
Abstract
Clinical decision-making in infant and early childhood mental health can be complex, shaped by clinical, legal, contextual, and personal factors. At the core of this complexity, however, lies an ethical dimension, which interacts with all other aspects of decision-making. This paper introduces a multidimensional model that places ethics at the centre of clinical formulation, offering a structured yet flexible approach to understanding complex challenges faced by practitioners. Through a series of illustrative cases, we demonstrate the model’s applicability across diverse practice settings. A Mother-Baby Unit case highlights tensions between maternal mental health and infant well-being. A home visiting case examines how to balance a mother’s autonomy with concerns for infant safety in the context of domestic violence. A neonatal case explores how a physician’s personal history influences treatment recommendations, raising questions about consent. A childcare case considers conflicts between institutional caregiving policies and parental preferences. These cases demonstrate how ethical considerations should underpin clinical reasoning, even when not obvious. By explicitly integrating ethics into clinical formulation, this model provides a tool for practitioners navigating complexity. It has applications in clinical training, professional development, and reflective supervision, fostering a culture of ethical awareness in infant and early childhood mental health practice.
Plain language summary
Making decisions in infant and early childhood mental health (IECMH) can be complicated. Clinicians must consider many factors, such as medical knowledge, legal rules, work environment, and their own personal experiences and beliefs. However, at the heart of these decisions is ethics - the question of what is right to do and good for the child and their caregivers. This paper introduces a model that helps professionals think through difficult decisions by putting ethics at the centre of their reasoning. We illustrate this model using real-world examples. One case from a Mother-Baby Unit explores the challenges of supporting a mother’s mental health while also protecting her infant’s well-being. Another case from home visiting services looks at how to support a mother in an unsafe relationship while ensuring her child’s safety. A neonatal intensive care case highlights how a doctor’s personal history can shape medical decisions, raising concerns about how parents can make informed choices. Finally, a case in a childcare setting examines tensions between professional caregiving policies and parental wishes. These examples show that ethical thinking should guide decision-making, even when the dilemma isn’t obviously ethical in nature. By using this model, IECMH professionals can better navigate complex situations. This approach can also support clinical training, professional development, and supervision, helping to create a culture of ethical awareness in the field.
