
Abstract
Low- and middle-income countries face heterogeneity in the way clinicians’ approach Autism Spectrum Disorder (ASD) diagnosis and treatment. The current study analyzes the diagnostic tools, laboratory tests, pharmacological and psychosocial interventions received by patients during the steps to diagnosis and treatment of two specialized care centers. Researchers interviewed families with a child with ASD receiving services at either a child psychiatric or a pediatric hospital. Of the total sample, 47% reported clinicians not using a diagnostic tool, 20% reported not receiving any psychosocial intervention, and 88% reported receiving a pharmacological prescription. Patients at the pediatric hospital were more likely to receive interventions with some components of Applied Behavioral Analysis, Early Start Denver Model, Treatment and Education of Autistic and Related Communication Handicapped Children, and Sensory integration therapy; while patients at the psychiatric hospital were more likely to undergo learning, daily living skills, and socialization therapies. Patients at the psychiatric hospital received significantly more requests to obtain auditory and vision tests whilst genetic testing and imaging were more common in the pediatric hospital. The range and variability in terms of diagnostic tools, laboratory tests, and treatment options observed for both sites reflect a lack of consensus. Recommendations to improve ASD diagnostic and treatment in Mexico are given.
Individuals with Autism Spectrum Disorder (ASD), often face psychosocial disabilities throughout their lifespan, which negatively affect their quality of life (Moyal et al., 2014). Diagnosis and treatment remain a challenge. Considerable diagnostic delays (Davidovitch et al., 2015; Zavaleta-Ramírez et al., 2020) and limited access to specialized therapeutic services have been reported worldwide (Bishop-Fitzpatrick & Kind, 2017). Care of ASD patients implies personalized interventions throughout the life span, representing significant social and financial costs for individuals, families and society (Buescher et al., 2014).
Clinical guidelines for ASD aim to standardize the complex process of diagnosis and treatment, which involves an extensive network, spanning from assessment tools, psychosocial interventions for the core symptoms and pharmacological treatment for comorbidities (Crowe & Salt, 2015; Volkmar et al., 2014). However, in practice, adherence to guidelines may vary among countries, care centers, or even between staff and medical specialties within the same center. For example, in the United States, Tchaconas and Adesman (2017) found that 76% of the clinicians in their study sample (neurologist or developmental-behavioral pediatricians) selected at least one inappropriate genetic test when presented with hypothetical ASD cases. The neuro pediatricians asked more frequently for electroencephalogram (EEG) tests and magnetic resonance imaging (MRI) scans in comparison with behavioral and developmental pediatricians. Although pediatricians are the first point of contact for parents, they often overlook the first ASD symptoms (Mandell et al., 2007). For example, in 2007 the American Academy of Pediatrics recommended to routinely screen for ASD (Johnson & Myers, 2007), yet results from a 2012 survey of primary care pediatricians showed that only 8% of them did so (Autism and Developmental Disabilities Monitoring Network Surveillance Year 2008 Principal Investigators, 2012). More recently, also in the United States, Wallis et al. (2020) found low rates of follow-up interview completion and children referral after positive ASD screening with the Modified Checklist for Autism in Toddlers - Revised with Follow-Up (M-CHAT-RF) in a primary care network. This indicates that ASD symptoms continue to be overlooked.
