
Abstract
The aims of the service evaluation were to examine the effectiveness of multi-family therapy for anorexia nervosa (MFT-AN) on family relationships, as well as to understand families’ experiences of MFT in a specialist child and adolescent eating disorders service between 2013–2021. Mixed-methods were used (t-tests and reflexive thematic analysis). Delivery was in-person in 2013–2019, and moved online from 2020 due to COVID-19. Responses from a total of 57 families and 190 people were analysed. MFT improved family functioning from pre-to post MFT as measured by the Systemic Clinical Observation in Routine Evaluation (SCORE-15). Sub-group analysis by family roles showed that at four-month follow-up, the effects were no longer significant among parents. On the contrary, preliminary analysis showed that although young people did not report any improvement at post-intervention, family functioning was reported to increase at follow-up. Four themes were constructed: being together as a family and as a group; individuality: everyone’s recovery is different; MFT as an emotion ‘hotpot’, and in-person versus virtual groups: not a one-size-fits-all. More robust follow-up data are needed to ascertain the effects of online MFT-AN.
Keywords
Introduction
Multifamily therapy for anorexia nervosa (MFT-AN) has its roots in eating disorder (ED)-focused family therapy (Dare & Eisler, 2000; Scholz & Asen, 2001). It is a recommended treatment for young people with AN (National Institute of Health and Care Excellence Guidelines [NICE], 2020). In MFT, the group of up to eight families and at least two facilitators engage in a variety of activities (e.g., small and large group discussions, role plays, and therapeutic games) in order to strengthen family relationships, gain a greater understanding of anorexia, create solidarity and mutual understanding and hold a mirror up to family functioning. The group can be further separated into mum and dad’s groups, sibling’s group and young person’s group during the tasks. The group will also eat together during snacks or lunch. The two main models of MFT for AN include the Maudsley MFT-AN model which offers 10 days of MFT alongside FT-AN sessions for a period of 6–9 months (Simic et al., 2021), as well as the MFT model developed at the University of Dresden (Scholz et al., 2005), which consists of up to 20 days over a period of 12 months.
Two systematic reviews examined the effectiveness of MFT (Baudinet et al., 2021; Zinser et al., 2022). In Baudinet et al. (2021), across 27 studies, they found improvements in ED symptoms and weight gain (e.g., Skarbø & Balmbra, 2020) for young people who were underweight. However, the findings were more mixed on the improvement in family functioning and family factors such as aspects of experience of care-giving, with some reporting improvements (e.g., Dennhag et al., 2021), and others with no change or deterioration (Geist et al., 2000). The review by Zinser et al. (2022) reviewed 15 studies, and concluded that there was no evidence that MFT improved family functioning or positive aspects of caregiving. A qualitative synthesis (Baudinet et al., 2021) shows that MFT was helpful for the family to view the ED symptoms from new perspectives, gain new skills, and reduce anxiety and guilt in families. Providing a new support network and allowing families to share experiences were also perceived benefits of MFT (Brinchmann & Krvavac, 2021). A qualitative study on MFT-AN for inpatients from five patients (Coopey & Johnson, 2022) revealed two overarching concepts (the role of the individual and the role of others) and four superordinate themes, two relating to the relationships within the family system: ‘process of understanding’, ‘reviving connection’, and another two relating to the development of the individual: ‘emerging from the eating disorder’ and ‘development of I’. Both reviews revealed some limitations of existing studies. Baudinet et al. (2021) noted that the unique contribution of MFT was difficult to ascertain as MFT was typically given as an adjunctive intervention. Zinser et al. (2022) also noticed that the effect of MFT dissipated when compared to another intervention.
However, challenges of MFT were also noted (Baudinet et al., 2021). These include making unhelpful comparisons or sharing unhelpful ‘tricks’ (Baumas et al., 2021), not catering to individual family needs and particularly the different pace of recovery for each person in the group (Baumas et al., 2021). Some participants also reported finding MFT intense, although some parents found the increased intensity helpful (Wiseman et al., 2019). Another finding was the differential perceived helpfulness versus actual improvements among different family members. It was found that young people with AN perceived that the intervention was more helpful for other family members, but improvements were consistently found among the patients (Salaminiou, 2005). The researcher postulated that what might be perceived as challenging might be needed for therapeutic effect to occur in hindsight.
