
Abstract
Plain language summary
This study explored children’s experiences of Dyadic Developmental Psychotherapy (DDP). DDP is a therapeutic model and parenting approach, grounded in what we know about attachment and early relational trauma to support children and families in their relationships together. It is widely used in England to support children from the care system in adoption, special guardianship, foster care, and residential settings. Six children who were accessing DDP interventions and were adopted or under special guardianship orders participated in the study. Study methodology was designed to put children at ease and address power imbalances. Techniques using play, storytelling and non-verbal communication, were employed to help children make sense of attachment relationships in the therapy space. These methods aimed to empower participants to express meaningful thoughts without fear of being wrong or judged. Research sessions were video recorded and transcribed for analysis using an in-depth qualitative approach to identify emerging themes. Themes closely aligned with the aims of DDP. Participants referenced sensitive attuned, interactions with both therapists and caregivers. Several children described the experience of feeling deeply understood. Because caregivers are active participants in DDP sessions, the experience of these interactions had the potential to foster an increased sense of closeness and trust. Children initially expressed scepticism or discomfort with this way of interacting. Trust took time to develop, was often fragile and easily ruptured. Therapist’s played an important role in repairing relational ruptures, helping rebuild trust and reinforce the child’s sense of relational safety. Findings provide rich insights into how DDP may facilitate therapeutic change and positively impact children’s experiences of themselves and their relationships with caregivers.
Keywords
Introduction
DDP is a caregiver-child psychotherapy which seeks to address some of the common mechanisms related both to attachment insecurity and developmental trauma (Hughes, 2007). It is commonly used in the UK to support children in the care system who have typically found permanence through adoption and special guardianship (Burch et al., 2022). These children often have histories of abuse or neglect (Selwyn et al., 2015). Their developmental outcomes can vary widely due to the complex interaction of biological, psychological, and social factors (Rutter et al., 2006; Smith & Pollak, 2021).
Developmental Trauma is a commonly used term to describe the psychological difficulties that may arise from early adverse relational experiences. These difficulties could be understood as once functional adaptations to hostile environments (Perry et al., 1995; Wadsworth, 2015). When children are placed in safer environments, their over-sensitive threat response systems may persist, making it harder to engage and trust in caregiving relationships (McCrory et al., 2010).
Informed by theories and research on developmental trauma, attachment, intersubjectivity and interpersonal neurobiology, DDP seeks to increase relational safety through applying principles of playfulness, acceptance, curiosity and empathy, with the aim of supporting and integrating emotional regulation, cognitive development, and autobiographical narratives. The components of DDP are described in detail in ‘Healing Relational Trauma Workbook: Dyadic Developmental Psychotherapy in Practice’ (Hughes & Golding, 2024).
In the first phase of treatment the therapist works with the caregivers to build a therapeutic alliance and invite them to incorporate ideas from the DDP model into their parenting approach. This alone may create shifts in understanding and promote increased connection with their child. Joint sessions with the child may be indicated once the caregiver-therapist alliance is established.
While DDP is grounded in sound theoretical underpinnings and therapists undergo significant training, efficacy and effectiveness for improving children’s attachment and trauma related difficulties, it has not been robustly tested through an RCT. DDP can therefore, at best be referred to as a promising intervention. A study by Becker-Weidman (2008) yielded positive results with significant improvement on measures for children in the DDP group at the one-year and four year mark, with scores for the control group deteriorating. However, the study lacked rigour, reducing validity of the data and confidence that the findings can be reliably attributed to the model.
Burch et al. (2023) undertook a longitudinal study of survey data from 150 adoptive parents who had accessed DDP . They found an association between the provision of DDP and improvements in children’s emotional difficulties and conduct problems, with similar improvements on the carer wellbeing scale. Results were maintained at 6 months. Without a control group, statistical associations cannot reliably be attributed to DDP, further emphasising the need for an RCT. In a qualitative study of DDP by Wingfield and Gurney-Smith (2019), caregivers reported increased understandings of their children and valued new methods of caregiving with increased acceptance. All but one of the 12 caregivers felt the intervention had been beneficial to their relationship with their child.
To the knowledge of the author there have been no academic explorations eliciting children’s views or experiences of DDP. More broadly, research into psychotherapeutic approaches which includes the experiences of children with traumatic histories (Capella et al., 2018; Jessiman et al., 2017; Midgley et al., 2018) suggests that supportive and non-judgemental relationships with therapists and caregivers were elements that fostered positive change.
This study offered the opportunity to explore children’s experiences of DDP, with a focus on what children view as the key components and perceived differences in their sense of attachment to their caregiver that may have come about through the therapeutic process, as the goal of DDP.
Methods
Research design
Semi-structured, play-based interviews with 6 children from separate families were analysed using Interpretative Phenomenological Analysis (IPA). IPA has been used exploring DDP experience with adoptive parents (Hewitt et al., 2018; Wingfield & Gurney-Smith, 2019).
Participants
The following participant inclusion criteria were used to increase homogeneity within the sample (Smith et al., 2021): • Aged 6-14. • Adopted or with a Special Guardianship Order. • Actively participating in a DDP intervention. • Completed at least 4 DDP caregiver-child sessions. • Had capacity to provide assent and engage in the research protocol without risk of distress.
