
Abstract
Introduction
Eating styles are a complex interplay of multiple factors that influence individual functioning and development (Gahagan, 2012). According to theories conceptualizing eating behaviours as resulting from a misperception of own internal states (Bruch, 1973; Herman & Polivy, 1980; Schachter & Rodin, 1974), empirical research refers to three eating styles in which eating is a response to emotional and external cues: emotional, external, and restrained eating. Emotional eating (EE) indicates the tendency to excessive eating in response to an affective state (Bruch, 1964), external eating (EX) refers to the tendency to eat in response to environmental stimuli, regardless of the internal state of hunger or satiety (such as the taste or smell of food; Schachter & Rodin, 1974) and restrained eating (RE) indicated a restrictive control over eating struggling against hunger sensations (Herman & Polivy, 1980). Individual eating styles significantly impact physical and mental health in the short and long run, and adverse outcomes include weight gain (Koenders & van Strien, 2011; Lowe et al., 2013), weight loss (Herle et al., 2018) and dysfunctional eating patterns, such as overeating, excessive dieting, and binge eating (BE; Burton & Abbott, 2019; Cella et al., 2022; Sultson et al., 2017). It is also noteworthy that childhood eating habits can persist into adulthood, potentially shaping adult eating behaviors and health (Małachowska & Jeżewska-Zychowicz, 2021) and contributing to the risk of developing conditions like cardiovascular disease (e.g., Kaikkonen et al., 2013) and full-syndrome eating disorders (Herle et al., 2018).
Childhood is a critical stage for developing eating styles, as they might persist into adolescence and adulthood (Scaglioni et al., 2018). Although children demonstrate self-regulation mechanisms for food intake from an early age (Birch & Fisher, 1998), their attitudes and behaviors towards food are largely shaped within the early mother-child relationship, where food symbolizes love, security, and satisfaction (Bruch, 1941). There is a substantial amount of evidence supporting the relationship between maternal control and children’s eating styles. Overly controlling feeding practices have been shown to impact children’s developing eating behaviours and weight status (e.g., DeCosta et al., 2017; Shloim et al., 2015). For instance, cross-sectional research has demonstrated that children with controlling parents are more likely to exhibit EE, EX, and RE (van Strien & Bazelier, 2007). Likewise, longitudinal studies have indicated that children subjected to maternal controlling feeding practices tend to eat in absence of hunger two years later (Farrow et al., 2015). Furthermore, a prospective study on young children demonstrated that maternal control and food restriction were associated with developing obesogenic eating behaviors, such as EE and a tendency to overeat (Rodgers et al., 2013). However, further research is required to delve into the controlling dimension of parenting. Maternal psychological control, defined by intrusiveness, guilt-induction, and manipulation (Barber, 1996), is critical in children’s development (Barber & Harmon, 2002). In her psychosomatic theory, Hilde Bruch, (1973) was the first to support such a relation, suggesting that maternal attitudes characterized by overprotection (i.e., control) seriously affect child’s emotional development and food habits. In such a disturbed environment, the food serves not only the child’s biological needs but is highly endowed with emotional value. The mother-child interaction is an emotional and affectional experience surrounding nutrition throughout life. A mother not attuned to her child’s needs may limit the development of accurate perception of hunger and satiety sensations, offering food in response to no-nutritional needs. In this sense, a controlling mother may preclude the development of a sense of personal needs, preventing the child from recognizing his/her own bodily sensations and confusing them with affective and interpersonal problems (Bruch, 1971). Thus, children may grow up not owning their own bodies, lacking awareness about their bodily signals and urges and being poorly equipped with adequate emotion regulation abilities (Bruch, 1941). Research has consistently highlighted a significant correlation between psychological control and difficulties in emotional regulation (Cui et al., 2014; Morris et al., 2017; Van Lissa et al., 2019). In addition, awareness of bodily signals is a precondition for effective self-regulation and emotional processes (Füstös et al., 2013; Herbert et al., 2012). Specifically, maternal psychological control showed unique effects on emotion dysregulation (Luebbe et al., 2014). Similarly, mothers’ control predicted children’s poorer emotional functioning over time (Cheung et al., 2016). Deficits in the ability to adequately regulate emotions have also been recognized as predictors of maladaptive eating behaviours, such as EE, EX, and BE (Aparicio et al., 2016; Czaja et al., 2009; Harrist et al., 2013; Weinbach et al., 2018).
