
Abstract
Objective
Emotion regulation, perfectionism, and rumination are perpetuating factors in anorexia nervosa (AN). Mindfulness can be protective and therapeutic. We aimed to understand the relationship between these factors and mindfulness in AN.
Methods
20 adolescent girls in the acute phase of the AN, 16 in remission, and 40 in the control group were evaluated.
Results
Mindfulness was lowest in the acute AN group. The difference in the acute AN group regarding body dissatisfaction, emotion dysregulation, perfectionism, and mindfulness disappeared after controlling for the effects of depression and anxiety. The predictors of disordered eating in the entire study population were body dissatisfaction and depressive symptoms. Emotion regulation and perfectionism were the predictors of mindfulness in the acute AN group and the entire study population. When mindfulness decreased, concerns about body shape increased in both acute AN and remission groups, while dietary restriction and disordered eating behaviors increased only in the remission group.
Discussion
Emotion regulation difficulties in acute AN could be related to depression and anxiety. Mindfulness interventions for emotion regulation could be used for depression during the acute phase while for perfectionism in remission. Early intervention for depression and body dissatisfaction seems protective, and mindfulness could be an appropriate intervention.
Introduction
Anorexia nervosa (AN) is a disorder in perceiving the size and shape of the body and is characterized by being under the minimum body weight for age and height, being afraid of getting fat, and wanting to be thin. Body dissatisfaction is the core symptom. Depression (around 35–50%) and anxiety disorders (around 11%) are common comorbidities (Buhren et al., 2014; Puccio et al., 2016). Emotion regulation, stress intolerance, and cognitive/emotional avoidance strategies are etiological factors (Racine and Wildes, 2015). Perfectionism and ruminations related to body shape and weight are perpetuating factors (Donahue et al., 2018). Besides the treatment of medical complications, psychotherapy is needed. Psychotherapy is based on understanding the meaning of these factors and the process of separation-individualization and identity formation. The effectiveness of third-wave behavior therapies has also been investigated. These therapies emphasize the emotion regulation strategies such as acceptance, psychological flexibility, and metacognition that modulate the experience of emotion (Linardo et al., 2017). Mindfulness-based therapies are among them.
Emotions are conditional, almost automatic behaviors, physiological responses, and strategies that occur in the face of important experiences. Emotions become dysfunctional when they are not suitable for the current situation, are too intense, and last too long. Restriction in eating and heavy exercise in patients with AN could be due to avoiding negative emotions (Haynos and Fruzzetti, 2011). Patients with AN have difficulties understanding and describing their internal states, accepting the emotion experienced at that time, and especially reaching the right strategy that mediates emotion regulation (Danner et al., 2014).
Perfectionism describes a trait of setting unrealistic goals and valuing oneself according to whether these goals are achieved (Shafran and Mansell, 2001). In maladaptive perfectionism, the idea that society expects a ‘perfect ideal body’ could result in body dissatisfaction and eating disorder (Donahue et al., 2018). High standards of appearance and weight could lead to AN (Nilsson et al., 2007). Perfectionism may predict adverse outcomes and poor prognosis in AN (Bardone-Cone et al., 2007), especially with difficulties in emotion regulation (Byrne et al., 2016).
Rumination is repetitive, involuntary thoughts on a particular topic in the past. People with ruminative thoughts focus on specific points and feel internal discomfort, but they do not try to overcome them (Watkins and Teasdale, 2001). Rumination related to body shape and weight in AN is a mediator between AN and perfectionism (Halmi et al., 2000) and has an affective component rather than physiologic (Fürtjes et al., 2018). Rumination is an avoidance strategy in emotion regulation, providing distance from the emotional experience itself, but paradoxically, it causes the exacerbation of negative emotions (Roemer et al., 2009). In literature, rumination is associated with depression the most (Watkins and Teasdale, 2001), and depression is the most common comorbidity in AN (Buhren et al., 2014; Puccio et al., 2016).
Mindfulness is defined as directing one’s attention to momentary, internal, and environmental stimuli without judgment, accepting the moment by experiencing instant experiences without being influenced by past experiences, emotions, or the future. Its basic components are present-focused attention, acceptance, non-judgment, and introspection (Kabat‐Zinn, 2003). Mindfulness can protect against repetitive negative thoughts and ruminations associated with perfectionism (Short and Mazmanian, 2013). Mindfulness-based therapies have been recommended recently in AN (Merwin et al., 2010). Mindfulness-based therapies enhance interoceptive awareness, acceptance, and paying attention in the present moment non-judgmentally. Mindfulness could reduce restrained eating, improve body image acceptance, and reduce emotional and impulsive eating in AN (Turgon et al., 2019).
In light of current knowledge, the only study on mindfulness in AN included adult women and was conducted on symptoms directly related to eating (Thompson-Brenner et al., 2019). No study evaluates the interrelationships among perfectionism, rumination, emotion regulation, and mindfulness skills among adolescent girls with AN after controlling for the effects of depression and anxiety symptoms. This cross-sectional, case-control study aimed to evaluate mindfulness skills, perfectionism, rumination, and emotion regulation in adolescent girls with AN and to understand their relationship with symptoms of eating disorders during the acute phase and remission. We also investigated the relationship of these variables with the level of body shape dissatisfaction. The hypotheses of this study were: 1. Even after controlling for the effects of depression and anxiety, high rumination and perfectionism levels and more difficulties in emotion regulation negatively affect mindfulness skills in adolescent girls with AN regardless of whether they were in the acute phase or remission. 2. Disordered eating behaviors are related to high emotion regulation difficulties, low mindfulness, high perfectionism, and high body dissatisfaction, even in the control group. 3. Mindfulness is negatively affected by perfectionism, rumination, and emotion dysregulation among the AN group. 4. Mindfulness is higher in remission than in acute AN.
