
Abstract
This study evaluated the effectiveness of a 3-session group intervention for parents who had received a diagnosis of autism for their child within the past month. The intervention group (N = 41) was compared to Treatment-as-Usual (N = 40): one meeting with a social worker after the diagnosis feedback meeting. Parental stress was evaluated in both groups within a week and then a month after the diagnosis. The findings indicate an increase in the experienced parental stress for the comparison group on all six indices, while in the intervention group there was an increase only on two indices. That is to say, the intervention reduced stress that occurred in the first month after the diagnosis. Further analyses revealed that parent satisfaction with the group intervention was the single most important variable in predicting stress reduction. We argue that parent support groups immediately after their child’s diagnosis are effective and important, and probably superior to a single post-diagnosis meeting.
Plain language summary
In this study, we looked at a program for parents whose child was recently diagnosed with autism. We compared a group of parents who went through a 3-session program with another group who had just one meeting with a social worker after getting the diagnosis. We checked how stressed these parents felt one week after the diagnosis and one month later. The results showed that the stress increased for the group with only one meeting, but for the group in the program, the stress increased only in a few areas. This means the program helped reduce stress in the first month after the diagnosis. We also found that parents who liked the group program were less stressed. This suggests that support groups for parents right after the diagnosis are helpful and important to reduce stress.
Introduction
Receiving a diagnosis of Autism Spectrum Disorder (ASD) is a major event in parents’ and families’ lives and often a cause of distress (Wayment et al., 2019). Parents experience a range of emotions while having to make important decisions regarding their child’s treatment plan (Pearson, 2017). In our clinic, we diagnose over 200 6–18-year-old children with autism each year. We find that one of our goals is to support the parents after they receive the diagnosis. We also wish to support and encourage parents and caregivers to embark on a treatment plan for their children and for themselves, but we find that parents often resist or hesitate, like one of the parents who asked the second author: “Why confuse the girl and flood her with therapies?”
In order to assist parents on this complicated journey, we started the post-ASD diagnosis group intervention that is the focus of the present study. The study explored the effectiveness of this intervention compared to Treatment-as-Usual, as well as factors that predict its effectiveness.
Parents’ experience of receiving their children’s diagnosis of ASD
Often experienced as a life changing event, a diagnosis of ASD for one’s child poses both practical and emotional challenges (Burton & Fox, 2022). The diagnosis entails a rearranging of the family structure, daily management, and requires support from psycho-social services, resources, and navigation of bureaucracy. Children with ASD have a pervasive impairment in reciprocal communication and in the ability to display emotions, engage and initiate social interaction, and are therefore dependent on high levels of caregiver support and mediation (Bonis, 2016). ASD diagnosis poses challenges to couples’ relationships, sibling relationships, and is correlated with higher incidence of negative health implications of primary caregivers (Masefield et al., 2020). Added to that are the financial implications of the child’s condition (Scott, 2010). Many children require additional services to those provided by the health and education systems, that bear high costs.
Emotional distress and stress are common for parents following ASD diagnosis (e.g., Crane et al., 2016). Parental stress has been found to be higher in parents to children with ASD than in parents whose children were diagnosed with other developmental disorders, and was found to be related to symptoms such as the child’s irritability, gastrointestinal problems and sleep difficulties (Valicenti-McDermott et al., 2015). Compared with other disorders, parents of children with ASD experienced more stress related to accessing a suitable educational placement (Ashworth et al., 2019). Difficult behaviors and symptoms associated with ASD are often the most challenging aspect of parenting a child with ASD, even more than communication and practical matters (Kissel & Nelson, 2016).
Navigating the behaviors and symptoms associated with ASD presents a profound challenge in parenting a child with ASD, with parents often reporting that these difficulties bother them more than the complexities of communication and practical matters (Kissel & Nelson, 2016). Nonetheless, this superficial distinction does not fully recognize the intricate interconnection between behavior and communication. In interventions with parents, it is important to clarify this interdependence to enhance understanding, acknowledging that addressing one aspect may inherently influence the other (Klinger et al., 2013).
