
Abstract
The objective of this research was to assess the efficacy of behavioral therapy interventions in the treatment of autism spectrum disorders (ASD). The study utilized the PubMed and Embase databases to locate randomized controlled trials, quasi-experimental treatment studies, and randomized clinical trial comparisons. The experimental group received treatment based on an applied behavioral approach, such as PECS, DTT, PRT, TEACCH, ESDM, and EIBI. After examining seventeen studies, the researchers found that each type of behavioral intervention had a positive impact. Naturalistic protocols that employed PRT and PECS improved ASD symptoms in general, despite their targeting of particular cognitive domains such as language. ESDM enhanced receptive language, particularly in preschool-aged children. Structured and integrated interventions, like EIBI and TEACCH, improved overall adaptive functioning. Combining DTT with a TEACCH program produced greater benefits in linguistic, affective-social, and personal autonomy domains. However, there is a scarcity of high-quality research available on behavioral interventions for ASD. Further comparative studies are necessary to identify cost-efficient interventions. For example, PRT and PECS significantly improved social communication skills in only 15–40 hours over six months. The authors emphasized the need for continued research and the application of evidence-based interventions in specialized settings.
Keywords
Introduction
Autism spectrum disorder (ASD) is a neurodevelopmental disorder characterized by persistent deficits in social communication and interpersonal interaction in multiple contexts. Common signs of ASD are having a deficit of social-emotional reciprocity, use of non-verbal communication behaviors for social interaction, and insufficiency in the development, management, and understanding of relationships (APA, 2022).
Autism spectrum disorders is a significant public health concern due to its early onset, prolonged duration, and numerous associated impairments (Yu et al., 2020). As a result, various treatments from different theoretical perspectives have been suggested (Howard et al., 2014). In current clinical practice, promising interventions are based on the principles of the behavioral approach (Lovaas, 1987). All forms of behavioral treatment come from the experimental analysis of behavior. This area of science studies the laws that influence people’s behavior in the environment. The continued study and application of these laws to socially significant problems is known as applied behavioral analysis (ABA) (Pervin et al., 2022). In summary, ABA involves the systematic teaching of small measurable units of behavior. The task chosen to be learned is identified based on the development profile, individual choices, and preferences depending on the person. These units are divided into small stages, each of which is taught in repeated and close teaching sessions, according to specific instructions. The student is guided to give simple answers, systematically incorporated into age-appropriate repertoires (learning without errors) through prompts and consequences that function effectively as reinforcement. Therefore, when applied to ASD, ABA focuses on treating the problems of the disorder by altering social environments, identifying the factors that favor preservation over time, and favoring the learning of adaptive and functional behaviors (Pervin et al., 2022). ABA is included among a series of approaches, known as behavioral interventions, which are placed along a continuum that goes from highly structured approaches to environmental ones. The environmental and social approaches are focused on the interests of children and integrated into the children’s daily activities (Howard et al., 2014).
One structured approach is discrete trial training (DTT; Werts et al., 2003). DTT is very popular and a type of behavioral intervention in which skills are taught through a procedure that includes three elements. The first component is the instruction given to the child, also known as the discriminating stimulus (= DS), which constitutes the antecedent stimulus that will lead to the control of behavior. The second component is the child’s response (= R) and the third one is the consequence of the child’s response (reinforcement stimulus = SR) (Leaf et al., 2016).
In the current clinical practice, promising interventions are based on the principles of ABA and developmental strategies – such as naturalistic developmental behavioral interventions (NDBI; Schreibman & Stahmer, 2014). A prominent NDBI with emerging evidence is pivotal response treatment (PRT; Koegel & Koegel, 2006). PRT strategies are child-focused and have a natural rewarding approach to strengthen the child’s motivation for social contact. Implementation procedures include: following the child’s interests, gaining the child’s attention, using clear instructions (prompts), providing immediate and contingent reinforcement in response to a child’s initiation or good attempt, and interspersing maintenance and acquisition tasks. In addition, caregivers are actively involved in the PRT program (de Korte et al., 2021).
Other researchers have emphasized the use of intrinsic motivation as a positive drive for learning. There are two key models utilizing this method. These models are known as the treatment and education of autism and communication handicapped children (TEACCH; Venter et al., 1992) and the early start Denver model (ESDM; Rogers et al., 2012). The TEACCH program stands out for its comprehensive and multidisciplinary approach compared to other treatments. Its goal is to promote independence and social inclusion through structured teaching, as described by Vivanti et al. (2016). On the other hand, the ESDM program is designed specifically for preschool children with ASD, in agreement with Colombi et al. (2018) because it mainly focuses on the development of communication skills and mutual social interaction. This approach involves structured sessions based on DTT, where a specialized operator leads intensive activities according to rigorous procedures (Wong et al., 2015).