Children who access DDP are usually between 8 and 18 years old (Purrington et al., 2023). In line with current research in DDP 1 this study focussed on pre-adolescent children. Pre-adolescence is usually defined as the ages of 6–12 (Bhana, 2010). To account for individual developmental differences and to expand the potential pool of participants, we extended the range from ages 6-14. There is no recommended number of sessions, however 20 is considered typical (Turner-Halliday et al., 2014). Children were excluded if they were within 2 sessions of a planned ending to avoid confusion in the data regarding endings.
Participant characteristics
• 6 participants aged between 8 and 12 years old. • 5 females, 1 male. • All white European, (broadly representative of the UK adopted population
2
). • 5 adopted children, 1 on Special Guardianship Order (SGO). • Referred from three accredited, experienced DDP therapists from various backgrounds (clinical psychology, child psychotherapy, and clinical social work). • Attended between 4 and 60 sessions of DDP with a mean of 36.7 sessions. This figure did not include the initial caregiver focussed phase of DDP, and it is anticipated children will have experienced DDP informed parenting prior to them commencing the caregiver-child phase. Adopted and SGO children may experience more complex difficulties in comparison to their non-care experienced counterparts, leading to a need for ongoing or recurring treatments (Tarren-Sweeney, 2010). This may justify the wide range in the number of sessions accessed.
Trauma histories were not explored to protect participant privacy, however therapists confirmed typical presentations for DDP referrals as children with attachment related difficulties presenting with signs of mistrust, fear of closeness in relationships, high levels of shame, and associated internalised and externalised behaviours (assessed through psychological interview, standardised measures and observations), with both children and caregivers needing emotional support.
Methods of data collection
Narrative story stem methodologies (NSSM) were chosen as a way of supporting children to share their experiences without asking them directly, which could culminate in inhibition and anxiety (Woolgar, 1999). Such research tools begin with a story stem, or cue and the participant is asked to continue the story verbally and through figurine enactments. Adapted from Hodges et al.’s (2000) Story Stem Assessment Profile (SSAP), four stems were developed which presented typical therapy scenarios or dilemmas. SSAP has been meaningfully used in research with adopted children to assess attachment representations (Hillman et al., 2020). The stems did not ask children directly about their experiences and instead allowed children to make representations in a displaced form by using a doll configuration similar to the SSAP.
To support children in answering direct questions and inspired by Pimlott-Wilson’s (2012) paper on visual research methods, an outline of a house was presented on a large piece of paper where children could draw or write about their experience. To support communication and in recognition that drawing and writing can be anxiety provoking for some children (Pimlott-Wilson, 2012; Young & Barrett, 2001), emotion stickers and feelings cards were on hand, reducing the pressure to talk (Fane et al., 2018).
For further detail on data collection and production methods, see Supplemental Materials and Christopher (2024).
Procedure
Recruitment
Accredited DDP therapists in the UK promoted the study to families where children met the inclusion criteria. The full protocol was shared with caregivers supporting informed decisions about their child’s involvement. Caregivers were offered a video call prior to consent to answer any questions. Children’s assent was sought through sharing of written child-friendly information and the opportunity of a video call with the researcher. Child assent was checked at the beginning of the research session and throughout.
Data collection
Research sessions were face-to-face with the intention of being more conversational than interrogatory. Interviews started with informal interactive games of the child’s choosing e.g. Dobble, Marble Run etc, to build rapport and reduce anxiety, followed by the story stems and picture tasks. Sessions ranged from 35 minutes–2.48 hours (mean 1.15) . The differences in the range related to the need for some children to break to play games between research activities to support emotional regulation.
Emotional regulation of the participants was prioritised and participants were offered the option for caregivers to stay which was accepted by four participants. Literature suggests the influence of parent’s supporting their children in research is complex. In some instances, it may hinder children from expressing their views, however it has also been found to support children sharing their views in research, leading to the collection of rich data (Gardner & Randall, 2012; Hillier & Aurini, 2018). Caregiver’s who supported their children were requested not to actively influence their children’s responses.
Data processing
With informed consent from the child and caregiver, the research session was video recorded to allow the researcher to attend to the child during the interview and accurately analyse the data. Data was transcribed verbatim. Observed non-verbal enactments, communication, and drawings were described in the transcript and included in the analysis.
Data analysis
Analysis was guided by Smith et al.’s (2021) framework and informed by Nizza et al.’s (2021) four quality indicators for IPA studies. Analysis was an iterative and inductive cycle beginning with familiarisation with the data, line by line coding, identification of patterns emphasising convergence and divergence, commonality, and nuance for each case, and then subsequently across all the cases.
Reflexivity
Reflexivity was integral at all stages, based on the assumption that we are all influenced by our biases (Yardley, 2000). This was practised through supervision, bracketing and reflexive exercises.
Quality and credibility
Drawing on Yardley’s (2000) framework for ensuring transparency in qualitative research, the research team triangulated and audited the data using multiple methods: • Two methods of data collection (story stems and picture task). • Therapist focus group, exploring their perception of children’s experiences (with therapists of participants excluded for confidentiality). Data was analysed using template analysis to identify converging and diverging themes from core data and used to refine themes. • Caregiver questionnaire exploring caregiver perceptions of their children’s experiences in therapy.
Triangulation supported corroboration and debate through multi-layered data, providing cogency and enhancing credibility. The focus group and caregiver data were used solely to support the core data without separate analysis to maintain IPA’s idiographic focus on the phenomena.
