
Abstract
People with Neurodevelopmental (ND) conditions are often unfairly stereotyped by society, without fully appreciating their strengths. As a result, their advantageous behaviours may be overlooked or ignored. Despite wide psychoeducation on ND in society there is a push from the scientific and ND community to move from a binary diagnostic system to an approach that encompasses the spectrum experienced by individuals. In view of this, we have developed the Portsmouth Alliance Neuro-Diversity Approach (PANDA), a coproduced method which helps facilitate understanding, communication and early support for individuals who may be Neuro-Diverse. 51 young people, their parents and attached professionals participated in the approach’s feasibility to improve wellbeing and symptom management measured by quantitative and qualitative means. Results showed a significant improvement in the child’s wellbeing, but not symptom management. Overall, this indicates the PANDA could facilitate a more holistic approach for referrals, information gathering, psychoeducation and cross-system relationship building to be used in conjunction with a traditional pathway. Though, this study is limited in scope, its main purpose is to inform future development of the approach. Additionally, more research investigating the specific narrative, and separate structure of the PANDA would be required to highlight the strengths and limitations of implementation.
Keywords
Introduction
Modelling Neurodevelopmental Conditions
Neurodevelopmental (ND) conditions have been understood and researched within the scientific community for well over 50 years. Most of the research in ND conditions being viewed through the medical model of “disorders” (Van Wijngaarden-Cremers et al., 2014). This model attempts to reduce or cure symptoms, identifiable via the deficits said to cause significant impairment to daily life (Baker, 2011). Seemingly however, ND conditions do not have a biological marker, with at best a genetic aetiology (Bai et al., 2019). Therefore, in their absence, the medical model mostly ascertains deficits based on behavioural deviations from the norm (Anckarsäter, 2010).
Due to the methodology of disorders classification, it tends to invalidate or dismiss advantageous, possible holistic reasons for, and society’s role in determining the appropriateness of these behaviours (Norbury & Sparks, 2013). This labelling of “disorder” and omission of advantages could enforce the societal view that these patterns of behaviours are inherently pathological and require a form of treatment to “cure” these “undesirable” conditions, to shift these individuals closer to the average (Falissard, 2021). The pathologizing model therefore does not differentiate between conditions resulting mainly from poor fit between person-environment and conditions that are the sole causes for the observable deficits (Baker, 2011), with the ND community exclaiming “It is society that disables us” (Kenny et al., 2016).
Despite the pathologizing, ND individuals do not typically view themselves within this treatment model (Kapp et al., 2013; Shaw, 2021), but these opinions are dismissed from the medical community as a lack of epistemic authority on the topic (Hens et al., 2019). However, those who are quick to dismiss the lived experiences are the same neurotypical researchers and professionals who contribute to the technocratic power structures (Evans, 2013). Despite this, there is recent push back against this top-down dictation of ND research, with The Shaping Autism Research UK advocacy group pushing for a more inclusive research methodology (Fletcher-Watson et al., 2021; Niner & Portman, 2021). Overall, there is a need for a newer, more progressive system to understand, support and explain ND differences.
Concept of Neurodiversity
Neurodiversity” was a term coined by Sociologist Judy Singer referring to the natural variation observed in the human brain in a non-pathological sense (Singer, 1999). It is now used to describe a range of neurocognitive developmental disorders, including Autism Spectrum Disorder, Attention Deficit Hyperactivity Disorder and Dyslexia (Doyle, 2020; Kapp et al., 2013).
Lead autism researcher Simon Baron-Cohen offered four key advantages that neurodiversity approaches and terminology provides over standard diagnostic procedures in his Editorial Perspective (2017): 1) Terminology is inclusive of scientific and philosophical underpinning of development being within a spectrum, that there is no single brain which is “normal”, as during development the brain can be wired up in many ways. 2) Avoids stigmatized labels which can be damaging to a child’s development (Gibbs and Elliott., 2015) thus fulfilling the need for more ethical, non-stigmatizing language and concepts for thinking about people who are different. 3) Neurodiversity would build a framework that takes a balanced view, to give equal attention to what a person can and cannot do. There is still disagreement within the ND community if diagnostic labels like ASD or ADHD are seen as helpful or problematic (Riccio et al., 2021), but they acknowledge that there is a need to focus on an individual’s talents which can be lost through diagnostic labelling (Kenny et al., 2016). 4) Neurodiversity is inclusive of the biological variation that is intrinsic to a person’s identity, which should be given equal respect alongside other forms of diversity.
Despite the neurodiversity movement, there is a gap within clinical and educational practice to develop a tool to help these professionals format discussions with individuals under the theme of neurodiversity.
Supporting Neurodiversity
Research has provided insight into the positive effects of environmental changes for neurodivergent individuals, and the benefits when removing societal barriers. This paper has noted major factors to support a neurodiversity approach.
