
Abstract
Binge-spectrum eating disorders (EDs; bulimia nervosa, binge eating disorder) often develop during adolescence and are associated with serious psychological and physical consequences. Current treatments for adolescents are highly behavioral in nature and while efficacious, many patients do not reach remission indicating that current treatments fail to target a key maintenance factor for EDs. One potential maintenance factor is poor family functioning (FF). In particular, high family conflict (e.g., arguing, critical comments) and low family cohesion (e.g., warmth, support) are known to maintain ED behaviors. Poor FF can (1) cause or exacerbate an adolescent’s use of ED behaviors to cope with life stress and/or (2) inhibit parents from being a resource to adolescents during ED treatment. Attachment-Based Family Therapy (ABFT) is specifically designed to improve FF, and thus may be a promising adjunct to behavioral ED intervention strategies. ABFT, however, has not been tested in adolescents with binge-spectrum EDs. Thus, the current study is the first to evaluate a 16-week adapted ABFT treatment for adolescents with EDs (N = 8, Mage = 16.00, 71.43% female, 71.43% White) fusing together behavioral treatment for EDs with ABFT for highest possible impact. Eight families were treated in an open pilot trial to examine treatment feasibility, acceptability, and preliminary efficacy on FF and eating pathology. Overall, findings were promising. ABFT + B treatment was feasible and acceptable and showed preliminary evidence that it could improve FF and ED behaviors. Future research will test this intervention in a larger sample and further examine the role of FF in maintaining ED symptoms.
Introduction
Binge-spectrum eating disorders (EDs), such as bulimia nervosa (BN) and binge eating disorder (BED), are psychiatric disorders that result in numerous psychological and medical consequences. Binge eating often develops during adolescence (Volpe et al., 2016) and duration of illness is linearly and negatively associated with likelihood of long-term remission (Reas et al., 2000). Thus, early intervention remains imperative. Yet, to our knowledge only six RCTs of treatments for adolescent BN or BED have been conducted (DeBar et al., 2013; Hilbert et al., 2020; le Grange et al., 2007; Le Grange et al., 2015; Schmidt et al., 2007; Stefini et al., 2017). The two first-line treatments for adolescent BN and BED are cognitive behavioral therapy (CBT) and family-based therapy (FBT), both of which are behavioral interventions that focus on reducing dietary restriction and normalizing eating patterns (Fairburn et al., 2003; Le Grange & Lock, 2009; Murphy et al., 2010). Further, although FBT and CBT have shown some efficacy with BN and BED, 50–75% of patients do not achieve remission (Hilbert et al., 2020; Linardon & Wade, 2018; Stice et al., 1996), suggesting these treatments may not target some other critical factors that maintain binge eating.
One such maintenance factor might be poor family functioning (FF). This domain is well researched, and a robust transdiagnostic predictor of youth mental health and behavioral problems (Benson & Buehler, 2012; Deng et al., 2006; Fosco et al., 2012; Fosco et al., 2016; Lucia & Breslau, 2006). Here, we adopt a definition of poor FF as (1) high levels of family conflict (e.g., arguing, critical communication) and (2) lack of family cohesion (e.g., low trust and support) both of which have strong ties to adolescent psychopathology (Benson & Buehler, 2012; Deng et al., 2006; Fosco et al., 2012, 2016; Lucia & Breslau, 2006). Poor FF produces negative affect (e.g., anger, shame) in the adolescent (Chung et al., 2009; Cummings et al., 2003), which leads to use of maladaptive coping behaviors to regulate or distract from the affect (Haedt-Matt & Keel, 2011). This model is partially supported for BN/BED where poor FF is cross-sectionally and longitudinally associated with binge eating (Cerniglia et al., 2017; Holtom-Viesel & Allan, 2014; Mcdermott et al., 2002; Tafà et al., 2017; Tetzlaff et al., 2016). Poor FF could precede the onset of BN/BED (Crowther et al., 2002) or arise in response to it (Erriu et al., 2020). Perhaps most critically, however, poor FF likely interferes with the ability of parents and caregivers to support the adolescent’s adoption of healthy behavior management strategies learned in a behavioral treatment. Without trust and warmth, adolescents may reject parents’ attempts to help the adolescent navigate negative emotions and behaviors. Consequently, parents can become impatient, reactive and reinforcing of negative coping strategies (see Figure 1). Model of family functioning and adolescent binge eating.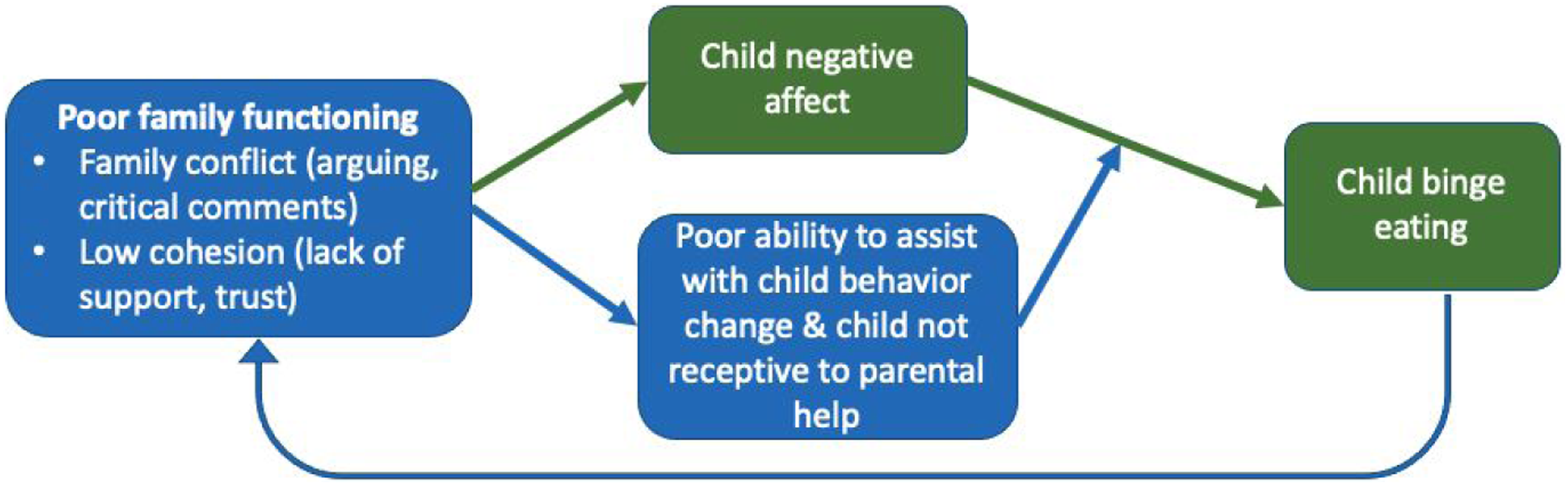
The dominant treatment models of binge eating rely heavily on behavioral interventions, with little focus on family functioning. In cognitive behavioral therapy (CBT, CBT enhanced [CBT-E]) for BN and BED, these behavioral strategies include self-monitoring, establishing regular eating patterns, and reducing attempts to restrict eating, which drive binge eating (Fairburn et al., 2015) and in the adolescent version of CBT, there is little explicit focus on family functioning (Lock, 2005). FBT (an evidence-based treatment for adolescent BN) focuses on promoting healthy eating behaviors (e.g. a regular eating schedule and reducing restriction/purging), with less focus and no specific guidance on navigating emotional conflicts that fuel or exacerbate the ED. A skilled family therapist would not ignore these issues, but this is not the lead goal of FBT as outlined in the treatment manuals (Lock & Le Grange, 2015). In a recent RCT comparing individual cognitive behavioral therapy to FBT for adolescent BN (the largest trial for adolescent BN to date), higher levels of family conflict predicted poorer treatment outcome, regardless of the treatment received (Le Grange et al., 2015). Other studies have found that maternal (Rienecke et al., 2016) and parental (Szmukler et al., 1985) criticism led to increased treatment dropout. In a longitudinal study, higher levels of parental criticism predicted less-favorable outcomes in patients with BN at the end of a six-year follow-up (Hedlund et al., 2003). Despite deficits in family functioning being associated with both elevated psychopathological symptoms (Cerniglia et al., 2017) and worse treatment response (Hedlund et al., 2003) no treatments have specifically targeted poor FF in adolescent binge-spectrum EDs.
