
Abstract
Background
The motor and vocal tics that characterise Tourette syndrome are stigmatizing and impact on quality of life. Behavioural interventions such as Exposure Response Prevention or Comprehensive Behavioural Interventions for Tics are first line treatment for Tourette syndrome, but availability is limited. This study is the first to explore the impact of an established manualised Exposure Response Prevention treatment protocol, developed for individual therapy, but here uniquely delivered intensively, to a group.
Methods
A naturalistic study comprised of a consecutive series of children (N = 20), aged 8–16 years (M = 12, SD = 2.17) were offered Exposure Response Prevention in one of two groups, delivered in series within a specialist clinic. Young people received the equivalent of 12 sessions (matching the manualised individual protocol).
Results
The YGTSS and Giles de la Tourette Syndrome Quality of Life Scale for Children and Adolescents (Satisfaction Scale) showed significant improvement following treatment with moderate to large effect sizes. Thirty-five percent of children demonstrated a reliable improvement on the YGTSS Global Tic Severity score.
Conclusions
These data suggest an established Exposure Response Prevention protocol can be delivered in an intensive, group setting with a positive clinical outcome. Replication in a randomized controlled trial is an important next step.
Introduction
Tourette Syndrome (TS) characterised by motor and vocal tics (APA, 2013), has a prevalence of 0.77–1% (Knight et al., 2012). It is frequently associated with comorbidities such as Attention Deficit Hyperactivity Disorder (ADHD) and Obsessive Compulsive Disorder (OCD; Abramovitch et al., 2015). Additionally, social and emotional difficulties (Cutler et al., 2009), impaired school functioning (Cubo et al., 2017) behavioural difficulties and a diminished quality of life (Eapen et al., 2016) are also frequently reported.
Behavioural therapy is the first-line intervention for TS delivered following psychoeducation (Andren et al., 2022). There are two broad behavioural approaches with an evidence base: first, Comprehensive Behavioural Intervention for Tics (CBITs; Woods et al., 2008) which incorporates Habit Reversal Training techniques (Azrin & Nunn, 1973) and second, Exposure and Response Prevention (ERP) originally developed by Meyer (1966) to treat obsessive-compulsive symptoms. Treatment effects of ERP for tics are comparable to those of HRT (Andren et al., 2021; Verdellen et al., 2004). The unique advantage of ERP is that it addresses multiple tics simultaneously in contrast to HRT/CBITs, which treats one tic at a time. Despite effect sizes in these studies being moderate to high (0.57–1.5) with significant reduction in tic severity (McGuire et al., 2014), behavioural treatments are not widely available (Hollis et al., 2016; McGuire et al., 2015).
To address the treatment bottleneck, various delivery methods have been developed. For example, an abbreviated CBITs program (Chen et al., 2020) and other case studies (Blount et al., 2014, 2018; Flancbaum et al., 2010) suggest intensive delivery offers a promising solution by reducing the number of appointments needed. However, much remains unknown about dose effects and optimum delivery formats (Chen et al., 2020).
Another viable option to the treatment shortage is group therapy. Learning in a social context has many unique benefits for young people (Lieberman, 2012), especially during adolescence where peer-to-peer learning is highly effective, often more so than adult didactic instruction (Yeager et al., 2018), potentially making carefully facilitated group work the optimum modality for psychoeducation, post puberty. For TS affected individuals, tics are suggestible (Tallur & Minns, 2010), so there has been some caution about offering group interventions to young people or adults with TS until relatively recently, however, existing data show a group setting for TS provides general benefits such as improved self-efficacy, reduced isolation (Murphy & Heyman, 2007) as well as augmenting TS specific treatment goals (Nussey et al., 2014).
Data are sparse, and while RCTs show some positive improvements, the pattern of change is variable, with weaker effects using the adapted CBITs intervention on vocal tics (Yates et al., 2016; Zimmerman-Brenner et al., 2021). Nissen et al. (2019) developed an HRT and ERP combined protocol in an RCT and found that group and individual delivery had equivalent efficacy, with large effect sizes reported in both cases. Beneficial effects were maintained at 1-year follow-up in both individual and group formats (Nissen et al., 2021). The case for CBIT or a combination of CBIT/ERP behaviour treatment in group therapy is promising.