Furthermore, studies of adherence to clinical guidelines in ASD mainly come from high-income countries and may not reflect the challenges faced by those countries with disadvantaged economies (Frakking et al., 2022; Palmer et al., 2011; Rutherford et al., 2016). For instance, in Mexico, while guidelines that align with international clinical standards for the diagnosis and treatment of ASD are available (Secretaría de Salud, 2012) the applicability in local clinic settings remains low. Specifically, these guidelines suggest inaccessible and unfeasible assessment tools that are expensive, not culturally adapted, lengthy to administer and require extensive training (e.g., Autism Diagnostic Interview-Revised [ADI-R], Autism Diagnostic Observation Scale [ADOS], Diagnostic Interview for Social and Communication Disorders [DISC]). Previous reports have shown that reduced availability and experience of trained staff, constrained budgets of clinical institutions, and large out-of-pocket costs for families are factors that affect how ASD patients are diagnosed and treated in low- and middle-income countries (Zavaleta-Ramírez et al., 2020). Mexico, though classified as a middle-to high-income country by the World Bank (https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html), still has large inequalities across regions in terms of access to health care services (Gutierrez et al., 2014). In regards to ASD, a recent study showed that only 1% of care units in Mexico have human resources and equipment to provide interventions for socio-communicative deficits (Zavaleta-Ramírez et al., 2018). The current study analyzes the diagnostic tools, laboratory tests, pharmacological and psychosocial interventions received by ASD patients during the steps to diagnosis and treatment. We report these values for two specialized care centers, a psychiatric and a pediatric hospital, that offer services of diagnosis and intervention for ASD.
Methods
Sample and procedure
We included 197 parents that participated in a previous study of a detailed pathway to ASD diagnosis (Zavaleta-Ramírez et al., 2020). The father’s mean age was 38.0 years (SD = 7.3), mother’s mean age was 35.1 years, (SD = 6.8). Only 45% of parents completed high school while 41% reported having obtained a bachelor’s degree. Around three quarters of the families (72%), had a monthly income of 323 United States dollars (ca. 6,000 Mexican pesos) or less. At both sites, ASD patients were predominantly male (87% and 88% pediatric and psychiatric, respectively). Patients at the psychiatric hospital were slightly older (mean = 8.9, SD = 3.6) than those at the pediatric hospital (mean = 7.1, SD = 2.7).
Clinical sites
The child psychiatric hospital “Juan N. Navarro” is a specialized center located in Mexico City. Child psychiatrists and psychologists’ offer diagnosis and treatment options, while neurologists and a geneticist oversee neurological and genetics comorbidities. Laboratory tests at this center are somewhat limited, but EEG tests are available. The hospital mainly treats patients from Mexico City and surrounding metropolitan areas. In the specific case of ASD, the hospital provides cognitive, physical, sensorial and speech therapies.
The pediatric hospital is located in Tuxtla Gutiérrez, Chiapas, a state in southern Mexico. A small team of psychologists and one child-adolescent psychiatrist provide diagnosis and treatment options, while pediatric subspecialists including a geneticist oversee all other medical specialties. This center has high-cost diagnostic tests, including MRI, EEG, genetic testing and audiometry. This hospital receives patients from both urban and rural areas. In the specific case of ASD, patients are not treated in-house but instead referred to state-run rehabilitation services at a different, but closely located, center (the National System for Integral Family Development or DIF, for its acronym in Spanish).
An important contrast to highlight among these locations is the rate of psychiatrists per inhabitants; while Mexico City has a rate of psychiatrists of 20.73 per 100,000 inhabitants; Chiapas has only .57 psychiatrists per 100,000 inhabitants (Heinze et al., 2016).
Tools
We used the Interview for Seeking Autism Resources in Children (I-SEARCH) developed by the authors and used in a previous study (Zavaleta-Ramírez et al., 2020). The interview is composed by 43 items arranged in three sections: (a) the sociodemographic characteristics of the child and caregivers, (b) a detailed chronological order of the diagnostic pathway which includes all professionals and clinical sites visited while parents sought a diagnosis for the child; this section also includes questions about diagnostic tools, laboratory tests, pharmacological and non-pharmacological interventions prescribed by the clinician and (c) questions related to the overall parents’ satisfaction with the diagnostic process. The full interview takes around 40 min to an hour to complete.
Statistical analysis
We provide descriptive statistics using frequencies and percentages, mean and standard deviation (SD), or medians and interquartile ranges (IQR). We compared diagnostic tools, laboratory tests, medications and psychosocial interventions between the two sites using a series of Chi-square tests and Fisher’s exact test when frequencies in at least one of the cells were small (<5). For each comparison, we report the corresponding confidence intervals and the odds ratio. Significance was set at p < .05. We used the statistical software R (R Core Team, 2018) to perform the analyses.
Ethical statement
Participants signed a consent form before starting the interview. The ethical review board approved procedures of both clinical centers.