Materials and Methods
Sample and Design
Data were collected from adolescent girls (aged 12–18) who were outpatients of the Department of Child and Adolescent Psychiatry, Hacettepe University Faculty of Medicine, between March 2020 and July 2020. This study was approved by the Institutional Review Board of Hacettepe University (2020/06-52). Written informed consent was obtained from both participants and their parents. The exclusion criteria were having a chronic medical and/or neurological illness other than psychiatry, being diagnosed with intellectual disability, or any psychotic disorder or bipolar disorder. All participants were evaluated with a semi-structured interview, Schedule for Affective Disorders and Schizophrenia for School-Aged Children, Present and Lifetime Version (K-SADS-PL), to diagnose psychiatric disorders in AN and Remission groups and rule out psychiatric disorders in the control group. The reliability and validity in Turkish were performed (Ünal et al., 2019).
Adolescents aged 12–18 who self-identified as girls and applied to our clinic with complaints such as not eating and/or weight loss were evaluated for the AN group. The adolescent girls with AN who needed hospitalization at the time of the evaluation were included in the study after 1 month of discharge. The Remission group consisted of adolescent girls with a history of AN whose symptoms did not meet the diagnosis of AN according to K-SADS-PL. Although there is no consensus on the remission criteria in the literature, we defined remission as a BMI ≥19 and a decrease in symptoms to at least a sub-threshold level for at least 3 months (Khalsa et al., 2017; De Young et al., 2020). The control group consisted of adolescent girls who applied to our clinic to get a report stating that they have no psychiatric problems or get counseling about a challenge in their lives (e.g., School change). A psychiatric evaluation has been performed for these applications. For this study, K-SADS-PL was applied to be sure they had no psychiatric disorders currently and in the past. One adolescent girl in the AN group was excluded because of her high BMI. Twenty adolescent girls were in the acute phase of the AN group, 16 were in remission, and 40 were in the control group. The groups were matched concerning sociodemographic level.
Measurements
Sociodemographic and Clinical Information Form
This form was developed by researchers. Sociodemographic, developmental, medical, and family histories were asked.
Eating Disorder Examination Questionnaire (EDE-Q)
This 7-point Likert-type scale assesses eating disorders attitudes and behaviors with 28 items. There are four subscales: Dietary restraint, eating concern, shape concern, and weight concern. The total score is calculated by averaging the four subscales, and higher scores indicate severe eating disorders (Fairburn & Beglin, 1994; Yucal et al., 2011).
Five Facets Mindfulness Questionnaire (FFMQ)
The questionnaire has 39 items that assess the tendency to be mindful in daily life (Baer et al., 2006; Kınay, 2013). The five facets are as follows: Observing (the tendency to observe internal and external experiences), Describing (the tendency to describe and label internal experiences in words), Acting with awareness (acting with awareness and undivided attention to the present activity or experience), Nonjudging (take a nonjudgmental stance toward inner experiences), and Nonreactivity (the tendency to allow thoughts and feelings to go without focusing or elaborating on them). Higher scores indicate a tendency to that facet of mindfulness, and the total score is also calculated.
Ruminative Response Scale- Short Version (RRS-SV)
This 4-point Likert-type scale evaluates the tendency to ruminate in response to sadness and depression with 10 items (Treynor et al., 2003). It contains two subscales: Brooding (a maladaptive rumination style that refers to mood pondering) and Reflection (reassessment of past and present events, feeling, and behaviors thoughtfully and unemotionally; it could be adaptive or maladaptive). Higher scores indicate a greater rumination tendency in that way. Turkish reliability and validity were conducted (Erdur-Baker and Bugay, 2010).
Difficulties in Emotion Regulation Scale (DERS)
This 5-point Likert-type scale consists of 36 items that evaluate the difficulties in emotion regulation in six subscales: Goals (difficulty in engaging goal-directed behaviors while experiencing negative emotions), strategies (limited access to emotion regulation strategies), impulse (controlling impulsivity while experiencing negative emotions), awareness (being aware of responses when facing with negative emotions), clarity (lack of emotion clarity), and nonacceptance (nonacceptance of negative emotions). Higher scores indicate the difficulty stated in that subscale, and the total score is also calculated (Gratz and Roemer, 2004; Rugancı and Gencoz, 2010).
Frost Multidimensional Perfectionism Scale (FMPS)
It has 35 items with six subscales: Doubts about actions (feeling unsure of the quality of one’s actions), Concern over mistakes (negative reactions to mistakes, thinking of mistakes as a failure), Parental expectations (thinking of parents’ high standards), Parental criticism (the belief that parents are overly critical), Personal standards (having extremely high standards for performance), and Organization (tendency to be orderly and organized). Each item is answered using a 5-point Likert-type style. Besides the total score, higher scores indicate the severity of perfectionism stated in that subscale. The organization is thought to have a distinct feature that is not calculated with the total score (Frost et al., 1990; Ozbay and Misirli Tasdemir, 2003).
Body Image Satisfaction Questionnaire (BISQ)
It is a 5-point Likert-type scale with 25 items, including general appearance, face, extremities, trunk, chest, upper torso, and sexual organs. The score of each body part is calculated by dividing the sum of points by the number of items in that body part. Higher scores indicate higher body dissatisfaction (Berscheid et al., 1972; Gökdoğan, 1988).
Beck Depression Inventory (BDI)
This inventory measures the severity of depression with 21 items. It is a 4-point Likert-type scale with a cut-off of 17 (Beck and Ward, 1961; Hisli, 1989).
Screen for Child Anxiety and Related Disorders (SCARED)
This 3-point Likert-type scale includes 41 items. A score of ≥25 may indicate the presence of an anxiety disorder (Birmaher et al., 1997; Karaceylan Cakmakci, 2004).
Statistical Analysis
Statistical analysis was performed by Statistical Package for the Social Sciences 22 (SPSS 22). The significance of the difference between the two groups was evaluated with an independent sample t test or Mann-Whitney U test, depending on whether parametric conditions were satisfied. In order to compare the variables between more than two groups, a one-way analysis of variance (ANOVA) or Kruskal-Wallis test was performed. Categorical variables were evaluated with Pearson’s Chi-Square or Fisher’s Exact test. Spearman’s correlation coefficient was used to determine the relationship between two continuous variables. Analysis of covariance (ANCOVA) was performed to determine the main effect of an independent variable on a dependent variable (age, CDI, SCARED). A linear regression analysis with the forward model was used to identify the factors affecting EDE-Q and FFMQ. p < 0.05 was considered statistically significant.