Emotion regulation difficulties play an important role in developing and maintaining dysfunctional eating behaviours (e.g.; Cella et al., 2022; Warne et al., 2022). Emotion dysregulation can manifest in several ways, including impulsivity, difficulty identifying and labelling emotions, and using maladaptive coping strategies (Sheppes et al., 2015). Empirical research suggests that difficulties in identifying and expressing emotions (i.e., differentiating emotions) may contribute to developing dysfunctional eating habits (Williams-Kerver & Crowther, 2020). Individuals struggling to differentiate emotions tend to engage in unhealthy eating behaviors and exhibit more dysfunctional eating habits, such as BE and EE (Larsen et al., 2006; Lavender et al., 2016). Conversely, those with better emotion differentiation abilities display healthier eating patterns (Katterman et al., 2014). Most existing studies (e.g., Spettigue et al., 2020; Svaldi et al., 2019) have primarily focused on adolescents and adults from clinical samples, examining dysfunctional eating habits with less focus on eating styles. Hence, the relationship between emotion differentiation and eating styles among children remains understudied.
Considering that psychological control has been linked to difficulties in emotion regulation abilities and the connection between emotion dysregulation and dysfunctional eating habits has been well-established, it prompts the question of whether emotion dysregulation mediated the pathway from maternal psychological control to eating styles.
The present study
According to the literature reviewed (e.g., Bruch, 1971), maternal psychological control and children’s emotion dysregulation have been linked to eating styles in children. However, an important question remains whether the child’s emotion dysregulation mediates the relationship between maternal psychological control and eating styles. Specifically, we consider the difficulties in differentiating emotions as a putative mediator in such a relationship. Based on these assumptions, we hypothesized a direct relationship between all study variables. Regarding indirect effects, we hypothesized that emotion differentiation difficulties significantly mediate the relationship between maternal psychological control and each eating style (EE, EX and RE).
Materials and methods
Participants and procedure
Participants were 324 elementary school children recruited from schools located in Southern Italy. The present study is part of a larger research project involving children’s eating styles. After receiving approval from schools’ headmasters, students were invited to participate via a letter addressed to their parents. Those who received active parental informed consent and provided oral assent were partaken in the study. Due to the restriction imposed by the prevention measures for the spread of COVID-19, data collection was conducted online through the Microsoft Teams platform. Children received a link to an online survey hosted on the Survey Monkey web site. The questionnaires were completed during regular school hours under the supervision of a research assistant. The administration took about 40 minutes. To protect the confidentiality, a unique code was derived for each individual who participated in the study. All procedures were in accordance with the Declaration of Helsinki and its later amendments (World Medical Association, 2013) and approved by the Ethic Committee of the host institution.
Measures
Participants completed a booklet of questionnaires.
Socio-demographic sheet
Participants completed a socio-demographic sheet collecting age and gender.
Maternal psychological control
The Psychological Control Scale–Youth Self-Report (PCS-YSR; Barber, 1996) is an 8-item measure assessing psychological control. Participants answered for their mother using a 3-point Likert scale ranging from 1 (“not like her”) to 3 (“a lot like her”). The questionnaire has demonstrated good psychometric properties (Barber, 1996). Internal consistency in the current study was α = .57.
Differentiating emotions
The Emotional Awareness Questionnaire (EAQ; Camodeca & Rieffe, 2013; Rieffe et al., 2007) is a 30-item self-report questionnaire measuring six key aspects of emotion awareness: (1) differentiating emotions; (2) verbal sharing of emotions; (3) not hiding emotions; (4) bodily awareness of emotions; (5) attending to others’ emotions; and (6) analyses of (own) emotions. Items are rated on a 3-point Likert scale from 0 (“Not true”) to 2 (“Often true”). Higher scores indicate a higher presence of the corresponding ability. We only used the differentiating emotions scale (α = .74) for the study. The measure has demonstrated strong validity and reliability (Camodeca & Rieffe, 2013).
Eating styles
The Dutch Eating Behaviour Questionnaire for Children (DEBQ-C; van Strien & Oosterveld, 2008) is a validated self-report measure assessing child’s eating styles: EE, EX, and RE Participants answered each item on a 5-point Likert scale from 1 (“Never”) to 5 (“Very often”). Averaging each subscales’ items yields three total scores, with higher scores indicating more severe disordered eating behaviours. The measure has shown good psychometric properties (van Strien & Oosterveld, 2008). In the current study, Cronbach’s alpha was .84 for EE, .62 for EX, and .66 for RE.