Though ERP group treatment is well established in other disorders (Whiteside et al., 2018) only one study to date has used a ‘pure’ ERP group intervention for TS (Heijerman-Holtgrefe et al., 2021) describing good outcomes, including improved tic profiles (d = .4) and quality of life (d = .6). This group (run by experts in tic behavioural treatment) used an innovative, intensive ERP protocol developed in consultation with service users included additional components, rather than strictly adhering to a published manualised ERP protocol. While patient involvement is a valid approach to service delivery methods (and one we support), the current paper explores the value of offering an existing manualised tic management protocol developed for individual therapy, in an intense group format. Establishing the effectiveness of an established protocol in a group context means that professionals less experienced in tic treatment will be encouraged to offer them to client groups. The importance of treatment fidelity in delivery of evidence-based interventions is well described (Breitenstein et al., 2010; Carroll et al., 2007; Mihalic, 2004). No investigation to date has examined the feasibility of using an established evidence-based ERP protocol, maintaining procedural fidelity, in a group setting.
The current study aimed to determine if an established, evidence-based ERP protocol, delivered in an intensive group format, leads to significant improvements in tic severity and quality of life outcomes in children with TS.
Methods
Design
A consecutive series of 20 children were recruited for two groups (n = 10 in each group) of identical format, run 4 months apart (July 2019 and November 2019).
Recruitment
Patients were recruited from a specialist TS clinic which accepts referrals from across the UK. Following a multi-disciplinary team (MDT) assessment, the details of which are described elsewhere (McFarlane et al., 2019), the group was offered to all patients who met the inclusion/exclusion criteria outlined below.
Participants
Inclusion criteria for the group were: (a) children aged 8–16 years old (b) diagnosed with Tourette syndrome (TS) or chronic tic disorder (CTD), according to the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (APA, 2013), (c) with at least moderate tic severity indicated by Yale Global Tic Severity Scale (YGTSS; Leckman et al., 1989) Total Score of >13 (or >9 for children with motor or vocal tics only) and (d) able to participate in all 3 days of the intensive group and the “booster day” scheduled 4 weeks after the group ended. None of the children offered the group intervention declined. Children with co-occurring ADHD, OCD, other anxiety or mood disorders were included (Table S1 in supplementary materials), unless the disorder required immediate treatment or was severe and would interfere with group participation. No children were excluded based on this criterion.
Exclusion criteria were: (a) insufficient spoken English to participate in the group (b) participation in ERP or CBITS/HRT sessions in the last year (c) substance abuse, (d) suicidality, (e) psychotic disorders, (f) severe autism spectrum disorders (ASD) or ADHD, which could interfere with a child’s ability to participate in the group. No children were excluded based on these criteria.
Gender, age, ethnicity and co-occurring conditions were derived from hospital records. Participants all had a diagnosis of Tourette Syndrome and were predominantly white males with a mean age of 12 years (SD = 2.17). High levels of comorbidity were present, consistent with TS populations (Hirschtritt et al., 2015) with 17 children (85%) diagnosed with at least one other psychiatric diagnosis (see Table S2 in the supplementary materials). Co-morbid neurodevelopmental conditions were common, 40% had ADHD and 25% had ASD. Children with ASD (10%) or ADHD traits (40%) were also identified during MDT assessment and required further assessment in order to make a formal diagnosis (see Supplementary Materials 1.1 and Table S3 for additional details on baseline characteristics of the sample).
Intervention
The Exposure and Response Prevention (ERP) protocol (Verdellen et al., 2011) comprised 12 weekly individual sessions (12 × 60 mins sessions = total 720 mins). In the present study the same protocol was offered in a group, intensive setting consisting of nine sessions (720 mins). See supplementary materials (Table S4) for a breakdown of sessions and (Outcomes) for intervention details. A booster day was offered 4 weeks post completion to consolidate learning and review progress (120 mins).
Procedure
Sessions were conducted at the hospital, according to the manualised protocol with minor adaptations for the group context (Verdellen et al., 2011). A schedule of the intervention and assessments of outcome measures is shown in Table S5 (see supplementary materials). Within 2 weeks of starting the group, the YGTSS was carried out by an experienced clinician who was part of the team, but not part of the treatment group, over the telephone. Children and their families completed all other baseline measures at the start of the first group session (time zero; t0) and the 4 week ‘booster day’ (time two; t2). Goal based outcome measures and feedback forms were additionally completed at the end of the intensive 3-day group (time one; t1). ERP exercises as per the protocol, were offered in small subgroups of two or three children with peer-to-peer learning (timing, counting tics and encouragement). Therapists rotated around the small groups and offered support. Sessions were delivered by two experienced Clinical Psychologists and an assistant psychologist.