Factor 1 - Psychoeducation
Psychoeducational courses have been shown to increase the levels of wellbeing and satisfaction in parents, teachers and neurodivergent individuals. (Zhou et al., 2019). These courses have also been shown to improve the child’s symptom management as reported by clinical staff, educational professionals, caregivers, and child (Dahl et al., 2020). De-stigmatisation, and reduction of ND individuals adopting stereotypical beliefs has been a possible reason for these improvements (Gibbs et al., 2020; Gibbs and Elliott. 2015). Parents have reported increased bonding with their child (Legg & Tickle, 2019). Implying that psychoeducation increases positive parental perceptions of ND, which may improve their neurodivergent child’s self-esteem by enabling parties to reframe to a strengths-based perspective.
Factor 2 – Professional Relationships
Despite the quality of the relationship between parents and clinicians being reported as crucial in improving parent experiences (Abbott et al., 2013), parents have reported feeling excluded by clinicians during the diagnostic process (Griffith et al., 2013; Potter, 2017). Additionally, Crane et al. (2018) found that autistic adults, parents, and healthcare professionals identified lack of awareness from teachers as a barrier for care. This can be supported by use of a need’s led approach viewing a child beyond these labels, which takes into consideration “threshold cases” where a child may not display enough “need” for a label but there are still significant needs present. Using a participatory design involving parents, neurodivergent individuals and education professionals should increase feelings of inclusion and break down barriers to support. This design promotes neurodivergent autonomy and empowers teachers in their approach (Leadbitter et al., 2021) and adopts the “nothing about us without us” (Charlton, 1998) mantra intrinsic to disability rights.
Factor 3 – Early Support
Parents typically report waiting around a year between having their initial concerns and seeking help through diagnosis with many parents citing the long wait times as the key cause of their stress (Crane et al., 2016). This stress is exacerbated when parents are alone finding information on the internet, sometimes believing “the worst-case scenario” (Connolly & Gersch, 2013). Overall, post-diagnosis support is reported as unsatisfactory by autistic adults, parents, and professionals (Crane et al., 2016; 2018; Potter, 2017), which is often anticlimactic and does not produce the support expected. There is an identified need for early access to a service that provides screened information packs and signposting to ongoing support networks, which result in positive attitudes to service and empowerment. (Connolly & Gersch, 2013).
At its core, the PANDA was developed to provide a holistic experience using the crucial factors mentioned above (i.e., psychoeducation, fostering professional relationships through inclusion and empowerment and providing timely assessment and early support). PANDA was coproduced with individuals with lived experienced and multidisciplinary professionals from field of education, health, and social care.
The aim of the current study was to evaluate the feasibility of introducing this new approach for neurodiverse young people. Two hypotheses for this pilot are: 1. The approach will improve the wellbeing of the child from the perspective of the professional, the parent/carer and the child. 2. The approach will improve the symptom management of the child from the perspective of the professional, the parent/carer and the child.
Methods
Recruitment process and enrolment of participants
Information about the study was disseminated to educational settings within the Portsmouth Local Authority, Solent NHS CAMHS and Education Psychologist Team. Only professionals who completed the Neurodiversity training were able to refer participants. Prior to inclusion, all participants received a phone call from a member of the research team. No compensation was offered.
Participants
51 young people participated, average age of 7.98 years (SD = 2.61; Range = 3–15 years) with 64.7% Males and 35.3% Females. 96% of the participants were referred from educational institutions while 4% were referred from health care.
Inclusion and exclusion criteria
Inclusion criteria were (1) Identified by a Neurodiversity trained professional as having an issue in one of the nine Neuro-Diversity subsections (2) Has a primary caregiver willing to participate. (3) Aged 3 – 18 (Inclusive). (4) In a Portsmouth educational institution. (5) Is in the catchment area for Portsmouth CAMHS.
Exclusion criteria to avoid potential data contamination was: (1) Participant in another research intervention trial in the past 2 months. (2) Undergoing treatment specific for ND conditions. (3) More than 4 months from starting a treatment process. (4) Primary caregiver insufficient use of spoken English that could exclude them from fully engaging with research materials.
Treatment fidelity
Each educational professional attended a structured training on the approach, split across three 4-hour long sessions. Moderation and support were offered in person during each session, alongside drop-in weekly supervision sessions with research team members to ensure treatment fidelity. The training manual was written by the developers of the approach, and relied on their extensive clinical, lived, and academic experiences.
Procedure
Protocol
1. Once referred, potential participants were screened in accordance with the project’s inclusion and exclusion criteria. A consent meeting was co-ordinated at the young person’s educational setting with educator, child, and parent present. 2. Participants were asked to complete baseline questionnaires and reminded not to discuss answers. Project materials were provided and required to be read before the next meeting 1–2 weeks later. Supplementary material for reading ages 7+ was provided. 3. This meetings aim was to complete the profile building and related strategies and resources. Confirmation was required before the meeting could proceed that participant had read the material provided. Repeat questionnaires were completed after the profile was completed. 4. Three months later, participants were met with again to reflect on the process. Questionnaires were completed again, and participants were asked if they consented to be contacted for the second qualitative stage of the project.
