
Abstract
This paper reports follow-up findings for an Mentalization based treatment (MBT) parenting intervention delivered to a community mental health sample. Parents completed the 12-week version of the Lighthouse Parenting Program (LPP) and were evaluated on parenting practices, parent-child relationships, parental mental health indicators, and child problem behaviour levels. We evaluated the extent to which improvements in mentalizing at follow-up mediated changes in parenting, parental adjustment, mental health, and child outcomes. Results included a reduction in parental coercive behaviours and child problems, improved parent-child relationship, and better parental psychological adjustment and mental health. Improvement in self-focused mentalizing were observed. Self-focused mentalizing mediated the changes in most outcomes from baseline to 3-month follow-up. These results provide strong preliminary evidence that the LPP improves parent and child outcomes.
Introduction
Parenting can be related to various positive developmental outcomes. By contrast, parenting behaviours can also increase a child’s psychosocial vulnerability and in some instances cause acute and long-term harm (Toth & Manly, 2019). Child abuse, unresponsive caregiving, and neglect impose a heavy social burden, and can become perpetuated intergenerationally (Langevin et al., 2021). The most significant parent factors implicated in cases of maltreatment include parental mental health (Langevin et al., 2021), personality disorder traits (Florange & Herpertz, 2019), parenting stress (Pereira et al., 2012), parental self-efficacy (Michl-Petzing et al., 2019), relational factors (Langevin et al., 2021), as well as parental mentalization (Sharp & Fonagy, 2008). Even in non-clinical populations these factors appear to predict daily parenting behaviours (Michl-Petzing et al., 2019). Therapeutic and psychoeducational interventions such as parenting programs that target these factors can reduce risk of maltreatment and improve child developmental outcomes. Yet more work is required to understand the mechanisms by which such important changes are generated.
Parenting programs appear to be effective at reducing child maltreatment risk factors and recurrence (Altafim & Linhares, 2016; Branco et al., 2022). Follow-up investigations are important for distinguishing those interventions that produce lasting changes from those that do not. Effect sizes at follow-up tend to be small; indeed, for some parents, the behavioural changes apparent at post-treatment diminish or disappear over time, although it is unclear why this occurs (Backhaus et al., 2023). More research is needed to understand the ways in which intervention, when it works, affects parent-child psychological and relational processes.
Mentalizing capacity and parenting behaviour
Mentalization is the capacity to infer the mental states (emotions, thoughts, beliefs, needs, intentions in oneself and others) that motivate behaviour and to utilise this information to navigate social interaction (Fonagy & Bateman, 2007). This multi-faceted and fluctuating capacity plays an important role in parenting and child development (Camoirano, 2017; Sharp & Fonagy, 2008). Mentalization also appears to scaffold parents and protect their experience of parenting under stress. For instance, mentalization predicts higher parental satisfaction in those parents who have themselves experienced disrupted attachment (Burkhart et al., 2017), it predicts positive parenting behaviours (Santelices & Cortés, 2022), and it reduces parental hostility when parents have poor emotion regulation (Gershy & Gray, 2020). Essentially, when parent and child internal states can be mentally represented, they can be converted from states of affective intensity into symbolic thought. This may be the cornerstone of emotional self-regulation and a range of consequent social skills.
In contrast, low parental mentalization predicts a range of vulnerabilities and problems for children and parents (Condino et al., 2022; Rostad & Whitaker, 2016). Mentalizing capacity distinguishes mothers whose attitudes and behaviours predict child abuse risk from those who show no significant indicators of risk (Hunter et al., 2022). Parents with a history of child maltreatment demonstrate hostility to mentalizing demands (Rosso, 2022). Synthesising the present state of this literature, Byrne et al. (2019) have suggested that child abuse can be understood as a consequence of dysfunctional or limited mentalizing capacity and the consequent risk that children’s mental states and behaviours can be interpreted in distorted or inaccurate ways. Mentalizing may therefore be an important consideration in efforts to reduce the social impact of child abuse and neglect. Researchers can begin to distinguish whether successful parenting interventions are those that improve one or more facets of parental mentalization (thus reducing the likelihood that affective impulses become expressed as problematic behaviours). This is a directly testable hypothesis, which can be evaluated by looking at the ways in which mentalizing mediates any impact of intervention on improved parenting outcomes.
