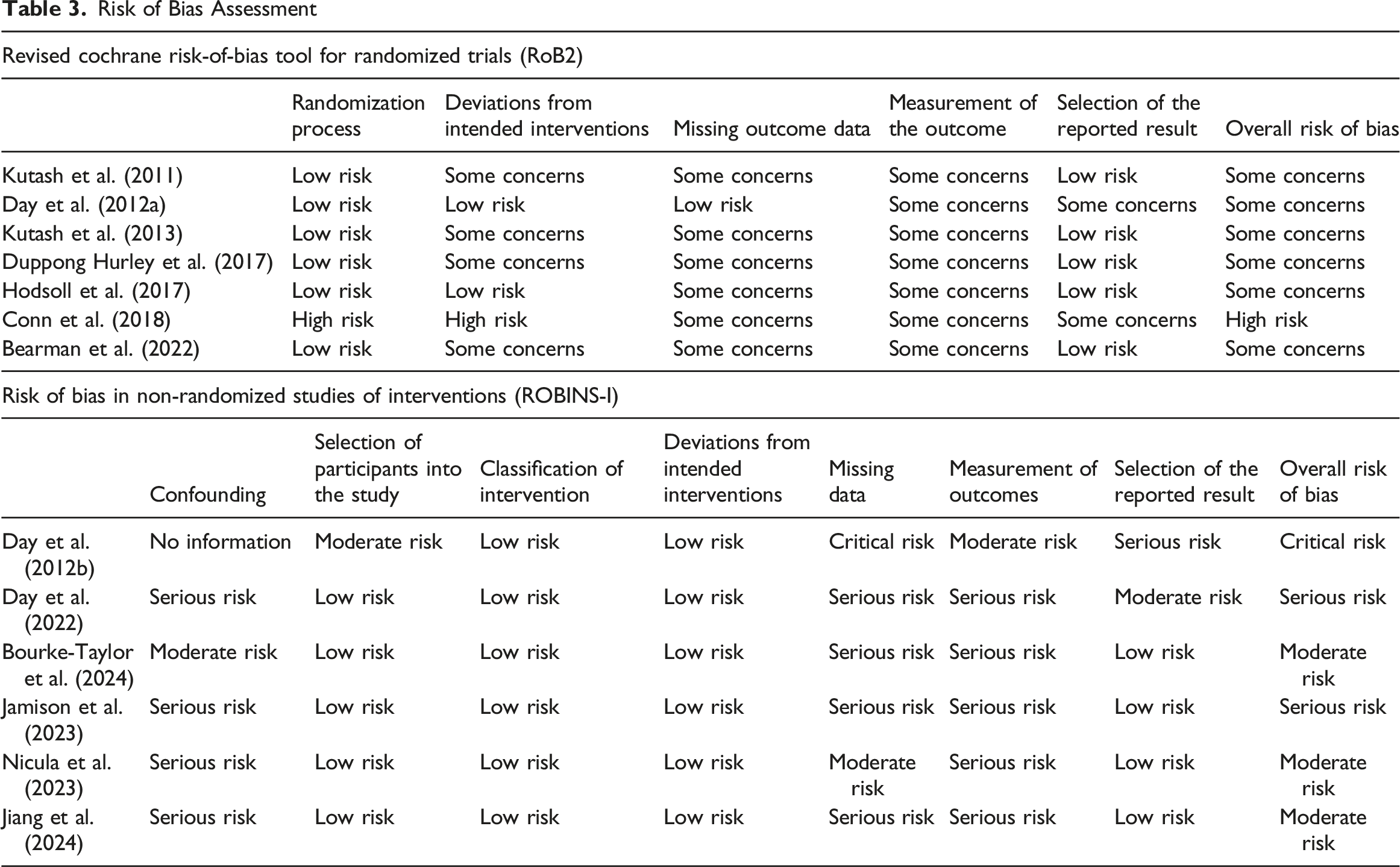
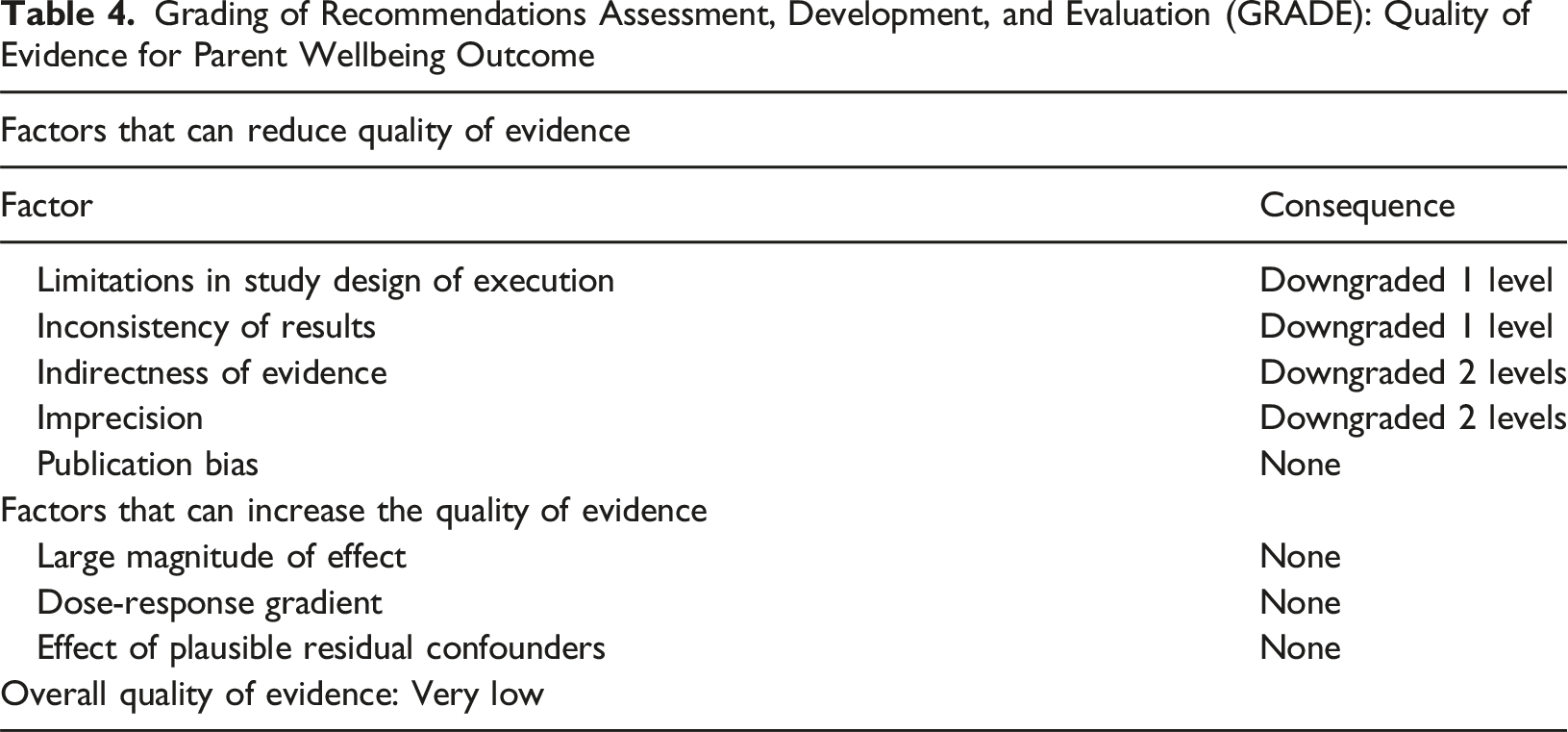
Risk of bias (ROB) assessment was completed by reviewers (Reviewer 1, Reviewer 2) for the initial search and reviewers (Reviewer 3, Reviewer 4) for the updated search using the Cochrane ROB 2.0 (Sterne et al., 2019) or the Risk of Bias in Non-Randomized Studies - Interventions (ROBINS-I) (Sterne et al., 2016) tools matching the corresponding study designs of the included articles. Considering the five domains of bias in the Cochrane ROB 2.0, a judgement of low ROB, some concerns of bias or high ROB in the outcome of interest (i.e., parent wellbeing) was applied. Similarly, a determination of bias in the outcomes measure of interest using the ROBINS-I was achieved by applying one of the following ROB judgement levels to the seven domains of this tool and to the study overall: low, moderate, serious, critical or no information. Initially, ROB assessment for one included study was completed collaboratively by two reviewers (Reviewer 1, Reviewer 2) for the initial search and again by two reviewers (Reviewer 3, Reviewer 4) for the updated search to ensure a shared understanding of the ROB domains. The ROB assessments for all remaining articles were completed individually and reviewers met to come to a consensus to resolve any disagreement. Given the small number of studies yielded through the screening process, no studies were excluded due to risk of bias concerns. The Grading of Recommendations, Assessment, Development and Evaluation (GRADE) (The GRADE Working Group, 2013) approach was applied independently by two reviewers (Reviewer 1, Reviewer 2) for the initial search and repeated for all articles included in the updated search by reviewers (Reviewer 3, Reviewer 4) to determine an overall quality of evidence for the entirety of the data set. The body of evidence in this review was considered in relation to the factors outlined by the GRADE approach that can reduce or increase the overall quality. As indicated in the GRADE handbook, information gathered from the evidence was used alongside reviewer justification, to upgrade or downgrade each GRADE factor by one or two levels depending on how strongly it was determined to influence the quality of the overall body of evidence (The GRADE Working Group, 2013).
