
Abstract
Background
Care-experienced young people (CEYP) have far higher rates of mental ill-health than their peers. Less is known about their wellbeing and the overlap between mental health and wellbeing in this population. Drawing on two samples of CEYP, we explored mental health and wellbeing profiles, the overlap between these, and basic predictors of symptom severity.
Methods
We recruited two samples of CEYP: 269 10-13-year-olds and 155 16-17-year-olds, and their primary caregiver. All participants were either in local authority (out-of-home) care or had been adopted from the care system in England and Wales. Participants completed standardised measures of anxiety-, depression-, PTSD-, and externalising symptoms, as well as standardised wellbeing measures.
Results
The majority of young people in both samples reported clinically-elevated symptomology, with mental health and wellbeing particularly poor in the late adolescents sample. Almost half of the 16-17 year old sample rated their wellbeing as poor. Overall, we found moderate associations between mental health and wellbeing. In early adolescents, these associations were less clear (many with clinically-elevated mental health reported average wellbeing), but for older teens poor mental health was closely related with the poorest reported wellbeing. There was no consistent evidence that age, gender, or ethnicity predicted wellbeing, but mental health was generally the poorest for older teens in residential care placements.
Conclusions
We found high levels of disorder-specific mental health symptomology in CEYP, with 16–17-year-olds having particularly high levels of mental health difficulties and low wellbeing. Results highlight the crucial role of early intervention and prevention in this group, before difficulties become entrenched and affect wider aspects of wellbeing.
Plain language summary
There is a lack of research on the mental health and wellbeing of care-experienced young people, which has an impact on the support young people receive. Our paper highlights common mental health symptoms (e.g. anxiety, depression, post-traumatic stress) among care-experienced young people over two key ages: early and late adolescence. We show that mental health and wellbeing are distinct but overlapping constructs, and that this overlap is particularly strong by late adolescence. Our findings highlight the urgent need for early intervention and preventative support for care-experienced young people, to reduce the likelihood of mental health difficulties and poor wellbeing as they approach adulthood.
Introduction
Care-experienced young people (CEYP) often face significant early adversity and interpersonal trauma, with child maltreatment being a primary reason for their entry into state care (known as local authority care in the UK; Department for Education, 2022). Research shows CEYP experience rates of mental health difficulties approximately five times higher than their peers; around half of children in care meet the criteria for a diagnosable mental health condition (Bronsard et al., 2016; Engler et al., 2022; Ford et al., 2007). Similarly, young people adopted from local authority care are at greater risk of mental health difficulties compared to their non-adopted peers (Paine et al., 2021) and are twice as likely to engage with professional mental health services (Barroso et al., 2017; Behle & Pinquart, 2016; Keyes et al., 2008).
While we have good evidence of the mental health needs of CEYP (although this evidence is predominantly from studies published almost 20 years ago), the UK evidence base for CEYP’s wellbeing is more recently emerging, and there is limited research on the intersection of mental health and wellbeing. Anthony et al. (2022) used national Welsh school survey data and found that CEYP had lower subjective wellbeing compared to their non-care-experienced peers, with those in residential care having the lowest subjective wellbeing. Wijedasa et al. (2022) presented self-reported mental health symptoms and subjective wellbeing profiles of CEYP aged 11–18 years during the COVID-19 pandemic, compared to the general population. CEYP reported higher mental health difficulties and significantly lower wellbeing compared with the general population (Wijedasa et al., 2022). Another large-scale study, with almost 5,000 CEYP, explored demographic and service level factors associated with wellbeing and found that a longer length of time in care, fewer placement moves and being male were associated with higher wellbeing (Suh & Selwyn, 2023). Associations between mental health and wellbeing were not explored in these studies.
There is an ongoing debate regarding whether mental health and wellbeing are distinct constructs or two ends of a single spectrum. The single continuum model posits that wellbeing is the absence of mental ill-health and that enhancing wellbeing can reduce mental health difficulties, and vice versa. Conversely, the dual continua model (Keyes, 2002) contends that mental health and wellbeing are separate but related constructs, implying that individuals can experience mental health difficulties while maintaining high wellbeing (Gautam et al., 2024). Proponents of the dual continua model argue that while mental health refers to an individual’s overall psychological state which allows them to function in daily life, wellbeing is a broader concept that encompasses life satisfaction, perceived quality of life and the ability to cope with stress and adversity (Keyes, 2002). There is growing evidence in the general population of young people that mental health and wellbeing are separate but related constructs (Kinderman et al., 2015; Patalay & Fitzsimons, 2016). For example, one study found there only to be a modest association between child reported mental health and wellbeing (Sharpe et al., 2016), and another reported that mental health and wellbeing have both shared and unique predictors (Patalay and Fitzsimons (2016). It is unclear if these findings hold amongst CEYP.
We aimed to characterise the mental health and wellbeing profiles of CEYP and explore the overlap in these constructs, during early and later adolescence, drawing on two samples of CEYP (one of 10–13-year-olds and one of 16–17-year-olds). Adolescence can be a period of significant change, including in mental health and wellbeing, which is potentially even more potent in a population of young people who have high rates of trauma exposure and experience high rates of instability (Stein & Dumaret, 2011; Tarren-Sweeney, 2008). Our second aim was to explore demographic and service level predictors of mental health and wellbeing for CEYP, including age (given mental health difficulties tend to increase over adolescence; Goldbeck et al., 2007; Rice et al., 2003); sex (with evidence females are more likely to experience internalising difficulties and males more likely to display externalising behaviours; Ford et al., 2007); ethnicity (seldom explored but some evidence that White CEYP experience higher mental health difficulties compared to CEYP from other ethnic groups; Hiller et al., 2023; Wijedasa et al., 2022) and placement type (with some evidence that young people in residential care have particularly poor mental health and wellbeing; Ford et al., 2007; Hiller et al., 2021). This evidence is important for understanding the applicability of key mental health and wellbeing theories for CEYP and for providing services with higher quality evidence on the needs of their young people, including any demographic markers of risk.
