
Abstract
Spatial cognition is the ability to detect, process, integrate, and formulate the spatial aspects of the environment. Spatial abilities, as perceptual doorway of information processing, influence on higher cognitive functions. This systematic review aimed to explore impaired spatial ability in individuals with Attention Deficit-Hyperactivity Disorders (ADHD). The data from 18 empirical experiments that explored at least one factor of spatial ability in individuals with ADHD was collected in accordance with the PRISMA approach. This study discussed several determinants of impaired spatial ability, including factors, domains, tasks, and measures of spatial ability. Furthermore, the impact of age, gender, and comorbidities are discussed. Finally, a model was proposed to explain the impaired cognitive functions in children with ADHD based on spatial abilities.
Keywords
Introduction
Attention-Deficit/Hyperactivity Disorder is a neurodevelopmental disorder with two main symptoms: inattentiveness and hyperactivity-impulsivity (Klein et al., 2012). The three prominent cognitive theories in ADHD are the executive theory (Barkley, 1997), delay aversion or motivational theory (Sonuga-Barke, Taylor, Sembi, & Smith, 1992), and the dual pathway theory (Sonuga-Barke, 2003). The executive theory stresses impaired executive function, the delay aversion theory suggests an impaired reward processing and the dual pathway theory considers a combination of two aforementioned theories. At the cognitive level, behavioral symptoms of ADHD are explained through impaired cognitive functions including inhibitory control (Schachar et al., 2000), working memory (Rapport et al., 2008), attention (Barkley, 1997), time perception (Nejati & Yazdani, 2020), emotional processing (Borhani & Nejati, 2018), reward processing (Wetterling et al., 2015), and social cognition (Nejati, 2022; Pineda-Alhucema et al., 2018).
At the neural level, ADHD is considered as abnormal or lazy frontal lobes and respective subcortical regions. Structural and functional neuroimaging studies in individuals with ADHD have identified alterations in different brain areas, including the right dorsolateral prefrontal cortex (Hart et al., 2013), the left inferior frontal gyrus (Samea et al., 2019), the right inferior frontal gyrus (Hart et al., 2013), the right ventrolateral prefrontal cortex (Norman et al., 2016), and the right inferior fronto-striatal area (Lukito et al., 2020). Beyond correlational studies, non-invasive brain stimulation found a causal association between stimulation of the frontal lobe and improvement in executive and motivational functions in children with ADHD. For instance, anodal transcranial direct current stimulation (tDCS) over the left dlPFC reduces ADHD symptoms (Allenby et al., 2018; Soff et al., 2017) and improves memory consolidation (Prehn-Kristensen et al., 2014), inhibitory control (Munz et al., 2015; Soltaninejad et al., 2015; 2019), selective attention (Bandeira et al., 2016), reward processing (Nejati et al., 2020), working memory, interference control (Nejati et al., 2017; Sotnikova et al., 2017), and sustained attention (Allenby et al., 2018). For a comprehensive review see (Salehinejad et al., 2019, 2020b; Westwood et al., 2020).
Spatial cognition: Definition and domains
Spatial cognition is the ability to detect, process, integrate, and formulate all spatial aspects of the environment, including spatial information of all sensory modalities (Sack et al., 2008) and inner mental images (Sack et al., 2005). The factors and domains of spatial ability are a matter of debate in the respective literature. For instance, Carroll (1993), based on a factor analysis study of more than 140 datasets, proposed five factors for spatial ability including Visualization (VIS), the ability to perceive complex patterns and mentally simulate how they might look when transformed (e.g., rotated, changed in size, partially obscured); Spatial Relations/Rotation (SR), the ability to solve problems quickly by using mental rotation of simple images; Closure Speed (CS), the ability to identify a familiar and meaningful visual object from incomplete (e.g., vague, partially obscured, disconnected) visual stimuli; Flexibility of Closure (FC), the ability to identify a visual pattern embedded in a complex distracting pattern; and Perceptual Speed (PS), the ability to find a visual pattern in a complex pattern (Carroll, 1993). Yilmaz (2009) added three supplementary factors to Carroll’s factors, including Spatial Orientation (SO), the ability to imagine the appearance of objects from different perspectives; Spatial-Temporal (ST), the ability to judge the speed of moving stimuli and Wayfinding (WF) (Yılmaz, 2009). Uttal et al. (2013) proposed a comprehensive framework that considers two axes for classifying spatial abilities, including intrinsic–extrinsic and static-dynamic domains (Uttal et al., 2013). In this model, the intrinsic-static domain refers to perceiving spatial configurations aimed at distracting background information such as embedded figure tasks and flexibility of closure. The intrinsic-dynamic domain indicates the ability to piece different components together to make a more complex configuration. The extrinsic-static domain refers to understanding abstract spatial principles and extrinsic-dynamic domain is the visualization of a dynamic environment from a different position.
Spatial cognition in individuals with ADHD
Given the flow of information processing, impaired higher cognitive functions in individuals with ADHD could be followed in deficient basic perceptual processing (Mihali et al., 2018). The role of impaired lower perceptual functions in deficient higher cognitive functions has been found earlier in other neurodevelopmental disorders such as children with learning disorders (Yazdani et al., 2021) and autism spectrum disorders (Nejati, 2019); Nejati et al., 2021).
At the neural level, limited attentional resources should be managed for proper allocation to the environment. This management requires a strong interaction between executive (frontal lobe) and perceptual (parietal lobe) systems through the fronto-parietal brain network (Corbetta & Shulman, 2002). Neuroimaging studies have found that parietal lobes have a pivotal role in the psychopathology of ADHD (Schneider et al., 2010; Smith et al., 2006). In children with ADHD, the volume and metabolism of parietal lobes are lower than typically developing children (Castellanos et al., 2002). The superior parietal lobes show weaker activity during a selective attention task in children with ADHD than in typically developing children (Booth et al., 2007). Furthermore, neuroimaging studies have found that fronto-parietal functional connectivity is reduced in children (Kelly et al., 2007) and adults (Wolf et al., 2009) with ADHD. Beyond correlational studies, methylphenidate improves attention by increasing the activation of parietal-temporal, fronto-striatal, and fronto-cerebellar connectivity (Rubia et al., 2009). Furthermore, transcranial direct current stimulation over the posterior parietal cortex improves executive functions (EFs) in children with ADHD (Salehinejad et al., 2020a).