Follow-up effects in mentalization-based parenting treatments
Mentalization based treatments (MBT) for parents attempt to improve their capacity to understand and respond sensitively to their own mental states (self-focused mentalizing) and to those of their children (child-focused mentalizing). Outcome evaluations are published for several such interventions (for recent reviews, see: Lavender et al., 2023; Lo & Wong, 2022). MBT interventions for parents appear to improve parental mentalizing, mental health, and the quality of caregiving (Camoirano, 2017). Relatively few studies have reported follow-up data in relation to such changes and no consistent pattern of results is yet detectable in those that have. For instance, Ordway et al. (2014) reported that an MBT parenting treatment improved child behavioural outcomes that were maintained at follow-up. Mentalizing continued improving beyond the termination of treatment, yet these improvements did not appear to relate to child behaviour. Suchman et al. (2011) reported that changes in one specific aspect of parental mentalizing (self-focused) were maintained at follow-up for the same intervention. Later results for the same intervention in a community mental health sample indicated improvement in child-focused, but not self-focused mentalizing, at follow-up (Suchman et al., 2017).
Conflicting results are also apparent in relation to psychological outcomes for MBT Parenting interventions. Several studies have reported that intervention groups cannot be differentiated from control groups or baseline measurements on depression and psychopathology measures at follow-up (Ordway et al., 2014; Suchman et al., 2011, 2017). Yet others demonstrate impressive changes in these factors (Salo et al., 2019; Suchman et al., 2017). There are many possible explanations for these observations, including sample characteristics and the range of ways in which mentalization has been operationalised and measured. No study has evaluated whether specific facets of mentalizing mediate these psychological outcomes.
Lastly, child outcomes have been reported in very few follow-up studies. Early evidence suggests that MBT parenting interventions generate improvements for children (Enav et al., 2019; Midgley et al., 2019), although much more is needed in this regard.
Current study
Early evidence suggests that MBT for parents improves parenting behaviours, family relationships, and mental health correlates (each of which are implicated in child abuse risk and parenting behaviour). However, these effects have mainly been observed at post-treatment and follow-up evaluations are rare. In addition, it is not clear which facets of mentalizing (if any) are mediators of change when a parenting intervention produces improvements in parenting variables. The present study directly addressed these gaps by evaluating parenting variables 3-month after the conclusion of an MBT Parenting intervention. Post-treatment effects for this intervention have been reported elsewhere (Gervinskaitė-Paulaitienė et al., 2023). In the current study we evaluated the extent to which improvement in mentalizing capacity mediated changes in parenting practices, parent-child relationships, family relationships, parental mental health indicators, and child problem behaviour levels. Three facets of mentalizing were tested: (i) self-focused, (ii) other-focused, and (iii) motivation to mentalize. We hypothesized that at follow-up, all outcomes would show improvements relative to baseline measurements. We hypothesised that all three facets of mentalizing would be higher at follow-up relative to baseline measurements. Lastly, we hypothesised that these changes in parenting, psychological adjustment and mental health, family functioning, and child problems would be mediated by improvements in each of the three facets of mentalizing.
Method
Design
This was a non-controlled one group pre-posttest study with 3-month follow-up. The study was approved by the Institutional Ethics Committee. Informed consent from all participants was obtained prior to their participation. Outcome measurements were taken at three time points: (i) before intervention (baseline); (ii) after intervention ended (post-test); and (iii) at 3-month follow-up. Participants completed all questionnaires online, accessing them via separate links. The post-test analysis of this study has been published elsewhere (Gervinskaitė-Paulaitienė et al., 2023).
In this paper we focus on the analysis of the 3-month follow-up. This study was pre-registered: https://doi.org/10.17605/OSF.IO/HX7VB
Participants
This study was implemented in five community mental health institutions who provide treatment for families and children. The sample consisted of 101 parents (82 mothers and 19 fathers) living in two cities in Lithuania (age range = 24–60; M = 39.1, SD = 5.74). Most parents were married/cohabitating (78%), 10% were divorced, 8% were single and 4% other. Most families had two children (54%), 23% had one child, and 23% had three or more children. Most of the parents had higher education (89%), 9% completed secondary education, and 1% had not completed school. Most parents were employed (80%), 13% were unemployed, and 7% were mothers on parental leave. Most parents had children with prior referrals to mental health or psychoeducational services because of a child’s problems (73%) and 45% had children who were currently receiving services. Many parents had their own prior experiences with a mental health service (73%) and 44% were currently receiving services. Parents were recruited in collaboration with group facilitators and other specialists. Invitations to participate in the study were also distributed through online groups and mailing lists related to parenting.