Introduction
Dimensions to Consider in Complex Decision-Making
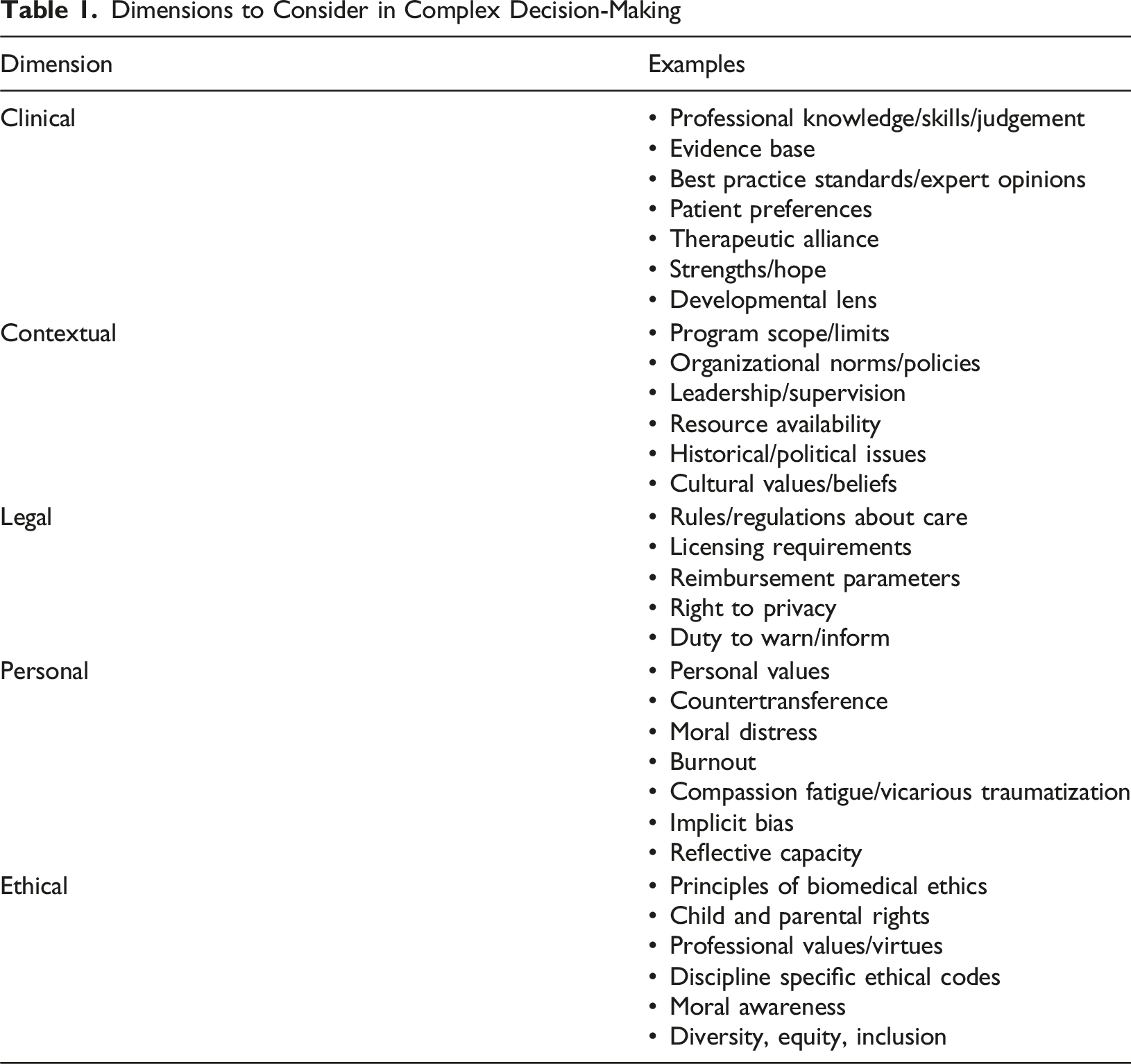
Special features of infant and early childhood mental health (IECMH) amplify the complexity of ethical issues in clinical practice (Lim et al., 2023). Infants are developmentally vulnerable and malleable compared to older children, adolescents and adults (Lyons-Ruth et al., 2017), and therefore, they are especially sensitive to their caregiving environments. Second, an infant’s utter dependence on adult caregivers necessitates that practitioners provide care to multiple patients with distinct interests that do not always align. Third, there is an emergent issue of specific infant rights and correlative parental duties of protection and provision of care (World Association for Infant Mental Health, 2014) that must be reconciled with parental and reproductive rights and duties of non-interference. Finally, because the field of IECMH is beset by workforce shortages, limited training opportunities, and inadequate resourcing relative to demand for services, questions of how practitioners can do good enough work without doing harm become paramount. A related challenge is the inherent (and essential) multidisciplinarity of the field, which creates areas of overlap, shortfall and ambiguity when it comes to practitioner scope, competency and professional governance.
These uniquely important challenges underscore the importance of adding an ethical lens to complex clinical decisions involving young children and their caregivers. Applying an ethical perspective to a decision involves asking questions relating to moral values and the “goodness” or “rightness” of actions that could be taken. Such questions serve to clarify underlying tensions, draw attention to missing facts, and highlight the moral principles, concepts and frameworks that should anchor decision-making. The ethical dimension of decision-making intersects with multiple other decision-making dimensions (i.e., clinical, legal, personal, contextual). Together, these dimensions are inextricably interconnected parts of the whole picture, but the ethical dimension is so essential to good practice that it should be considered the heart of complex decision-making.