Outcome Measures
Primary Outcome Measure
Yale Global Tic Severity Scale (YGTSS)
The YGTSS (Leckman et al., 1989), is the gold standard measure of tic severity and impairment. The Global severity score (range 0–100) is composed of an Impairment score (0–50) and a Total Tic score (0–50), which sums total motor (0–25) and total vocal (0–25) tic scores. We defined a 25% tic reduction as a positive response on the Total Tic Severity scale (Jeon et al., 2013). The YGTSS has good inter-rater reliability (Leckman et al., 1989) and test re-test reliability is high at 0.94 (Storch et al., 2005).
Secondary Outcome Measures
Goal Based Outcomes (GBOs)
GBOs (Law & Wolpert, 2014) are routinely used to evaluate progress towards a patient’s treatment goals. Each parent and child completed the appropriate version and rated how close they felt they were to achieving their goal on a Likert Scale from 0 (Not at all) to 10 (Goal reached). Participants were invited to establish up to three goals (i.e., GBO 1, GBO 2, GBO three; parent/child rating separately), but some chose to create one or two. Goals were typically about finding successful ways to manage tics. GBOs have acceptable internal consistency (α coefficient of 0.7; Edbrooke-Childs et al., 2015). We considered a reliable change index for GBOs at 2.45 points (Edbrooke-Childs et al., 2015).
The Gilles de la Tourette Syndrome Quality of Life Scale for Children and Adolescents (C&A-GTS-QOL)
Quality of life was measured using the C&A-GTS-QOL (Su et al., 2017), a 27-item patient-reported scale with good acceptability, reliability (α > 0.7) and validity. It comprises four subscales describing Psychological, Physical, Obsessive compulsive and Cognitive aspects of life. Scores for the subscales are generated by summing items and normalising total scores to a 0–100 range (lower scores indicate better QOL). A life satisfaction subscale (GTS QOL satisfaction score) presented on a visual analogue scale (0–100 range) is scored in the opposite direction, so higher scores indicate greater satisfaction.
Additional measures taken at baseline to characterise the sample are described in the supplementary materials section 3.1.
Statistical Analyses
Measures were collected and where relevant analysed at three time points: t0, t1 and t2. The YGTSS showed one outlier on all subscales apart from the Motor subscale (using inspection of a boxplot). Difference scores were not normally distributed for the Vocal (Shapiro-Wilk’s test = 0.002) and Impairment (Shapiro-Wilk’s test = 0.016) subscales. Therefore, difference scores were based on the median change in scores; these changes were tested using Wilcoxon signed rank test/Sign test as appropriate and converted into effect sizes (r value; Fritz et al., 2012). The GTS QOL C&A, showed no outliers (assessed by inspection of a boxplot) and difference scores were normally distributed (lowest p value on Shapiro-Wilk’s test >.281), so difference scores were based on the mean change in scores; these changes were tested using paired samples t-tests and converted into effect sizes (Cohen’s d; Cohen, 2013). GBO scores had outliers and were not normally distributed (Shapiro Wilk’s < 0.05). Here difference scores were based on the median change in scores. To maintain a conservative approach, we limited analysis of GBO data to a descriptive comparison of change against benchmark data i.e. the UK Increasing Access to Psychological Therapies program for children and young people—CYP IAPT—data set from 2011 to June 2015, which includes data from 75 separate services (Law & Wolpert, 2014). Results on the YGTSS Global severity score, GTS QOL Total, GTS Satisfaction and GBOs were analysed at the individual level by reliable change analysis, which determines whether the degree of change on each measure was statistically reliable, and not due to measurement-error (Jacobson & Truax, 1991). This allows for classification of participants as either (i) reliably improved, (ii) reliably deteriorated, or (iii) not changed. Differences in patient characteristics/outcome measures between the first and second ERP groups were tested using independent t-tests/Mann-Whitney U tests for continuous variables and chi-square/fisher’s exact tests for categorical variables (results are presented in supplementary materials sections 1.2 and 1.3 and Figures S1, S3 and S5).
Qualitative Feedback
Patient feedback is an important part of the acceptability and feasibility assessment. We developed an 8-item questionnaire (see ‘Feedback form’ in Supplementary Materials). Questions 1–5 were answered using a set of predefined categorical answers, six to eight were open-ended, in which participants could provide free text responses. For the open-text questions only, responses were grouped into categories based on the principles of content analysis (Cole, 1988).
Results
Feasibility
There were no patient dropouts or missing data on the primary outcome measure.
Outcomes
Primary—Tic Severity (YGTSS)
Median Score (Interquartile Range) by Time Point and Effect Sizes for YGTSS Subscales.