Focus Groups
Focus groups were split according to their respective participant membership, either parents/carers or educational professions with convenience sampling. Participants met in groups of 4–5 for about 1.5 hours. Groups were facilitated by two of the authors.
Interviews
Interviews were conducted for the young people. These participants met with two of the authors at their educational institution for roughly 1.5 hours. The facilitators outlined the purpose of the interview to discuss their experience with profiling.
Materials
(Child) Outcome Rating Scale
The Child Outcome Rating Scale (CORS) and Outcome Rating Scale (ORS) are a self-reported four-item analogue scale to measure the change of life functioning due to interventions. These four areas include: symptom distress; interpersonal well-being; social role; and overall wellbeing. The ORS and CORS differ on the accessibility of language used. The ORS uses language reflective of a 13-year-old’s reading level, while the CORS has more child friendly language and pictures of faces in each dimension to facilitate understanding (Duncan et al., 2003). Research on the measures demonstrates high reliability and validity (Murphy, & Rakes, 2019), and is a routine measure used in CAMHS (Child and Adolescent Mental Health Services).
Strength and Difficulty Questionnaire
The Strengths and Difficulties Questionnaire (SDQ) is a behavioural self-reported questionnaire. The SDQ asks 25 statements on a 3-point Likert scale (Not True, Somewhat True, Certainly True). There are three versions of the SDQ based on the person completing the questionnaire; Parental, Teacher and Student. The SDQ is a well-established tool with good reliability and validity (Muris et al., 2003).
Quantitative Analysis
Both the wellbeing and symptom management efficacy-related measures were analysed using a series of repeated measures ANOVAs with a baseline score, profile building score and post-intervention score as a within-subjects repeated measure factor.
Qualitative Analysis
Interview and focus group data was analysed using thematic analysis (Braun & Clarke, 2006). The first stage of the analysis, transcribing, was performed by the third author of the paper, and during this process initial thoughts and ideas were noted down. In the second stage, data was read and re-read several times and descriptive codes were generated, which was then reviewed by the first author. The authors considered how to retain the variation of the initial codes, while producing higher order themes to group the codes. The research question of the impact of PANDA in the lives of participants informed this process. Themes were reviewed prior to defining and naming them, to which they were finalised.
Results
Quantitative Results
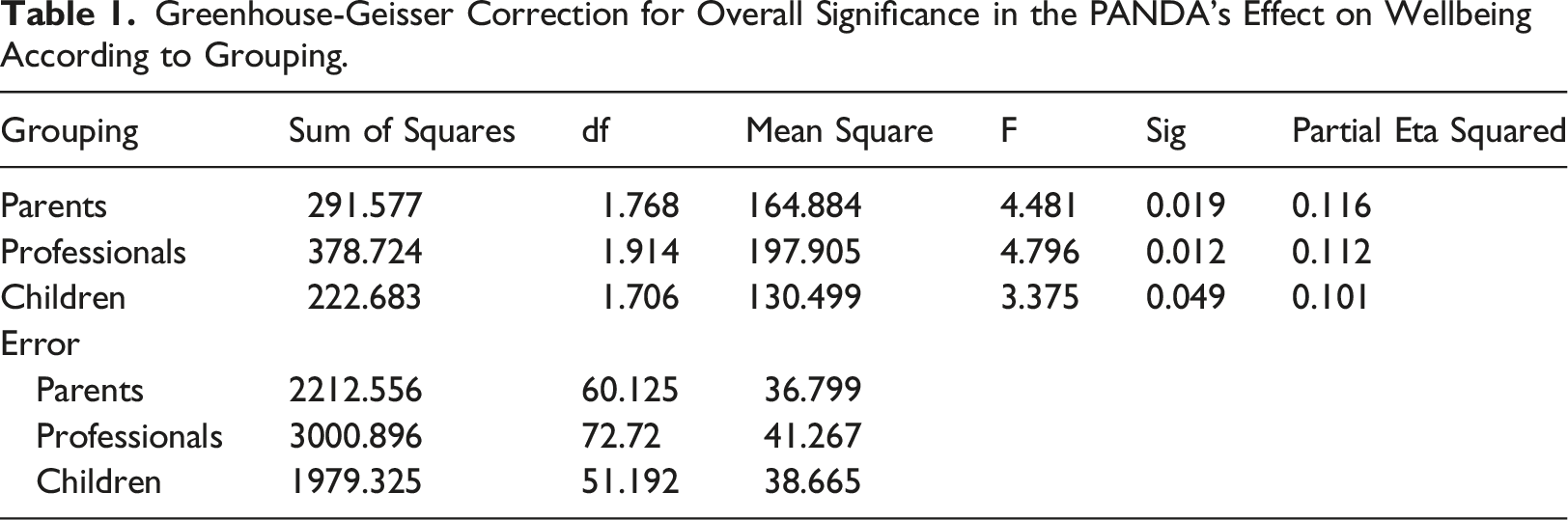
Greenhouse-Geisser Correction for Overall Significance in the PANDA’s Effect on Wellbeing According to Grouping.