Despite the fact that sizeable research studies and reviews exist, few studies examined online MFT-AN using mixed-methods in routine clinical settings. In our service (an specialist ED Child and Adolescent Mental Health Service [CAMHS]) in England, an unpublished audit was conducted by a trainee clinical psychologist in 2015. Ten families completed the Systemic Clinical Observation in Routine Evaluation (SCORE-15). The questionnaire scores and self-rated outcome were discrepant: whilst there was no signficant change in SCORE-15 scores, self-rated usefulness, ability to cope and severity of problems were improved. Based on the qualitative feedback, activities around food appeared to be those with most negative feedback reported by young people. As the previous audit only involved a small number of families, it would be useful to examine a larger set of data. The current report is a mixed-method service evaluation of MFT-AN groups that took place from 2013–2021. Prior to COVID-19, the groups were face to face. Since the COVID-19 pandemic in 2020, the groups took place online via Zoom/Microsoft Teams. The aims of the evaluation were to examine (i) effectiveness of MFT on family relationships and (ii) families’ experiences of MFT.
Method
Setting
The specialist CAMHS community service has been delivering MFT-AN since 2013 as an adjunctive intervention to family-based treatment. It is offered to all families whose young person is diagnosed with AN and may benefit from intensifying the treatment. Each group consists of two to three lead facilitators who were either MFT-trained at the Maudsley Centre for Eating Disorders (MACAED) or received in-house trainings from other clinicians in the service. The format and content of MFT largely follows the book Multi-family Therapy: Concepts and Techniques by Asen and Scholz (2010). The rest of the therapy team consists of observers who support the running of group activities such as observing and taking note of the family dynamics during the group. Families first join an introduction evening, and the actual intervention consists of four consecutive days in face-to-face MFT (pre-pandemic), and three consecutive days in virtual MFT (2020–2021). Both formats also comprise three follow-up days spread across the next four months.
Participants
Particpants were families who participated in MFT between 2013–2021. A total of 190 people completed at least one feedback form/questionnaire. Families were informed that the feedback and questionnaires would be used for the purpose of service improvement in addition to monitoring individual’s progress. For the in-person MFT groups from 2012–2019, 47 families took part and provided at least one questionnaire entry during any timepoint for analysis. For the virtual MFT groups from 2020–2021, ten families took part and provided at least one data during any timepoint for analysis. The age of the young people with AN ranged from 13 to 17.5.
Ethics
The study was classified as a clinical audit. It was approved by the Trust’s audit team and registered on the local NHS Foundation Trust quality improvement database.
Design and Analysis
Quantitative data included questionnaires collected at various timepoints (day one to three/four of MFT and at 4-month follow-up). Questionnaires collected included Systemic Clinical Observation in Routine Evaluation (SCORE-15) and Caregiver Skills scale (CASK). SCORE-15 is a self-report measure of family processes which consists of 15 Likert-scale items and six separate indicators. The score ranges from 15–75, lower scores indicate better family functioning. Good internal consistency, test-retest reliability, construct validity and criterion validity have been demonstrated (Hamilton et al., 2015). CASK was developed to assess caregiver skills (Hibbs et al., 2015). The items assessed were in line with the cognitive interpersonal maintenance model of EDs (Schmidt & Treasure, 2006). Paired-t-tests were used to examine the differences in SCORE-15 scores pre- and post-MFT. Missing data were not imputed. A priori power calculation showed a minimum of 34 people to achieve 80% power and an effect size of 0.5.
The qualitative feedback were taken from feedback forms after each day of the MFT. The questionnaire asked for feedback about the specific tasks and general feedback about the day. The end of MFT questionnaire also asked about people’s general experiences of the programme. The free texts were analysed using reflexive thematic analysis (TA) (Clarke & Braun, 2021). This was chosen because of its emphasis on developing and interpreting patterns. Critical realist ontology was adopted and analysis was located within the service context (Vincent & O’Mahoney, 2018). SHY extracted all relevant qualitative data from all the feedback sheets over the years and read the data several times before coding. A recursive process of text coding followed, capturing both semantic and latent meanings. Data were coded in different orders to maintain a fresh perspective over the data. Theme development, revision and adjustments were done using pen and paper.
Reflexivity
Reflecting on researchers’ subjectivity is an important step of reflexive TA. At the time of writing, SHY and SW were both clinicians in the CAMHS Eating Disorders team. The interpretation and analysis were influenced by systemic ideas due to our clinical orientation, where we focused on understanding family roles and systemic factors influencing each person’s mental health. We also held in mind our relationship to MFT - SHY was involved as an observer in the virtual MFTs between 2020–2021, and SW was involved as the lead facilitator in face to face and virtual MFTs between 2017–2021.