Ethical considerations
Ethical approval was sought from the University of Hertfordshire’s Health, Science, Engineering and Technology Department (protocol number: LMS/PGT/UH/05305). Participants and their caregivers were informed that participation was voluntary and their care would not be impacted by their decision to take part. Information was provided verbally and in writing prior to consent. Written consent was obtained from a caregiver with parental responsibility and child assent was obtained verbally prior to participation. It was made clear that consent and assent could be withdrawn at any time.
Steps were taken to protect children and families from risks of harm including opportunities to debrief, and support after the interview from their DDP therapists. A protocol for managing distress was developed and shared with therapists and caregivers. Given the potential histories of harm and abuse, participants were encouraged to only share what was comfortable and were gently guided to remain on the topic of their experience of their therapy.
Results
Overview of themes
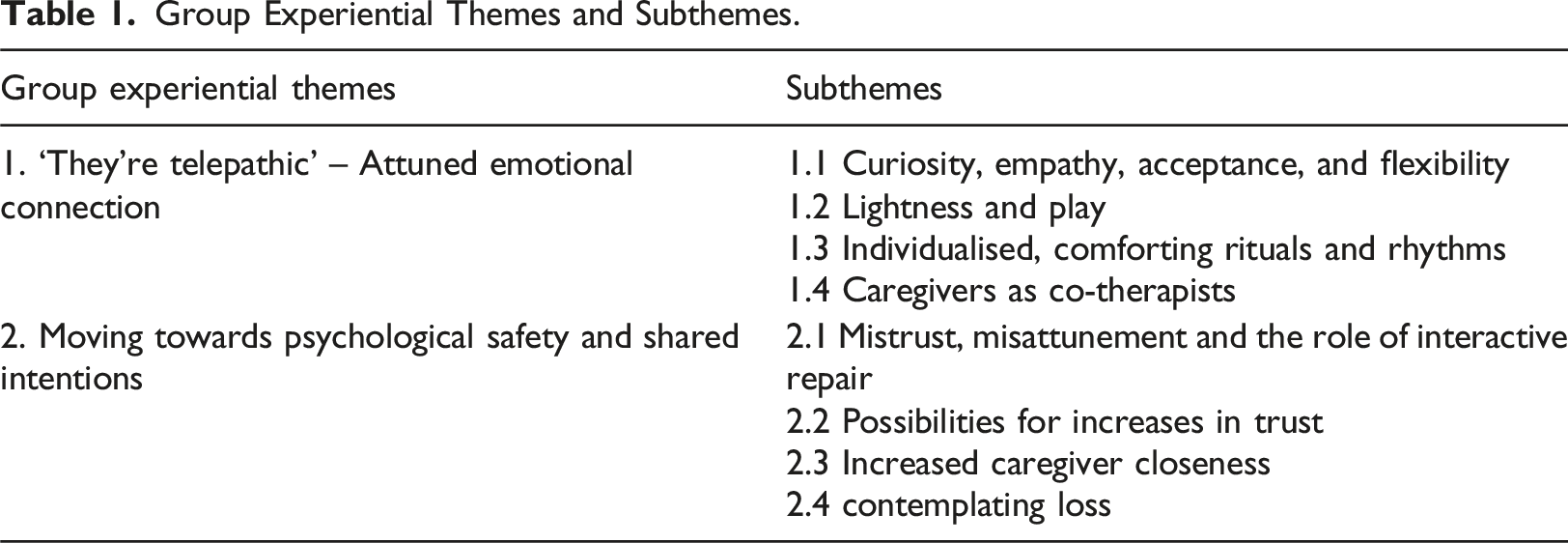
Group Experiential Themes and Subthemes.
Identification of Recurrent Themes.
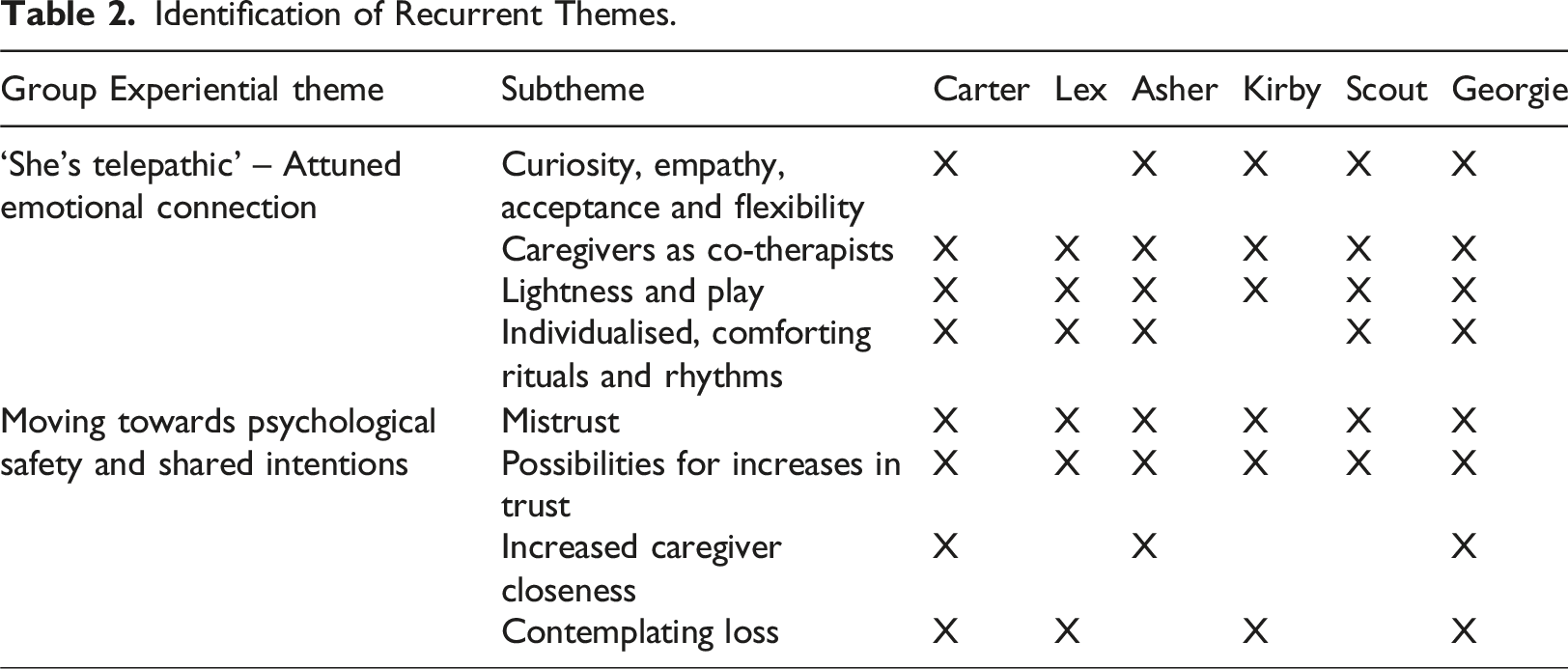
N.B. Gender neutral pseudonyms and ‘they/them’ pronouns have been used to protect confidentiality and promote inclusivity. Quotes included are from children who were able to verbally express their experiences, other children may have provided data for themes through non-verbal expressions, character depictions, or through their pictures. Where it was not clear if a child was referring to the caregiver or therapist in the data, we have used the term ‘adult’ in the descriptions.
Theme 1: Emotional attunement: “They’re telepathic”
This first theme captures the depicted qualities of interactions between therapists, caregivers, and children, with subthemes describing these qualities in more depth. Asher described this experience as like their therapist was ‘telepathic’.
Subtheme 1.1: Curiosity, empathy, acceptance, and flexibility
In five of the six accounts, therapists were portrayed as warm, curious, empathetic, accepting, compassionate, playful, flexible and understanding. In story stems where children experienced discomfort (e.g. ‘crying outside) there were themes of therapists frequently exploring this with curiosity and empathy rather than problem solving or reassuring. Interactions felt non-evaluative (acceptance).