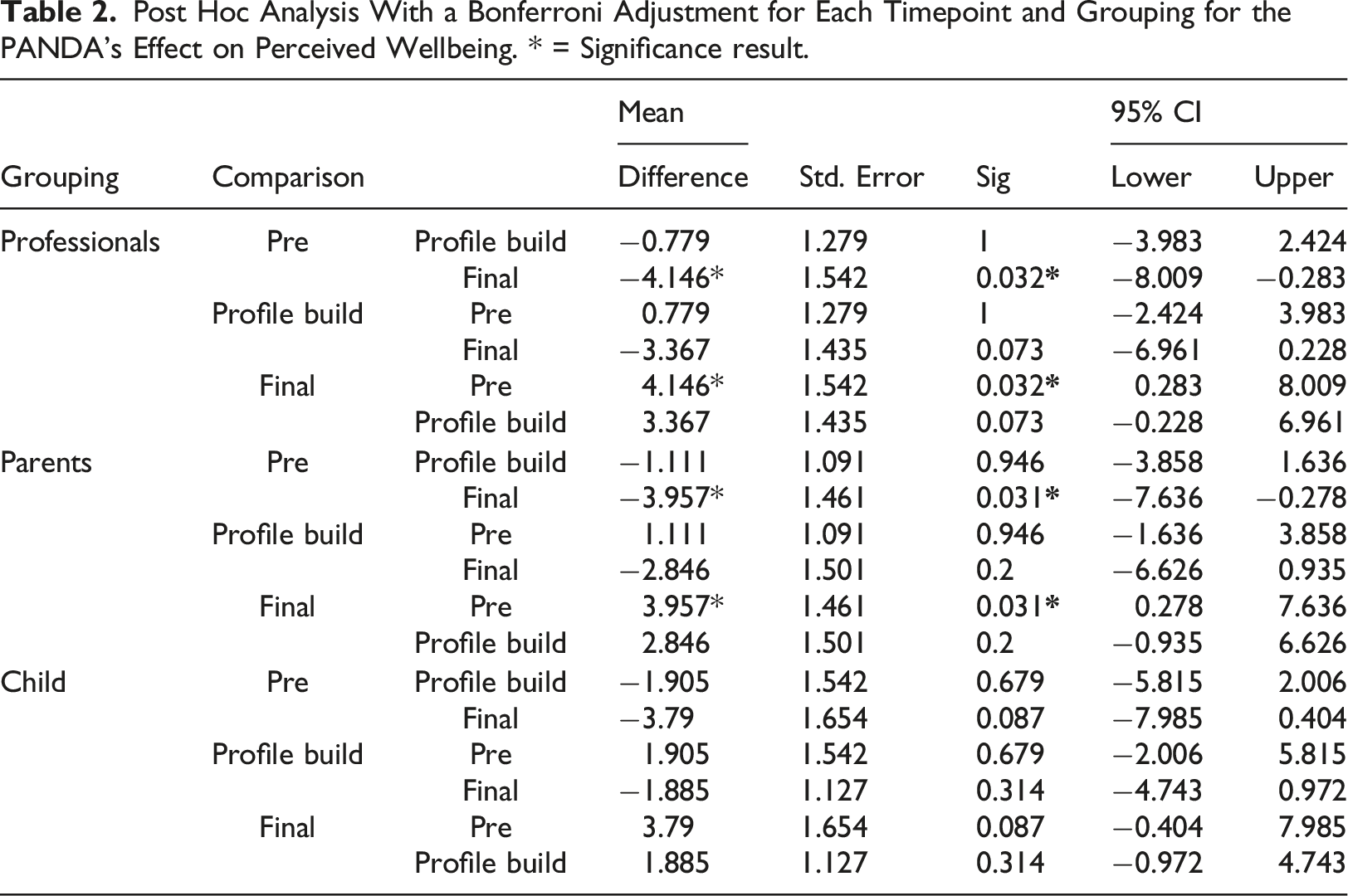
Post Hoc Analysis With a Bonferroni Adjustment for Each Timepoint and Grouping for the PANDA’s Effect on Perceived Wellbeing. * = Significance result.
