
Abstract
Children with congenital heart disease are more likely to receive special educational services in schools and have an increased risk of mental health issues. We explored the lived experiences of parents caring for a child with heart disease and concurrent mental health issues in Denmark. Semi-structured interviews with ten parents (age 39–57 years) to these children (age 5–17 years) were analysed using interpretative phenomenological analysis. Three Group Experiential Themes (GETs) were generated from the analysis: The first GET, Parental roles and caring behaviours, described parental struggles of fulfilling their parenting role ideals and experiences with stigmatization of MHI. GET two, Parental reflections on their illness explanations, portrayed how parents utilize different illness explanations to make sense of their child’s MHI. GET three, Differences in access to help and support, captured how the CHD affected overall access to mental health support. The results may inform various topics of importance for health professionals to address in their clinical encounters with these families.
Plain Language Summary
Congenital heart disease is the most common congenital condition, affecting approximately 1% of newborns. Parents of these children often experience substantial psychological distress due to the fear of losing their child, the burden of hospital stays and surgeries, and concerns about their child’s future health. Additionally, children with congenital heart disease more often require special education services and face a higher risk of mental health issues. Parenting a child with mental health issues also presents specific challenges, as parents may find it hard to access proper help for their child, may feel stigmatised or have feelings of blame and guilt. We explored the lived experiences of parents raising a child with both heart disease and mental health issues in Denmark by interviewing ten parents (aged 39–57) of children (aged 5–17). Through qualitative analysis, we identified 3 themes of importance for these parents: (1) Parental roles and caring behaviours: Parents struggled with meeting their own parenting ideals and dealing with the stigma of mental health issues. (2) Parental reflections on their illness explanations: Understanding the child’s mental health issues was important. Parents often perceived a connection between their child’s heart disease and mental health issues, influenced by biological, psychological, or social factors. (3) Differences in access to help and support: Parents described how their child’s heart disease impacted their ability to obtain mental health support. Some felt that the heart disease delayed access to mental health support, while others leveraged the physical condition to secure mental health support. Overall, these findings might assist health professionals in providing better support to these families in clinical settings.
Keywords
Introduction
Congenital heart disease (CHD) affects approximately 0.8–1% of new-borns. The challenges of raising a child with a CHD are evident. Diagnosis and treatment may cause substantial parental psychological distress, as parents often endure prolonged hospitalisations with their child, worry about their child’s future health and fear losing them (Wei et al., 2015). At home, parents must acquire new ‘expert’ skills to properly attend to their child’s physical needs (Svensson et al., 2020). Accordingly, parenting a child with CHD has been described to comprise several everyday paradoxes like balancing vigilance and normality (Svensson et al., 2020). In addition, children with CHD are 50% more likely than their peers to receive special educational services in schools (Riehle-Colarusso et al., 2015). Especially, higher rates of cognitive disabilities, autism, attention deficit hyperactivity disorder (ADHD) and severe stress reactions have been reported (Lau-Jensen et al., 2023; Miles et al., 2023). Further, an increased risk of tic disorders, attachment disorders and eating disorders, respectively, in children with CHD compared to the general population have been suggested (Miles et al., 2023). Explanations for these increased risks are likely various and possibly include genetic factors, reduced foetal cerebral oxygenation, delayed brain maturation, structural brain abnormalities and injuries, operative complications, surgery-associated risk factors and psychosocial factors (Howell et al., 2019).
Parenting a child with mental health issues (MHI) often has adverse effects on the entire family, affecting siblings and straining parents’ relationship (Chan & Leung, 2020; Leitch et al., 2019). In addition, parents may grapple with comprehending or making sense of their child’s MHI and blame themselves for the problems their child is facing (Hasson-Ohayon et al., 2019). At the same time, parents play an important role in accessing mental health support for their children, which often includes navigating complex healthcare and educational systems (Laugesen & Groenkjaer, 2015).
Overall, literature suggests that raising a child with a CHD and concurrent MHI is likely a complex, demanding situation. However, studies exploring parents’ experiences of caring for a child with CHD and concurrent MHI are few and mainly focused on parental perceptions of child vulnerability. In some studies, parents of children with CHD were reported to downplay and normalise delayed child development (Lee & Rempel, 2011; Møyen Laane et al., 1997; Rempel et al., 2009), whereas other studies reported that the parents perceived their children as more vulnerable and noted more child behavioural and social difficulties (Oates et al., 1994; Vrijmoet-Wiersma et al., 2009).