Parents experience a range of emotions following their child’s ASD diagnosis. For example, Hutton and Caron (2005) reported that among families interviewed shortly after receiving their child’s ASD diagnosis, 52% felt relieved, 43% felt grief and loss, 29% reported feeling shock or surprise and 10% self-blame. Families are reported to need support in order to exhaust their rights and advocate for their children in the realms of public services and education, while managing emotional, familial and practical day-to-day matters (Banach et al., 2010). Oftentimes, parents feel highly burdened and overwhelmed around the time of the initial diagnosis, especially in the face of mental health recommendations of comprehensive treatment programs to be implemented immediately following diagnosis. The emotional difficulties include the taxing responsibilities, the abrupt disillusionment about life expectations for the diagnosed child (Gentles et al., 2020), and perceived stigma (Salleh et al., 2020).
Studies reflect the extent to which parenting a child with ASD can also lead to personal growth and cultivating a positive outlook despite the painful experience and challenges. This ability is dependent on both external and internal factors – especially social-emotional support and motivation for ascribing meaning to experience (Wayment et al., 2019).
Diagnosis after the age of 6
This study explores the experiences of parents with children aged 6–18 who are receiving their initial ASD diagnosis. Such diagnoses at this age often bring a mix of emotions, including frustration over past confusion and misdiagnosis, relief, and validation (Aggarwal & Angus, 2015). Late diagnoses are commonly associated with adjustment challenges during key life transitions. A broader study involving 455 children of various ages identified shared concerns among parents of children with ASD, with parents of school-age children expressing greater worries about mental health compared to parents of toddlers (Pfeiffer et al., 2021). Additionally, parents of school-age children are particularly focused on securing appropriate educational placements (Ashworth et al., 2019; Freudenstein et al., 2020; Gindi, 2019).
Interventions targeting parental stress
Previous interventions aimed at addressing parental stress and pragmatic challenges in the caring for their children following the diagnosis, focused on mitigating stress and promoting self-efficacy and advocacy skills (Leadbitter et al., 2022). Understanding the type of support parents require is vital to create targeted and well-suited interventions (Banach et al., 2010). In one investigation of the types of support sought by parents, it was discovered that 93% indicated they sought support from other families in their condition, and 80% sought support from professionals (Twoy et al., 2007). Guralnick and colleagues (2008) examined the effects of four types of support on reducing parent-related and child-related stress. Parent-related stress was defined as resulting from attributes of the parent, such as incompetency or depression. Child-related stress was associated with attributes of the child, such as moodiness or maladaptive behavior. The study found that among the types of support received by parents, only specific parenting support that addressed their own child’s needs (e.g., child-related) had an impact on both parent-related stress and child-related stress. General support from the community or from friends was not sufficient as a support factor in its own right.
The benefits of group settings
The importance of the group setting is related to the need for contact with other parents who share their experience, the possibility to learn from others, to create a supporting network and to bring up issues that would not have been considered otherwise (Lunsky et al., 2017). In one study of a post-diagnosis parent group, emphasis was placed on enabling parents’ exchange of ideas and experiences as well as mutual enrichment and support between the group members (Banach, 2010). Research suggests that frontline professionals and parents’ experience with them around the diagnostic process have an impact on parents’ attitudes and coping with other service provides later (Boshoff et al., 2018). Utilizing the group model as a first line support-intervention after diagnosis, can help mitigate negative effects and emotions, as well as establish trust and rapport with service figures that will later be generalized in other circumstances.
Focusing on self-efficacy, emotional sharing and processing, as well as coping strategies and tools in the group setting, help normalize experiences, and help parents focus on what they can do. It exposes them to both the possibilities and the challenges lying ahead. This helps also by reducing uncertainty, gaining a sense of control after feeling helpless during the diagnostic process, and can help form a sense of hope and meaning that can alleviate stress and inspire parents to a path of personal growth (Rutherford et al., 2019). This in turn can facilitate other beneficial effects for the child and their family, by supporting the cultivation of a stronger sense of familial closeness and unity and deepening the understanding of the child. Parents utilizing support groups were reported to have more adaptive coping strategies in comparison to parents that had never utilized them, or that had utilized them only in the past (Clifford & Minnes, 2013). The study found that accessibility and focus on participants’ needs were most crucial to group interventions for parents to children with ASD. Not all empirical examinations of group interventions for parents of children with ASD demonstrated effectiveness. In a study of a parent support group for fathers of children with ASD, the researchers found little to no improvement in measures of depression, optimism, marital satisfaction, and parenting stress despite the fathers’ validation of the experience as rewarding (Elfert & Mirenda, 2015).