Finally, there are competency-based methods that concentrate on particular cognitive fields and functional capabilities. The Picture Exchange Communication System (PECS; Bondy & Frost, 1998) is a prime example of this and can be incorporated into integrated techniques or used alone to improve communication abilities (Lerna et al., 2012, 2014).
Despite this knowledge, scientific evidence is not always consistent in describing the effectiveness of these treatments and requires further supporting evidence. For instance, the most recent meta-analysis (Yu et al., 2020) analyzing 14 randomized control trials in which 555 participants were included revealed significant outcomes on socialization, communication, and expressive language due to the adoption of ABA-based interventions (i.e., ESDM, PECS, and DTT). Nonetheless, significant effects for the outcomes of autism general symptoms, receptive language, adaptive behavior, daily living skills, verbal and non-verbal intelligence quotient, restricted and repetitive behavior, and motor and cognition were not reported by Yu and colleagues. Our study aimed to replicate the systematic literature review including the most recent studies. Furthermore, another goal was to highlight whether there were different outcomes between various behavioral interventions compared to each other.
Methods
Information sources and search strategy
The following databases were searched: Pubmed, Medline, Embase, and PsycInfo. The main keywords utilized in the article searches included the following: autism spectrum disorder, autism, autistic disorder, ASD; behavioral interventions, behavior therapy; applied behavior analysis, ABA; picture exchange communication system, PECS; discrete trial teaching, DTT; pivotal response treatment, PRT; treatment and education of autistic and communication handicapped children, TEACCH; early start Denver model, ESDM; early intensive behavioral intervention, EIBI. The search considered the title and abstract or topic and included only journals in English. Finally, the search was limited by date: the databases were searched considering the last 10 years.
Eligibility criteria and study selection
Studies were included if they met the following criteria: (1) the study should be a randomized controlled trial (RCT), a quasi-experimental treatment study, or a randomized clinical trial comparison; (2) participants were between the ages of 0 and 18 years old; (3) participants were diagnosed with ASD and their symptomatology was measured by a recognized scale (i.e., ADOS: Autism Diagnostic Observation Scale); (4) the treatment used in the experimental group was part of the behavioral interventions (ABA, PECS, DTT, PRT, TEACCH, ESDM, EIBI); (5) the treatment used in the control group was traditional intervention (i.e., conventional language therapy, parental guidance, intensive family therapy, and social skill training); (6) the study included at least one standardized continuous outcome measure related to autistic manifestations. Studies were excluded if they (1) were qualitative, reviews, meta-analyses, case studies, theses, dissertations, or conference presentations; (2) did not specifically measure the symptomatology of ASD; (3) did not administer a form of behavioral intervention (ABA, PECS, DTT, PRT, TEACCH, ESDM, EIBI).
Selection of outcome measures
The general symptomatic outcomes of ASD, including socialization outcomes, communication outcomes, expressive language outcomes, receptive language outcomes, adaptive behavior outcomes, daily living skills outcomes, and intelligence quotient outcomes, were selected in this study.