Current review
In the present study, we aimed to review impaired spatial abilities in individuals with ADHD. We tried to propose a model to explain ADHD impairments based on spatial disability.
Methods
Search strategy
Keywords related to spatial abilities were identified during the initial search through review articles. Then, systematic searches were conducted on Science Direct, PsycINFO, and PubMed, with no publication date limit. Keywords searched included “ADHD” OR “Attention Deficit-Hyperactivity Disorder” AND (“spatial ability” OR, “spatial skill” OR, “spatial perception” OR, “visual perception” OR, “mental rotation” OR, “spatial relation” OR, “flexibility of closure” OR, “closure speed” OR “perceptual speed” OR, “spatial orientation” OR, “visualization” OR, “spatial-temporal” OR, “wayfinding”). Each keyword was also searched separately. Additional searches were also performed in Google Scholar. Only publications in English were included.
Selection criteria
Two independent reviewers (SK and FM) initially selected articles based on titles and abstracts. Then SK removed duplications and integrated search results. Full-text articles were assessed for eligibility by another reviewer (VN). Figure 1 shows the PRISMA diagram. PRISMA diagram.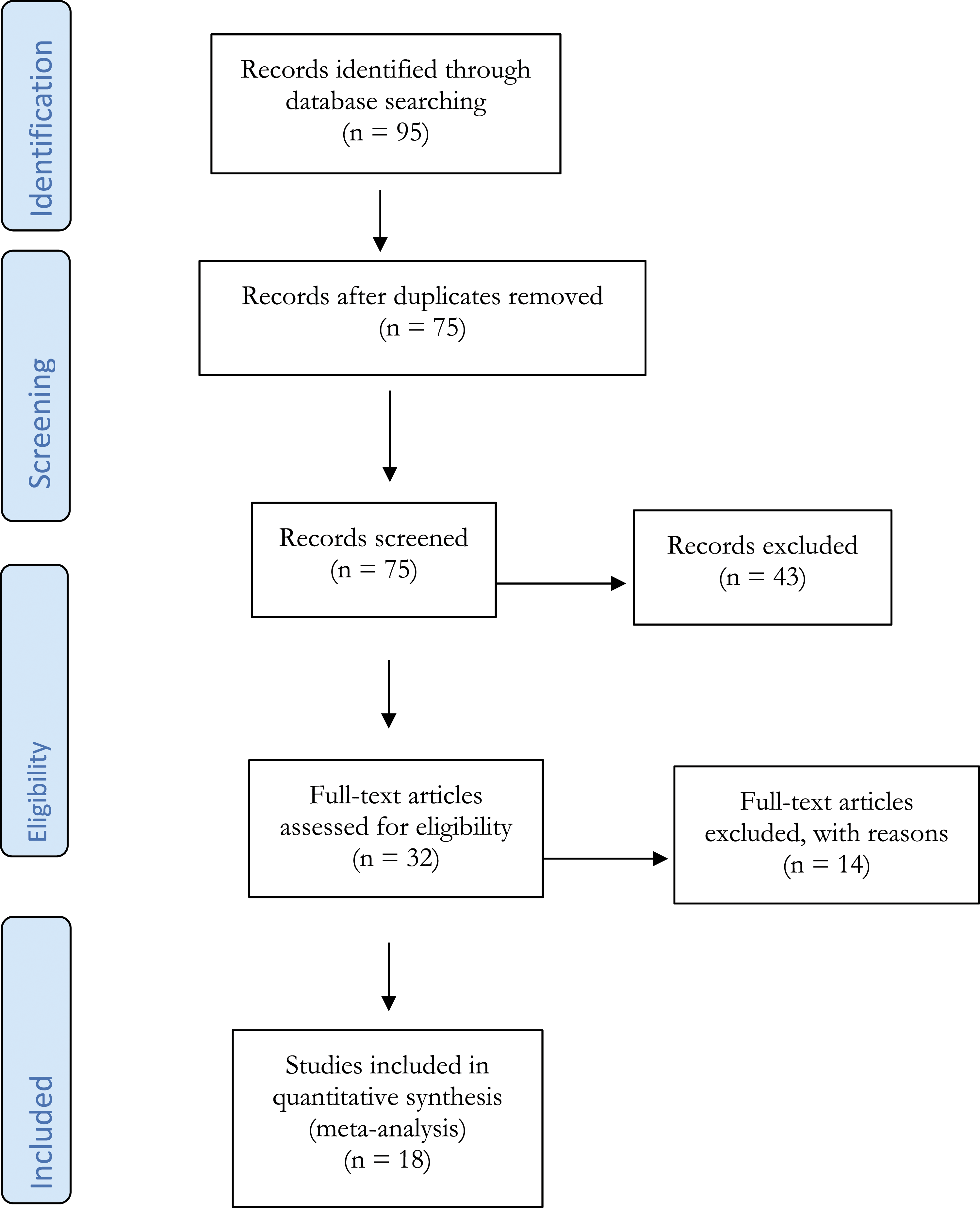
Studies were identified as eligible if the following inclusion criteria were met: (1) studies which included assessments of spatial abilities, (2) studies with participants with ADHD or attention problems, (3) studies with neuropsychological tasks.
Data extraction and analysis
The outcome was tasks performed in each study. These tasks were the Test of Visual Perceptual Skills-Third Edition (TVPS-III), the Developmental Test of Visual Perception (DTVP-2), the Wechsler Adult Intelligence Scale- Fourth Edition (WAIS-IV), Line Bisection Tests (LBT), Frostig Developmental Test of Visual Perception (FDTVP), Mental Rotation Tasks (MRT), block design subtest of the Wechsler Intelligence Scale for Children-revised (WISC-R), Visuospatial Processing Speed Task (VPST), Computerized Block Design Task (CBDT), modified Block Design Task (BDT), the Aptitude Test for School Beginners (ASB), Large-Scale Spatial Navigation (Corridor task, Route learning task, landmark recall task, naming task, route learning task), a series of movements to determine temporal and spatial difficulties, Sensory Integration and Praxis Tests (SIPT), the design copying subtest of NEPSY-II, the A’TEST, Judgment of Line Orientation (JLO), Developmental Test of Visual-Motor Integration (DTVMI) and visual tracking.