One treatment that may help potentiate behavioral treatment is Attachment-based family therapy (ABFT). This model is a structured, empirically-supported emotion-focused family treatment originally designed for adolescent depression and suicidality. Data suggest ABFT can reduce negative family factors that fuel adolescent self-destructive behavior and this reduction in negative family factors mediates treatment outcome (G. S. Diamond et al., 2014; G. S. Diamond et al., 2019; G. S. Diamond et al., 2002; Ewing et al., 2015; Rognli et al., 2020). ABFT posits that family high conflict and low warmth can maintain and/or exacerbate psychological symptoms or maladaptive behaviors (Ewing et al., 2015). ABFT aims to identify underlying relational factors that drive poor FF (e.g., lack of parent-child attunement and basic emotion coaching skills). The model also helps therapists identify ruptures to relational trust and safety. Adolescents develop a more coherent attachment rupture narrative and improved tolerance of negative emotions (G. Diamond et al., 2021). Therapists help teens develop a “voice” to speak up about felt injustice rather than internalize this distress as low self-worth and self-punishment. Similarly, ABFT aims to increase parents’ reflective functioning; the ability to understand and empathize with adolescent felt experiences. This reduces parents’ reactivity and negative emotional expression, thus increasing their capacity for warmth and support. These individual skills are consolidated in family conversations where therapists engineer a positive attachment experience; parents listen while adolescents talk about difficult things (e.g., divorce, parental depression, feelings of being unloved and unlovable). In this way, ABFT aims to improve trust and safety between parents and their adolescent, thus reducing family conflict and increasing warmth. When the secure base of family life reemerges, parents are better able to support adolescent recovery and adolescents are more receptive to parent’s help.
Given the limited efficacy of behavioral treatments for BN/BED, it is likely that a treatment that fuses behavioral strategies for treating disordered eating (e.g., self-monitoring, reducing dietary restriction) with ABFT would have the greatest impact. By combining behavioral treatment (BT) strategies for BN and BED with ABFT, the two main pathways to disordered eating can be simultaneously targeted (Stice, 2001). BT strategies were drawn primarily from CBT for Eating Disorders (Fairburn, 2008) and include self-monitoring (i.e., writing down everything one eats and drinks), normalizing eating patterns (e.g., eating 3 meals and 1-2 snacks per day), and incorporating palatable foods into one’s diet, which all work to reduce dietary restraint (Fairburn et al., 2003). Further, as described above, ABFT has the potential to improve the efficacy of behavioral strategies by increasing the likelihood that parents can be effective drivers of change. As such, ABFT is well poised to be an effective augmentation to behavioral treatment for binge-spectrum EDs. However, ABFT has yet to be tested in a sample of adolescents with eating disorders. Thus, we conducted a small case series of a 16-week treatment for binge-spectrum eating disorders combining ABFT with behavioral strategies for eating disorders. We examined initial feasibility, acceptability, and changes in eating pathology and family processes.
Methods
Participants
Participants (N = 8) were adolescents (ages 12–18) with clinically significant binge eating and their associated primary caregivers. Participants were included in the study if they were able to speak, write, and understand English, were between the ages of 12–18, had a body mass index (BMI) of 18.0 kg/m2 or greater, and experienced 12 or more objectively or subjectively large binge episodes for the past three months. Participants were excluded from the study if they were at acute suicide risk, if no parent or guardian agreed to participate in the study, were currently receiving psychological treatment for an eating disorder, were currently receiving weight loss treatment, were experiencing a co-morbid clinically significant psychological disorder that would require attention beyond the study treatment and/or would interfere with study treatment (e.g., active psychotic disorder, acute substance dependence), or had a diagnosis of intellectual disability or autism spectrum disorder. The current study included 5 cisgender female adolescents (71.43%), 1 transgender male (14.29%), and 1 cisgender male (14.29%). Adolescent participants in the current study were 71.43% White (n = 5), 14.29% biracial (n = 1), and 14.29% Latinx (n = 1). Mean age of adolescents in the current study was 16.00 years (SD = 1.77). At baseline, 4 participants were diagnosed with OSFED bulimia nervosa, 2 with bulimia nervosa of low frequency, and 2 with binge eating disorder. One participant dropped out of treatment after session one due to COVID-19, and one participant was withdrawn from the study early in treatment due to need for inpatient support following acute suicidality; thus, we describe results from the 6 adolescents who completed treatment below. All participant names have been changed within this manuscript to protect privacy and confidentiality.
Procedures
Participants were recruited nationwide, given the remote nature of the study, via social media advertisements, and from the local Philadelphia area via professional referrals from the Center for Weight Eating and Lifestyle Sciences (WELL Center) at Drexel University. Social media advertisements included the following language: “Does your teen struggle with his or her eating? The WELL Center is currently recruiting teens and their parents to participate in a program aimed at helping families better support their teens with eating problems.”
Adolescent participants and a caregiver they lived with completed a phone screen to assess initial eligibility. During the phone screen, adolescent participants were asked to report current eating disorder symptoms (e.g., frequency of binge-eating and compensatory behaviors assessed via questions drawn from the Eating Disorder Examination 17.0; Cooper & Fairburn, 1987) and additional questions that corresponded with each of the inclusion/exclusion criteria described above.
Participants then completed a virtual baseline assessment. Eight adolescent participants and their families were deemed eligible and invited to participate in the study and receive treatment. All intervention was conducted via HIPAA-compliant Zoom platform due the COVID-19 pandemic.
Measures
Eating Disorder Symptoms
Adolescent eating disorder symptoms, including binge eating, compensatory behaviors, and body image concerns, were measured using the Eating Disorder Examination 17.0 (EDE; Cooper & Fairburn, 1987), a semi-structured clinical interview. The full EDE was administered at baseline and post-treatment. An abbreviated version of the EDE, which included only the binge module and compensatory behaviors section, was administered at all mid-treatment assessments (4 weeks, 8 weeks, and 12 weeks).
Perceived Criticism and Emotional Involvement
Perceived criticism and emotional involvement (i.e., expressed emotion) were measured using the Family Emotional Involvement and Criticism Scale (FECIS; Shields et al., 1994), a 14-item self-report measure. The FEICS was administered to all adolescents at baseline and post-treatment. An example item from the FECIS is, “My family is always trying to get me to change.” Items are scored on a 5-point Likert scale (i.e., 1 = Almost Never to 5 = Almost Always). This measure consists of two subscales, Emotional Involvement (Cronbach’s alpha = .76) and Perceived Criticism (Cronbach’s alpha = .82), with total subscale scores for each ranging from 7 to 49 (Shields et al., 1994).
Depression
Depression was measured using the Beck Depression Inventory-Second Edition (BDI-II; Beck et al., 1996), a self-report measure. The BDI-II was administered at all study assessments with both adolescents and parents. Total scores for the BDI-II range from 0 to 63 (i.e., 0–13 = Minimal, 14–19 = Mild, 20–28 = Moderate, 29–63 = Severe). Prior studies have indicated high reliability estimates for the BDI total score (Cronbach’s alpha = .90)(Osman, Downs, Barrios, et al., 1997).