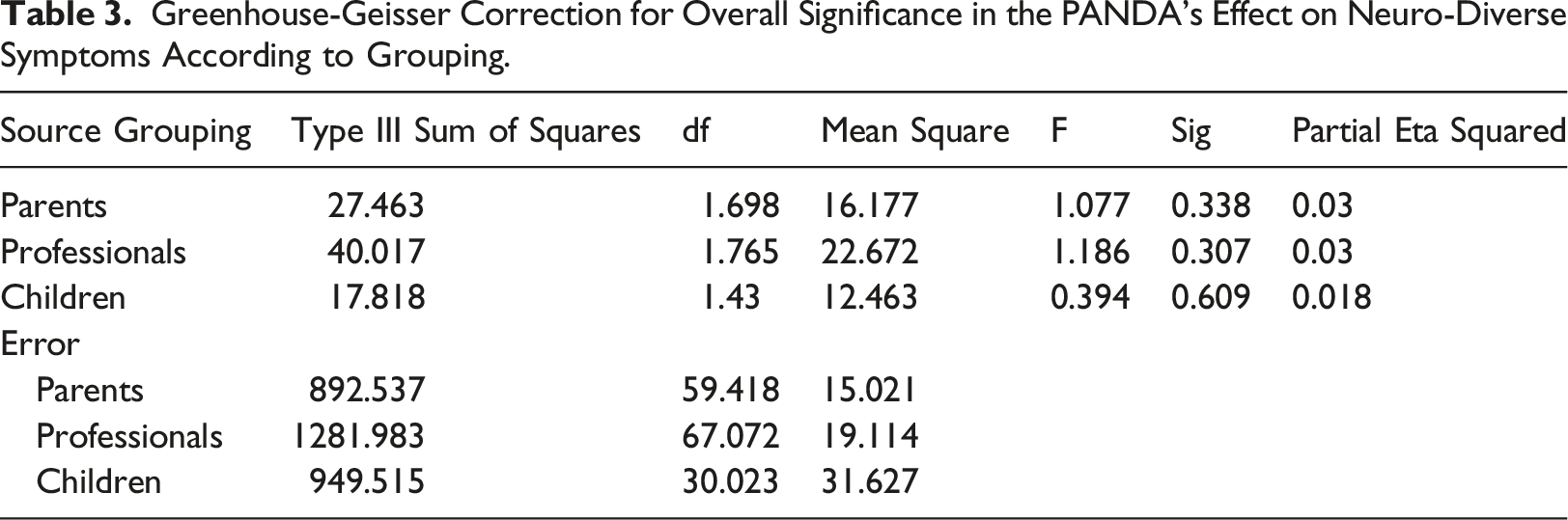
Greenhouse-Geisser Correction for Overall Significance in the PANDA’s Effect on Neuro-Diverse Symptoms According to Grouping.
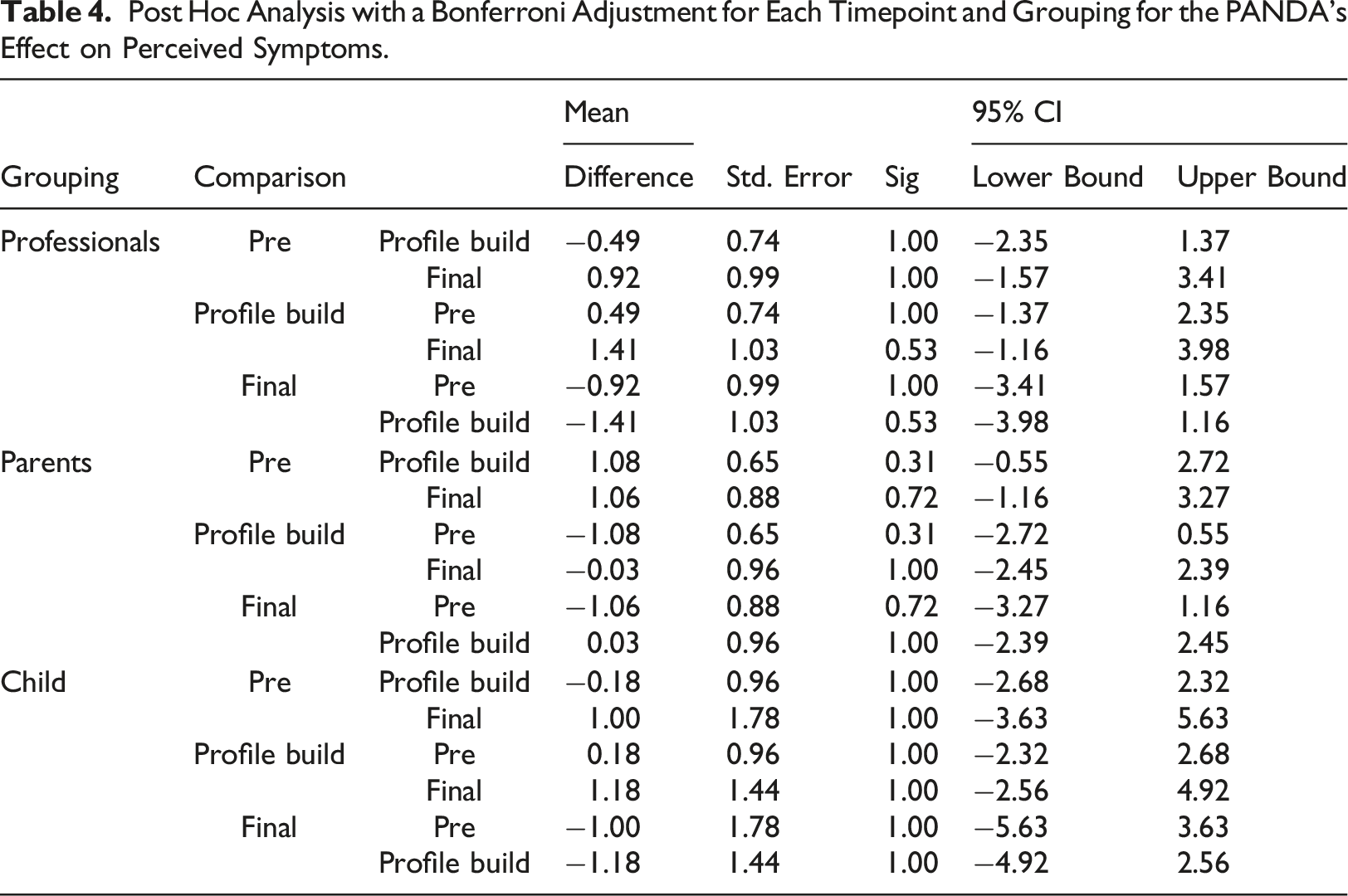
Post Hoc Analysis with a Bonferroni Adjustment for Each Timepoint and Grouping for the PANDA’s Effect on Perceived Symptoms.
Qualitative Results
Four major themes emerged from the data.
Theme 1: Supporting the System
All participants discussed how the PANDA supported the educational, familial, and personal system.
Increase in Child’s Wellbeing
These were specific changes that either the child, the parent or the professional observed since starting the project. Comments were made on improvement of physical health, with one child mentioning that they have lost some excess “body weight” due to “boxing”, and another child noting that they “don’t argue anymore really” with their parent. Parents also noticed a positive shift in the child’s behaviour, one claiming their child has “been coming home with more stickers” from school.
Empowerment
A key subtheme in empowerment was the concept of feeling listened to. As one teacher mentioned regarding an interaction with a parent -
The children also echoed this experience; one teacher believed that a child feels “More listened to and more like somebody’s tried to understand him now.” The children expressed their experience of feeling listened to during this approach and expressed the importance of “every child need[ing] to be in the meeting so they know what’s going on”. This sense of listening also facilitated the empowerment for professionals and families to take control of the support put in place. As one teacher noted - “I think that they went away and made positive changes at home as well and it wasn’t just what we were doing in school to support their child, but they went home and really thought about what they were doing in their household.”
Useful Materials