Results
Diagnostic Tools and Screening Scales Reported for ASD Diagnosis.
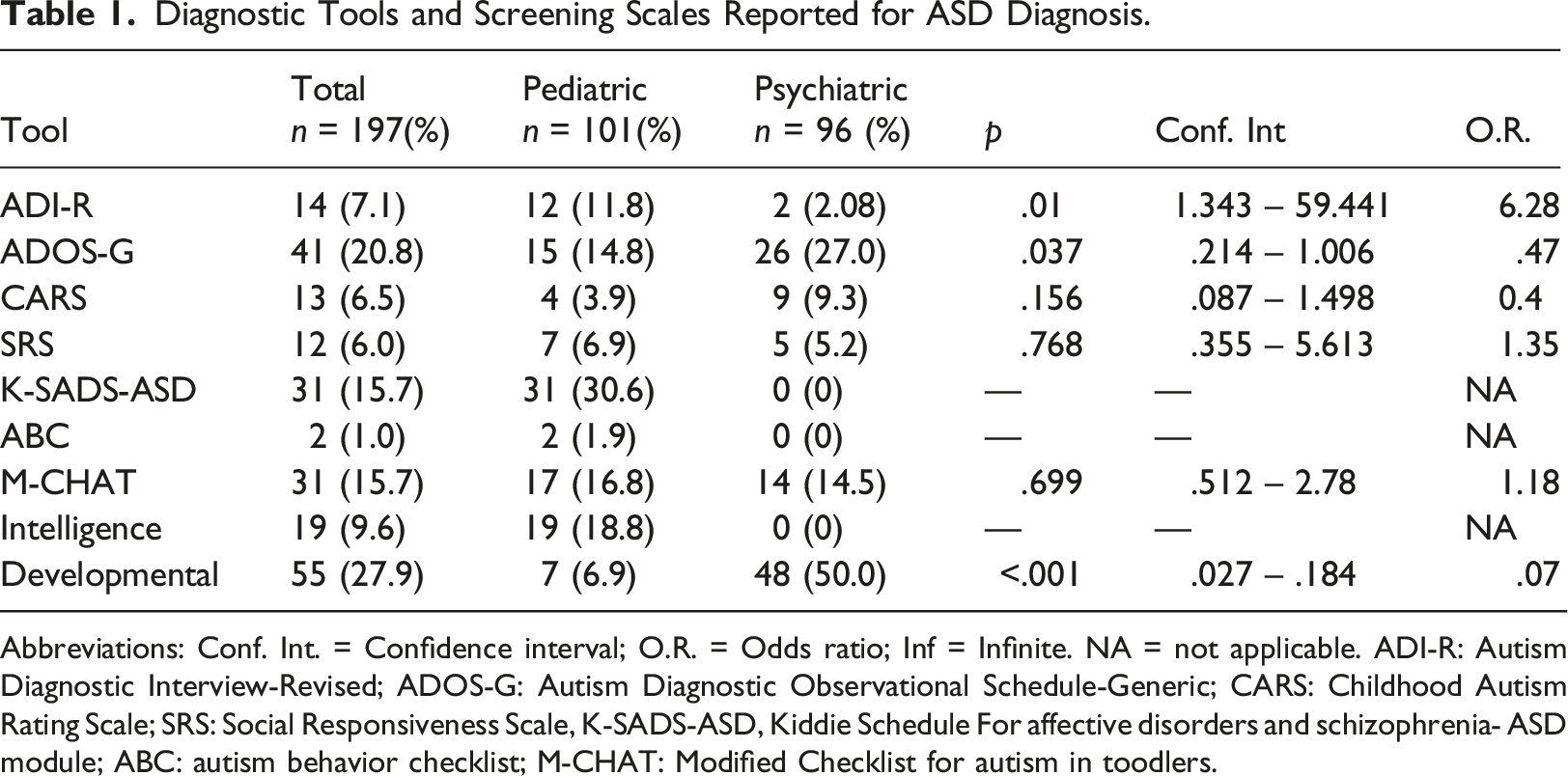
Abbreviations: Conf. Int. = Confidence interval; O.R. = Odds ratio; Inf = Infinite. NA = not applicable. ADI-R: Autism Diagnostic Interview-Revised; ADOS-G: Autism Diagnostic Observational Schedule-Generic; CARS: Childhood Autism Rating Scale; SRS: Social Responsiveness Scale, K-SADS-ASD, Kiddie Schedule For affective disorders and schizophrenia- ASD module; ABC: autism behavior checklist; M-CHAT: Modified Checklist for autism in toodlers.