Participants frequently depicted therapist’s flexibility as they shifted cyclically between lightness and depth with the adults moving at a pace the child could tolerate. Asher described how the child in their stories did not wish to talk about feelings, and the therapist flexibly shifted into a more playful and regulating stance to re-establish safety. they’d {child} say ‘I don’t really feel comfortable sharing this’. And then the adults would maybe do something different and make them{child} comfortable. (Asher)
When the character in one of Kirby’s stories was anxious, the therapist used a rhythmic tone of voice, conveying flexibility and communicating that the child character was not trapped into exploring their trauma in that moment, giving the choice to end the session early (acceptance/empathy). The therapist communicated that the child character was welcome back the following week conveying an open and engaged attitude, without evaluation. They {therapist} said, ‘Would you like to go home or stay here until the time?’ and {the child} said ‘I wanna go home’ and {the therapist} said ‘ That’s fine and it was nice to see you. See you next Friday’ (Kirby)
Subtheme 1.2: Lightness and play
Lightness (interactions that were light-hearted and not problem saturated) and play created the relational conditions to support emotional regulation, providing the opportunity for children to engage in therapeutic dialogue. Scout for instance had developed the expectation that the adults would use play in an emotionally connecting way to help them feel less anxious. They {therapist/caregivers) just like instead of carrying on talking about stuff {the child} doesn’t feel comfortable talking about, they like helped them relax…. They played with {the child}, instead of just carrying on. (Scout)
Asher had a similar expectation. In their stories the connected playfulness appeared to enable the child character to feel safe enough to tolerate exploratory conversations. They {the adults} play a game with them [….] Maybe it would make them more comfortable sharing. (Asher)
This seemed a key element of the therapy experience as the therapist conveyed interest not just in difficulties or trauma history, but also in everyday experiences. Playfulness and lightness were relational. It gave opportunities for adults to delight in and celebrate children, discovering strengths and bracketing more in-depth conversations to make them more tolerable.
Subtheme 1.3: Individualised comforting rituals and rhythms
Themes in children’s stories suggested sessions were regularly punctuated with familiar, non-verbal comforting rituals and rhythms, such as games, drinks, and snacks. These synchronised rituals seemed significant in building trust and safety and were highly individualised to each child.