Method
Participants
Demographic Characteristics of the Sample.
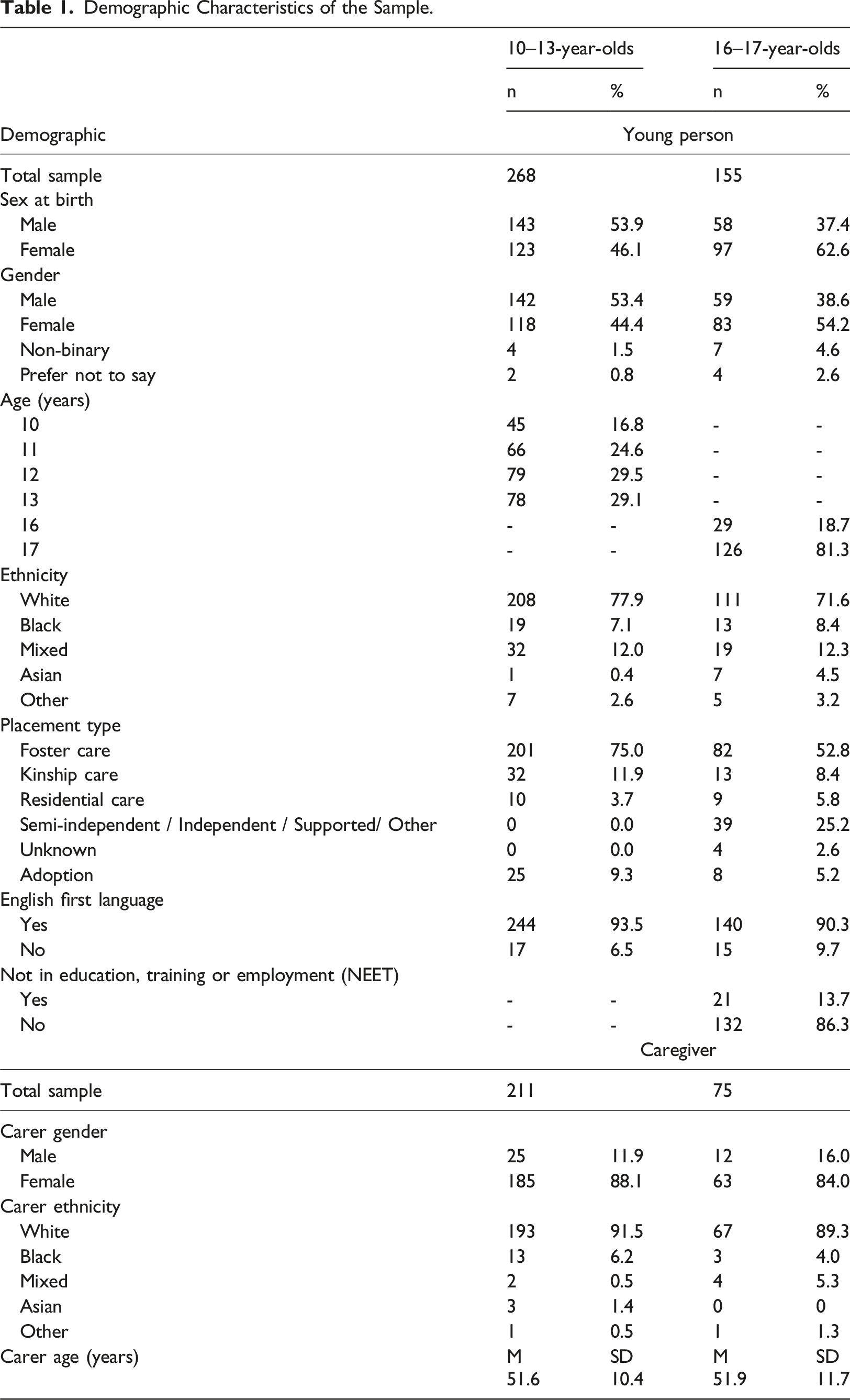
For all participants there was the option for their caregiver to participate. For consistency, we use the term caregiver to refer to any primary caregiver of the participant, whether a foster carer, kinship carer, adoptive parent, or keyworker (for those living in residential care). For the younger group, 216 (80%) caregivers participated, while for the older group, 75 (48%) caregivers participated. The lower participation in the older group was because many of the young people in local authority care reported not having a consistent and trusted adult who they would want to report on their mental health. Descriptive data for the caregivers are in Table 1.
Procedure
We used baseline data from an ongoing longitudinal research study that is registered on the Open Science Framework [https://osf.io/7qx54]. Ethical Approval was obtained from the University College London Research Ethics Committee (Ref: 22253/001), along with approval from the Association of Directors of Children’s Services and research governance requirements of the participating Local Authorities. Safeguarding and risk escalation procedures were in place and mental health assessment summary letters were sent to social workers or (adoptive) parents when necessary.
