
Abstract
Youth non-suicidal self-injury (NSSI) and suicidality have increased worldwide, yet funding is limited, and the workforce is stretched. This context of scarcity and risk influences service responses: thresholds for accessing services are raised, with increased gatekeeping. This commentary draws on behavioural and attachment theories to describe how reactive resource allocation can be harmful and inadvertently maintain distress. This occurs through unpredictably providing and then withdrawing access to mental health services. The mental health system itself can be seen as a participant in the therapeutic relationship, providing inconsistent and unpredictable responses to suicidal young people. Trauma- and attachment-related difficulties influence youth perceptions, and small interactions with services can maintain suicidality. When this pattern is recognised, it is possible to alter service responses to emulate interpersonal qualities that provide a sense of safety for those who seek help. For example, predictable responses, clear communication, validation throughout case progression, and consistent adherence to boundaries, all increase trust within the agency-client relationship.
Plain Language Summary
Young people’s mental health is worsening worldwide. There is not enough help available. Self-harm and suicidal behaviours are common. Services have few resources, so make decisions about who can get help based on severity. Cases are closed and re-opened without consistency, and young people feel uncertain about whether they will get help or not. This can lead to young people feeling rejected by the service. Sometimes their suicidal behaviour increases because of this feeling. This is even more common in young people who have experienced trauma in their lives before engaging with the service. This pattern between the service and the young person can be harmful, even though the service is trying to help. Instead, services should try to behave like a consistent and caring parent, to help young people to feel more secure. For example, services can make sure they communicate with the young person in a predictable manner. They can also show the young person they care, by telling them that their feelings are valid and taking their concerns seriously. Services can also make sure they follow their own rules, such as keeping information confidential. When services do these kinds of things, then young people and their families are more likely to trust the service and feel supported. This can lead to young people being safer overall.
Introduction
Context: The Youth Mental Health Crisis
Over the past two decades, there has been a sharp increase in reported psychological distress among youth, and in particular an increase in suicidality and non-suicidal self-injury (NSSI) (Bertuccio et al., 2024; Piao et al., 2022; Young et al., 2025). This mental health crisis has caused consternation among researchers, professionals, and the public, yet no significant improvements or trend reversals have occurred (Bradley, 2023; Fleming et al., 2022; Menzies et al., 2020). Many sociocultural factors contribute to mental health outcomes (e.g. Hashemi et al., 2021; Kisely et al., 2021; Telfar et al., 2023), and there is a simple mismatch between mental health needs among youth and the capacity of available services. However, when youth with severe and complex mental health problems do access mental health services, these can be ineffective and families are left feeling frightened and frustrated (Every-Palmer et al., 2022; Gilmour et al., 2019; Taylor et al., 2018). Youth who are high service-users, and who present with chronic suicidality, are difficult to treat (Burns et al., 2008; McCutcheon et al., 2007; Thabrew et al., 2018).
Previous literature has explored the dynamics surrounding youth NSSI and suicidality with some depth (e.g. Grandclerc et al., 2016; Sadath et al., 2024; Simes et al., 2022). Acheson and Papadima (2023) frame the recent escalation in terms of adolescent identity development and relational need. This is situated within a current ecological context that increases distress, while also reinforcing the expression of the same through diagnostic language and suicidal discourse. Within services, there is a shift away from meaning-making and relational foci towards risk management and the supply of strategies via short-term treatments for discrete disorders. This type of practice risks an escalation pathway towards adult-oriented case conceptualisation, such as personality disorders and the anticipation of long-term relational and emotional instability (Acheson & Papadima, 2023).
A case example allows for an in-depth exploration of youth experiences and behaviour patterns, in a specific system of care. Aotearoa New Zealand (A/NZ) has a nationwide health system that provides community-based and inpatient mental health services to children and adolescents. Although there are some regional variations, Te Whatu Ora (The Ministry of Health) oversees the universal free public service, pathways for accessing this are similar across the whole country. Sutcliffe and colleagues (2024) conducted a cluster analysis of youth self-report data in A/NZ, which yielded results indicating alarming levels of psychological distress. The two most severe clusters comprised 22% of the sample, with the final group of 6.4% having high internalising scores, NSSI, and a reported previous suicide attempt (Sutcliffe et al., 2022, 2024). These data suggest that about one in five A/NZ adolescents needs assessment and psychological support, with about one in twenty needing ongoing monitoring and treatment.
