
Abstract
Background
Obsessive-compulsive disorder (OCD) and autism spectrum disorder (ASD) often co-occur and have overlapping symptom profiles. Detection and diagnosis of ASD in youth with OCD can therefore be challenging but is crucial to inform care planning.
Aim
The current study aimed to provide a psychometric evaluation of the Social Communication Questionnaire (SCQ), a widely used parent-report measure for assessing ASD traits, in youth with OCD.
Method
In total, 484 young people with an ICD-10 diagnosis of OCD completed a battery of measures as part of a specialist clinical assessment.
Results
Exploratory factor analyses (EFA) suggested a multidimensional factor solution for the SCQ, although an adequate factor solution was not identified due to cross-loading and/or weak loading items. The SCQ had good internal consistency (KR20 = 0.85), and good convergent validity with the Strengths and Difficulties Questionnaire (SDQ) Prosocial Behaviour subscale (r = −0.52) and Peer Problems subscale (r = 0.48). The SCQ differentiated those with versus without a clinical diagnosis of ASD with reasonable accuracy (area under the curve = .76).
Discussion
The current findings support the use of the SCQ as a measure of ASD traits in youth with OCD, suggesting that this quick and easy-to-administer measure could aid detection of ASD in this population.
Plain language summary
Obsessive-compulsive disorder (OCD) and autism spectrum disorder (ASD) often occur together and have some similar symptoms. Because of this, identifying ASD in young people with OCD can be difficult but is important for planning their care. This study looked at how well the Social Communication Questionnaire (SCQ), a parent-completed questionnaire commonly used to identify ASD traits, works for young people with OCD. The study involved 484 young people who had been diagnosed with OCD. Their parents completed different questionnaires as part of a specialist clinical assessment. Scores on the SCQ were related to other measures of social behaviour, and less strongly related to measures of other difficulties, meaning that the SCQ seems to measure what it is supposed to. The SCQ was able to distinguish between those with and without an ASD diagnosis with a reasonable level of accuracy. The findings suggest that the SCQ is a useful tool for detecting ASD traits in young people with OCD. Since it is quick and easy to use, it could help professionals identify ASD in this group more effectively.
Keywords
Introduction
Obsessive-compulsive disorder (OCD) is an impairing condition affecting approximately 2% of children and adolescents according to epidemiological studies (Douglass et al., 1995; Heyman et al., 2001). OCD commonly co-occurs with neurodevelopmental disorders, including autism spectrum disorder (ASD) (Aymerich et al., 2024). Previous research has found that approximately one in four young people with OCD who attend mental health services have an additional diagnosis of ASD (Martin et al., 2020). Importantly, young people with comorbid OCD and ASD are more likely to experience greater functional impairment, higher levels of concurrent psychopathology, poorer insight into their OCD, higher levels of service utilisation, and poorer treatment outcomes, compared to those without ASD (Griffiths et al., 2017; Jassi et al., 2021; Martin et al., 2020; Murray et al., 2015).
Detection and diagnosis of ASD among youth with OCD is of paramount importance for informing OCD treatment and broader care planning. However, data suggest that ASD is diagnosed, on average, more than 2 years later in youth with OCD compared to those without OCD (mean age at ASD diagnosis of 13 years 4 months vs. 10 years 9 months, respectively) (Martin et al., 2020). This delay is clinically significant, and for many young people will be the difference between receiving an ASD diagnosis before versus after secondary school transition, which is often a critical period when support needs to be optimised. It is unclear why the diagnosis of ASD is delayed in youth with OCD, but one possibility is diagnostic overshadowing. There is considerable overlap in the core features of OCD and ASD, including repetitive or ritualistic behaviours and a need for routine and ‘sameness’. For example, lining up items such as toys may be a behaviour observed in young people with OCD and ASD, however it serves different functions in each. In OCD, the behaviour is typically ego-dystonic, and something that an individual does not want to do but feels compelled to in order to reduce anxiety and/or prevent a feared outcome from occurring. In ASD, the behaviour is usually ego-syntonic and often pleasurable (Pazuniak & Pekrul, 2020). It is plausible that when a young person has a pre-existing diagnosis of OCD, clinicians may be prone to misattributing certain ASD-related features to OCD. A key priority therefore is to improve detection of ASD among youth with OCD.
A range of tools have been developed for assessing ASD in young people. The gold-standard tools are clinician-administered interviews and observation schedules, such as the Autism Diagnostic Observation Schedule (ADOS) (Gotham et al., 2006) and Autism Diagnostic Interview (ADI) (Lord et al., 1994). However, these are time-consuming to administer and require specialist training and clinical expertise, and hence there are often barriers to accessing these assessments. Questionnaire measures of ASD traits have many advantages, including being quick, easy, non-intrusive and inexpensive to administer. They can serve as a useful initial screener and indicate where full clinical assessment is warranted, ensuring optimal allocation of resources. One such questionnaire measure is the Social Communication Questionnaire (SCQ) (Rutter et al., 2003). The SCQ is a widely used, parent-report questionnaire, based on the ADI. The SCQ has been well-validated in young people with ASD with excellent internal consistency (0.83–0.87) (Avcil et al., 2015; Brooks & Benson, 2013), and high sensitivity and specificity for detecting ASD (Berument et al., 1999). The SCQ was originally found to have a 4-factor structure (Berument et al., 1999), but subsequent studies have found that a three-factor structure (representing abnormal language/social interaction, communication, and restrictive and repetitive behaviours subscales) provides a better fit to the data (Grove et al., 2019; Wei et al., 2015).