The child character in Georgie’s story stems (example below) was partial to a game of Uno, suggesting this was a familiar ritual in Georgie’s own therapy experiences. Georgie appeared to know that the adults were allowing them to win each time, but they nonetheless seemed to enjoy the experience of winning and being celebrated by the adults. This ritual seemed to provide a regular and predictable message from the adults that Georgie was worth celebrating in a way that Georgie could tolerate. {child} ‘can we play a game? Maybe Uno flip as you know that is my favourite game of all entire time and I always win, nobody else can ever beat me.’ {Therapist} ‘yes of course. I have never done it before’ {therapist} said having a cheeky smile on their face. {Child} ‘Of course you have, I’ve seen you play it 100 times, but you always let… you always loose. (Georgie)
For Asher, it was the drinks and snacks which they looked forward to the most in their sessions and suggested that without these, they felt hungry and irritable. This element appeared important to Asher for their emotional regulation and although we do not know Asher’s history, this element may be especially relevant for children who have experienced previous neglect that includes unpredictable or inadequate experiences of being fed. Researcher: Why do you think it's important that you have snacks and drinks? Asher: To feel relaxed and not feel hungry. [Asher was looking through the feelings cards. Asher picked up the irritated and hungry feelings cards and showed them to the researcher]. (Asher)
Subtheme 1.4: Caregivers as co-therapists
Participant’s story stems illustrated caregivers playing active roles in therapy sessions. They were frequently portrayed as emotionally attuned and nurturing, and in some stories there were examples where this was first modelled by the therapist. Asher was able to articulate how having their caregiver present enabled shared narratives, providing caregivers with a greater understanding of their needs. Happy that they are there so you don’t have to explain it all to them again at the end… Yeah. And they have more understanding of why you get upset or grumpy. (Asher)
Theme 2: Moving towards psychological safety and shared intentions
The data suggested participants experienced hesitation and mistrust in the process, especially during their early sessions, and establishing a sense of trust with the therapist took time. It was unclear from the data when these shifts in trust took place; however, there were marked individual differences in this journey, unrelated to length of time in therapy.
Subtheme 2.1: Mistrust, misattunement and the role of interactive repair
For some children, exploration can feel exposing, and children learn to defend strongly against this vulnerability. Some children appeared to anticipate rejection, whereas Kirby appeared to feel unsafe. I drew a scared face. Good and scared the first time, so I drew a scared face. They {therapist} don’t know you. And they don’t know me and you don’t know who they are and you don’t know what they’ll do. (Kirby)
Relationships in therapy had the potential to remain fragile. On the few occasions when therapists or parents were not attuned (some story stems set this dynamic up), children quickly felt angry, alone and confused. It was now the second time they’d {child} been here and they’d got very used to it. {therapist} and {the child} were already friends, but then they had been from the start, but now they seemed like enemies now, as they were talking about something that {the child} didn’t want to talk about. They were trying to get {the child’s} attention, but it wasn’t really working. (Georgie)
For the most part, these relational ruptures were quickly repaired by therapists. Kirby for example depicted the child character’s emotional dysregulation as the adults (therapist/caregivers) attempted to direct the conversation to talk about feelings. Rather than continue, the therapist supported repair through curiosity as to whether the child was tired and needed a break. The child and the caregivers walked out of the session all holding hands, suggesting relational repair, which was facilitated by the therapist. This suggests safety could be fragile and the child quickly moved into a defensive stance, with the therapist in the story re-establishing safety and emotional connection (repair), whilst being aware of the child’s tolerance levels.
Subtheme 2.2: Possibilities for increases in trust
The story stems were designed to elicit changes in the participant’s journey through therapy with a story stem set in a first session and another in a later session (see Supplemental Materials). Responses suggested there were changes for all participants, albeit in different ways, as they moved from initial mistrust into increasing trust ‘it gets easier, and it is a good thing to do’ (Asher)
Asher described how therapy initially felt ‘unusual’ and ‘awkward’, possibly it was a different way of interacting and being with their caregiver. As therapy progressed, having conversations with caregivers and therapists felt easier: You do end up not feeling anxious, not feeling worried and you do feel happy and you do feel kinda like at more at ease talking about stuff instead of going home thinking ‘ I shouldn’t have said that’. Cos now I can just say all kinds of things that I couldn’t. Asher (picture task)
Subtheme 2.3: Increased caregiver closeness
Asher was able to articulate how relational changes extended into homelife with signs of increased closeness and understanding, leading to greater attachment security. Yeah. And they have more understanding of why you get upset or grumpy[….] And they are better tempered now[….]And we are playing games quite a lot. It’s made a big impact. (Asher)
Carter was able to notice some relational changes with their caregivers and described how this was first modelled by the therapist. They suggested that their caregivers were more emotionally regulated, leading to increased closeness and a reduction in moments of disconnection. They’re calmer. But {therapist} is always calm[…] Less arguments I guess […] and lots and lots and lots and lots of fun! And new games. (Carter)
Subtheme 2.4: Contemplating loss
It makes sense that contemplating the end of the therapy could bring up feelings of loss as therapy progresses, especially once safety has been established. Children who had been attending sessions for some time possibly anticipated this future loss. Four participants indirectly referred to loss in their accounts.