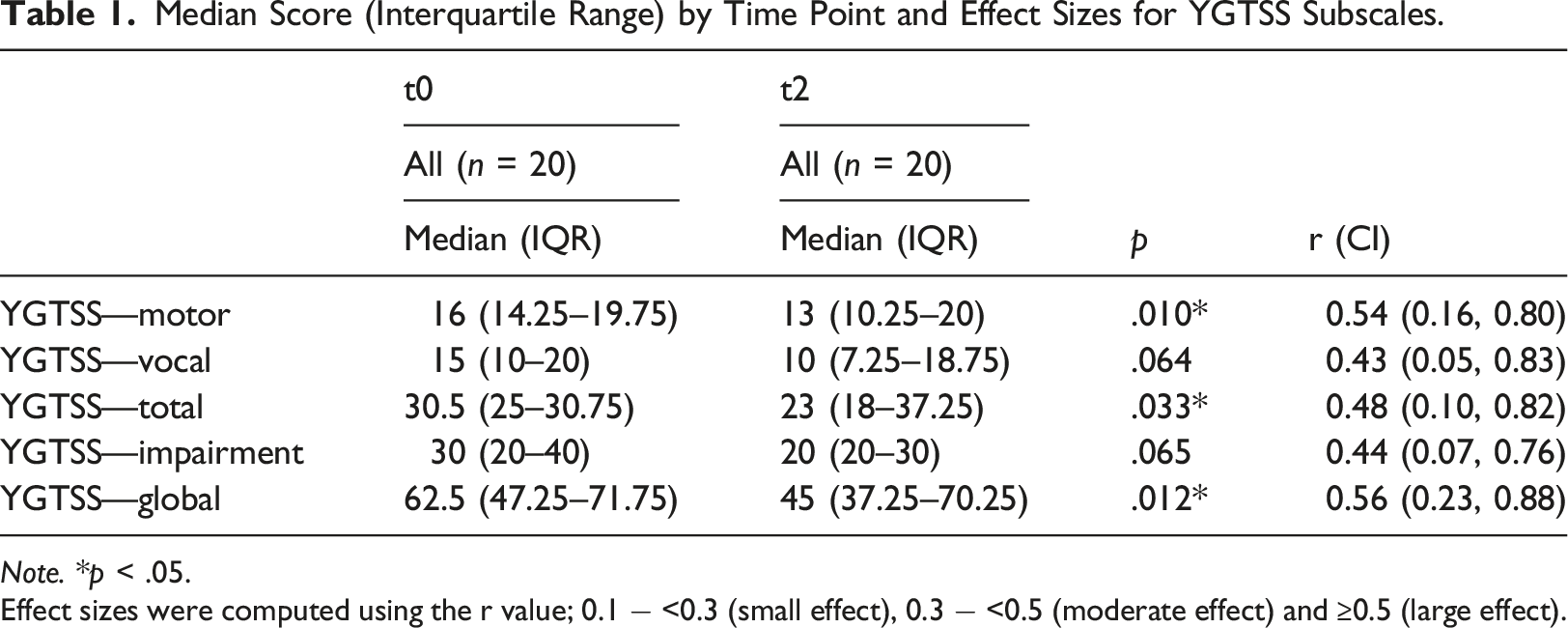
Note. *p < .05.
Effect sizes were computed using the r value; 0.1 − <0.3 (small effect), 0.3 − <0.5 (moderate effect) and ≥0.5 (large effect).