Two independent reviewers (SK and FM) extracted data from each study by using an excel spreadsheet. The summary statistics included in most of the studies were the number of participants in the control and test groups, mean age, and standard deviations (SDs).
Risk of bias
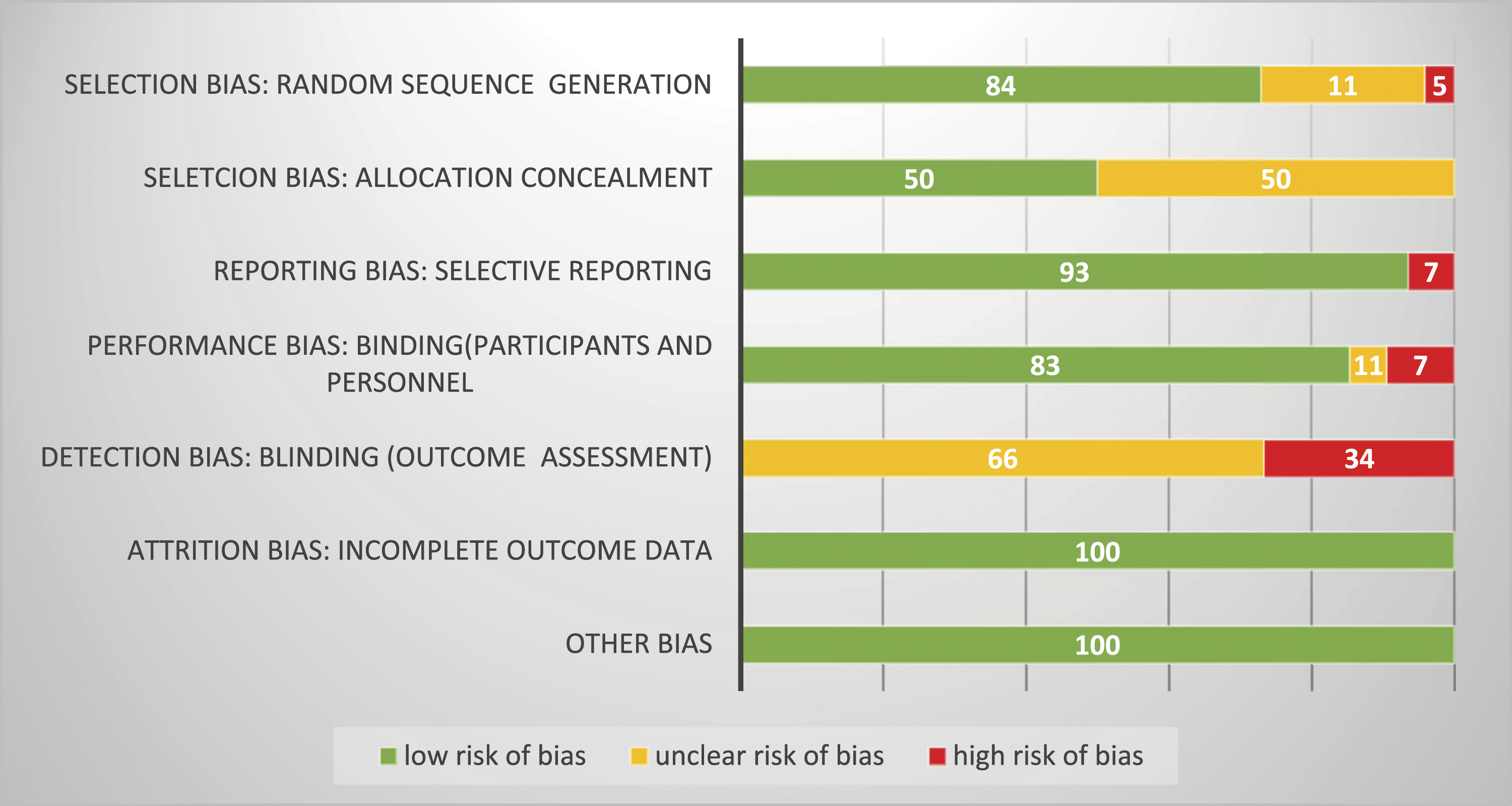
The Cochrane Collaboration tool was used to assess the risk of bias in each study (Higgins et al., 2011). The authors judged the risk of selection bias, performance bias, detection bias, attrition bias, reporting bias, and other biases. The final judgment is displayed in Figures 2 and 3. The risk of bias was categorized as low, high, and uncertain. Risk of bias assessment. Abbreviation: RSG: random sequence generation, AC: allocation concealment, SR: selective reporting, PB: participants and personnel binding OB: outcome assessment blinding, IO: incomplete outcome data, O: other biases. Bias assessment of included studies using the Cochrane risk of bias tool.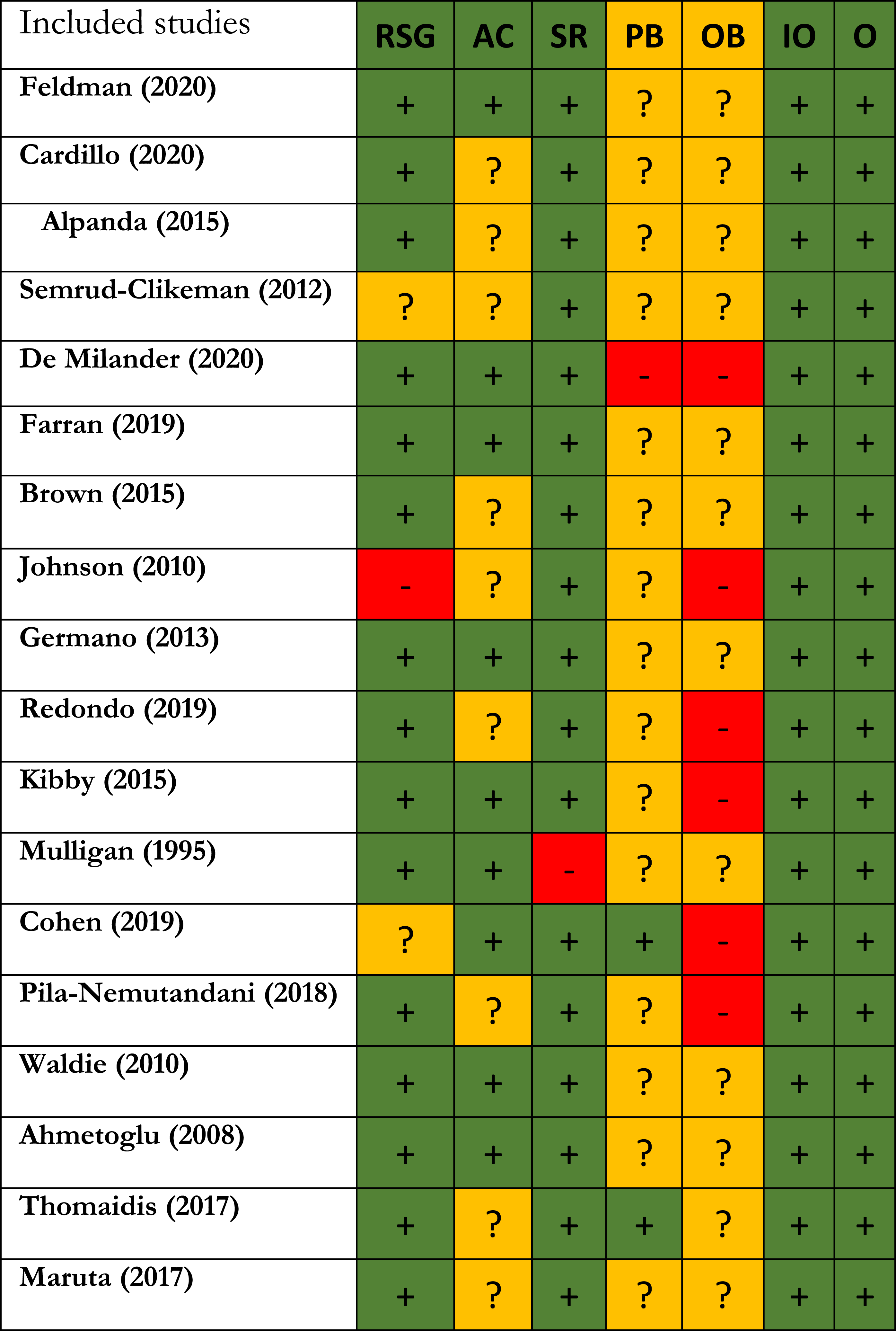
Results
Included studies
Eighteen studies were included in the review, which evaluated 7204 participants in total, 1402 participants with ADHD, 40 participants with autism spectrum, 21 participants with non-verbal learning disability, 20 participants with Williams syndrome, 51 participants with reading disorder, 51 participants with reading disorder comorbid with ADHD, 9 participants with developmental dyslexia, 15 participants with ADHD comorbid with other disorders and 5613 healthy controls. Sample sizes ranged from 36 to 4480. Out of the 18 studies, 12 studies used 2-group comparison, 4 used 3-group comparison, and 2 used 4-group comparison.
Out of the 18 studies, two studies used the Test of Visual Perceptual Skills-Third Edition (TVPS-III), two studies used the Judgment of Line Orientation (JLO), and two studies used the Wechsler Adult Intelligence Scale- Fourth Edition (WAIS-IV). The following tests and tasks were each used only once: Developmental Test of Visual Perception (DTVP-2), Frostig Developmental Test of Visual Perception (FDTVP), Mental Rotation Tasks (MRT), block design subtest of the Wechsler Intelligence Scale for Children-revised (WISC-R), one Line Bisection Tests (LBT), Visuospatial Processing Speed Task (VPST), Computerized Block Design Task (CBDT), modified Block Design Task (BDT), the Aptitude Test for School Beginners (ASB), Large-Scale Spatial Navigation (Corridor task, Route learning task, landmark recall task, naming task, route learning task), a series of movements to determine temporal and spatial difficulties, Sensory Integration and Praxis Tests (SIPT), the design copying subtest of NEPSY-II, the A′ TEST, Developmental Test of Visual-Motor Integration (DTVMI) and visual tracking.
In the reviewed studies, two studies utilized the Test of Visual Perceptual Skills-Third Edition (TVPS-III) and found children with ADHD had worse performance in visual-spatial relationships (Redondo et al., 2019), no difference in visual discrimination (Kibby et al., 2015; Redondo et al., 2019), visual memory (Kibby et al., 2015; Redondo et al., 2019), visual closure (Redondo et al., 2019) and visual figure-ground (Redondo et al., 2019).
Two studies used the Wechsler Adult Intelligence Scale- Fourth Edition (WAIS-IV) and found no difference in the Matrix Reasoning subtest among adults with and without ADHD (Brown et al., 2015; Cohen & Kalanthroff, 2019). Moreover, one study found that adults with ADHD performed better in picture completion and block design subtests, indicating no deficits in visuo-spatial abilities (Cohen & Kalanthroff, 2019). One study used the block design subtest of the Wechsler Intelligence Scale for Children-revised (WISC-R) and found that children with ADHD did not differ significantly from TD in terms of visual-spatial configuration (Alpanda, 2015). There was a significant difference regarding the time period of visual-spatial configuration (ADHD used less time).
Two studies used Judgment of Line Orientation (JLO), and one found no difference among children with and without ADHD, indicating no deficits in spatial abilities among ADHD children (Semrud-Clikeman, 2012), while the other found poorer performance in children with ADHD (Alpanda, 2015). The former study also used the Developmental Test of Visual-Motor Integration (DTVMI) and found poorer performance of children with ADHD regarding visual motor integration (Semrud-Clikeman, 2012).