Although not a clear example of an anticipated ending, in one of Carter’s stories, someone new answered the therapy room door instead of the usual therapist. The child character appeared confused and although they initially seemed to accept the therapist’s explanation, the session ended abruptly when the child got their foot stuck in a cup. This could be a projection of underlying worries about change, or endings. …and {caregiver} said, “what’s wrong?”. She said “it was the wrong person who answered the door” “Oh dear!” and {therapist} said “that was my friend”… {therapist} said, ‘Oh that was my friend who’s come over for the week to stay on holiday she must have answered the door by accident.’ And then {child} got up and danced and slipped on the cup and got her foot stuck in it and then sadly they had to go home to take it off. (Carter)
Discussion
In keeping with the double hermeneutic element of IPA and the aim of the study, the results were interpreted with a focus on what children viewed as the key components of their experience and perceived differences in their sense of attachment to their caregiver that may have come about through the therapeutic process, as the goal of DDP. Results inferred that participant’s experienced a dynamic journey through therapy where the qualities of the interactions (with therapist, and caregiver as the co-therapist) were salient and potentially influenced increased caregiver closeness and connection. An increase in trust and enriched depth within relationships may engender feelings of vulnerability. A cycle of interactive repair between therapist (and caregiver) and child seemed important to maintain the process of developing trust. At times, therapy was challenging, nonetheless most participants were able to express benefits of the therapy, with some depictions of increased connection and closeness with caregivers. An illustration of this non-linear process and the key components involved in developing trust in DDP (from the participant's perspectives) can be seen in Figure 1. Below, the key components and perceived differences in participant’s sense of attachment to their caregiver, as derived from themes in the findings, are considered in relation to theory and research. Limitations are considered and implications for practice and research are discussed. The dynamic experience of DDP intervention through the Lens of the child.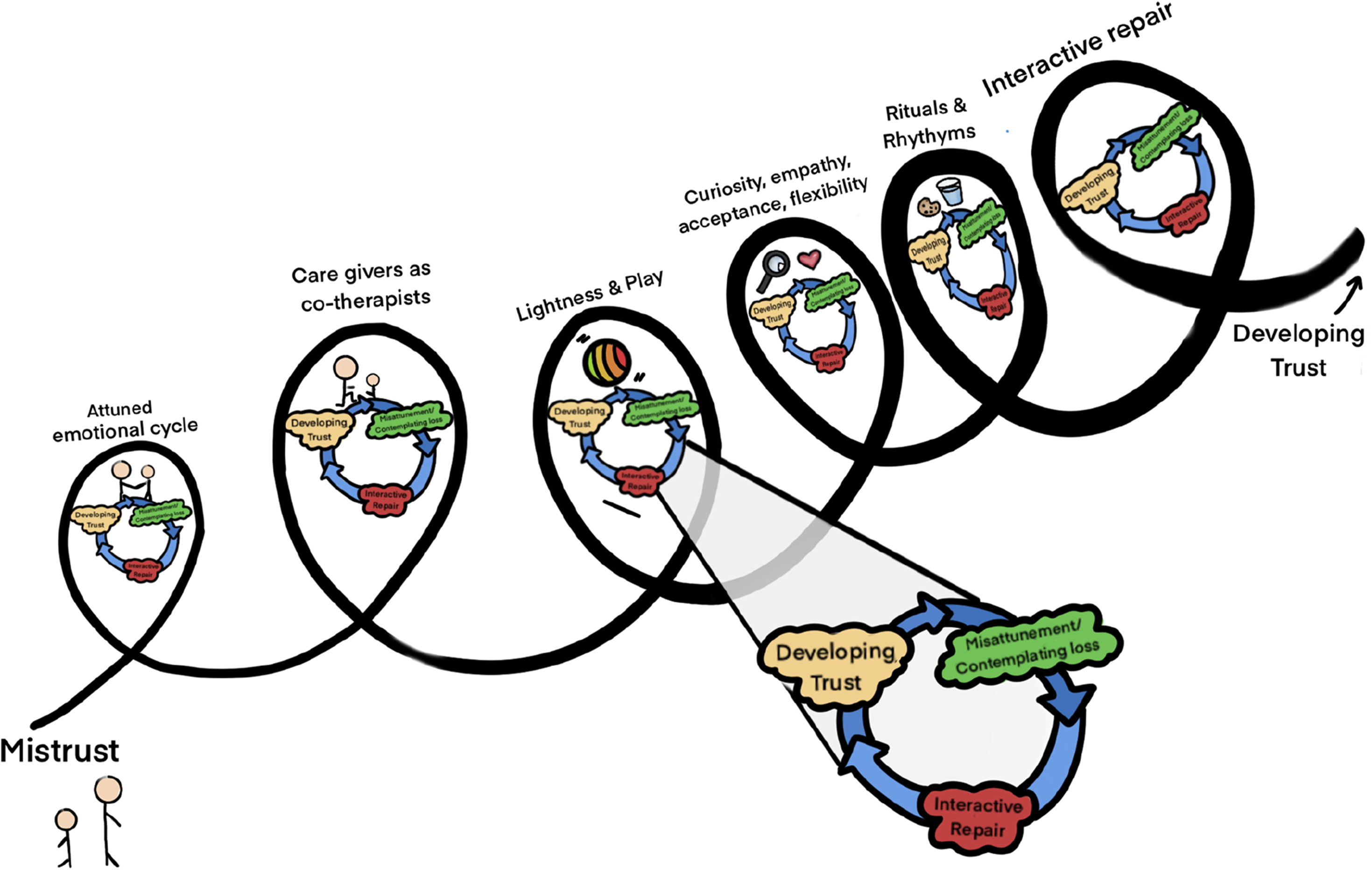
What did children see as the key components of DDP and how did they experience them?