Method
The intervention
The study focused on a 3-session post-ASD diagnosis group intervention for parents of 6–18-year-old children. Parents in this intervention were offered to proceed to a three-session group model based on co-facilitation by two experienced professionals including clinical psychologists and social workers. The group took place within a month after receiving the diagnosis. The purpose of the presented intervention was to acknowledge the child’s parents as the most vital and important resource in their child’s well-being. Parents are often the child’s case managers, advocates, and main support and attachment figures. Receiving the diagnosis was understood as a time of great strain that also demands them to focus on pragmatic issues, and to orchestrate and tailor the most suitable set of interventions for their child’s needs. The group was intended to supply parents with required professional knowledge and with pragmatic and emotional support specifically around their child’s diagnosis, and also to encourage them to further find the right supports for their children and for themselves.
The intervention follows previous research in the field with a combination of support and psychoeducation (Banach et al., 2010; Lunsky et al., 2017). The main novelty is that the groups were integral to the assessment process, and were offered immediately after receiving the diagnosis, so that no more than a month had passed from the diagnosis to the beginning of the group intervention. The three sessions were focused on processing and accepting the child’s diagnosis, and referring the parents and families to community and state services for further support. This short-term focused intervention did not refer to highly personal content due to its limited scope. However, following completion, parents were invited to proceed to a long-term group for a deeper, more personalized parental guidance and emotional processing. Furthermore, they were referred to designated therapies and services offered by the center.
The purpose of the study was to assess the effectiveness of the parent group in alleviating parental stress, and to understand the variables associated with better effectiveness.
The center where the study was conducted provides comprehensive assessments to 6–18-year-olds suspected of having ASD. It is a public multidisciplinary autism center that offers comprehensive evaluations and treatment facilities for 6–18-year-old children from across Israel. Over 3000 psychotherapy sessions and 200 assessments are performed in the center each year. When, at final feedback meeting with the diagnosticians, the children received a diagnosis of ASD, the parents were invited to either attend the post-ASD diagnosis group (intervention group) or a single session with a social worker (comparison group). The importance of participation in the group was underscored to them as a means to receive guidance and emotionally process the diagnosis. A group began on the first Monday of each month, and thus the group sessions took place within a month of receiving the diagnosis.
The three group sessions took place over three consecutive weeks. Each month, the parents of 2–4 children who were diagnosed accepted the invitation to participate in the group. Sometimes both parents attended and sometimes one of them, so that each group included 4–8 participants.
Procedure
Data used in this study includes groups conducted between 2019–2022. There were several cases where both parents came to the first session and later only one of them stayed to participate in the other two sessions. Only those parents who had fully participated in the entire process, had given their consent to participate in the study, and had completed all the questionnaires were entered into the study. After receiving approval from the hospital’s institutional review board (0420-19-TLV), the invitation to participate in the group was delivered via phone call, along with a non-binding invitation to participate in the study voluntarily. Parents who agreed to participate in the study were invited to arrive 30 minutes before each session to complete the study questionnaires. Members of the same couple completed the questionnaire separately. Parents’ participation was anonymous, and was coded by the 3 last digits of their ID number without using their names. Each session lasted for one and a half hours and included the following contents:
Session I
The first session included a presentation of the group’s purpose: the importance of talking and processing emotional responses regarding the diagnosis and parents’ role in the care of their child. Furthermore, facilitators presented and elaborated about the rights and services available to parents and families, and the actions and attitudes required to exhaust them. Parents were encouraged to share thoughts, emotions, and questions openly. This session was usually characterized by strong emotional responses and feelings such as despair, confusion, and uncertainty about their and their child’s future. Also, anger and frustration towards professionals and about lost years without the right diagnosis arose, as well as, in some cases, a sense of relief.