Laboratory Tests Requested in Children With ASD.
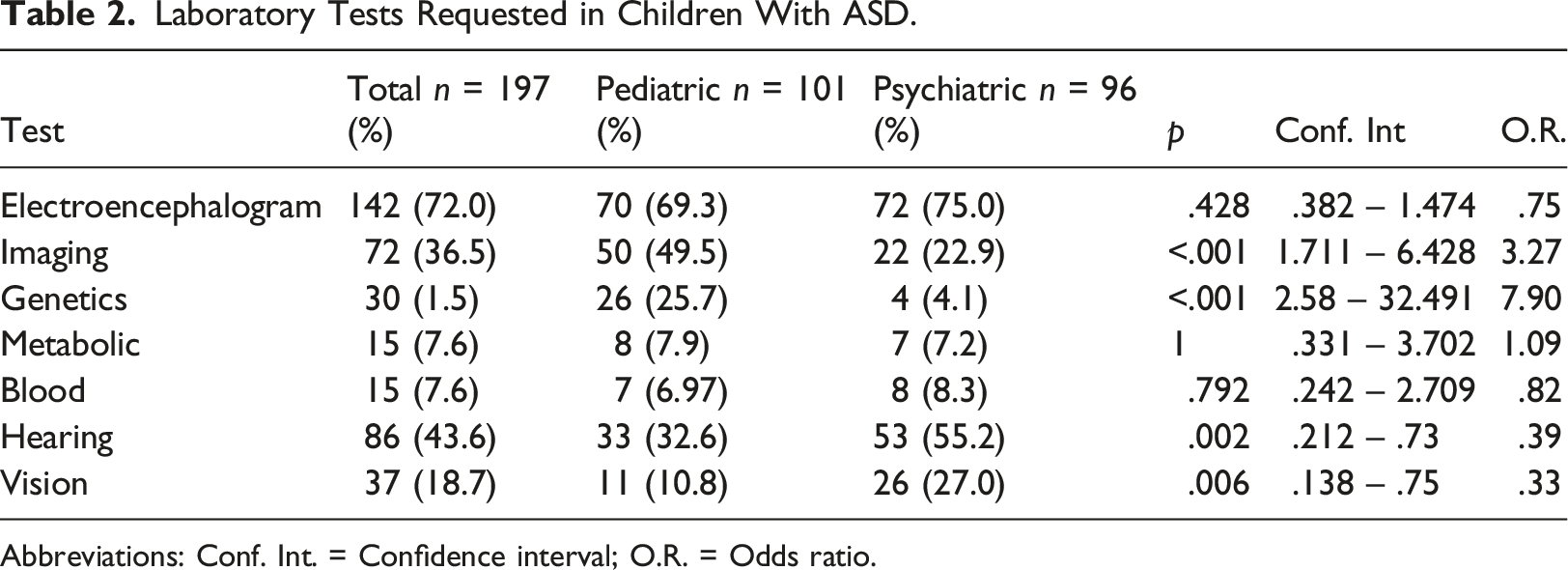
Abbreviations: Conf. Int. = Confidence interval; O.R. = Odds ratio.
Medications Prescribed in Children With ASD.