Key component one: Emotional attunement
As described in Theme 1, participants depicted experiences of sensitive verbal and non-verbal interactions that made them feel deeply understood, reflecting emotional attunement. These individualised, interactions were conceptualised from participant data as a key component in the DDP experience, highlighting how children perceived and valued attuned interactions with therapists and caregivers during therapy.
Attunement is a relational concept referring to the ability to recognise, understand and sensitively respond to another’s emotional needs (Fonagy et al., 1991; Ostlund et al., 2017; Stern et al., 1985). Attunement has been highlighted as an important mechanism for change within the DDP research (Hewitt et al., 2018; Turner-Halliday et al., 2014; Wingfield & Gurney-Smith, 2019), and child psychotherapy more generally (Capella et al., 2018; Jessiman et al., 2017; Midgley et al., 2018).
Key component Two: Attuned curious exploration and mentalisation
In Theme 1.2, participants depicted therapist’s curious, exploratory, interpretative interactions which seemed to suggest the therapist was mentalising for the child. Mentalisation describes the internal process of understanding oneself and others. Bateman (2022) suggests, mentalising experiences in therapy have the potential to bring about arousal patterns that replicate secure attachment relationships. Change processes in therapy may occur when therapists make small, in-the-moment interpretations that connect to subjective reality (Fonagy & Bateman, 2006). The salience and recurrence of examples of these interactions in the data implied this was experienced as a key component of the therapeutic experience.
Therapists light and non-judgemental curiosity of the therapists appeared to be experienced as tolerable, creating space for co-creating new meanings, aligning with the goals of DDP (Hughes & Golding, 2024). Feedback from caregivers in research into DDP and other dyadic psychotherapeutic approaches, suggests the therapist’s non-judgemental and curious stance may enhance the caregiver’s curiosity in the child’s internal world (Midgley et al., 2018; Wingfield & Gurney-Smith, 2019) . Through this process, children may idenitify with the therapists’ (and caregiver’s) curiosity, becoming more curious about their own and others’ minds (Fonagy & Bateman, 2006).
Key component three: Coregulation through light, playful interactions
Participants depicted relational, playful, fun and light aspects of the therapy, which appeared to be experienced as enjoyable and emotionally regulating. DDP is intentional in this approach to foster relational safety, helping children stay open and engaged. Some participants shared how these light and playful experiences supported their emotional regulation, enabling them to tolerate deeper exploration whilst maintaining connection with the therapist. For example, playing a game helped Asher to feel comfortable ‘sharing’. This aligns with findings in Wingfield and Gurney-Smith (2019) where parents noted the therapists’ playful stance supported children to be less guarded. Hughes et al. (2019), suggest this light, playful connected experience may allow children to explore closeness and intimacy in a way that feels safer than more direct forms of affection.
Key component four: Relational repair
Findings indicate that while there were instances of reciprocity, participants remained vigilant to potential threats in the therapeutic relationships. For example, Georgie’s perception of the therapists’ shift from friend to foe during a moment of misattunement highlighted the fragility of trust that may be a feature for children with early relational trauma. Tronick (1989, 2017) described intersubjective attachment relationships as inherently messy, with fluctuations between matched and mismatched states. He suggested that through such reparations, children develop positive self-representations and they learn they have agency within their relationships.
Key component five: Importance of agency in the therapeutic process
Exploration may feel uncomfortable for children who have developed defences against thinking about stressful events and past traumas. Participants depicted therapists providing messages that they were not trapped into exploring their trauma, as represented in Kirby’s example in Theme 1.1. Focussing on creating safety through attuned dyadic interactions and moments of lightness may be helpful for supporting children to enter conversations where new meanings about themselves and their experiences can be co-created (Capella et al., 2018). Allowing young people agency in their care may counterbalance children’s difficulties with control and trust, improving stability (Hughes et al., 2019; Jessiman et al., 2017).
How did children experience any differences in attachment security that came about through the therapeutic process?
Differences in attachment security One: The therapeutic journey
Participants depicted elements of mistrust into their story stems of the initial session. There were variations in the manifestation of this with some fearing the therapist and others anxious about rejection. Tangible progress was evident with participants depicting increased comfort, and increasingly connected moments with their therapist ‘it gets easier, and it is a good thing to do’.
Interpersonal neurobiology (Schore, 2001, 2021; Siegel, 2010, 2012) offers valuable insights into children’s initial mistrust. Porges (2011) posits that when young children experience threat, their dorsal vagal circuit is activated, triggering defensive nervous system responses. Children who faced repeated activation of their threat systems develop more robust defense systems than social engagement systems (De Bellis, 2001; Teicher et al., 2003). DDP focusses on creating safe relational experiences that soothe the nervous system helping children shift from chronic defensiveness (Baylin & Hughes, 2016), to more open and engaged stances. The data inferred that participants in the study began to enjoy their sessions more and tentatively trust the therapists’ curiosity. Such conditions may create increased opportunities for exploration, play and learning.
Differences in attachment security Two: Therapeutic caregiving and increased closeness
Caregivers were generally portrayed as emotionally attuned and curious, suggesting they were well prepared and orientated to DDP. Turner-Halliday et al. (2014) interviewed experienced DDP therapists who emphasised that the caregiver-child relationship was key for maintaining long term therapeutic change. Caregiver-child psychotherapeutic interventions require the therapist to consider not only their own therapeutic alliances with the child and caregiver but also the dynamics between the parent and child in the room. Current literature suggests this ‘in the moment’ focus presents opportunity to address past and present parenting realities, allowing for co-creation of new meanings (Jessiman et al., 2017; Turner-Halliday et al., 2014).