Session II
The second session started with discussions about personal questions that had come up during the week. Afterwards, an overview of current methods and approaches to ASD treatment was presented. This part included a description of the various therapies offered and their goals (speech therapy, occupational therapy, individual and group therapy, parent counseling). The changes that may be anticipated in the therapeutic interventions were described as well as the importance of cooperation and integration between the different therapeutic approaches and disciplines and the educational teams. The importance of creating a continuum between educational, community and therapeutic support was stressed along with an accentuation of the role of parent counseling across the life cycle.
Session III
The third and final session started with notes and questions from the past week. The main topic discussed in this session was family dynamics: the dynamics between siblings, the difficulties that the neurotypical siblings endure and witness, the relationship with extended family, and more. This session also involved disclosure of the diagnosis to the children and later to other circles. This topic usually brought forth a discussion between the parents that highlighted the tension between the fear of label or stigma, and the need for open discussion and advocacy, for them to receive the maximum benefits of care and services. The last part of the session was devoted to feedback about aspects of the intervention that were helpful and parts that were missing. Parents were also given a choice to continue in a weekly parent’s group conducted by a senior psychologist.
Sample recruitment
The researchers are placed in an autism clinic for 6–18-year-old children in the center of Israel. Each month, the center receives around 100 referrals for individuals who may have ASD, and conducts approximately 220 assessments a year of which 30% are diagnosed with ASD. All parents who received a diagnosis of autism during the years 2018–2022 were approached to participate in the study. They were given a choice of support following the diagnosis: the parents who attended the group and agreed to participate in the study formed the intervention group, while the parents who met a social worker and agreed to participate in the study formed the comparison group.
Design
Parents who were in the process of diagnosis and agreed to participate received questionnaire #1 that surveys demographic factors, and assesses their motivation to receive parents’ counseling, and stress levels. Following the diagnostic summary meeting, parents received questionnaire #2 – to assess their satisfaction with the diagnostic process and their motivation to receive parent counseling. In each session, parents completed questionnaires to assess their satisfaction following the first and second group sessions.
Following the last group session, parents completed a questionnaire to assess their motivation for therapy and parent counseling, and their stress levels.
The comparison group participants also completed questionnaires #1 and #2 in the same way. After a month, they were contacted again and asked to complete a questionnaire about their motivation for therapy and parent counseling, and their stress levels.
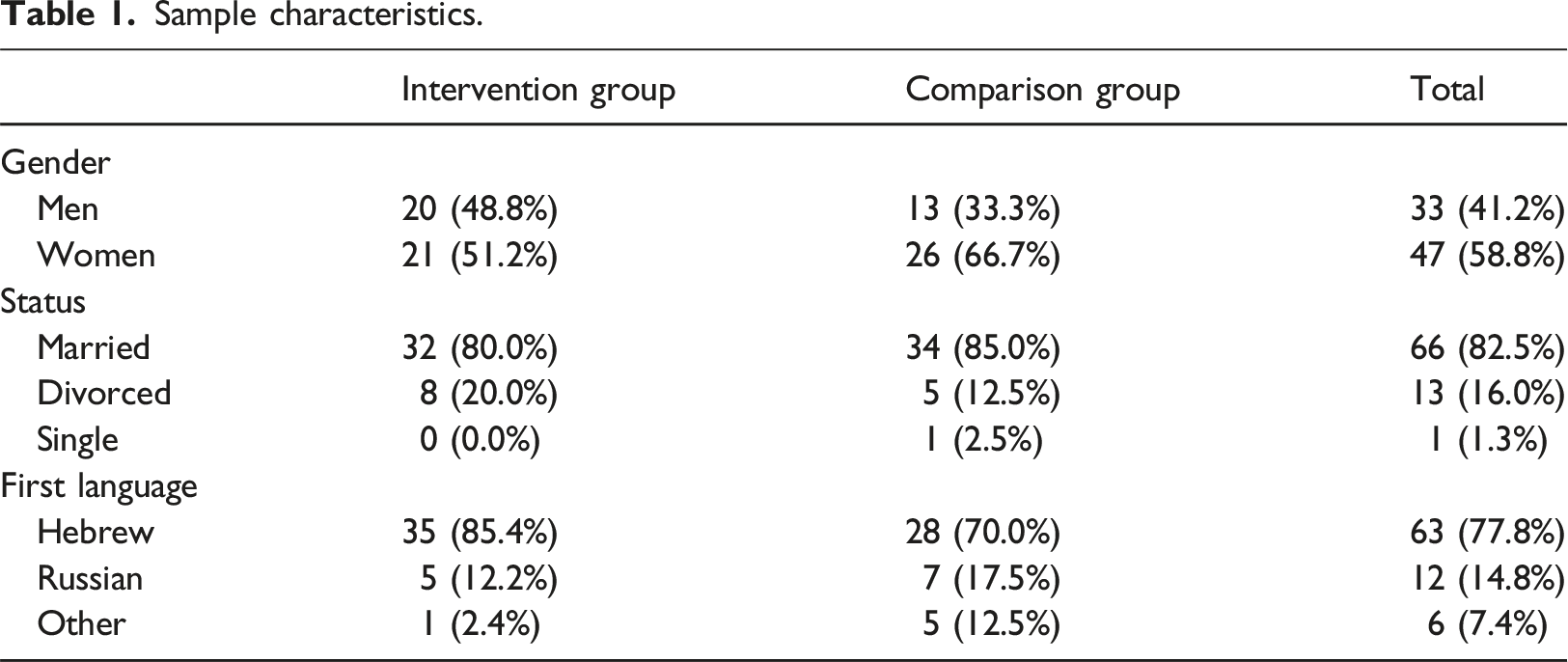
Participants
Sample characteristics.
Measures
The purpose of the present study was to examine the effectiveness of the post-ASD diagnosis group for parents to children diagnosed with ASD. It was hypothesized that the level of stress would decrease following the intervention, compared with the comparison group. The hypothesis was examined with regard to the components of the PSI.
Results
Reliability
Reliability of the different indices.
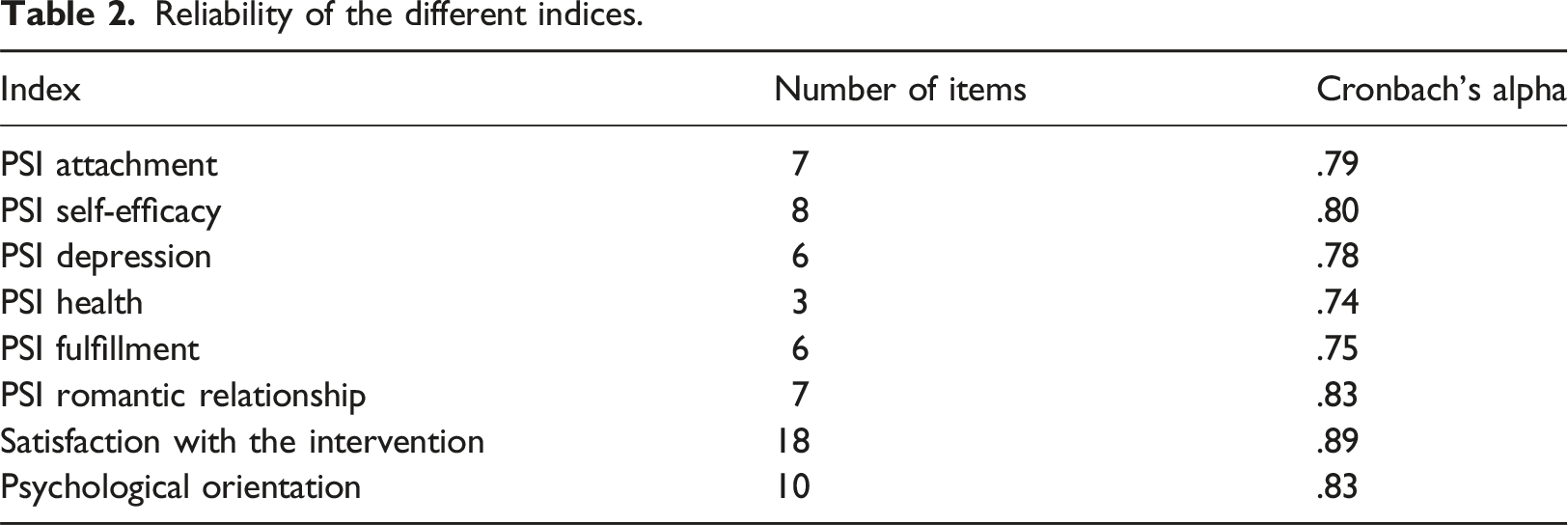
All the values indicate a satisfactory level of reliability. The measure of each index was computed by averaging the responses of the items included in the index.
