
Abstract
The study explores the role of the Eye to I© intervention model in facilitating advancement through social stages of play in which skills contribute to the quality of social interaction and communication in children with autism. Data were collected on 11 participants, ages of 2–6 years, formally diagnosed with autism, receiving Eye to I© Social Communication therapy at Potentials Therapy Center, New Delhi, India. Eye to I© is developed in-house at Potentials and is further discussed in the paper. All participants attended a form of group intervention. A mixed-method design included quantitative measures administered pre and post intervention (Communication DEALL Developmental Checklist, Communication Matrix) and video coding of Social Communication sessions. Qualitative measures were semi-structured parent interviews conducted at the end of intervention. Thematic analysis and quantitative statistical analysis results show that by the end of the Eye to I© intervention period children engaged in social stages of play of greater developmental complexity and showed increased scores in assessments of social skills as well as generalization of skills. This suggests that skill acquisition necessary to directly support two diagnostic criteria areas of autism as per DSM-V; i.e., communication and social interaction occurred during the period of intervention.
Introduction
Autism Spectrum Disorder (henceforth referred to as ‘autism’) is a complex neurological condition that emerges early in childhood and is characterized by impaired social communication and interaction, restricted interests, and increased repetitive behaviors (American Psychiatric Association, 2013). Impairments in social interaction are marked by nonverbal behaviors such as reduced shared eye gaze, distinct body posture, limited variation in facial expressions, and restricted social and emotional reciprocity (Whitman, 2004). In neurotypical development, socio-emotional skills naturally emerge supporting attachment between the developing child and others which facilitate exploration and engagement with physical and social environments (Yates et al., 2008). This attachment and exploration are directly linked to success in adult competence to form meaningful social relations, self-regulation, managing emotions, and academic achievement (Denham, 2006; Myers et al., 2006; Thompson & Lagattuta, 2006). Autistic children, however, struggle to intercept and respond to social cues thereby limiting attachment formation, subsequent exploration and hampering chances of building meaningful social relations in childhood and beyond (Golan et al., 2010; Magiati et al., 2014; Rai et al., 2018). Therapeutic interventions which address attachment and exploration skills early in development are effective and have long term impact (Gibson et al., 2021; Martínez-Pedraza and Carter, 2009; Nyeste, 2010).
In India the need for early intervention is clear. Recent data shows that 1 in 100 children under the age of 10 have autism, and nearly 1 in 8 have at least one neurodevelopmental condition that affects learning and communicating (Arora et al., 2018; Singh et al., 2019). Furthermore, diagnosis of autism often occurs at age four even though signs of autism can be detected between one to 3 years of age (Manohar et al., 2019) - indicating a need for interventions that address and identify skill deficits in early child developmental stages.
Social communication & play in ASD
Social communication is communication intended for the purpose of reciprocal exchange of information and forming relations involving speech, gestures, sounds, facial expressions, gaze, tone of voice, and body language (Kossyvaki, 2017; Mehta, 1987). Though autistic persons exhibit heterogeneous characteristics and challenges (APA, 2013) almost all experience difficulty in aspects of social communication such as social-emotional reciprocity (Bauminger & Kasari, 2000), responding to joint attention, and initiation of communication (Chawarska et al., 2016; Franchini et al., 2018, Prizant & Fields-Meyer, (2001). Further, Schumann et al. (2009) hypothesized the ‘interactional instinct’, an innate tendency of the child to take initiative to form attachment and social affiliation - behaviors that contribute to social communication (Schumann et al., 2009). It is proposed that skills emerging from the interactional instinct promote affiliation and attachment include directed eye gaze, joint attention, facial expressions, pre-linguistic vocal perception (such as pitch and rhythm), and neurobiological processes of mirror neural networks. Significantly, these same skills and processes are underdeveloped in children with autism (Baron-Cohen et al., 1996; Yates and Hobson, 2020).
Play: a social communication tool
Play is the primary context in which children build emergent social-communicative skills and establish social competencies (Mathieson & Banerjee, 2010). It is a multifaceted, social construct (Eberle, 2014) represented by object play, symbolic play (Orr & Geva, 2015), games with rules (Piaget, 1952), and more (Marsh et al., 2016). Hughes (2003) defines three essential characteristics present in all forms of play: freedom of choice, personal enjoyment, and a focus on the activity itself rather than its outcomes. However, when play is perceived as a discrete set of skills with precisely operationalized scripts and training sequences instead, the very essence of play and its powerful effects on overall learning and development are threatened (Wolfberg & Schuler, 2006). Specifically, this can occur when that discrete goal might fail to match up with the developmental skill level of the player. Thus, it is imperative to recognize the essence of play as a developmental process in which the play itself becomes a medium through which children develop multiple skills of social competency (Craig-Unkefer & Kaiser, 2002; Gray, 2011; Zigler and Bishop-Josef, 2009).
Social stages of play
Play is fundamental to social-emotional and cognitive development, learning, and social skills (Siraj-Blatchford, 2009). Historically, Parten (1932) divides play into six fundamental social stages of increasing complexity: onlooker, solitary, parallel, associative, cooperative. This work remains a basic guide to skill progression in stages of early childhood development (Lee et al., 2022). Critics of Parten state that associative and cooperative stages are difficult to parse and that play itself may vary culture to culture (Drew, 2022). However, when these social stages of play are defined by the use of skills to engage within a child’s cultural context - then the cultural differences of play manifest in interpretation of the skills in context and not the ability to use the skill itself. For example, the timing and duration of directed eye gaze may vary depending on cultural context, but the use of directed gaze as a tool for interaction can be seen as a skill of joint attention and social cognition (Stephenson, et al., 2021). Thus, Parten’s social stages of play provide a scaffolding for the development of social interaction skills in early childhood.
In neurotypical development these social stages unfold from infancy to age five. A typically developing child might exhibit play skills enabling associative play at age four and skills of cooperative play 1 year later at 5. However, as documented above, the acquisition of skills and social competencies (such as joint attention and social reciprocity) that characterize parallel, associative and cooperative play stages are frequently delayed in autistic children. Early intervention models that target joint attention skills and social competencies show that autistic children participate in more socially and cognitively complex play (such as symbolic pretend play with peers) within a 6-month intervention period (Chang et al., 2018; DiStefano et al., 2016; Goods et al., 2013). Thus, early intervention that specifically addresses and facilitates skills represented in stages of play holds measurable value. Given the current limits of research and services in South Asia, it becomes critical to explore the impact of therapeutic early interventions with strategies for play skills and measurements of play stages in the Indian context (Arora et al., 2018; Singh et al., 2019, Gokhale, 2021).
Present study
The present study explores the role of the Eye to I© Intervention model in development of skills that facilitate communication and social interaction in autistic children. Eye to I© is an intervention model that uses play as a medium and incorporates an array of therapeutic modes (social communication sessions, special education, occupational therapy and oromotor articulation therapy) to target social, emotional, and cognitive development across developmental domains (Kharbanda & Gupta, 2015). Intervention is delivered by trained professionals in 2:1 or 1:1 therapist-child ratio settings. A minimum of two therapists are involved with each child. Therapeutic content and progress is guided by individual needs, and includes parent training. A codebook is used as a quantitative tool to evaluate gradations of social play stages by measuring verbal and non-verbal skills like gaze direction, body orientation, and reciprocal interaction. Qualitative data also suggests that these skills can contribute towards increased purposes of communication. Further representation of qualitative data is shared in Figure 13 in this paper’s results section.
The rationale behind the Eye to I© codebook is to establish a correlation between the acquisition of interaction skills inherent in play and increased skills in other developmental domains. We aim to validate the accuracy of the coding by demonstrating correlation with overall social developmental progress as measured by two standardized tools: CDDC and Communication Matrix.
Objectives
1. This paper aims to explore the correlation between Eye to I© intervention, increases in play skills, and increases in other areas of development. 2. Specifically, this paper aims to demonstrate the efficacy of Eye to I© intervention in fostering increases in complexity of the social stages of play during engagement with a therapeutic play partner wherein complexity and engagement in play are aligned with development of social interaction and communication skills.
Method
Participants
Although initial baseline measures (CDDC, Communication Matrix questionnaire and first video recording) were collected from 29 participants, various factors prevented all participants from maintaining session frequency within the intervention period resulting in a final sample size of 11 participants (N = 11). All participants were recruited from Potentials Therapy Center, New Delhi, India and received Eye to I© therapy. There was no control or comparison group for this initial study. The sample consisted of more males than females (Table 1). Participants were between 36 months and 66 months with most participants between 48 and 54 months (Table 2). The inclusion criteria were as follows: 1. A formal diagnosis of autism by a recognized diagnostic organization or a private practitioner in Delhi, NCR. Diagnoses relied on an array of diagnostic tools such as M-CHAT, CARS, and Social Communication checklists, with primary use of ISAA (Indian Scale for Assessment of Autism) by the National Trust of India. At the time of data collection, 10 participants had a formal ASD diagnosis and 1 was diagnosed with social communication ‘deficits’. Follow up communication post-intervention confirmed a later diagnosis of autism. 2. Attended individual Social Communication therapy sessions (SCS) with trained Eye to I© therapists at Potentials Therapy Center on average two or more times, with a minimum of once-a-week attendance due to occasional absence for personal reasons. None of the participants had 100% consistency in frequency of attendance due to the length of the intervention period. However, all participants completed the 61 sessions in the range of 5–7 months. No previous Social Communication therapy. 3. Attended peer group therapy (2 or more children) or classroom settings: a. Social Communication group therapy at Potentials, or b. Special Education, Speech or Occupational group therapy, or c. Group class setting with consistent intensity and frequency for duration of intervention. Sample demographics: gender. Sample demographics: age.

The tables below represent the age and gender distributions of the study’s sample.