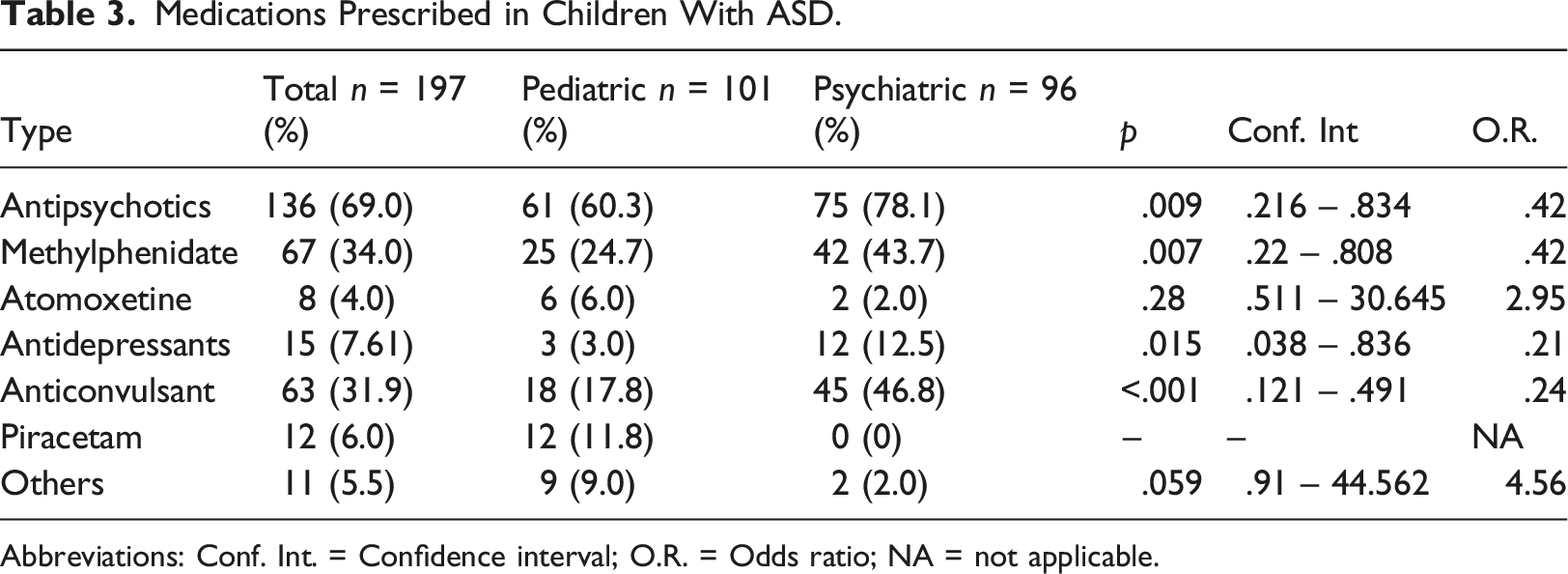
Abbreviations: Conf. Int. = Confidence interval; O.R. = Odds ratio; NA = not applicable.
Psychosocial Interventions in Children With ASD.
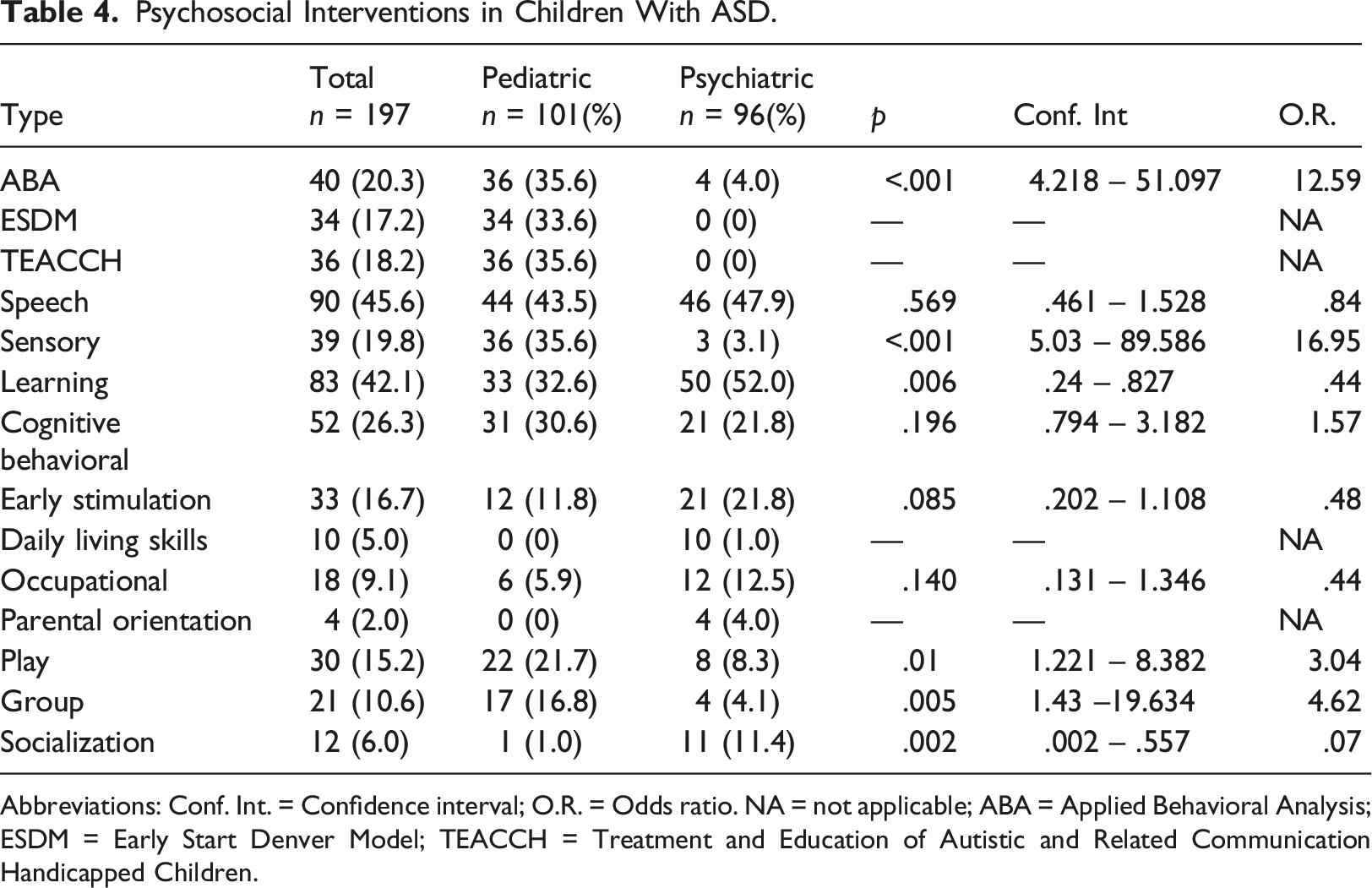
Abbreviations: Conf. Int. = Confidence interval; O.R. = Odds ratio. NA = not applicable; ABA = Applied Behavioral Analysis; ESDM = Early Start Denver Model; TEACCH = Treatment and Education of Autistic and Related Communication Handicapped Children.
Discussion
Diagnostic tools
In terms of diagnostic tools, we found considerable heterogeneity reflecting differences in the array of trained staff available and patient care models between both sites. While the first impression may show an apparent lack of consensus, international clinical guidelines do not favor any particular tool. Hayes et al. (2018) reviews the use of diagnostic tools in the United Kingdom and suggests a range of tools without explicitly recommending any particular measure. Both the American Academy of Child and Adolescent Psychiatry (AACAP; Volkmar et al., 2014) and the National Institute for Health and Clinical Excellence (NICE; Crowe & Salt, 2015) guidelines recommend the use of a semi-structured interview and observation to guide the clinicians’ criteria for ASD. Hathorn et al. (2014) suggests that if the referring child development clinicians adheres to guidelines, the specialist diagnostic services can expect to confirm an ASD diagnosis on the same day of assessment in over half of cases. If any aspect of a clinical guide may lower the delay to diagnosis, these should be promptly adopted.