Of note, the psychometric properties of the SCQ may vary across populations (Corsello et al., 2007; Wei et al., 2015). Thus, it is important to evaluate its properties in the specific populations where it may have clinical value. There is a particular need to establish its utility in OCD populations given the overlap in the clinical expression of OCD and ASD. The current study therefore aimed to provide a psychometric evaluation of the SCQ in a sample of young people with a diagnosis of OCD. We hypothesised that the SCQ would have a high internal consistency, good convergent and divergent validity (i.e., greater correlations with measures of ASD-related difficulties such as some SDQ subscales, than other psychopathologies), and a 3- or 4-factor structure (Berument et al., 1999; Wei et al., 2015). We further hypothesised that the SCQ would discriminate well between young people with versus without a clinical diagnosis of ASD.
Methods
Participants
Participants were 484 young people aged 5–18 years old (Mean = 14.9, SD = 2.0), who attended the National and Specialist OCD, BDD and Related Disorder Clinic at the Maudsley Hospital in London. Referral criteria for the service included intellectual functioning in the normal range (i.e., absence of global learning disability). All participants had a primary diagnosis of OCD according to the International Classification of Diseases (ICD)-10 diagnostic criteria (World Health Organisation, 2015), following specialist multidisciplinary team assessment, which also assessed for other comorbidities, as previously described (Nakatani et al., 2011). Of the total sample, 213 participants (44%) also had a confirmed diagnosis of ASD, 209 (43%) did not have ASD and 62 (13%) had a query relating to ASD or information regarding ASD status had not been recorded. ASD diagnoses were typically assigned prior to the referral to the specialist OCD Clinic by a Consultant Psychiatrist in a community Child and Mental Health Service (CAMHS), often in conjunction with an ASD structured diagnostic assessment as previously described (Jassi et al., 2021). No participants had a diagnosed global learning disability, as per the service referral criteria (see above).
Measures
Social Communication Questionnaire (SCQ)
The SCQ is a widely used, 40-item questionnaire based on the Autism Diagnostic Interview Revised used to assess autistic features (Berument et al., 1999). The questionnaire is specified for use with children aged 4 years and older, and a mental age of above 2 years (Rutter et al., 2003). It is completed by parents, with the first of the items not contributing to any total score calculation but identifying whether the individual is verbal or non-verbal. Each item is binary, with the total score ranging from 0–39. A cut-off score of ≥15 has been shown to have good sensitivity and specificity for identifying ASD (Berument et al., 1999). There are two forms of the SCQ; The ‘Lifetime’ version considers an individual’s entire developmental history whereas the ‘Current’ version focusses on the previous three-months. The present study employed the current form due to its ability to measure current difficulties.
Strengths and Difficulties Questionnaire (SDQ)
The SDQ is a 25-item measure of behavioural and emotional difficulties that can be used in children and adolescents aged 4–17 (Goodman, 1997). The current study employed scores from the parent-report version in order to compare against the SCQ. The SDQ has five subscales with five items each assessing: emotional problems, conduct problems, hyperactivity problems, peer problems and prosocial behaviours. The total score for each subscale ranges from zero to 10, except for the prosocial scale which is scored from 0–5. Higher subscale scores are indicative of greater difficulties, except for prosocial behaviour where a higher score denotes better functioning. All items, excluding the prosocial scale, can be combined into a ‘total difficulties’ score, which ranges from 0–40. The SDQ has been shown to have excellent psychometric properties (Goodman, 2001). Elevated SDQ total and subscale scores have often been observed in young people with ASD (Russell et al., 2013). Specifically, the Peer Problems and Prosocial Behaviour subscales of the parent-report SDQ, have been frequently reported to have a specific association with ASD traits (Grasso et al., 2022; Salayev & Sanne, 2017).
Children’s Obsessional Compulsive Inventory Revised (ChOCI-R)
The ChOCI-R is used to assess OCD symptoms and associated impairment in children and young people aged 7–17 years (Shafran et al., 2003). The parent-report version was used in the current study for comparison with the SCQ. The ChOCI-R consists of 32 items separated into two sections: ‘compulsions’ and ‘obsessions’, each comprising 16 questions. Both sections start with 10 questions regarding OCD symptoms followed by six questions regarding severity and impairment associated with OCD symptoms. The total score is generated by summing the 12 impairment and distress items, which are each scored on a zero to 4 scale, with higher scores indicating greater severity. These yield an overall total score ranging from zero to 48, and a sub-total score of zero–24 for each of the obsession and compulsion subscales. The ChOCI-R has been demonstrated to have excellent internal consistency and good convergent and discriminant validity (Uher et al., 2008).
Procedure
The present study used data collected as part of a larger assessment battery administered to those participating in clinical trials or utilizing clinical services at the National and Specialist OCD, BDD and Related Disorder Clinic. All data was collected as part of routine clinical practice during the initial intake assessment and approval for the study was granted by the South London and Maudsley CAMHS Audit Committee.