Results
Quantitative Analysis
Data quality was poor. Data were not available for all families due to inconsistencies in data collection and recording in the service. As they were historical data with multiple system and database changes, it was not possible to ascertain if it was due to lost to follow-up or data entry error. It was also not possible to link the data with demographic information of families. Due to the data lost to follow-up, only descriptive statistics were reported for the virtual MFT groups in Supplementary Information. CASK scores were lost in face to face MFT. For SCORE-15 scores, we were able to report the data from 2013–2021.
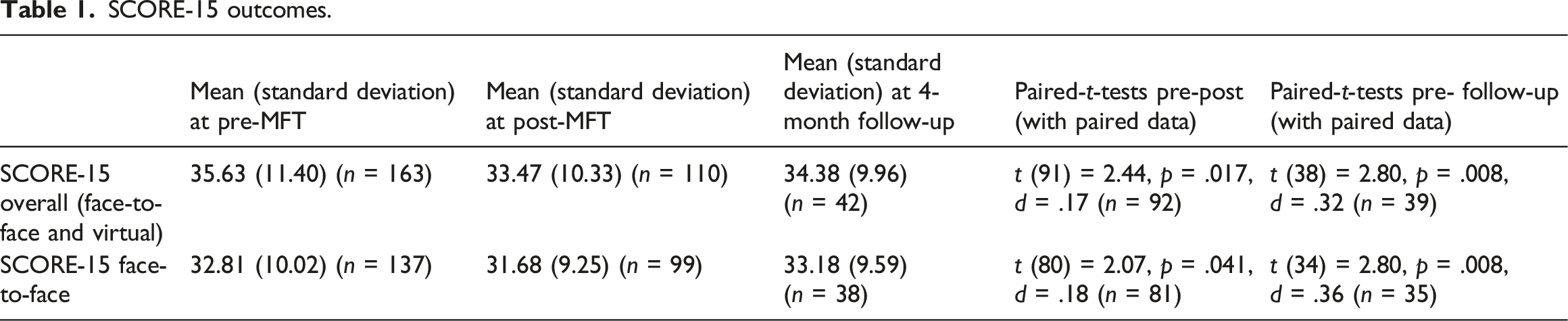
Overall SCORE-15 Scores
SCORE-15 outcomes.
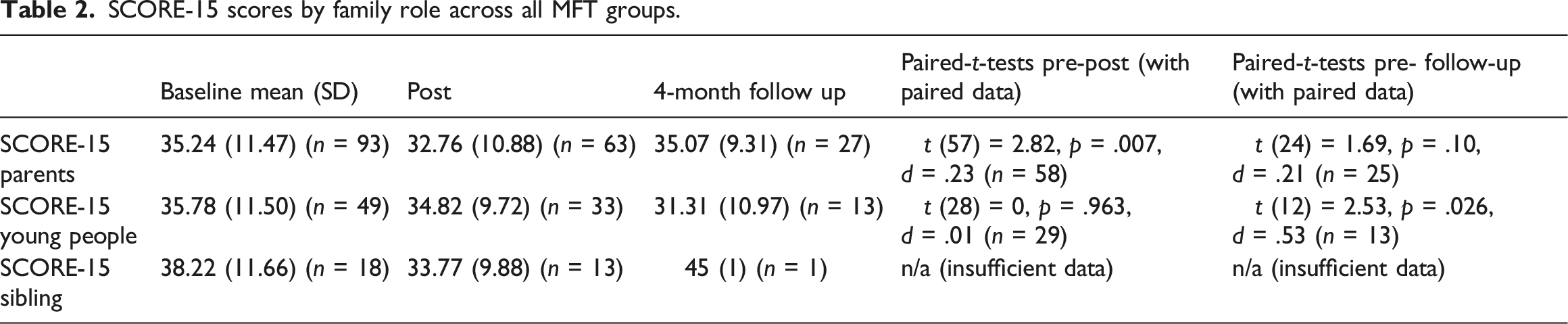
SCORE-15 Outcome by Family Role
SCORE-15 scores by family role across all MFT groups.