Acceptability and Feasibility
Acceptability and feasibility of treatment was measured using the Acceptability and Feasibility of Treatment questionnaire, derived from several of our team’s previous treatment trials (Manasse et al., 2021a; Manasse et al., 2021b). This self-report measure was administered to both adolescents and their parents at post-treatment. An example item from the Acceptability and Feasibility of Treatment questionnaire is, “How effective was the treatment at improving your communication between members of your immediate family?” Participants were asked to rate each item on a 0 to 5 scale. Items were examined individually therefore a total score was not calculated for this measure. Of note, the Acceptability and Feasibility of Treatment questionnaire did not assess participant reactions to each component of the intervention, precluding a full understanding of participants’ full experience. Acceptability was also measured using a feedback interview developed by our team and administered with parents and adolescents separately at the post-treatment assessment.
Body Mass Index
Participants were asked to weigh themselves and measure their current height at home with a scale and a measuring tape and study staff calculated BMI using participant reported height and weight at the baseline assessment. BMI was used to ensure eligibility (i.e., a BMI > 18.0) and to monitor safety (i.e., to ensure no participant became underweight during the course of the study).
Therapeutic Alliance
Therapeutic alliance was measured using the Working Alliance Inventory (WAI; Horvath & Greenberg, 1989), a self-report measure. The WAI was administered at all post-treatment assessments to adolescents and parents. An example item from the WAI is, “My therapist and I have established a good under- standing of the kind of changes that would be good for me.” The appropriate items were reversed scored and a total score was derived.
Conflict About Eating
Conflict about eating was measured using a measure we developed, the Parent Involvement Questionnaire, as we could not find an established measure of this construct. This self-report measure was administered to adolescents at all assessment points. An example item from the Parent Involvement Questionnaire is, “How often do you have conflict with one or more of your parents about your eating behaviors?” Individual items were examined to characterize conflict between parent-child dyads; total scores were not calculated for this measure.
Family Conflict
Conflict between adolescent and parents was measured using the Conflict Behavior Questionnaire (CBQ). This 20-item self-report measure was administered to adolescents at baseline and post-treatment. An example item from the CBQ is, “At least three times a week, we get angry at each other.” Participants were asked to rate each statement as true or false based on their experiences with their current primary caregiver in the past 2 weeks. Total scores were calculated by summing the total number of statements that participants indicated as being true. Total scores ranged from 0 to 20; 11 is considered the clinical cutoff for clinically significant conflict. Prior studies have indicated high reliability estimates for the CBQ total score (Cronbach’s alpha = .93; Rengasamy et al., 2013).
Structure of ABFT + B Treatment
ABFT involves five tasks, or processes, that support the parent-child relationship. The first half of treatment (Tasks 1–4) focuses on improving the quality of the parent-child relationship through the identification, verbalization, and processing of conflict in the family. The process of repair begins in Task 1 (relational reframe), when the therapist helps family members to access their longing for rebuilding trust and strengthening the relationship as a first goal of therapy. Then adolescents are encouraged in individual sessions (Task 2, Adolescent Alliance) to identify and articulate their experiences of the attachment failures (e.g., mis-attunement, neglect, parentification) and commit to a discussion of these experiences with their parent(s). Parent(s), in simultaneous individual sessions (Task 3, Parent Alliance) are encouraged to consider how their current stressors and own intergenerational legacies affect their parenting and their adolescent’s experience, which typically leads to greater empathy for their adolescent’s challenges. The therapist brings the family members back together in Task 4 (Attachment). Here, therapists help adolescents discuss their experiences of relationship ruptures with the parent. Therapists help parents support their adolescent in describing how these ruptures have strained their bond and damaged trust. Parent(s) are coached to respond in a caring, empathic, and respectful manner. As warmth and trust begin to emerge, the second half of treatment focuses on promoting adolescent autonomy and extra familial functioning (e.g., improving school performance, finding a job, returning to social activities; Task 5, Competency Building). The number of sessions in each task is flexible depending on patient need, though the total duration of treatment is 16 weeks (See Appendix A for more information).
In the present study, therapists and individuals or families met approximately bi-weekly in weeks 2–5 and once weekly in week 1 and weeks 6–16. For further information, Appendix A shows an outline of the 16 session ABFT + B treatment. Due to the pilot nature of integrating ABFT with behavioral eating disorder treatment, each family had two therapists (one who was expert in eating disorders, and another who was expert in ABFT). Consistent with the nature of the ABFT treatment, therapists had some flexibility with the timing of each task (e.g., Task 4 may take more than 1 week), however, Appendix A provides the ideal timing of each task across the ABFT + B treatment. Behavioral (BT) components were integrated with ABFT sessions in two ways. First, during Tasks 1, 2 and 3, therapists provided psychoeducation and BT treatment strategies (e.g., regularizing eating, self-monitoring of eating) in tandem with Tasks 1 and 2. Task 4 is process-oriented and focused on creating a corrective attachment experience between adolescent and parent, thus BT components were not integrated into Task 4 processes. During task 5, therapists integrated BT treatment skills to support the family in working together to change eating behavior.
Statistical Analyses
All analyses were conducted using SPSS version 26.0. Descriptive statistics of central tendency and variability were calculated for frequency of ED behaviors, and self-report questionnaires. We employed the thematic analysis framework (Braun & Clarke, 2006) to identify several themes from qualitative interviews completed with adolescent and parent participants at post-treatment (see Appendix C for interview questions). The first author (SM) first identified broad response categories, and all participant responses were then reviewed and categorized by two authors (SM & EL), and consensus was reached through discussion where categorizations disagreed.