Parent Engagement in Review
Parent partner involvement is reported in alignment with the stages of the review process outlined in the ACTIVE framework of involvement in a systematic review (Pollock et al., 2019). Parent partners were recruited through an open call in a Parent’s Partnering in Research Facebook group. Parent partners contributed to the language of the research question and had critical input in determining inclusion and exclusion criteria, including finalizing our conceptualization of the construct of parent as well as the list of included EBD. Parents also had direct influence on data extraction by identifying content to be extracted. Parent input at the level of the research question, inclusion and exclusion criteria as well as methods for data extraction were reflected in the registered protocol. Parent partners contributed their lens of lived experience to the interpretation of data and development of this manuscript. Lastly, parent partners are included as co-authors on the manuscript and will make use of their established networks to coordinate knowledge dissemination efforts within parent and clinical communities.
Data Analysis
Given the variability in outcomes measures and a high level of heterogeneity in the populations and peer-led parenting interventions in the included studies a meta-analysis was not completed. Evidence of heterogeneity was examined in data tables presented in the results summarizing features of the included studies. Therefore, a narrative synthesis of the data was completed aligning with the objectives of this systematic review. P-values and mean group differences are presented to report on the intervention effects related to outcomes of parent wellbeing and collated in a table. These metrics were selected as they were consistently reported across the included studies. The range of outcomes related to wellbeing are presented in a table as well the specific outcome measurement tools used to measure these constructs. Peer-led parenting interventions are described in table format in alignment with the TIDieR reporting guidelines (Hoffmann et al., 2014).
Results