Results
Sociodemographic and Clinical Variables
Clinical Characteristics of Groups.
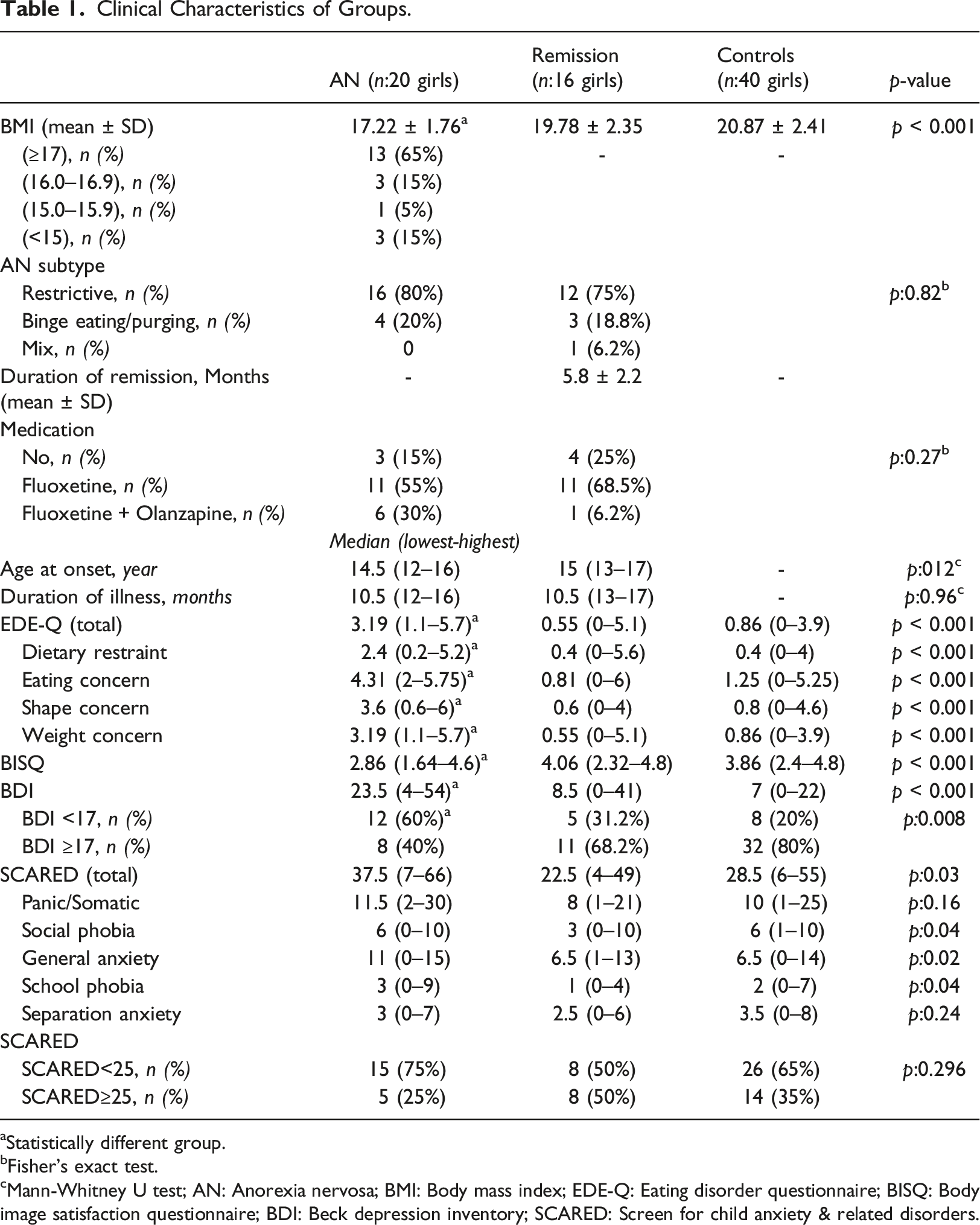
aStatistically different group.
bFisher’s exact test.
cMann-Whitney U test; AN: Anorexia nervosa; BMI: Body mass index; EDE-Q: Eating disorder questionnaire; BISQ: Body image satisfaction questionnaire; BDI: Beck depression inventory; SCARED: Screen for child anxiety & related disorders.
Mindfulness, Rumination, Emotion Regulation, and Perfectionism in Groups.
