
Abstract
This repeat measures study assessed the progress of 45 children in a therapeutic residential school in terms of attachment, trauma/loss, affect regulation and educational attainment. The aim was to build a profile of complex trauma in severely maltreated children and estimate any changes over a two year period. Attachment, trauma and affect regulation were assessed using the Child Attachment and Play Assessment (CAPA), based on Crittenden’s Dynamic Maturational Model of attachment (DMM). Based on a matrix combining attachment risk, unresolved loss or trauma and observed high or low states of physiological arousal, 51% of children improved and 33% showed deterioration. There was a general improvement in education scores but no significant gains made by children whose stories were assessed with unresolved trauma. While insecure attachment can act as a buffer against severe maltreatment, unresolved trauma or loss is pernicious and continues to affect children’s development. Specific Adverse Childhood Experiences (ACEs), rather than ACE accumulation, influenced improvement compared with deterioration. In particular perinatal neglect may have had a particularly potent impact on change. DMM Type A+ attachment was more susceptible to loss of regulation than Type C+ and the two attachment patterns require different approaches. The CAPA offers a more finely calibrated analysis than that obtained by the more usual questionnaire assessment of complex trauma and is useful in devising treatment plans for individual children.
Plain Language Summary
This study should be of interest to anyone who wants to know more about the impact of abuse and neglect on children aged 7 to 13 years, and what factors might hinder positive change. These 45 children had experienced such severe levels of abuse they were living in a well-established therapeutic children’s home. The research assessed the children six months after they entered the home and two years later, before they left. As well as educational attainment we were interested in types and levels of abuse (Adverse Childhood Experiences) and psychiatric diagnoses. The main focus was attachment and what is termed complex or developmental trauma. All children have an attachment strategy. Attachment is the way we organise our behaviour with other people when we feel angry, scared or want comfort and protection. Complex trauma refers to the damage caused by abuse and neglect that attachment behaviour cannot cope with. Hence, only some abused children are traumatised. Trauma leads to breakdowns in communication and instinctive behaviours of flight, fight or freeze. You can read more about our approach on our website The-CAPA.com. Our main finding was that while attachment offered these children some protection, trauma did not go away and the traumatised children had considerable problems in terms of poor educational achievement and diagnoses of depression and attachment disorder. 51% of the children improved while 33% actually deteriorated. It was possible that some children felt safe enough to start to think about their lives and were going through a period of depression which made it look as if they had not made any progress. Some children assessed as deteriorated had likely suffered as babies with young mothers, under 20, or mothers with severe mental health problems. We think use of this assessment offers more detailed information than trauma questionnaires and can help plan interventions for individual children.
Introduction
A defining feature of child abuse trauma is that, unlike post-traumatic stress disorder (PTSD), there is usually not a single identifiable event but a history of multiple episodes of abuse. Hence the use of the terms complex trauma or complex post-traumatic stress disorder (CPTSD) to distinguish it from PTSD. Remarkably, given the origins of the problem, more attention has been given to child abuse trauma in adults than children. For example, the International Statistical Classification of Diseases (ICD-11) does not have separate criteria for complex trauma in children (World Health Organization, 2022).
The United States National Child Traumatic Stress network identified seven domains of impairment in children exposed to complex trauma: attachment, sensorimotor/somatic problems, affect regulation, dissociation, behavioural regulation, cognition and self-concept (Cook et al., 2003).
Adverse childhood experiences (ACEs) (Felitti et al., 1998) can be divided into direct child maltreatment (physical and sexual abuse, neglect) and intra or inter parental problems leading to disruptions in caregiving; i.e. domestic violence, substance abuse, imprisonment, mental illness (Maneiro et al., 2023). Whether complex trauma is a matter of the severity, type of risk, or accumulation of ACEs is not clear (Lacey & Minnis, 2020; Sidebotham et al., 2016; Sölva et al., 2020). ACEs are useful in research but they have been criticised for reasons including problems in data collection, oversimplification and lack of applicability to individuals (Kelly-Irving & Delpierre, 2019).
The other defining feature of complex trauma is that abuse is usually perpetrated by the child’s attachment figure(s). When the only person available for protection is also the source of threat this leads to ‘fright without solution’ (Hesse & Main, 1999, p. 484) that can produce so called ‘disorganised’ attachment.
Not all abused and neglected children are traumatised but they all use an attachment strategy. Contrary to theory, studies still find securely attached children in maltreated populations. For example, a meta-analysis of attachment in institutionalised children found rates of attachment security as high as 74% (Lionetti et al., 2015). In their review of this problem, De Klyen and Greenberg concluded we lack a ‘widely accepted system that includes the entire spectrum of attachment experiences’ and findings ‘illustrate(s) the limitations of the conventional attachment measures’ (2016, p. 656).
From the conception of his theory Bowlby saw insecure attachment as carrying risks for development but also functional to survival in adverse environments (Bowlby, 1980). Various writers have re-emphasised this, in particular Crittenden (2006, 2016) and Belsky (2006), so that rather than the number or types of ACEs what matters is the ability of the child to organise defences against trauma, including insecure attachment strategies. Likewise psychiatric diagnosis has shifted in emphasis from prioritising the severity of traumatic experience (DSM-3) to the impact of trauma on the sufferer (DSM-4 and DSM-5) (APA, 2013).
Validation of the CPTSD diagnosis produced a number of clinically useful scales (e.g. Briere et al., 1995). These are predominately questionnaires with little use made of semi structured or play based interviews. An exception is the narrative story stem procedure, used in this study and explained below.
Removal from attachment figures is itself harmful (Crittenden & Spieker, 2023) and can be considered another adverse childhood experience. But in serious cases of maltreatment, children are adopted or placed in foster or residential care. Despite its negative reputation the use of residential care in England is increasing (National Audit Office, 2025). Evaluating outcomes of residential care is complicated by the fact that, compared to foster care, these children have experienced more adverse childhood experiences (Briggs et al., 2012) and show greater levels of diagnosable mental health disorders (Oakley et al., 2018; Sanders, 2020) and special education needs (Schoenwald et al., 2022). Whether it is the severity of problems at entry or residential care itself that contributes to poorer outcomes is not clear. Wright and Colleagues (2019) concluded that typical developmental outcomes are possible for young people in residential care when staff provide secure boundaries, warmth, sensitivity and playfulness within routine daily care.
Theory: Crittenden’s Dynamic Maturational Model of Attachment
The majority of attachment studies have used the Ainsworth-Main system that employs the well-known ABC + D categories: A - Anxious avoidant, B - Balanced/secure, C - Anxious ambivalent and D – Disorganised. This study used Crittenden’s Dynamic Maturational Model of attachment and adaptation (DMM) (Crittenden, 2006, 2016) and the DMM is briefly outlined here.