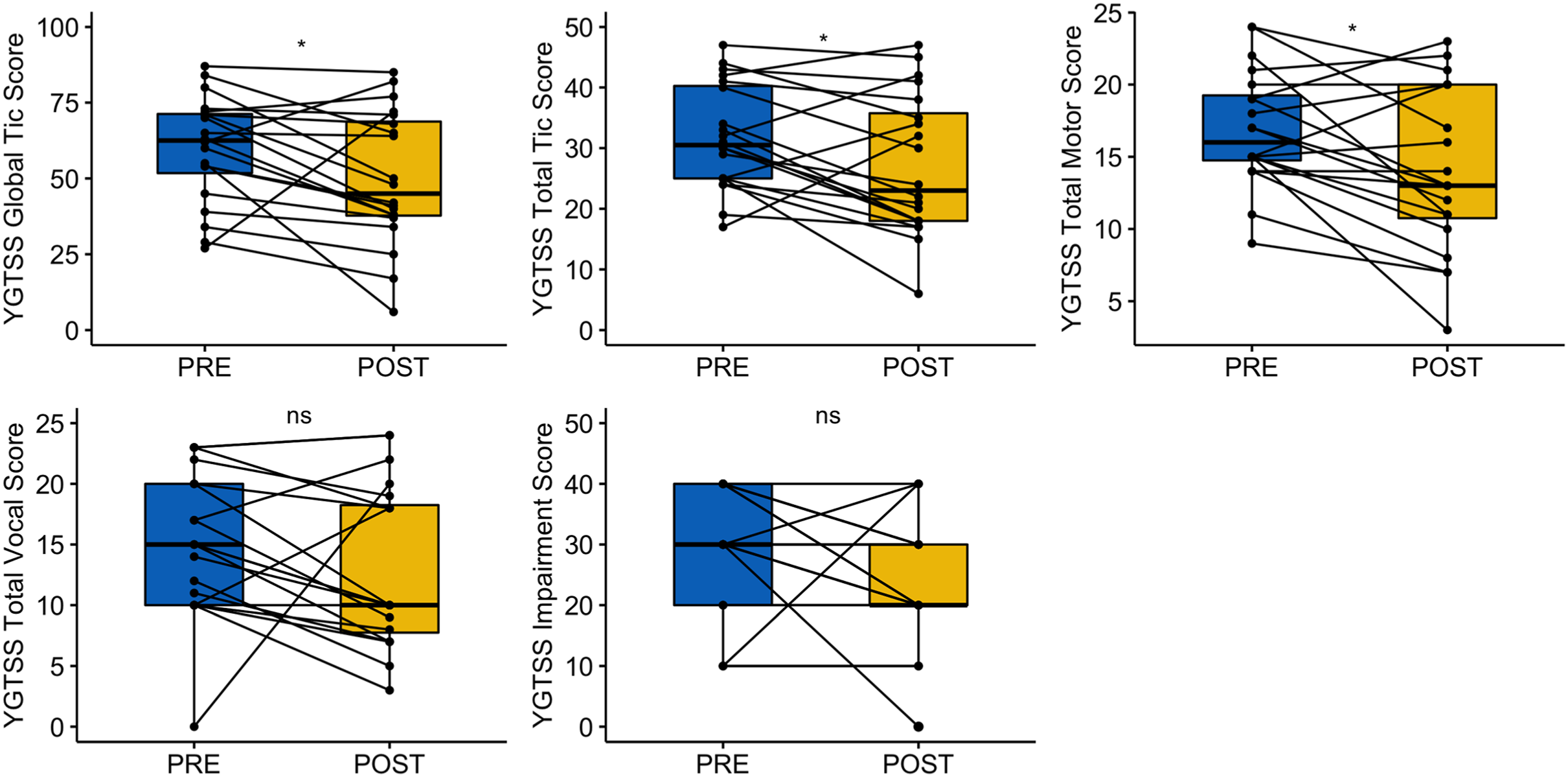
Change in tic severity pre and post-intervention on the Yale global tic severity scale’s (YGTSS) global severity score and YGTSS Subscales (total tic, motor, vocal and impairment scores).
Secondary—Quality of Life (GTS QOL) and Patient Rated Goal-Based Outcomes (GBO)
Mean Difference Scores (Time 0 – Time 2), Paired Samples t-Tests Results and Effect Sizes (Cohen’s d) for GTS QOL Subscales.