Mental health presentations to hospitals have drastically increased over the past decade (Young et al., 2025), and specialist out- and in-patient services in Aotearoa/NZ do not currently have capacity to meet this need (Haycock, 2023). This leaves ineligible youth relying largely on psychopharmacological treatment through their GP, or private practitioners if they are fortunate. Recommendations for mental health apps or text and crisis numbers for support abound, but these do not provide individualised treatment (Healthify He Puna Waiora, 2024). There is a high prevalence of complex and severe presentations among youth referred to Child and Adolescent Mental Health Services (CAMHS). By the time they are seen in person, youth may already have attempted suicide, and families are very frightened for their safety (NZ Government, 2018).
There is a mismatch between the level of need and the capacity of the available services (Every-Palmer et al., 2022; NZ Government, 2018). This results in inadvertently perverse service responses that increase youth mental distress. This commentary therefore aims to do the following, using A/NZ as a case example: (1) describe how behavioural and attachment theories underpin youth mental health presentations, (2) describe how young people’s interactions with mental health services are influenced by their relational perceptions, and (3) describe key clinical implications.
Behavioural Theory – Its Relevance to Youth Mental Health Presentations
The intermittent schedule of reinforcement is a powerful driver for human behaviour. In a youth mental health setting, intermittent access to treatment can create a higher rate of bids for services. In behavioural terms, this withdrawal of service provision constitutes a negative punishment, or the removal of something desirable. This makes it less likely that the preceding behaviour, the reporting of symptom improvement, will re-occur. This can also be framed as positive reinforcement, whereby the addition of services increases the likelihood that the help-seeking behaviour will re-occur. Mental health practitioners are aware of this, and youth suicidality can sometimes be seen by them and other young people as ‘attention-seeking’ or ‘manipulative’, with service responses escalated only if it is seen as serious and genuine (Crouch & Wright, 2004; Dixon-Ward & Chan, 2022). Sometimes, professionals refuse to treat in an attempt to avoid this dynamic – with the belief that ‘you have to be cruel to be kind’ (MacDonald et al., 2021; Williams, 1998). Phrases are used, such as saying a young person ‘has an intent to die’ to differentiate those who are deemed in need of treatment from those whose suicide attempts are deemed non-serious (and therefore may be safely ignored) (Andover et al., 2012). It is inaccurate to view NSSI and suicide attempts as non-serious – risk assessment is an imprecise science, and NSSI and former suicide attempts are a significant predictor of completed suicide (Grandclerc et al., 2016).
Attachment Theory – Its Relevance to Youth Mental Health Presentations
Attachment develops in infancy, with caregiving responses over time shaping a person’s expectations for comfort and safety. Describing the relationship between a person and those close to them, attachment is observable and can be classified, and has implications for child development (Sroufe et al., 1999). Anxious attachment is characterised by heightened emotional expression, a strong need for closeness, worries about relationships, fear of rejection, and a ‘self-amplifying cycle of distress’ (Pearse et al., 2020). Many youth with severe mental health needs are unable to self-regulate and self-soothe, and can engage in ‘resist-refuse’ or ‘push-pull’ behaviours when professional validation is offered (Swee et al., 2020). Some of these may seem developmentally typical for the adolescent period but are amplified when clients are psychologically distressed. For mental health professionals under stress themselves, this can be confusing and frustrating (Leddie et al., 2022), and sometimes help can be withdrawn as a result.
Typical Service Responses
Services intend to be ‘minimally sufficient’ to avoid unnecessary service provision. Staff also consider whether a client’s referral warrants a service when compared to others’ needs. Intake workers therefore create formal or informal thresholds for access to services, and triaging work involves determining the severity of the client’s presentation (MacDonald et al., 2021). These service thresholds vary considerably, and can depend on service capacity at the time of referral (Barbour et al., 2002).