Effectiveness of the intervention
Descriptive statistics of intervention and comparison group pre- and post-intervention with the results of the 2 × 2 ANOVAS and estimates of effect size.
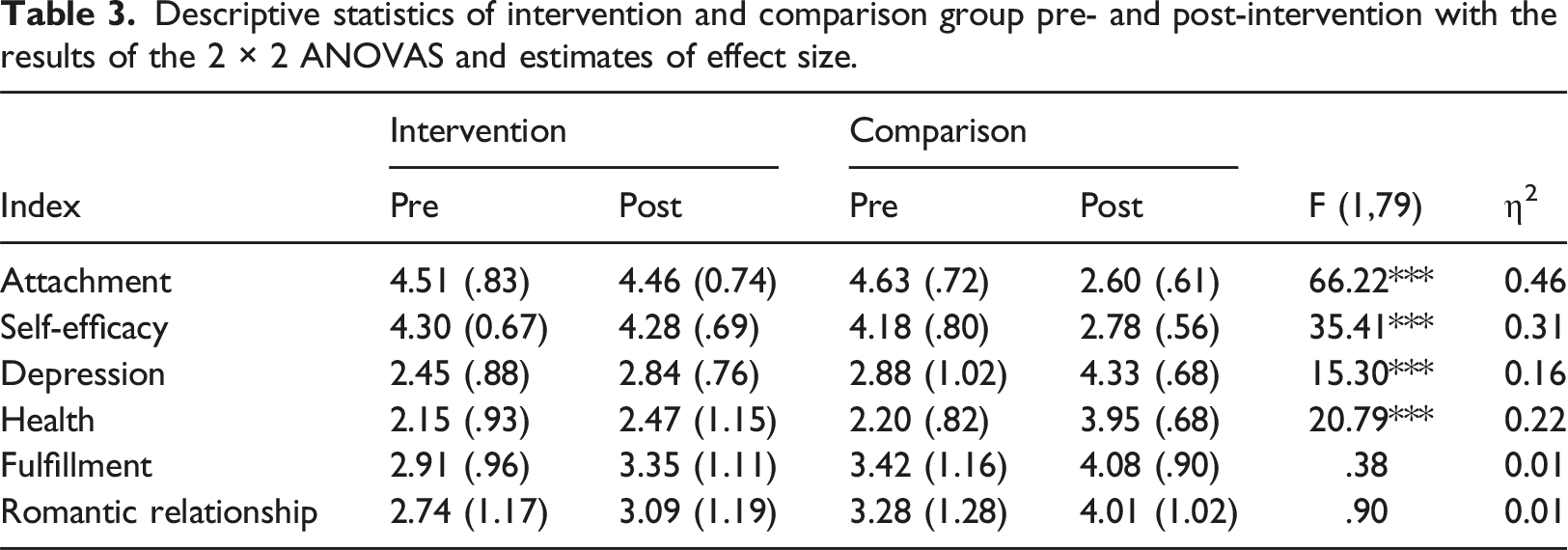
We can see two different patterns emerging in the results: an interaction effect for the attachment, self-efficacy, depression and health indices, and a main effect for the fulfillment and romantic relationship indices.
To examine the interaction effect for the first four indices, posterior comparisons were conducted between the pre- and post-measurements, in each group. The comparisons were conducted for the four indices. The results for the attachment revealed a significant decrease in the comparison group (t (39) = 11.55, p < .001), and no change in the intervention group (t (40) = 0.36, N.S). The results for self-efficacy revealed a significant decrease in the comparison group (t (39) = 7.81, p < .001), and no change in the intervention group (t (40) = 0.13, N.S). The results for depression revealed a significant increase in the comparison group (t (39) = 6.68, p < .001), and no change in the intervention group (t (40) = 0.01, N.S). The results for health revealed a significant increase in the comparison group (t (39) = 9.15, p < .001), and no change in the intervention group (t (40) = 1.30, N.S). For the indices of fulfillment and romantic relationship, the analyses revealed significant main effects (F (1,79) = 9.80, p < .002) and (F (1,79) = 7.42, p < .008), respectively.