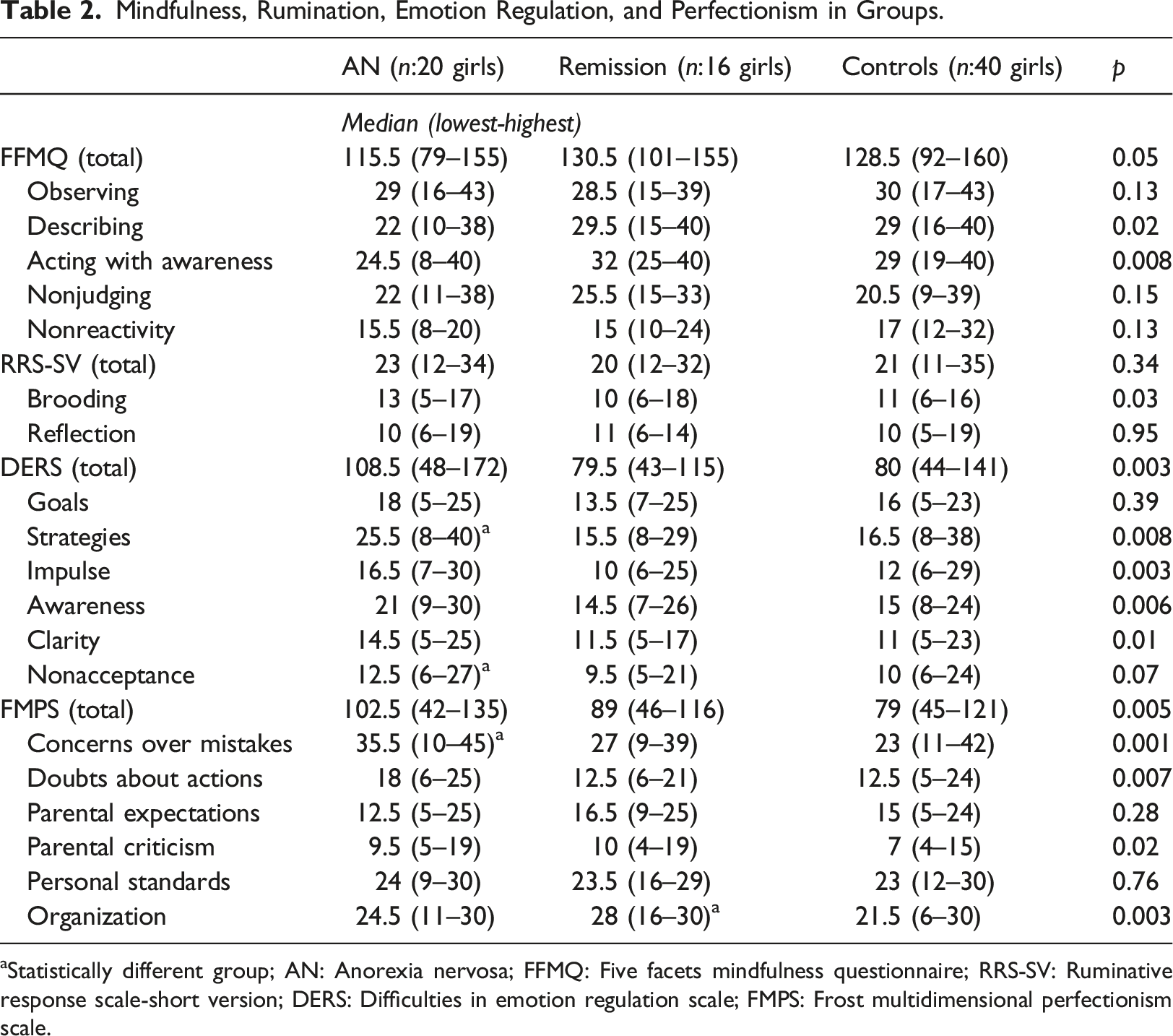
aStatistically different group; AN: Anorexia nervosa; FFMQ: Five facets mindfulness questionnaire; RRS-SV: Ruminative response scale-short version; DERS: Difficulties in emotion regulation scale; FMPS: Frost multidimensional perfectionism scale.
After controlling for the effect of age, EDE-Q, DERS, and BDI were still significantly higher in AN than in the other groups, while BISQ was still significantly lower in AN than in other groups. The SCARED score was still significantly higher in AN (34.98 ± 2.96) than in the Remission group (19.53 ± 3.4) even after controlling for the effect of age (Controls: 29.42 ± 2.11; F: 5.64, p < 0.01). The mindfulness score was significantly lower in AN (Median: 115.5 (70–155)) than in Control (Median: 128.8 (92–160)) group (p:0.022; Remission: 130.5 (101–155)). However, after controlling for the effect of age, the mindfulness score in AN (116.38 ± 3.74) became significantly lower than in both Remission (131.81 ± 4.38) and Control (128.04 ± 2.66) groups (F: 4.18, p < 0.05).
Corrected Total Scores of Scales According to Depression and Anxiety Symptoms.
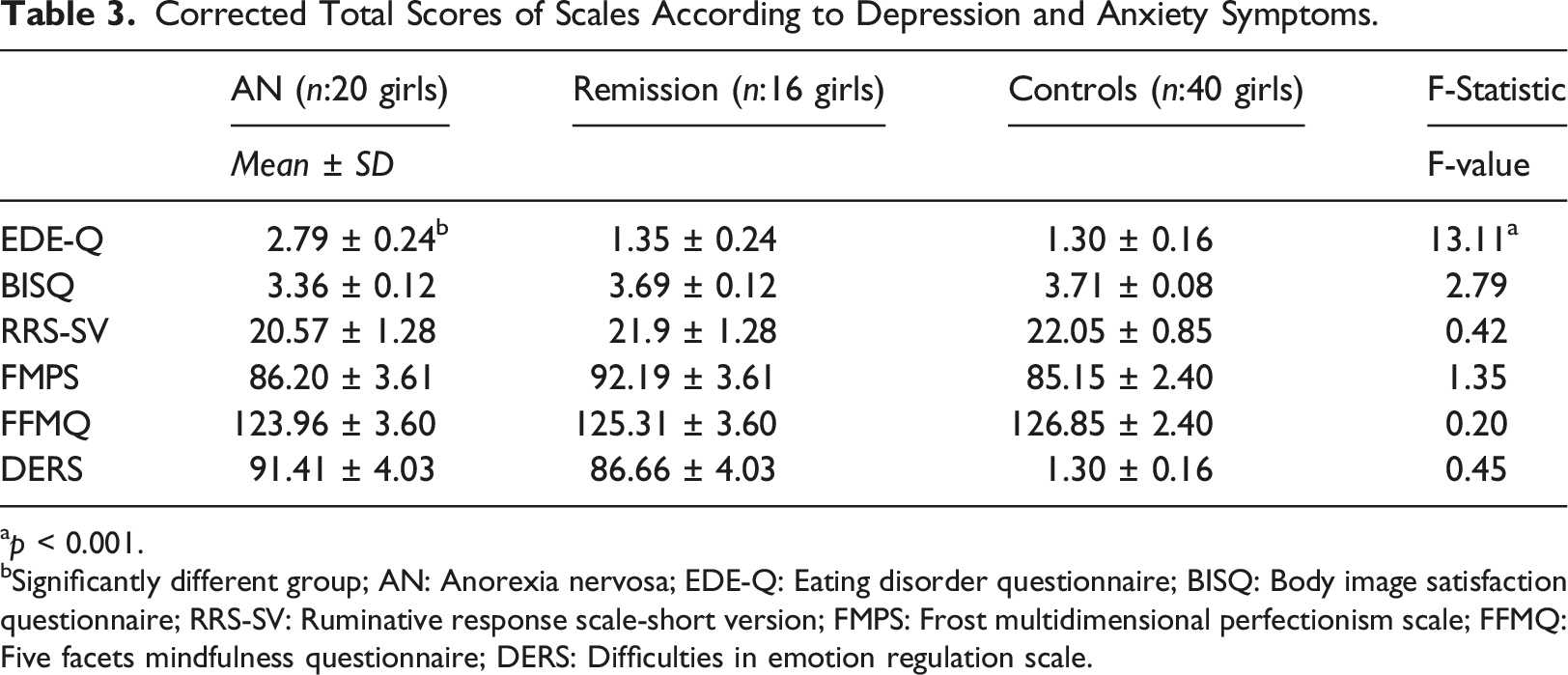
ap < 0.001.