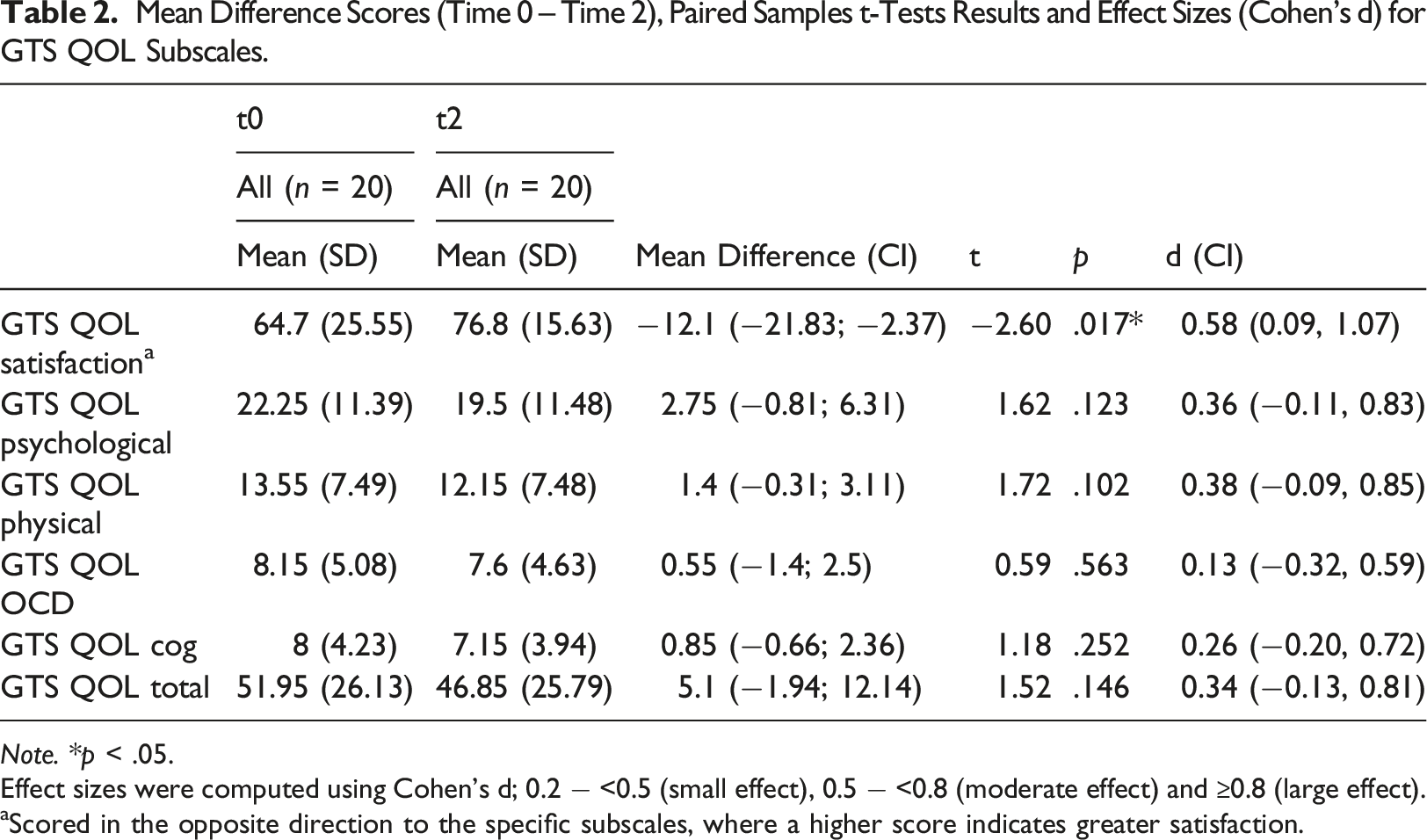
Note. *p < .05.
Effect sizes were computed using Cohen’s d; 0.2 − <0.5 (small effect), 0.5 − <0.8 (moderate effect) and ≥0.8 (large effect).
aScored in the opposite direction to the specific subscales, where a higher score indicates greater satisfaction.
Descriptive Statistics by Time Point for Parent and Child GBOs.
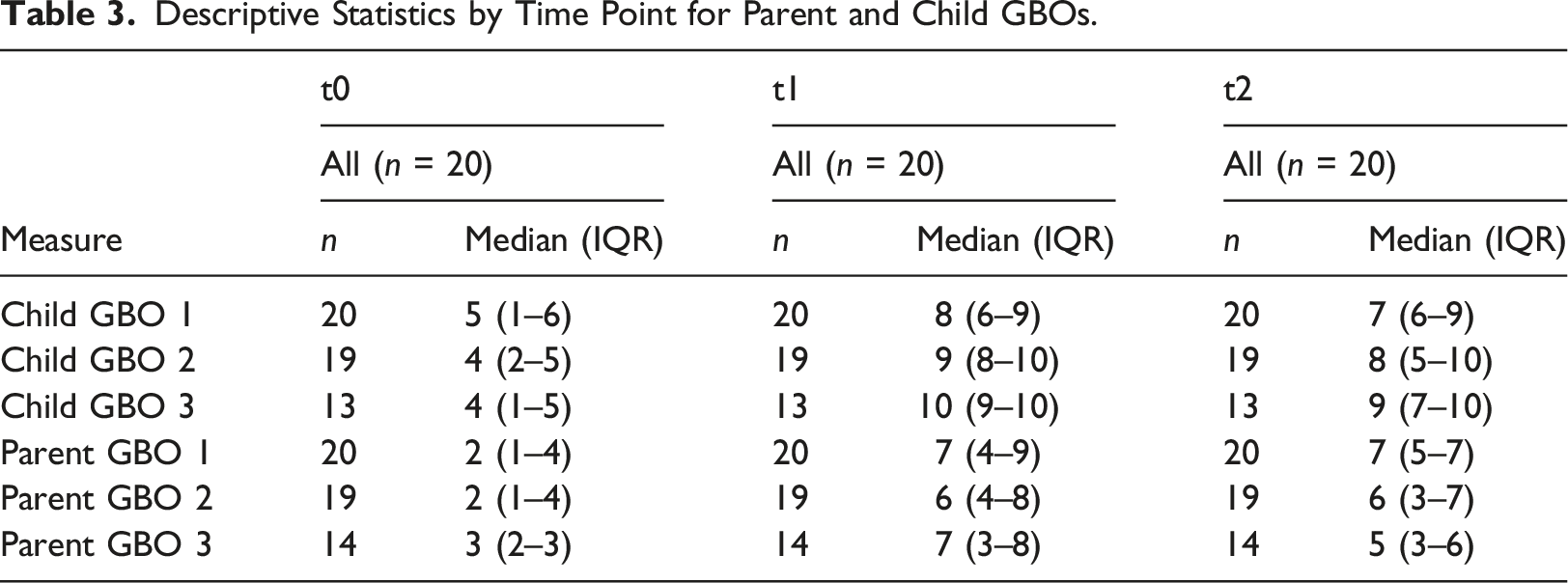
All child and parent-reported GBO scores showed median increases (implying patients reported being closer to their therapeutic goal following treatment) from t0 – t1 and t0 – t2. All child GBOs and parent GBO three showed a small decrease from t1 – t2, the period post the group ending to follow-up. The mean increases in goal ratings from t0 – t2 were 3.72 (self-reported) and 3.51 (parent-reported). This compares to a mean increase in goal ratings of 3.73 (self-reported) and 3.7 (parent-reported) in the CYP-IAPT study (Wolpert et al., 2016; median increases in GBOs were not available for benchmarking, which is why mean difference scores are reported here). Reliable improvement between t0 and t2, was seen in 14/20 (70%) for child-rated GBOs and 15/20 (75%) for parent-rated GBOs (using averaged GBO 1, GBO two and GBO three scores where available for each rater). None showed reliable deterioration between t0 and t2.
Qualitative Feedback
Overall, responses from the feedback questionnaire suggested high levels of acceptability (see Figures S6 and S7 in the supplementary material). The majority of young people described the group as enjoyable, useful and effective and stated they would recommend it to a friend. 80% of young people had no suggestions for future improvements according to free text questions.
Discussion
The current study is unique in examining whether an established manualised evidence-based ERP protocol, developed for individual therapy, maintains efficacy when delivered in an intensive group format. We found positive treatment outcomes with an overall large effect size (r = 0.56) for the YGTSS Global severity score. Thirty-five percent of participants achieved reliable improvement with 45% showing clinically meaningful change overall. These findings align with previous trials using a clinically developed ERP group treatment, which showed positive effects of a similar magnitude (Heijerman-Holtgrefe et al., 2021). Our data show an adapted group intensive delivery of an evidence-based manualised ERP intervention for tics is effective and feasible. ERP has potential advantages over the CBITs protocol as all tics are treated simultaneously rather than one by one as in the CBITs approach. Therefore, an ERP group could offer efficiencies on a number of dimensions. Clinicians less experienced in tic treatment delivery may find these data useful as it suggests an existing ERP manualised treatment can be used ‘off the shelf’ in intensive treatment groups, an important consideration given the current treatment bottleneck.