One study used the Developmental Test of Visual Perception (DTVP-2) and found that children with ADHD performed weaker in the subtest of spatial position, visual closure, and visual-motor speed (Germano et al., 2013). Another study used the Frostig Developmental Test of Visual Perception (FDTVP) and found weaker hand-eye coordination and constancy of shape (Ahmetoglu et al., 2008). No difference was found between ADHD groups and control in spatial relationships (Ahmetoglu et al., 2008; Germano et al., 2013)position in space (Ahmetoglu et al., 2008), figure-ground perception (Ahmetoglu et al., 2008; Germano et al., 2013), constancy of form (Germano et al., 2013) and copy (Germano et al., 2013).
One study used Line Bisection Tests (LBT) and found rightward bias in children with ADHD (Waldie & Hausmann, 2010). Another study used Mental Rotation Tasks (MRT) and found no difference in the mean response time among children with and without ADHD, indicating no evidence of a specific spatial processing/mental rotation deficit in ADHD (Feldman & Huang-Pollock, 2020). One study used Visuospatial Processing Speed Task (VPST) and found that children with ADHD displayed less visuospatial processing speed. Moreover, no statistically significant difference was found between ADHD and TD regarding visuo-perceptual abilities, as measured by the Computerized Block Design Task (CBDT). Lastly, using the modified Block Design Task (BDT), the study concluded that children with ADHD performed less well in visuo-constructive abilities (Cardillo et al., 2020).
One study used the Aptitude test for School Beginners (ASB) and found no significant difference in visuo-spatial rotation among children with and without ADHD (de Milander et al., 2020). Large-scale spatial navigation tasks revealed no deficits in large-scale spatial cognition among children with ADHD (Farran et al., 2019). Another study used a series of movements to determine temporal and spatial difficulties and concluded no difference in temporal ability. However, the study found that children with ADHD demonstrated spatial difficulty in movement control in the rightwards direction (K. Johnson et al., 2010). Another study used the Sensory Integration and Praxis Tests (SIPT) and showed worse performance of children with ADHD in space visualization, design copy, and post-rotary nystagmus (Mulligan, 1996).
Characterstics of reviewed study and summary of results.

Note. ADHD: attention-deficit/hyperactivity disorder, TD: Typical development, ODD: Oppositional Defiant Disorder, CD: Conduct disorder, GAD: General anxiety disorder, MDD: Major depressive disorder, DD: Dyslexia disorder, LD: Learning disability, SPD: Sensory processing disorder, PDD: Pervasive developmental disorder, RD: Reading disorder, ASD: Autism disorder, AS = Asperger syndrome, SCP: Social communication disorder, OCD: Obsessive compulsive disorder, C: Combined, AD: Attention deficit, HI: Hyperactive/Impulsive, ED: emotional disturbance, ANX: anxiety, motor disabilities, SD: sleep disorders.
Discussion
The results of the included studies in this systematic review showed heterogeneous findings in different factors of spatial abilities. We discussed these results with respect to presumably relevant factors, including factors, domains, tasks, and measures of spatial ability. Furthermore, other potential factors such as comorbidities, age, and gender of participants were discussed.
Relevance of factors and domains of spatial ability
The results could be discussed at three levels: spatial ability as a global construct, spatial factors, and spatial domains. With respect to spatial ability as a global construct, 15 out of 18 included studies found impairment, in at least one spatial factor, in individuals with ADHD. Three studies found no differences between individuals with and without ADHD in spatial ability. These studies used a subscale of Aptitude test for School Beginners (ASB) (Brown et al., 2015; de Milander et al., 2020; Feldman & Huang-Pollock, 2020; Kibby et al., 2019), visual discrimination subtest of Test of Visual Perceptual Skills-Revised (TVPS-R) (Brown et al., 2015; de Milander et al., 2020; Feldman & Huang-Pollock, 2020; Kibby et al., 2019) and matrix reasoning subtest of Weschler adult intelligence test IV (Brown et al., 2015; de Milander et al., 2020; Feldman & Huang-Pollock, 2020; Kibby et al., 2019). As the studies mentioned above do not cover all factors/domains of spatial ability, we may conclude that spatial ability as a global construct is impaired in individuals with ADHD.
Given the spatial factors, the results are mixed. Spatial relation/rotation in individuals with ADHD was worse (Alpanda, 2015; Germano et al., 2013; Mulligan, 1996; Redondo et al., 2019; Waldie & Hausmann, 2010), similar (Ahmetoglu et al., 2008; Alpanda, 2015; de Milander et al., 2020; Feldman & Huang-Pollock, 2020; Germano et al., 2013; Semrud-Clikeman, 2012), or better (Cohen & Kalanthroff, 2019), compared to typically developing control. Visualization in individuals with ADHD was worse (Ahmetoglu et al., 2008; Cardillo et al., 2020; K. Johnson et al., 2010; Mulligan, 1996; Pila-Nemutandani et al., 2018), similar (Cardillo et al., 2020; Germano et al., 2013; K. Johnson et al., 2010), or better (Cohen & Kalanthroff, 2019) than typically developing children. No difference was found between individuals with and without ADHD in figure-ground perception (Ahmetoglu et al., 2008; Germano et al., 2013; Mulligan, 1996; Redondo et al., 2019), form constancy factor (Brown et al., 2015; Cohen & Kalanthroff, 2019; Germano et al., 2013; Redondo et al., 2019) and visual discrimination (Kibby et al., 2015; Redondo et al., 2019). Individuals with ADHD had lower performance in spatiotemporal factors compared to a healthy control group. At the level of spatial factors, we cannot present a clear profile for individuals with ADHD.