Body mass index
Information about weight and height was collected by parents to derive the body mass index (BMI). BMI was calculated and transformed into age- and sex-specific z-scores according to the World Health Organization BMI-for-age growth charts (WHO, 2023).
Data analysis
Descriptive statistics were conducted by means of the IBM Statistical Package for the Social Sciences (SPSS v.26; IBM Corp, 2019). Means, standard deviations, and frequency were computed for all study variables. A path analysis was conducted using maximum likelihood (ML) estimation with the R package “lavaan” (Rosseel, 2012) to estimate the relationship between maternal psychological control, difficulty in differentiating emotions and eating styles (EE, EX, and RE). Age, gender and BMI-for- age were included as covariates to control their effect. To evaluate the model fit, the following indices were used: (a) the Chi-square statistic (χ2), which should not be significant (Barrett, 2007); (b) the Root Mean Square Error of Approximation (RMSEA); (c) Standardized Root Mean Square Residual (SRMR); (d) the Comparative Fit Indices (CFI); (e) the Tucker-Lewis index (TLI). CFI and TLI values greater than .90, and SRMR and RMSEA values of less than .08 are deemed representative of an acceptable model (Hu & Bentler, 1999). The bias-corrected bootstrap confidence intervals for product terms (5000 repeated sampling) were used to test for significant indirect effects (Preacher & Hayes, 2008). According to Hayes (2013), an indirect effect is deemed statistically significant when the bootstrap confidence interval within the lower and the upper bound (95%) does not include zero. Finally, a multigroup analysis (ML estimator) was conducted to test measurement invariance between genders, while age and BMI-for-age were entered as covariates. The Chi Square Difference Test (∆χ2) was used to test for differences, comparing a model in which all regression coefficients are freely estimated and a constrained model in which parameters are forced to be equal between groups.
Results
Participants characteristics
Participants characteristics.
Means, standard deviations, correlation coefficients and reliability estimates (cronbach’s alpha) of the study variables.