In this report, we propose a conceptual model to help clinicians formulate the multiple dimensions of complex decisions in IECMH, placing the ethical dimension at the centre (Figure 1). The other dimensions of complex decision-making noted in Figure 1 vary in salience according to the specific features of a case and come into and out of salience with the clinician’s awareness and attention. When facing complex clinical decisions, systematically considering these dimensions may be clarifying, yet we submit that the ethical dimension should always be a primary consideration, even if not the immediate focus for clinicians. The ethical dimension helps to link, balance and bring perspective to the other dimensions of a complex clinical decision, and is thus central and essential. Multidimensional Model for Formulating Complex Clinical Decisions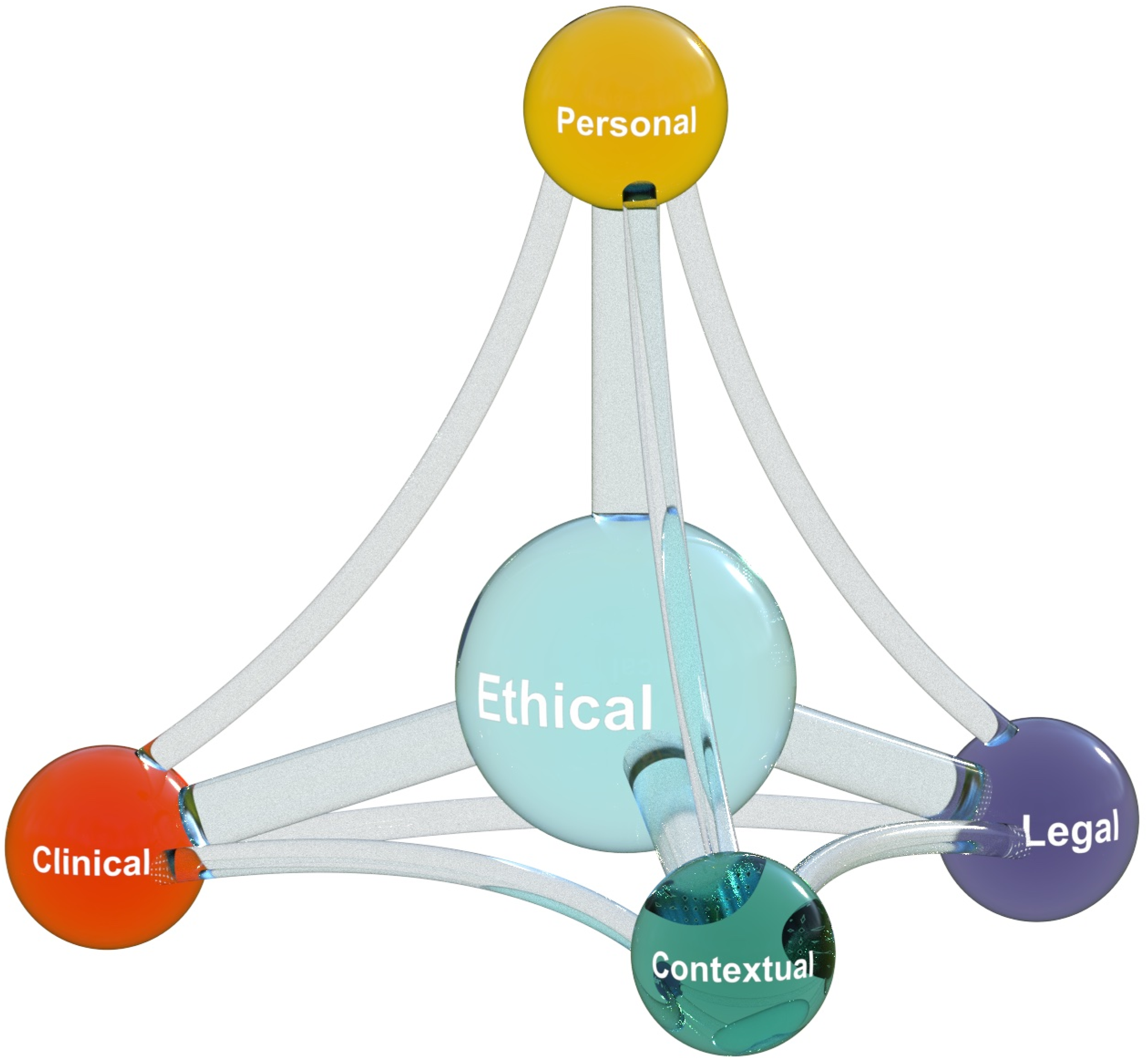
A Multidimensional Model for Formulating Complex Decision-Making
This model is designed as a practical tool for individual clinicians, within peer groups and multidisciplinary teams, and in reflective supervision, as examples. The model does not prioritize the other four dimensions, but it does assume that the ethical dimension is essential to good practice and should be acknowledged when formulating a complex clinical decision. This model emphasizes the interconnectedness of all dimensions and the importance of systematically considering each, with ethics as the linchpin.