Qualitative Analysis
Four themes were constructed: being together as a family and as a group; individuality: everyone’s recovery is different; MFT as an emotion ‘hotpot’ – a mixture of strong emtions, and online versus virtual group: not a one-size-fits-all.
Being Together as a Family and as a Group
This theme includes both intrafamilial and interfamilial levels of analysis. Families expressed a shared reality and a sense of togetherness at MFT where MFT provided a space to discuss issues away from the usual family circumstances.
In terms of interfamilial system, mums mentioned that MFT allowed them to meet others who were going through the same thing and feeling the same way; a dad mentioned being connected with other families; some siblings described being good to meet other siblings as friends do not understand; young people with AN described having a space where fears, expectations, worries were shared. A young person said, ‘It feels annoying to talk to friends about ED, so it’s nice to talk about it without feeling like an inconvenience’ (Young person B).
Regarding intrafamilial effects, families described MFT brought the families together as all family members were involved in working as a family team in the activities. This allowed them to review the family as a unit and realise different family roles, particularly the role of siblings. Two mums mentioned how they underestimated the role of siblings and how much they carry in their roles. The family tasks also brought to light the bigger picture. These include the effects of AN on the whole family rather than individual symptoms, as well as the wider family life outside AN. A young person depicted this using an analogy: ‘choosing the game of life and not the game of anorexia’ (Young Person R). For example, a mum said, ‘Anorexia is a small part hopefully of the families history and to look forward from it’ (Mum I). Another mum described something similar: ‘Our child chose not to add AN to the timeline as in general scheme of life, anorexia was felt to be a small part of it…diagnosed in the last 7 months’ (Mum A). In terms of expectations, whilst some parents found the course generic and lack specific guidance and ideas on how to ‘tackle’ AN, others suggested to future families: ‘Don’t go in hoping it’s a treatment for anorexia itself, it’s to help with the family dynamics around anorexia and how each person plays a role in helping each other’ (Family N).
Mums seemed to particularly find the space useful. For example, a mum mentioned that she experienced less self-blame. Another mentioned that it was her first time expressing how she felt, as she was not able to before due to being worried about upsetting other family members. Another mum hoped that seeing other families’ experiences would help with their own: ‘[it] helps to understand my own feelings as a bit better through talking or through seeing others sharing…for young people to hear their own family members and also hear experiences and emotions of other families’ parents and siblings e.g., seeing someone else’s dad cry might help a young person appreciate how their own dad feels etc.,’ (Mum M).
On the other hand, family tasks might re-enact family conflicts. One of the exercises on family goals caused conflicts between parents and the young person. An example was that a young person could only think of long term goals but did not commit to short term goals such as tackling fear foods, leaving parents feel frustrated and the young person feel overwhelemd. Families expressed the importance of being open and honest in the space. However, it could be seen as challenging as some young people did not like being ‘under the spotlight’, where their problems were being discussed in big groups. A mum worried that her young person was not being honest: ‘If [my child] is unable to see a future without AN, [they] would only be saying things to please the parents as that’s what they wanted to hear’ (Mum E).
Individuality: Everyone’s Recovery is Different
The flip side of the togetherness was how individuality was considered and conceptualised. Several young people and parents mentioned the competitive nature of AN and how ‘illness thrives on comparisons’: some described feeling ‘fake’ (i.e., that they felt their eating disorder was less ‘valid’ than others) as they never over-exercised. Several families expressed that MFT might be more helpful for parents than for young people and would not recommend young people coming. A mum said, ‘I am satisfied but my daughter told me that it keeps her back and is holding her back. Maybe it’s just better for the parents’ (Mum A). A dad speculated that it might be because the young person was struggling to accept and face the challenges of trying to deal with AN. A young person felt the group only discussed ‘sad stories about AN’ which she had heard enough, and wanted to hear more about ‘how people beat AN’. On the other hand, a young person thought MFT might be difficult but helpful: ‘I do think I have a different outlook on anorexia. In the long term I think the effects will be good but I feel very on edge and tired now.’ (Young person I).
Several families described that more consideration might be needed regarding group composition. For instance, single-parent families might have different experiences in the group, and younger participants might feel intimated by older teenagers. On the contrary, the heterogeneity might be valued by others: a sibling said, ‘the more different views and voices that are given, especially the young person’s, the more useful the course will be’ (Sibling L).