The following describes a typical treatment pathway in A/NZ (see Figure 1) (Miller & James, 2025). Following referral, professionals undertake risk assessment at an initial appointment, and often the outcome is that the referral is subsequently discharged to their GP. Sometimes a safety plan is made and shared with the young person and their family, and sometimes not. Symptoms may initially reduce, but a re-escalation of distress often occurs, resulting in several re-presentations to CAMHS or emergency departments (Young et al., 2025). Ongoing services may then be provided and the young person and their family may receive further assessment, case management, and perhaps short-term therapy (Thabrew et al., 2018). This often feels like a relief for the young person and their family: professionals are providing help and support. Following an improvement, the case is then discharged again, leading to another cycle of escalation and re-presentation. This is one example, yet the principle is the same – there is a provision and withdrawal of services that rests on the agency’s perception of the young person’s level of risk and need. Hypothetical Adolescent Thoughts and Feelings Alongside CAMHS Case Progression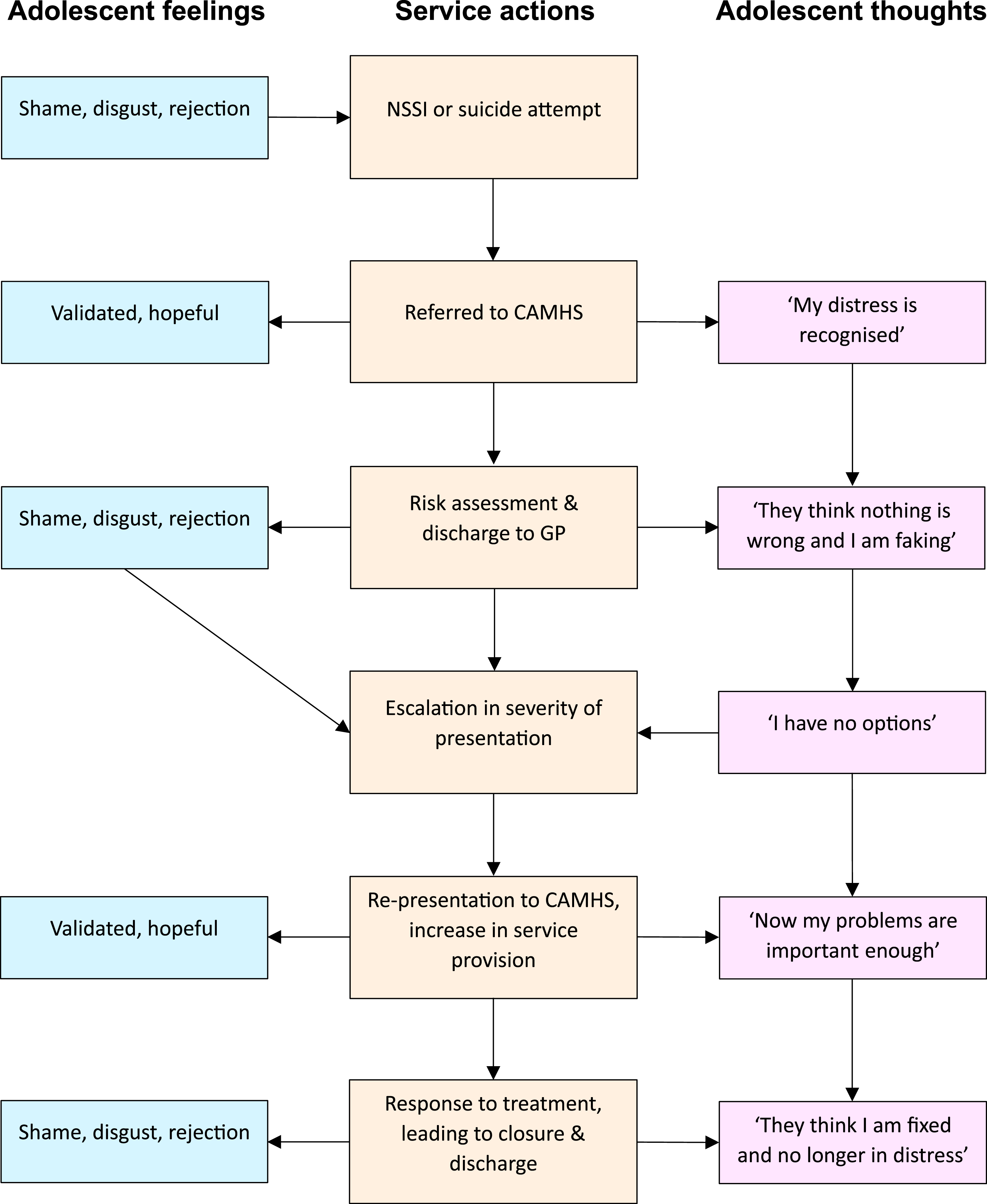
Perceptions of Typical Service Responses
Feelings of shame, self-disgust and rejection often accompany instances of NSSI or suicide attempts (Chu et al., 2017; Sadath et al., 2024; Schienle et al., 2020). Adolescents receiving treatment in A/NZ for suicidality are more likely than other CAMHS clients to have more complex backgrounds and experiences, including sexual abuse, substance use, and a range of family psychosocial stressors (Fortune & Lambie, 2005). Young people feel lonely and do not want to be a burden (Buitron et al., 2016). When receiving a service, recognition by others can lead to feeling validated and hopeful. Health professionals are empathetic and see the situation as important to address, and this is felt as reassuring – although also sometimes frightening and uncomfortable (Marzetti et al., 2023).