Statistical analyses
Descriptive statistics were employed to assess the demographic and clinical characteristics of the sample. The symptom profile of the sample was looked at using descriptive statistics and graphs depicting frequency of SCQ item endorsement for the whole sample as well as OCD + ASD and OCD subsamples.
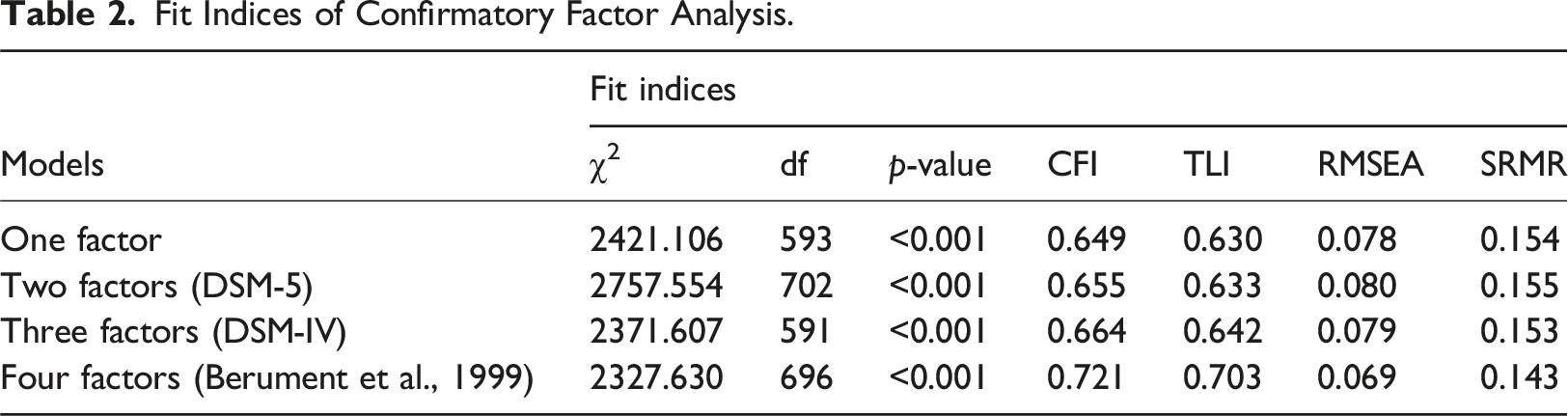
Confirmatory factor analysis (CFA) was conducted on the whole sample to test the following models, in keeping with previous research (Grove et al., 2019): a one-factor solution including all 39 items; a two-factor solution mirroring DSM-5; a three-factor solution mirroring DSM-IV; and a four-factor solution, consistent with the original SCQ factor analytic study (Berument et al., 1999). As per Grove et al., (2019) the two factor (DSM-5) and three factor (DSM-IV) solutions included 36 items, whereas the one factor and four factor models included all 39 items. For the CFA, we used the estimator weighted least square mean and variance adjusted (WLSMV) given the categorical nature of the items, and Promax rotation, which allows factors to correlate. Model fit was evaluated using the root mean square error of approximation (RMSEA) (Steiger & Lind, 1980), comparative fit index (CFI) (Bentler & Chou, 1987) and the Tucker-Lewis index (TLI) (Tucker & Lewis, 1973). RMSEA scores below 0.08 and 0.05 indicate good and excellent model fit, respectively (Browne & Cudeck, 1992). TLI and CFI scores above 0.90 are indicative of a good model fit (Brown, 2006; Hu & Bentler, 1999).
To explore reliability and internal consistency, item-total correlations were calculated using the Kuder-Richardson reliability coefficient (KR20), with a cut-off value of >0.8 being considered good (Fayers & Machin, 2007). KR-20 was chosen due to the binary nature of the scored items on the SCQ. Convergent and divergent validity of the SCQ was determined by examining the correlation of the SCQ total score with the SDQ total score its subscales (Emotional Symptoms, Conduct Problems, Hyperactivity/Inattention, Peer Relationship Problems, Prosocial Behaviour), and the ChOCI-R total score and its subscales (Obsessions, Compulsions). To accomplish this, Pearson correlation analyses were performed.
Discriminant analysis was performed to test whether SCQ item responses could predict ASD status in our sample. Items 2–40, inclusive, were entered into a stepwise discriminant analysis based on OCD and OCD + ASD groups. An evaluation through entry and removal of each item was done, and the final model was determined by partial F values. Wilks’ Lambda was used to indicate variance explained by the model.