Unlike the infant based ABC + D model, Crittenden’s DMM identifies an array of self-protective patterns that increase with maturation. These are given in Figure 1. At the risk of over simplification, attachment strategies differ in terms of fight, fight, freeze or cling (FFF). Children using Type A inhibit (they freeze) displays of emotion forbidden by maltreating adults, in particular anger, fear or desire for comfort, and focus on the perspectives of their carers (Crittenden, 1992). Put simply they try ‘to be good’. Types A1-2 and C1-2 are based on the Ainsworth-Main patterns and are considered normatively insecure and feature rarely in complex trauma. The A3-8 patterns are variations of a false self, culminating in an A8 profile. Children deploying type C engage in a struggle with carers using displays of anger and vulnerability. The notations A+ and C+ are used as a generic category for A3-8 and C3-8 respectively. The ABC + D disorganised category loosely covers the DMM A+ and C+ patterns, hence the term ‘disorganised’ does not figure in the DMM. In complex and dangerous environments people may use a combination of A and C or A/C (Crittenden, 2016). DMM A+ and C + Patterns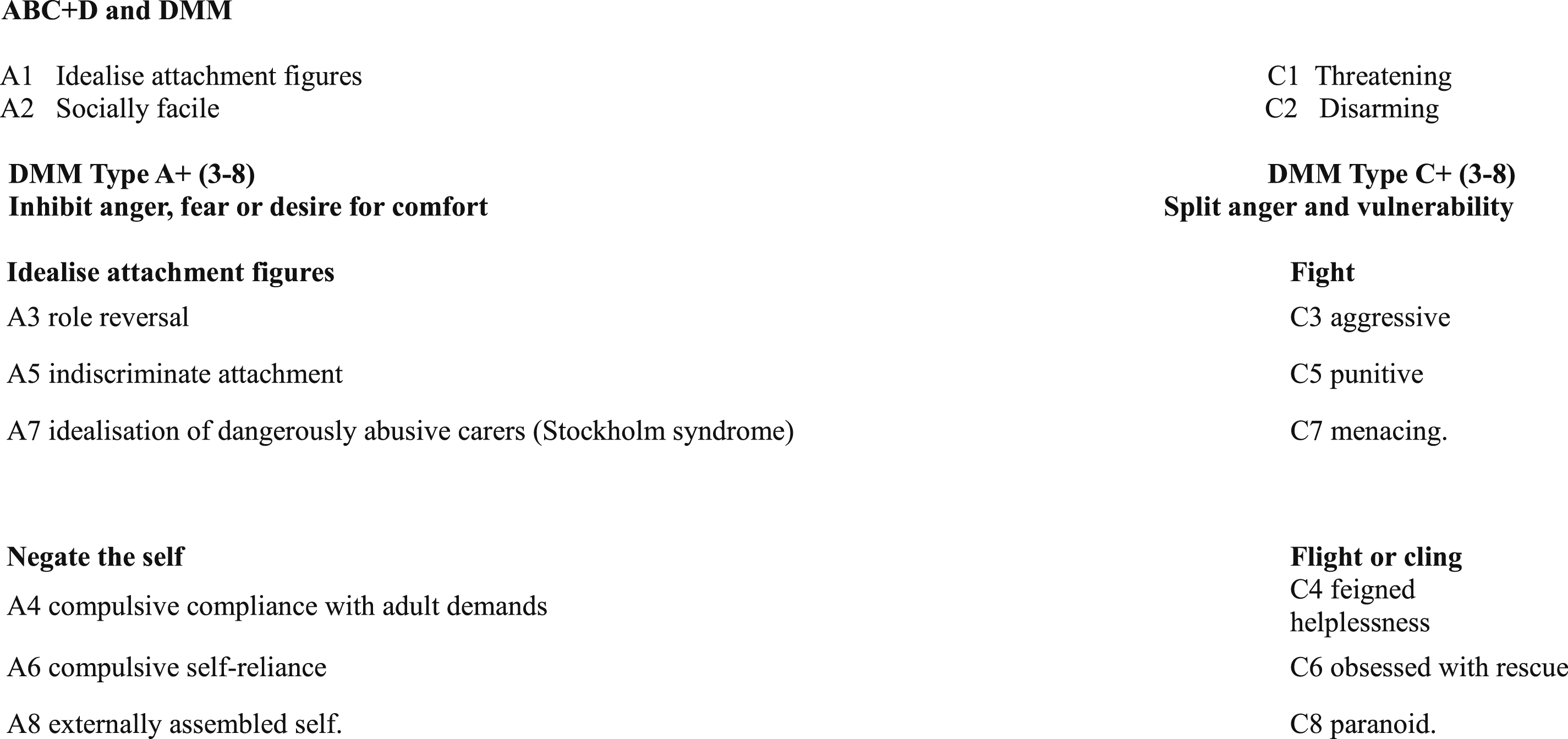
Trauma, Affect Regulation and the Body
An important issue for the assessment of complex trauma is discriminating between attachment behaviour and the effects of trauma. Attachment is a theory of affect regulation whereby infants’ relationships with their attachment figure enables them to co-regulate their feelings and gradually manage their own arousal (Ainsworth et al., 1978; Bion, 1962/1991). Thus attachment behaviour is a means of regulating social engagement. The DMM A+ and C+ patterns describe various forms of social engagement. For example, role reversal (A3) or feigned helplessness (C4). These patterns are strategic, i.e. they are not random, uncontrolled or ‘disorganised’ but function to manage interactions with other people. Conversely, trauma is defined by a lack of social engagement. The child’s emotions and behaviour do not focus on social engagement but self-protection; in extreme cases rage or running away. In the DMM, trauma follows a graduation from conscious processing to the largely unconscious and somatic. At one end the child has access to at least some information about traumatic events and can tell a story about it using language or play (Gil, 2017). At the other trauma is ‘written in the body’ (Lucero, 2018; van Der Kolk, 2015). This is shown in Figure 2. Developmental Trauma – Mental and Somatic representation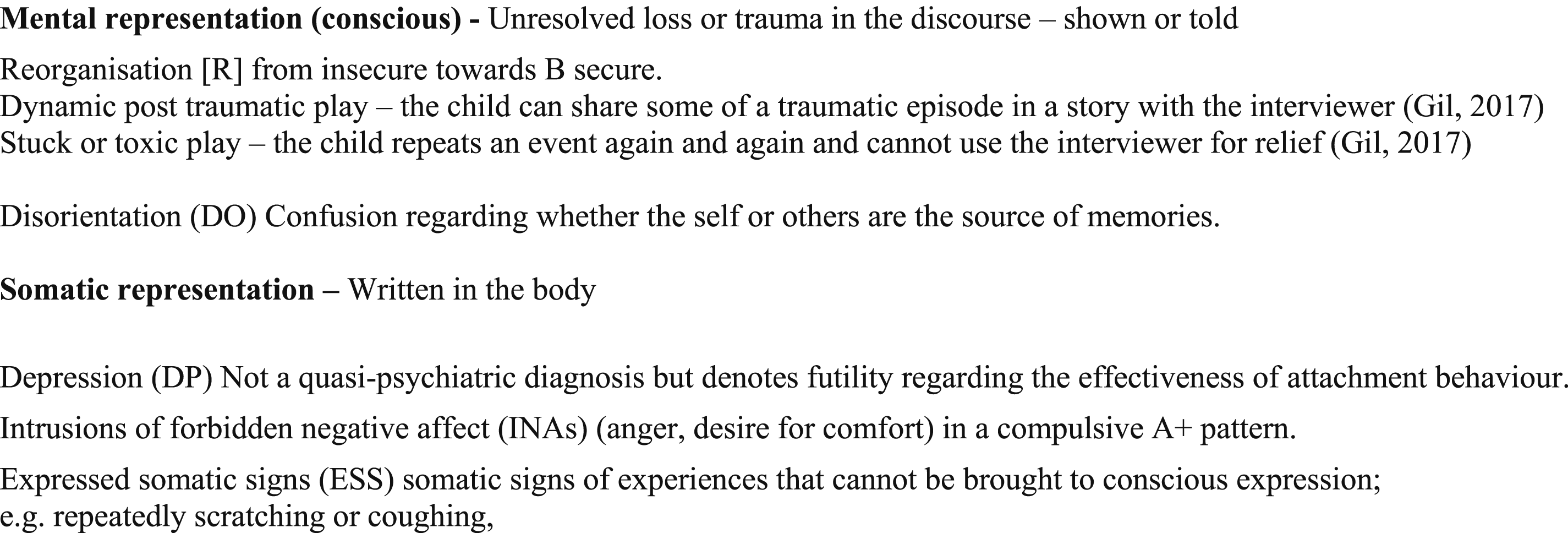
Mental representation means the child can re-present to the self and an attentive adult something of what has happened to them. In somatic representation, trauma is locked in the body so the child has chronic problems with very low or very high arousal. The DMM terms these ‘modifiers’ because, rather than the temporary disruptions experienced in conscious representation of trauma, they have a chronic effect on the self-protective functioning of the child’s attachment strategy (Crittenden, 2016; Farnfield & Onions, 2022). Because children using Type A+ feel responsible for managing their own arousal this inevitably leads to failures: either the depression modifier (see Figure 2) or what the DMM terms intrusions of forbidden negative affects (INAS). In the latter, forbidden displays of anger become rage while desire for comfort may result in what look like ‘inappropriate sexual behaviour’.
Research Approach
The study aimed to build a profile of complex trauma in a sample of severely maltreated children in residential care. Specifically: Attachment, mental and somatic representation of trauma, affect regulation and educational achievement. It also aimed to further demonstrate the construct validity of the CAPA.