Clients’ perceptions of health professionals are shaped by prior experiences of asking for help and their own pre-existing attachment representations. When discharge inevitably occurs, young people may interpret this as professionals thinking that there is nothing wrong, or that they were faking or exaggerating their distress (Dixon-Ward & Chan, 2022). Youth may feel as though they cannot express their distress without suicidality – the ‘emergency siren’ that quickly elicits reassurance. They may feel personally betrayed or rejected, resulting in a deep sense of shame and anger (Sadath et al., 2024). Sometimes, this intense emotion can lead to a further escalation in externalising or internalising problems, which in turn ‘force’ services to provide more help in response to crisis. Throughout this cycle of service response and discharge, there are many micro-interactions that alternate between perceived validation and rejection, serving to create relational uncertainty and increase anxiety in the client (see Figure 1). This type of suicidal cycle in young people is sometimes framed as attention-seeking, or an emerging personality disorder (Moselli et al., 2023). Indeed, some clients can be unpredictable, with relational actions echoing the response of an infant with a disorganised attachment style (Zortea et al., 2021). For example, affect dysregulation occurs along with hostile, dissociative, or avoidant responses (Černis et al., 2019). Health professionals can feel confused and frustrated when offered help is rejected or ignored, leading to their own frustration – which is also sometimes expressed towards the young person (Gvion et al., 2021).
Young people are aware that when assessing referrals, professionals ask about suicidality to determine whether they should be helped. Marzetti and colleagues (2023) explored A/NZ youth experiences of suicidality, finding that some participants felt it was necessary to disclose suicidality and NSSI in order to get help. Participant Yasmin said, I had to be like I’m going to kill myself if you don’t refer me [for mental health support]. Like I had to say that to her [Yasmin’s GP] more than once…because she had already been dismissive, but I felt this is the only way… (p. 509, Marzetti et al., 2023). Another study of A/NZ young people who used crisis helplines captured the uncertainty while trying to access help in the midst of distress. One participant expressed this, saying Uhm, it varies all the time and it’s quite hard to experience that because you’re in distress and you don’t know if you’re going to get a response or yeah, just you don’t know if you’re going to get a response (Stace, 2024, p. 87). Media stories on the youth mental health crisis in A/NZ have also highlighted the perception from young people that they need to attempt suicide, or at least be in crisis, in order to be listened to (e.g. Bradley, 2023; Cooke, 2021).
A meta-ethnography of qualitative studies, examining youth experiences of mental health services, summarised the findings of four studies (Gilmour et al., 2019). These highlighted the difficulty in finding and then accessing mental health services, feelings of shame and lack of trust in professionals, and the importance of face-to-face engagement, connection, and honest communication. Primarily, suicidal young people wanted to be heard, but were alert to perceived slights: I had very high standards for people. . .if they looked down on me or said something that made me mad, just something a bit off beat, it would completely ruin it. I’d want to leave… (Murray & Wright, 2006, p. 161). There can be an interpersonal function when seeking help for suicidality, that includes the need to communicate to others the extremity of their felt distress (Steggals et al., 2020). Some health professionals recognise this cycle of distress and understand that it is largely outside a young person’s conscious control. Yet when discharge is done well following effective treatment, a sense of invalidation is less likely. This is because the decision has been reached through collaborative decision-making and a shared understanding of the young person’s progress via measurement-based care. This latter approach requires considerable skill, but in turn amplifies clients’ agency, rather than undermining it (Acheson & Papadima, 2023).
Mental health services themselves thus become a participant within the therapeutic relationship. Some formulation models explicitly describe patterns between families and agencies (e.g. Connor & Fisher, 1997), but services themselves do not evaluate their own effectiveness with these in mind. If the agency was a parent, they would be alternating warm responsiveness with dismissive behaviour, eliciting feelings of anxiety and uncertainty for those on the receiving end (Jones et al., 2015; Marzetti et al., 2023). For young people who struggle to take others’ perspectives and to self-regulate, the uncertainty and perceived invalidation elicit attachment-related distress.
Services are operating within a pressured system, and prioritise based on the highest perceived need (Haycock, 2023). Yet families are seeking to ‘create a trusting and respectful relationship between a child or young person, their family, and a therapeutic team’ (NZ Government, 2018, p. 49). The analogy of the parent-child relationship reveals some simple approaches that are within the control of the service, which relate to increasing security and trust within relationships. These include predictability, emotional availability, sensitivity and attunement, consistent boundaries, and consistency across settings (Morris et al., 2017).