One of the reasons for the apparent non-adherence to a particular set of assessment tools in Mexico could be that local ASD clinical guidelines recommend tools that require training for appropriate use (Secretaría de Salud, 2012). The expenses of using gold standard instruments such as ADI-R and ADOS for diagnosing ASD is a limitation in low- and middle-income countries (De Vries, 2016). The only international gold standard validated measure for ASD diagnosis in Mexico is the CARS (Flores-Rodríguez et al., 2022) and the M-CHAT for screening (Albores-Gallo et al., 2012). Availability of brief, culturally validated, inexpensive tools could increase their use among Mexican clinicians. Currently there are two free access tools for ASD screening and diagnosis, developed and validated in Mexican samples: the Valoración del Espectro Autista en Niños Hispanos (VEAN-Hi; Albores-Gallo et al., 2016) and the Entrevista de Criterios Diagnósticos del Trastorno del Espectro Autista (CRIDI-ASD interview; Albores-Gallo et al., 2019), which are yet to be incorporated into local clinical guidelines. Larger efforts to disseminate these tools than those done so far are needed to convince policy makers to incorporate them in the next publication of the Mexican clinical guidelines.
Laboratory tests
The most frequently requested test was EEG (72%). The European Society for Child and Adolescent Psychiatry guideline (Fuentes et al., 2021) recommends these tests to rule out epilepsy and seizures. Similarly, tests to rule out hearing or vision abnormalities are crucial as individuals with ASD show hyperacusis and peripheral audiological dysfunction with a higher rate than their typically developing peers (Demopoulos & Lewine, 2016; Tas et al., 2007). Sensorial loss, hypersensitivity to sound, and otitis are examples of other auditory conditions often associated with ASD (Stiegler & Davis, 2010). Along the same lines, ophthalmologic dysfunction is around three times higher in children with ASD than in typically developing controls (Chang et al., 2021). It is worrisome that only a minority of the sample of the pediatric hospital had hearing and ophthalmologic assessments, although in the psychiatric hospital the percent of the sample was higher. Formal vision and hearing tests are important to discard visual and/or auditory issues in ASD. In our study, clinicians at the pediatric hospital may be relying on a previous newborn hearing screening rather than referring patients for a formal test. A possible explanation for the higher rate of audiological issues seen at the psychiatric hospital ASD clinic is that the pathway to diagnosis often begins after parents are referred by a phonology specialist.
Of note is that genetic testing was requested in only 1% of the sample, mostly in the pediatric hospital given the availability of laboratory tests. Genetic factors have a meaningful role in the etiology of ASD, with recent studies showing 80% heritability (Tick et al., 2016). The AACAP guidelines recommend genetic testing, such as G-banded karyotype, fragile X testing, or chromosomal microarray (Volkmar et al., 2014). Detecting a genetic etiology of ASD allows the clinicians to put together a targeted management plan for the medical manifestations of the syndrome as well as counseling about prognosis and recurrence risk (Hyman et al., 2020). While they can be extremely informative, these tests are not widely available due to high costs. Mexican regulations stipulate narrow metabolic screening in public health institutions, despite broader metabolic testing already screening for over 60 conditions that may relate to ASD. However, the latter is only available at private hospitals. A cost benefit analysis should be included in future modifications of our interview, the I-SEARCH, to evaluate their influence of the tests’ outcome on the diagnostic delay.
Medications
We found a higher use of medication compared to other countries. Different studies found that 29%–70% of ASD patients received at least one medication for treatment (Frazier et al., 2011; Hsia et al., 2014). In our study, the frequencies of prescription of antipsychotics were higher than samples in the United States, even when compared with Hispanics patients (Quebles et al., 2020). The most frequently antipsychotic prescribed was risperidone in both sites, which is in line with clinical practice guidelines for the treatment of irritability and disruptive behaviors (Crowe & Salt, 2015; Fuentes et al., 2021; Volkmar et al., 2014). A survey study in ten countries found that antipsychotic drugs were the most frequently prescribed drug class for both adults and children with ASD, followed by stimulants, mainly methylphenidate (Hsia et al., 2014).