The research setting was a therapeutic special school and children’s home in the UK which we are calling Drysdale to protect the identity of the school and the participants. Drysdale is a not-for-profit charity providing education, care and treatment to children aged 5–13 who have experienced early years adversity and trauma (Dockar-Drysdale, 1991). Children stay for 38 or 52 weeks per year and the average length of stay is three years. The integrated psycho-social approach of Drysdale is well documented (Diamond, 2009; Price et al., 2018; Colley & Seymour, 2021; Onions et al., 2024). Psychodynamic thinking, collaborative working and reflective practice underpin the approach and whilst children may be offered various individual or group therapies, the therapeutic milieu of daily living is where the ‘therapy’ takes place. The population of children typically present with complex post-traumatic stress disorder (CPTSD), usually because of early familial maltreatment and neglect (Lofthouse et al., 2024).
Method
Ethical Considerations
Ethical approval for the original study was given by Institute of Education, UCL. The data for this study are part of a larger set reported elsewhere (Gutman et al., 2018).
Participants
The parents and carers of forty-five children gave their written consent for the use of their anonymised data. Fifty children were assessed but the data of 5 children could not be included either because they did not want their faces to be appear on the film or they terminated the procedure prematurely. In a previous paper we reported on data from 41 children (Farnfield & Onions, 2022). Subsequent revision has increased the number to 45. The four children included in the data analysis for this paper did not differ significantly on any demographic variables or numbers of ACEs to those in the previous paper.
Data Collection
The data outlined below were collected over a six-year period, for each participant at two time points. Time 1 (T1) six months after the child started at Drysdale and time 2 (T2), 2 years later. The following demographic data were collected: number of siblings; age of parents at child’s birth; mother’s substance abuse in pregnancy; substance abuse by either parent in first year of child’s life; parental imprisonment; parent mental illness in child’s first year; parent learning disability; non organic failure to thrive (NOFT); neglect; physical abuse (PA); child sexual abuse (SA) and domestic violence (DV), DSM-5 psychiatric diagnoses (APA, 2013) and medication. These were subsumed into ACE scores. Educational attainment data were collected using four of the academic progress indictors according to national curriculum levels, specifically: reading, writing, speaking and listening, and shape, space and measure (Gutman et al., 2018).
Procedure
Children were assessed using the Story Stem Assessment Profile (SSAP) (Hodges et al., 2000). The SSAP uses the established narrative story stem procedure whereby the interviewer gives the beginning of the story and asks the child to ‘tell me and show me what happens next’. It shows good construct validity when used with community, abused and adopted children (Hillman et al., 2020). The children were asked to complete the same 14 stories at both time points. The procedure was video recorded and each session took 60 - 65 minutes.
Data Analysis
The SSAPs were analysed using the Child Attachment & Play Assessment (CAPA). The CAPA has excellent construct validity regarding differentiation of maltreated children from community comparisons (Farnfield, 2016, 2025). There is also significant correspondence between CAPA coding for unresolved trauma and the Trauma Symptoms Checklist for Young Children (Briere, 2005) (Zhang et al.,in preparation). In keeping with other discourse based attachment assessments, the SSAP and the CAPA are not questionnaires and do not produce alpha scores.
The CAPA reports on four dimensions: 1. DMM attachment strategies with the addition of quasi autistic (QA); this is defined by low level of symbolic play, concrete thinking and absence of relationship with the interviewer. Although, in the DMM, A8 is an adult pattern, A8 has been part of the CAPA coding since its inception. 2. Mental representation of unresolved loss and trauma (Ul & Utr); this is determined by dysfluency in the child’s speech or play. 3. Somatic representation. Observed low or high arousal. 4. Story themes that repeat across two or more stories.
The first author blind coded all 90 story stems and two raters coded a subset of 12 stems (ICC = .916 with 95% confidence interval = .66–.99) giving an overall agreement of moderate to excellent.
Demographic Data
The participants were forty-five children, 30 male and 15 female: 87% white, 13% black African or dual heritage. Their age at T1 ranged from 7 to 11 years (mean 8.7 years). Forty of the children were first born. The mean number of siblings was 2.7 and mean birth order 2.1. Seven children had no siblings. At T1, 38% were living with at least one of their birth parents (18% with birth mother) and 2 with grandparents. These two groups were collapsed and labelled ‘kin care’. 38% were in foster care, 18% adopted and one was from another residential placement (subsumed into the foster group). The mean age of the children’s mother at birth was 23.7 years with a mode of 19 years; 64% of first born children were born to a mother <20 years of age (X2 (1, N = 30) = 4.043, exact p < =.063).
The number of previous placements ranged from 0 to 7 (mean 2.6) with one outlier with 22 placements. Eleven children (24%) changed placement during the study period. Children who changed placement were more likely to be girls (X2 (1, N = 45) = 6.016, exact p < =.026) and in foster care (X2 (1, N = 45) = 7.565, exact p < =.011).
Fifteen children (33%) had negative life events during the study period that could be expected to hinder their progress. These were divorce of foster carers, adoption breakdown and serious illness of their primary carer.
Comparison Group
Thirty children from the school sample were compared with 30 children from a comparison group drawn from an English Local Authority Children’s Services Child Protection Team. The children were matched for age, gender, ethnicity and whether living with kin, adopted or in foster care.
Statistical Analysis
Associations and differences between groups were tested using chi-square for categorical data with Phi (
To evaluate change between T1 and T2, a matrix was devised using 4 dimensions with scales ranging from 0 to 4. The dimensions were (see Figure 2 for abbreviations): modifier (0 absent, 1 partial DP, 2 one from INA, ESS, DO, full DP, Dissociation, Hypervigilance and Paranoia); Unresolved loss (absent 0, present 1); Unresolved trauma (absent 0, present 1); Attachment risk (0 = A1-2, C1-2, R 0, 1 = A3-4, C3-4, 2 = A5-6, C5-6, QA, 3 = C7-8, A8, 4 = A/C 4). The scores from the four dimensions were summed to form a total score. Total scores at T2 were subtracted from those at T1 to produce a change score yielding three groups of children: those who had improved, deteriorated or showed no change. Finally, a multinomial logistic regression was performed with improvement, deterioration and no change as the dependent variables and study variables as covariates.
Missing Data
The range of missing data for ACEs was 9–44% with an average of 33%. Cases with missing data were omitted for bivariate analysis. For continuous variables and regression analysis, missing data were replaced by estimate of means.