Results
Treatment Feasibility & Acceptability
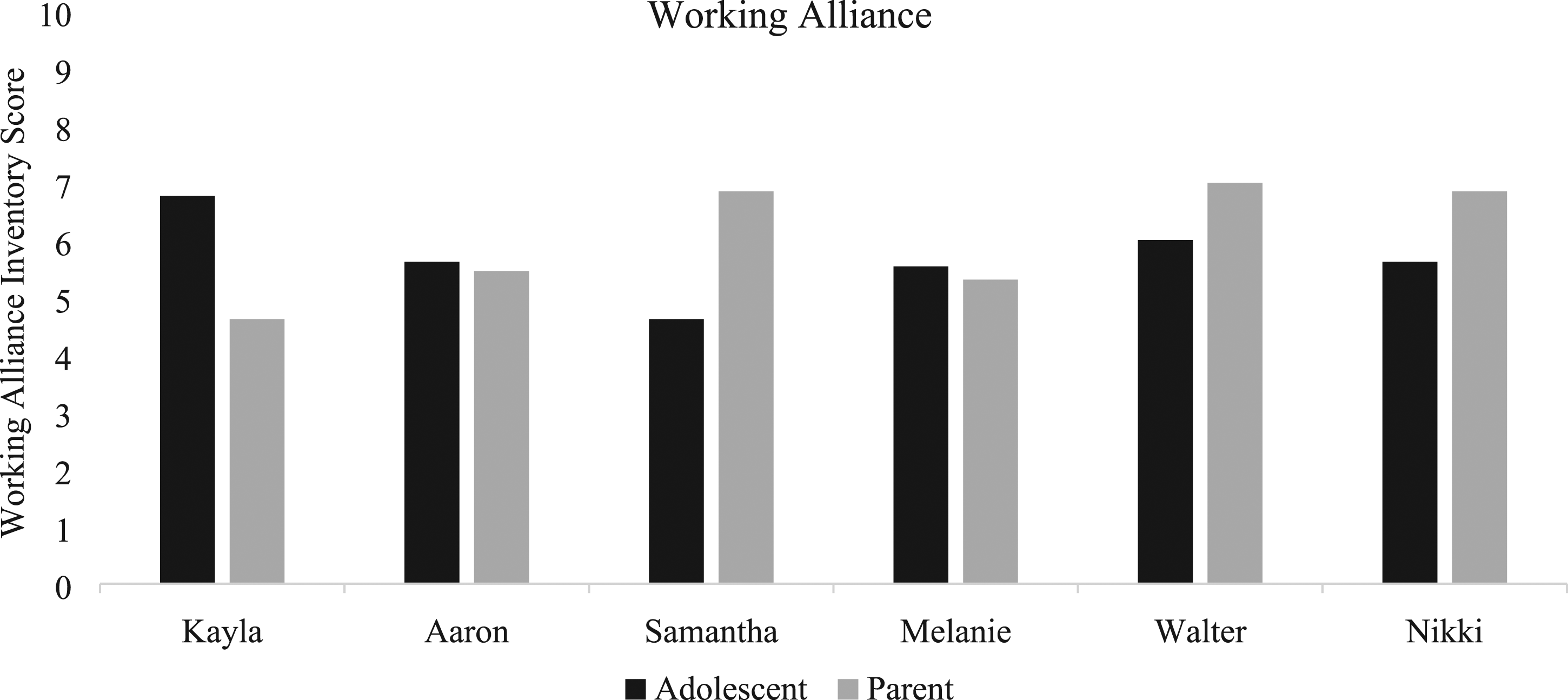
The treatment was feasible to deliver, as evidenced by six out of eight patients completing the full ABFT + B (75.00% retention). One participant dropped out of treatment after session one due to falling ill with COVID-19 and one participant was withdrawn from treatment due hospital admission for suicidality. The treatment was also found to be fairly acceptable to adolescents, on average rating 3.29/5 for looking forward to sessions, 3.86/5 for the usefulness of sessions, 3.43/5 for wanting to continue treatment (Figure 2). Adolescent working alliance was high on average (M = 5.60/8, SD = 1.54; Figure 3). Parents found the treatment to be highly acceptable, rating 4.6/5 for their overall satisfaction with the treatment on average. Parent working alliance was also quite high (M = 6.29/8, SD = 0.79; Figure 3). Adolescent acceptability scores at post-treatment. Adolescent (top) and parent (bottom) working alliance at post-treatment.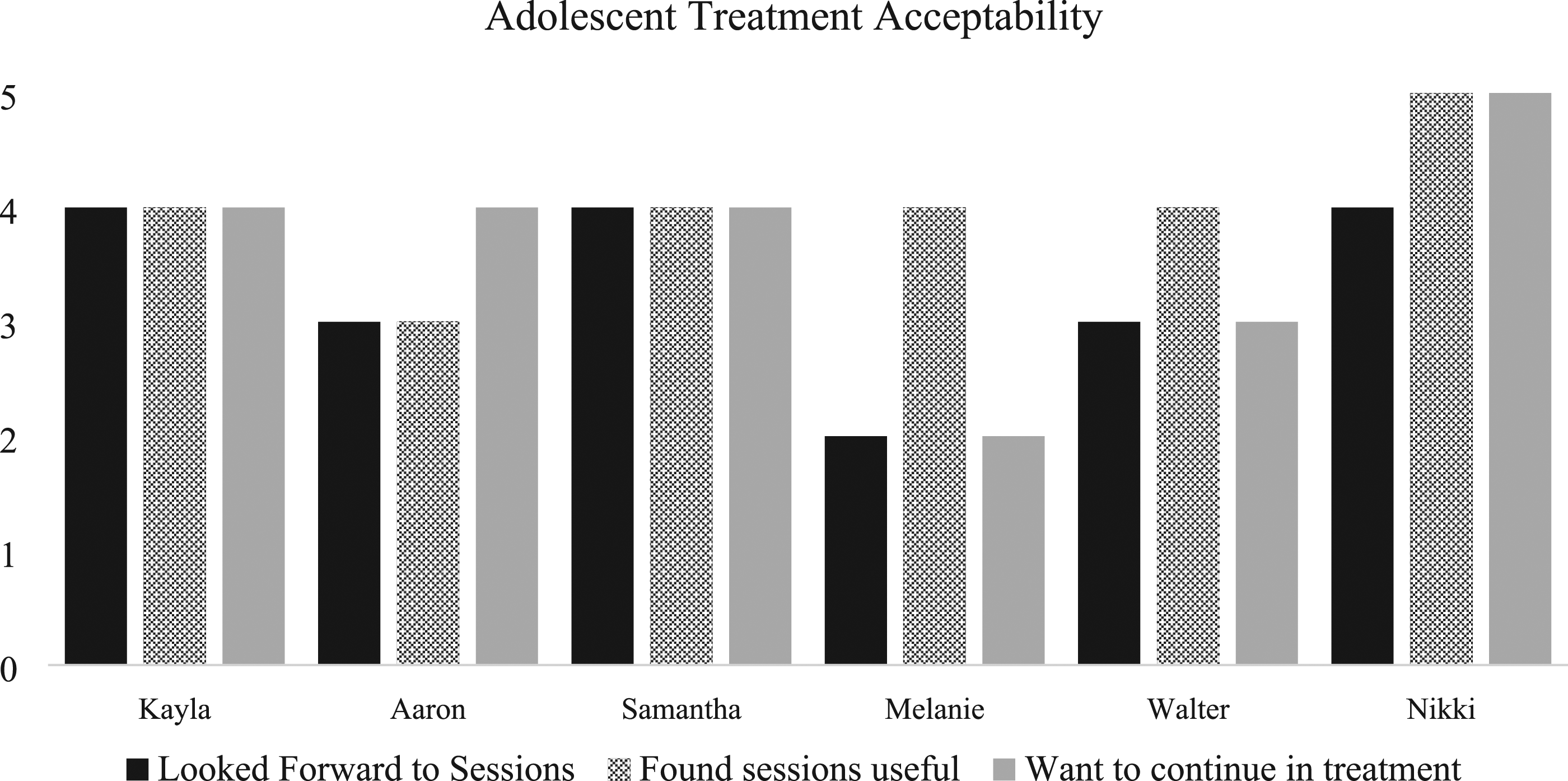
Qualitative Feedback
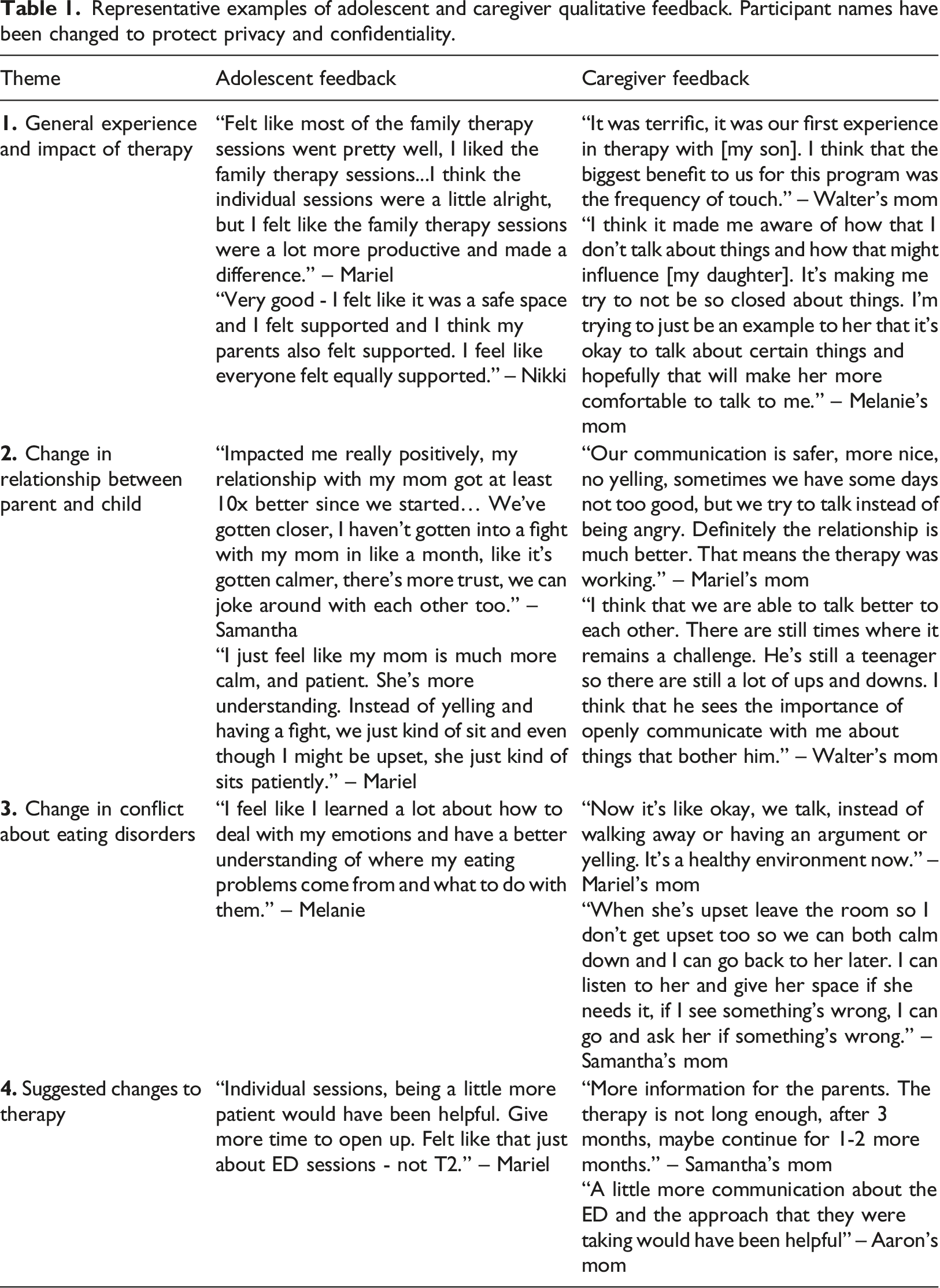
Representative examples of adolescent and caregiver qualitative feedback. Participant names have been changed to protect privacy and confidentiality.
Change in Family Conflict
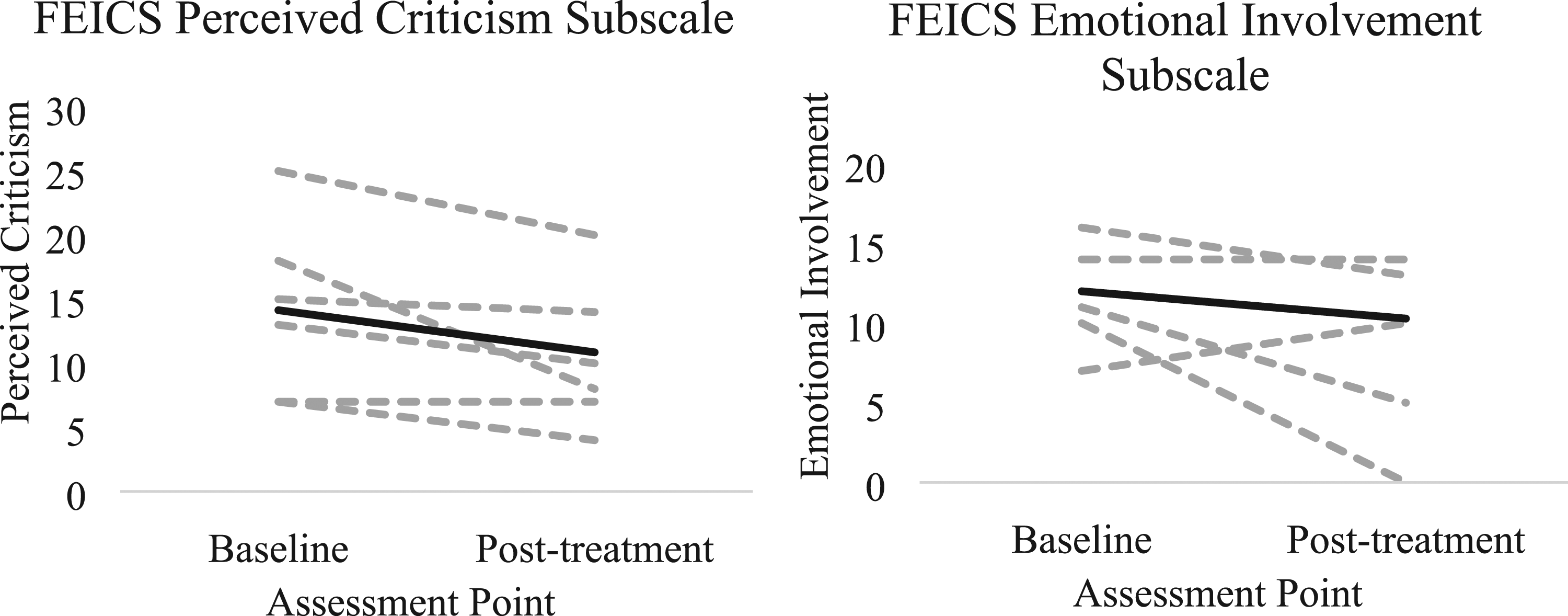
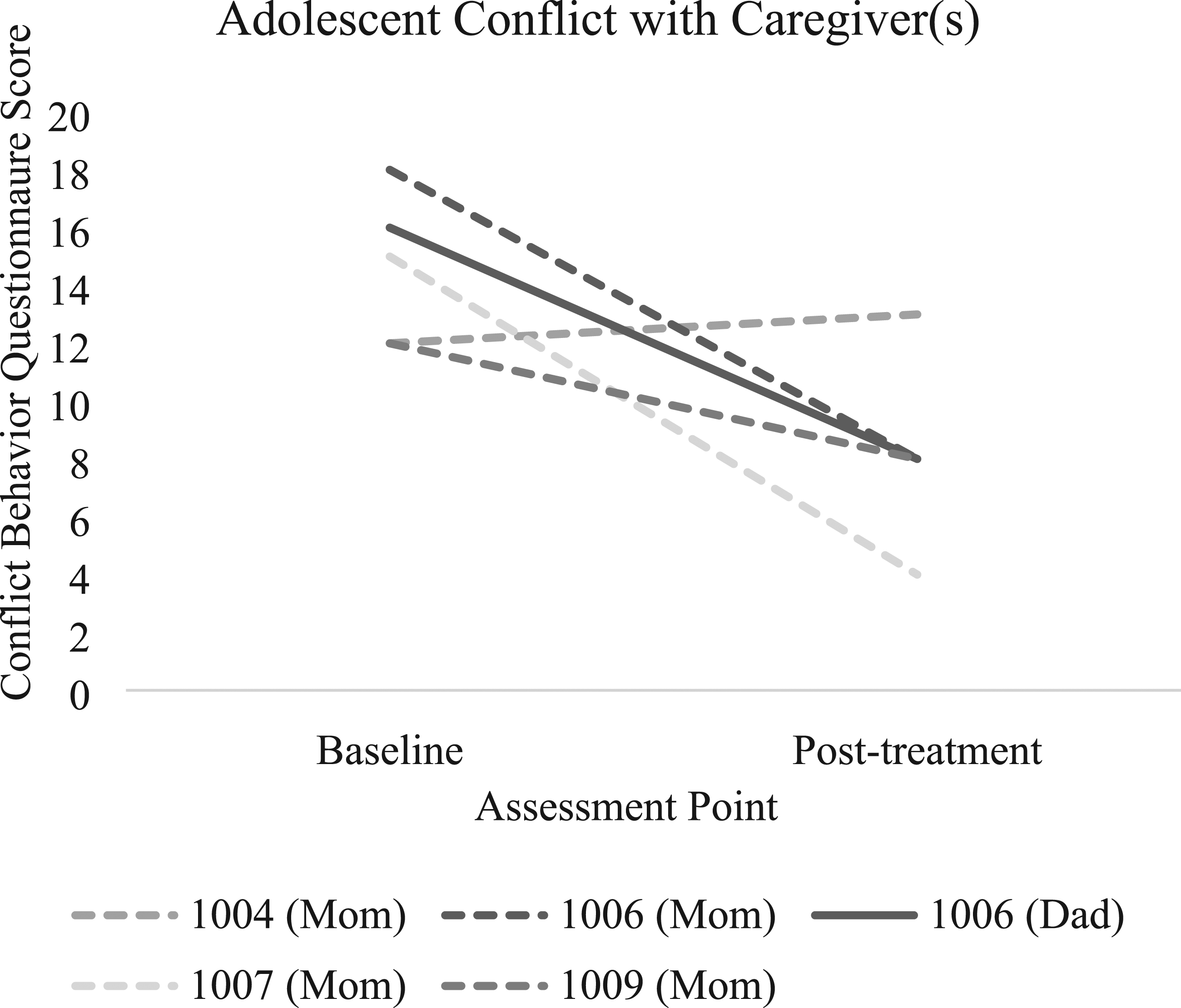
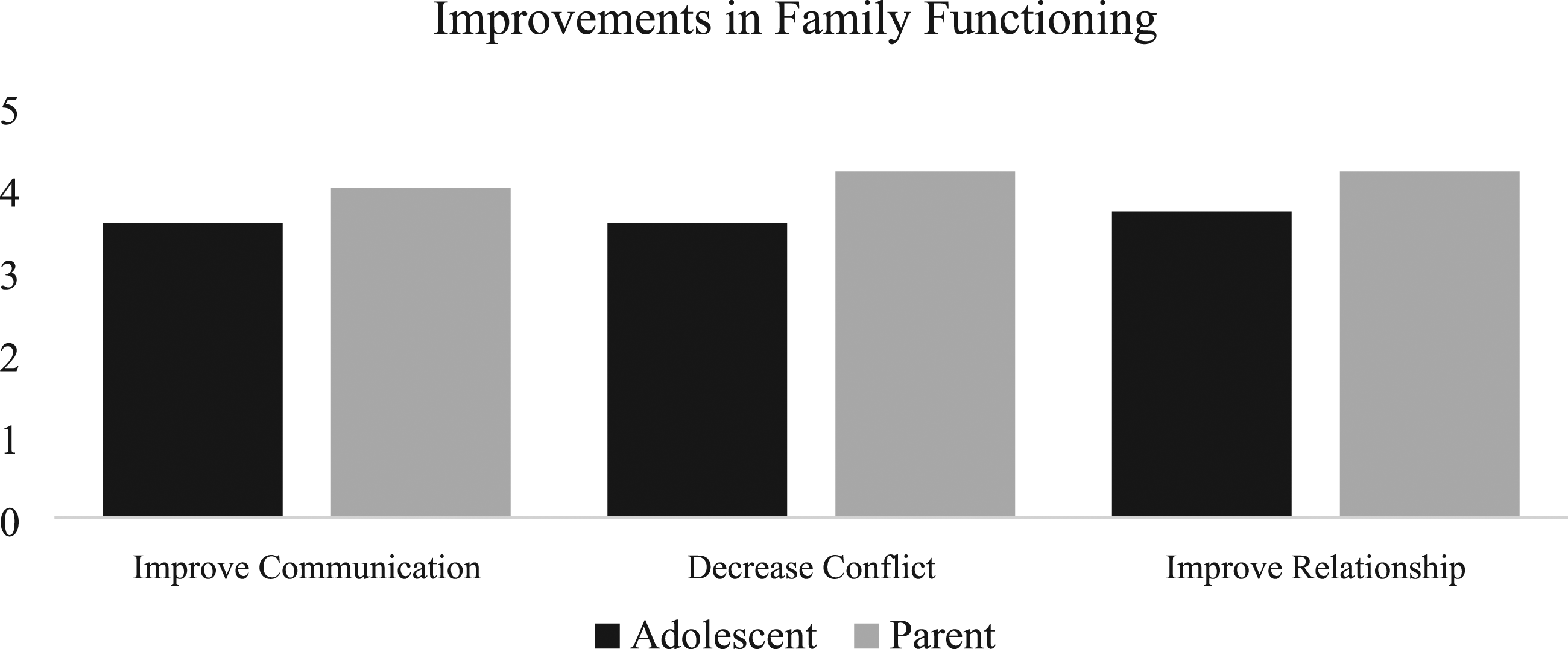
We saw differences in reported frequency of conflict about eating behaviors over the course of treatment (Figure 4). We also saw decreases on average in adolescent perceived criticism (MBaseline = 14.14, SDBaseline = 6.28; MPost-tx = 10.86, SDPost-tx = 5.30) and parent emotional involvement (MBaseline = 12.00, SDBaseline = 3.00; MPost-tx = 10.29, SDPost-tx = 5.79; Figure 5). We also observed moderate decreases on average in adolescent reported conflict in general (MBaseline = 15.33, SDBaseline = 2.94; MPost-tx = 7.67, SDPost-tx = 3.14; Figure 6). Adolescents also perceived improvements in family functioning at post-treatment, rating 3.57/5 (with 5 as the greatest possible amount of improvement) on average for improvement in communication with their caregivers, 3.57/5 for decreasing conflict with caregivers, and 3.71/5 for improving their relationship with caregivers (Figure 7). Parents rated 4.0/5 on average