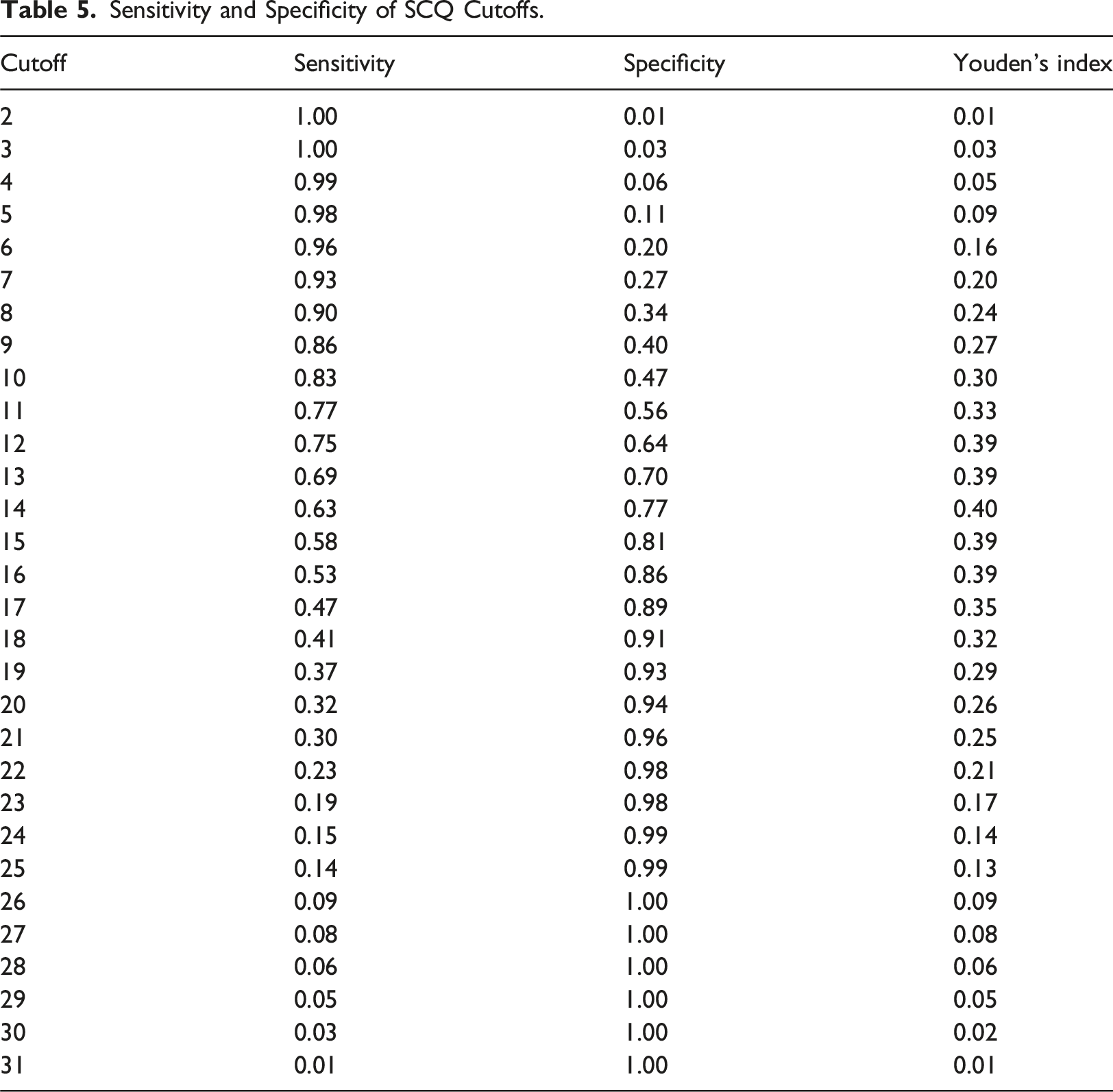
A receiver operating characteristics (ROC) plot was used to assess the sensitivity and specificity of the SCQ in discriminating between those with and without a clinical diagnosis of ASD. Sensitivity is the proportion of true positives that is correctly identified by the test, while specificity is the proportion of true negatives that is correctly identified by the test. A ROC curve involves plotting sensitivity against 1 – specificity, and the Area Under the Curve indicates the accuracy of the diagnostic test, with 0.5 indicating that the test performs at chance level while 1.0 indicates perfect accuracy. Youden’s Index (Sensitivity + Specificity - 1) was calculated and used to identify the cut-off with the best balance of sensitivity and specificity.
CFA and EFA were conducted in Mplus version 8.8 (Muthén & Muthén, 1998-2017). The remaining analyses were carried out using SPSS 27 (IBM Corp. Released 2020).
Results
Sample characteristics
Demographic and Clinical Characteristics.