bSignificantly different group; AN: Anorexia nervosa; EDE-Q: Eating disorder questionnaire; BISQ: Body image satisfaction questionnaire; RRS-SV: Ruminative response scale-short version; FMPS: Frost multidimensional perfectionism scale; FFMQ: Five facets mindfulness questionnaire; DERS: Difficulties in emotion regulation scale.
The Correlation Analysis
Correlations of EDE-Q with Other Scales.
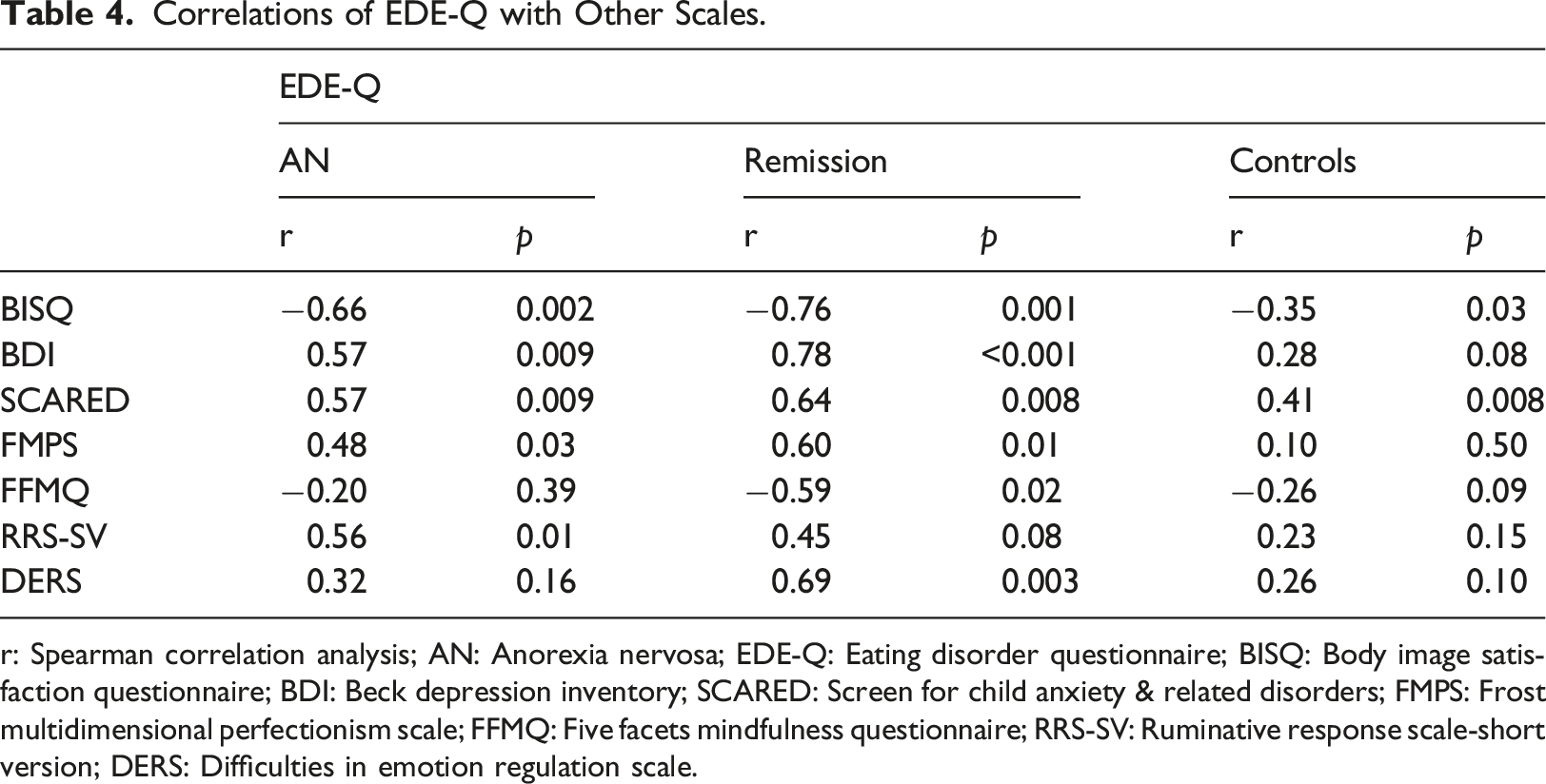
r: Spearman correlation analysis; AN: Anorexia nervosa; EDE-Q: Eating disorder questionnaire; BISQ: Body image satisfaction questionnaire; BDI: Beck depression inventory; SCARED: Screen for child anxiety & related disorders; FMPS: Frost multidimensional perfectionism scale; FFMQ: Five facets mindfulness questionnaire; RRS-SV: Ruminative response scale-short version; DERS: Difficulties in emotion regulation scale.