Results
ACEs, Diagnoses and Placement
Bivariate Correlations With ϕ Values Between ACEs, DSM5 Diagnoses and Placement
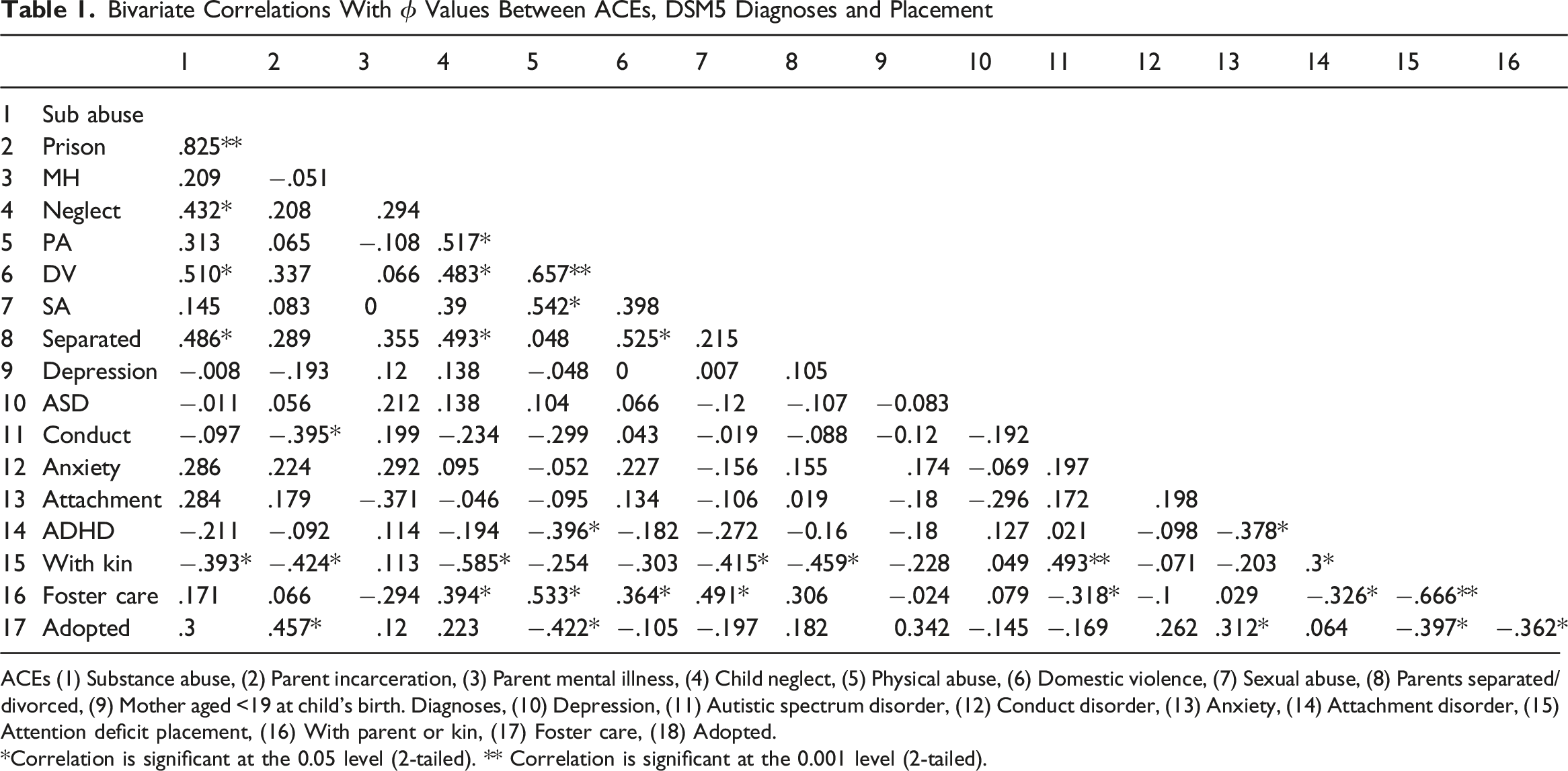
ACEs (1) Substance abuse, (2) Parent incarceration, (3) Parent mental illness, (4) Child neglect, (5) Physical abuse, (6) Domestic violence, (7) Sexual abuse, (8) Parents separated/divorced, (9) Mother aged <19 at child’s birth. Diagnoses, (10) Depression, (11) Autistic spectrum disorder, (12) Conduct disorder, (13) Anxiety, (14) Attachment disorder, (15) Attention deficit placement, (16) With parent or kin, (17) Foster care, (18) Adopted.
*Correlation is significant at the 0.05 level (2-tailed). ** Correlation is significant at the 0.001 level (2-tailed).
There were no significant correlations with ACEs and age, ethnicity, parent learning disability or birth order of the child. Fostered children had significantly more ACEs than adopted children or those living with kin (mean difference −1.525, t = −2.853, df 43, p = <.007) and children in kin care significantly less (mean difference 1.996, t = 4.121, df 43, p = <.001 d 1.244). Females suffered sexual abuse more than males (.387, p = <.009).
The mean number of ACEs for children with no previous placements was 2.8 and those with 1–3 placements 4.7 (t = −3.224, df 32, p = <.003). The mean number of ACEs for children who changed placement while at the school was 5.5 compared with 3.7 for those who did not (t = −3.423, df 43, p = <.001). Mother’s age at the child’s birth was negatively correlated with number of ACEs (−.560, p = <.001).
Principal component analysis (PCA) using oblimin rotation and kaiser normalisation identified two components with an eigenvalue greater than one. (1) Substance abuse, mental health and parental separation; (2) Mental health (determinant = .195, p = <.001). The two components explained 58% of the variance.
A second PCA was conducted adding age of mother at child’s birth. Three components were identified: (1) Substance abuse, parental separation, mother aged <20 years at child’s birth and domestic violence. (2) Physical and sexual abuse and (3) Mental health (determinant = .170, p = <.014). The three components explained 64% of the variance.
At T1 91% of the children had at least one DSM-5 diagnosis. The number of diagnoses ranged from 0 to 5 with a mean of 2 (56% had two diagnoses). The most common diagnoses were: attachment disorder (69%), conduct disorder (56%) anxiety disorder (36%), attention deficit hyperactivity disorder (ADHD) (31%), autistic spectrum (ASD) diagnosis (9%) and depression (7%). Internalising 13.3% (n = 6), externalising 44% (n = 20) and dual internal/external 24% (n = 11). Children living with kin were more likely to be diagnosed with ADHD or conduct disorder than fostered children. Adopted children were more likely to have a diagnosis of attachment disorder.
At T1, 40% were on medication for social-psychological problems and 66% of these were diagnosed with ADHD. At T2 this had dropped to 16% but was still higher than expected (X2 (1, N = 45) = 12.434, exact p <= .001). Of the children who changed placement, only one (9%) was on medication at T1 (X2 (1, N = 45) = 5.795, exact p <= .031).
Attachment
Distribution of DMM Patterns at T1 and T2
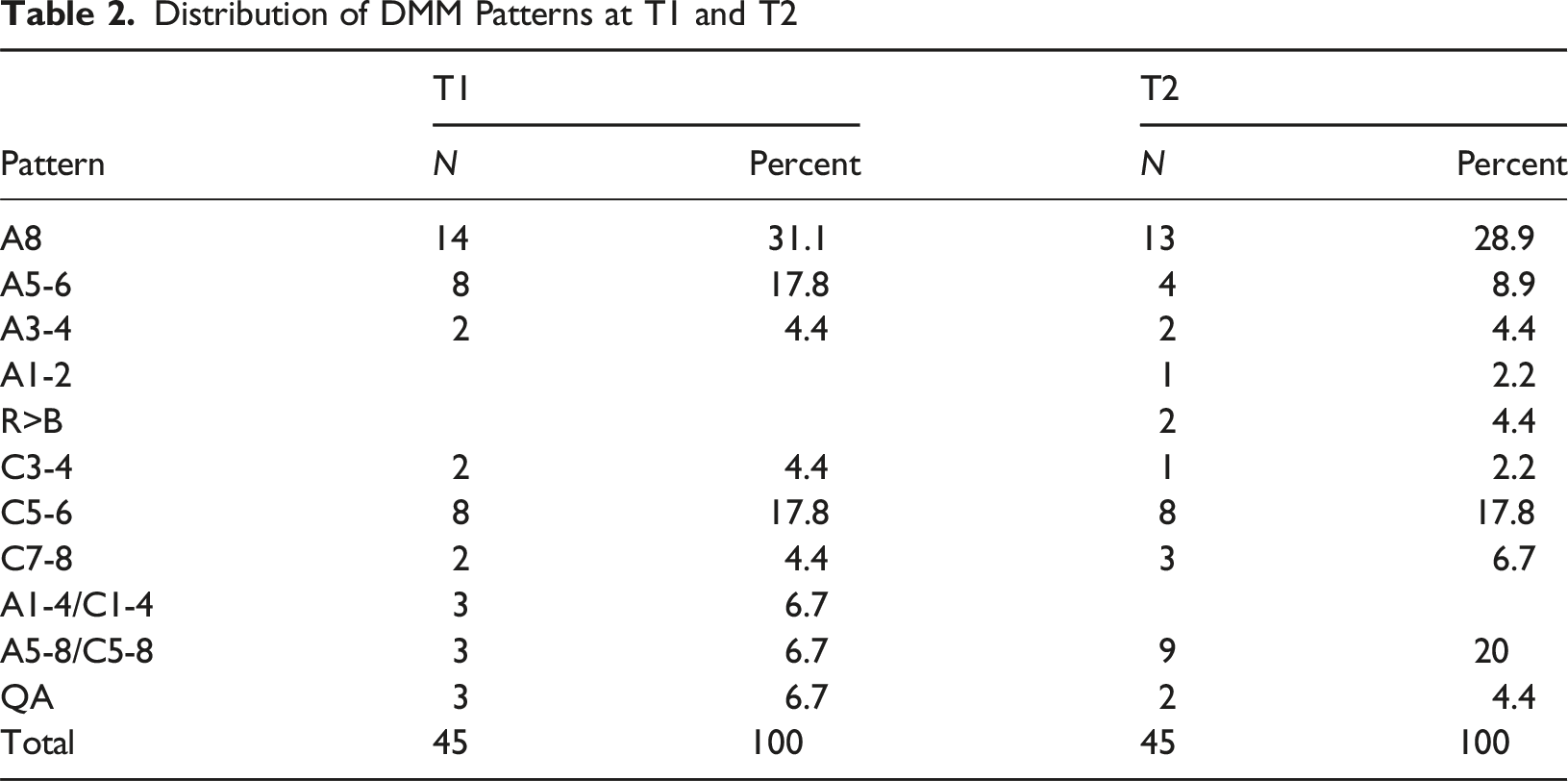
Using a 3-way A, C and A/C distribution, with quasi autistic (QA) rated as A, overall stability of attachment was 64%, Cohen’s kappa was moderate (.442, exact p = <.001). The most stable group were C+ (83%), followed by A+ (70%). A/C was the most labile, with only 1 stem rated A/C at both time points (17%).