The aim of this study was to explore the lived experiences of parents caring for a child with CHD and concurrent MHI. Such information may allow healthcare professionals to better understand these families' specific challenges and address those in clinical encounters.
Methods
Methodological approach
Interpretative phenomenological analysis (IPA), an inductive and idiographic approach, was applied in this study. It aims to explore the participant’s particular lived experiences in detail. Participants’ sense making is considered influenced by their context, that is the context of health care settings and societal stigmatization of MHI. The method further recognises that the investigator interprets not only the participants’ experiences, but also the participant’s own interpretations of these experiences (double hermeneutics) (J. Smith & Osborn, 2015). IPA is suitable for small sample sizes and exploration of topics that are ‘complex, ambiguous and emotionally laden’ (J. A. Smith & Osborn, 2015), characteristics that align with the nature of the current research.
Setting
The study was conducted at the Research Unit of the Department of Child and Adolescent Psychiatry, Aarhus University Hospital Psychiatry, Denmark and registered within the Open Science Framework (OSF) (https://doi.org/10.17605/OSF.IO/93NB6). The study formed part of the Mind the Heart research project, which aims to (1) explore the feasibility of using an online parent/child-completed assessment for common mental issues in children with CHD, and (2) develop a website on this subject targeted health professionals and families. In relation to the website development, end users were interviewed to identify website user needs and to explore parental lived experiences. The current study is based on the latter data.
Recruitment
Parents were recruited through (1) notifications on social media and in a Danish online magazine for parents to children with CHD, (2) a paediatric cardiology outpatient clinic and (3) professional networks. The main author (JLH) assessed parents by phone. The following inclusion criteria applied: (1) child age 0–17 years, (2) diagnosis of a CHD and (3) concurrent or prior MHI (as defined by parental perception of the child’s psychological, social and academic function). To increase recruitment, children with a non-structural heart disease diagnosed within their first living year were also included (to simplify, commonly referred to as CHD). Purposive sampling was applied, aiming for variation in child sex, age and subtype of CHD and MHI. In line with IPA principles, a small sample size was obtained, as the aim of the analysis was to give an in-depth and comprehensive understanding of the particular phenomenon of parenting a child with both CHD and MHI. Sample size adequacy was evaluated throughout the analytical process, guided by information power. During the stepwise analysis, attention was paid to primarily the richness of the individual accounts, and secondly to variations, similarities and differences between accounts (Malterud et al., 2016; Pietkiewicz & Smith, 2014; J. Smith & Osborn, 2015).
Data collection and analysis
Semi-structured interviews were conducted by JLH. The interview guide (see Supplemental 1) was developed by JLH with discussions and feedback from the entire research team. The guide was designed to explore (1) parental experiences of caring for a child with CHD and MHI; (2) parental understandings of their child’s MHI and their thoughts on any association between CHD and MHI and (3) how parents helped their child cope with MHI. A pilot interview was conducted, transcribed, read and reread and discussed by the entire research team. Subsequently, slight adjustments to the guide were made with added questions on how parents experienced seeking support for their child’s MHI. Questions were open-ended and neither leading nor value-loaded. JLH had no prior relation to the participants.
The interviews were conducted between May 2022 and December 2022 (duration: 59–94 minutes (mean: 77 minutes)) using online video technology. They were recorded and transcribed verbatim by JLH and two research assistants (ASDR and LENL) using a transcription guide. Interviews, transcriptions, and analyses were performed in the original language (Danish), and quotes were translated for publication. The interviews were analysed in a stepwise manner according to IPA principles (Smith & Nizza, 2022), assisted by Nvivo 12 (Nvivo Software, QSR International Pty Ltd, 2018). Each interview was analysed independently by main author JLH before moving on to the next. Firstly, the interviews were read several times for familiarization. Initial thoughts and ideas were noted and subsequently developed into experiential statements. Experimental statements with meaningful connections were clustered to form personal experiential themes. To verify that the analysis was systematic, supported by data and not confined to one perspective, the three first interviews were coded independently by JLH and DRH, who discussed their exploratory noting, initial thoughts on organisation of experiential statements and personal experiential themes before analysis proceeded to the next interviews. Finally, a cross case analysis identifying patterns across interviews was performed and group experiential themes (GETs) were generated through iterative discussions and agreed upon by the entire research group at meetings. The researchers paid attention to convergence and divergence within and across participants and diverging viewpoints between the researchers were discussed to enhance and broaden the analysis, drawing on principles of reflexive triangulation (Shenton, 2004).