Procedure
First, baseline scores were established with the CDDC scale, taken from the caregiver. Subsequently, the participant attended three to five sessions ensuring: a. familiarity with the physical space b. therapist - child rapport
Then, baseline scores were established with the Communication Matrix scale, administered by the therapist of the participant. Further, participants attended Social Communication therapy two to three times per week, however, due to the lengthy intervention period, concerns emerged regarding natural inconsistencies in attendance. Hence, the intervention period was measured as completion of 61 sessions. Although this resulted in some variability in the frequency of sessions, the overall quantity of therapy was consistent and the intervention time period was approximately 5–7 months for each participant. Further, temporal frequency of sessions depends on the baseline skills of the child where some require two sessions, others three sessions or more per week. Video was recorded after every 10th session resulting in six videos - sessions 1, 11, 21, 31, 41, 51, and 61. All therapy sessions were 45 minutes. After six videos the Eye to I© Codebook was used to analyze each video. Coders were qualified psychologists who were trained by reviewing theoretical underpinnings of play and observing multiple examples of behaviors from each code and subcode. Thereafter coding was practiced on sample videos (not part of this study). Training was considered complete when five sample videos were coded with a minimum of 80% matching codes as a trained social communication Eye to I therapist. After 61 sessions parents filled the CDDC again, and therapists repeated the Communication Matrix. After data collection, a semi-structured interview with open-ended questions elicited parent response regarding quality of interaction, changes in their child’s skills and behavior, and therapy at Potentials.
Measures
1. Pre and post-assessment of individual Social Communication therapy sessions Assessed using behavioral coding of periodic video recordings of the individual Social Communication therapy sessions of each participant in the sample. Six sessions were video-recorded with a gap of 10 sessions between each video recording; session 1 was the baseline assessment (pre-test assessment) and session 61 was the post-test assessment. Videos were then coded using the Eye to I© codebook. Coding was done blindly by three independent researchers, after establishing IRR (85% or more). During data analysis, emphasis was given to video 1 (session 1) and video 6 (session 61), however a progression over the course of six videos (61 sessions) was mapped for each participant showing changes in engagement in social stages of play (See Appendix E for graphical representation of individual growth across social stages; See Appendix B for Eye to I© Social Stages of Play codebook). 2. The Communication Matrix (Oregon Health & Science University, Rowland, 2012) Assessment of seven levels of Communication: Pre-Intentional Behavior, Intentional Behavior, Unconventional Communication, Conventional Communication, Concrete Symbols, Abstract Symbols, and Language. Assessment by Social Communication therapists working with respective participants. Administered pre-intervention (to establish a baseline) and again post-intervention (completion of 61 sessions). (See Appendix D) 3. Communication DEALL Developmental Checklist (henceforth referred to as ‘CDDC’) Profile of overall development across eight domains; providing indicators for intensity and types of interventions required (Karanth, 2005, 2007). The parent fills out a questionnaire in the presence of the researcher. CDDC highlights specific domains that impact social communication, such as receptive language, expressive language, cognitive skills and social