The CAPAs of 29 children (64%) were rated in the same pattern at both time points; 15 (33%) moved to or from A/C. Two were rated QA at both time points. Only one was theoretically discrepant, moving from QA to C5-6.
Change in attachment security was determined using the attachment risk scale used in the matrix (0 = A1-2, C1-2, R 0, 1 = A3-4, C3-4, 2 = A5-6, C5-6, QA, 3 = C7-8, A8, 4 = A/C 4). There was no significant change between T1 and T2 (mean .0444). Using a three way distribution there was no significant difference between attachment pattern and number of ACEs at either time point. At T1, there was a significant correlation between attachment risk and number of placements (r = .304, N = 45, p < .042 two tailed) and a negative correlation between attachment risk and number of siblings (r = −.356, N = 45, p < .016 two tailed).
There was no significant difference between the three way attachment strategies of the school sample at T1 and the local authority comparison group (X2 (2, N = 60) = 2.957, p = <. 228). But the school sample had significantly more stems rated A8 (37% compared with 13%) (X2 (1,N = 60) = 4.356, p = <. 037).
Attachment and Diagnoses
At T1, 81% of anxiety disorders were in the A+ group (X2 (2, N = 45) = 5.881, exact p = <. 046, ϕ.358) and 75% at T2 (X2 (2, N = 45) = 6.593, exact p = <. 044, ϕ.395). Omitting dual diagnoses, and using the 3 way distribution, at T1 and T2 only Type A+ were diagnosed with internalising disorders; Type C+ had more externalising disorders than expected and this was significant at T2 (X2 (4, N = 34) = 10.387, exact p < =.034) ϕ.553).
Trauma and Loss
Distribution of Utr and Uloss at T1 and T2
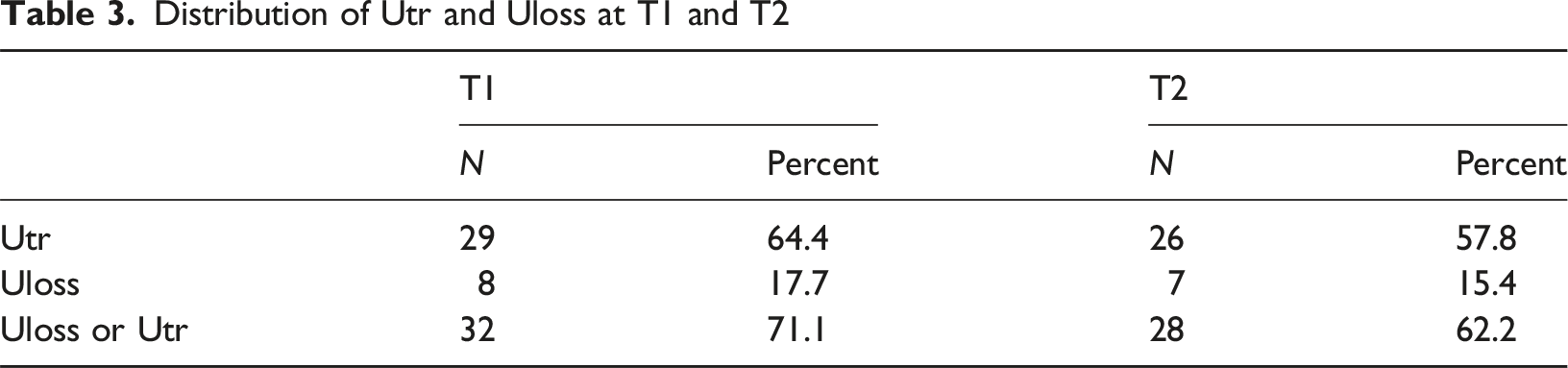
At T1 the A+ pattern accounted for 65% of Utr and C+ for 24%. At T2 the distribution was 58% Type A+ and 19% C+. Children using an A+ strategy at T1 were significantly more likely to be assessed with Utr at T2 than Type C+ (X2 (2, N = 45) 11.523, exact p = <. 003; kappa (.4184, p = <.001).
Bivariate Correlations With ϕ Values Between Loss, Trauma, Story Themes, ACEs and Diagnoses
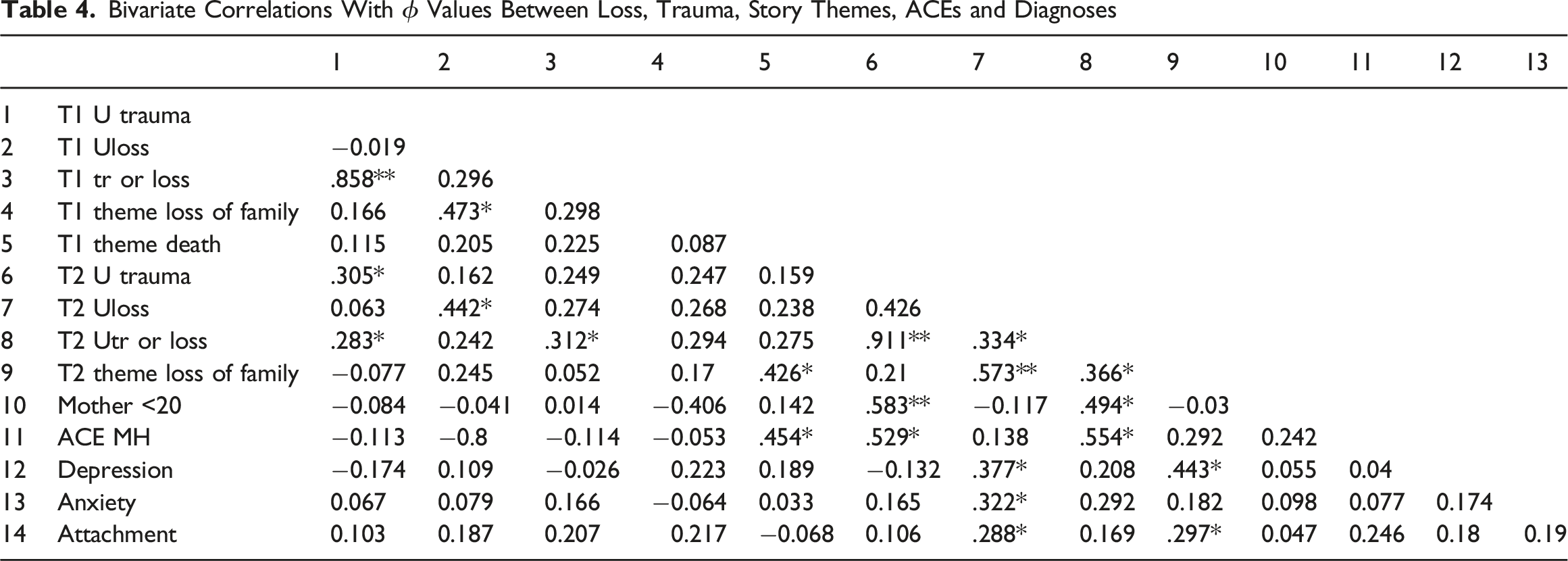
There were no significant correlations at T1, other than story themes containing death. At T2 unresolved loss was associated with diagnoses of depression, anxiety and attachment disorders. Children whose story themes depicted loss of family were also likely to be diagnosed with depression and attachment disorder. Unresolved trauma correlated with parental mental illness and a birth mother <20.