For those in care, senior local authority staff in the thirteen participating local authorities provided informed consent for young people to participate in the research. Young people provided their own informed assent (or consent if 16+ years old). Caregivers provided informed consent for their own participation. In total, local authority consent was provided for 2,951 young people. Of those, 1,064 young people (36%) were either not contactable due to incorrect contact details (10%) or were not eligible to participate (26%; e.g., were not in the age range). Of the remaining 1,872, 421 CEYP participated (equating to 22% of those contactable and eligible). In addition, adoptive parent-child dyads were recruited via adoption networks. Here, the parent provided informed consent and young person provided informed assent (or consent if 16+ years old).
Among the 809 young people (43%) who declined participation after contact, the main reasons were young people not being interested or they stated that it was not a good time. Following receipt of consent/assent, young people and their caregiver completed questionnaires. These were either completed online via RedCap (online software), via post, over the telephone, or during an in-person home visit.
Measures
All measures were completed by young people and their caregiver, unless specified.
Internalising and externalising difficulties
The 25-item Strengths and Difficulties Questionnaire (SDQ; Goodman et al., 2001) consists of two subscales each of 10 items, which measure internalising (emotion and peer problems) and externalising difficulties (conduct and hyperactivity problems). The five-item subscale for prosocial skills is not reported here. Each item is rated on a zero (not true) to 2 (certainly true) scale. Scores on each subscale are summed to give total internalising and externalising difficulties scores from 0-20, with higher scores indicative of a higher level of symptoms. Total difficulties scores are the sum of the internalising and externalising subscales, giving possible values from 0-40. Cronbach’s alpha for SDQ total difficulties was .83 (10-13-year-olds) and .86 (16-17-year-olds). The SDQ uses a four-category system to categorise internalising, externalising and total difficulty severity (close to average, slightly raised, high, very high).
Anxiety and depression symptoms
The Revised Child Anxiety and Depression Scale (RCADS-25; Ebesutani et al., 2017) is a 25-item self-report questionnaire, assessing anxiety and depression symptoms. The measure contains 15-items measuring anxiety symptoms (total score range = 0–45); and 10-items measuring depression symptoms (total score range = 0–30). The items are summed to give total anxiety and depression symptoms from 0-75. Each item is rated from zero (Never) to 3 (Always) with higher scores indicating higher levels of anxiety and/or depression symptoms. Cronbach’s alpha for RCADS total scores was .92 (10-13-year-olds) and .95 (16-17-year-olds). Scores can be transformed into sex and age adjusted t-scores and compared to clinical cut-offs based on normative datasets. These cut-offs are used to create a categorical variable with three groups: normal, at the borderline clinical threshold, and above the clinical threshold.
Post-traumatic stress disorder symptoms (PTSD)
The 8-item Child Revised Impact of Events Scale (CRIES-8; Perrin et al., 2005) was used to assess young people's PTSD symptomology. Items are scored on a four-point scale (0 = not at all; 1 = rarely; 3 = sometimes; 5 = often) and summed to give a total score, with scores of 17 and above indicating possible PTSD. Cronbach’s alpha for total CRIES scores was .85 (10-13-year-olds) and .88 (16-17-year-olds). A dichotomous variable was also created with scores 17 and above in the ‘above threshold’ group. The measure has good psychometric properties (Deeba et al., 2014; Verlinden et al., 2014).
Subjective wellbeing
The 14-item self-report Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS; Tennant et al., 2007) was used to assess subjective wellbeing, including affective-emotional aspects, cognitive aspects, and psychological functioning for individuals. Items are scored on a Likert scale from 1 (none of the time) to 5 (all of the time). Total scores range between 14 and 70, with higher scores representing higher levels of wellbeing. The scale has been reported to be valid and reliable across a range of child and adolescent populations in the UK (Clarke et al., 2011; Tennant et al., 2007). Cronbach’s alpha for total subjective wellbeing scores was .87 (10-13-year-olds) and .90 (16-17-year-olds). Scores can be divided into high, average and low wellbeing using cut points at plus or minus one standard deviation based on general population samples (Tennant et al., 2007). These categories are derived from the top 15% of scores (scores of 60–70; high wellbeing) and bottom 15% of scores (scores of 14–42; poor wellbeing) from UK population normed data (Stewart-Brown & Janmohamed, 2008).
School satisfaction
The School Satisfaction Scale (SSS; Huebner et al., 2001) is an 8-item school subscale of the 40-item self-report Multidimensional Students’ Life Satisfaction Scale (Huebner, 1994). The SSS measures student life satisfaction across five key domains. Items are scored on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). Items are summed to give total scores; higher scores indicate higher levels of school satisfaction. Cronbach’s alpha was .75. School satisfaction was not measured in the older age group (16–17 years old) because many would have been in learning environments other than secondary schools (e.g. Further Education Colleges).
Caregiver reported health-related quality of life
Health-related quality of life was reported by carers/parents using the KINDL-R Questionnaire (KINDL; Ravens-Sieberer & Bullinger, 1998). The questionnaire consists of 24-items across six dimensions: physical wellbeing, emotional wellbeing, self-esteem, family, social contacts, and school. Items are scored on a 5-point scale ranging from 1 (never) to 5 (all the time), with higher scores indicating better quality of life. The six dimensions form six subscales with four items each. The ‘family’ subscale refers to the home the young person was living in. Cronbach’s alpha for total KINDL scores was .75 (subscales α = .65 to .88). The KINDL does not have clinical cut-off scores based on normative population data.