Inclusion criteria were: (i) have at least one child, aged 12 or less; (ii) parents themselves had been referred or self-referred for mental health services due to mental health, child rearing or family problems, and/or have a child who had been referred for mental health or psychoeducational services due to their emotional, behavioural, or developmental problems; (iii) speak Lithuanian; and (iv) agree to participate in the study. Parents were excluded from the study if: (i) their referral required inpatient treatment; (ii) their referral indicated incompatibility with group treatment; (iii) they experienced significant intellectual disability; or (iv) they were in another parenting program.
Measures
Parenting and family adjustment scales (Sanders et al., 2014)
This scale assesses parenting practices and parent/family functioning. It contains 30 items and has 7 subscales. Higher scores denote higher levels of dysfunction. In this study, Cronbach’s α was good for all subscales except one, which was unacceptable and thus excluded from analyses (Coercive Parenting = .71; Positive Encouragement = .72; Parent–Child Relationship = .85; Parental Adjustment = .80; Family Relationships = .78; Parental Teamwork = .79; Parental Consistency = .38).
The parental stress scale (Berry & Jones, 1995)
This scale evaluates stress related to child rearing, capturing demands and rewards of parenting. The 18 items sum to produce a total stress score, which in this study had good reliability (α = .89).
Brief parental self efficacy scale (Woolgar et al., 2023)
This 5-item scale measures how confident parents are that they can manage the tasks and demands of parenting. It produces a single score, which in this study had good reliability (α = .81).
Mentalization scale (Dimitrijević et al., 2018)
This 28-item scale evaluate three aspects of mentalization: self-related (MentS-S), other-related (MentS-O), and motivation to mentalize (MentS-M). Higher subscale scores denote a higher capacity for mentalization. In this study, reliability ranged from acceptable to good (αTotal = .86; αMentS-S = .69; αMentS-O = .74; αMentS-M = .79).
Patient health Questionnaire-9 (Kroenke et al., 2001)
This 9-item scale screens respondents for depressive symptoms. It produces a single score, which in this study had good reliability (α = .85).
The Generalized Anxiety Disorder scale-7 (Spitzer et al., 2006)
This 7-item scale screens respondents for generalized anxiety disorder symptoms. It produces a single score, which in this study had excellent reliability (α = .91).
The Level of Personality Functioning Scale-Brief Form 2.0 (Weekers et al., 2019)
This 12-item scale assesses personality functioning, with higher scores indicating more impaired personality functioning. This scale had good reliability in this study (α = .83).
Strengths and Difficulties Questionnaire (Goodman, 1997)
This scale asks parents to rate their child’s emotional and behavioural problems. We used a total problem score, which is obtained by summing 20 items that measure hyperactivity, emotional, conduct problems, and problems with peers. If parents had more than one child, they were asked to fill out the SDQ for whichever child experienced the most difficulties at that time.
Intervention
The Lighthouse Parenting Program (LPP) is a manualised MBT Parenting intervention originally developed for implementation with parents who have harmed or neglected their children (Byrne et al., 2019). It combines psychoeducational and psychotherapeutic interventions to improve parental mentalizing and strengthen parent-child relationships. The full program is 20-week long and comprises weekly group and fortnightly individual therapy sessions. We selected the 12-week adaptation of the program for this study (Byrne & Ruggiero, 2018) since it was developed for use with parents in community mental health settings. This version does not include individual therapy (group only). The program manual details the tasks, content, and recommended activities for each of the 12 modules. The aim of the program is to increase parental mentalizing through experiential activities, discussions of educational material, and by encouraging and modelling mentalizing in group sessions. MBT individual and group skills are employed by the facilitators throughout the program. The LPP uses metaphors (such as lighthouse, safe harbour, etc.) to convey attachment and mentalization concepts to parents.
All parents attended an individual intake session with one of the group facilitators, to prepare for entry into the program. Each session was 2 hours duration with a short break. There were nine groups running in five locations with 7–15 participants per group. Two facilitators led each group. All facilitators were qualified psychologists who received LPP training from the program authors (G.B. and M.R.). Facilitators attended weekly group supervision delivered by one program author (G.B.) and a second accredited LPP supervisor.