for improvement in communication with their child, 4.2/5 for decreasing conflict with their child, and 4.2/5 for improving their relationship with their child (Figure 7). Adolescent reported frequency of conflict about eating behaviors across treatment (sample average is noted in black). Adolescent perceived criticism and parent emotional involvement (as measured by the FECIS) over the course of ABFT + B treatment (sample average is noted in black). General adolescent-reported conflict with each of their primary caregivers at pre- and post-treatment. Adolescent (left) and parent (right) reported ratings of improvements in family functioning at post-treatment.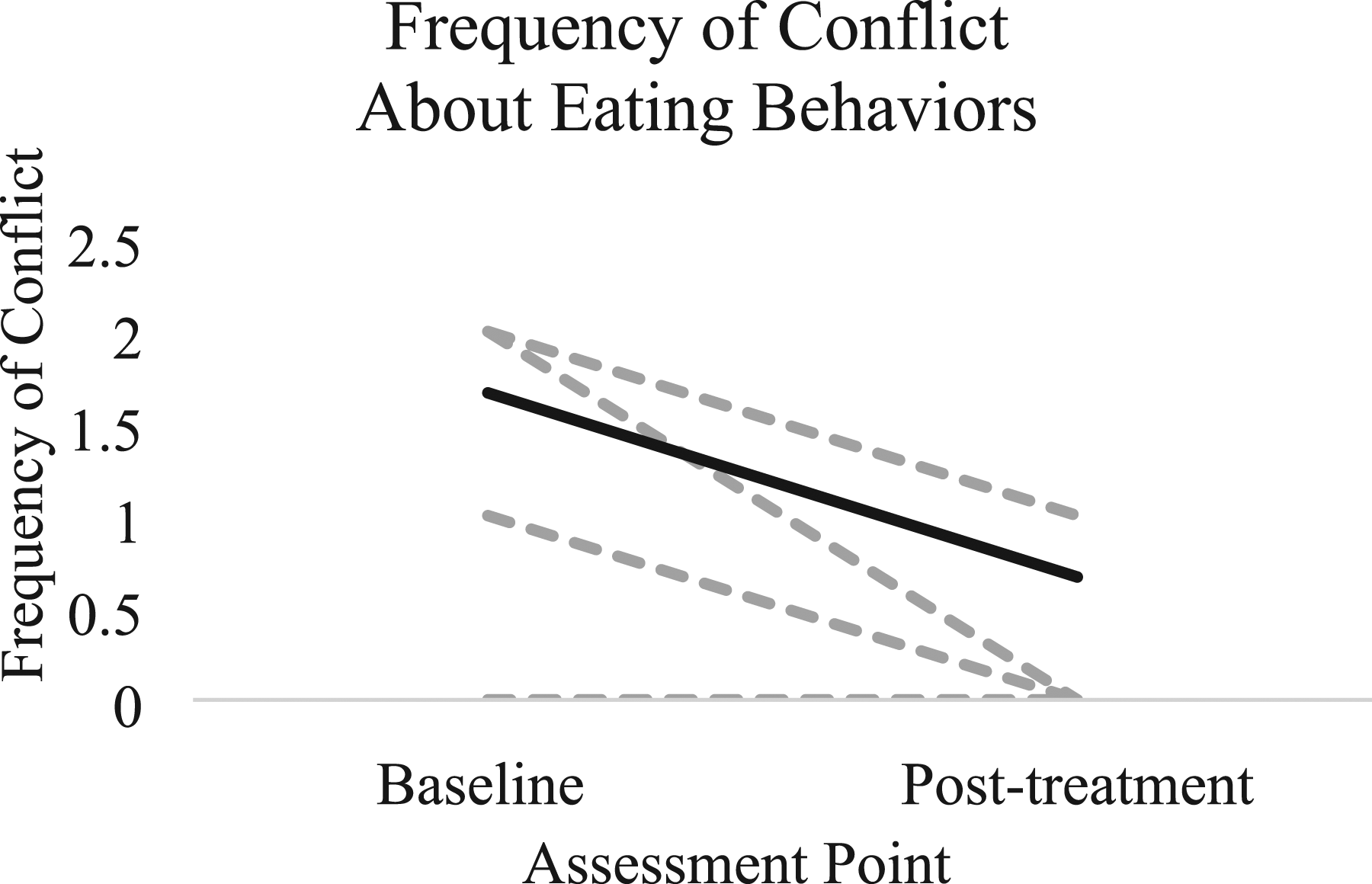
Change in ED Symptoms
Most participants showed improvement in eating disorder symptoms across the treatment, with four out of six participants reaching abstinence from binge eating at post-treatment (Figure 8). We also saw an average reduction of 2.07 points in participants’ EDE global scores (Baseline M
EDE
= 3.44, SD = 1.61, and post-treatment M
EDE
= 1.37, SD = 1.40). Adolescents also perceived reductions in their ED behaviors, rating 3.71/5 on average for perceived improvement in ED behaviors on the treatment acceptability questionnaire. Parents rated 3.8/5 on average for perceived improvement in their child’s ED behaviors on the treatment acceptability questionnaire. Eating pathology over the course of ABFT + B treatment (sample average is noted in black, with each dotted line representing a single participant).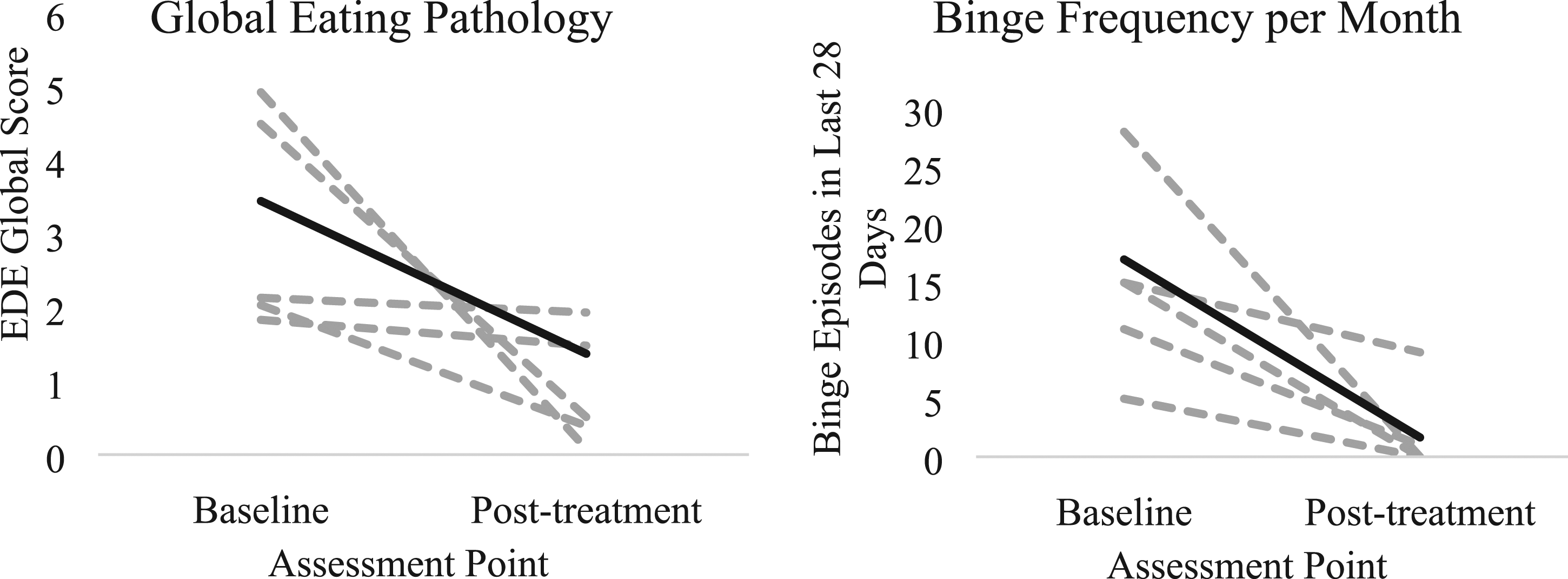
Adolescent and Parent Depression
We observed large decreases in adolescent depressive symptomatology across the treatment (MBaseline = 37.33, SDBaseline = 12.53; MPost-tx = 18.50, SDPost-tx = 13.13; Figure 9). We also observed moderate decreases in parent depressive symptomatology across treatment (MBaseline = 12.00, SDBaseline = 5.48; MPost-tx = 7.00, SDPost-tx = 4.95; Figure 9). Adolescent and parent depressive symptoms at pre- and post-treatment (sample average is noted in black).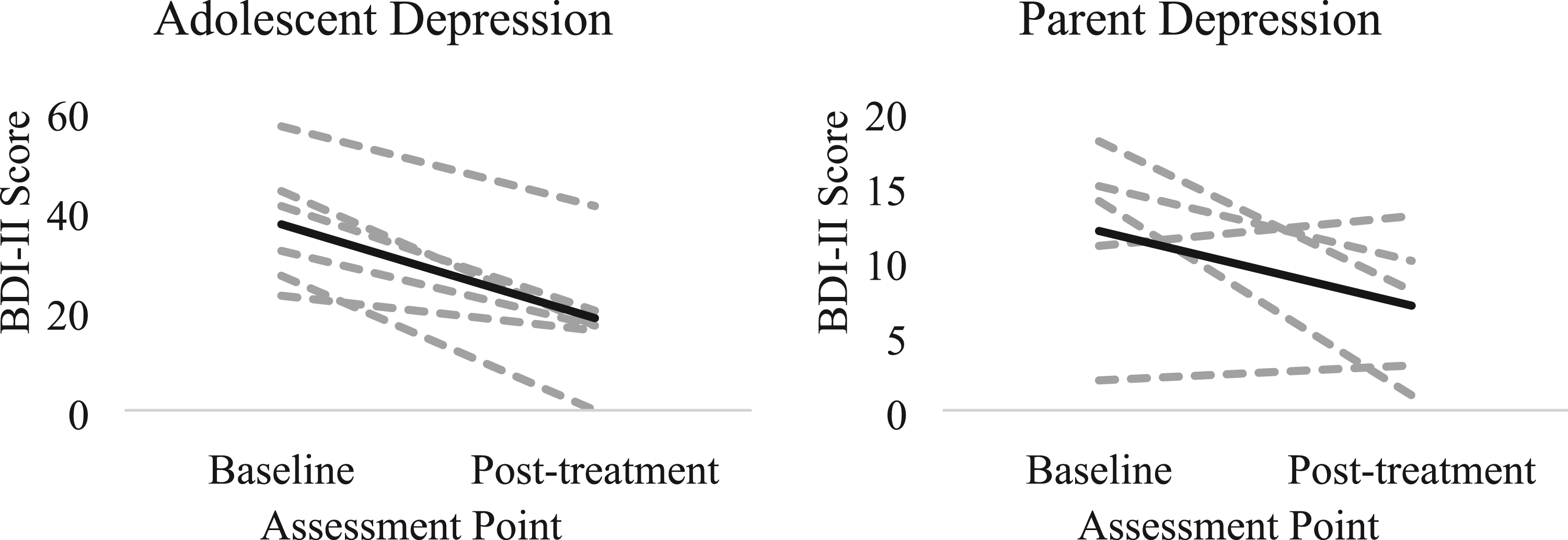
Discussion
This the first study to test ABFT in eating disorders and one of the first to fuse behavioral strategies with a process-based family therapy. Overall, in our case series, ABFT + B appeared to be feasible and acceptable, and was associated with large changes in eating pathology and improvements in family functioning.