The approach’s materials were spoken about frequently. Specifically, two children were able to mention the ease of descriptors this approach had; one described it as “Like a graph to kind of see like what’s actually happening … you could actually see how high or low it is.” Another said, “a lot easier and you can just see [what you] need more help in” Parents also commented on its ease of use, and “thought it was a really nice tool to use. Very easy, it was nice having it all on one page.” and though despite it “take[ing] time … a useful way to spend your time.”.
Theme 2: Psychoeducation
Another theme generated was the usefulness of psychoeducation.
Medical Indoctrination
One persistent sub-theme in psychoeducation was the issue around Medical Indoctrination, and the importance that labels have in society. Many teachers were able to reveal the importance that labels have to families, even after completing the project- “Some of our parents … still feel that they want a label, and they are still asking for a referral to CAMHS and an ND assessment. Parents don’t seem to understand it and I don’t know if it’s because I’m not explaining it properly because I think it’s great”
This discussion around labels and their importance allowed reflections of the professionals’ experience after labels are received, that many “parents will come back to [the professional] and say, “well all they did was give me a diagnosis”. But further added that “This is why you need to engage in this [PANDA] process … it’s a piece of work and you’ll have an action plan that will help you help your child.”. Interestingly, parents rational for wanting a label was due to it facilitating “some extra support … because it could potentially be that [my child] may struggle in mainstream with his behaviours and may need some more support as time goes on.”
Clarifying Misunderstanding
Many parents and professionals were able to reflect how their assumptions of the child’s behaviour were challenged with this approach. Two examples were present from teachers when commenting on explaining the profile to co-workers were - “[Co-Workers] suddenly go “oh I didn’t realise that” and they try some of these strategies and they go “oh that’s brilliant that works really well”. “When I pulled it together into a report, staff have read it and said - “oh so that explains why such and such” and “okay this is what we can do about it”.