Three children in the current study described an increase in co-regulated and playful moments at home, suggesting that these interactions were becoming normalised, allowing opportunities for more joyful connection. Similarly, caregivers in Wingfield and Gurney-Smith’s (2019) study valued shared experiences, viewing them as strengthening the caregiver-child relationship, noticing improvements that transcended the therapy space.
Reflections on findings
The findings have several important clinical implications. They highlight the value of skilled practitioners who can provide the consistent, emotionally attuned interactions depicted as important by participants, whilst also facilitating the caregiver-child relationship. As a result, therapy outcomes are likely to be moderated by therapist effects (Baier et al., 2020). The findings also underscore the importance of robust training and DDP supervision to ensure therapists are equipped with the necessary relational skills. Training alone, without development through supervision, may not be sufficient to achieve the level of expertise required.
The active presence of the caregiver in therapy, and the significance of this relationship in fostering changes in attachment security, reinforces the first phase of the DDP approach. Allocating sufficient time and attention to building a strong alliance with the caregiver is likely to be crucial for success.
Play, playfulness and rituals were integral to the relational process, with implications for resources such as providing drinks, snacks, and creating inviting therapy spaces. Equally important are the emotional resources needed to offer the attuned, coregulating experiences vital to the process.
The dynamic nature of the intervention where there is a potential to shift from mistrust towards greater psychological safety is difficult to predict. In some cases, long term engagement may be necessary to foster increased attachment security and develop conversations that may lead to coherent autobiographical narratives. It may be helpful to view DDP as just part of a broader treatment plan, offering safety in relationships and laying the foundations for healing and trauma processing.
This study focussed on the experiences of children in adoption and special guardianship placements. However, children in foster care, residential placements, and other care settings may have different experiences with DDP, which would be valuable to explore. Additionally, examining the experience of DDP across diverse cultures and settings is important to gain a more comprehensive understanding.
Strengths and limitations
The play-based methodology and phenomenological philosophy of the study afforded opportunities to explore the essence of children’s experiences, focussing on key components and perceived differences in attachment security. The novel design allowed opportunity for children to creatively illustrate their experiences through play, reducing the pressure of direct questioning. Consistent with the findings in a review by Sun et al. (2023), the use of multiple data collection methods proved valuable in capturing rich data, minimising power imbalances, and encouraging children to feel comfortable.
This study supports the collaborative inclusion of young children who have trauma histories, in research, provided the design is sensitive and thoughtful. The methodology offers potential to generate discussion about how to meaningfully elicit children’s views about their care. While barriers exist – such as obtaining ethical approval to interview traumatised children, securing consent for children no longer living with birth families, and engaging children who may not trust adults – these challenges are not insurmountable to engaging this group in research. The study offers a rare opportunity to understand children’s experiences and perspectives which are often underrepresented in research regarding services and interventions (Luke et al., 2018; Sun et al., 2023).
Due to the study design, there were limitations in drawing conclusions about the impact of any factors such as trauma history, length of time in treatment, gender, age, relational context etc. Future research could explore these variables to better understand the effects.
The purposive sampling strategy deployed in this study capturing only children who progressed with DDP and had the emotional capacity to engage in the research, presents limitations. Arguably their experiences are unlikely to be negative. A design where participants are recruited prior to treatment commencement, and retained even if they discontinue treatment could mitigate this limitation, yielding more balanced findings. As a result the data cannot definitively identify the mechanisms of change in DDP practice, although elicited important insights into what children may perceive as important to their DDP therapeutic experience. It is anticipated that this deeper understanding of DDP from the child’s perspective will complement existing and emerging DDP research, shedding light on change processes typically evidenced quantitatively.
The results, drawn from a DDP sample, captured valuable insights into the dynamics of dyadic relationships. Whilst some findings may overlap with other psychotherapeutic approaches, others may be unique to DDP. Further research could help clarify what distinguishes DDP from other therapeutic models.
Conclusion
This is the first academic study focussing on the qualitative experiences of children undergoing DDP interventions. Findings suggests that the qualities of attuned relationships with the therapeutic adults were salient over any event or technique. Consistent with preliminary and somewhat limited literature supporting DDP (Purrington et al., 2023), and in alignment with DDP’s core aims, findings infer that the attuned presence of the therapeutic adults may influence the degree of perceived change in attachment security. By generating the relational conditions that blend affective states with reflective functioning, and through the active involvement of caregivers, DDP may foster opportunities for increased attachment security, facilitate trauma resolution, and support children and their families to learn to thrive.
Supplemental Material
Supplemental Material - Dyadic developmental psychotherapy for children with developmental trauma histories: An exploration of children’s therapeutic experiences
Supplemental Material for Dyadic developmental psychotherapy for children with developmental trauma histories: An exploration of children’s therapeutic experiences by Jessica Christopher, Caroline Cresswell, and Julie Davies in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgments
We would like to thank the 6 very special children who participated in this research, along with their families and clinicians. We would also like to thank the 5 DDP clinicians who took part in the focus group, and the DDP Institute. Finally, we would like to thank Dr Kim Golding for consultation and support of the project and Nicky Gooden for providing an Expert by Experience perspective.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
Anonymous task data is stored on the University of Hertfordshire GDPR compliant one drive and is available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.