We were successfully able to integrate behavioral strategies with ABFT and there was only one treatment dropout, indicating that the treatment was feasible to deliver. Additionally, the treatment was acceptable, as both quantitative and qualitative data indicated that parents were highly satisfied with the treatment and highly aligned with therapists. Adolescent ratings of the treatment and the therapist were between neutral and positive; such ratings are consistent with other ED treatment studies for adolescents (DeBar et al., 2013; Hilbert et al., 2020; Manasse et al., 2021a). However, neither adolescents nor parents reported feasibility and acceptability of specific treatment components. As ABFT is highly emotion-focused, it is possible that adolescents were emotionally uncomfortable during sessions, leading to somewhat lower acceptability scores. In summary, however, parent and adolescent ratings of acceptability and therapeutic alliance indicate adequate acceptability of the treatment.
We observed mixed evidence that the treatment improved family functioning (i.e., family conflict and cohesion). Adolescents reported that conflict with their mothers decreased to a large degree, but that expressed emotion (i.e., parental criticism) did not. Although we did not empirically compare parent and adolescent ratings of improved communication, decreased conflict, and improved relationship, it appeared that parents rated greater improvements in these areas compared to adolescents, with the exception of decreased conflict as adolescents reported decreases in conflict. Interestingly, qualitative data from both parents and adolescents overwhelmingly supported the notion that ABFT + B enhanced family communication, reduced conflict, and improved parent-child relationships overall. As such, it is possible that our measures did not fully tap into the ABFT + B’s mechanisms (with the exception of conflict) and the sample size is too small to assume these outcomes are reliable. We also did not measure the family’s culture around food and/or specific communication styles surrounding body image, weight and food, which may strongly influence child reports of family functioning and/or expressed emotion. Future studies should employ other measures of family functioning (perhaps those specific to eating behavior) that may be more sensitive to ABFT’s impacts and/or examine other potential mechanisms (e.g., attachment security).