Data analysis
All analyses were performed using IBM SPSS Statistics (Version 27). To evaluate group differences, we used Mann-Whitney for outcome measures and Chi-square for demographic characteristics (comparing completers with drop-outs; comparing those who participated in the follow-up assessment and those who did not). A paired samples t test was performed to test the differences between outcome scores at baseline and follow-up. Cohen’s d was calculated to interpret effect sizes. An alpha level of p < .05 was used for all analyses. Mediation hypotheses were tested using Mediation and Moderation Analysis for Repeated Measures Designs MEMORE (Montoya & Hayes, 2017). MEMORE is a SPSS macro available from the author’s website (https://www.akmontoya.com/spss-and-sas-macros). MEMORE estimates total, direct, and indirect effects in a two-condition within-participant design. In this mediation analysis the independent variable was “intervention”. In the analysis, the changes in dependent variables and mediators from baseline to follow-up were calculated. The significance of indirect effects was estimated using the bootstrap method of inference (with 5000 runs), providing 95% confidence intervals (CI) for an indirect effect. An indirect effect is considered statistically significant if the confidence interval excludes zero (Montoya & Hayes, 2017).
Results
From all parents (N = 101) who started the program, 89 (88%) parents finished it. From completers, 75 participated in follow-up (see Figure 1). Comparisons of completers (n = 89) and drop-outs (n = 12) showed no differences in outcomes, except for employment status (more employed parents finished the program and more mothers on maternity leave dropped out). Further, we compared parents who completed the program and the follow-up assessment (n = 75) with parents who completed the program but did not participate in follow-up (n = 14). They differed on MentS at baseline (Mann-Whitney U = 238.0, p = .010), parents who did not participate at follow-up reported higher MentS scores (mean rank = 60.67) compared to parents who did participate (mean rank = 40.72). Study flow.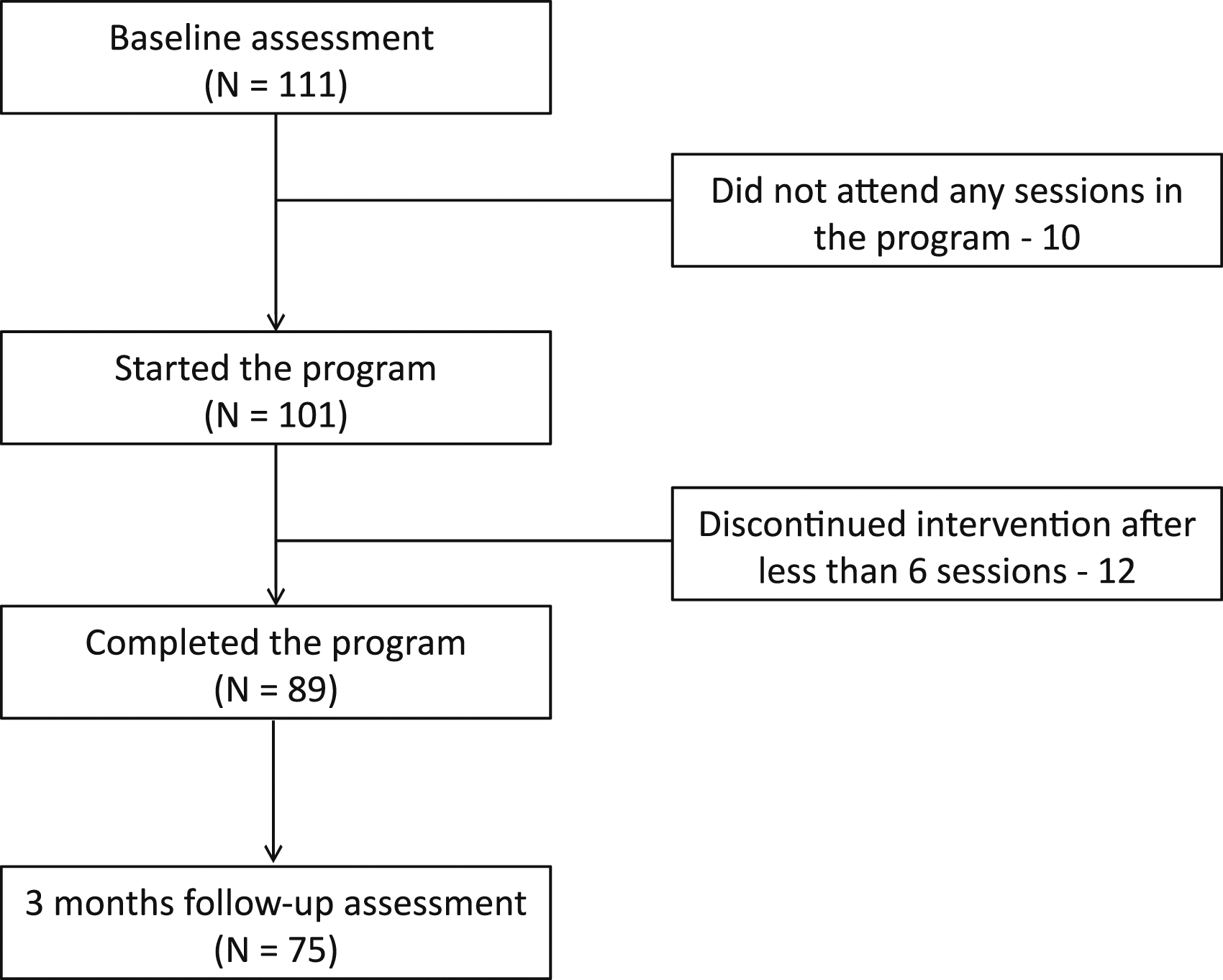
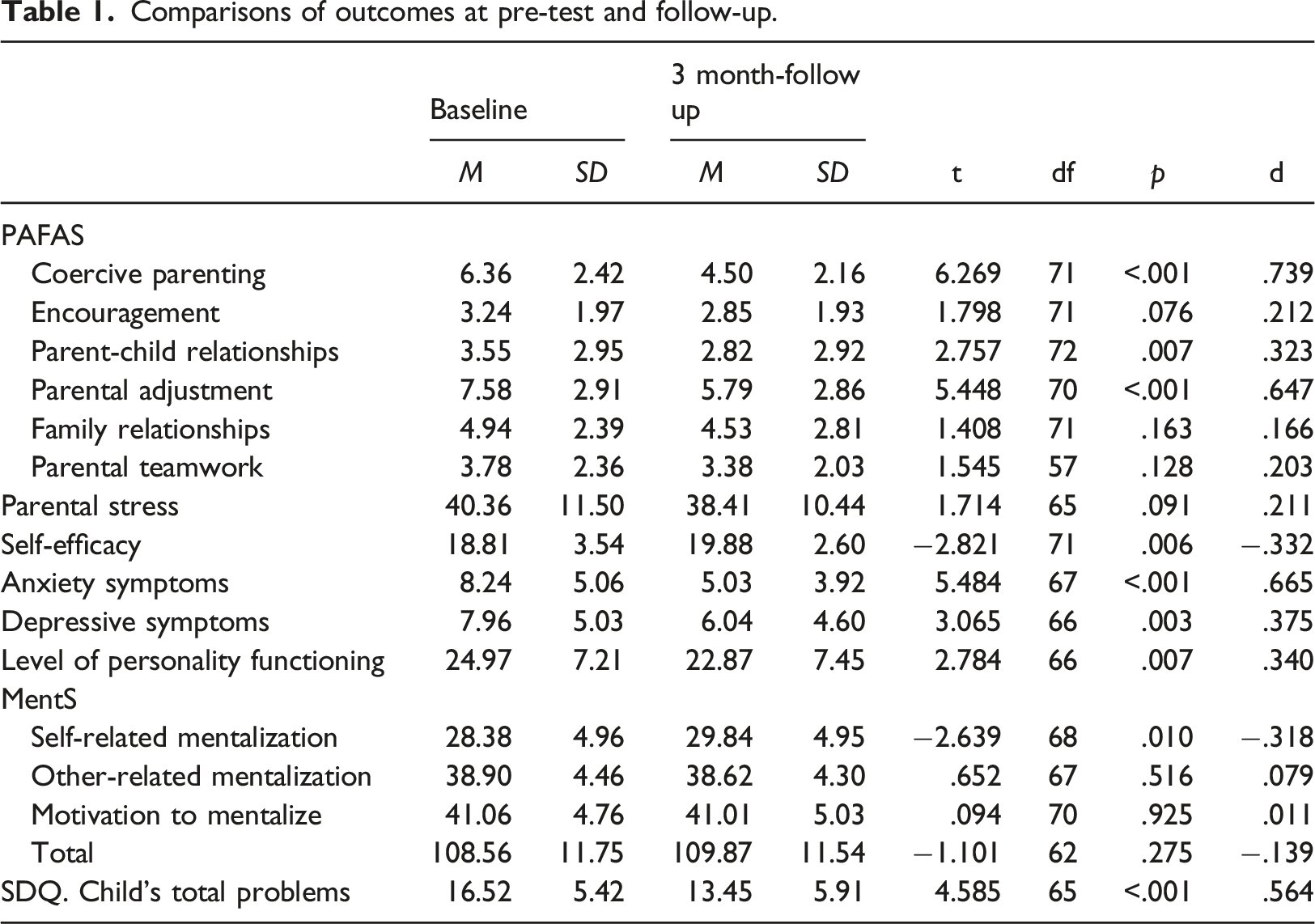
Comparisons of outcomes at pre-test and follow-up.