With a dimensional perspective, the results are more impressive. In the static-internal domain, measured by form constancy, visual discrimination, and matrix reasoning tasks, individuals with and without ADHD had similar performance (Ahmetoglu et al., 2008; Brown et al., 2015; Cohen & Kalanthroff, 2019; Germano et al., 2013; Kibby et al., 2015; Mulligan, 1996; Redondo et al., 2019). Similarly, in the static-external domain, measured by figure-ground task, the performance of individuals with ADHD remained intact (Ahmetoglu et al., 2008; Germano et al., 2013; Mulligan, 1996; Redondo et al., 2019). The dynamic-external domain, measured by spatiotemporal tasks, was impaired in individuals with ADHD (Maruta et al., 2017). The dynamic-internal domain, measured by spatial orientation/relation/rotation and visuo-constrictive/perceptual/motor tasks, revealed heterogeneity of results with impaired or intact performance in individuals with ADHD (Ahmetoglu et al., 2008; Alpanda, 2015; Cardillo et al., 2020; de Milander et al., 2020; Feldman & Huang-Pollock, 2020; Germano et al., 2013; K. Johnson et al., 2010; Mulligan, 1996; Pila-Nemutandani et al., 2018; Redondo et al., 2019; Semrud-Clikeman, 2012; Waldie & Hausmann, 2010).
Spatial dimensions could be placed in a spectrum based on perceptual or cognitive demand (Figure 4). In detail, the domain could be placed as internal-static, internal-dynamic, external-static, and external-dynamic, from perceptual to cognitive pole in order. The impaired spatial abilities in children with ADHD were related to the cognitive pole of the spectrum of spatial dimensions. The impaired EFs in individuals with ADHD (Barkley, 1997) could explain this impairment. Notwithstanding the direction, bottom-up or top-down, the spatial and cognitive impairments in children with ADHD are associated with and have influence on each other. Spatial domains and respective supported higher cognitive function.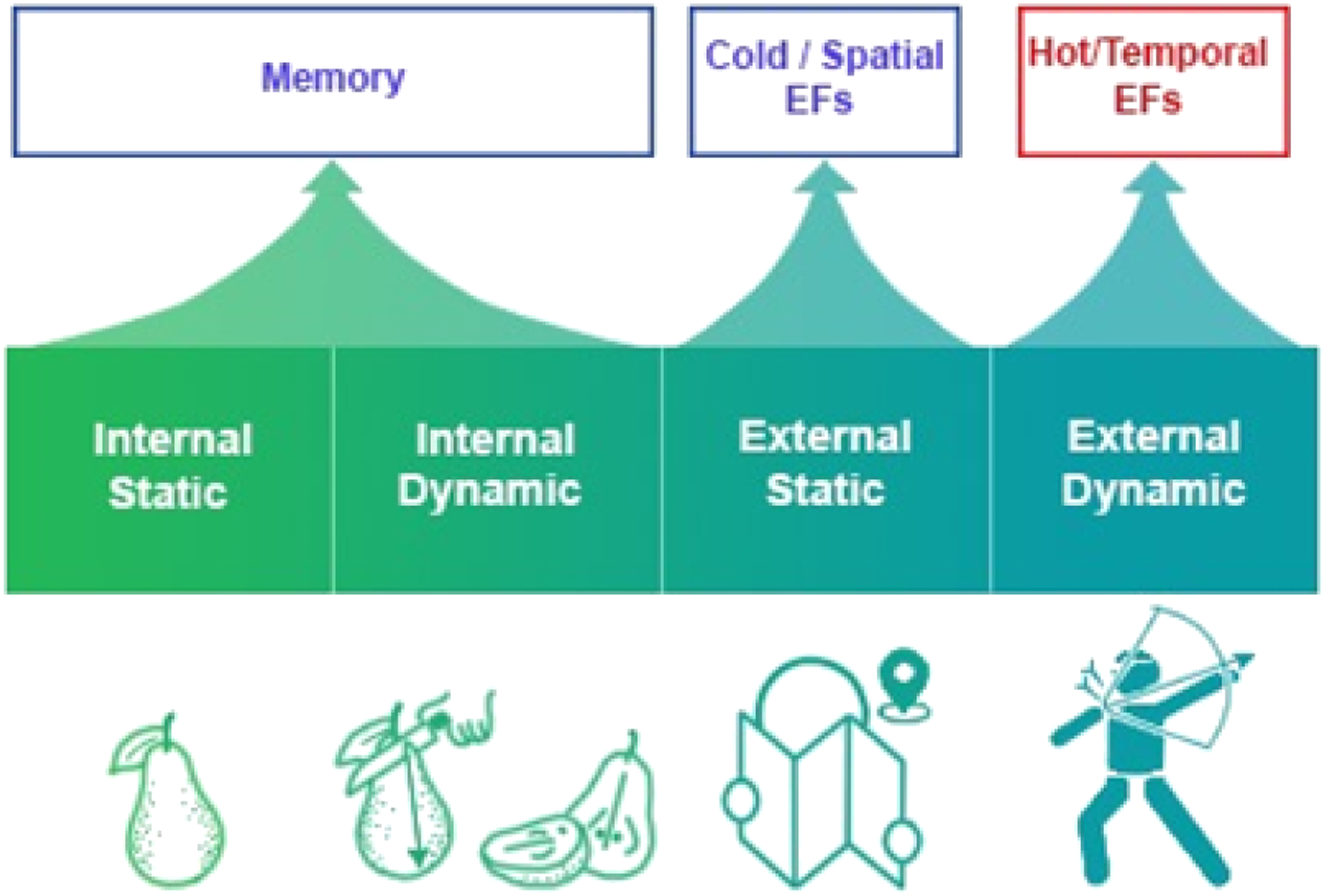
The relevance of tasks and measures
In the reviewed studies, 14 tests (25 subscales) were used to evaluate spatial abilities in individuals with and without ADHD. The heterogeneity of the tests that assess different factors should be taken into account as a limitation. For instance, in the visuo-spatial factor, two types of Block Design test, classic (Cohen & Kalanthroff, 2019) and computerized (Cardillo et al., 2020), were used with different levels of complexity. Similarly, in visuo-spatial factor, one test was based on drawing a complex geometric design, requiring precise hand movements (Semrud-Clikeman, 2012), while the other tests required mental transformation of given figures without motor demand (de Milander et al., 2020; Feldman & Huang-Pollock, 2020). Although the spatial factors of these tasks are similar, different motor demands of the tasks make it difficult to compare their results.