Demographics
Age, gender, and ethnicity were self-reported by both age groups. Age was measured in years; options for gender identity included boy, girl, non-binary, and prefer not to say, with a free report option if the above options did not apply. Of note, whilst only a few young people chose 'prefer not to say', many of these participants identified as gender nonconforming in the free-report text. For statistical analyses, given the small number of non-binary or ‘prefer not to say' responses (see Table 1), gender was categorised as boy (coded as 0) and girl, non-binary, or preferred not to say (coded as 1, hereon referred to as girls and non-binary for brevity). As a sensitivity check, we re-ran the analysis coded only as boys (0) and girls (1) (which excluded participants not in these categories), and there was no difference in the results. Ethnicity was collected from the following categories: White, Black, Mixed, Asian, Other. For statistical analysis, given the small number of Black, Mixed, Asian and ‘Other Ethnicity' young people, this was collapsed into White (coded as 0) and non-White (coded as 1).
Service level factor
Placement type was recorded as where young people were living at the time the measures were completed. Placements included non-biological foster carer, kinship foster care, residential care, semi-independent accommodation, independent accommodation, other accommodation, and adoption. For analysis, this was collapsed into (0) “family-based care” (foster, kinship, adoption), and (1) “non-family based care” (e.g., residential, semi-independent).
Data analytic plan
Data were analysed using SPSS v25. Our primary aims were to explore (1) the mental health and wellbeing profiles of care-experienced young people during early and late adolescence, (2) to explore associations between mental health and wellbeing outcomes, and (3) to understand whether demographic and service level factors predicted mental health and wellbeing outcomes in these groups. In both age groups, self-reported anxiety and depression symptoms were positively skewed so square root transformations were applied. Among the 10–13-year-olds, carer-reported child physical wellbeing was negatively skewed, so an inverse transformation was applied. We then used bivariate correlational analyses to understand the basic associations between the mental health and wellbeing outcome variables in each age group. Despite transformation, carer-reported child physical wellbeing remained skewed. Associations were checked using non-parametric tests (Spearman’s rho), with discrepancies noted (see Table 3). Fisher r-to-z transformations were conducted to assess differences in correlation effect sizes.
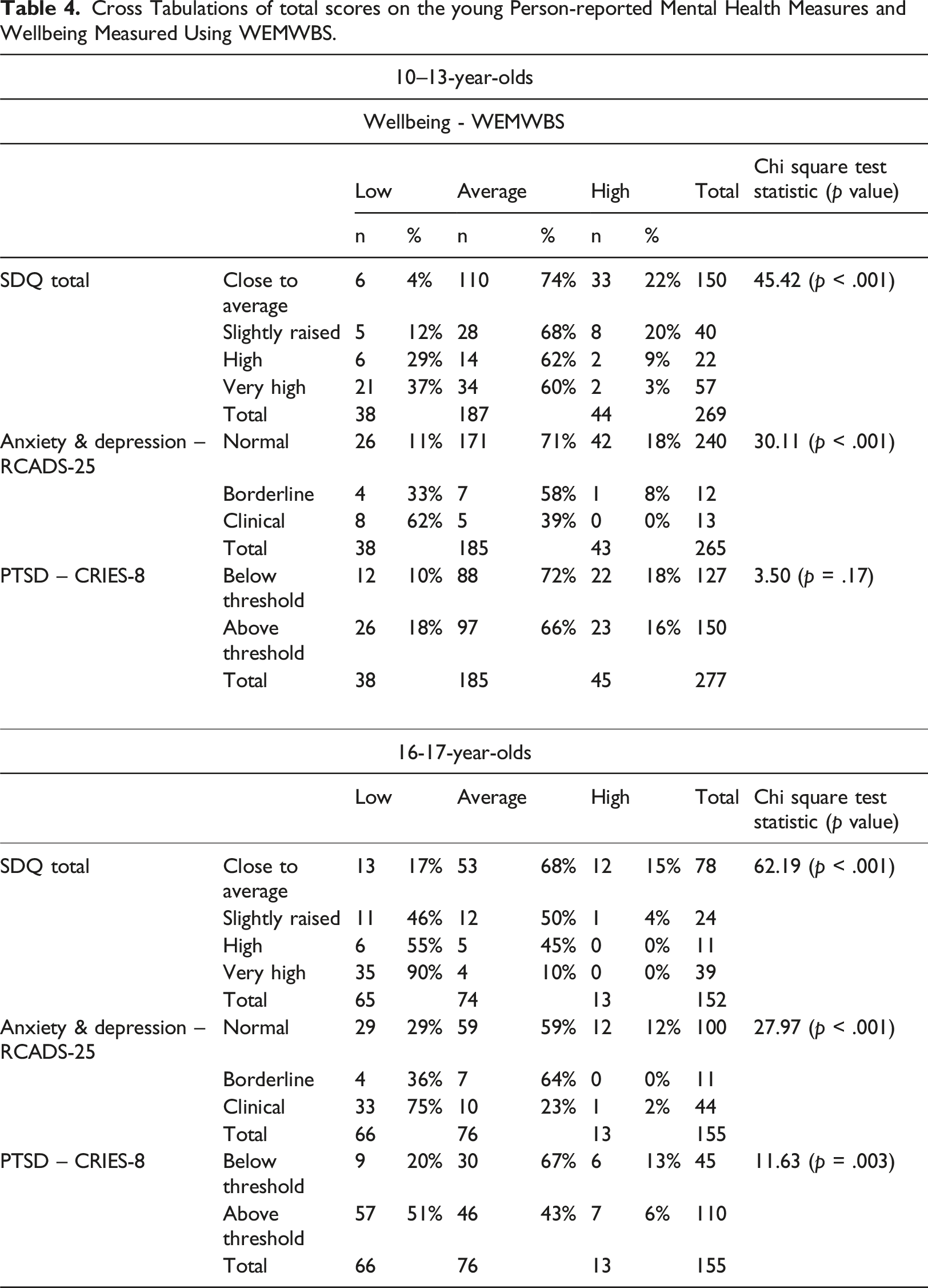
Chi-square tests were used to explore whether high mental ill-health (defined as scoring above established clinical-threshold on the CRIES-8, RCADS-25, SDQ; see Methods) was associated with the poorest wellbeing (defined as the lowest 15% of WEMWBS scores, from nationally normed data (see Measures). This analysis sought to more robustly explore whether poor mental health and poor wellbeing could be considered similar in CEYP, given implications for service delivery.