and emotional skills, as well as other domains including gross motor skills, fine motor skills, and activities of daily living. Administered pre-intervention and again post-intervention (completion of 61 sessions). (See Appendix C) 4. Semi-structured parent interview (See Appendix A for semi-structured interview questionnaire). Parents interviewed post-intervention (completion of 61 sessions). Questions in two areas: a. Generalization of skills to environments and people beyond the Eye to I© therapeutic setting. b. Quality of life of participants and family including experiences sharing emotions, empathy, and connection with family members.
Research design
This study followed a mixed-method to accommodate both pre-designed quantitative measures (CDDC, Communication Matrix, Eye to I© Codebook) and qualitative measures in the form of semi-structured interviews. The purpose of this study is to explore the efficacy of Eye to I© intervention and the possible validity of the Eye to I codebook as a measurement of social interaction skills and guide to therapeutic goal planning. Due to the small sample size this study was conceived as a pilot study in which results could suggest the need for a randomized control trial with a larger sample size in the future.
Results
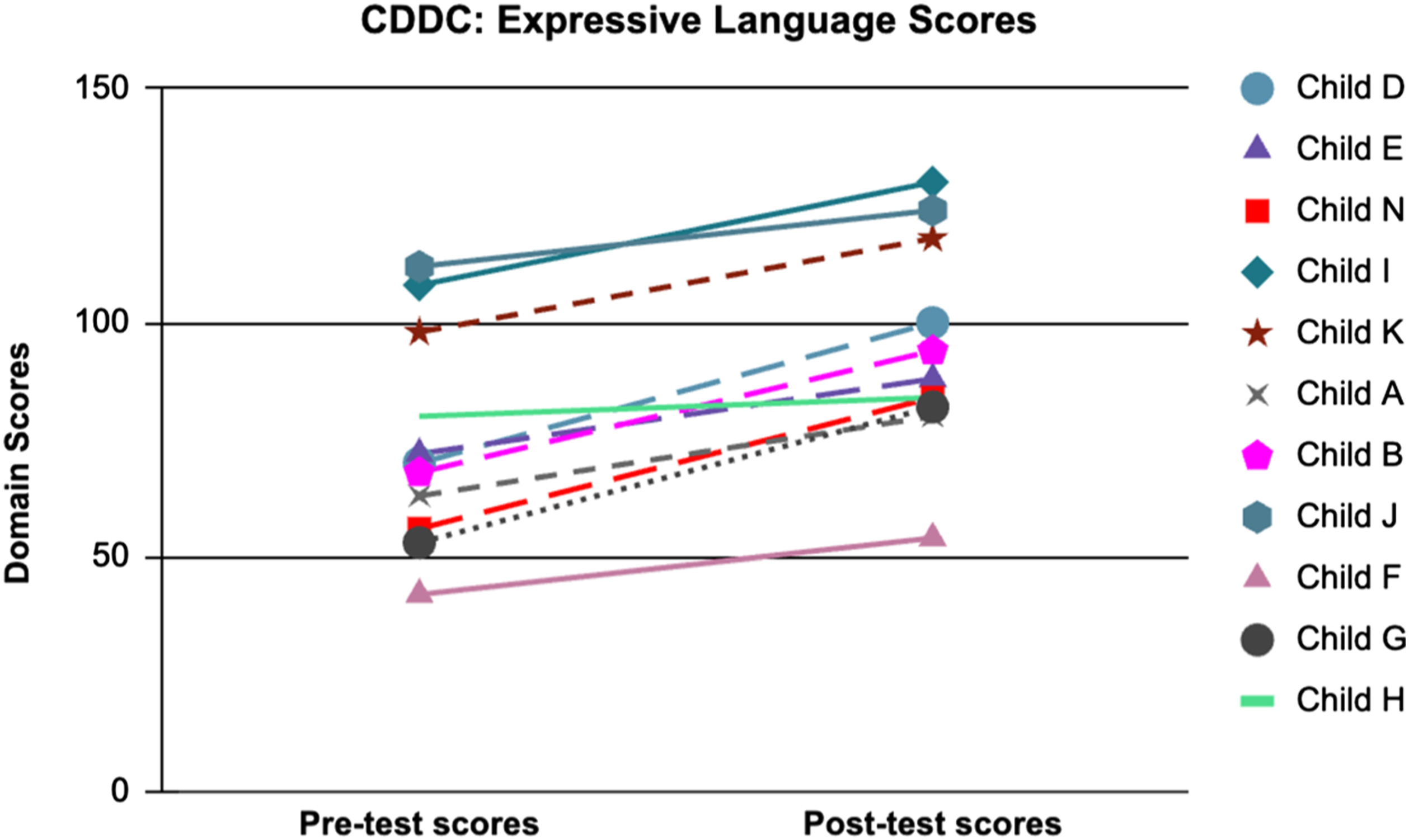
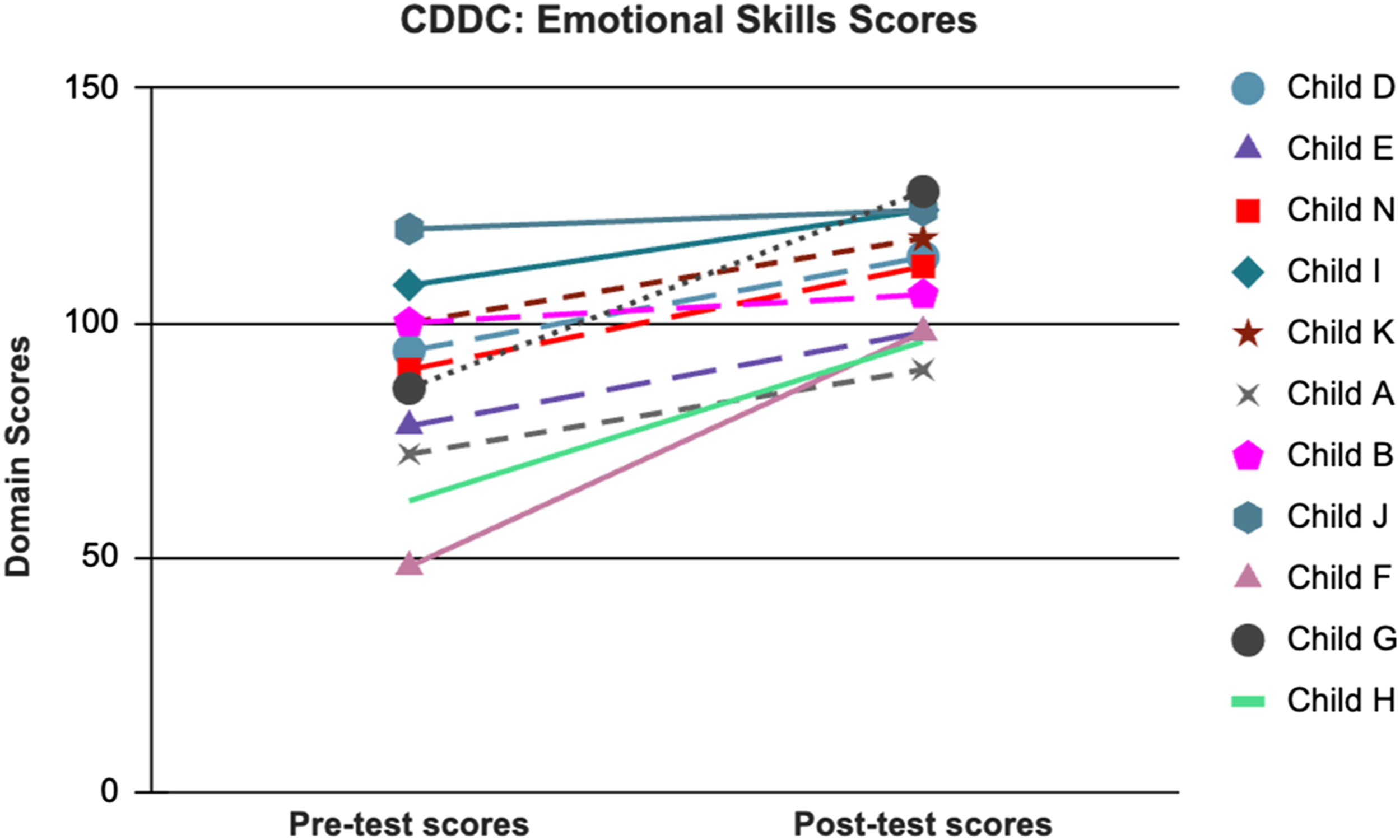
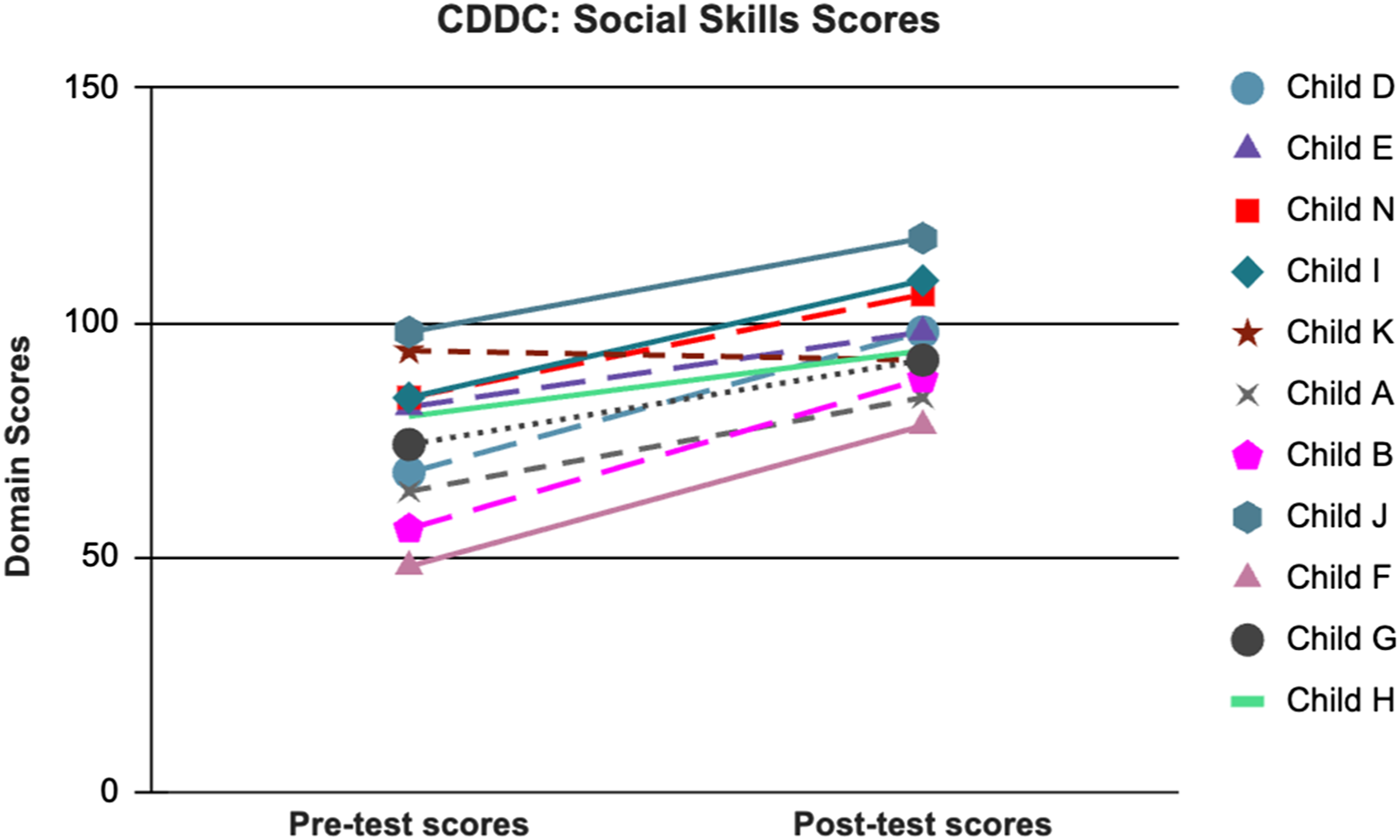
Three measures (CDDC, Communication Matrix, and the Eye to I© Codebook) were administered as a baseline pre-intervention of Eye to I© Social Communication therapy (pre-test) and upon immediate conclusion of the intervention period of 61 sessions (post-test). The raw scores taken from the Communication Matrix, CDDC, and the Eye to I© Codebook were then subjected to inferential analysis using SPSS. A non-parametric test was chosen since the sample size is small (N = 11) and normal distribution of scores cannot be assumed. All three measures, (CDDC, Communication Matrix, and the Eye to I© Codebook), follow an ‘author-developed’ coding system/rating scale and require rating of sample ‘behaviors’ from structured observations. CDDC and Communication Matrix suggest the use of the rating given as a score, addition of which gives a final score. The Communication Matrix measures communication skills in terms of intentionality of communication and the complexity of use of that communication, i.e., ‘how’. These parameters of measurement are independent of ‘age of skill acquisition’, and instead based on current skill level, where higher scores are assigned to gains in more complex skills (Rowland, 2012). Additionally, as the chronological age of autistic children cannot be assumed as a normative scale against which to measure the development of skills, ranking of the participant skills gained based on the Communication Matrix and CDDC scales was a more suitable approach. Our study aimed to track intervention effects overtime (increases in complexity of the social stages of play during engagements with a therapeutic play partner) and hence measured play engagements of the same children at multiple times (after every 10th session, over 61 sessions). Looking at these qualities of the data, Wilcoxon’s matched-pairs signed rank tests were utilized to analyze the data (Figures 1–4). CDDC Pre-test and Post-test scores of receptive language (RL) and expressive language (EL) skills. CDDC Pre-test and Post-test scores of receptive language (RL) and expressive language (EL) skills. CDDC Pre-test and Post-test scores of Emotional (EM) and Social Skills (SOC) skills. CDDC Pre-test and Post-test scores of Emotional (EM) and Social Skills (SOC) skills.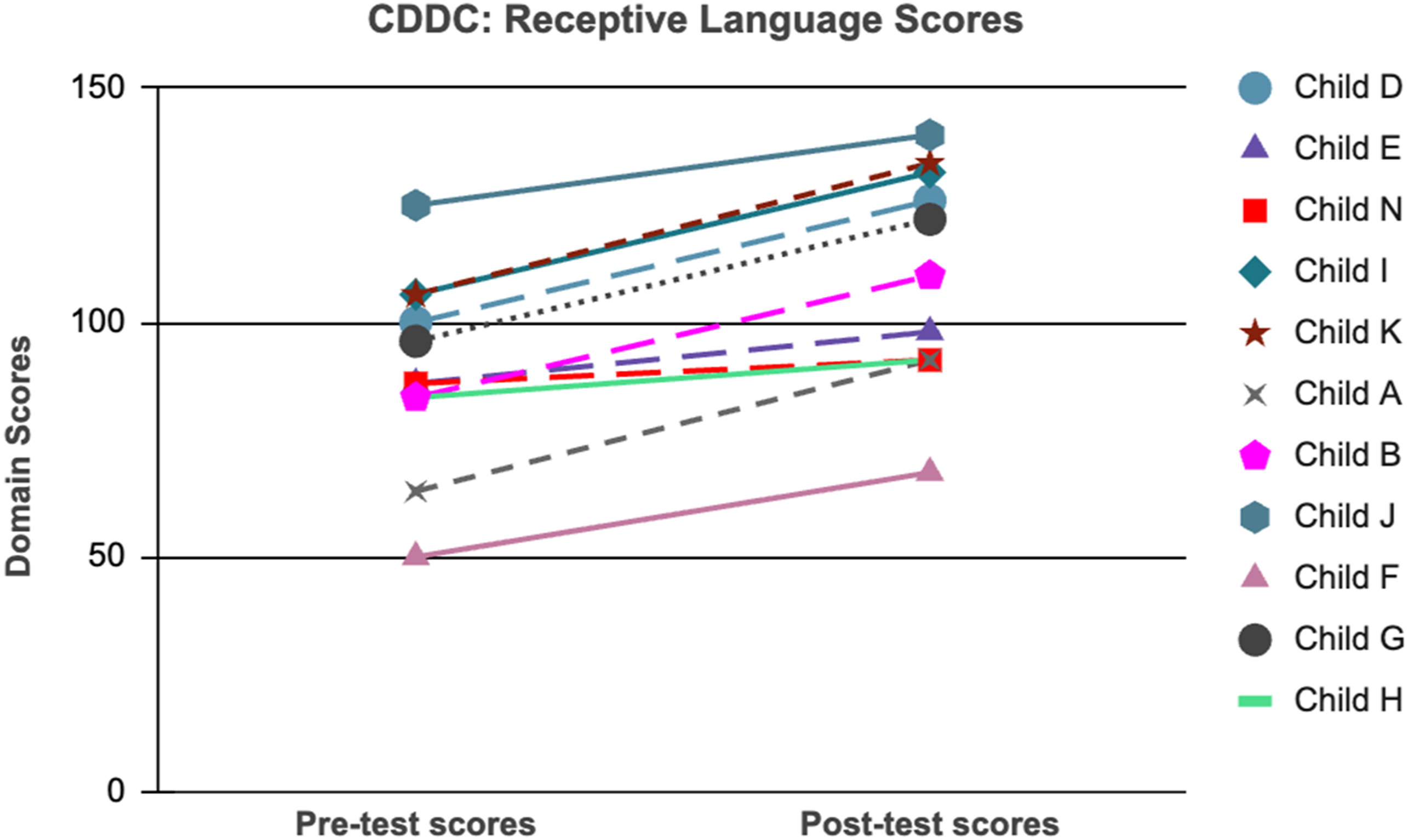
Results from Wilcoxon’s signed rank tests of pre and post-test scores from CDDC, communication matrix, and social stages from the eye to I© codebook.