Mediational analysis.
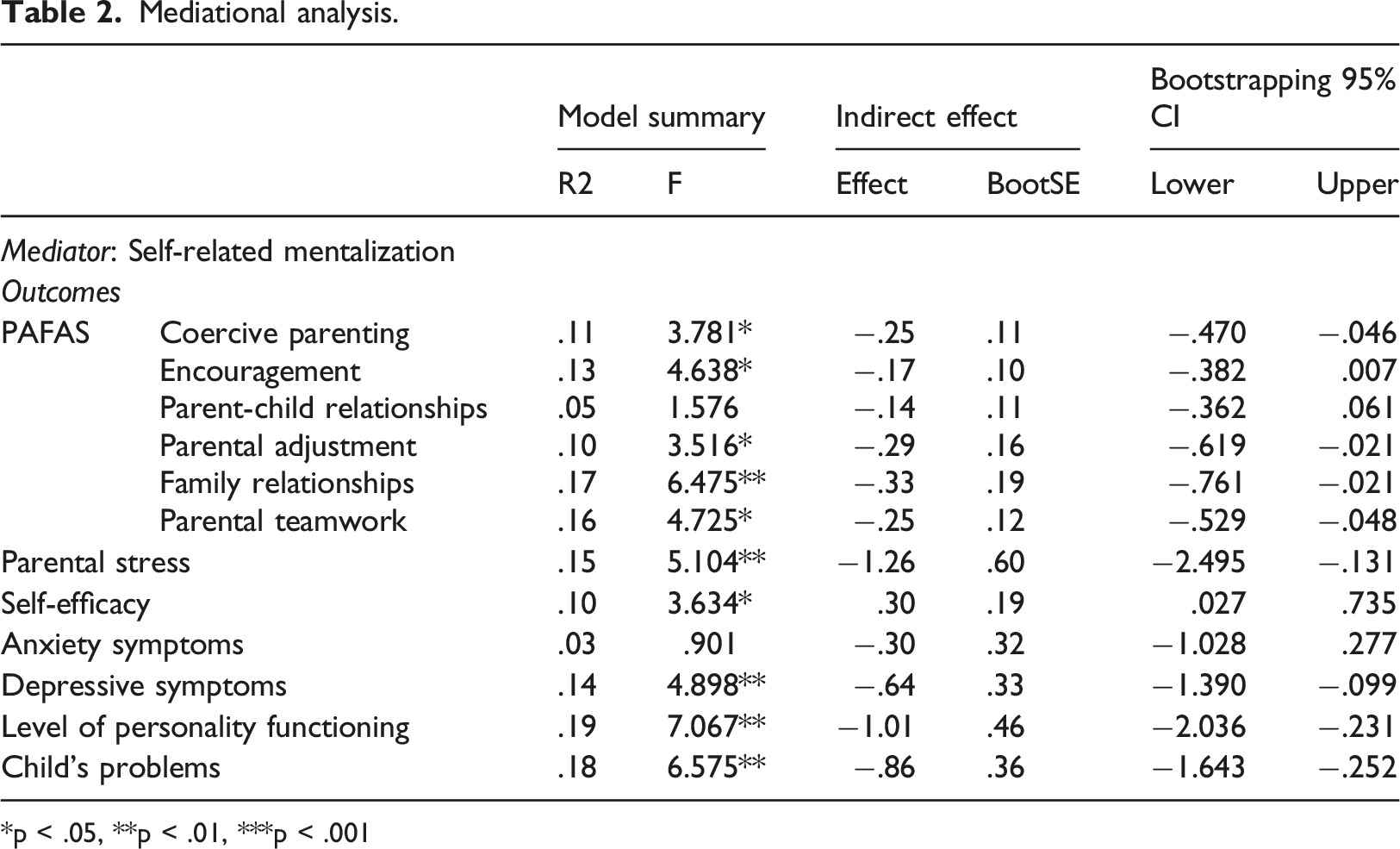
*p < .05, **p < .01, ***p < .001
Several significant mediational effects were detected. Improvement in self-related mentalization mediated the effect (at follow-up) of intervention on: (i) reduction of coercive parenting practices; (ii) improvements in parental emotional adjustment, family relationships, parental teamwork, self-efficacy, and personality functioning; (iii) decreases in parental stress and depressive symptoms; and (iv) reduction of child behavioural problems. However, improvement in self-related mentalization did not mediate the effect of intervention on changes in parent-child relationship and positive encouragement.