While impacts on family functioning measures were mixed, ABFT + B was associated with changes in binge eating, global eating pathology, and depression symptoms. Changes in binge eating and eating pathology are comparable to or larger than other adolescent treatment studies for binge-spectrum eating disorders. For example, 66.7% (4/6) of participants achieved binge eating remission at post-treatment. Interestingly, not only did adolescent depression improve, but parent depression also clinically improved. It is possible that reduced conflict and improved relationship quality through ABFT + B positively impacted parental psychological status. It is possible that ABFT + B could be a good fit for families with adolescents and caregivers experiencing current/past depression which is consistent with the fact that ABFT was originally developed for depression. Although the sample is small, changes in eating disorder and psychological outcomes associated with ABFT + B indicate that it is a highly promising treatment for adolescent binge-spectrum eating disorders worthy of further investigation.
The present study was characterized by numerous strengths and weaknesses. Strengths included patients with binge eating and varying levels of restrictive/compensatory behaviors (see Appendix B for detailed information on participant ED behavior engagement) and the fact that the treatment was remotely-delivered, supporting its potential scalability. However, a major limitation was the small sample and open trial design; future research should conduct a clinical trial of ABFT + B against an active control group. Additionally, due to the pilot nature of integrating ABFT with behavioral eating disorder treatment, each family had two therapists (one who was expert in eating disorders, and another who was expert in ABFT). This may be seen as both a strength and a limitation of the current study, since this design offered the best integration of ABFT and ED treatment. However, although these therapists were of varied training levels, two therapists per client may not be scalable and as such, future studies might train therapists in both eating disorder treatment and