There was a marked improvement in motor tics and though there was a moderate effect size improvement in vocal tics, it did not reach statistical significance, reflecting a pattern in previous CBITS (Yates et al., 2016) and ERP TS groups (Heijerman-Holtgrefe et al., 2021), but this may be a reflection of the group tic profile (Yates et al., 2016). While impairment and most QoL scores did not improve significantly as a result of the group, this may be due to the complexity of the group recruited. The population of children recruited had high levels of co-occurring conditions alongside tics, which are commonly described as more impactful on QoL than tics themselves (Atkinson-Clement et al., 2022) and may have impacted impairment ratings. Although the samples were too small to test for statistical difference, on visual inspection of the data, the first group appeared to have better outcomes (see Figures S1 and S3 in supplementary materials). Similar differences comparing children participating in a group intervention at different times of the year were found by Yates et al. (2016), who hypothesised this was due to one group coinciding with the return to school, which some participants found stressful and may have impacted on QoL. Similarly, in our study the first group was carried out in July, during the summer, whereas the second was carried out in November, where young people were in school and may have been experiencing additional stressors. Though tics are suggestible for young people with existing tics, there was no clear evidence participants’ tics increased following exposure to other young people’s tics in the group, providing reassurance to families who might be concerned about this (Woods et al., 2010). Overall QOL ‘satisfaction’ improved following treatment and, while physical aspects on the QOL measure improved they did not reach significance. Heijerman-Holtgrefe et al. (2021) reported an improvement on the summed QOL subscales of the same QOL measure but neither individual subscale nor ‘satisfaction’ scores were reported. In broad terms, the message is similar across both studies: improvements in both tic profile and QoL following treatment. These outcomes might be considered cornerstones of viable treatment for the TS population.