JLH, DRH and CUR are female medical doctors, trained in child and adolescent psychiatry. JLH is a PhD-student, DRH is an associate professor experienced in qualitative research and IPA and CUR is a clinical professor. ASDR and LENL study Public Health Science at Aarhus University, Denmark, and both hold experience in transcribing interviews and the use of qualitative methodologies. As the research team counted researchers with experience in child and adolescent psychiatry, expert knowledge was ensured. Furthermore, researchers were mindful of preconceptions based on their professional backgrounds.
To ensure trustworthiness of the study as described by Shenton (Shenton, 2004), credibility of the analysis was enhanced through use of a well-established research method, thorough participant information and encouragement to be frank, iterative questioning and use of a reflective commentary.
Ethics
The study was conducted according to the guidelines of the Danish Research Ethics Committee (case no. 1-10-72-274-21) and approved by the Data Protection Agency at Aarhus University (journal no. 2016-051-000001, 2730). All participants received written and oral information and signed a written consent form prior to the interviews.
Findings
Participants
Participant characteristics and demographic details.
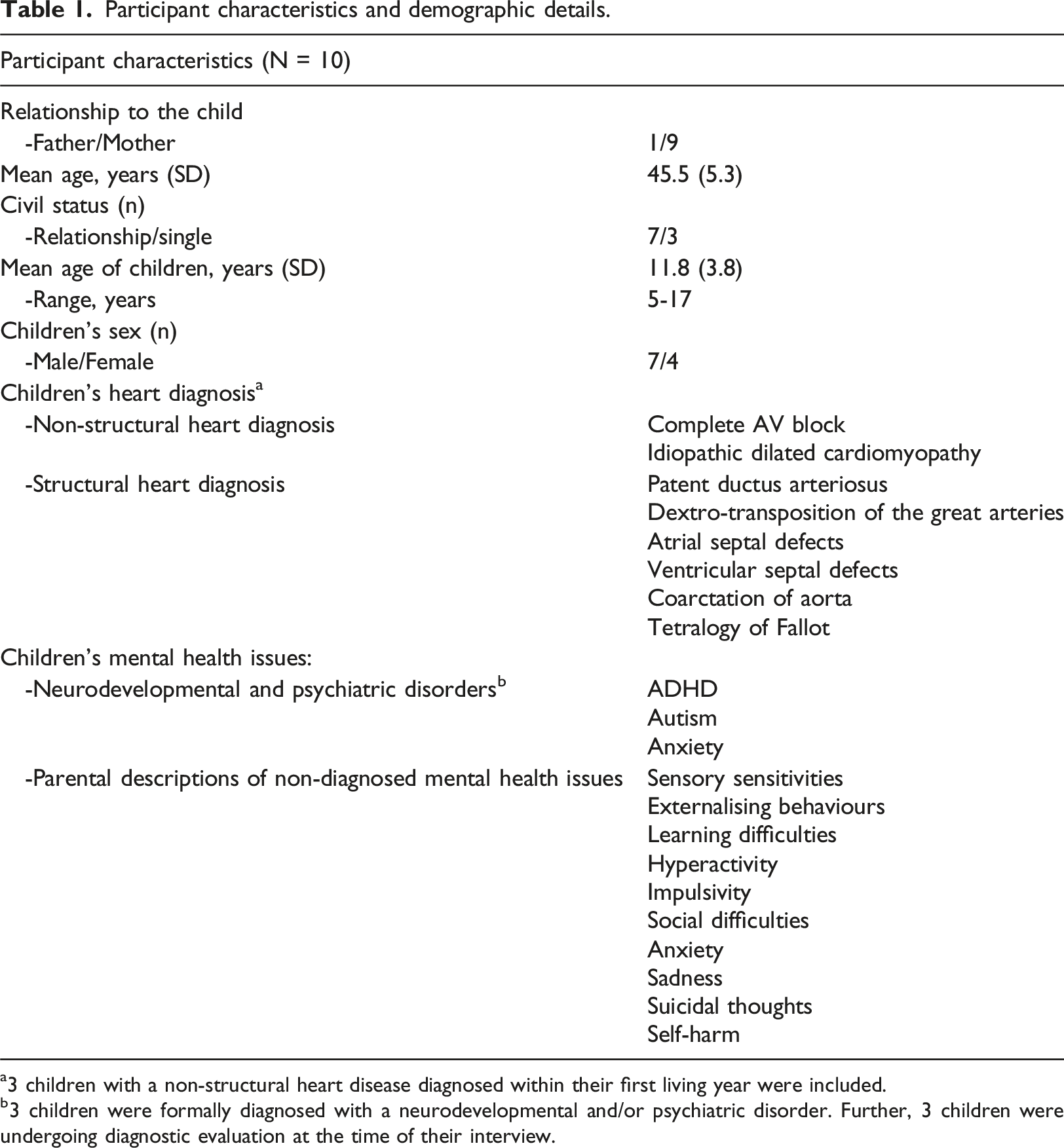
a3 children with a non-structural heart disease diagnosed within their first living year were included.