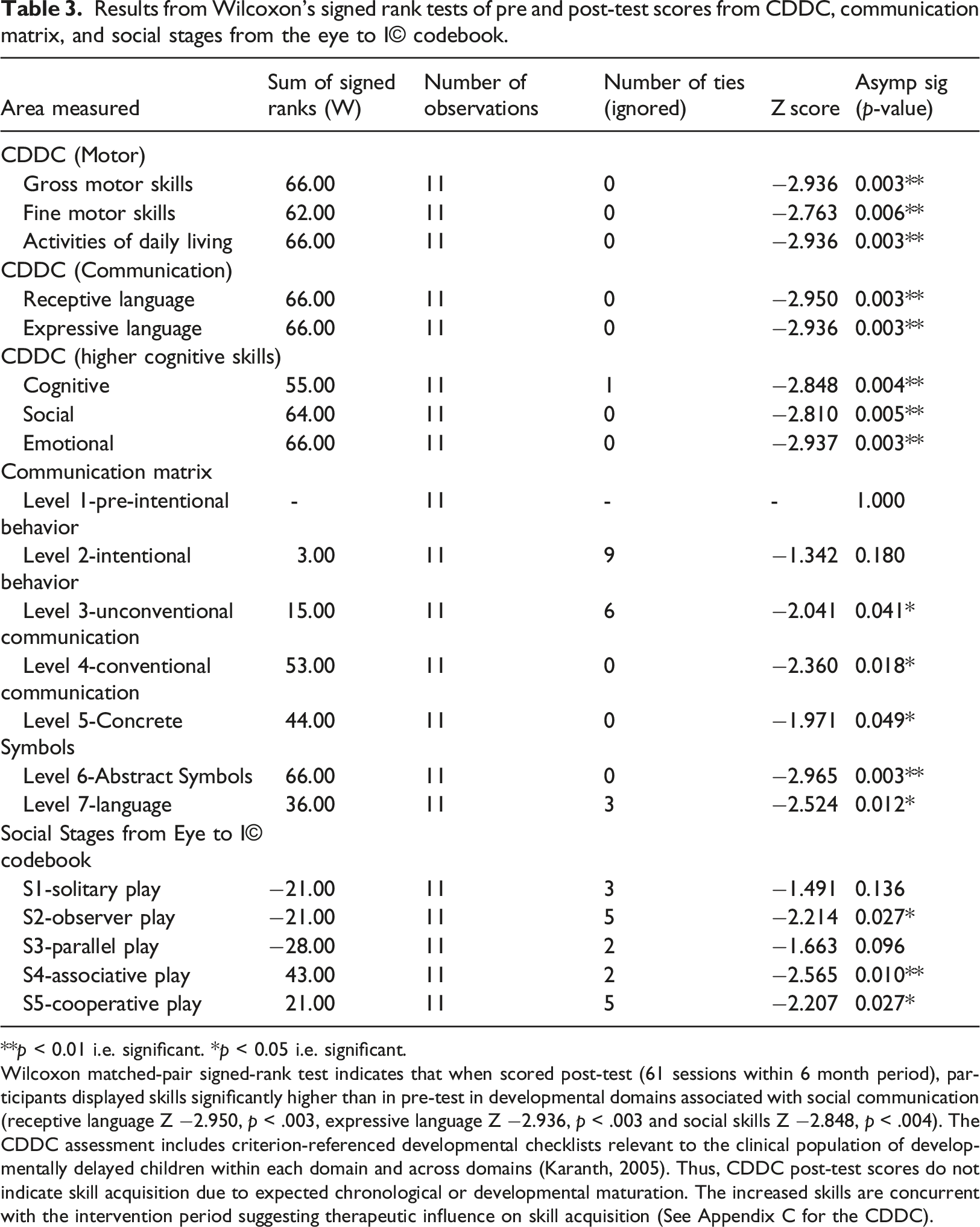
**p < 0.01 i.e. significant. *p < 0.05 i.e. significant.
Wilcoxon matched-pair signed-rank test indicates that when scored post-test (61 sessions within 6 month period), participants displayed skills significantly higher than in pre-test in developmental domains associated with social communication (receptive language Z −2.950, p < .003, expressive language Z −2.936, p < .003 and social skills Z −2.848, p < .004). The CDDC assessment includes criterion-referenced developmental checklists relevant to the clinical population of developmentally delayed children within each domain and across domains (Karanth, 2005). Thus, CDDC post-test scores do not indicate skill acquisition due to expected chronological or developmental maturation. The increased skills are concurrent with the intervention period suggesting therapeutic influence on skill acquisition (See Appendix C for the CDDC).
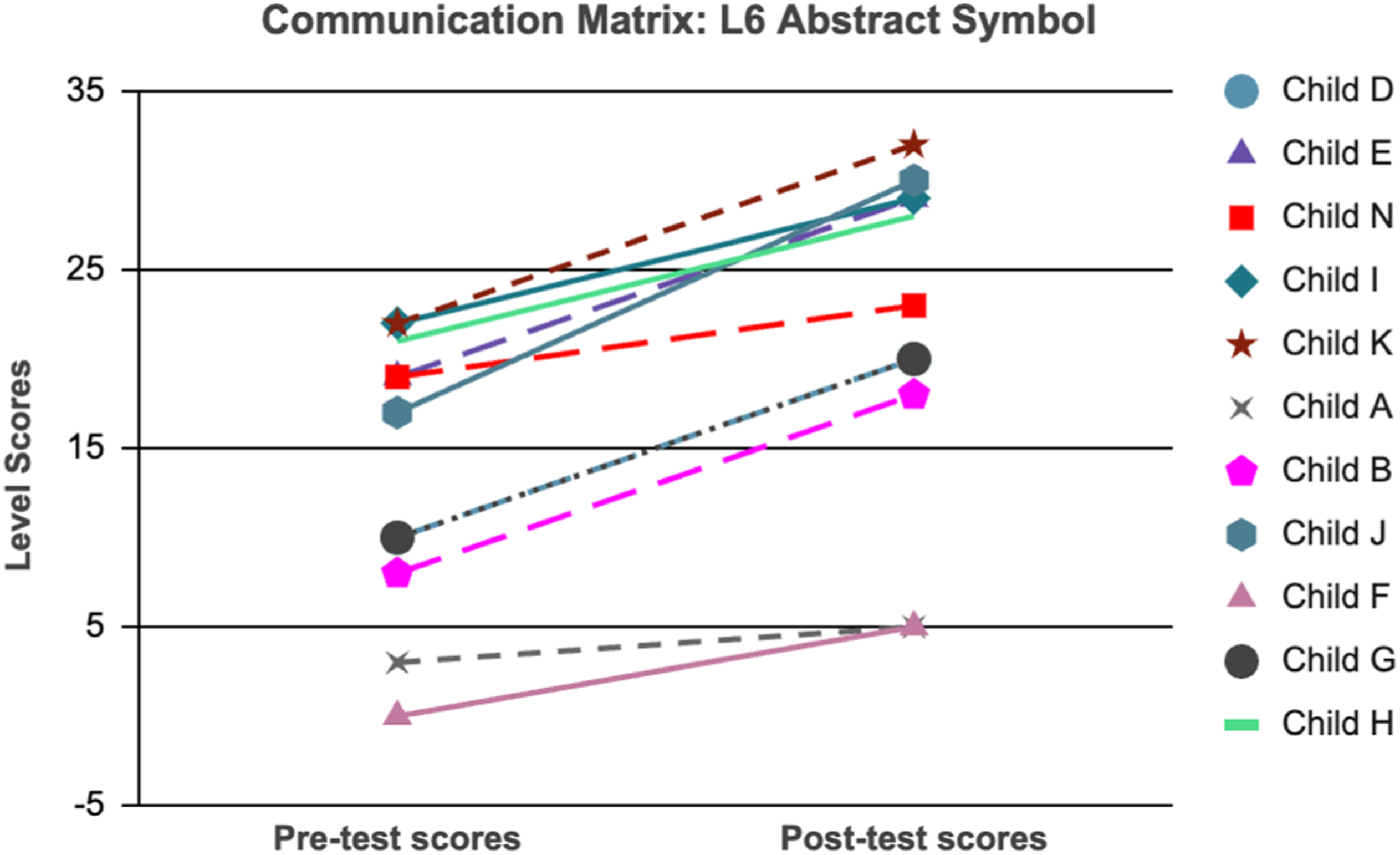
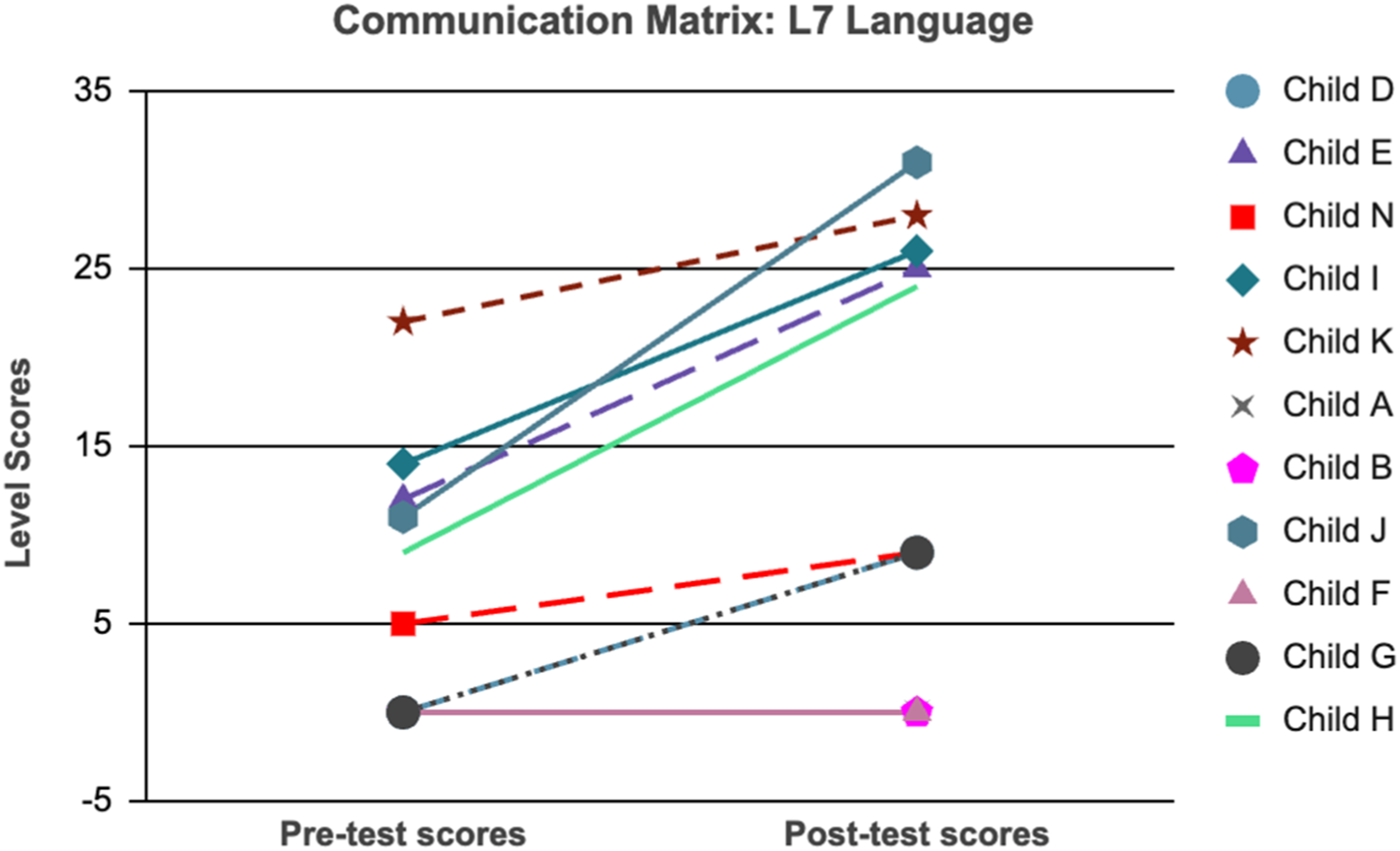
Communication Matrix scoring revealed that all participants were at maximum score (maximum skill) for the pre-intentional stage (L1) and nine out of 11 participants already had all skills of intentional stage (L2) of communication pre-test and hence showed no significant difference pre and post intervention for these two stages (Z 0, p < 1.0, Z-1.342, p < .18 respectively). At these stages, behavior is not yet used to communicate intentionally. Caregivers interpret the individual’s needs and desires from behaviors such as body movements, facial expressions, vocalizations and eye gaze (Rowland, 2013). Intentional communication behavior begins in the unconventional communication stage (L3) in which the manner of communication involves socially recognized conventions such as iconic gestures, pictures (L 4-5) and robust language (L 7). As depicted in Figures 5–7, Wilcoxon’s Sign Rank test shows post-test skills to be significantly higher in the subscales measuring higher levels of communication: Unconventional Communication (L3 Z −2.041, p < 0.041), Conventional Communication (L4 Z −2.36, p < 0.18), Abstract Symbol (L6 Z −2.965, p < 0.003), and Language (L7 Z −2.525, p < 0.12) of the Communication Matrix (Rowland, 2011; Rowland & Fried-Oken, 2010 as cited in Rowland, 2012). Communication Matrix Pre-test and Post-test scores of three levels: Conventional Communication (L4), Abstract Symbol (L6), and Language (L7). Communication Matrix Pre-test and Post-test scores of three levels: Conventional Communication (L4), Abstract Symbol (L6), and Language (L7). Communication Matrix Pre-test and Post-test scores of three levels: Conventional Communication (L4), Abstract Symbol (L6), and Language (L7).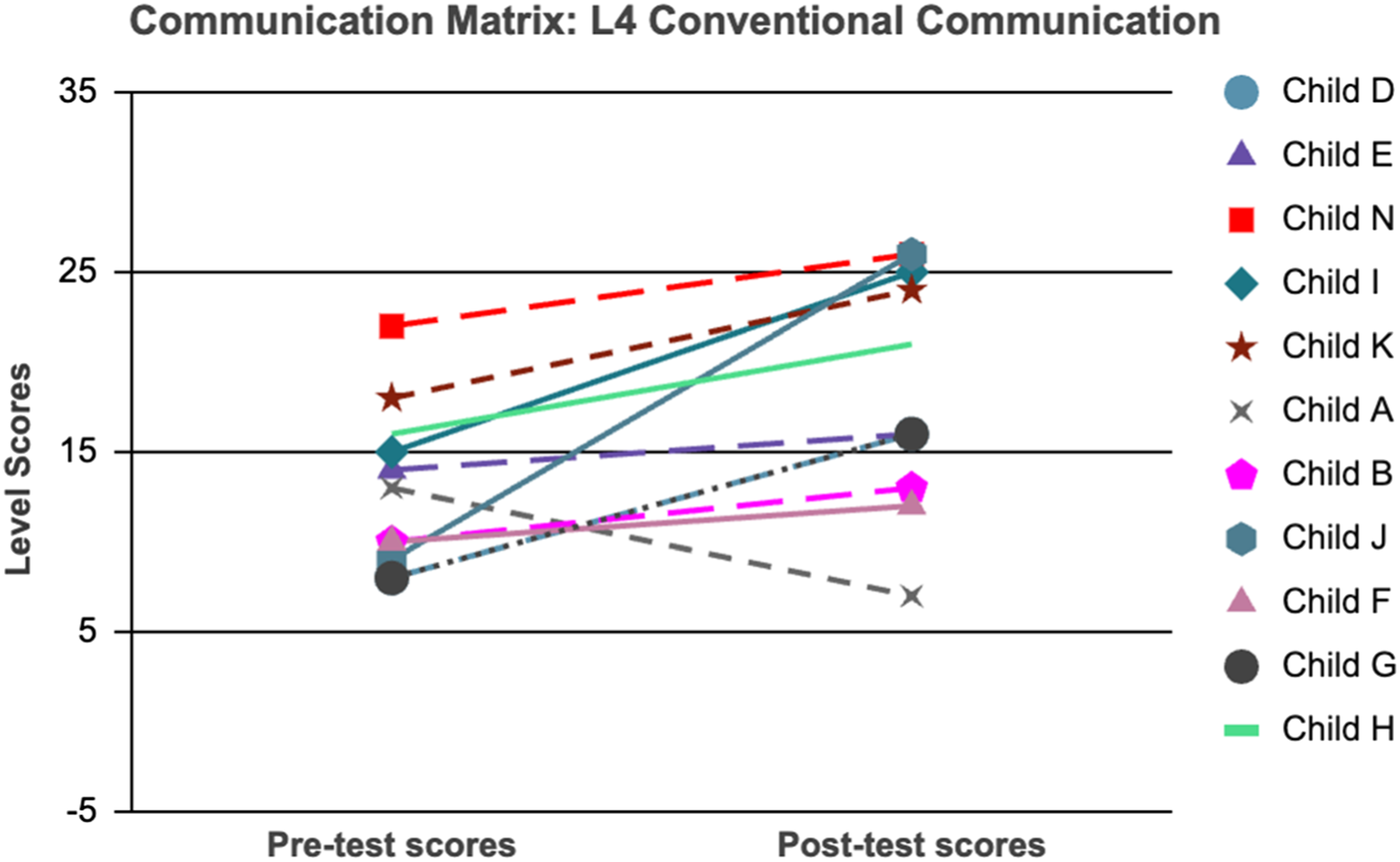