Results
Study selection
Figure 1 presents the PRISMA chart that shows the results of the search. The search across databases produced 1,478 records. After removing 698 duplicates, 789 records were screened based on the title and abstract, 673 of which were excluded. 116 full-text articles were assessed for eligibility and 99 of them were excluded. The reasons were: 63 were excluded because of the absence of a control group; 1 study could not provide full text after contacting the author; 9 studies did not meet the requirement for participants; 25 studies did not include relevant outcomes; and 1 study did not adequately describe the procedure of the implemented treatments. Finally, 17 randomized controlled trials, quasi-experimental treatment studies, and randomized clinical trial comparison studies were included in this review. Flow diagram of study selection.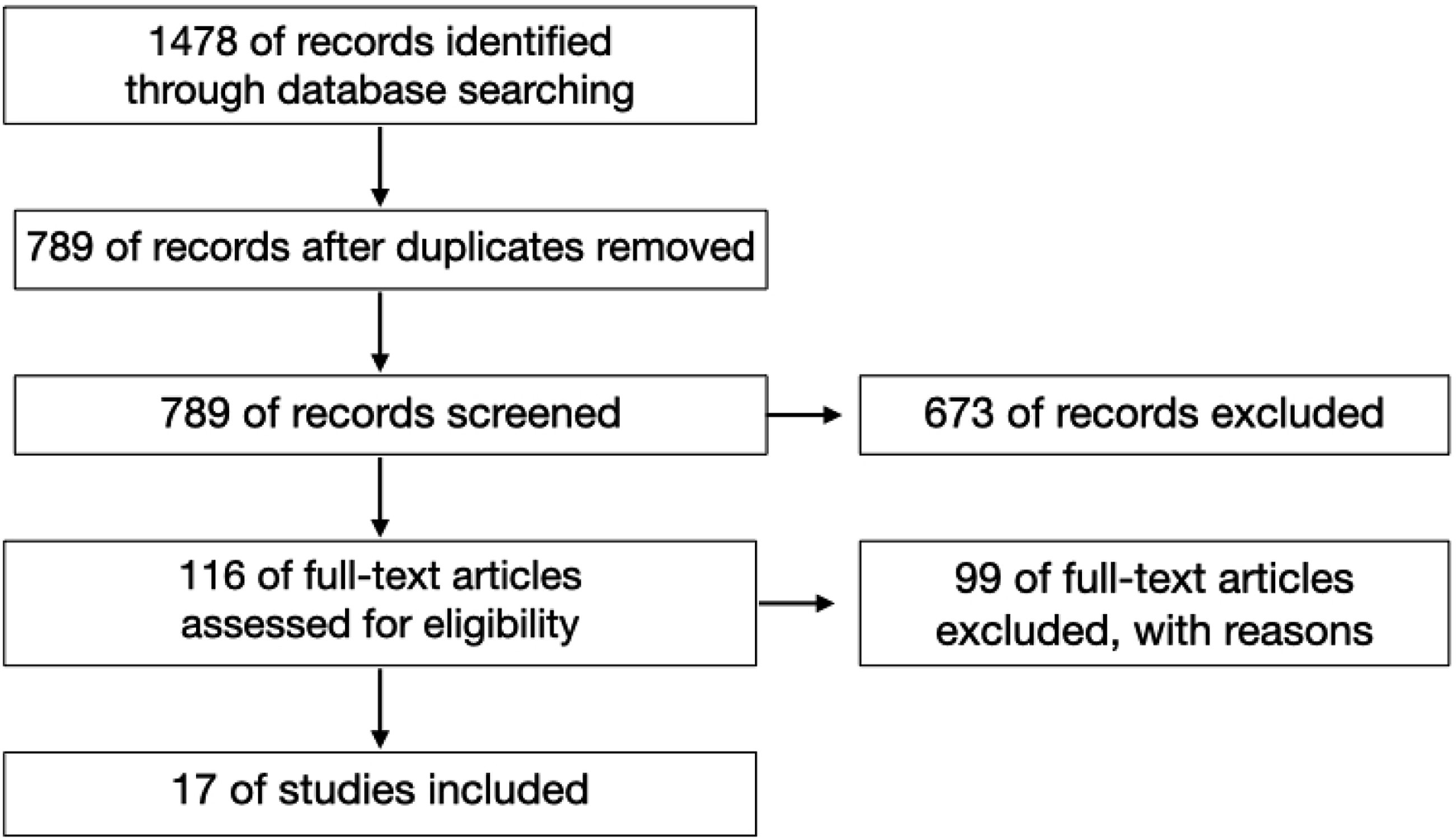
A summary of controlled studies characteristics.