A systematic search across seven databases yielded ten studies that met the inclusion criteria, and three additional studies were identified for inclusion from searching the references of included articles as illustrated in the PRISMA flowchart (Figure 1). After the initial search, 618 duplicates were removed by Covidence before screening and 1043 articles were screened for eligibility at the title and abstract level. At this level of screening, an additional 34 duplicates were removed manually. A full-text review for eligibility was conducted for 103 articles from the initial database search plus an additional 26 articles as identified through an ancestral search. The thirteen selected articles were published between the years 2011 to 2024. Prisma flow diagram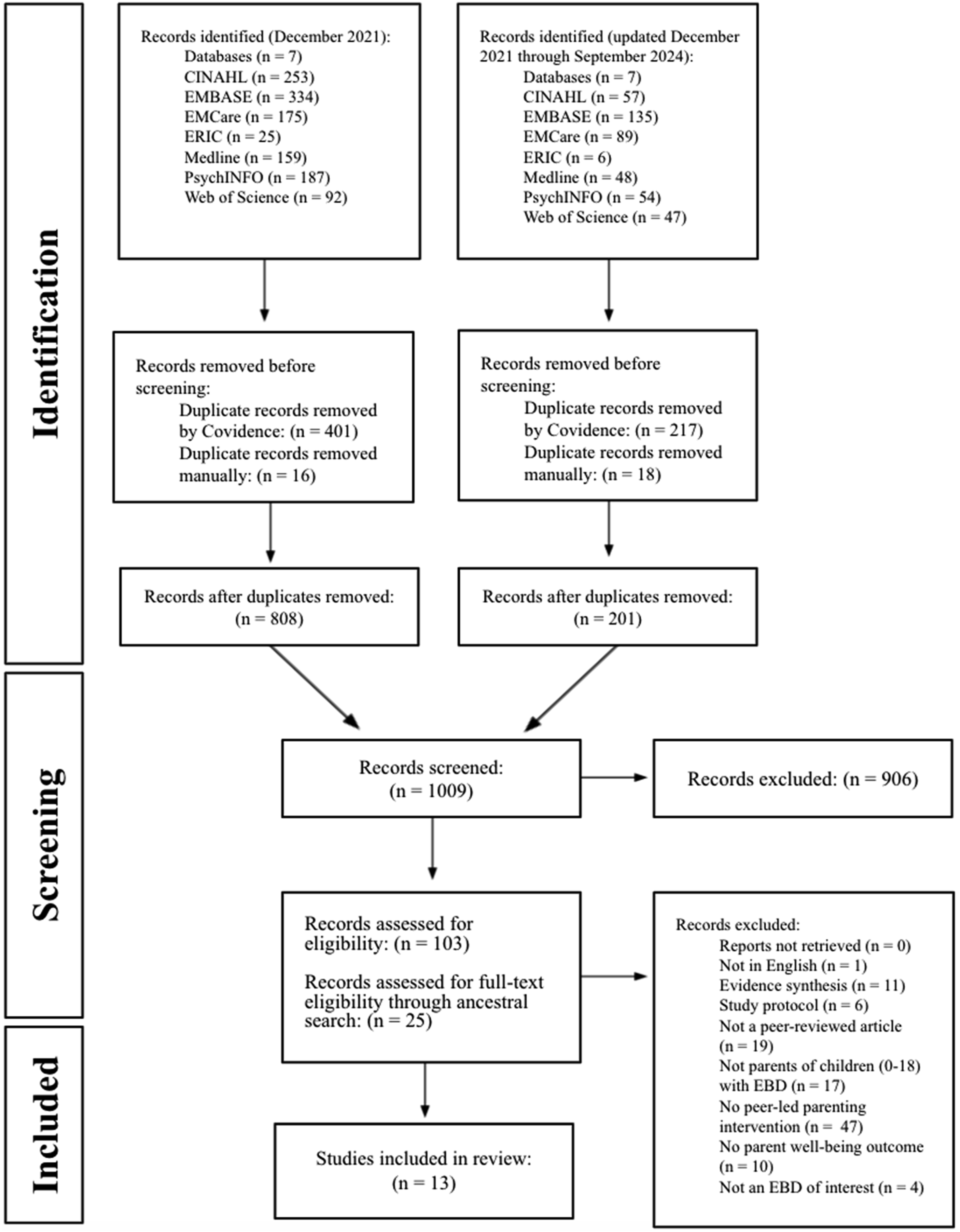
Across the thirteen included articles, the study designs represented include randomized control trials (n = 4), pilot multisite randomized controlled trials (n = 2), a parallel randomized controlled trial (n = 1), a nonrandomized control trial (n = 1), a pre-post cohort study (n = 1), a pragmatic cohort design (n = 1), a longitudinal follow-up study (n = 1), a mixed methods study (n = 1), and a pilot study (n = 1). Studies were completed in the United States of America (USA) (n = 6), United Kingdom (UK) (n = 4), Australia (n = 1), Canada (n = 1) and Singapore (n = 1). In most studies, participants were primarily mothers (n = 12), however studies also included other participants including fathers (n = 4), adoptive parents (n = 1) and foster parents (n = 1). The EBD populations represented include emotional difficulties (n = 3), mental health conditions (n = 3), generalized behaviour disorder (n = 2), anorexia nervosa (n = 1), generalized emotional or behavioural difficulties (n = 1), aggression, oppositional, or defiant behaviours (n = 1), eating disorders (n = 1), and ADHD/ADD and anxiety/mental health problems (n = 1). Several child-related outcomes were identified across studies, including children’s emotional behavioural problems (n = 4), child mental health problems (n = 4), depression, anxiety, and stress (n = 3), eating disorder symptoms (n = 1), eating disorder assessments (n = 3), academic functioning (n = 1), in-school suspensions (n = 1), child and adolescent psychopathology, (n = 1), and psychosocial impairments due to eating disorder features (n = 1). Almost all studies implemented child and parent outcome measures (n = 12).