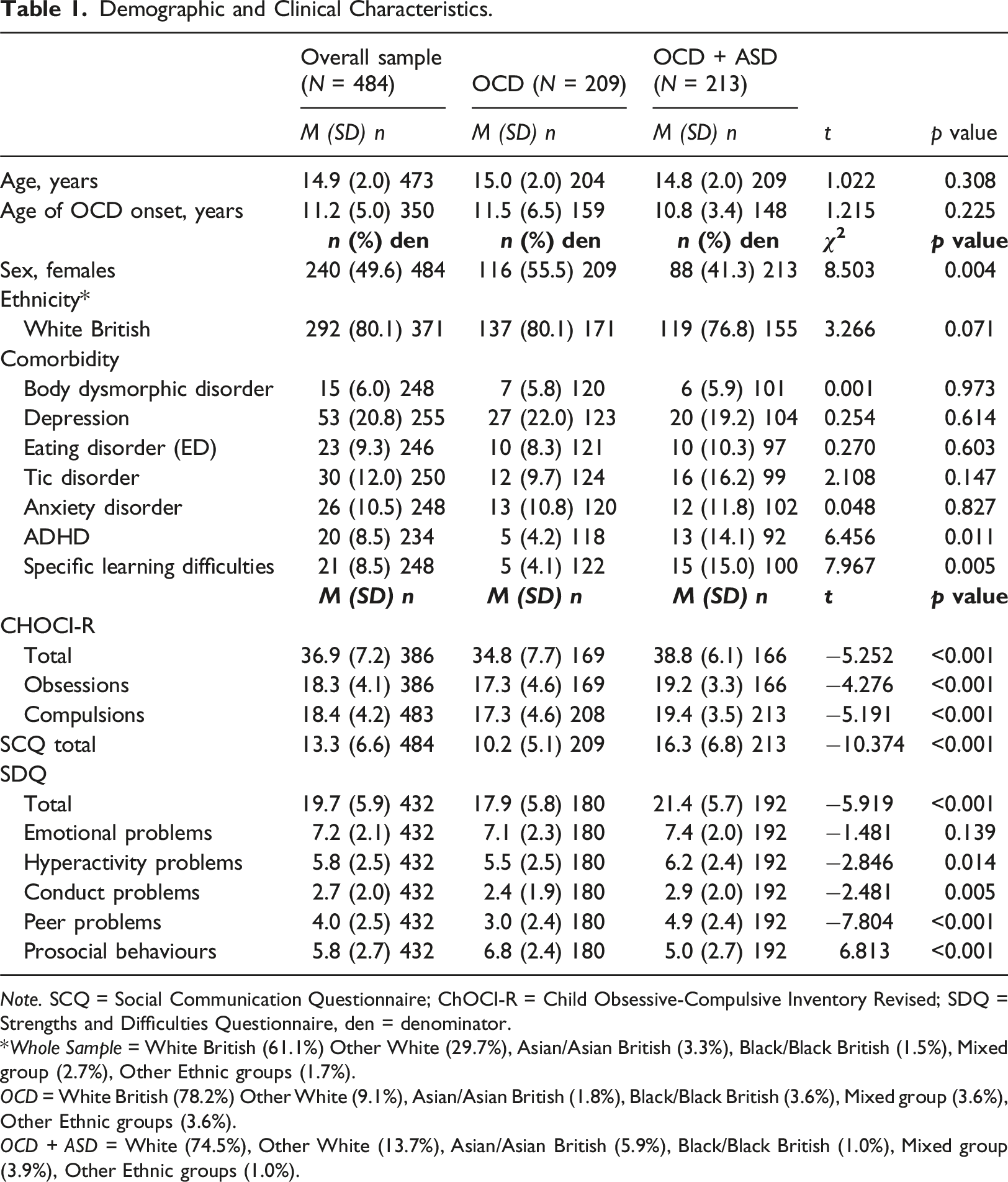
Note. SCQ = Social Communication Questionnaire; ChOCI-R = Child Obsessive-Compulsive Inventory Revised; SDQ = Strengths and Difficulties Questionnaire, den = denominator.
*Whole Sample = White British (61.1%) Other White (29.7%), Asian/Asian British (3.3%), Black/Black British (1.5%), Mixed group (2.7%), Other Ethnic groups (1.7%).
OCD = White British (78.2%) Other White (9.1%), Asian/Asian British (1.8%), Black/Black British (3.6%), Mixed group (3.6%), Other Ethnic groups (3.6%).
OCD + ASD = White (74.5%), Other White (13.7%), Asian/Asian British (5.9%), Black/Black British (1.0%), Mixed group (3.9%), Other Ethnic groups (1.0%).
The frequency of endorsement of individual SCQ items for the whole sample and the OCD and OCD + ASD subsamples is shown in Supplemental Figures S1 and S2 respectively. The most commonly endorsed item for the whole sample was ‘not sharing interests’ (endorsed by 89.5% of parents), and the least frequent was ‘mixing pronouns’ (endorsed by 8.3% of parents) (see Supplemental Figure S1).
As expected, the vast majority of SCQ items were endorsed more frequently by parents of the OCD + ASD group than the OCD group (see Figure S2). Group differences were greatest for item 33 assessing ‘normal facial expressions’ (rated as atypical for 2.9% of the OCD group vs. 25.4% of the OCD + ASD group), followed by item 27 assessing ‘smiling back’ (atypical for 6.2% of the OCD group vs. 31% of the OCD + ASD group) and item 14 assessing ‘interest in 5 senses’ (atypical for 12.4% of the OCD group vs. 57.4% of the OCD + ASD group).
On some items, those with OCD scored positive more frequently than those with OCD + ASD, most notably item 23 assessing ‘using gestures to show needs’ (atypical for 81.3% of the OCD group vs. 71.8% of the OCD + ASD group) and item 32 assessing ‘gesturing for attention’ (atypical for 30.1% of the OCD group vs. 19.7% of the OCD + ASD group).
Factor structure
Fit Indices of Confirmatory Factor Analysis.