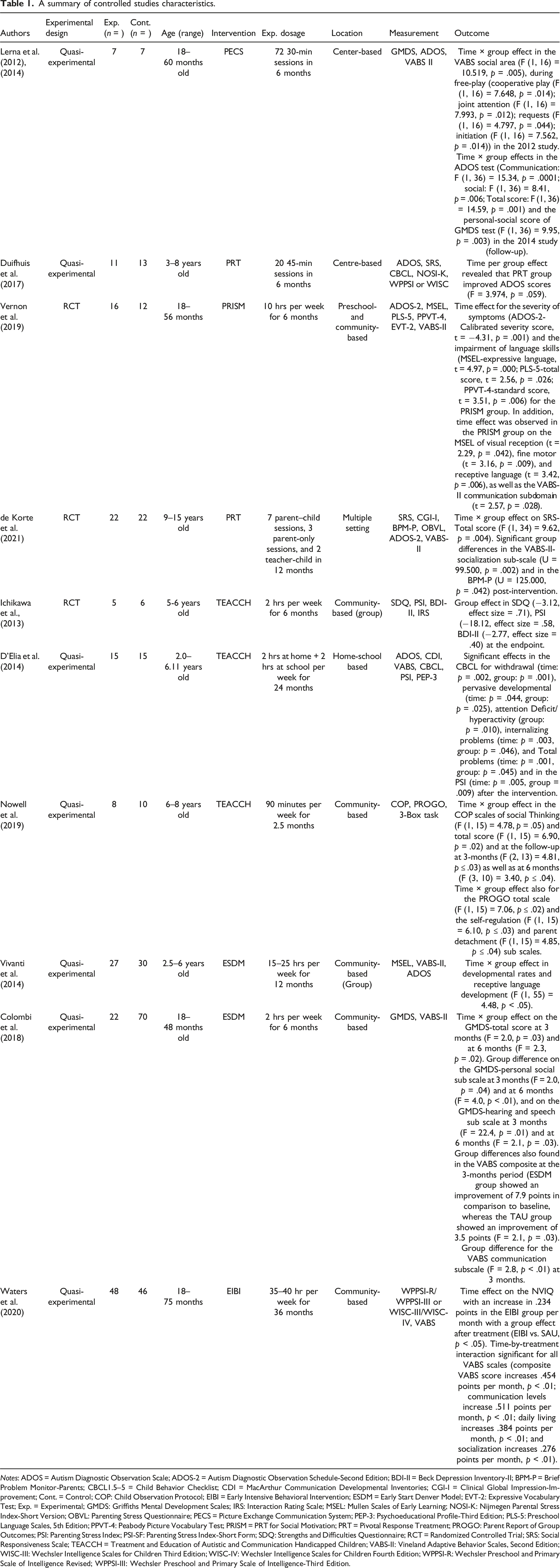
Notes: ADOS = Autism Diagnostic Observation Scale; ADOS-2 = Autism Diagnostic Observation Schedule‐Second Edition; BDI-II = Beck Depression Inventory-II; BPM-P = Brief Problem Monitor‐Parents; CBCL1.5–5 = Child Behavior Checklist; CDI = MacArthur Communication Developmental Inventories; CGI-I = Clinical Global Impression‐Improvement; Cont. = Control; COP: Child Observation Protocol; EIBI = Early Intensive Behavioral Intervention; ESDM = Early Start Denver Model; EVT-2: Expressive Vocabulary Test; Exp. = Experimental; GMDS: Griffiths Mental Development Scales; IRS: Interaction Rating Scale; MSEL: Mullen Scales of Early Learning; NOSI‐K: Nijmegen Parental Stress Index-Short Version; OBVL: Parenting Stress Questionnaire; PECS = Picture Exchange Communication System; PEP-3: Psychoeducational Profile-Third Edition; PLS-5: Preschool Language Scales, 5th Edition; PPVT-4: Peabody Picture Vocabulary Test; PRISM = PRT for Social Motivation; PRT = Pivotal Response Treatment; PROGO: Parent Report of Group Outcomes; PSI: Parenting Stress Index; PSI-SF: Parenting Stress Index-Short Form; SDQ: Strengths and Difficulties Questionnaire; RCT = Randomized Controlled Trial; SRS: Social Responsiveness Scale; TEACCH = Treatment and Education of Autistic and Communication Handicapped Children; VABS-II: Vineland Adaptive Behavior Scales, Second Edition; WISC-III: Wechsler Intelligence Scales for Children Third Edition; WISC-IV: Wechsler Intelligence Scales for Children Fourth Edition; WPPSI-R: Wechsler Preschool and Primary Scale of Intelligence Revised; WPPSI-III: Wechsler Preschool and Primary Scale of Intelligence-Third Edition.
A summary of comparative studies characteristics.