b3 children were formally diagnosed with a neurodevelopmental and/or psychiatric disorder. Further, 3 children were undergoing diagnostic evaluation at the time of their interview.
Themes
Three GETs were developed reflecting parental experiences of caring for a child with CHD and MHI (see Figure 1). The first GET, Parental roles and caring behaviours, described parental struggles of fulfilling their parenting role ideals and stigmatization of MHI. GET two, Parental reflections on their illness explanations, portrayed how parents utilize different illness explanations to make sense of their child’s MHI. GET three, Differences in access to help and support, demonstrated how the CHD in various ways affected parental help seeking behaviours and overall access to mental health support. All participants were pseudonymised with female pronouns to ensure their anonymity. Sentence truncation is marked by ellipsis. Summary of group experiential themes (white boxes) and Subthemes (grey boxes).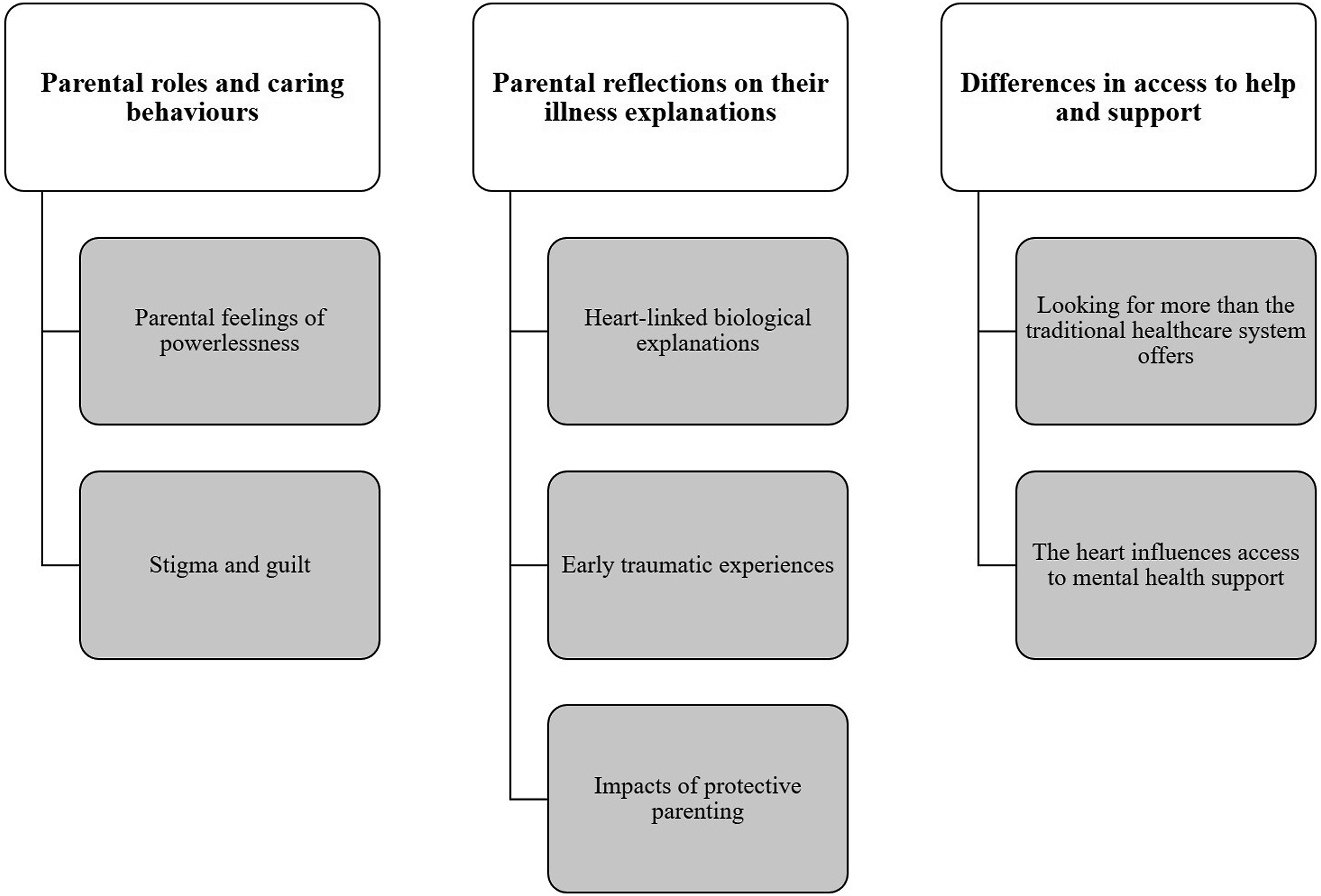
Parental roles and caring behaviours
Parental feelings of powerlessness
Laura, the mother of a child with severe depressive symptoms and self-harm, explained the difference between caring for her child’s CHD and MHI: “I would actually rather have …(cries) …that she was sicker with the heart compared to this [MHI]. Because that I can relate to. I can't understand this [MHI] … … The child needs [heart] medicine and we provide it for her. We do what we can… …Ehm, this stuff [MHI] is more difficult, because it is hard to do anything… … you feel more powerless. But my parental love is not a determinant for my child’s [physical] health... …My ability to, as a parent, to take control of medication and dosing periods is” (Laura).
For Laura, treating her child’s CHD was well defined and somehow out of her hands, thus not directly reflecting her parenting skills as she adhered strictly to the doctor’s directions. Thus, her capability to follow these instructions made her feel accomplished in her parental role caring for her child’s CHD. Doing well in caring for her child’s mental health was more difficult. Laura described difficulties with both understanding the MHI and further with concrete involvement in caring for the mental health problems. Caring for her child’s MHI was more intertwined with general parenting skills and even parental love than caring for CHD related needs. It was further perceived as more dependent on her ability to nurture and love her child, and thus left her with feelings of grief, incapability and powerlessness.
Stigma and guilt