Summary of Interventions
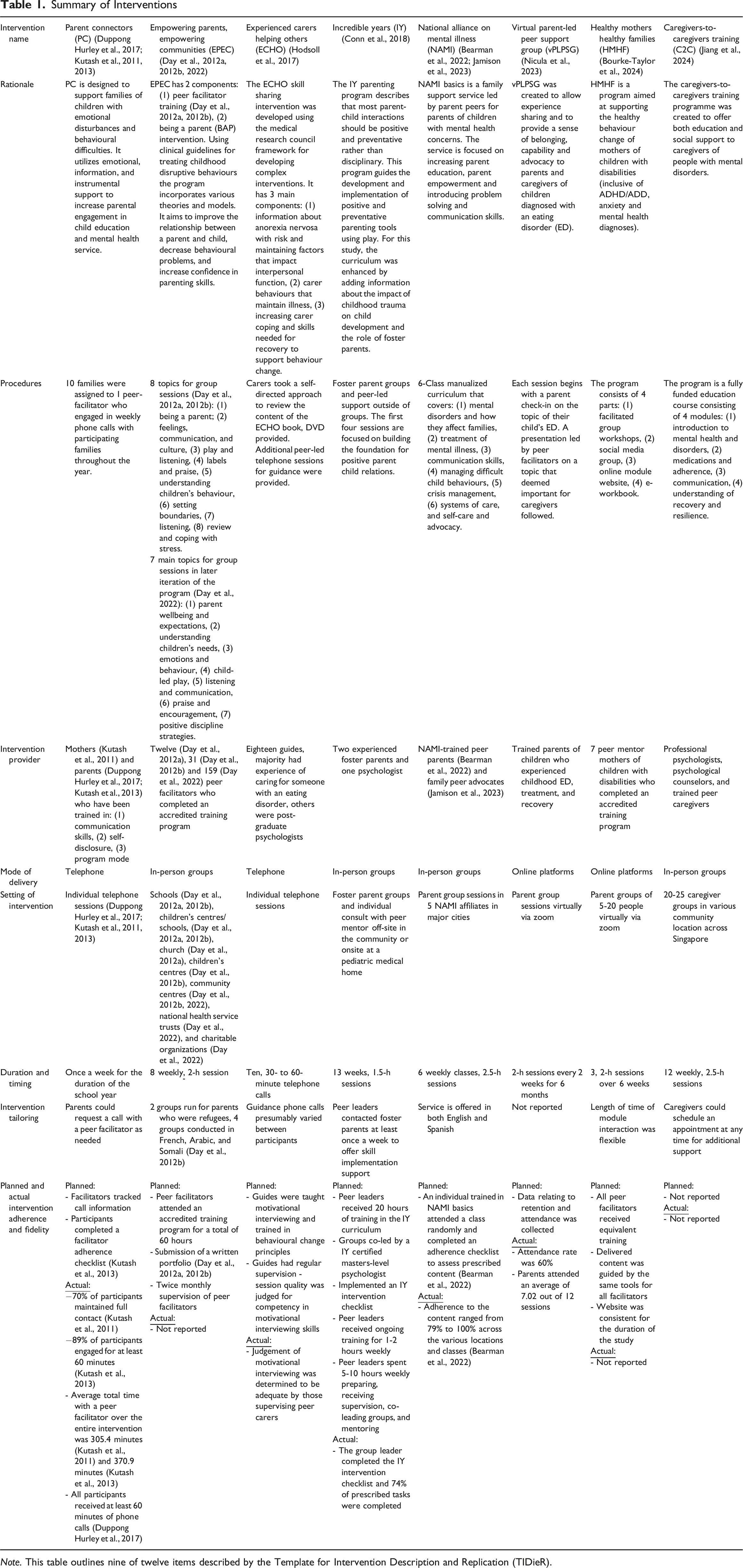
Note. This table outlines nine of twelve items described by the Template for Intervention Description and Replication (TIDieR).
PC is a peer-led intervention, developed to decrease stress and improve family coping and engagement (Duppong Hurley et al., 2017; Kutash et al., 2011, 2013). EPEC consists of two components: 1) peer-facilitator training and 2) the BAP parenting course (Day et al., 2012a, 2012b, 2022). BAP is a completely peer-led intervention by parents who have received training to facilitate the program aiming to improve the parent-child relationship, decrease behavioural challenges and increase parenting confidence (Day et al., 2012a, 2012b, 2022). IY uses play to support the development of positive parenting practices and was co-led by a parent peer and a psychologist (Conn et al., 2018). ECHO aims to increase carer coping and skills related to supporting a child with anorexia nervosa and was primarily led by healthcare workers but had a parent coaching component led by peers (Hodsoll et al., 2017). NAMI Basics is run by NAMI-trained parent volunteers focused on increasing parent education and empowerment (Bearman et al., 2022; Jamison et al., 2023). vPLPSG is facilitated by trained peer parents to empower parents of children with eating disorders (Nicula et al., 2023). Similarly, HMHF has multiple online components facilitated by peer mentors aimed at promoting healthy behavioural changes amongst mothers of children with disabilities, including conditions such as anxiety and ADD/ADHD (Bourke-Taylor et al., 2024). C2C offers educational and social support to caregivers and is led by a team of psychologists, psychological counselors, and peer caregivers (Jiang et al., 2024).