Modifiers
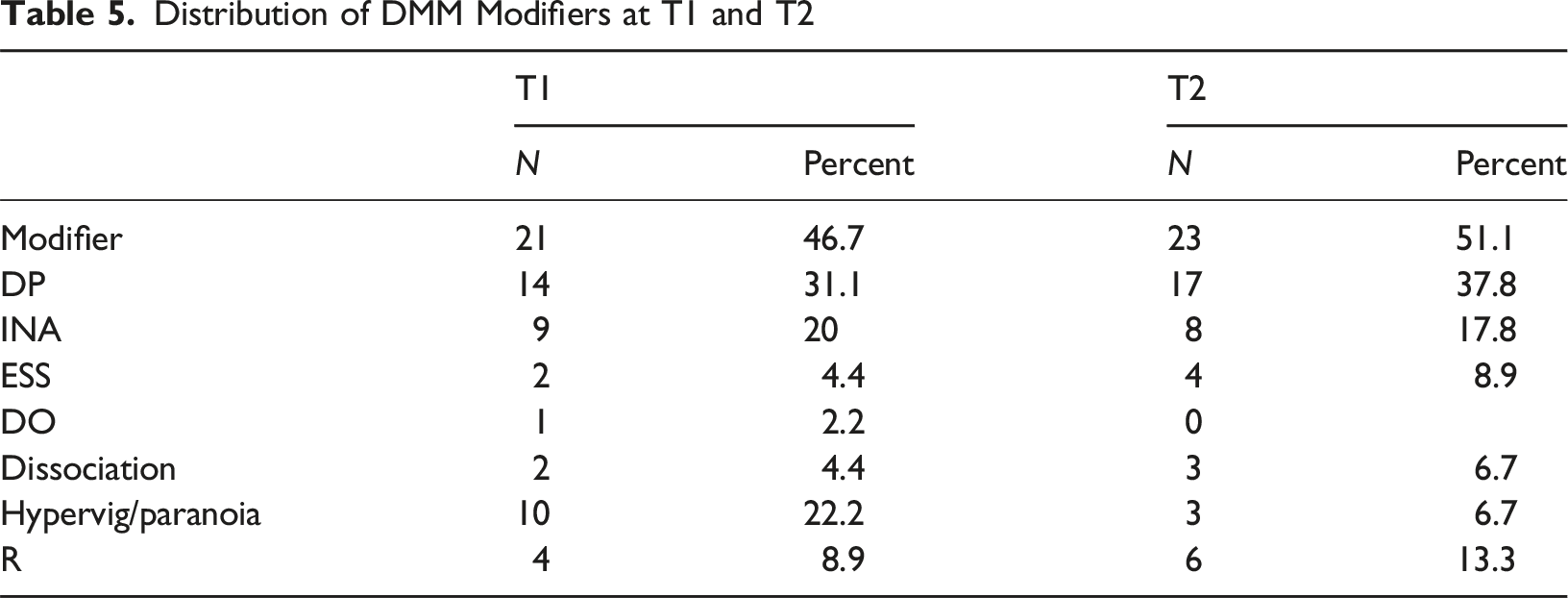
Distribution of DMM Modifiers at T1 and T2
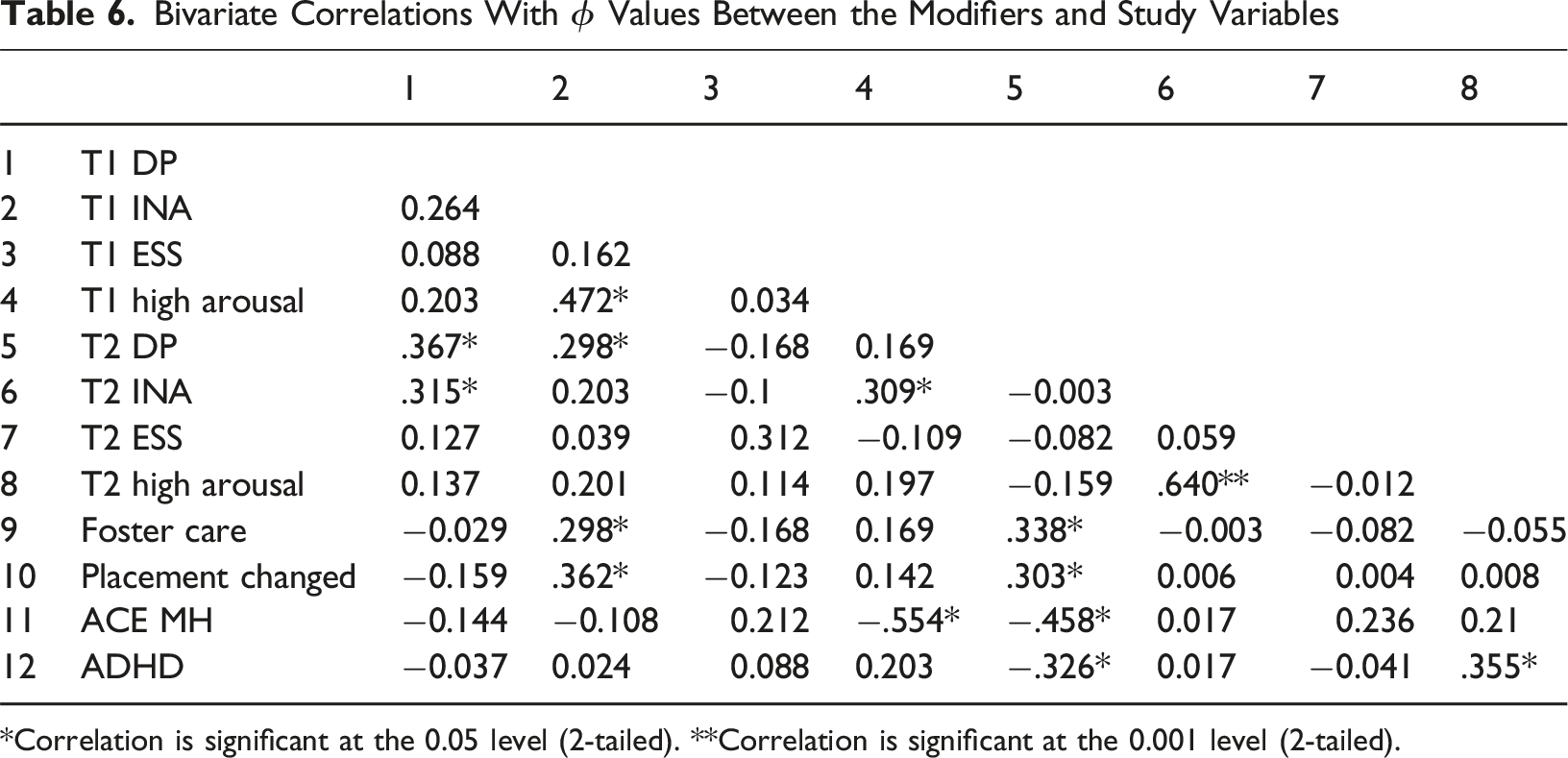
Bivariate Correlations With ϕ Values Between the Modifiers and Study Variables
*Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.001 level (2-tailed).
There was an association between DP at T1 and INAS at T2, and between INAS at T1 and DP at T2. There was no significant relationship between the modifiers and number of ACEs nor the modifiers and number of previous placements. There was an association between: INAS at T1 and both foster care and changing foster placement; placement change and DP at T2. Controlling for gender, there was a significant correlation between INAS and boys who changed placement, but not girls (X2 (1, N = 45) = 6.887, exact p <= .031).
At T2 the DP modifier showed a positive association with foster care and a negative with parent mental health and ADHD. DP at T2 was negatively associated with being on medication at the T1 (X2 (1, N = 45) = 5.688, p <= .017). At T2 all four ESS were diagnosed with conduct disorder (X2 (1, N = 45) = 3.512, exact p <= .085).