Importantly, the clinical, legal, personal and contextual dimensions are rarely sharply distinct from the ethical dimension (or from one another). The clinical imperative to make treatment recommendations based on expert scientific and theoretical understandings of human development and psychopathology only carries weight if we accept that clinicians have an ethical obligation to provide treatments that benefit the patient (i.e., the principle of beneficence). The contextual dimension requires weighing factors within the proximal (e.g., organizational mandates) and distal (e.g., historical/political factors) contexts. The legal imperative to comply with laws only carries weight if we accept that it is generally “right” and “good” to uphold laws that apply equally to all people and reflect the democratically expressed will of the people (i.e., an account of justice). The imperative to provide good care requires self and other awareness implicit in the personal dimension.
We contend that there is practical value in considering these overlapping dimensions and considering them systematically to highlight the moral component of clinical decision-making by articulating a distinct ethical dimension. We use a series of composite cases to illustrate clinical dilemmas and how the model can be useful in clarifying the issues involved.
Case Desciption
Case 1
Darya and her 3-month-old infant Samira are hospitalized in a Mother Baby Unit. Darya is a single mother recovering from a manic relapse, with a background of bipolar disorder and mild intellectual disability. Darya’s mood symptoms have stabilized over 6 weeks of treatment, but she has ongoing difficulties providing safe and consistent care to Samira, who appears distressed when interacting with Darya. The medical team wants to extend the admission to support Darya’s developing parenting skills. The nursing team wants Darya discharged home and Samira discharged to the care of her grandparents.
Clinical Dimension
The treating psychiatrist convenes a care team meeting to discuss this complex dilemma and introduces the multidimensional model for formulating complex decisions. She highlights the difference in clinical opinion between the medical and nursing staff. She notes that based on the usual trajectory for a person with bipolar disorder and intellectual disability, Darya will most rapidly regain her functional capacities and achieve her recovery goal of caring for Samira independently in an inpatient setting, with intensive support from the multidisciplinary team. She then notes that from a nursing perspective, based on close extended observations of Samira’s mental state and her interactions with Darya, Samira is showing signs of significant stress, including progressive withdrawal from social interactions and slowing growth according to her growth chart.
Personal Dimension
The psychiatrist helps the team explore the strong emotions stimulated by this case. The team reflects on the influence of overidentification with Darya and/or Samira, individual differences in the perception of and meaning attributed to Samira’s crying, and difficult recent experiences the team has had where infants were separated from their mothers on the ward.
Legal Dimension
The team reflects together on Darya’s voluntary treatment status and her recent comments about wanting to leave hospital soon to “get on with her life”. The social worker reminds the team that there are legal orders from Child Protective Services in place, which would prevent Samira being discharged from hospital into Darya’s care without taking the matter back to Court.
Contextual Dimension
The nurse unit manager reflects on how Darya’s admission has been very long compared to the usual length of stay on the ward, which is typically focused on stabilising acute mental health symptoms and making referrals to community-based services for ongoing support. There is a lengthy list of new referrals waiting for admission, and there is pressure coming from administration to ensure that the ward is maintaining patient flow.
Ethical Dimension
The psychiatrist leads a team discussion of the ethical tensions underlying this complex decision. The team considers the competing ethical imperatives of respect for Darya’s personal autonomy in relation to her psychiatric treatment, advancing Darya’s interests by supporting her to achieve her self-identified goal of caring for Samira independently, and protecting Samira’s interests by relieving her from the suffering associated with exposure to serious lapses in caregiving attunement. The team use their expert knowledge about infant brain development to bring perspective to the pace of Darya’s recovery and the impact that prolonged stress might have on Samira’s experience and development. By combining an expanded awareness of the influences on clinical decision making and a commitment to centering the ethical dimension of the decision, the team weighed the various factors differently and felt like they could take a more balanced approach to the case.
Case 2
Sam is the mother of a 33-month-old boy and a 9-month-old girl. Sam lives with the children’s father, Max, and cares for the children at home while he works. Max is often stressed and is irritable and sometimes violent with Sam. A parent support home visitor sees bruises on Sam, but she begs the home visitor not to disclose this to police or child welfare services and says Max would “never hurt the children”. She declines a safety plan, has nowhere else to go, and has no intention of leaving Max. She has heard that the domestic violence shelter is “terrible” and does not want her children there.
Clinical Dimension
The home visitor was aware of the impact of young children witnessing domestic violence (e.g., Lundy & Grossman, 2005) and consulted with her supervisor. She noted that she did not really trust Sam’s assertion that Max would not hurt the children. The supervisor helped the home visitor consider what materials to share with Sam that might help her understand the vulnerable situation into which she was placing her children.