Analysis of results from these researched measures (CDDC and Communication Matrix) show gains in increasingly complex skills used to communicate (Communication Matrix) as well as skill increases in domains of receptive language, expressive language, emotional and social skills (CDDC) over the course of the intervention period. This suggests that Eye to I
The third quantitative measure, the Eye to I
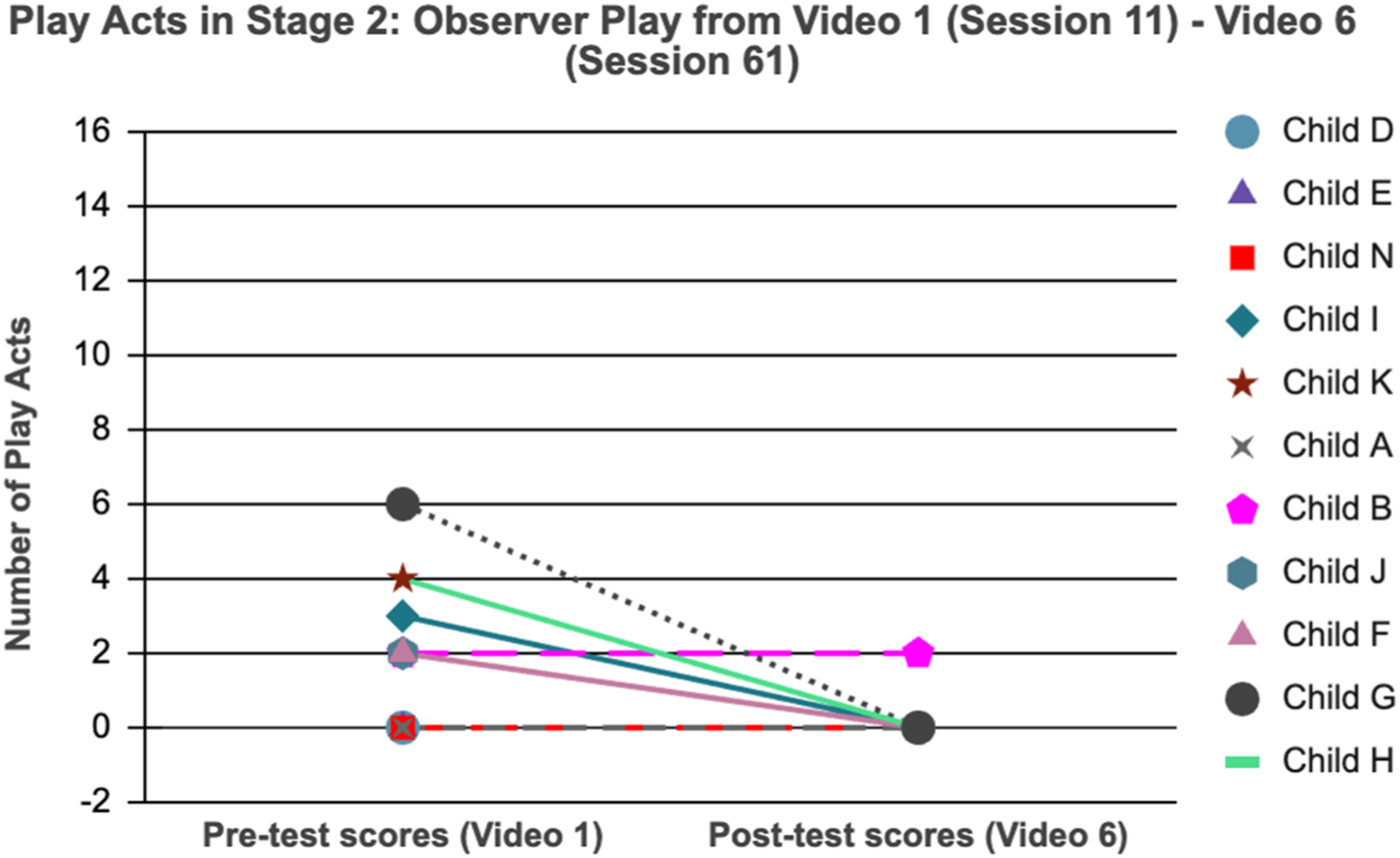
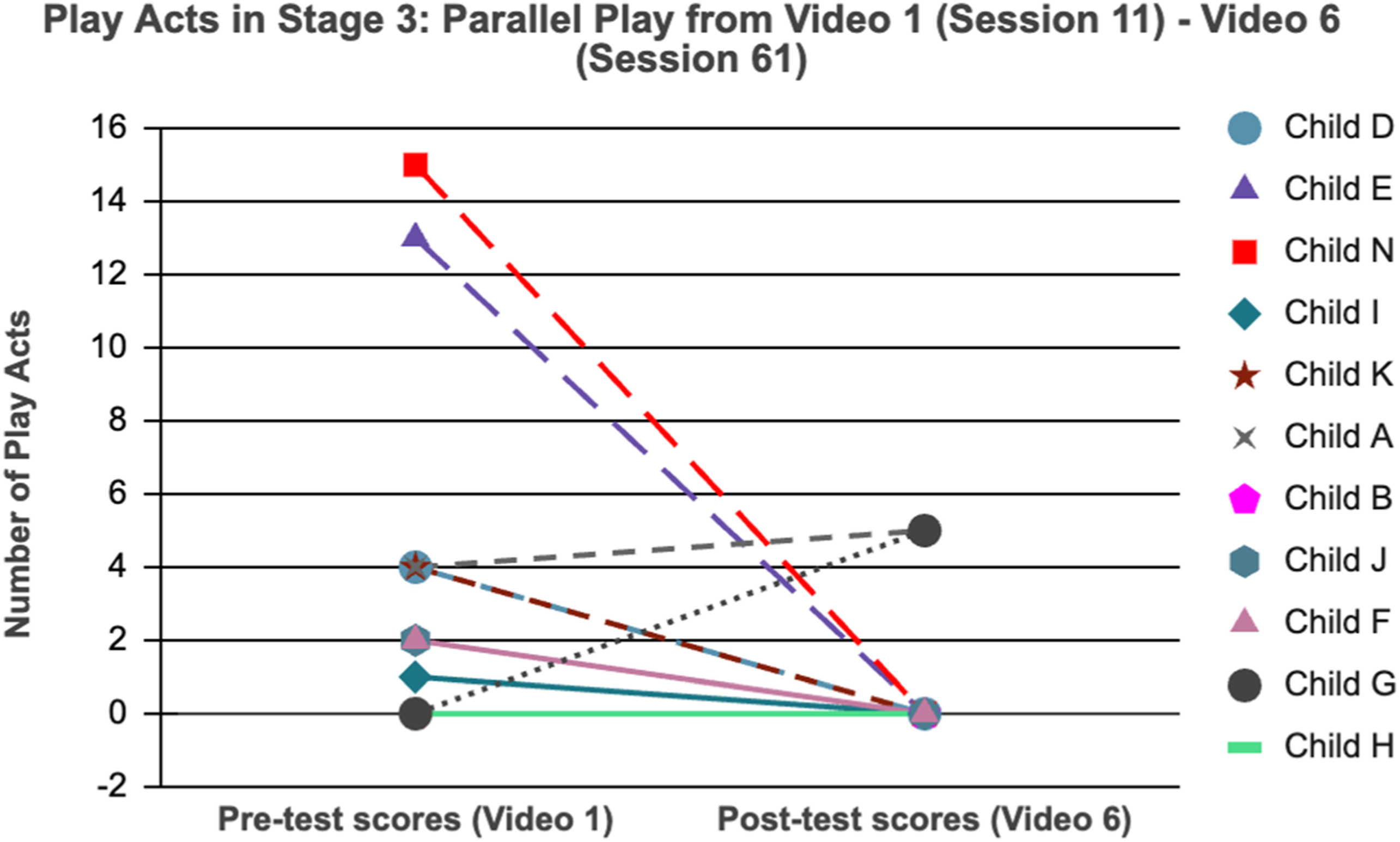
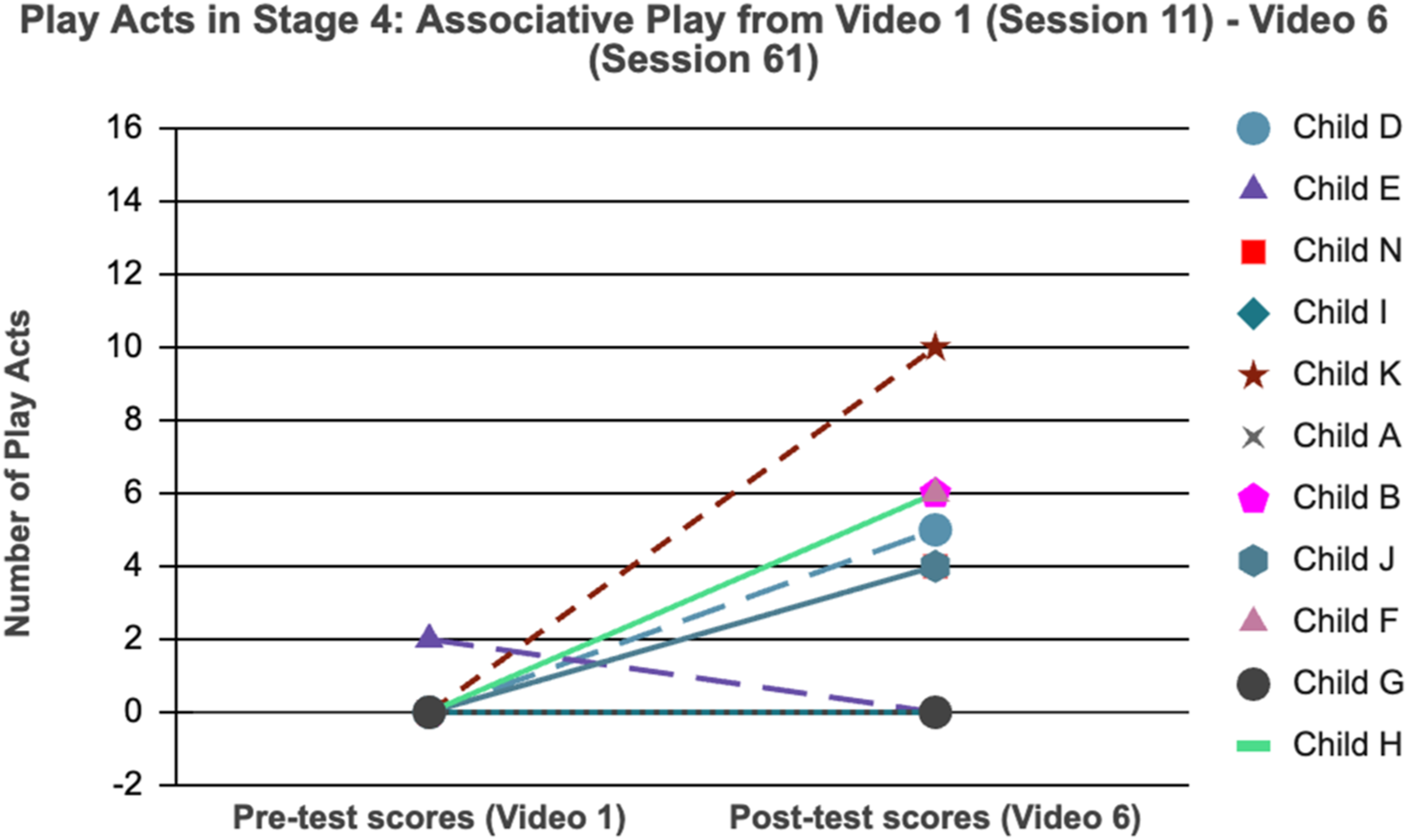
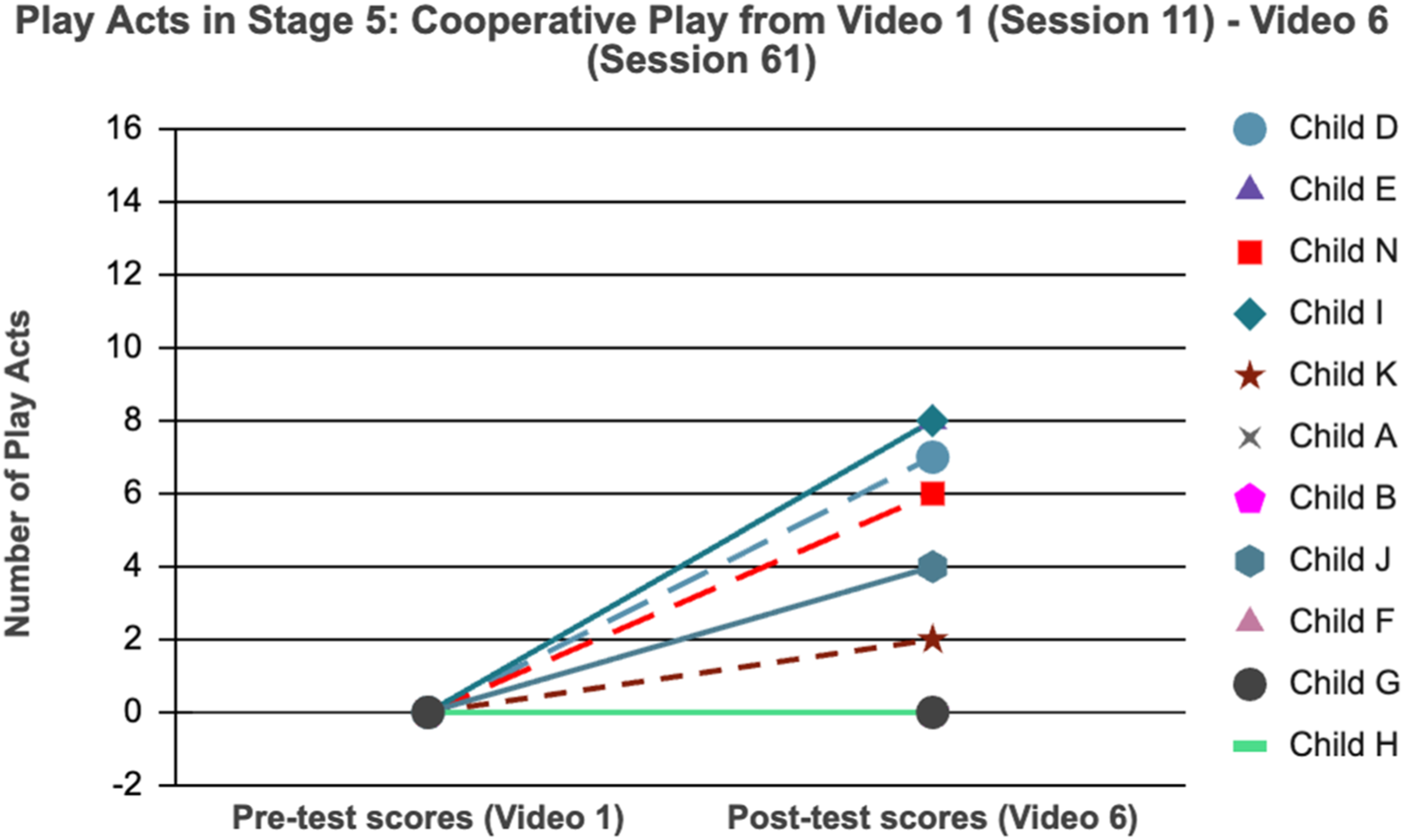
Figures 8–12 illustrate that recorded number of play acts in solitary, observer and parallel stages of play (S1, S2, S3) reduced for nine out of 11 between pre-test and post-test video analysis while engagement in associative and cooperative play increased. These figures also depict individual trajectory, such as that of participant G, showing very limited skills at baseline (pre-test video analysis of no play acts in four out of five play stages) and an increase from baseline to skills recorded in S3 (Parallel) indicating emerging social interaction. Engagement in parallel, associative and cooperative play (as represented by S3, S4, and S5 in the Eye to I codebook) involves increasing skills of intentionality and social reciprocity measured through the presence of joint attention behaviors such as imitation, proximity to others, bids for attention, sharing of material, and more (See Appendix B: Eye to I Codebook). The Eye to I codebook analysis reveals that participants acquired skills necessary to engage in greater interaction present in complex social stages of play S4 (Associative) and S5 (Cooperative). The typically developing child will engage in solitary and observer play at 2.5 years and need at least 12–18 months to acquire the social skills required for associative play reached at approximately 4 years. In the present study participants moved from observer play to associative play in less than 1 year, indicating that gains in social skills were not due to chronological age and natural development alone. Video analysis shows that the participants gained intentional use of skills in reciprocity and joint attention to facilitate social engagement. This intentional use and application of skills is recorded by the Eye to I© codebook. These codes align with the results from the two other quantitative measures (CDDC and Communication Matrix) supporting the notion that the Eye to I Codebook warrants further investigation as a measurement of skill assessment. The results from all three pre-test and post-test quantitative measures show that acquisition of skills involving social interaction and communication occurred during the Eye to I© intervention period. Number of play acts per participant at each stage of social play in Pre-test and