Education
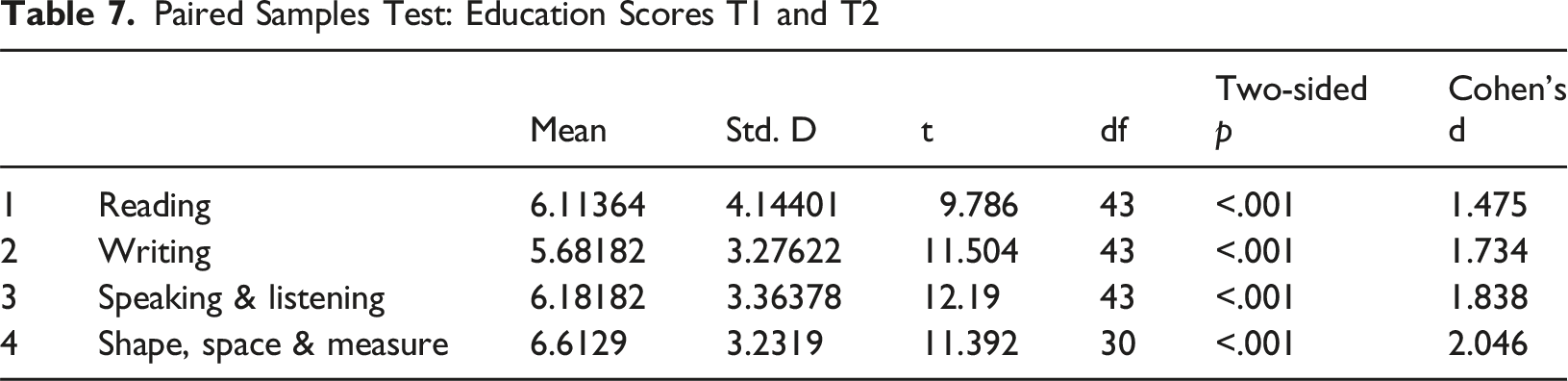
Paired Samples Test: Education Scores T1 and T2
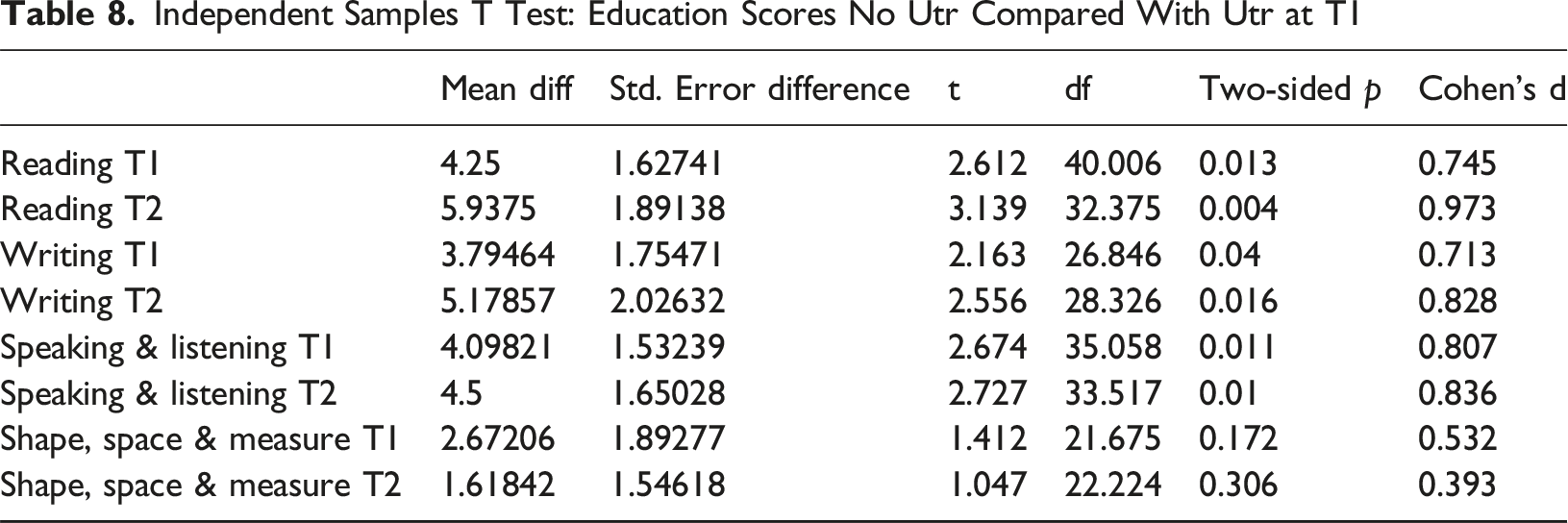
Independent Samples T Test: Education Scores No Utr Compared With Utr at T1
Change Matrix
The means for all five dimensions (arousal, trauma, loss, attachment risk and total score) at T1 were higher than those of the Local Authority comparison group but only attachment risk was significant .733 (t = −3.241, df 56, p = <.002; Cohen’s d 1.362). Means for the 5 dimensions were higher at T1 than T2 but not significant; mean for total scores was 4.1333 at T1 and 3.866 at T2 (t = .791, df 44, p = <.433).
Fifty one percent (n = 23) of participants showed scores which improved, 16% (n = 7) showed no change and 33% (n = 15) showed a deterioration.
At T1, improvers had higher means scores for attachment risk and for total risk than those whose score had deteriorated. Mean difference for attachment −.765 (t = −2.946, df 36, p = <.006; Cohen’s d .782) and for total risk score at T1 -1.382 (t = −2.253, df 36, p = <.016, d1.645).
There was no significant relationship between change and diagnosis, gender or ethnicity. At T2 girls had significantly lower scores on arousal than boys, mean difference 1.0 (t = 3.864, df 43, p = <.001) Cohen’s d = .818, and also on the total risk scale, mean difference 1.60 (t = 2.520, df 28.14, p = <.018) Cohen’s d = 2.009. The mean number of ACEs including mother’s age were: improved 3.47, no change 4.1 and deterioration 4.6 (deterioration v improvement t = 1.659, df 29.36, p = .108 two sided, p = 0.54 one sided, Cohen’s d .554).
Bivariate Correlations Between Change and Study Variables
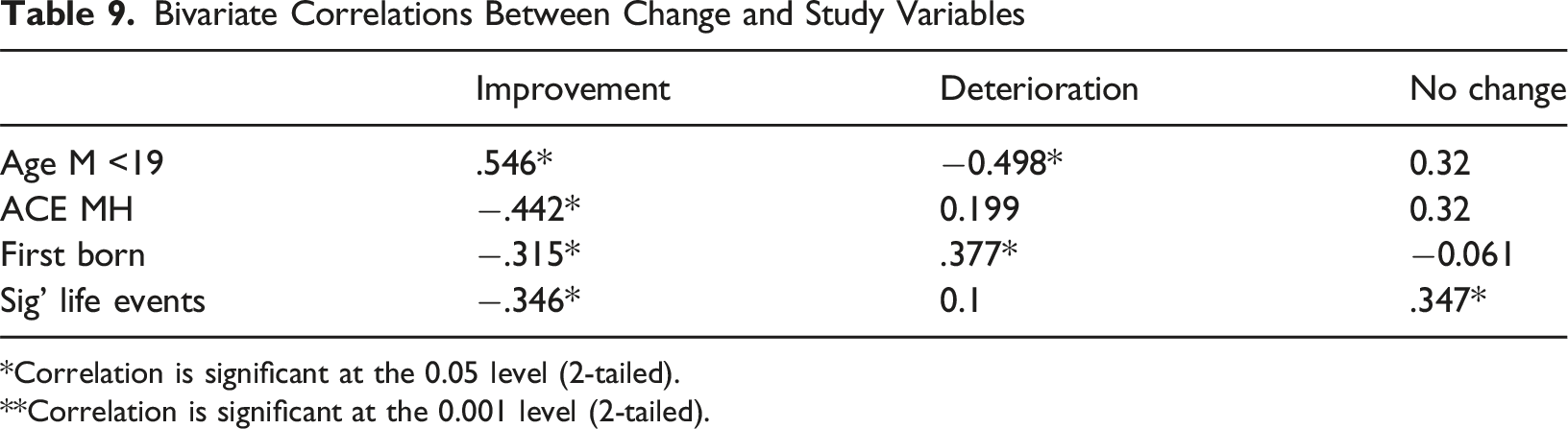
*Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.001 level (2-tailed).
Two multinomial logistic regressions were performed with improvement, deterioration and no change as the DV. In the first, covariates were number of ACEs, siblings, previous home placements and mother’s age. Thirty one cases were analysed and the overall model was found to be statistically significant (X2 (8) = 36.546, p = .004). Number of siblings (7.437 p = .024), placements (8.002 p = .018) and mother’s age (11.800 p = .003) made a significant contribution to the model but not the number of ACEs (.466 p = .791). Compared with children with deteriorating scores, children assessed as improved had more siblings (1.000 p = .035, OR = 2.718) older mothers (.382 p = .020 OR = 1.465) and more previous placements (1.026 p = .033 OR 2.790). Only 4 children’s cases were entered under no change and there were no significant correlations. Overall percentage for correct prediction was 74.2% (88% improvement, 80% deterioration and 0% no change).