Correlations of EDE-Q Subscales with Mindfulness.
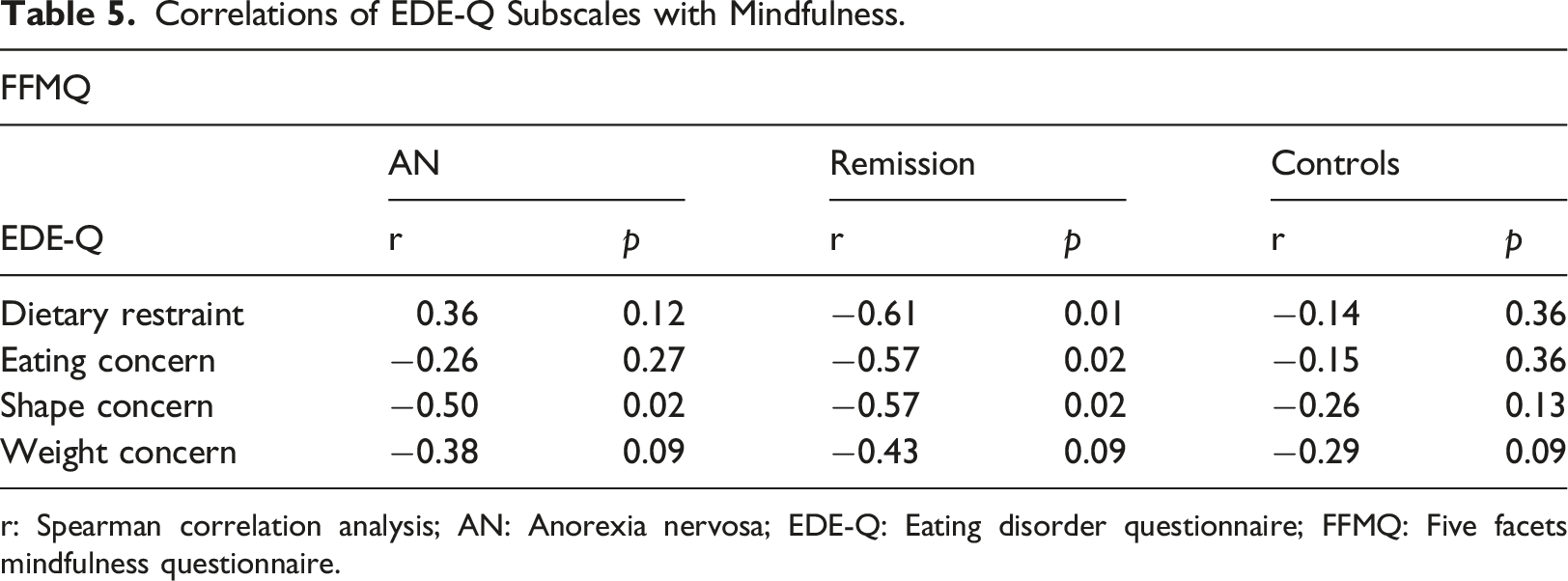
r: Spearman correlation analysis; AN: Anorexia nervosa; EDE-Q: Eating disorder questionnaire; FFMQ: Five facets mindfulness questionnaire.
Correlations of Mindfulness (FFMQ) with Other Scales.
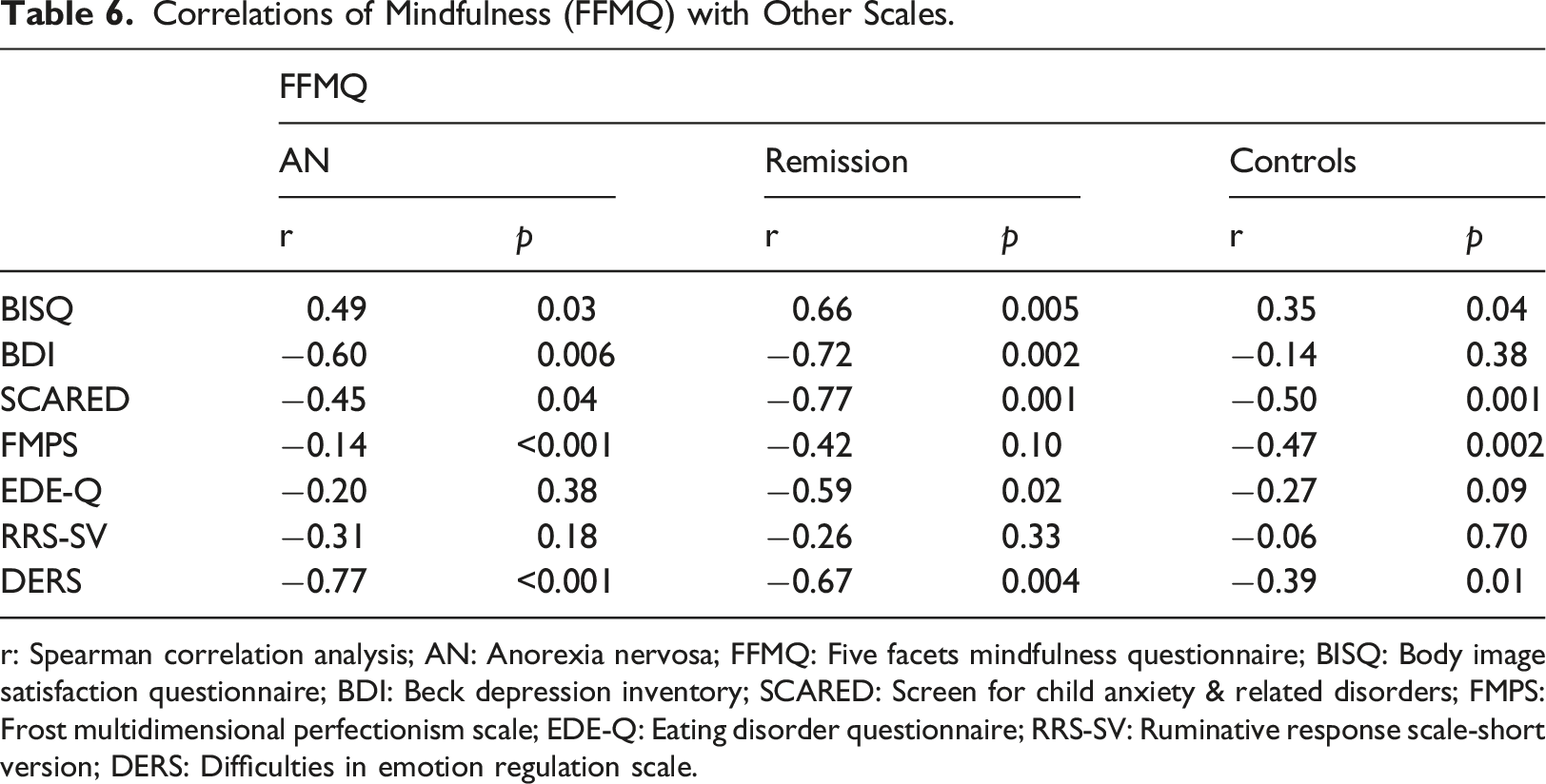
r: Spearman correlation analysis; AN: Anorexia nervosa; FFMQ: Five facets mindfulness questionnaire; BISQ: Body image satisfaction questionnaire; BDI: Beck depression inventory; SCARED: Screen for child anxiety & related disorders; FMPS: Frost multidimensional perfectionism scale; EDE-Q: Eating disorder questionnaire; RRS-SV: Ruminative response scale-short version; DERS: Difficulties in emotion regulation scale.