All participants described getting closer to reaching their therapeutic goal following the group, and 70% reached threshold for a reliable change on GBOs. The magnitude of change was similar to reports from CAMHS nationwide studies (CYP-IAPT study; Wolpert et al., 2016). The study’s low attrition and high attendance rates also suggest acceptability and feasibility of the group intervention. As is true for any TS behavioural treatment (Capriotti et al., 2014) intensive group treatment was not universally effective (55% did not show clinically meaningful change), and for some children, may not be appropriate. Possible reasons for this are discussed in more detail by Heijerman-Holtgrefe et al. (2021) and include reduced time to practise in between sessions compared to individual treatment and less flexibility/time to address a child’s individual difficulties.
The results on the primary outcome measure are promising, nonetheless, it is important to consider the study’s limitations. This is a small study with no control group, randomisation or blinding. Participants were all children and adolescents with mild to severe TS symptoms and complex comorbidities typical of the wider TS population (Eapen et al., 2004). Still, our centre is more likely to manage relatively complex cases given its tertiary referral status. Showing a positive response in a relatively complex group, is likely to indicate the treatment protocol will be effective (and possibly more so) in TS populations in community services. The 4 week follow-up period may inadvertently capture natural course fluctuations (Roessner et al., 2011), and longer follow-up studies are needed. While careful attention was paid to the treatment protocol described by (Verdellen et al., 2011), we did not use a fidelity checklist, similar to those used in previous studies (Sukhodolsky et al., 2009).
Replication of the study with a larger sample as an RCT—including a health economic analysis—is warranted. It is possible non-specific group factors such as social support, feeling accepted or reducing stigma had a generalised positive effect on well-being which could theoretically indirectly impact on tic profiles. These non-specific group effects are important to explore as “fitting in with peers” is a key factor influencing QOL in children with TS (Cutler et al., 2009). Such effects are discussed elsewhere in an RCT comparing psychoeducation and HRT treatment groups in a TS population (Yates et al., 2016).
This study provides promising indications that a manualised ERP tic treatment developed for individual therapy can be delivered in an intensive group format as an acceptable, feasible and effective option, offering increased accessibility to treatment, reducing tic severity and improving quality of life for young people with TS.
Supplemental Material
Supplemental Material - Applying an Established Exposure Response Prevention Protocol for Young People With Tourette Syndrome in an Intensive, Group Format: A Feasibility Study
Supplemental Material for Applying an Established Exposure Response Prevention Protocol for Young People With Tourette Syndrome in an Intensive, Group Format: A Feasibility Study by Maria Hadji-Michael, Matteo Catanzano, Eve McAllister, Isobel Heyman, Oliver Lack, Tara Murphy, and Jane Gilmour in Clinical Child Psychology and Psychiatry.
Footnotes
Acknowledgements
All research at Great Ormond Street Hospital NHS Foundation Trust and UCL Great Ormond Street Institute of Child Health is made possible by the NIHR Great Ormond Street Hospital Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of the NHS, The Beryl Alexander Charity, Great Ormond Street Hospital Children’s Charity, the NIHR or the Department of Health.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MC’s employment at the start of the project was funded by The Beryl Alexander Charity and Great Ormond Street Hospital Charity.
Correction (June 2023):
This article has been updated with Dr Isobel Heyman’s bio since its original publication.
Ethical Approval
The Great Ormond Street Hospital for Children NHS Foundation Trusts’ Clinical Audit Team approved this study as part of a service evaluation (audit reference number: 2420). Although it was decided that the collection and analysis of data did not require ethical review by an NHS research ethics committee, care was taken to ensure ethical standards were met. No personally identifiable information was described in this study.
Supplemental Material
Supplemental material for this article is available online.
Author biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.