Finally, we were interested in whether demographic features (age, gender, ethnicity) and service-level (placement type) variables were associated with outcomes. For the 10–13 year olds, placement type was ultimately not included as the vast majority were in a family-based placement (see Table 1). For the 16-17 year-olds, age was not included, as these data were only available as a whole year (i.e., either 16 or 17). First, we used bivariate and point biserial correlations to explore basic associations between the predictors and symptom severity, focused on child-reported outcomes (SDQ, RCADS, CRIES-8, WEMWBS scores). Where associations were significant (p < .05), we conducted linear regressions to explore the strongest predictors of mental health and wellbeing. The largest group was treated as the reference group (see Measures) for the binary demographic variables.
Results
Descriptive statistics
Among the 10–13-year-olds, 54% were male and 78% were White. Three-quarters (75%) were in foster care, with a mean current placement length (if in care) of 4.2 years (range 0–12.9 years). Among the 16-17-year-olds, 39% were male, 70% were White, and 55% were in foster care (mean current placement length = 6.3 years; range 0–16.9 years). Full sample descriptive data are reported in Table 1.
Mental health characteristics of CEYP
Mental Health and Wellbeing Outcome descriptive Statistics.
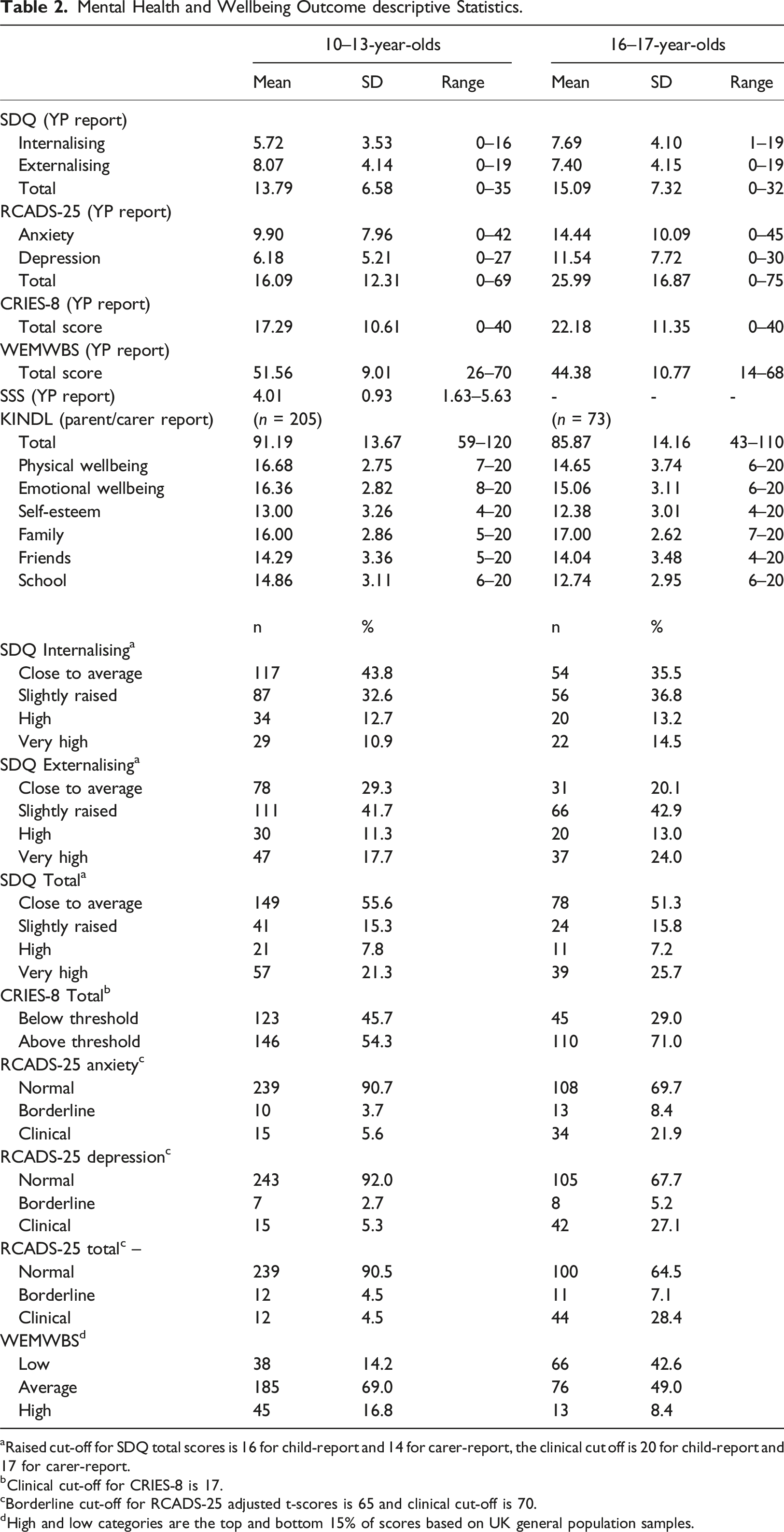
aRaised cut-off for SDQ total scores is 16 for child-report and 14 for carer-report, the clinical cut off is 20 for child-report and 17 for carer-report.
bClinical cut-off for CRIES-8 is 17.
cBorderline cut-off for RCADS-25 adjusted t-scores is 65 and clinical cut-off is 70.
dHigh and low categories are the top and bottom 15% of scores based on UK general population samples.