While IY (Conn et al., 2018), ECHO (Hodsoll et al., 2017) and C2C (Jiang et al., 2024) are co-led by a parent and a mental health professional, all other interventions were only led by parent peers. (Bearman et al., 2022; Bourke-Taylor et al., 2024; Day et al., 2012a, 2012b, 2022; Duppong Hurley et al., 2017; Jamison et al., 2023; Kutash et al., 2011, 2013; Nicula et al., 2023). EPEC-BAP (Day et al., 2012a, 2012b, 2022), NAMI (Bearman et al., 2022; Jamison et al., 2023), and C2C (Jiang et al., 2024) are community-based interventions. Four interventions were facilitated using phone or online platforms ECHO (Hodsoll et al., 2017), PC (Duppong Hurley et al., 2017; Kutash et al., 2011, 2013), vPLPSG (Nicula et al., 2023) and HMHF (Bourke-Taylor et al., 2024) and one was delivered using a combination of community and home-based delivery (Conn et al., 2018). IY (Conn et al., 2018), EPEC-BAP (Day et al., 2012a, 2012b, 2022), NAMI (Bearman et al., 2022; Jamison et al., 2023), vPLPSG (Nicula et al., 2023), HMHF (Bourke-Taylor et al., 2024), and C2C (Jiang et al., 2024) are group-based interventions. The group-based interventions generally ran 2-3 months in length with weekly meeting opportunities (Bearman et al., 2022; Bourke-Taylor et al., 2024; Conn et al., 2018; Day et al., 2012a, 2012b, 2022; Jamison et al., 2023; Jiang et al., 2024), except vPLPSG, which spanned 6 months (Nicula et al., 2023). ECHO is self-directed in nature with individual opportunities to connect with a peer coach (Hodsoll et al., 2017), and PC (Duppong Hurley et al., 2017; Kutash et al., 2011, 2013) consisted of individual telephone sessions.
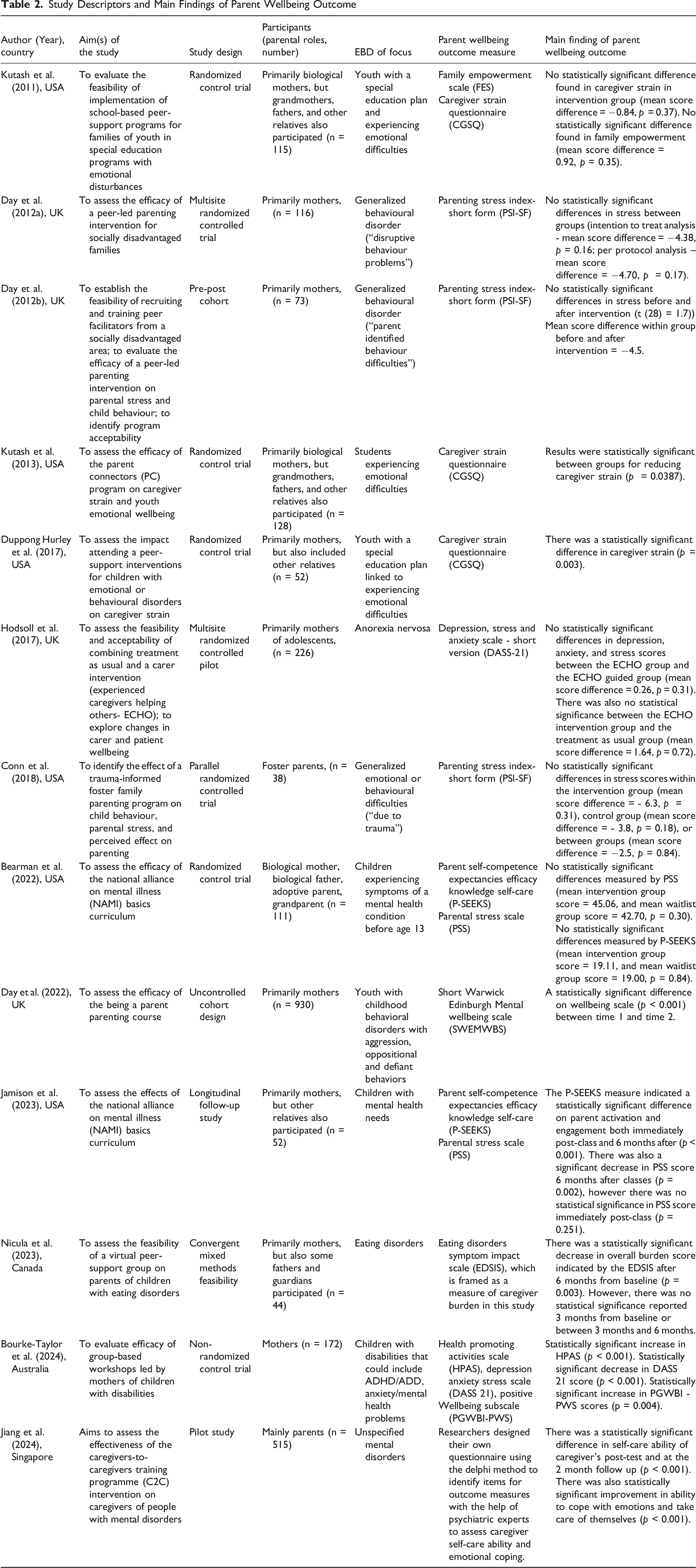
Study Descriptors and Main Findings of Parent Wellbeing Outcome
Risk of Bias and Quality of Evidence
Risk of Bias Assessment
Grading of Recommendations Assessment, Development, and Evaluation (GRADE): Quality of Evidence for Parent Wellbeing Outcome
Discussion
Findings from this review demonstrate the use of peer-led parenting interventions in the EBD population. This review described eight unique peer-led parenting interventions, with varying levels of peer involvement and across different EBDs. In the included studies, parent wellbeing was represented by eleven different outcomes. Seven studies reported statistically significant improvement in parent wellbeing outcomes. The six studies that did not report statistically significant improvement showed a trend toward improved parent wellbeing on outcome measure scores, which aligns with parent input from qualitative work exploring the impact of participating in peer-led interventions.