Key Implications and Recommendations for Clinical Practice
Despite the strains on the mental health system, practice changes can be implemented within systems and by individual practitioners that may alter the patterns and experiences described in previous sections. Some general guidelines and recommendations are outlined below, intended to aid professionals who want to avoid this interactional process. These may also help inform health system managers in reviewing and improving system effectiveness. Key themes include increasing agency predictability, providing sensitive and flexible care, having clear boundaries, and improving the consistency of practice across different parts of the system.
Improve service predictability wherever possible, by communicating in a manner that is easily understood and checking for this understanding before moving on (Taylor et al., 2018). Slowing down and allowing time to digest information aids comprehension. When in crisis, it can be hard to remember what a professional has said, so written outcomes are valuable, or even allowing families to voice-record summaries and next steps on their phones so they can listen again later. Young people and families often say they have understood something, or agree to a plan out of a desire to please professionals (Coyne et al., 2015). In A/NZ this is particularly true for Māori, Pacific people, people whose English is a second language, or who come from cultures where health professionals hold high status (NZ Government, 2018). Even though this takes a little more time, it can increase families’ confidence in their own understanding, reducing the likelihood of unnecessary re-presentations.
Cultivate awareness that young people may interpret discharge as a personal rejection or an invalidation of their distress (Taylor et al., 2018; Wasson Simpson et al., 2022). Directly address this during discussions with the young person and their family and acknowledge that case closure does not mean that all problems are resolved. Minimising the remaining issues, in an attempt to justify the decision, can feel dismissive (Idenfors et al., 2015). Allow young people to express their feelings in response to discharge. Feelings of rejection may be prevented, especially when this follows ongoing discussions with the young person regarding their progress in treatment. It also provides the opportunity for a more detailed intervention and management plan to be created collaboratively, increasing youth safety (Simes et al., 2022). Reminding young people that a re-referral to mental health services is an option can reduce the feeling of rejection – and they should receive specific written information on how to do this (Idenfors et al., 2015). This supports youth autonomy and provides the sense of the service as a ‘safe haven and secure base’, encouraging a type of attachment between the client and the service (Pitama et al., 2007).
Undertake risk assessment and other high-stakes engagements sensitively, considering the young person’s emotional state at the time and their perceptions of your motivation. Repeated screening for suicidality does not increase risk (Hom et al., 2018), but it can send the message that rapport-building only occurs with the goal of gaining an accurate risk assessment (Taylor et al., 2018). Do not finish the engagement immediately following the direct questioning, instead use opening and closing processes in a balanced manner (Lacey et al., 2011). Sensitivity can be manifested through noticing individual young people’s characteristics, remembering these, and giving genuine attention with curiosity and humour (McCutcheon et al., 2007). Give extra time to the engagement where possible, without an agenda of completing processes. In A/NZ, young people see a relaxed professional connection, and sharing of backgrounds, as particularly important (Stubbing & Gibson, 2022).
Consistent boundaries are recommended for practitioners and services, as well as with young people accessing the service (Taylor et al., 2018). These are challenging within a healthcare setting, often due to factors outside practitioners’ control. This would look like services adhering to stated timeframes, and being clear about reasons and alternative options when referrals are denied (NZ Government, 2018; Taylor et al., 2018). Confidentiality must be upheld when promised, even from other professionals within the service. At the same time, when information needs to be shared this should be done promptly and following correct processes. Practitioners working with a new young person should read any previous plans or reports, and contact other services when requested to do so (O'Reilly et al., 2013). In A/NZ, ensuring the GP receives instructions on aftercare, cc’d to the young person themselves, would demonstrate this consistency of care. These types of actions can prevent family frustration with contradictory professional advice, and having to share personal information repeatedly – and can increase trust (Gilmour et al., 2019; McCutcheon et al., 2007; Taylor et al., 2018).
Conclusion
Systemic responses to youth suicidality can be lifesaving, but they can also inadvertently increase distress and therefore risk for further harm. Behavioural and attachment-related factors can inadvertently combine to drive suicidality, even while services are being provided. Given this pattern, CAMHS services and mental health practitioners should address these directly, alongside implementing principles of effective practice that have been well covered in other literature (e.g. Eapen et al., 2022; McGorry et al., 2018; Stubbing & Gibson, 2021). In implementing these, conceptualising the service-young person relationship as analogous to the parent-child relationship will lead to more compassionate and effective treatment. Ultimately, services must critically examine their own response patterns, and change these, to improve safety for youth with chronic suicidality.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.