Discussion
In our study, follow-up observations largely supported hypothesis 1: (i) coercive behaviours had reduced; (ii) the parent-child relationship had improved; (iii) parents were more emotionally adjusted; (iv) parents had less mental health symptoms; (v) parenting self-efficacy improved; and (vi) child problems had reduced. Parents had improved in their ability to mentalize their own internal states (partial support for hypothesis 2), and this improvement in mentalizing generated the changes we observed in most outcomes from baseline to follow-up (partial support for hypothesis 3). These results provide strong preliminary evidence that the LPP improves parent and child outcomes by influencing at least one facet of parental mentalization (self-mentalizing).
We had expected all dimensions of mentalization to improve after LPP. However, only self-focused mentalization improved, whereas no change was observed in other-focused and motivation to mentalize. Previous studies of MBT parenting interventions have measured mentalization related to the parent-child relationship, observing improvements (Enav et al., 2019; Salo et al., 2019). In a small study of LPP with high-risk parents, mentalization did not improve (Byrne et al., 2019). The few follow-up studies of MBT parenting interventions appear to show that improvements in mentalization are maintained (Salo et al., 2019; Sleed et al., 2013). The change in self mentalizing that we observed in this study is consistent with Suchman et al. (2011), confirming that it is important to treat this as a multi-dimensional phenomenon and not a single outcome in intervention research. Fonagy and Luyten (2018) have suggested that the capacity to represent internal self-states pre-dates the capacity to distinguish and represent others’ minds as separate entities. So it may be unsurprising that a short-term mentalizing intervention has the greatest effect on this facet of mentalizing. Our results suggest that self-focused mentalizing may be of particular importance in parenting interventions.
The results observed here have several alternative explanations. The increase in self-focused mentalizing might be linked to the fact that LPP invites parents to attend to, and reflect, on their own emotional experiences in their attachment relationships and in the group. Participants are mentalized ‘live’, whereas their children are not present to observe when mentalizing turns to their experiences. Furthermore, our chosen mentalizing measure uses generalised item wording and does not specify, for example, that attention be paid to the child who was in focus during the program when responding to items. It is possible that any changes in other-focused mentalizing and motivation to mentalize are specific (related to target children only) and not yet generalised after the 12-week intervention. Without the inclusion of a control/comparison group and an evaluation of these capacities in relation to a target child, it is not possible to comment further on this result.
Our results show reduction in coercive parenting, i.e., parents less frequently shouted at children, got angry with them, used physical discipline, and engaged in control through inducing guilt and shame. As these behaviours are associated with a risk of child maltreatment (Sanders et al., 2014), their decrease is important for maltreatment prevention. Our results are comparable with other child abuse prevention programs (Altafim & Linhares, 2016). Moreover, we distinguished that this decrease in coercive parenting was mediated by improved self-related mentalization; that is, as parents better understand their own mental states, their coercive behaviour reduced. This is consistent with Fonagy’s (2003) suggestion that lower mentalization is related with aggressive behaviours and provides a context for the relationship between parental emotion dysregulation and hostile parenting (Gershy & Gray, 2020). Increased self-focused mentalizing might help parents to regulate themselves better in emotionally charged interactions with the child and not resort to coercive behaviours.