In the qualitative results of a systematic review examining peer support for parents of children with chronic conditions, parents identified that peer support provided a sense of belonging and reduced feelings of isolation (Shilling et al., 2013). In studies completed with parents of children with disabilities and challenging behaviour, benefits such as reduced feelings of depression, loneliness and guilt as well as an increased sense of control and confidence were associated with parent peer support (Bray et al., 2017; Dew et al., 2019; Shilling et al., 2013). Some of the benefits associated with peer support relate directly to common conceptualizations of parent wellbeing such as reduced feelings of depression or increased confidence (i.e., self-efficacy), while for others the positive impact on parent wellbeing such as experiencing a sense of belonging can be inferred. The interventions described in this review varied in their format (e.g., in-person, online, telephone), duration and frequency. Further research is needed to explore parents’ perceptions of peer-led parenting interventions in parents of children with EBD and their preferences for format to gain an understanding of what components of the intervention have a positive impact on parent wellbeing.
The concept of parent wellbeing is represented in a broad range of literature including childhood disability and medical complexity (Bourke-Taylor et al., 2021; Bradshaw et al., 2019; Resch et al., 2012), autism spectrum disorder (Giallo et al., 2011; Rutherford et al., 2019) and mental health (Mayberry & Heflinger, 2013; Saed O’leimat et al., 2019). Although the term parent wellbeing has a strong presence in the literature, there is a large amount of heterogeneity in how it is conceptualized and measured as a construct. Some of the constructs used as proxies for parent wellbeing in the child health literature include: stress (Bradshaw et al., 2019; Rutherford et al., 2019), depression (Bradshaw et al., 2019; Giallo et al., 2011; Risi et al., 2021), anxiety (Bradshaw et al., 2019), quality of life (Bradshaw et al., 2019; Rutherford et al., 2019), self-efficacy (Giallo et al., 2011; Rutherford et al., 2019), parenting satisfaction (Rutherford et al., 2019), caregiver strain (Mayberry & Heflinger, 2013) and family functioning (Bradshaw et al., 2019).
The Conceptual Model of Factors Influencing Parent Wellbeing, was developed from work with parents of children with disabilities and provides guidance related to constructs that may influence parent wellbeing (Resch et al., 2012). This dynamic model situates parent wellbeing as being influenced by factors related to the parent or child (e.g., demographics, child’s disability) as well as environmental/social factors (e.g., access to information and services, social and community inclusion) (Resch et al., 2012). The inconsistent findings in improved parent wellbeing may be due, in part, to the challenges in measuring this multi-faceted and dynamic construct. Given the dynamic relationship in the personal and environmental contexts that may shape parent wellbeing further research completed directly with families is needed to define this construct comprehensively and meaningfully.