Post-test. This data was obtained using the Eye to I© codebook. Number of play acts per participant at each stage of social play in Pre-test and Post-test. This data was obtained using the Eye to I© codebook. Number of play acts per participant at each stage of social play in Pre-test and Post-test. This data was obtained using the Eye to I© codebook. Number of play acts per participant at each stage of social play in Pre-test and Post-test. This data was obtained using the Eye to I© codebook. Number of play acts per participant at each stage of social play in Pre-test and Post-test. This data was obtained using the Eye to I© codebook.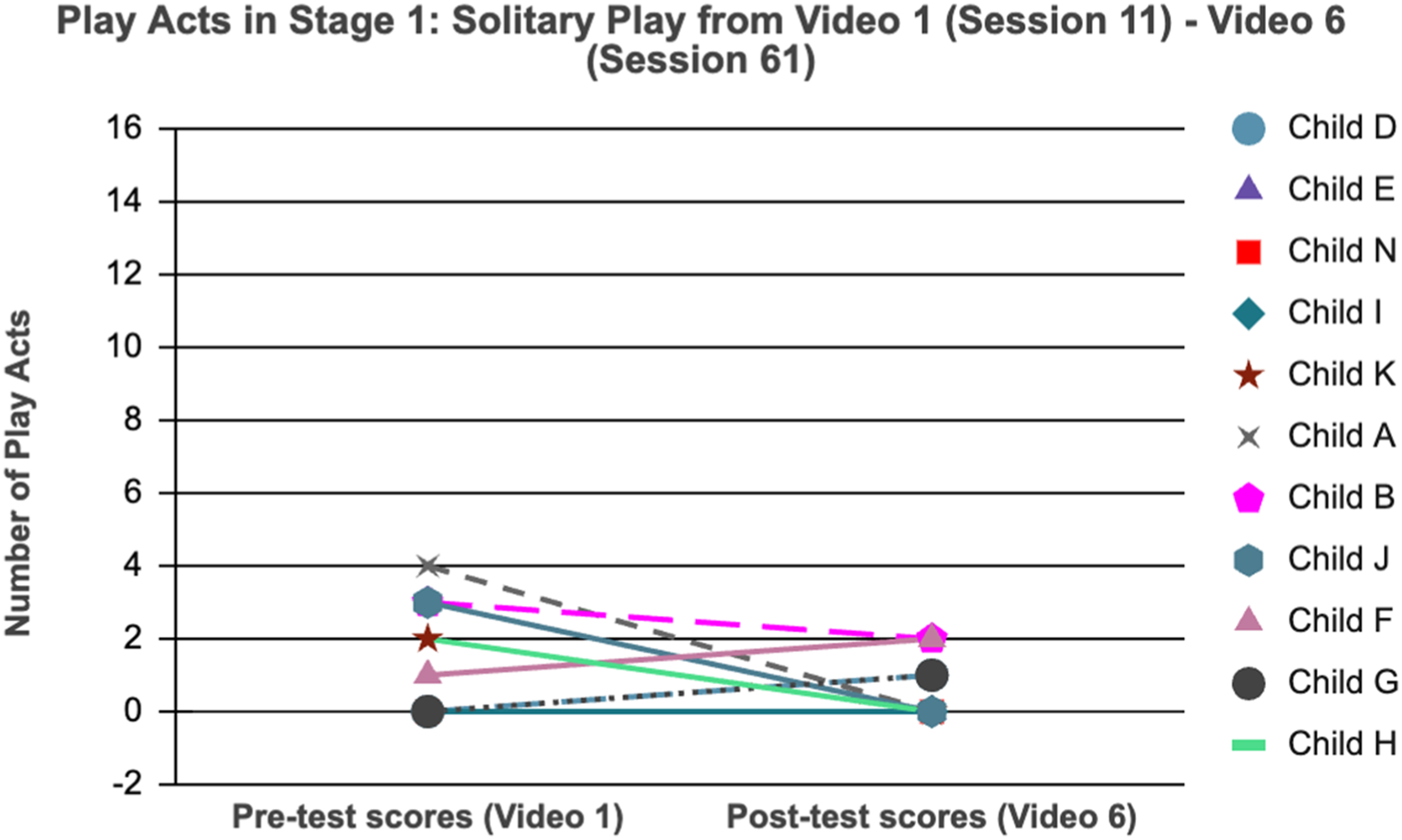
Reflections and insights from parent interviews post-intervention
The present study used thematic analysis to understand core themes defining parental experiences of children’s social development during intervention. Recorded audio interviews were transcribed by research coders who were not a part of the intervention team. The transcriptions produced were then subjected to coding with a bottom-up approach. Through this process, codes were identified from verbatim that were later grouped into sub-categories based on common patterns. A handful of such sub-categories then came together to form themes of this paper as described in Figure 13. Theme: Therapeutic Targets of Eye to I© and subthemes of social communication, play-based behaviors, and shared quality experience.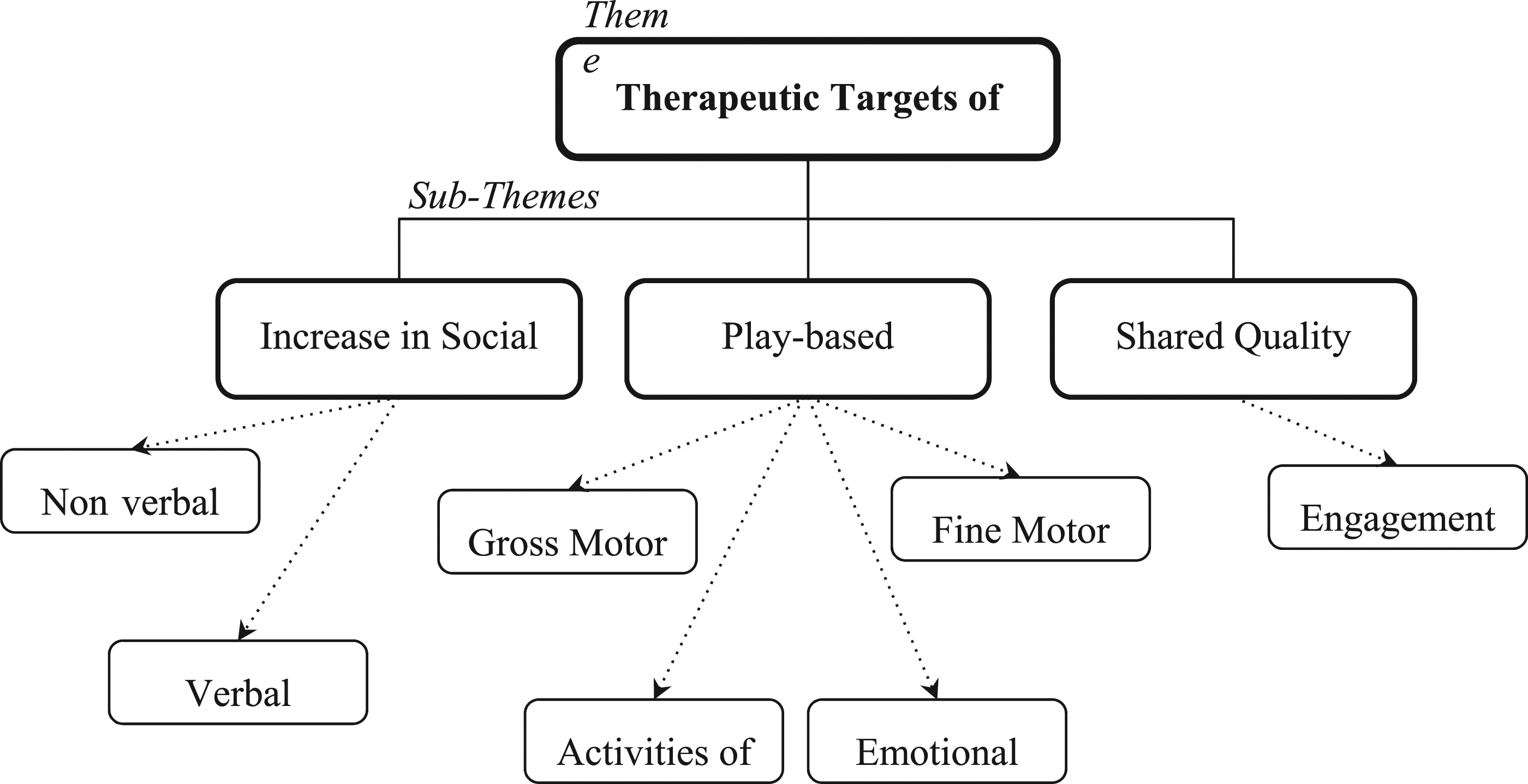
Thematic analysis further supports the statistical analysis showing increased social engagement and complexity in interaction post Eye to I© intervention. Parental assessment of Eye to I© evaluates the quality and impact of therapeutic targets of play behaviors, social communication and shared quality experience (Figure 13). Parents expressed that skills learned in therapy during the intervention generalized to interactions beyond therapy, illustrating that play intervention can contribute to positive social learning across contexts (Gibson, et al., 2021). For example, one parent mentioned “[He is] acknowledging people, communicating much more to people, making conversation and initiating with people. Interaction with neurotypical children has improved, has been talking more and initiating,... has become more independent” (child I parents). Another reported their child showed increased skills in social communication, and emotional growth, “G is interacting more, playing with kids was always there but not the acceptance of a different opinion coming from another child during play. But now even if G does not give their inputs, G finds happiness and more acceptance with other kids and what they want to play” (child G parent).