Internal consistency
The KR20 value for the whole sample was 0.85, demonstrating good internal consistency. In addition, KR20 values when individual items were deleted ranged from 0.84 to 0.86 (see Supplemental Table S6), supporting the adequate contribution of all items to the measure. For the OCD group, KR20 value was 0.81 while for the OCD + ASD group this was 0.84.
Convergent and divergent validity
Scale Intercorrelations for the Whole Sample.
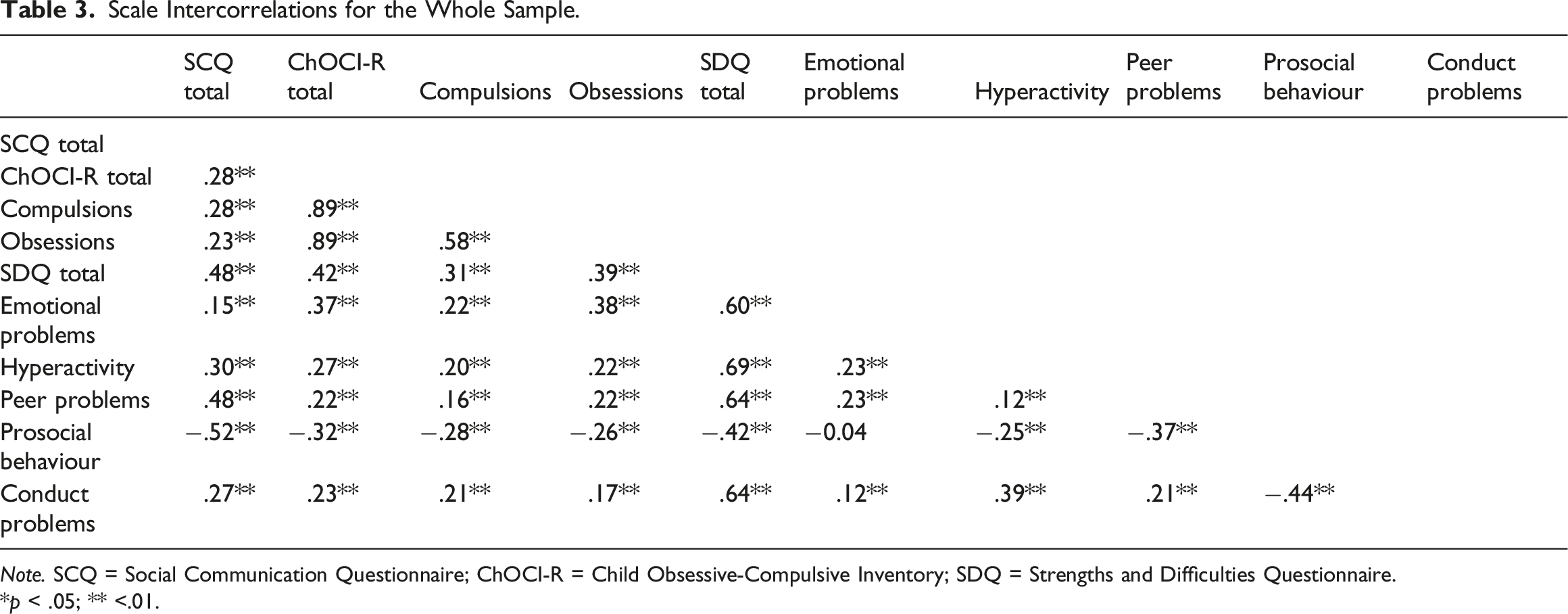
Note. SCQ = Social Communication Questionnaire; ChOCI-R = Child Obsessive-Compulsive Inventory; SDQ = Strengths and Difficulties Questionnaire.
*p < .05; ** <.01.
Discriminant analysis
Discriminant analysis was performed to test whether SCQ item responses could predict ASD status in our sample. Following the entry and removal of each item, as determined by partial F values, the final model contained 8 items. Wilks’ Lambda had a value of 0.64, indicating that the model explained about 36% of the variance.
Discriminant Analysis Results.