Associations between mental health symptoms and wellbeing
Mental health and wellbeing scores were moderately negatively correlated in both age groups, with higher mental health difficulties associated with lower wellbeing scores. The exception to this was PTSD symptoms (discussed below).
10–13-year-old CEYP
Pearson Bivariate Correlations Between Mental Health and Wellbeing Measures for 10–13-Year-olds and 16–17-Year-olds.
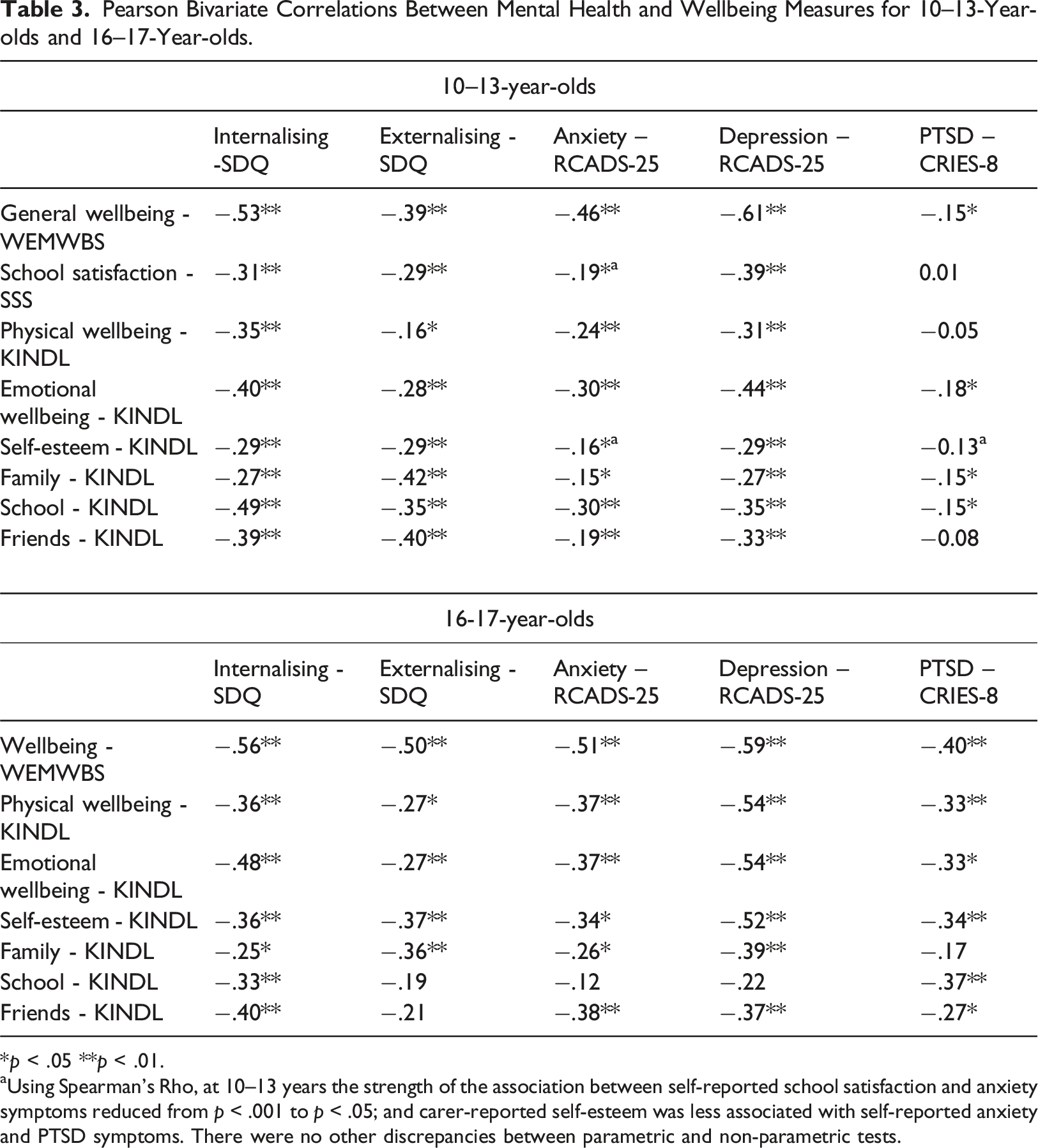
*p < .05 **p < .01.
aUsing Spearman’s Rho, at 10–13 years the strength of the association between self-reported school satisfaction and anxiety symptoms reduced from p < .001 to p < .05; and carer-reported self-esteem was less associated with self-reported anxiety and PTSD symptoms. There were no other discrepancies between parametric and non-parametric tests.