ABFT. This study also did not measure family cultures surrounding food, which likely impact how children perceive their family functioning in the context of the ABFT + B treatment. Future studies should explore the role of family cultures around food more fully. Additionally, this study was unable to distinguish between the impact of ABFT versus the behavioral strategies; future research should aim to isolate the impact of ABFT on family functioning and disordered eating behavior. This could be assessed through additional questions on the qualitative interview or through quantitative means, such as creating a list of major treatment strategies and asking families to rate each for perceived helpfulness. A final limitation is that there are several components to the ABFT model and treatment; it is possible that only one or a few of these components are necessary, but the present study design does not allow for identifying active components.
In summary, ABFT + B is a feasible and acceptable treatment that has impacts on family functioning and disordered eating behavior. Future studies should further examine its efficacy and for whom it will be most effective.
Supplemental Material
Supplemental Material - Attachment-Based Family Therapy to Improve Family Functioning in Adolescent Binge-Spectrum Eating Disorders: An Initial Evaluation Via Case Series Design
Supplemental Material for Attachment-Based Family Therapy to Improve Family Functioning in Adolescent Binge-Spectrum Eating Disorders: An Initial Evaluation Via Case Series Design by Stephanie M. Manasse, Jody Russon, Elizabeth Lampe, Allie King, Sophie Abber, Claire Trainor, Lindsay Gillikin, Suzanne Levy and Guy Diamond in Clinical Child Psychology and Psychiatry
Footnotes
Author’s Contribution
SM conceptualized the study design and methods. SR and LG oversaw data collection. JR, EL, AK, SR, CT, LG were involved in initial drafting and revision of the manuscript. SL and GD reviewed the manuscript and were involved in the revision process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Manasse is supported by an award from the National Institute of Health (K23DK124514).
Ethical Approval
All study procedures were approved by the Drexel University Institutional Review Board and all subject provided informed consent.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.