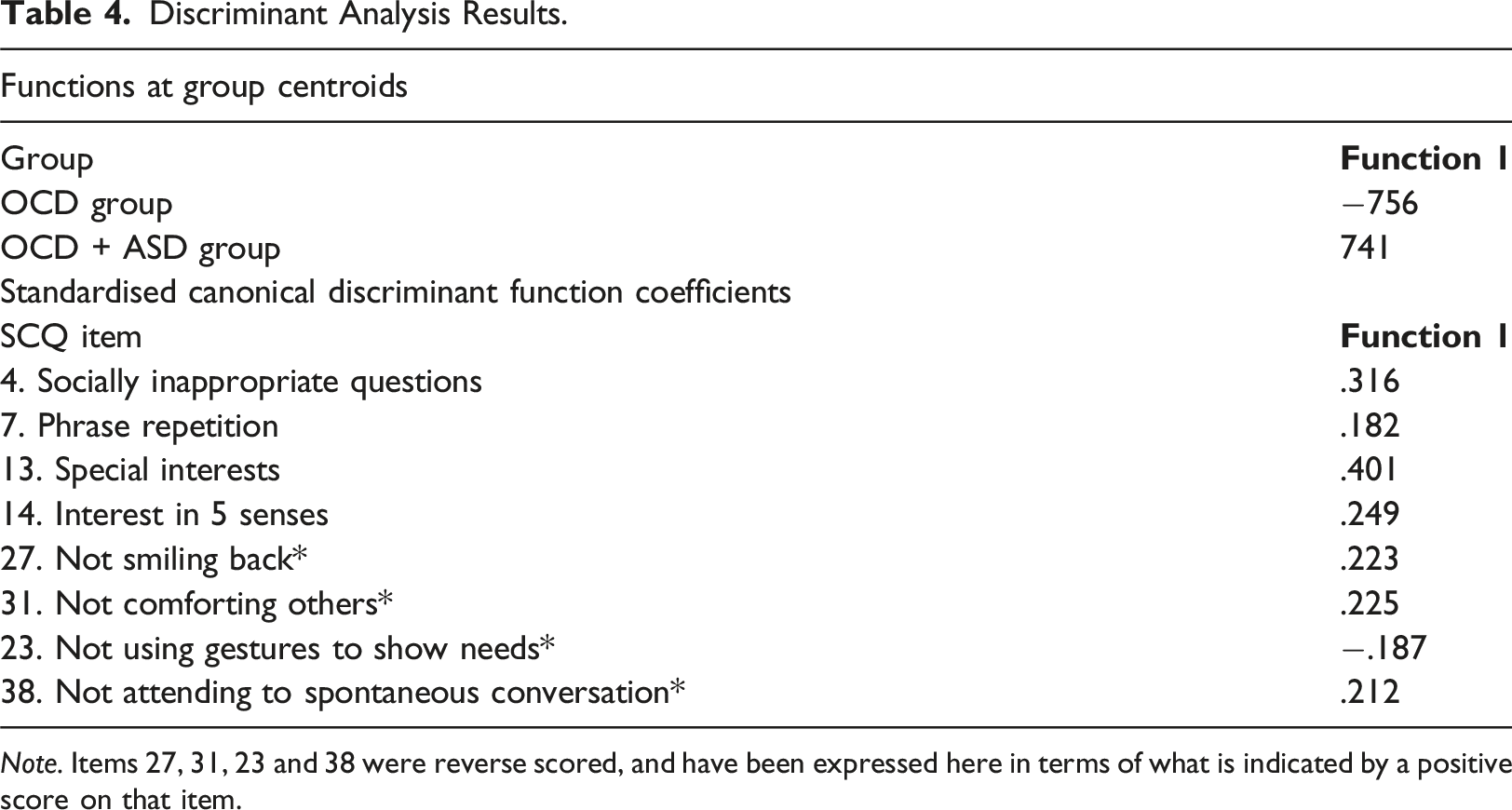
Note. Items 27, 31, 23 and 38 were reverse scored, and have been expressed here in terms of what is indicated by a positive score on that item.
ROC analysis and cut-off estimation
Sensitivity and Specificity of SCQ Cutoffs.
Discussion
The current study is the first to evaluate the psychometric properties of the SCQ, a widely used measure of ASD traits, in a clinical sample of young people with OCD. Since ASD is a common comorbidity in young people with OCD, and the two disorders can be difficult to disentangle, valid and reliable ASD screening tools have important clinical utility. Overall, our findings indicate that the SCQ has good psychometric properties in young people with OCD, and support its use as an ASD screener in this population.
More specifically, we found good internal consistency, suggesting that the SCQ is a cohesive scale, which is in agreement with previous findings (Avcil et al., 2015; Brooks & Benson, 2013). Furthermore, internal consistency showed minimal variation when we tested the effect of individual item deletion, thereby providing further support for internal reliability. We also found evidence to support convergent and divergent validity of the SCQ in our OCD sample. As predicted, the SCQ total score showed a large, negative association with the prosocial behaviour subscale of the parent-report SDQ, which has been shown to have a specific association with ASD (Salayev & Sanne, 2017). We also observed a moderate-to-large, positive correlation with the peer problems SDQ subscale, consistent with previous research showing an association between peer difficulties and the SCQ as well as ASD generally (Charman et al., 2015; Iizuka et al., 2010). As expected, we found that the SCQ was weakly correlated with other parent-report measures of child psychopathology, including OCD, emotional problems, conduct problems, and hyperactivity. Of particular importance to the current study was the relatively small correlation of the SCQ with OCD symptoms (r = 0.28). This finding suggests that there is not substantial measurement overlap between the SCQ and ChOCI-R, despite some items being similar across measures (e.g., the presence of rituals).