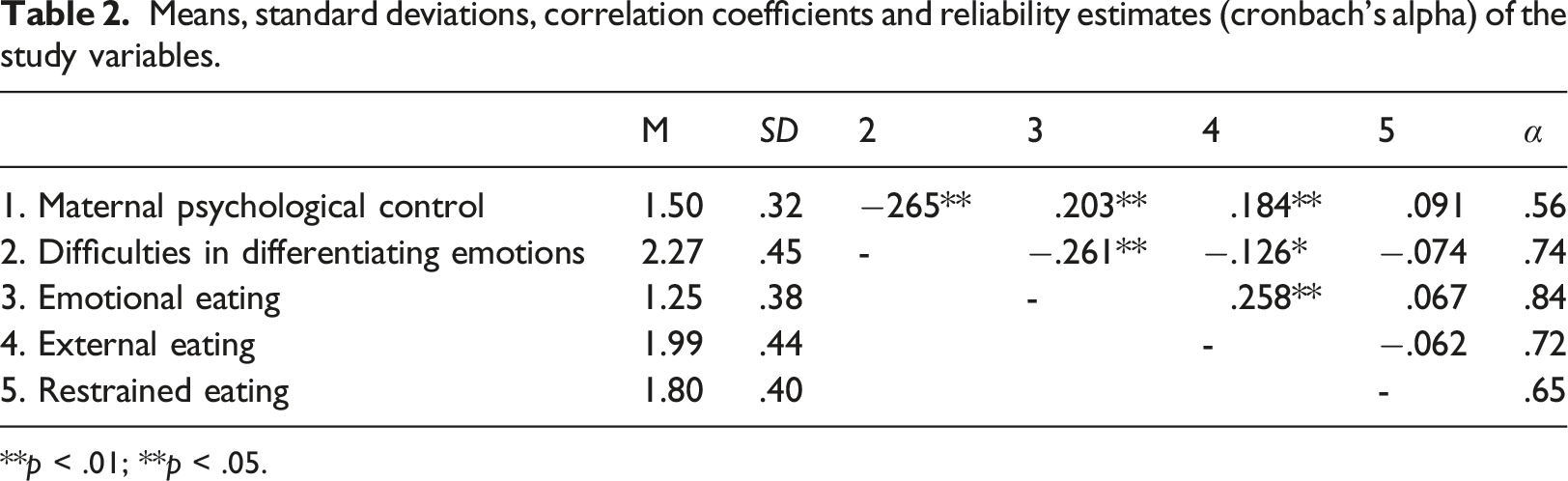
**p < .01; **p < .05.
Path analysis
The model tested showed an acceptable fit to the data (χ
2
(3) = 3.966, p = .256; RMSEA = .032; CFI = .990; TLI = .911; SRMR = .018). All the direct paths from maternal control to eating styles were statistically significant, except for the path toward RE (β = −.880, p = .379). Also, maternal control was significantly related to difficulties in differentiating emotions (β = −4.664, p < .001). Out of the eating styles included in the model, EE was the only one significantly associated with emotion differentiation difficulties. Based on the bootstrap resampling method, difficulties in differentiating emotions significantly mediated the relationship between maternal control and EE (β = 3.198, 95%CI [.033, .118]; p = .001). More details are reported in Figure 1. Regarding invariance across gender, results showed a non-significant effect (∆χ
2
(15) = 12.732; p = .623) for comparison of models, suggesting that variables’ interplay operated similarly across gender. Standardized path coefficents.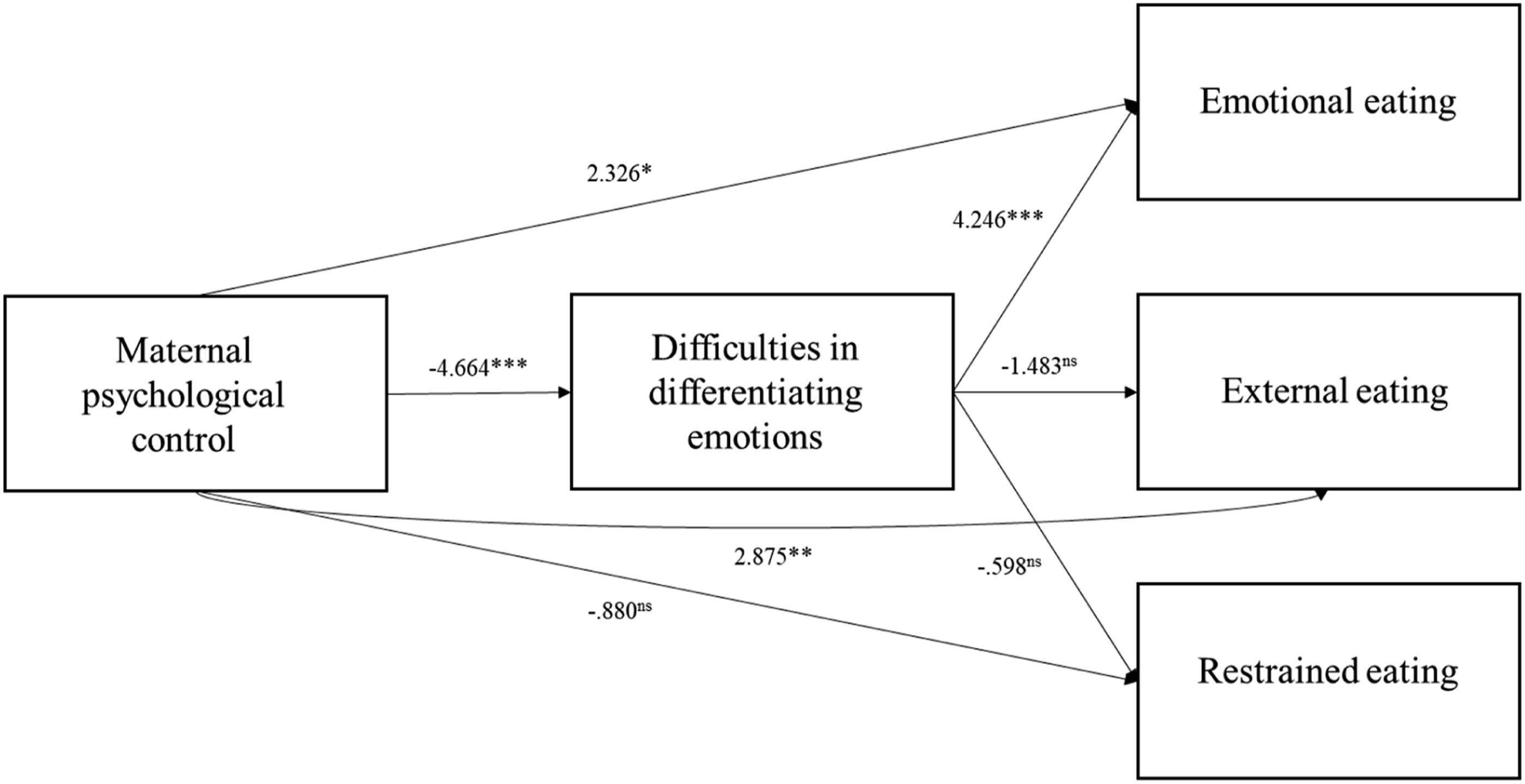
Discussion
The present study investigated the mediating role of difficulties in differentiation emotions between maternal psychological control and eating styles within a sample of Italian children aged between 8 and 11 years old. Partially confirming our hypotheses, maternal psychological control was directly associated with EE, whereas no significant associations were found with EX and RE. Also, maternal psychological control indirectly affected EE via difficulties in emotion differentiation. These findings indicate that a controlling mother and a deficiency in differentiating emotions may work together to explain the eating style among children and have important implications for future research and practice.
Consistent with previous literature (Escobar et al., 2014), the mother-child relationship quality was directly related to EE. However, the direct path was not observed for EX and RE. Therefore, other dimensions of the mother-child interaction may influence such habits. For example, Francis and Birch (2005) found that maternal preoccupation influences daughters’ RE. Moreover, children who perceived more maternal encouragement to be thin and weight concerns reported higher RE (Anschutz et al., 2009). On the other hand, maternal feeding practices (e.g., the reward for behaviour and lower covert restriction) were prospectively associated with food responsiveness (i.e., eating in response to external food cues; Jansen et al., 2018). Also, eating in response to external cues was associated with high maternal control in feeding (Morrison et al., 2013).
The direct path between maternal psychological control and EE is in line with previous studies that found similar link across different age groups. For example, within their integrative model of BE risk in adolescence, Cella et al. (2022) demonstrated that an overprotective maternal parenting (i.e., control and intrusiveness) was directly associated with EE. Also, young adults who experienced a lower quality of maternal care during infancy were more likely to show emotional overeating (Ergang et al., 2019).