Legal Dimension
The supervisor also suggested determining what reporting mandates might be in play, noting the variation in child welfare legislation and reporting standards across different jurisdictions around the world. They learned that the law in their jurisdiction was clear about the requirement to report to Child Protective Services where children have been direct victims of violence, but more ambiguous in situations where children have witnessed violence.
Contextual Dimension
The home visitor was sympathetic to Sam’s description of the available shelter as she had heard troubling stories about it, especially regarding handling the needs of young children. Further, the home visitor knew that the shelter was often full and could not guarantee more than an overnight stay.
Personal Dimension
When asked about her strong emotional response to the situation, the home visitor disclosed that she had experienced violence in a previous relationship and found it frustrating and distressing to hear of Sam’s indecision about leaving. She acknowledged that sometimes she felt impatient with Sam’s uncertainty and critical of her unwillingness to leave.
Ethical Dimension
The supervisor reminded her that both mother and children had needs and risks and suggested an ethical analysis. They agreed that Sam’s autonomy to make decisions regarding her own well-being was important, especially for someone who was experiencing abuse. On the other hand, allowing Sam to remain in a situation of high risk of harm seemed a violation of the principle of non-maleficence. After considering the children’s risk of psychological and physical harm, they concluded that the right thing was for the home visitor to continue advocating for Sam to leave, ever mindful that the home visitor’s previous experience with partner violence elicited unhelpful internal pressure and needed to be managed.
Case 3
Lily, born at 25 weeks weighing 700 grams, is critically ill in the NICU. Ventilator pressures needed to keep her oxygenated are further damaging her underdeveloped lungs. As her course worsens, her parents begin to discuss with the medical team what Lily’s quality of life will be if she survives and are considering comfort care. On the first of the month, a different neonatologist comes on service and begins to manage Lily’s care. He tells the parents that no one knows for sure what her prognosis is and counsels maximum support. On rounds when the parents are not present, he declares, “No one dies on my watch,” and adds that he was himself born prematurely. To sort through the ethical implications of the situation, the palliative care psychologist offered discussion with clinical team members.
Clinical Dimension
Although the clinical details of the case (e.g., the need for invasive procedures, pain, results of examinations, and the infant’s responses to care) contributed to the decision of the parents to consider comfort care, the clinical tension was about the degree to which their voice was heard in decisions about care, and the degree to which the neonatologist’s assessment was biased by his personal experience.
Contextual Dimension
For parents, the NICU is a confusing, frightening, and intimidating setting where infants’ conditions can change quickly and unexpectedly. Parents’ protective urges are usurped by the staff when the infant is critically ill. In addition to navigating the unique culture of the NICU, parents also must deal with practical matters such as jobs, care of other children, finances, recovery from pregnancy, and garnering family and social support. Family-centred care and shared decision-making, considered a NICU standard of care (Craig et al., 2015; Harrison, 1993; Stark et al., 2023; Sullivan & Cummings, 2020), can be complicated due to parental unavailability, disagreements with or lack of cooperation between parents and staff, or lack of support with financial or psychosocial challenges. Until the arrival of the new neonatologist, the staff and family were working together on decisions about the infant’s care. Because of the neonatologist’s uniquely powerful role, parents feared that their wishes might be overlooked.
Legal Dimension
The team identified no immediate legal concerns, such as medical mismanagement, parental caregiving competence or safety, or threats of workplace violence, and recognized that trusting relationships, like that which had developed between the parents and the medical team, can prevent litigation even when mistakes are made.
Personal Dimension
Although the neonatologist acknowledged his experience of being a ‘preemie’, the staff was concerned that his attitude reflected biases that would disrupt the established decision-making processes, risk increased parental stress and undermining trust the family had in the care being delivered, spur conflict and moral distress among the clinical team members, and potentially result in overtreatment of the infant.
Ethical Dimension
In consultation with a palliative care psychologist, the staff agreed that the central ethical question was: Was the neonatologist’s judgement and recommendations so distorted that it interfered with the ability of the parents to provide properly informed consent in relation to Lily’s medical care? The psychologist pointed out that the way physicians describe clinical dilemmas profoundly affect how parents understand their choices. Thus, personal biases and experiences can tilt decisions by parents (Lantos, 2018; Sullivan & Cummings, 2020). The ethical principle of autonomy is the foundation for informed consent, and the team developed a plan to raise their concerns to the neonatologist and facilitate a plan that prioritized family concerns and included team and physician perspectives.