Regression Analysis
The sample size in the AN group was not sufficient for regression analysis with all scales. Body image satisfaction (BSIQ), rumination (RRS-SV), and perfectionism (FMPS) were entered in linear regression with the forward model because of their high correlation scores with EDE-Q. Only BSIQ stayed in this model and explained 41% of the variance of EDE-Q (R-squared: 0.41, p:0.002). On the other hand, when linear regression analysis with the forward model was performed for mindfulness (FFMQ), perfectionism (FMPS), emotion regulation (DERS), and BISQ were entered. Only DERS stayed in the model and explained 64% of the variance of FFMQ (R-squared: 0.64, p:0.002).
All scales were entered in linear regression analysis to find all participants’ associated factors of eating disorder (EDE-Q) and mindfulness (FFMQ). For EDE-Q, the forward model was used, and in Model 1, BSIQ explained 53% of the variance (R-squared: 0.53, p < 0.001). When depression (BDI) entered Model 2, it explained 61% of the variance (R-squared: 0.61, p < 0.001). Depression and body image dissatisfaction were the predictors of disordered eating in the entire population. When the forward model was used for FFMQ, emotion regulation (DERS) explained 47% of the variance in Model 1 (R-squared: 0.47, p < 0.001), and perfectionism (FMPS) explained 52% of the variance in Model 2 (R-squared: 0.52, p < 0.001). Emotion regulation and perfectionism were the predictors of mindfulness in all participants (Table 7).
Discussion
Associated Factors of Eating Disorder (EDE-Q) and Mindfulness (FFMQ) in All Groups.
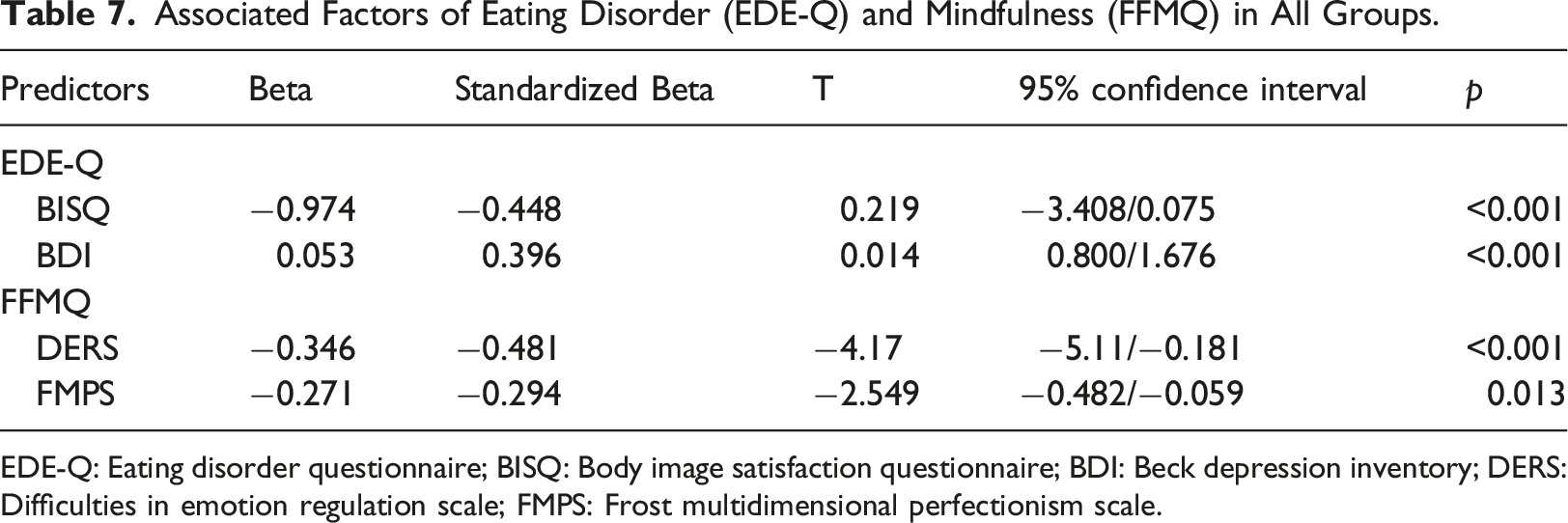
EDE-Q: Eating disorder questionnaire; BISQ: Body image satisfaction questionnaire; BDI: Beck depression inventory; DERS: Difficulties in emotion regulation scale; FMPS: Frost multidimensional perfectionism scale.