16-17-Year-old CEYP
For the older sample, there were moderate to strong negative correlations between subjective wellbeing and every mental health measure (r = −.40 to −.59), indicating that higher mental health symptom scores were associated with lower general wellbeing scores (Table 3 and supplemental material). From the caregiver report of wellbeing (n = 72), young person-reported mental health symptoms were significantly correlated (small to medium effects) with carer-reported ‘family relationships’, school, and friendship wellbeing, although these aspects of wellbeing were not consistently associated with all mental health measures (see Table 3 and supplemental material).
Proportionate overlap between high mental ill health and low wellbeing
Cross Tabulations of total scores on the young Person-reported Mental Health Measures and Wellbeing Measured Using WEMWBS.
Demographic predictors of mental health and wellbeing
10-13 year old CEYP
The only demographic variable associated with mental health was gender. Point-biserial correlations indicated that identifying as a girl or non-binary was associated with higher levels of anxiety and depression symptoms (rpb = .13) compared to identifying as a boy (this finding remained when only comparing females and males). Alternatively, age was the only demographic variable associated with wellbeing, with older age associated with worse child-reported wellbeing scores (WEMWBS: r = −0.13). Ethnicity was not associated with outcomes (see supplementary materials for full results). As there was only evidence of single variables associated with outcomes, we did not run further regression analyses.
16–17-year-olds
Gender and ethnicity showed small but significant correlations with self-reported wellbeing, with young people identifying as a girl or non-binary reporting poorer wellbeing compared to boys (rpb = −.16) and non-White young people reporting better wellbeing (rpb = .18). Placement type was weakly correlated with all mental health outcomes but not wellbeing. CEYP in non-family style care reported higher internalising and externalising symptoms (rpb = .25), anxiety and depression (rpb = .22), and higher PTSD symptoms (rpb = .20). Gender was weakly associated with internalising and externalising difficulties (rpb = −.23) and anxiety and depression (rpb = .18), with girls and non-binary young people reporting higher mental health symptoms than boys.
In the regression models including gender, ethnicity and placement in a single step, gender remained a unique predictor of mental health symptoms but not wellbeing. Being a girl or non-binary was associated with higher reported internalising and externalising difficulties (β = 1.77, p = .03) and anxiety and depression (β = 0.24, p < .01) compared to boys. Ethnicity remained a unique predictor of both mental health and wellbeing, with non-White young people reporting fewer internalising and externalising difficulties (β = −0.18, p = .02) and higher reported wellbeing (β = 0.16, p = .04) compared to White young people. Placement type also remained a significant unique predictor of mental health only, with non-family based care associated with higher reporting of internalising and externalising difficulties (β = 0.25, p < .01), anxiety and depression (β = 0.22, p < .01) and PTSD symptoms (β = 0.20, p = .02).
Discussion
We aimed to characterise the mental health and wellbeing profiles of CEYP during early and late adolescence, explore associations between mental health and wellbeing outcomes, and examine whether demographic and service level factors predicted both mental health and wellbeing. We found high levels of mental ill-health and noticeably higher levels in later adolescence. Findings also provided nuanced insight into overlaps between mental health and wellbeing, but limited consistent evidence that demographic or placement factors were robustly associated with symptom scores.
There is a paucity of evidence on the mental health and wellbeing needs of CEYP in the UK, beyond the annually reported SDQ (DfE, 2022). What is available consistently shows increased mental ill-health and lower wellbeing of CEYP, compared to the general population (Ford et al., 2007; Wijedasa et al., 2022). Here, we provide further evidence for the disorder-specific symptom profiles and wellbeing needs of CEYP and demonstrate that need is greater in later adolescence. Self-reported wellbeing was particularly poor in our older sample, suggesting a faster trajectory of worsening wellbeing than might be expected in the general population of older teens (Clarke et al., 2011; Morey et al., 2016; Sadler et al., 2018). That is, 42% of the 16–17-year-olds scored themselves in a poor wellbeing range, which would be expected of only 15% of a normed population. These findings highlight the urgency of early mental health intervention and prevention approaches for CEYP to address mental health before it worsens, or to prevent difficulties developing in later adolescence.
There is growing evidence that CEYP face additional barriers to accessing best-evidenced mental health support in a timely manner (e.g., Hiller et al., 2021; McGuire et al., 2022; McGuire et al., 2024; Phillips et al., 2024). CEYP who are 16-17-year-old are often facing other complex challenges not faced by their non-care-experienced peers, whilst also navigating the transition into early adulthood – particularly uncertainty about their living situation and a dramatic change in support and services available as they ‘age-out’ of the care-system (Stein, 2019; Stubbs et al., 2023). Almost 40% of our older sample were in non-family style placements, such as residential care homes or semi-independent placements. Reasons for being in these types of placements can be complex and sometimes this is the right type of placement for the young person’s needs (Cameron-Mathiassen et al., 2022; Holmes et al., 2018). However, these types of placements were associated with worse mental health and wellbeing in 16-17-year-olds. This likely reflects a cycle of worsening mental health, placement breakdowns, and a move to non-family care, which is widely highlighted in the literature on CEYP (Konijn et al., 2019; Maguire et al., 2024), further reflecting the urgency of high-quality, timely mental health care for CEYP. Our findings show that demographic factors are generally not reliable markers of mental health and wellbeing outcomes. For the younger sample (10-13-year-olds), being older and identifying as a girl were associated with slightly worse reported mental health, although not on all measures. For the older sample, being a girl and being White were both associated with slightly worse reported mental health, although not on all measures.