In general, the results yielded a significant increase among the parents in the comparison group for all six indices of parental stress, whereas among parents in the intervention group, there was an increase in two indices only.
Predicting reduction of parenting stress
Multiple linear regression to predict reduction in parenting stress based on the different independent variables.
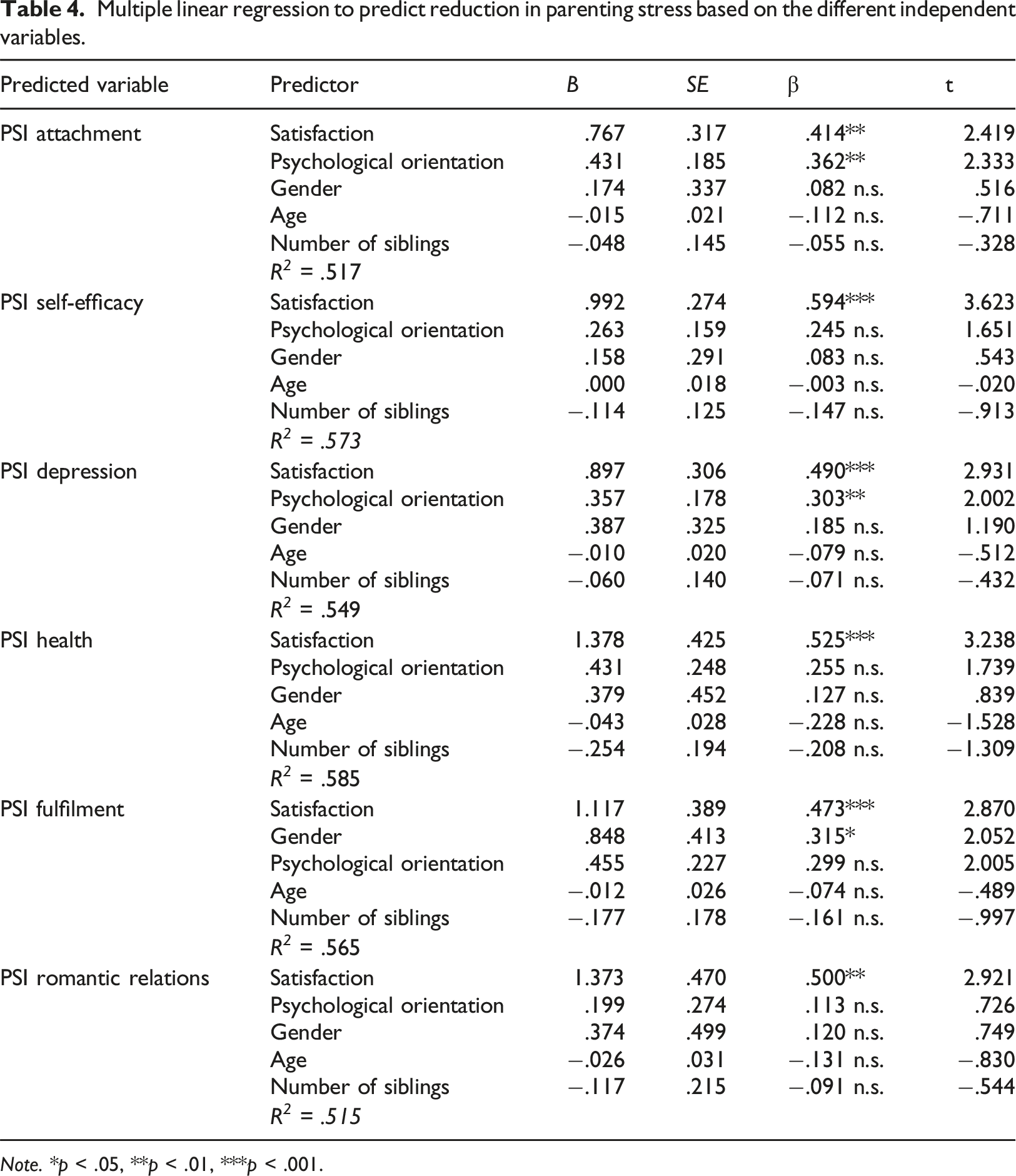
Note. *p < .05, **p < .01, ***p < .001.