Laura further speculated: “What on earth have we done for this to go so wrong?” (Laura).
Laura suffered from guilt and self-blame in relation to her child’s MHI, potentially reflecting an internalization of the stereotypical stigma of parents being responsible for their child’s MHI.
Henriette, mother of an adolescent with social difficulties and suicidal ideations, described how reading about MHI in other children with CHD changed her illness understandings: “Maybe, that it is not something I have inflicted on him in my upbringing, ehm, that maybe there is another reason”.
Henriette also suffered for internalized stigma and blame, however, learning about other children with similar conditions relieved Henriette from her fear of holding sole personal responsibility for her child’s development of MHI. She started acknowledging that several factors may contribute to MHI development.
Kristina, the mother of an adolescent diagnosed with autism, described: “Others consider it MUCH more important and MUCH more comprehensive to have been operated in your heart than to live with autism – ‘You just have to learn to live with it [the autism]’, really. Oppositely, I think we learn how to live with the heart, but we cannot learn to live with the autism in today’s society”.
Kristina found everyday life with her child’s autism more challenging than living with his CHD. In her view, societal expectations placed upon her and her child of finding a way to keep going despite the autism contradicted their own experiences and needs. The sentiment of ‘just learn to live with it’ for her implied that autism was more of a personal responsibility than CHD, ranking autism as somehow inferior to CHD.
Parental roles and caring behaviours were characterized by parental struggles with feelings of powerlessness in their need to fulfil their parenting role ideals when caring for their child’s MHI which they found more intangible. Caring for the MHI was perceived a personal responsibility with less support and guidance in comparison to caring for the CHD. Parents experienced both public- and self-stigma related to MHI, contradicting their need for support. However, acknowledging the existence of more than one contributing factor to MHI provided relief from guilt.
Parental reflections on their illness explanations
Heart-linked biological explanations
Maj, the parent of a child with anxiousness, reflected on potential explanations for her child’s MHI: “Maybe there are some neurological changes in the brain also, when something is wrong with the heart. Ehm, that is what I think. But yeah, how would I know”.