There was an improvement in the parent-child relationship quality. Parents felt more reciprocal warmth and were more satisfied with the relationship. It is important to note that there were no significant differences in the relationship from pre-to post-test in this sample (Gervinskaitė-Paulaitienė et al., 2023). It might be that these changes need time to unfold, as seen elsewhere (Suchman et al., 2017). Although related to the intervention, this improvement was not generated by the increase in self-focused mentalizing.
Parental emotional adjustment, self-efficacy, and family functioning are important risk factors in child maltreatment (Langevin et al., 2021; Michl-Petzing et al., 2019; Pereira et al., 2012). We observed each of these factors improve at follow-up. Other risk factors for maltreatment (parenting stress, family relationships/parental teamwork) did not improve. However, in the mediational analysis, changes in all five outcomes were predicted by changes in self-focused mentalizing. This is a complex, although important finding. Parenting stress on its own, for instance, may be a poor measure of intervention success, since in some parents (such as those who utilise primarily avoidant attachment processes) it might be hoped that the capacity to be affected by the task of parenting increase during treatment, so that it can then be regulated in new ways. In this study we observed that improvements in self mentalizing predicted improvements in all of the important predictors of maltreatment, regardless of whether parents’ experiences of stress and family relationships became more or less severe.
Depressive symptoms, anxiety symptoms, and personality functioning all improved at follow-up. This is consistent with the extensive literature documenting that MBT interventions improve affective and personality disorder symptoms (Malda-Castillo et al., 2019). The present study suggests that a relatively short MBT parenting intervention might have mental health benefits. Improvements in self-focused mentalizing predicted the change in depressive symptoms and personality functioning, but not anxiety. There is a close link between depression and attachment processes (Halstensen et al., 2021). As such, LPP interventions pay close attention to parents’ historic and current attachment processes throughout the program (Byrne et al., 2019). Parents describe that having opportunities to reflect on their attachment experiences in a safe group environment are an important element of the program (Gervinskaitė-Paulaitienė et al., 2023). Our observations that personality functioning also improved via increases in self-focused mentalizing align with the conceptual and functional closeness others have identified between these phenomena (Zettl et al., 2020).
Parents indicated that their children’s behavioural problems had reduced at follow-up. These results concur with prior studies reporting improvements in child problems after MBT parenting interventions (Enav et al., 2019; Midgley et al., 2019). The mediational analysis suggests that improved self-focused mentalizing predicts decreases in child problems. It is important to note that parents themselves report their child’s problems. It cannot be ruled out that parents’ views of their children, changed and that this subsequently influenced the way in which they perceived their children’s problems.
Limitations and future directions
Several design limitations warrant consideration. There was no control/comparison group used for this study. Future studies of LPP should build in a control/comparison condition to improve internal validity and enable causal conclusions to be drawn. A 3-month follow-up is relatively short and replication studies could use longer periods where feasible. We used self-report measures for outcome variables, which can be prone to social desirability and faking-good response patterns. Narrative-based measures and behavioural observations are more time intensive to administer but might reduce these assessment risks. Live evaluations of mentalizing are extremely time intensive but offer a gold-standard in terms of the delineation of mentalizing capacities. Our results suggest that improvements in self-focused mentalizing are an appropriate clinical target for intervention studies focused on parenting groups or problems (e.g., for those struggling with parental adjustment, low self-efficacy or using coercive practices), but that improvements in this single facet may not be sufficient to increase positive encouragement or parent-child relationship quality.
Conclusion
This study provides evidence that the effectiveness of MBT parenting interventions is detectable at follow-up. It was the first parenting intervention study to evaluate the ways in which facets of mentalizing mediate the effect of intervention on a range of parent and child outcomes. We showed that the 12-week adaptation of LPP produced a range of important outcomes in a community mental health sample of parents at follow-up. Reduction of coercive parenting practices, parental stress, child behaviour problems and improvements in parental mental health, family relationships, parental teamwork, and self-efficacy were mediated by the improvements in self-focused mentalizing that the intervention generated in the sample. Risk factors associated with child maltreatment were positively impacted by the program.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the European Social Fund (project No 09.3.3-LMT-K-712-230152) under grant agreement with the Research Council of Lithuania (LMTLT). This study was pre-registered: ![]()