In the second, all the ACEs were entered as covariates using estimated means. 45 cases were analysed and the overall model was found to be statistically significant (X2 (16) = 28.026, p = .031). Mental health (9.633 p = .008), physical abuse (8.587 p = .014) and domestic violence (8.354 p = .015) made a significant contribution to the model. Compared to those with deteriorating scores, children assessed as improved had fewer parent mental health ACEs (−2.226 p = 058 OR .108), those who did not change had suffered less physical abuse (−6.996 p = .035 OR .001) but more domestic violence (6.856 p = .040 OR 949.285). Compared with improvers, no change had experienced more physical abuse (5.549 p = .023 OR 257.095) and domestic violence (6.522 p = .047 OR 679.980). Overall percentage for correct prediction was 66.7% (82% improvement, 47% deterioration and 57% no change).
Discussion
The main finding from this study is that while attachment is important, more attention should be given to deepening our understanding of affect regulation: why do some children find it so hard to regulate their behaviour? Why do they have periods of calm then suddenly fly into a rage? Why are educational results for looked after children so poor? What do the diagnostic labels we give to traumatised children actually mean? This research offers a few pointers.
The children in this study were at the extreme end of traumatic experience. They had more adverse childhood experiences than the comparison group of children under child protection and, in common with Westlake and Colleagues’ (2023) meta-analysis of residential care, they had more externalising than internalising diagnoses. They likely entered residential care because they could not be managed in the community.
The lack of change on the indicators we used is at first sight disappointing. After 2 years in a therapeutic residential setting fifty one percent of the children showed a reduction in representations of trauma and a third were estimated to have increased trauma representations. Children with fewer trauma representations had significantly higher scores for attachment risk at T1. Put bluntly, they were so insecure at entry to Drsydale there was little room for further deterioration. The mental processing of trauma requires safety and it is possible that some of the children assessed as having increased trauma representations were going through a period of reorganisation that entailed depression; hence the increase in the depression modifier, which may have skewed results at T2. This is a common phenomenon in therapy, the idea of feeling worse before getting better (Shedler, 2022). That improvement was associated with children who were offered and engaged with individual therapy suggests these children had reached the window of tolerance (Siegel, 1999) necessary for therapeutic change. In addition, during the study a third of the children experienced negative life events, mainly loss of a carer through divorce or adoption breakdown, that may have impaired any progress.
None of the children with zero recorded ACEs were unresolved regarding trauma. Other than that the number of ACEs had much less impact on trauma representations than types and constellations of ACEs. The main problems for the children whose scores deteriorated may have been the impact of being born to young unsupported mothers under the age of twenty and/or maternal mental illness during their perinatal period. There is strong evidence that disruptions of care in infancy can lead to developmental difficulties, including affect regulation, with boys being more at risk than girls (Harris et al., 2023; Power et al., 2021). Girls in this study had lower observed physiological arousal than boys. Lyons-Ruth (2025) argues that infant neglect is more salient than threat (physical abuse, being shouted at or threatened) with regard to effects on brain development. Some of the children with deteriorating scores had chronic problems with regulating physiological arousal that may have been present from the first years of life.
The association of improvement with a higher number of previous placements is, at first sight, puzzling. Whatever changes occurred in their family placement, none of the children moved from Drysdale and it is possible the staff acted as stable secondary attachment figures.
Unlike most ABC + D studies, none of the stems were rated secure or normative insecure at T1 and only three at T2. The goal of producing secure attachment in children as traumatised as these is, at least in the short term, unrealistic. An important finding is the number of children using the externally assembled self or Type A8 pattern (31% at T1 and 29% at T2). The A8 attachment strategy is predicted to develop from multiple home placements (Crittenden & Landini, 2011) and this study is the first to provide empirical evidence. Children using this pattern are ‘actors’ who pretend to be the child other people want them to be. This makes it hard to distinguish from secure attachment, perhaps one of the reasons for the bias towards a B attachment pattern in other studies. Identifying this pattern in looked after children is important when planning for placements and interventions with an emphasis on careers helping the child find a true self.
The shift at T2 to the A/C strategy is likely due to the added complexity of forming attachments to the school staff while still bound to a long term family placement.
Taken across the two study time points children in A+ showed a wave of arousal from very low (depression) to manically high and were more likely to be diagnosed with anxiety disorder. Children, particularly boys, who showed explosive intrusions of negative affect (INAS) at T1 were more likely to change placement and to show the depression modifier at T2. This suggests it may be possible to predict behavioural problems early enough in a placement to avoid breakdowns.
At a more general level, children whose stories were assessed as unresolved loss at T2 were significantly more likely to be diagnosed with depression, anxiety or attachment disorders and, crucially, to play out scenes depicting loss of family. For these children ‘attachment disorder’ was less a medical problem than the response to loss of their family, whether birth or previous foster carers is not clear.
Type C+ proved to be better organised than A+ in that it showed less unresolved trauma and was more stable over the 2 year period. This supports the hypothesis that type C+ is informed by a traumatic history while A+ is derailed by it. The type C+ strategy uses fight, flight and cling to, sometimes subtly, coerce attachment figures and other carers into attending to the child’s needs. It is interesting that C+ had significantly more externalising disorders; using this argument it was less a matter of a ‘disorder’ and more the result of a strategy – an organised way of engaging with and managing other people. This means the child in Type C+ is better able to control their behaviour and is also more resistant, in attachment terms, to change.
An important message from this study is that unresolved trauma and loss is pernicious. Trauma showed a stability of 69% over a 2 year period; higher than attachment at 64%. Trauma had a significant impact at both time points on all but one of the education measures. This included children living with kin (88% with a birth parent) who had significantly lower ACEs but no significant difference in trauma. This chimes with Mezzacappa et al. (2001) study of boys attending therapeutic schools; controlling for IQ and medication status, they found abused children experienced impaired cognitive development. It also suggests that one way to improve education results for looked after children is to treat unresolved trauma.
Although this paper has not examined the psychodynamic, collaborative and reflective approach of Drysdale in any detail, the model of intervention is relational and at its core is the focus on supporting education and care staff to make solid trusting relationships with traumatised young children, as this has been a real deficit for them. Many readers will appreciate that the work can be challenging and therefore effectively supporting staff underlies the model. Here, support means thorough and ongoing training about the complex needs of these children, alongside an embedded model of reflective practice as outlined by Price and colleagues (Price et al., 2023).
Validity of the CAPA
Few studies have used narrative story stems with children of this age. Stability for three way, A + C + A/C, attachment was 64% over 2 years with 69% for unresolved trauma. Only one change in attachment was theoretically discrepant and this was a child diagnosed with pervasive developmental delay. Validation of the ABC + D Manchester Child Attachment Story Task (MCAST), with children aged 5–7 years, found 76.5% of ABC categories (71% for insecure) and 69% of D remained stable over a median 5.5 month period (Green et al., 2000). This study compares favourably with their D.
The convergence of the DMM-CAPA A+ pattern with DSM-5 anxiety disorder, and empirical validity of A8 and the A + DP/INA arousal cycle is particularly encouraging, as is the further validation of the unresolved trauma coding. The CAPA offers a more finely calibrated analysis than that obtained by the more usual questionnaire assessment of complex trauma and is useful in devising treatment plans for individual children.
Limitations
With a high number of variables and a sample of only 45 the findings from this study must be treated with caution. In addition the missing data on some ACEs necessitated a parsimonious approach to analysis. The children were asked to complete 14 stories, which took over an hour. Some children disengaged or, for reasons of anonymity, did not show their faces on the video. These factors made coding more difficult. Finally the matrix we devised to assess change likely misses more subtle indications of improvement.
Footnotes
Ethical Consideration
Ethical approval for the original study was given by University College London.
Consent to Participate
Informed verbal consent to take part in the interviews was given by the children.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Mulberry Bush School.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Caryn Onions was until recently senior research officer at the Mulberry Bush and Steve Farnfield was paid by the Mulberry Bush to analyse and report on the data.
Data Availability Statement
Anonymised data is available on request.