Case 4
When meeting with a mental health consultant, teachers in the infant room of a childcare center described frustration with a mother – Rosa – who insisted on a strict feeding schedule for her infant, Carlo. Rosa’s requirements conflicted with the center’s policy of feeding “on demand.” Staff also felt that Rosa did not bring enough food for Carlo, who always seemed “fussy”, which they believed was due to hunger. They had considered two solutions: (1) discharge the family so staff did not collude with practices counter to policy; or (2) increase the amount and frequency that Carlo was fed without telling Rosa.
Clinical Dimension
The consultant helped staff focus on the dilemma of balancing their beliefs about Carlo’s needs and Rosa’s express wishes about the feeding schedule. They reviewed their history with the mother, considered who had had positive interactions with her and who might be best positioned to discuss with her their concerns about feeding the baby. The consultant suspected that it was already clear to Rosa that the staff did not seem to agree with her feeding approach and were subtly critical of her, which no doubt had made her even more resolute.
Contextual Dimension
In this childcare program, there was a strong belief in observing and responding to babies’ cues, including feeding “on demand”. Thus, the disagreement about feeding was not just about feeding, but about a challenge to a deeply held caregiving philosophy of the center. The consultant was well aware of the values and practices of the staff and appreciated their individualized approaches to caregiving. Nevertheless, she also recognized that the mother – within reason - ought to have the final say over her child’s care. This led her to ask the staff to consider how vital adherence to the center’s policy about feeding was for the classroom’s functioning and whether cultural differences could be tolerated.
Legal Dimension
With the staff, the consultant concluded that there was not sufficient concern about weight gain or health that might trigger a legal remedy to the situation, and there was no violation of childcare regulations.
Personal Dimension
Furthering the discussion, the consultant helped staff articulate and reflect on their intense feelings — worry for the baby and frustration at not being able to provide the care they believed met the baby’s needs. The consultant helped the staff generate strategies for managing their upset.
Ethical Dimension
Finally, the consultant guided the discussion to the desire of the childcare staff to do the right thing for Carlo and for their program, while simultaneously respecting Rosa’s wishes. She framed the central ethical question as, “Do the harms of adopting Rosa’s schedule outweigh the harms of deceiving her?” Together, they discussed what would it mean for Carlo, Rosa, the staff, and the parent-staff relationship to covertly oppose the mother’s wishes. This led them to reflect on how deception would betray the trust Rosa had invested in the staff, and they concluded that they should accept her wishes. At the same time, the director agreed that with support from the consultant, she would attempt to progress a dialogue with Rosa to better understand the origins of her strict feeding schedules and to look for opportunities to develop buy-in for a more flexible approach.
Conclusion
We believe that the field of IECMH needs conceptual tools to support clinicians, who regularly encounter ethically complex scenarios in their work with infants and their families (Zeanah et al., 2023a). This multidimensional model is intended to provide a practical, intuitive and integrative approach to formulating complex clinical decisions that complements the current patchwork of ethical guidance available to IECMH practitioners (Zeanah et al., 2023b). Although this model emerged from IECMH, it could be applied in other mental health contexts, recognizing that the constellation of ethically pertinent issues would change, e.g., end-of-life ethics with older adults; coercion and consent for people with serious mental illnesses; capacity and confidentiality with adolescents.
Accentuating ethics in infant and early childhood clinical practice has implications for the pre-service preparation, ongoing professional development, and supervisory/consultative support of clinicians. Each of these experiences provides an influential opportunity to consider varying perspectives and intervention strategies and to pursue self-awareness in the service of professional integrity. The model described in this article may be fruitfully applied in each of the contexts that shape practitioners or nascent practitioners to establish ethics as a central and robust aspect of their work.
Enhancing the ethical reasoning and decision-making skill of the IECMH field overall is a substantial matter, necessarily involving the many systems and settings that influence the lives of young children and their caregivers. The impact of the model described in this paper will be greatest when it is integrated into environments that work to create and maintain a culture of moral sensitivity and reflection, with regular opportunities to practice ethical formulation with support.
Footnotes
Consent to Participate
The cases described are composite cases created from an amalgamation of clinical material, and not based on any individual case.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.