The final area of thematic analysis is parent experience and critique of the therapeutic targets and the Eye to I© model. The role of play within therapy and parent-child interaction was a significant area of learning for parents. This is exhibited by the following comments: “play is awesome, a lot of changes I’ve seen in my child because of the model” (child F parent); “I also learnt better how to play with my child” (child K parent). Meanwhile child A parent mentioned unaddressed goals, “A has become slightly stubborn, so that is definitely something that still needs to be worked on by the team […] There is no change in this aspect”. Continuing to develop understanding from a parental lens is crucial to assessment of the model. The qualitative aspect of this paper afforded insight into unique observations that could only come from the parent perspective. For instance, child C parent said, “if parents can have cameras in the reception area [...] they can see what the child is doing, will be a great learning for them”. The interviews recorded in this research revealed seemingly small details of the parent experience that can add to, and further enhance, the execution of the Eye to I© model and the role of play in development of social communication skills in autism.
Discussion
This study displays the continuous and upward learning process of the participants as demonstrated by the results from three measures and corroborated by findings from parent interviews. Quantitative and qualitative data show that, over the course of intervention, participants engaged in increasingly complex social stages of play during therapy sessions and greater social interaction in non-therapeutic environments using skills associated with social competencies which facilitate communication. Quantitative measurements point to skills gained across multiple developmental domains, especially in social skills and communication. The Eye to I© codebook tracked skills such as gaze and proximity associated with joint attention and social interaction and measured not only the presence of these skills but how they were used to express greater social reciprocity in social stages of play. Participants in the present study showed an increase in skills across all stages of play in approximately 6 months though in typical development children acquire the requisite skills to participate in complex social stages of play over the course of 18 months or longer (Chang et al., 2018). In addition, qualitative data from parent interviews paints a picture of growth in emotional sharing and intergenerational family communication - desired outcomes for many Indian families seeking guidance regarding their child’s autism diagnosis (Das et al., 2017). These findings open the door for further, more rigorous investigation of Eye to I© intervention, and specifically the Eye to I© codebook and its detailed tracking of skills that contribute to joint attention, reciprocity and the aspects of social interaction and communication compromised in autism.