One parent mentioned “nightmares and sleeping habits” their child revealed and how this approach allowed them “to identify that this was a problem (and) a challenge for him. Which again I – I perhaps hadn’t thought about but again it’s linked to neurodiversity”.
Positive Environmental Changes
Positive environmental changes were made to support the young people both at home and school because of project participation. One parent commented on how the PANDA helped her to reframe her perspective on her child’s behaviours: “It’s made me stop and think and perhaps with some behaviours not being on it as much from a like a discipline perspective and trying to like understand why”. Teachers in the project also began to change their approach and build a more neurodiversity-supportive classroom: “the more you do something like this the more change will happen” as things become more routine. These positive environmental changes are corroborated by one SENCO who said, “it wasn’t just what we were doing in school to support their child but [parents] went home and really thought about what they were doing in their household”. The positive environment was also felt by the young people, especially “less arguments”: “instead of like, for example, I do something and then like and then [mum] get annoyed at me for it she’ll kind of like talk to me first”.
Theme 3: Comparison to Traditional Pathway
Significant comparisons were made between this approach and the traditional NHS neurodevelopmental pathway at Portsmouth CAMHS, mainly from parents and teachers.
Person Focused Approach
There was significant number of participants comparing the PANDA to assessment and labelling. Some teachers described “the parents were looking at what the child’s actual issues are as opposed to just giving them a label and saying they could have all these things, so I think it’s brilliant” and identifying that the PANDA is “massively looking at the child’s strengths as well”. The approach was often described as holistic, for example “doing it this way … in a more holistic way will give them more support because actually they can focus on the thing that is the issue and we can help them with resources to support that area.”. Also, from a SENCO’s point of view: “it’s quite a nice tool to … looking holistically as an overview of a child”.
Shared Perspective
Perspective sharing through collaboration was a key goal of the approach and improved understanding for all participant groups. From a SENCO’s perspective, “by working with the parents it shows you what we’re doing in school. That was an eye opener for parents to realise what we’re doing, but also the staff to hear what children are like at home”. This is also evident from a parental perspective, one parent “found it very interesting because [school] have put in place specific strategies” to support their child. From a young person’s perspective, being a part of the meetings meant parents and teachers “learnt a bit more about like my personal life and things that I keep to myself”.
Theme 4: Resistance to Change
Parental and teacher resistance to change was one negative aspect of the PANDA which was mainly discussed by professionals. This was particularly present in implementing the PANDA care plan, and it easily being set aside as not an essential part of a child’s care or within the system’s ability to carry out. Many professionals agreed in the focus group that “you’re asking the teachers to make a change they can be a bit resistant.” This resistance was also reflected regarding the attitudes of some of the parents. SENCO’s discussed that “the biggest thing with parents though is I know they haven’t read the information” which meant resources were not implemented at home. Some children also commented on things being “kind of the same” at school and mentioned how they “don’t think” there has been a significant change in teachers’ behaviours.
Discussion
Results from a mix methodology provided positive quantitative data and significant strong medium effect size on wellbeing from the PANDA. The analysis indicates that the PANDA improves the wellbeing of the child from the perspective of the professional, parent and the child. However, there is not enough evidence in this paper to suggest the PANDA has any positive effect on the symptom management of the child. Even so, this study provided a foundation for an evidence based holistic approach for neurodiversity, and information on how the PANDA can be improved for a future version. The study’s data suggests that the core idea of the PANDA providing a holistic framework for the system to engage with is a good starting point. Especially since it builds upon previous research on similar factors having a positive effect on wellbeing in neurodiverse populations (Zhou et al., 2019). However, it is difficult to decipher which part of the PANDA facilitated this effect. This paper can make some suggestions on why wellbeing improved when interpreting the identified themes.
Firstly, the material about neurodiversity tailored for non-professionals allowed for a structured discussion and perspective sharing between parents, educators and the children. This discussion has been viewed as vital for relationship building between the systems, as participants in the study have mentioned how they have felt listened to and understood for the first time. This perspective sharing and listening to each side has been deemed in previous research as a high priority for the neurodiverse community (Clark & Adams, 2020), as it helps fight against the stigmatisation and negative stereotypes that are held by individuals in society.
Secondly, the psychoeducational material enabled better understanding within the system, which will increase empathy towards the child, and decrease stigmatisation. Again, between all groups, each mentioned how due to taking part in the PANDA, they have learnt something new about the child, and have therefore changed their own behaviour to better support the child’s needs. Mirroring previous research, the study supports those increasing problem-solving skills related to the behaviour and supporting them instead of negatively reacting to the behaviour (DaWalt et al., 2018) and reframing will reduce the amount of time individuals remain in a state of confusion waiting for answers (Connolly & Gersch, 2013; Crane et al., 2016).