The lower BMI, higher eating disorder score, and lowest body satisfaction in the AN group, even after controlling for the effects of depression and anxiety, are compatible with the literature (Steinglass et al., 2020). The lowest anxiety level in the Remission group may be due to their treatment history.
In the AN group, body dissatisfaction was correlated with emotion regulation difficulties, but emotion dysregulation was not correlated with eating disorder behaviors. Besides, the significance of higher emotion regulation difficulties scores in the AN group than in the other groups disappeared after controlling for the effects of depression and anxiety. On the other hand, in the Remission group, both body dissatisfaction and eating disorder behaviors were correlated with emotion regulation difficulties. Also, body dissatisfaction and depression correlated in the Remission group. We suggest that during the acute phase, difficulties in emotion regulation may be due to comorbid depression and anxiety symptoms, while during the remission phase, emotion regulation strategies may be more related to the psychological aspects of AN. Emotion regulation is not an AN-specific feature but a transdiagnostic feature (Svaldi et al., 2012), so it could be a mediator in the transition from one comorbidity to another during AN. Some studies considered difficulties in emotion regulation as an independent variable not associated with anxiety (Haynos et al., 2015).
Maladaptive perfectionism is associated with AN (Halmi et al., 2000). In follow-up studies, perfectionism persists even after the weight becomes normal (Bastiani et al., 1995; Srinivasagam et al., 1995). This study found a positive relationship between eating disorders, perfectionism, and body dissatisfaction in the AN and Remission groups. Besides, emotion dysregulation was correlated with perfectionism in all groups, and body dissatisfaction and depressive symptoms were found as predictors of eating disorder symptoms in the entire study population. Consistent with past research (Byrne et al., 2016; Donahue et al., 2018), these results suggest that body dissatisfaction in a depressive adolescent girl could trigger eating disorders combined with perfectionism and emotion dysregulation. The current findings revealed that clinicians should target perfectionism as well when treating depressive symptoms in both the acute and remission phase of AN. Depression can increase emotion dysregulation and lead to a decrease in coping with the distress caused by perfectionism.
The only relationship between rumination and eating disorders was in the AN group. In a study, rumination and perfectionism were predictors of eating disorders (McLaughlin and Nolen-Hoeksema, 2011). Besides, in another study, rumination was considered a mediator between perfectionism and eating disorder symptoms (Halmi et al., 2000). The results of the regression analysis of our study did not support these findings. The small sample size could be the reason. Our study’s highest brooding score in the AN group is consistent with the literature (Rawal et al., 2010). Brooding is thought to be related to depression (Treynor et al., 2003), and in our study, brooding in the AN group may also be associated with depression. However, we found a correlation between the total rumination score and depressive symptoms only in Control and Remission groups. Content in ruminations differentiated into different psychological disorders, and food and weight-related ruminations are the key maintenance factors in AN (Fürtjes et al., 2018). Although RRS-SV does not contain items related to eating disorders, we thought that the rumination of body dissatisfaction and eating in the AN group might lead to pathological eating and body-related preoccupations during the active period of AN.
Mindfulness can protect against eating disorders by reducing ruminations about eating, weight, and body shape (Dunne et al., 2021). People with high mindfulness have significantly lower maladaptive perfectionism, rumination, and mental distress (Short and Mazmanian, 2013). In this study, mindfulness was negatively correlated with body satisfaction in all groups, and emotion dysregulation and perfectionism were the strongest predictors of mindfulness. Mindfulness was the lowest in the AN group and was correlated with perfectionism in AN. When adolescent girls’ mindfulness lowers, they could feel dissatisfied with their appearance and start criticizing themselves for perfectionism. Given this, mindfulness could be a protective factor in AN. In our study, the relationship between depressive symptoms and mindfulness was only present in the AN and Remission.
Additionally, the difference in mindfulness between groups disappeared after controlling for the effects of depression and anxiety. Negative self-evaluation with emotion dysregulation may trigger depressive symptoms, and depression with body dissatisfaction was the predictor of disordered eating. Treatment of depression may increase motivation and decrease body dissatisfaction and emotion dysregulation (Gregertsen et al., 2019; Puccio et al., 2016). We think mindfulness would be effective for depression and anxiety in the acute phase while for emotion regulation and perfectionism in the remission phase.
In summary, when we consider our hypotheses: 1. Mindfulness correlated negatively with depression in both AN and Remission groups, while it correlated negatively with anxiety in all groups. The difference in AN from other groups in terms of lower mindfulness scores disappeared when the effects of depression and anxiety on all these psychological aspects were controlled. Even after controlling for the effects of depression and anxiety, high perfectionism levels and more difficulties in emotion regulation negatively affect mindfulness skills in all participants. 2. Disordered eating behaviors are related to depressive symptoms and high body dissatisfaction in all groups. 3. Mindfulness is negatively correlated with emotion dysregulation in all groups. 4. Mindfulness is higher in remission than in acute AN. However, this difference becomes statistically insignificant after controlling for the effects of depression and anxiety. Depression is one of the poor prognostic factors in AN (Franko et al., 2018), and it persists even after weight gain (De Young et al., 2020). Mindfulness could be effective for the symptoms of AN and depression and psychological aspects of AN like emotion dysregulation and perfectionism, which are important for prevention and recurrence.
This study has some limitations. Although we specified the remission criteria according to the literature, these criteria have not been determined strictly in the literature. Additionally, it is challenging to understand treatment effects in the Remission group because of the absence of assessments during their active period. The control group in our study consisted of individuals who applied to the psychiatry outpatient clinic. While we did apply a psychiatric evaluation to ensure these participants had no psychiatric disorders, we acknowledge that this control sample may have limited generalizability to a larger population. A homogeneous Remission group created with accurate criteria for comparison is recommended. Besides, follow-up studies in which the before and after treatment scores of scales are compared, should be carried out with larger samples.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.