Conclusion
In conclusion, this paper demonstrates that participants in Eye to I© Social Communication therapy show increases in social skills, complexity of play engagement and family interaction during the period of intervention. Additionally, the Eye to I© codebook is introduced as a detailed measurement which both defines and assesses play behaviors according to social stages of play. The aim of this codebook is to measure specific skills of social reciprocity so that in turn practitioners can address those skills within therapeutic intervention. Eye to I intervention does just this and the results of this study suggest it as an effective method. The findings in this study support the notion that, with further study, the Eye to I© codebook could be both an assessment tool and a guide for further therapeutic inputs that facilitate social interaction and communication in autism. Furthermore this study contributes insights to a limited body of research surrounding autism in India by giving voice to parent’s experience with the intervention process and introducing Eye to I© as a culturally adaptable intervention and measurement based in developmental skill acquisition.
Limitations and future research suggestions
This study aims to provide a window onto the skill acquisition needed for improved engagement in social interaction and communication. However, it is limited by the small sample size restricting generalization of results. An increased sample size using robust quantitative tools could be used in upcoming research giving the findings an empirical advantage. Further research involving a randomized control trial would more thoroughly inform on the validity of both the Eye to I© therapeutic intervention and the codebook as a measure of skill acquisition while overall developing a greater understanding into the therapeutic efficacy of focusing on social stages of play. This association between advances in social play and the specific examples in the codebook of how to flexibly facilitate and maintain participation could be of immense benefit to practitioners in India where general norms often adhere to restricted scripts and rehearsed scenarios. Future research comparing participants in Eye to I© intervention and participants in alternative intervention could further illuminate gains and shortcomings not seen here. In addition, further studies could use the Eye to I© codebook as a template for exploring the association between social and cognitive stages of play, and the role of emotional regulation in inculcating social skills in autism.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.