For this parent, CHD and MHI illness explanations were potentially intertwined and connected through biological factors, however, she felt uncertain and alone in her attempts to make sense of her child’s MHI. This biological explanation was in line with explanatory models of several parental accounts, further including for example neurological changes in the brain, brain damage or impaired oxygen delivery to the brain during labour, in early life or during open heart surgery, unknown side effects to heart medications or a genetic link between CHD and MHI.
Early traumatic experiences
Karen is the mother of a child with a complex CHD and two major cardiac surgeries within the first week of life. Karen recalls her own feelings of self-blame and powerlessness as she could not sufficiently comfort her child during this period. She reflected on the possible influences of these experiences on her sons anxiousness: “I think it is unavoidable, that it has an impact on a human to experience, or to a small child, to experience so much pain and lack of comfort in the beginning of life”.
Karen felt that her child must have been affected by the painful and traumatic early childhood experiences and separation from parents and that CHD thus influenced the development of MHI due to early psychological stress and trauma.
Impact of protective parenting
Karen further explained how her son developed anxiety in adolescence. She felt that her own traumatic experiences with her son’s heart disease and treatment, had influenced her to become a very protective mother guarding her son from any obstacle. In retrospect, she rationalised: “I think, at least that is my belief as it is right now, that it has contributed to him having this insecurity as to whether he is good enough and what he can do by himself.” (Karen).
Karen felt that her anxious parenting style contributed to her child’s development of anxiety as she believed that her behaviour prevented him from learning and growing through challenges.
Parental reflections on their mental illness explanations demonstrated how parents tried to make sense of their children’s' MHI. Such sense making was important for the parents and most of them wavered between utilising both biological and psychosocial illness explanations for the MHI. Some of the explanations entailed parental self-blame and guilt whereas others encompassed factors out of their control.
Differences in access to help and support
The heart influences access to mental health support
Kristina described how, prior to her son’s neurodevelopmental diagnosis of autism, health professionals continuously explained his motor, social and communicative disabilities as sequelae to his heart surgery: “I am pretty sure that my son would have had his psychiatric diagnosis, or his neurodevelopmental diagnosis sooner than he did because his heart definitely interfered with everything I said”.
Kristina felt misunderstood in her concern for her child’s development because health professionals focused exclusively on CHD, thus rationalizing her child’s neurodevelopmental delays as being caused by CHD.
Mona, the mother of a child with social difficulties, explained how her child’s CHD stopped her from seeking mental health evaluation as she was once told that children with CHD might experience developmental delays: “We have probably given her more time, actually. Because, maybe I have thought, she would catch up”.
Mona rationalised her child’s MHI as expected in view of the CHD, resulting in hopes that the child would be able to improve over time, and therefore she did not seek help for her child’s behaviour and mental problems sooner.
Conversely, Maj, the mother of a young boy with anxiousness and regulatory difficulties, noted: “It has been easier for us to say: ‘Lucas has a heart defect……and that has caused these mental difficulties that we would like to get help for’. It is definitely a sort of clinical validation of an issue that they [teachers and school psychologist] understand”.
Maj reflected on using the CHD as an asset when seeking mental health support in schools, as she perceived that others were more likely to acknowledge MHI when the child also suffered from a CHD. In her experience, CHD was a more societal accepted condition than MHI, thus reflecting her experience of societal stigma and possibly also her own stigmatization of MHI.
Looking for more than the traditional healthcare system offers
Mie, the mother of a child with impulsive and hyperactive behaviour, noted: “I find it hard to believe that we can find a public family counsellor who specialises in helping children with traumatic experiences after heart surgery who also have ADHD symptoms”.
Mie found it difficult to reconcile the dualistic division of healthcare into mental and physical issues into her needs of a health care professional capable of encompassing both her child’s CHD and MHI.
Parents described employing trauma therapy, infant therapy, mental field therapy, body therapy and osteopathy to replace or supplement public health services. Such methods were described by the parents to consider, in a more holistic manner, the intertwined nature of early life CHD experiences and the child’s MHI.
Access to help and support described how the child’s CHD impacted parent’s decision-making about when and where to seek support for the child’s concurrent MHI. For some parents, the child’s CHD potentially delayed mental health evaluation and/or support due to normalisation of the MHI by both health providers as well as from parents. For others, it paved the way for such support as the CHD bypassed barriers related to stigmatization of the MHI. For some parents, navigating a highly specialised and dualistic healthcare system was challenging and lead them to seek alternative offers outside the established system.