Additionally, maternal psychological control indirectly affected EE, operating via difficulties in differentiating emotions. The mediating role of emotion dysregulation has long been acknowledged. Vandewalle et al. (2014) demonstrated that a rejecting mother influences youngster’s EE through maladaptive emotion regulation strategies. Similarly, emotion suppression and difficulties in identifying emotions perceptively mediate the relationship between lower parenting quality in infancy and EE during adolescence (van Strien et al., 2019). Theoretical accounts and empirical research suggest that the family environment plays a crucial role in the development of emotion regulation skills, which are also important for healthy psychological functioning (Bruch, 1964; Morris et al., 2007). Positive parenting has been related to mature emotional expression, while experiencing intrusive control is strongly related to difficulties in differentiating and regulating emotions (Morris et al., 2013). Studies have demonstrated that maternal psychological control can interfere with the development of effective emotion regulation abilities in children (Graziano et al., 2010), leading to increased emotion dysregulation and internalizing and externalizing problems (Braet et al., 2014). This may be because parental control can prevent children from learning to identify and express their emotions, making it difficult to regulate them healthily and adaptively. So, by preventing the development of more adaptable emotion differentiation abilities, maternal psychological control may trigger EE. According to the psychosomatic theory (Bruch, 1973), a mother unable to adequately respond to her child’s emotional needs, by a stereotyped use of food as a tool to handle any distress, may impede the child from developing into a separate, self-reliant, and independent being. Excessive and inappropriate feeding rooted in prolonged overprotection and control disrupts the growing-up process, as children may lack identity and personal needs. In such an environment of emotional chaos, the symbolic significance of food may underlie perceptual and conceptual confusion (Bruch, 1964). Specifically, children cannot recognize and differentiate their needs, confusing their own emotional and physical demands (i.e., hunger and satiety) due to the continued abundance of nourishment and protection (Bruch, 1941). It has been suggested that parents who actively engage in teaching their children about emotions (recognizing, labelling, expressing, and managing emotions) may facilitate their child’s emotional development and self-regulation (Anderson & Keim, 2016; Gottman et al., 1996). Thus, we could hypothesize that a high level of intrusiveness impedes the appropriate process of self-management, such that children do not learn the appropriate appetite regulation abilities (i.e., eating in response to hunger cues and not eating beyond fullness) and rely on misleading internal cues to initiate and terminate eating. Emotional states, physiological arousal and overwhelming experience are confused with hunger and satiety signals and lead the child to eat in response to such emotional stimuli.