MFT as an Emotion ‘Hotpot’ – A Mixture of Strong Emotions
Strong emotions were expressed. Whilst some activities were fun and relaxing, other activities and coming to MFT itself generated difficult emotions. For young people, emotions such as uncomfortable, intense, exhausting, and numb were mentioned. That said, a sibling mentioned MFT was awkward but it was worth it. Some dads expressed feeling emotional, finding it tough and stressful. However, towards the end of MFT, a dad described the experience overall as ‘ultimately calming’. Mums also expressed how intense MFT was: ‘Anxiety about participating in MFT manifest in self-harm and a lot of anger and resentment [from their child]. Hopelessness was another emotion described: ‘maybe the reality is that there isn’t a total cure ever and that is more than heartbreaking’. However, other mums also described hope, tears and laughters.
One activity that was particularly distressing and challenging was the shared lunch. Participants mentioned that people with AN liked planning and did not like surprises: ‘it was hard enough to get your child stick to the meal plans, lunch was challenging and ended up with skipping a meal altogether’ (Mum S). One suggested not offering choice for families to choose but rather working towards eating together: ‘don’t offer choice about a shared lunchtime, instead state that we have worked towards eating together over the last 3 days and that we will all have 10 minute for comfort break and gathering/plating food then its back to the screens with A/V ‘on’ for duration of lunch suggest a progressive plan eg day 1 snack to day 3 lunch’ (Mum E).
In-Person Versus Virtual Groups: Not a One-Size-Fits-All
Whilst some issues of the online format were pointed out by some participants (e.g., dialogues being more stilted, body language being missed, technical issues affecting the flow of the groups, young people not having their cameras on which affected the group dynamics), some participants thought online groups might be cheaper to organise in a way that could roll out for more people. Some actually found the online format helpful as they could be in their own comfortable environment: ‘it is a tiring course so being at home really helped’ (Parents E). A participant suggested allowing comfort/screen breaks every 40–50 minutes in virtual MFT. On the contrary, long journey time for consecutive days could be tiring for face to face groups.
Discussion
The current service evaluation aimed to extend the previous audit by using mixed-methods to examine the effectiveness of MFT on family relationships as well as explore the families’ experiences of MFT. Our evaluation also contributes to the wider research on MFT in AN as we incoporated analysis of virtual groups and sub-groups based on family roles.
Overall, we found that MFT, regardless of online/in-person format, improved family functioning from pre-to post MFT as measured by SCORE-15. This was different from the previous audit in 2015 within our service. Differences in sample size might contribute to the differences in results. However, it was less certain if the effects were sustained at 4-month follow-up given the data lost to follow-up. This potentially demonstrates that recovery is not linear, although it is difficult to interpret given the families received treatment as usual between the datapoints. Findings about family functioning and relationships post-MFT were mixed (Baudinet et al., 2021; Zinser et al., 2022), demonstrating the importance of qualitative findings to explore patterns of meanings and experiences not captured from the numbers.
Four themes were generated from reflexive TA: (i) being together as a family and as a group, (ii) individuality: everyone’s recovery is different, (iii) MFT as an emotion ‘hotpot’ – a mixture of strong emtions, and (iv) in-person versus virtual groups: not a one-size-fits-all. The qualitative findings largely echo previous studies, such as providing new perspectives (Baudinet et al., 2021; having a new support network (Brinchmann & Krvavac, 2021), as well as some ‘less helpful’ aspects of MFT, including unhelpful comparisons and people having different pace of recovery (Baumas et al., 2021). There was value in being able to learn from other families, for example, one of the quotes was about how seeing someone else’s dad cry might help a young person appreciate how their own dad feels, which relates to the idea of shared learning in the meta-synthesis from Baudinet et al. (2021). Scholtz et al. (2005) also described a therapeutic ‘hothouse’ effect that is difficult to create in a single family setting, and hypothesised that learnings can be accelerated through intensifying interactions and experiences. The strength of our current analysis is a larger sample size than other qualitative studies as well as incorporating siblings’ views in addition to the parental and young people’s views. Other additional insights include people’s experiences of an online delivery of MFT, which fits with some families but not others. From our experience, some online MFT groups were difficult to deliver when all young people refused to turn on their cameras. It was useful to hear from some families that doing an intensive and emotional therapy programme in their comfort of their own homes felt safe and more comfortable.