Discussion
This study explored the lived experiences of parents caring for a child with CHD and concurrent MHI. Three GETs were generated: (1) “Parental roles and caring behaviours”: Parents struggled to fulfil their parenting role ideals and with stigma and self-blame in relation to their child’s MHI. However, for some, acknowledging that several factors could contribute to the MHI provided relief from guilt. (2) “Parental reflections on their illness explanations”: Being able to make sense of the child’s MHI was important, and parents’ understandings often contained some link between their child’s CHD and MHI, mediated by biological and psychosocial factors. (3) “Differences in access to help and support”: Having a CHD affected parental help seeking behaviours and access to mental health support and services. For some, CHD was perceived as closing doors and delaying support for MHI, whereas others actively used the physical condition to open doors to achieve mental health support. In general, parents wished for a more holistic approach to their children; one that went beyond what they felt was provided within the public healthcare system.
The child’s MHI induced parental feelings of inadequacy, whereas parents found themselves to be more capable of supporting their child’s CHD. Brosig et al. found that the majority of parents to children with severe CHD (without MHI) reported that learning to manage their child’s CHD made them feel better about themselves (Brosig et al., 2007). Conversely, parents in the present study perceived that their child’s MHI was more intangible than their child’s CHD. This made it harder for them to “learn to manage” their child’s MHI, which caused despair. Other studies have documented how parents to children with MHI (without CHD) tended to internalize stigma and blame themselves for causing and/or maintaining their child’s MHI through their parenting, thus not meeting their “good parent” ideal (Eaton et al., 2016; Lautenbach et al., 2012). Moses et al. found that parents attributing their child’s (without CHD) mental disorders to external non-self-factors tended to blame themselves less (Moses, 2010). In the present study, some parents described how learning about poor mental health in other children with CHD provided release from guilt. The dual presence of CHD alongside MHI possibly offered the parents a framework that eased their self-blame by linking MHI with the heart condition. Thus, one might speculate whether parents to children with a CHD and MHI with predominantly biological understandings of the MHI experienced self-blame to a lesser degree than parents who emphasized early traumatic experiences or perceived their own parenting behaviours as important contributors to MHI. In a review of qualitative evidence relating to children with ADHD (without CHD), Laugesen et al. correspondingly synthesised that parents attributing their child’s ADHD to their own parenting skills tended to self-blamed more than those who viewed ADHD as a medical disorder (Laugesen & Groenkjaer, 2015).
In this study, parents felt stigmatized regarding their child’s MHI. They noticed more attention on their child’s CHD but lacked empathy and support for the MHI from friends and family. This focus on CHD contradicted their experience, as the MHI had a greater impact on their daily lives than the more stable CHD. In line with this, Lautenbach et al. described how mothers who had a child with severe mental illness and an additional first-degree relative with a serious physical condition experienced a support system that seemed much more familiar, acceptant and attentive to somatic conditions than to mental illness (Lautenbach et al., 2012). Pattyn et al. found that internalized (self-) stigma reduced the perceived importance of medical care from i.e. psychiatrists, while perceived public stigma diminished the value placed on help from family and friends (Pattyn et al., 2014). In the present study, some parents utilised the CHD to access mental health support, as they found that the CHD increased the societal understanding and acceptance of the MHI, possibly reflecting not only their experience of societal stigma but also their own stigmatization of MHI. The parent thus potentially used the CHD to circumvent this stigmatization of MHI.
The parents’ explanations for their children’s MHI often involved self-blame, biological factors or stressful life events; a common perception among parents of children with severe mental illness (Hasson-Ohayon et al., 2019). However, it remains unknown whether parents to children with a physical illness and comorbid MHI have more complex illness understandings or, oppositely, are more prone to simplified monocausal understandings. In the present study, some parents rationalised the MHI by reference to the child’s CHD. In other studies, parents to children with CHD have been reported to normalise child behaviours and delays. Lee et al. described how parents to children with hypoplastic left heart syndrome downplayed their children’s developmental delays and expressed fewer concerns about these delays which they justified referring to the children’s severe CHD (Lee & Rempel, 2011). They tended to regard milestone achievements, however delayed, as reassurances of health, which might have discouraged them from seeking out early intervention (Rempel et al., 2009). Laane et al. speculated that parents to children with a CHD might be more likely to recalibrate expectations and accept disabilities as life experiences had changed their values (Møyen Laane et al., 1997). On the other hand, other studies have found that parents to children having undergone cardiac surgery reported more child behavioural and social difficulties than parents of healthy children, even though teachers did not correspondingly note more difficulties (Oates et al., 1994) and parents perceived their children as more vulnerable than parents to healthy children (Vrijmoet-Wiersma et al., 2009). Thus, parents to children with CHD might react with either an increased or decreased sensitivity to their child’s MHI, both of which may potentially impact their help-seeking behaviours. More knowledge about these mechanisms would help identify those parents for whom reassurance of health or more support might be helpful.