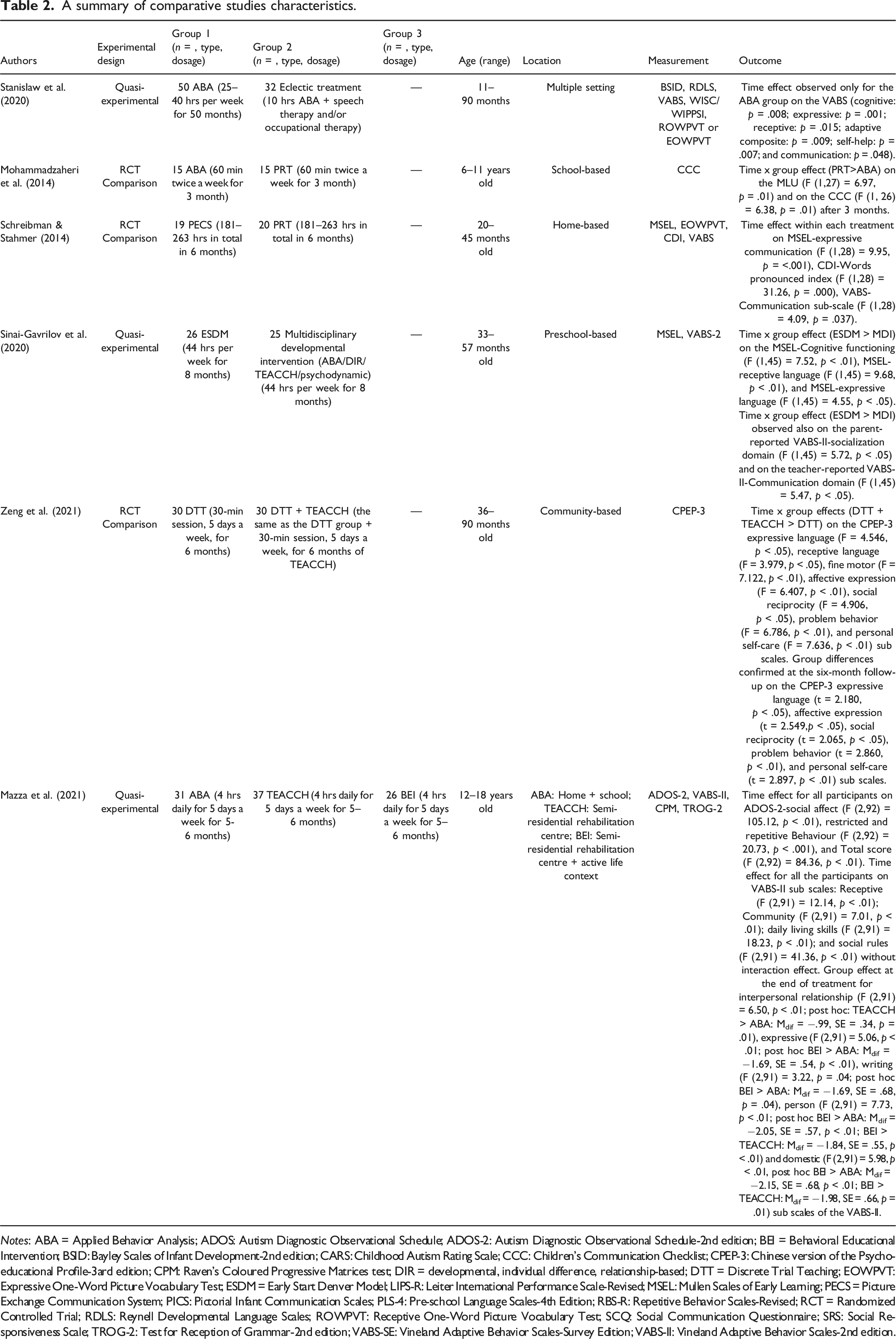
Notes: ABA = Applied Behavior Analysis; ADOS: Autism Diagnostic Observational Schedule; ADOS-2: Autism Diagnostic Observational Schedule-2nd edition; BEI = Behavioral Educational Intervention; BSID: Bayley Scales of Infant Development-2nd edition; CARS: Childhood Autism Rating Scale; CCC: Children’s Communication Checklist; CPEP-3: Chinese version of the Psycho-educational Profile-3ard edition; CPM: Raven’s Coloured Progressive Matrices test; DIR = developmental, individual difference, relationship-based; DTT = Discrete Trial Teaching; EOWPVT: Expressive One-Word Picture Vocabulary Test; ESDM = Early Start Denver Model; LIPS-R: Leiter International Performance Scale-Revised; MSEL: Mullen Scales of Early Learning; PECS = Picture Exchange Communication System; PICS: Pictorial Infant Communication Scales; PLS-4: Pre-school Language Scales-4th Edition; RBS-R: Repetitive Behavior Scales-Revised; RCT = Randomized Controlled Trial; RDLS: Reynell Developmental Language Scales; ROWPVT: Receptive One-Word Picture Vocabulary Test; SCQ: Social Communication Questionnaire; SRS: Social Responsiveness Scale; TROG-2: Test for Reception of Grammar-2nd edition; VABS-SE: Vineland Adaptive Behavior Scales-Survey Edition; VABS-II: Vineland Adaptive Behavior Scales-2nd edition.