Furthermore, the main measures of the tests are different in regard to accuracy and/or speed. There is a trade-off between accuracy and speed, the accuracy of an action varies with its speed (Woodworth, 1899). Speed and accuracy provide two sources of information in cognitive tasks; speed provides an index of the accessibility of an item, whereas accuracy reflects the availability of an item (McElree, 2001). In the reviewed studies, Redondo et al. (2019) found worse accuracy but better speed in visuo-spatial ability in children with ADHD than in typically developing children.
Notwithstanding the outcome measure, the pattern of responding provides additional information, especially in children with ADHD, which shows variable performance across tasks (Nejati et al., 2022). One method to discover the pattern of responding is mathematical modeling on the accuracy and the speed of responses. One reviewed study in children with ADHD used Drift Diffusion Modeling (DDM) and found different patterns of responding to mental rotation tasks in children with ADHD. This study found similar performance accuracy as a conventional measure but greater variance and higher error rate as DDM measures in children with ADHD (Feldman & Huang-Pollock, 2020).
The relevance of comorbidity
Six out of the 18 studies excluded comorbid disorders (Ahmetoglu et al., 2008; Brown et al., 2015; Cardillo et al., 2020; Germano et al., 2013; Maruta et al., 2017; Pila-Nemutandani et al., 2018), nine studies had ADHD children with at least one comorbidity (Farran et al., 2019; Feldman & Huang-Pollock, 2020; K. Johnson et al., 2010; Kibby et al., 2015; Mulligan, 1996; Redondo et al., 2019; Semrud-Clikeman, 2012; Thomaidis et al., 2017; Waldie & Hausmann, 2010), and three studies are silent about comorbidities (Alpanda, 2015; Cohen & Kalanthroff, 2019; de Milander et al., 2020). Given the results, the variety of the tasks and results did not permit us to obtain a solid conclusion about the role of heterogeneity in the results. One included study evaluating the role of comorbidities, compared ADHD children with and without comorbidity with typically developing children, and found spatial impairments to be more prominent in ADHD children with comorbidities (Redondo et al., 2019).
The relevance of age and gender
Based on Piaget’s developmental theory, spatial abilities develop around the age of 12 (Piaget, 1956). Some other pioneers state that spatial abilities reach the adulthood level at the age of 9–10 (Levine et al., 1999). Notably, males advantage in spatial ability appear by age 10 and remain constant through age 18 (E. S. Johnson & Meade, 1987). ADHD is a psychiatric disorder in children, and its persistence rate to adulthood is 32% (Faraone et al., 2004). Taken together, research has demonstrated that spatial abilities tend to improve with age, while the prevalence of ADHD tends to decrease with age. This can be explained by the possible relationship between improved perceptual/spatial abilities and the development of ADHD. Two included studies performed on adults with ADHD found intact form constancy (Brown et al., 2015) but impaired visuo-temporal performance (Maruta et al., 2017) compared to controls. The pattern is similar to children with ADHD in the above-mentioned internal-static and external-dynamic demands.
With respect to gender differences, ADHD has a male-to-female ratio of approximately 4:1 (Cantwell, 1996; Ramtekkar et al., 2010). Furthermore, earlier accounts consider spatial ability as an inherently male ability (Levine et al., 2016; Wang, 2020). In the present study, four out of the 18 included studies evaluated gender differences in spatial ability and found similar performance in boys and girls with ADHD (Alpanda, 2015; Pila-Nemutandani et al., 2018) or better performance in girls with ADHD (Ahmetoglu et al., 2008; Thomaidis et al., 2017). However, Alpanda (2015) found faster responses to visuo-spatial tests in boys with ADHD, explaining the lower accuracy based on the speed-accuracy trade-off. In sum, the male superiority in spatial ability was not found in individuals with ADHD. Previous meta-analyses of various spatial ability tests have found substantial gender disparities in the results of the mental rotation test, which is not a suitable indicator of all aspects of spatial ability (Bartlett & Camba, 2023).
Toward a spatial theory of ADHD