Most of the parents in the present study desired a more holistic approach to their children’s CHD and MHI and used complementary medicine alone or as a supplement to conventional mental health services. In line with this, Wang et al. found that one of the primary reasons for using complementary medicine in children with MHI (without CHD) was a desire for a more natural and holistic approach that treated “the cause and not just the symptoms” (Wang et al., 2018). Zisman et al. found that children with developmental disabilities, such as autism spectrum disorder, stuttering and learning disabilities, were more likely than typically developing children to use complementary medicine, and that the likelihood hereof increased when the child had a chronic medical condition (Zisman et al., 2020).
Overall, the identified GETs offer insights into the experiences of parents to children with a CHD and comorbid MHI. Specifically, the study reveals how parents try to make sense of their children’s' MHI and how they often feel that their support needs are not met by friends, family or the public health care system, potentially reflecting continuous internalized and societal stigmatization of MHI.
Strengths and limitations
Some limitations associated with our study population should be mentioned. The self-referred informants were a selected group of parents with a potential specific interest in the possible link between the heart and mind. Also, as mothers’ and fathers’ perspectives might differ, another potential limitation was that 9 out of 10 parents were mothers. The study also had several strengths. The sample showed variety with regard to predefined criteria: child sex, age and subtype of CHD and MHI, which in that way ensured the intended representation of parental perspectives. Additionally, the stepwise analytic process with several rounds of discussion meetings strengthened the selection of final GETs. The study was reported according to the Consolidated Criteria for Reporting Qualitative Research (COREQ) guideline for qualitative research and criteria were widely met (see Supplemental 2) (Tong et al., 2007).
Implications for practice
An improved understanding of parental lived experiences of caring for a child with a CHD and MHI may allow clinicians to validate these families’ situations, which might in turn strengthen the alliance and help families and clinicians address these children’s physical and mental health issues. In particular, the potential insecurity among the parents with regard to how to understand the child’s MHI may potentially impede help-seeking and thereby the provision of early support and is therefore an important point of attention.
Conclusion
Overall, this study offers new insights into parental experiences of caring for a child with CHD and comorbid MHI. It underscores the contrasting ways parents perceive their child’s CHD and MHI, thereby highlighting the importance of parental sense making of MHI and the benefits hereof, such as acceptance and alleviation of feelings of guilt. The study further illuminated a paradox in the perceived intensity of attention and support directed towards the child’s CHD and MHI from friends, family and the social and healthcare system, which may run counter to the parents’ needs. It further sheds light on the stigmatization that still exists around MHI. Lastly, the study demonstrated how the child’s CHD affected parental help seeking and potentially impacted the overall access to mental health support.
Supplemental Material
Supplemental Material - Linking heart and mind - lived experiences of parents to children with congenital heart disease and mental health issues
Supplemental Material for Linking heart and mind - lived experiences of parents to children with congenital heart disease and mental health issues Julie L Hejl, Ditte R Hulgaard, Anne Sofie D Rasmussen, Lærke Emilie N Larsen and Charlotte U Rask in Clinical Child Psychology and Psychiatry
Supplemental Material
Supplemental Material - Linking heart and mind - lived experiences of parents to children with congenital heart disease and mental health issues
Supplemental Material for Linking heart and mind - lived experiences of parents to children with congenital heart disease and mental health issues Julie L Hejl, Ditte R Hulgaard, Anne Sofie D Rasmussen, Lærke Emilie N Larsen and Charlotte U Rask in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgments
We want to show our gratitude to all the parents in this study. We further thank the staff at the paediatric cardiology clinic at Aarhus University Hospital. Furthermore, the authors thank Professor in Congenital Heart Diseases Vibeke Hjortdal for providing expert knowledge on CHD and assisting in the recruitment of participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project received funding from the Danish Heart Association and the Danish Heart Foundation’s local association Esbjerg/Fanø (20-R143-A9431-22160) and the Jasha Foundation (R. no. 2023-0288). The funding sources had no role in the study design, collection, analysis and interpretation of data; in the writing of the report; or the decision to submit the article for publication.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.