In our OCD sample, the SCQ was able to differentiate between those with and without a co-occurring diagnosis of ASD with moderate accuracy, with 79% being correctly classified. Moreover, our analyses indicated that the items that best discriminated between those with and without ASD were those pertaining to special interests, asking socially inappropriate questions and sensory interests. In a previous study looking at the SCQ, these items were among the 28 items that were able to significantly differentiate between young people with ADHD versus ASD (Mouti et al., 2019). Interestingly, in another previous study of the SCQ, these items were not among the 10 items found to distinguish between young people with ASD versus Tourette syndrome, indicating that discriminant ability of individual items on the SCQ appears to vary across diagnostic groups (Eapen et al., 2019). The eight SCQ items that best predicted ASD status in the current study were primarily in social and communication domains. Unlike ritualised and repetitive behaviours, these may be the groups of symptoms that best differentiate ASD and OCD. The current findings could be helpful to those conducting clinical assessments as it highlights the areas to focus on to help establish a diagnosis of ASD in this population, particularly when grappling with disentangling ASD indicators and OCD symptoms. The results of our ROC analyses indicated that the conventional SCQ cut-off score of equal to or greater than 15 may be conservative for detecting ASD among adolescents with OCD. We found that a cut-off of equal to or greater than 14 produced the best balance between sensitivity and specificity. However, the most appropriate cut-off should be determined in the context in which the measure is used, and in some settings, there may be value in using a lower cutoff in order to increase sensitivity, and reduce the possibility of overlooking a diagnosis of ASD. For example, a lower cutoff of greater than or equal to 10 corresponded to high sensitivity (.83), albeit lower specificity (.47).
Although the current study found evidence of good internal consistency, convergent and divergent validity, and discriminant ability, it was not possible to determine the factor structure of the SCQ. Confirmatory factor analysis indicated that none of the previously hypothesised one-, two-, three- or four-factor models provided a good fit for our data, and an exploratory factor analysis failed to produce a good fitting model. It is notable that previous factor analytic studies of the SCQ have produced highly variable results, with some studies identifying 3-factor and 4-factor solutions (Avcil et al., 2015; Oner et al., 2012), and others finding no good fitting factor solution (Grove et al., 2019). The lack of clear factor structure in the current study may partly reflect heterogeneity within our sample, with respect to demographic and clinical characteristics. While our analyses indicate that the SCQ is likely to have a multi-factor structure, our results suggest that a single total score may nevertheless have clinical utility in discriminating ASD traits in young people with comorbid OCD. We did not have a sufficiently large sample to stratify our analyses (e.g., by sex, age, ethnicity) or to test measurement invariance across subgroups, and future studies should seek to examine this.
The current findings should be considered within the context of several limitations. First, ASD diagnoses were made in routine clinical practice, rather than being consistently based on a gold standard, structured diagnostic assessment. In addition, a proportion of the sample did not have confirmed ASD diagnostic status; either this information has not been recorded (n = 1) or they had been documented as having possible ASD but no confirmed diagnosis (n = 61). Second, the sample was drawn from a specialist clinic that tends to see relatively severe and complex cases of OCD, and findings may therefore not be generalisable across settings. Similarly, the sample also largely comprised of white British young people and therefore may not be representative of the wider population. Additionally, because all participants in current study had an IQ within the normal range, findings may not be generalisable to young people with ASD and global learning disability. Third, it is plausible that the properties of the SCQ vary across different OCD dimensions, and future studies should seek to examine this. For example, ordering/arranging OCD symptoms, may more appear similar to repetitive behaviours in autism. Therefore, the SCQ may be more likely to highlight false positives, for young people with these OCD symptoms compared to, for example, contamination symptoms. Finally, the current study assessed the validity of the SCQ in a sample of children with psychiatric and/or developmental and/or behavioural concerns (OCD and ASD). Future studies could benefit from including a healthy control group (Aldosari et al., 2019). This would further test the potential use of the SCQ for routine clinical screening.
In conclusion, the findings from this study suggest that the SCQ is a valid and reliable measure of ASD traits in young people with OCD, and indicate that a cut-off of 12–14 may be optimal in identifying ASD. Our findings align with previous studies that have validated the use of the SCQ in young people with comorbidities such as Tourette’s Syndrome (Eapen et al., 2019) and intellectual disabilities (Sappok et al., 2015). The SCQ has the potential to aid clinicians in differentiating symptoms of OCD and ASD, and could promote detection and diagnosis of ASD in youth with OCD.
Supplemental Material
Supplemental Material - An evaluation of the psychometric properties of the social communication questionnaire in young people with obsessive-compulsive disorder
Supplemental Material for An evaluation of the psychometric properties of the social communication questionnaire in young people with obsessive-compulsive disorder by Ilke Ozcan, Pablo Vidal-Ribas, Ellie Roberts, Amita D Jassi, Nicole Clancy, Chiara Causier, Victoria Hallett and Georgina Krebs in Clinical Child Psychology and Psychiatry
Footnotes
Author Contributions
IO undertook analyses and wrote sections of the manuscript. PVR undertook analyses and reviewed/edited the manuscript. ER assisted in analyses and writing the manuscript. NC assisted in data collection and edited the manuscript. CC reviewed and edited the manuscript. AJ and TH contributed to the design of the study and reviewed/edited the manuscript. GK conceived the study, undertook analyses, and wrote sections of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr Vidal-Ribas is supported by grant RYC2021-033369-I, funded by MCIN/AEI/10.13039/501100011033 and the European Union « NextGenerationEU/PRTR», and the CERCA program from the Generalitat de Catalunya. Dr Krebs has received research funding from the Wellcome Trust, the British Academy, and honoraria from Elsevier for editorial work.
Ethical statement
Data Availability Statement
Aggregate data can be made available upon request.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.