A multiple linear regression to predict reduction in the PSI attachment index yielded a multiple R of .517, a multiple R of .573 was found for the self-efficacy index, .549 for PSI depression, .585 for PSI health, .565 for PSI fulfilment, and multiple R of .515 for PSI romantic relations. All Rs were statistically significant (p < .001). The strongest predictor in all six analyses was parents’ overall satisfaction with the intervention. Psychological orientation was significant for the attachment and depression indices, and gender was significant for fulfilment, with men gaining more after undergoing the intervention. Apart from gender in the abovementioned index, the socio-demographic variables had no effect on the effectiveness of the intervention.
Study limitations
The study relies primarily on the measure of parental stress. Future research would do well to examine a wider variety of variables such as acceptance of the diagnosis, and quality of child-parent relationships. Another limitation is that the parental stress was examined at only one post-intervention point: a month after diagnosis. It would have been important to examine parental stress after a longer period of time. It is possible that the group intervention had only postponed the reduction in stress but had not prevented it.
Discussion
Parents whose children have recently been diagnosed with ASD face serious challenges of grief and uncertainty about their future (Crane et al., 2016). The intervention presented in this study was designed to alleviate parent stress and facilitate the continuity of treatments for children and their parents. The research hypothesis was not supported, and the parents’ stress was not reduced after three intervention sessions. The surprising finding in this study was that parents who received treatment-as-usual showed a significant increase in most parenting stress indices, while parents in the intervention group did not. It seems that participation in post-ASD diagnosis intervention groups prevented this worsening. This may explain the findings of a previous study of a parent support group for fathers of children with ASD, where the researchers found little to no improvement despite the fathers’ endorsement of the experience as helpful (Elfert & Mirenda, 2015).
This research was unique as it examined parents immediately after receiving a diagnosis and a month later. The unexpected finding is that there is a significant elevation in parental stress during that time. While more research is needed to substantiate the finding, it does indicate that there is a need to support parents more directly during this period. Future research may also examine parental post-diagnosis stress at several points along the timeline.
The main novelty of this post-ASD diagnosis group intervention is in that it is offered as an integral part of the diagnostic process. For example, the main post-diagnosis group research that was done to date included parents who had received a diagnosis within the past six months, while in this study no more than a month had elapsed from the diagnosis to the beginning of the intervention, and in some cases less than a week. Given these findings, we would argue that such interventions should be an integral part of the diagnostic process, especially given the increase in parental stress within the first month after receiving a diagnosis in the comparison group.
The study focused on children diagnosed after the age of six, and the unique characteristics of this population should be acknowledged. These parents come with children who have previously been diagnosed with such diagnoses as anxiety and attention deficit disorder, and were coping with difficult behaviors such as aggression for many years (Aggarwal & Angus, 2015). The diagnostic procedure often takes place after long processes that can sometimes last years. Given this background, knowing that these parents were directed to a group intervention to help them process the diagnosis, reassured both the parents and the staff.
The findings suggest that sociodemographic factors had little to do with the effectiveness of the group intervention, while satisfaction with the sessions was a strong predictor. This is an encouraging finding that the success of the intervention is in the clinicians’ hands rather than due to variables clinicians have little control over.
The difference between the intervention group and the comparison group seems to indicate the importance of emotional processing with other parents in a similar situation (Rutherford et al., 2019). Processes of mutual identification are powerful and help parents feel that they are not alone in their grief. The difference between the individual and the group intervention was not in the provision of psychoeducation or empathy by professionals, but rather in the meeting with other parents and the experience of the group dynamics that helped them feel supported, understood and strengthened. It was surprising for the facilitators to see how difficult it was for parents to leave the therapy room at the end of each meeting, and their urge to connect with other parents and exchange information and advice with them. In this sense, the intervention can also provide parents with a sense of community and connection with other families and professionals. This can help build a network of support and resources to help families navigate the journey of coping with autism.
Footnotes
Acknowledgements
We wish to thank the Marot staff who contributed to the groups, and especially Michal Cohen Hadaya, Noy Oppenheim, Neta Sharoni, Kay Mishoris, Tchelet Baron and Noa Tapuach for their assistance at different stages of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.