The parent partners on our research team emphasized the impact of lived experience on what parents perceive as meaningful indicators of wellbeing as well as their perceptions of the value of peer-led interventions. As clinicians and researchers, we need to find ways to authentically represent the influence of lived experience when conceptualizing dynamic constructs such as the wellbeing of parents of children with EBD. We suggest that qualitative, exploration-driven research engaging parents of children with EBD is needed to begin understanding perceptions of wellbeing and the value of peer-led parenting interventions for this population so outcome measures can authentically and accurately measure this construct. Additionally, to enhance the authenticity of conceptualizing parent wellbeing, we advocate for the inclusion of the parent voice in project development. By engaging parents as interest-holders in aspects of research outside of the traditional role related to data collection, the opportunity to develop meaningful research questions, acceptable interventions and relevant results is enhanced by the expert knowledge they contribute through lived experience (Morris et al., 2011; Nguyen et al., 2019). When planning to engage parents in the research process a planned and thoughtful approach is recommended to facilitate meaningful engagement for all parties involved. Co-creation approaches to research have been used in the field of mental health and centre the expertise of individuals with lived experience in all project phases to ensure outputs are meaningful to those most impacted by a problem (Moll et al., 2020; Mulvale et al., 2019). Further, frameworks such as the Involvement Matrix (Smits et al., 2020) exist that can support researchers in planning for research engaging diverse interest-holders such as parents, children, and mental health service providers (Hamilton et al., 2018; Pollock et al., 2019).
Limitations
A systematic approach to searching and article selection was employed, however, there is a risk that relevant literature was missed or screened out. Although, use of search parameters was minimized to attempt to capture all relevant literature, only peer-reviewed research was included meaning that applicable information in the grey literature (e.g., community parenting program websites, program testimonials by parents) was excluded. Although including only peer-reviewed articles aligns with our research question examining the effectiveness of peer-led parenting interventions on outcomes of parent wellbeing, the exclusion of grey literature restricts analysis to parenting programs with published evidence. This excludes data that may not inform conclusions about intervention effectiveness but could contain clinically relevant insights about this intervention approach. To pilot the data extraction form and ROB assessment, reviewers completed these steps collaboratively for one article for both the initial and updated searches. Despite the small number of articles included, the review team agreed that jointly piloting data extraction and ROB assessment for one article enhanced rigour and reviewer consistency for the remaining studies.
Conclusions
Peer-led parenting interventions are a model used with the EBD population. Eight different parenting interventions with varying degrees of peer-led components were described in this study. Findings indicate the potential for peer-led parenting interventions to have a positive impact on parent wellbeing. However, given the very low quality of the body of evidence, these findings need to be interpreted with caution. The variation in the findings related to the peer-led parenting interventions described and outcomes measuring parent wellbeing indicate a need for future parent-engaged research to determine how to meaningfully measure parent wellbeing, to better understand parents’ perceived value of peer-led parenting interventions and to determine what aspects of peer-led parenting interventions positively impact parent wellbeing.
Supplemental Material
Supplemental Material - Examining the Effect of Peer-Led Parenting Interventions on the Well-Being of Parents With Children With an Emotional or Behavioural Disorder – A Systematic Review
Supplemental Material for Examining the Effect of Peer-Led Parenting Interventions on the Well-Being of Parents With Children With an Emotional or Behavioural Disorder – A Systematic Review by Meaghan Reitzel, Kayla Brissette, Ledina Hasanagic, Mona Elmikaty, Lori Letts, Briano Di Rezze, Oksana Hlyva, Anne MacLeod and Michelle Phoenix in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgements
Our team would like to acknowledge the contributions of Health Sciences Research Librarian Laura Banfield who provided guidance in the development of our search terms and strategy.
Ethical Considerations
Given the nature of the study design (evidence synthesis) ethics approval and participant consent was not required.
Authors Contributorships
Authors MR, LL, BDR, KB, AM and OH contributed to the conception of this work including the development and approval of the protocol, comments and edits to drafts of the manuscript and provided approval for submission of the final manuscript. First author MR led development and execution of the search strategy as well as drafting the initial manuscript. Author’s KB, LH, ME and MR completed the screening, data extraction, data synthesis, and manuscript development in consultation with senior author MP. Parent partners AM and OH provided consultation over the course of the study, providing expert knowledge from their lived experiences.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (FBD-187473).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available within the article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.