A key focus of our work was understanding the overlap between mental health and wellbeing. We explored this to understand the relevance of current theories on mental health and wellbeing for CEYP, but also because increasingly research suggests that services (particularly children’s social care) consider these concepts to be relatively unique, with implications for service development (e.g., developing wellbeing services that do not provide direct mental health support; McGuire et al., 2024). There is mounting evidence in the general population that mental health and wellbeing are separate but related constructs (Kinderman et al., 2015; Patalay & Fitzsimons, 2016). Our findings also show that mental health symptoms and wellbeing of CEYP are separate but related constructs, in line with the dual continua model (Keyes, 2005). This held true for self-report and for carer-report on multiple aspects of child wellbeing. However, there were some differences by age group. For the younger sample, while mental health and wellbeing were correlated (except for PTSD symptoms) many young people reporting clinically elevated mental ill-health self-reported average wellbeing (although few reported ‘good’ wellbeing). By late adolescence, this was much rarer and there was a stronger overlap between these constructs (e.g., among those who scored in the clinical range for anxiety and depression, 75% also rated their wellbeing as poor). This suggests that the overlap between mental health and wellbeing sits within a developmental context, reflecting an interplay between biological changes, psychological factors (e.g., worsening mental health corroding wellbeing), social pressures that can characterise adolescence (Cilar Budler & Stiglic, 2023; Goldbeck et al., 2007; Patalay & Fitzsimons, 2018; Yoon et al., 2023), and pressures unique to older adolescence in care or with care-experience (previously highlighted). Findings emphasise the need to consider CEYP’s needs holistically, including mental health and wellbeing together. Furthermore, there is a window where CEYP might be able to maintain relatively good wellbeing, which diminishes as they approach later adolescence.
Strengths and limitations
There are few primary research projects on CEYP, and even fewer including self-report on mental health and wellbeing (usually mental health is reported by caregivers or social workers). This means we have comparatively little information on their mental health needs, compared to other populations of youth. Despite the many complex challenges of recruiting this population, it is crucial that we develop a stronger evidence-base of needs to support service decision-making. Nevertheless, findings should be considered in light of limitations. Most of the sample were recruited via local authorities, which requires complex consenting procedures. Only 22% of potentially eligible young people ultimately participated. Thus, we cannot guarantee that this is a fully representative sample of CEYP, although SDQ scores are comparable to national data published by the Department for Education (with approximately 40% scoring in the borderline or high range). Caregiver report was only available for 46% (n = 72) of the older sample, reflecting that many young people perceived that there was not a trusted adult who they wanted reporting on their mental health. Next, we have used standardised screening tools not diagnostic tools so we cannot say whether or not a child met full diagnostic criteria (although this was not our research aim). We also used clinical cut-offs that have predominantly been developed on non-CEYP populations. The CRIES-8 PTSD screening tool has a cut-off only validated with children who have experienced one-off traumas, but available literature suggests a lower (not higher) cut-off might be more appropriate for CEYP (Tarren-Sweeney, 2019). Additionally, the WEMWBS cut-offs are based on total general population norms, not young people specifically, and therefore should be interpreted with some caution. Nevertheless, our mean WEMWBS scores were similar to other studies with adolescents, albeit lower for the older age group (Clarke et al., 2011; Morey et al., 2016). Finally, we intentionally reported on the samples separately as we wanted to understand mental health during key transition periods (i.e., primary and early secondary school; emerging adulthood). This has provided interesting information on the different levels of needs and circumstances (e.g., placements) experienced by these two age ranges. However, we have not statistically compared these samples. These two smaller samples also meant that we were unable to explore ethnicity in a more meaningful way than collapsing into a binary (White vs. non-White) variable. Future research should aim to collect sufficient numbers of participants from ethnic minorities to enable a more nuanced analysis.
Conclusion
We found high levels of disorder-specific mental health symptomology in CEYP. By exploring this in two distinct age ranges, we demonstrated the importance of early intervention or prevention, with a strong contrast apparent between the age groups. Almost three-quarters of 16–17-year-olds reported clinically high PTSD symptoms, and almost half of 16-17-year-old CEYP reported poor wellbeing. We also found moderate overlap between mental health and wellbeing, with these constructs particularly aligned by 16-years-old. Our findings highlight the urgent need for high quality support for the mental health and wellbeing of CEYP, so all CEYP can thrive as they move through adolescence and into adulthood.
Supplemental Material
Supplemental Material - The mental health and wellbeing of care-experienced young people during early and later adolescence
Supplemental Material for The mental health and wellbeing of care-experienced young people during early and later adolescence by Bethan Carter, Katherine H Shelton, Lisa J Holmes, Eva A Sprecher, Maryam Javed, John McLeod, Jeongeun Park, Julie Selwyn, Iram Siraj, Charlotte Robinson and Rachel M Hiller in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgments
We would like to acknowledge the contributions of all children, young people, caregivers, social workers, local authorities, and adoption agencies who participated in the ReThink study without whom this research would not have been possible. We would also like to thank the care-experienced advisory boards who have guided this research and the third sector organisation partners on this project, CoramVoice and Adoption UK.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the The ReThink Programme was funded by the UKRI (MRC) awarded to RH and LH (MR/W002132/1).
Ethical statement
Data availability statement
Analytic code, data and research materials are available on request to the corresponding author. Data presented here are, in part, baseline data from an ongoing longitudinal project (pre-registered) and will be available via UK Data Service at the conclusion of the full project
Supplemental Material
Supplemental material for this article is available online.
Appendix
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.