Limitations and future directions
Although the present study provided an incremental understanding of the underlying mechanisms linking maternal psychological control and eating styles in children, some limitations should be addressed. Firstly, our sample included only Southern Italian children. Although there is a paucity of studies exploring such relationships, we cannot generalize these results to other populations. Future research should continue exploring them among more diverse sample. Also, studies involving a clinical sample of children are needed. Second, the cross-sectional design of this study prevents claims regarding temporal ordering of the variables. As such, future research could use a longitudinal and cross-lagged design to detect directionality and temporality between maternal control, emotion differentiation difficulties and children’s eating styles. Third, the assessment was limited to self-report measures, which could increase the associations among the variables due to shared method variance. Fourth, our results rely on child’s perception of maternal psychological control. It could be useful to include parent-reports and take potential discrepancies into account. Thus, future studies could benefit from using a multi-method (e.g., interview, experiments) and multi-informant (e.g., parents) assessment. Additionally, observational assessments of parent-child interactions would strengthen future research. Fifth, children’s BMI was reported by parents rather than mechanically measured. Information on other sociodemographic characteristics that may be important to consider (e.g., socioeconomic status, family climate, child health and medical problem) was not collected. Future research should consider the potential impacts of such variables. Lastly, as selection bias cannot be controlled (parents agreed for their children participation), our results should be interpreted with caution.
Implication
Our findings have important clinical and practical implications. Eating in response to emotional states has been acknowledged as an obesogenic trait which significantly contributes to dysfunctional eating habits, such as BE (Cella et al., 2022), weight gain and obesity in both youth and adults (Dakanalis et al., 2023; Frayn & Knäuper, 2018). Moreover, emotional eating is associated with common symptoms (e.g., BE, loss of control over eating; Cella et al., 2022; Goossens et al., 2007) within the eating disorder psychopathology (i.e., BE disorder and bulimia nervosa; American Psychiatric Association, 2013). Therefore, understanding underlying mechanisms that drive EE among children may help clinical practice in the management of risk factors that are more proximal to the onset of eating disturbances and be useful to avoid detrimental pathways to more severe psychological and health conditions (e.g., noncommunicable diseases associated with unhealthy eating habits). From a practical perspective, our findings suggest that a mother’s excessive interference and intrusion into her child’s emotional and psychological well-being, known as maternal psychological control, can negatively impact the child’s eating habits. The study emphasizes the significant role of a child’s capacity to regulate their emotions in order to manage negative feelings and make healthy food choices. As a result, practitioners should offer mothers appropriate support and guidance, focusing on their parenting style and their child’s emotional regulation skills, to establish effective preventive strategies as early as possible. Additionally, our findings stress the necessity of identifying and intervening with children at risk of developing problematic eating behaviours at an early stage. It is important for healthcare professionals, such as paediatricians, psychologists, and nutritionists, to receive training in recognizing early signs of risk and providing appropriate interventions and support to children and their families. Early intervention starting from childhood can aid in the development of a child’s identity and understanding of personal needs, ultimately influencing healthy behaviour choices.
Conclusions
Despite the limitations above, the present study adds to the extant literature by exploring the relationship between maternal psychological control, deficits in emotion differentiation and EE among children. Awaiting further research, our findings have important clinical and practical implications. The results offer empirical support for etiological models (e.g., Bruch, 1973) purporting the importance of mother-child interaction in enhancing the risk for dysfunctional eating style during infancy, also showing that the quality of such dyadic relationship has an indirect effect via difficulties in differentiating emotions. Contextualizing our results within the psychosomatic framework (Bruch, 1973), EE may express emotional difficulties generated within the mother-child relationship. Additional research is required to further explore and understand the variables’ interplay in the manifestation of EE among children, a critical next step in advancing this line of research.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.