The overall number of prescription drugs may reflect the comorbidity of psychiatric hospital patients. While we could not identify the treatment target, the proportion of stimulants reported mirrors the prevalence for ADHD as a comorbidity of ASD reported in other studies (Houghton et al., 2017); in Mexico, amphetamines are not available and methylphenidate is the main choice of drug. Furthermore, physician specialty may influence prescriptions, like the nootropic drug piracetam chosen by neurologists and the high number of prescriptions of anticonvulsants in the psychiatric hospital even while clinical guidelines do not recommend using neither antiepileptics nor piracetam for treating core symptoms of ASD (Crowe & Salt, 2015).
Psycho-social interventions
Although most patients in both clinical sites received a referral for at least one psychosocial intervention, it is still worrisome that 20% report not receiving any. A systematic review suggests that the intervention with the largest strength in terms of evidence is Applied Behavior Analysis (ABA) (Virués-Ortega, 2010). Neither the public health nor the education system provide these interventions in Mexico. Moreover, insurance companies do not cover these treatments, so parents must pay these costs out of pocket. Therefore, it is not surprising to find children with ASD without appropriate therapies despite the ongoing interest of their parents in receiving them.
When resources are limited, clinicians should choose interventions with the most robust scientific evidence (Penner et al., 2018). For instance, in our study, speech therapy is the most frequently prescribed, despite having the least evidence for core symptoms in ASD (Fuentes et al., 2021). In relation to therapy for socio-communicative deficits, only five professionals certified in the Denver Model and sixteen in ABA are listed in Mexico, all of them work in the private sector. Most psychologists in both health centers lack proper certification and training in these therapies. The main reason is the high costs associated with these methods. Health care leaders might be interested in promoting less expensive therapies such as Parent-Mediated Therapy (Pickles et al., 2016) or others that provide intervention techniques to parents for being delivered at home that have shown efficacy for ASD symptoms (Wetherby et al., 2014).
In our sample, a third of the children received an intervention with a component that includes a model specialized for ASD (e.g., ABA, ESDM and TEACCH); all of these children were from the pediatric hospital. This is probably the result of a founder effect, as a single clinician in the pediatric hospital is responsible for this; using an eclectic model that combines adaptations of these and applies them to the families of the patients. When specialized staff is limited, this model offers an alternative. Additionally, these therapies are delivered in facilities outside the hospital as a result of an exchange of services between two, closely located, institutions. In low-middle income countries, interchangeable services between clinical institutions may be the only way to provide this integrated care service. Choosing which treatment option to recommend is one of the most significant challenges for a clinician, particularly when the resources are scarce. Although ASD clinical guidelines could assist clinicians by providing the best evidence available, the range of choices, availability and facilities shows that the evidence needs to first consider what is feasible. While guidelines for the clinical management of ASD already exist in Mexico, the heterogeneity found in this study suggests that in the next update, these should address the low and middles income areas and populations of the country where tools, procedures, and intervention have limited availability.
Our study does not evaluate which model of care is better. In the future, it may be convenient to evaluate the effectiveness and cost-benefits of these two care models, in order to add evidence for the implementation of diagnostic and therapeutic processes adapted to the cultural and economic reality. Finally, the development and dissemination of free, culturally adapted and validated diagnostic tools such as VEAN-Hi (Albores-Gallo et al., 2016) and the CRIDI-ASD interview (Albores-Gallo et al., 2019) may be needed to cut costs and increase adherence at least at the local level.
Conclusion
Our study suggests a lack of consensus among health care facilities in regards to ASD diagnosis and treatment. In order to improve this, we recommend: (a) updating the clinical guidelines to efficiently use resources in a way that promotes the best clinical practices and reduces diagnostic delays, (b) incorporate culturally-responsive and low cost instruments which may increase acceptance and engagement within the clinical community and (c) embrace psychosocial treatments with the most robust evidence that provide a good fit for the economic reality of the population and finally, (d) adopt the strategy of service exchange between sites in order to make the most out of limited resources.
Footnotes
Acknowledgements
We would like to acknowledge the patients and families whose generous contribution made this study possible. In addition, we acknowledge Miguel Nava Arredondo and Patricia Jasso Garcia who assisted in performing the interviews of the parents.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.