Study characteristics
The local Institutional Review Board approved all the studies, informed consent was obtained from the participants’ parents.
A summary of the characteristics of the studies can be found in Table 1 and Table 2.
Discussion
We reviewed DTT, PRT, TEACCH, ESDM, EIBI, and PECS interventions to evaluate the effectiveness of these types of approaches on children with ASD. By excluding studies with single group pretest-posttest design and single case studies, this work aimed to identify and evaluate the effectiveness of controlled clinical trials, both RCT and non-randomized or quasi-experimental trials. All the studies that compared the scores of an experimental group with those of a control group were included. Subsequently, controlled studies (n = 11) were distinguished from comparative ones (n = 7). When only examining the controlled studies, the control group received typical treatment methods such as conventional language therapy, parental guidance, intensive family therapy, and social skill training. However, in two of these studies, the control subjects were the same as those on the waitlist. The varying impacts of diverse behavioral therapies are emphasized in the comparative studies. We observed significant effects for general and specific outcomes regarding expressive and receptive language, adaptive behavior, and daily living skills as well as social area skills. For instance, the use of PECS is a technique that only enhances the language domain, yet Lerna et al. (2012, 2014) described positive effects on the overall social area investigated. On top of this, a general improvement in the child’s symptoms and global profile based on the ADOS and Griffiths Mental Development Scales (GMDS) scales was described at the end of the treatment as well as at the follow-up. Anyhow, for an in-depth analysis of the research studies involving the efficacy of all of the programs with Assisted Augmented Communication (AAC) see Ganz (2015 1985), because in our work they have not been included. Significant improvements in overall functioning have also been described by Waters et al. (2020) implementing EIBI. These authors found a significant increase in the global intelligence quotient (IQ) and non-verbal intelligence quotient (NVIQ), underlining the strong impact of the intervention on adaptive behavior. Similar results have also been described by Vivanti et al. (2014) and Colombi et al. (2018) with the application of ESDM. These researchers described an improvement in cognitive functioning but only at the level of receptive language. PRT, like EIBI, involves caregivers of children with ASD and has a positive impact on participants' overall profile. In particular, a significant decrease in symptoms detected through the ADOS and a considerable increase in communication skills, assessed through the Preschool Language Scales (5th Edition, PLS-5), Peabody Picture Vocabulary Test (4th Edition, PPVT-4), and Mullen Scales of Early Learning
In short, the comparative analysis showed that all of the behavioral methods (PECS, EIBI, ESDM, PRT, and TEACCH) are effective in improving social-communicative and linguistic skills. Furthermore, PECS and PRT had direct effects on the cardinal symptoms of the disorder (Schreibman & Stahmer, 2014), while other therapies (EIBI and TEACCH) further enhanced the global adaptive functioning (Mazza et al., 2021). Likewise, comparative studies have highlighted the greater efficacy of intensive interventions. For instance, Zeng et al. (2021) underlined that participants benefit in the linguistic, affective-social, and personal autonomy domains by adding a TEACCH and a DTT intervention to their therapy programs. Similarly, Stanislaw et al. (2020) proved that a highly intensive ABA intervention potentiates the effects on language and social-communicative skills in comparison with a low-intensity ABA treatment combined with other methods. Mazza and colleagues (2021) as well as Sinai-Gavrilov et al. (2020) demonstrated that early behavioral intervention favors the improvement of language skills and interpersonal relational skills as well as the learning of both personal and domestic autonomy.
The authors aimed to highlight effective treatment options and encourage further exploration. One notable finding was that certain behavioral therapies, such as PRT and PECS, which only require 15–40 hours over 6 months, can still significantly improve communication abilities and social engagement. By incorporating these cost-efficient interventions grounded in behavior analysis principles, a foundation can be laid for broader acceptance of such therapies.
Conclusions
In recent years, there has been a significant increase in research focused on conducting randomized controlled trials (RCT). Notwithstanding, our review has revealed that only a handful of studies meet the quality standards due to concerns surrounding low methodological rigor. Consistent with the findings of Sandbank et al. (2020), only 30% of these studies are controlled. Conducting a high-quality study is challenging, involving data collection, protocol compliance, and treatment adherence (Keenan et al., 2010). Nonetheless, behavioral treatments have manifested their effectiveness, and it is crucial to make them more widely available. As such, we strongly urge greater efforts toward applying therapies founded on behavioral principles, which would give ASD patients and their families access to evidence-based treatments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.