Spatial ability as early perceptual processing plays a key role in several higher cognitive functions such as learning and memory (Denis & Loomis, 2007), cold EFs such as working memory, cognitive flexibility, and inhibitory control (Miyake et al., 2001), hot EFs such as time perception (Riemer et al., 2016), and empathy (Lamm et al., 2007). We can classify cognitive functions in two categories: Early/basic perceptual and late/higher cognitive, rooted in perceptual processing. Different domains of spatial ability underpin respective higher cognitive functions. Internal-static and internal-dynamic domains refer to a within object perception and classification, feed memory formation and storage. The external domains, indicating a between object perception, are required for executive functions. EFs are dynamic information processing functions that manipulate information. This leading position of EFs can be explained in the two static/spatial and dynamic/temporal domains. Static or spatial EFs lead to a broad perspective on information and form an abstraction from a dominant point of view. Dynamic or temporal EFs provide an opportunity to act and change the point of view dynamically based on prediction, anticipation, and expectation (Nejati & Yazdani, 2020). Spatial EFs, also called cold EFs, are impaired in individuals with ADHD based on (cold) executive theory (Barkley, 1997). Temporal EFs, also called hot EFs, including time perception and reward processing, are impaired in individuals with ADHD based on (hot) motivational theory (Sonuga-Barke et al., 1992). Spatial/cold EFs are rooted in the external-static domain, while temporal/hot EFs originate from the external-dynamic domain of spatial ability (Figure 4). Earlier accounts state that about half of the individuals with ADHD have intact cold EFs (Nigg et al., 2005; Willcutt et al., 2005), which is comparable to partial impairment in external-static domain of spatial ability based on our review (Figure 5). Cognitive theories of ADHD and respective cortical areas.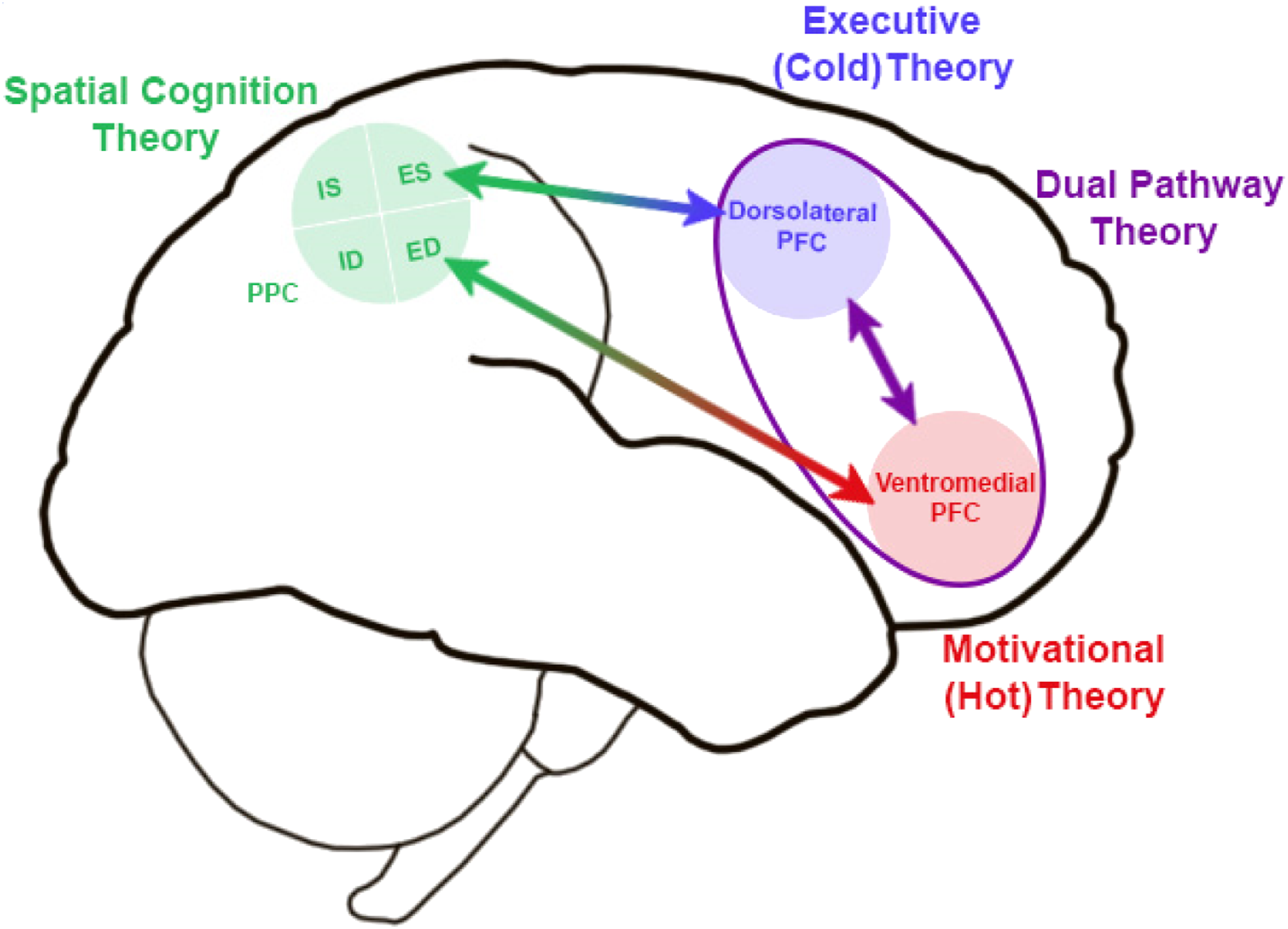
We can propose a spatial cognition theory of ADHD to explain the cognitive profile of individuals with ADHD by impaired spatial ability. None of the earlier theories, like the dysexecutive theory or the motivational theory, can explain the cognitive profile of individuals with ADHD (Nigg et al., 2005; Sonuga-Barke, 2003; Willcutt et al., 2005). Sonuaga-Bark (2003) proposed the dual pathway theory, which merges the two theories mentioned above, to explain the variety of cognitive profiles in individuals with ADHD. In the spatial cognition theory, we propose a common perceptual resource for both cold EFs, the dysexecutive theory, and hot EFs, the motivational theory. This perceptual resource has separate domains for cold and hot EFs, explaining different profiles in individuals with ADHD (Figure 4).
The proposed theory can be supported by earlier neuroimaging studies, which found the role of the parietal lobe in the psychopathology of ADHD (Schneider et al., 2010; Smith et al., 2006). Furthermore, the proposed interaction between spatial resources and higher cognitive functions could be explained by neuroimaging studies which found reduced functional connectivity in the fronto-parietal pathway in individuals with ADHD (Kelly et al., 2007) (Wolf et al., 2009).
Conclusion, limitation, and future directions
The present review found individuals with ADHD to have intact internal domains, partially impaired external-static domain, and impaired external-dynamic domain of spatial ability. Impaired EFs in individuals with ADHD can be explained through the impaired spatial domains, proposed as the spatial theory of ADHD. Some limitations should be taken into account for the present review study. The first one is the heterogeneity of the tasks used in the included studies. The variety of cognitive measures did not allow a meta-analysis of the results. Classifying the tests based on the spatial factors did not solve the problem to obtain a clear result, but the dimensional approach made an impressive conclusion. Another limitation is comorbidity of ADHD with other neurodevelopmental disorders, including ASD and SLD, with well-documented perceptual/spatial impairments.
Future studies can approach the spatial impairments of individuals with ADHD based on the proposed classification of the current study.
The impact of spatial training in the external-static and external-dynamic domains on the cold and hot EF could be investigated in future studies to provide experimental evidence for the proposed model.
Footnotes
Acknowledgements
V.N. conceptualized the study, and wrote the manuscript. S.K. and FM searched the database, and extracted results. This project was conducted by personal grant of the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.