Young people’s and siblings’ views (e.g., it’s challenging but worth it’) also helped understand the qualitative finding of the differential effect on SCORE-15 among different family members. Quantitative data were limited and did not permit meaningful t-tests to be done for the siblings sub-group. However, exploratively, whilst parents reported better family functioning pre-post MFT, young people did not experience any change in family functioning. Interestingly, an improvement in family functioning was reported by young people with AN at follow-up (although the sample size was small at follow-up, n = 13). The quantitative data complement the finding in Salaminiou (2005), where improvements were consistently found among the patients, although young people reported that they thought the intervention was more helpful for other family members rather than themselves. A quote from a young person in this evaluation also indicated that young people felt MFT could be helpful in the long-term, but at the time of the treatment, they simply felt on edge and tired. One possible explanation was a response bias where only young people who found the treatment helpful responded to the questionnaire. Baudinet et al. (2021) suggested that the perceived disparity might be attributed to the stage of recovery of the patients. Another possibility might be that although treatment might bring up difficult emotions and conflicts, they may be needed for therapeutic effects to occur. This also begs the question of seeing treatment outcomes in a dichotomous way – some of the young people might resent the treatment initially due to anxiety and find the treatment ‘unhelpful’ as it brought up negative emotions. At follow-up, they might experience the treatment as helpful further to recognising they had the space to express and experience intense emotions, and started to experience the changes in family communication after MFT.
Limitations
Despite the strengths of the current study (including virtual MFT and using data in routine settings), our evaluation has several limitations. This highlights the difficulty in routine service evaluation owing to changing databases and missing data which affects the power of the data. As aforementioned, the poor data quality made it difficult to ascertain if the missing data were due to drop-out or data input error over the years. Although we were able to analyse the SCORE-15 data, it was difficult to analyse data from CASK and for the virtual MFT groups. Poor data quality also meant we were unable to retrieve demographic details such as gender, age, and duration of eating disorders. Moreover, as this is an evaluation in routine setting, there was no control group; families also underwent intervention as usual between post-intervention and follow-up period. This could affect the current analysis and interpretation of follow-up data.
Research Implications
In the future, with greater sample size, it would be useful to conduct sub-group analysis based on family roles and sub-scale analysis on CASK to further understand the specific impacts of MFT on caregiver skills and family relationships.
There was also a higher mean SCORE-15 in the online MFT groups than the in-person groups. Our speculation is that this could be due to COVID-19 pandemic and possible increase in family conflicts when everyone stayed at home. It would be useful to also explore clinicians’ as well as observers’ experiences of online MFT as they are little-explored.
The qualitative findings yield some interesting areas for future research. For example, single-parent families and divorced families might experience MFT differently, and future research can routinely collect family structures as part of the demographic information and explore their experiences using qualitative methodology.
Clinical Implications/Recommendations for Service
The large amount of missing data and the time spent on cleaning the data shows the importance of keeping a centralised database and having a clear protocol of data entry and scoring in a routine clinical setting where turnover is high.
The qualitative findings provide useful suggestions regarding planning of activities such as managing shared lunch and snacks, and taking group composition (e.g., family structures, age of the young people) into consideration when planning groups. Both qualitative and quantitative feedback show that online groups are potentially feasible and effective. Future groups could be inclusive and run online/in-person groups in an alternate manner and explain to people and pros and cons of each so families could choose. Also, rather than reducing anxiety and the difficult emotions in MFT, it remains a clinical and research question as to how they can be managed to increase treatment accepability especially among young people, whilst enabling the families to experience difficult emotions in a therapeutic and contained way.
In conclusion, this mixed-method evalution contributes to the field of MFT-AN research with a relatively large sample over the years in a routine setting, and incorporates siblings’ views and effects of online delivery.
Supplemental Material
Supplemental material - Service evaluation of multi-family therapy for anorexia groups between 2013–2021 in a specialist child and adolescent eating disorders service
Supplemental material for Service evaluation of multi-family therapy for anorexia groups between 2013–2021 in a specialist child and adolescent eating disorders service by See Heng Yim, and Sam White in Clinical Child Psychology and Psychiatry.
Footnotes
Author contributors
SHY designed the evaluation and analysed the data. SHY wrote the first draft of the manuscript with support from SW. SW supervised the design and write-up of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was classified as a clinical audit hence ethical approval was not needed. It was approved by the Oxford Health NHS Foundation Trust’s audit team and registered on the Oxford Health NHS Foundation Trust quality improvement database.
Correction (August 2023):
This article has been updated with minor textual corrections since its original publication.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.