Thirdly, the PANDA enables a person focused approach, including systemic changes. Participants reflections mentioned how they learnt something new about the child, which also included the child’s interests and what works between the home and school environment. Parties were able to share their experiences and how to best use the child’s strengths to support their weaknesses, mirroring past studies (Cascio et al., 2020; McConkey et al., 2020).
It would be insightful for future research to investigate the content of the profile building discussions, and care plan implementation as it would provide vital insights into the PANDA’S strengths, and future development. Finally, this paper wishes to highlight an interesting pattern within the symptom management data despite its statistical insignificance. The child SDQ scores were between the parents’ and professionals’ scores throughout each of the three meetings, specifically the teacher having a negative bias and parents having a positive bias when compared to the child. However, when examining the pattern between the first and second meeting, the scores of the professionals and parents converged together, closer to the child’s perspective. Even though this convergence was non-significant, it reflects some of the qualitative data of parents and professionals learning something new about the child. Again, this is only a descriptive set of observations, but future research could take extra measurements to examine the perspectives of each member to identify if this occurs again.
Limitations
With the methodology of the study itself, it can be perceived that this pilot has significant limitations. Especially when identifying the age range, the exclusion and inclusion criteria and wide range of symptoms which would be included for the project. Future studies could investigate the PANDA’s effectiveness when controlling for age, gender, symptoms, education.
Conclusions
Overall, the data suggest that PANDA can be an effective approach to improve the perceived wellbeing of the child from the professional, parental and individual’s perspective. This is likely to be due to the holistic discussion and accessibility of the material. It is possible for it to serve as an initial assessment and intervention in a stepped-care model by providing information and guiding participants in need of a more individualized treatment. The accomplishment of the approach’s effect on wellbeing would not have been as successful without the co-produced model when being created. More research is required to gain specific information on the strengths and limitations of the PANDA, especially when it comes to the observable impact on the behaviour, coping mechanisms and problem-solving skills in everyday life.
Footnotes
Acknowledgements
Line Manager - Nigel Sampson. Thank you for assisting in my integration into Solent NHS Trust, and your continuing support for further training and respect you show to me on a regular basis. You have truly been one of the most supportive managers I have had in my career who always fought for my personal development. Clinical Supervisor – Dr Kate Benham. Thank you for taking time out of your busy work schedule to support my own professional development. The opportunities you have provided have been incredibly vital to reflect on my position in society, with my clients and how I conduct my own therapeutic practice. Though you were not officially part of this project, I still wish to acknowledge your influence on me. Due to your mentoring, I witness a shift in how I think about evidence based psychological practices and the public system at large. This did not just inform this research but also the project may be implemented in the system. Psychology Placement Student – Isobel Horsfall Turner. Though your name is already on the paper, I still wish to take the time to thank you for all the hard work you have completed for this project. It can’t be underestimated how important your position was, with data collection, transcribing and report editing. I am not only keeping my promise to have your name on the paper, but I am also incredibly proud to have my name next to yours. I witnessed an incredible amount of growth in your research and therapeutic skills during project, and I am sure that whatever you decide you want your career to be, you have the skills and intelligence to take you there. Portsmouth Parent Voice - Elise Meyer. Portsmouth Parent Voice has been a vital ally in educating and advocating for neurodevelopmental conditions and the parental/carer experience with the NHS system. I hope to see their charity grow and continue to advocate for parents’ voices in the future. Elise Meyer has continuously been a grounding colleague for this project, displaying the importance of co-production within the NHS. She has taught me so much about the importance of service user experience, and to always keep them in mind. I only hope to continue with this nugget of knowledge as I continue to grow in my career. Dynamite - Joe McLeish and Carly Blake. Dynamite provides an excellent perspective of neuron-diverse individuals and suggesting changes to the system at large. I wish to see their charity grow and continue to inform how professionals and parent/carers continue to work with neuro-diverse individuals. Special thanks to Joe McLeish and Carly Blake, for providing weekly updates with a wide variety of perspectives, and their own insight on their experience with Portsmouth Institutions. Jonathan Prosser. Now Chief Clinical Information Officer pushed for a neurodiverse approach within Portsmouth CAMHS and who continues to advocate for more inclusive and thought-provoking ideas within the Trust. Dr Colin Barnes Clinical Effectiveness and Improvement Manager of Solent NHS trust, who mentored and supervised the author of this paper through the methodology creation and ethical application. I have personally learnt a lot from your research mentoring and will continue to use this knowledge in my future career. Liz Robinson Principle Educational Psychologist, who helped facilitate the educational community’s involvement with the project. Without your leadership and activism, the engagement with the approach would not have achieve such a high level of success as it did.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The feasibility of the Neuro-Diversity Approach was evaluated as an open within-group trial as a potential step pre-referral to Portsmouth’s Child and Adolescent Mental Health Service (CAMHS). Participants provided written consent, or consent via parents, and the study was approved by the UK’S National Health Service’s (NHS) Research Ethics Committee (IRAS-287858).