
Abstract
Background
Knowledge of the continuity of sleep problems and the associations between sleep and psychiatric symptoms in child psychiatric patients is scarce.
Objectives
To investigate the persistency of sleep problems and how sleep at preschool age predicts sleep problems and psychiatric symptoms at school age in child psychiatric patients.
Methods
Participants (n = 68) were child psychiatry outpatients at Helsinki University Hospital in 2015–2017. Caregivers evaluated sleep with the Sleep Disturbance Scale for Children (SDSC) and psychiatric symptoms with the Child Behavior Checklist (CBCL) at baseline (age 4–7 years) and again at follow-up (age 8–13 years). Family background information was collected at both time points.
Results
Sleep problems at preschool age predicted sleep problems at school age (R2Adjusted = .48, p < .001). Persistent sleep problems associated strongly with the intensity of psychiatric symptoms (p = .001). Internalizing symptoms were predicted by sleep problems (p = .038) even after controlling for age, sex, and psychiatric symptoms at preschool age.
Conclusion
Sleep problems are prevalent and persistent and relate to psychiatric symptoms in children treated at child psychiatry clinics. These results emphasize the need for identification and treatment of sleep problems in these children.
Keywords
Introduction
Sleep has a significant role in healthy physical and mental development. It has particular importance for maturing brains, as it facilitates development of emotion regulation, behavioural control, and cognitive functions (Jiang, 2019; Kopasz et al., 2010). At population level, up to 40–45% of children experience sleep problems at least for brief periods (Kahn et al., 1989; Simola et al., 2012). Too short and poor-quality sleep have been associated with daytime fatigue, attention and short-term memory problems, language and learning difficulties, and emotional and behavioural problems (Huhdanpää et al., 2018; Paavonen et al., 2003; Simola et al., 2014; Steenari et al., 2003). Previous longitudinal studies with community samples of preschool and school-aged children reported sleep problems to predict later cognitive, psychosocial, and physical difficulties (Simola et al., 2014).
According to a Finnish epidemiological study, 35% of children having sleep problems at preschool age still had them at school age e.g. 9% had persistent sleep problems (Simola et al., 2012). Population-based studies have reported persistent sleep problems to affect children’s mental health far more adversely than short-term sleep problems, and to significantly increase the risks for a wide range of psychosocial difficulties (Quach et al., 2009; Simola et al., 2014).
Child psychiatric patients have been reported to have more sleep problems (Aronen et al., 2014; Huhdanpää et al., 2018; Ivanenko et al., 2004, 2006) and shorter sleep duration (Huhdanpää et al., 2018) than children in community samples. Child psychiatric patients with sleep problems also have more psychiatric symptoms than patients without sleep problems (Huhdanpää et al., 2018; Ivanenko et al., 2004, 2006). Child psychiatric patients can be even more vulnerable to the effects of sleep problems on brain maturation and psychiatric symptoms than normative children (Huhdanpää et al., 2018; Ivanenko et al., 2004, 2006).
Although research shows an evident relationship between children’s sleep and emotional and behavioural development and suggests a bidirectional relationship between sleep difficulties and psychiatric symptoms (Kahn et al., 2013; Steinsbekk & Wichstrøm, 2015), longitudinal studies among child psychiatric patients are rare. The frequency of persistent sleep problems and their association with psychiatric symptoms in child psychiatric patients remain poorly known. Longitudinal studies on sleep in child psychiatric patients are warranted to examine whether sleep problems predict later psychiatric symptoms in clinical samples. A deeper knowledge of sleep problems’ continuity and the relation to the intensity of psychiatric symptoms would be beneficial and may help in developing more accurate treatments for child psychiatric patients in the future.
The aims of this follow-up study of young child psychiatric patients were to investigate (1) the persistency of sleep problems, (2) how preschool age sleep problems predict sleep quality at school age and (3) how they relate to and predict psychiatric symptoms at school age.
Subjects and Methods
Subjects
The baseline sample was recruited from child psychiatric outpatient clinics at Helsinki University Hospital (Helsinki and Vantaa) between March 2015 and May 2017. The inclusion criteria for the children in the baseline sample were (1) age 4–7 years, (2) Finnish-speaking parents, and (3) in daycare(Huhdanpää et al., 2018) .
Data for the follow-up were collected between January 2021 and June 2021. Sixty-nine families of the baseline sample (n = 176) attended the follow-up.
Address for the baseline families for follow-up was collected from the Digital and Population Data Services Agency in Finland. Addresses were available for 171 of 176 participants. Contact letters and questionnaires were sent to the families, and they were reminded up to three times in case they did not reply. Of the 171 families, 5 families declined participation. The response rate at the follow-up was 40.4% (n = 69). One case was excluded due to incompletely filled questionnaires with over half of the answers missing.
The follow-up respondents (n = 68) did not differ in a Chi-square test from non-respondents (n = 108) in their demographic characteristics (age, sex, parental educational level, living situation (all p-values > .05)) or in their baseline psychiatric symptoms (CBCL total score) (p = .299) or sleep problems (SDSC total score) (p = .375), being above clinical cut-off points.
Measures
Background information
A background questionnaire was given at both baseline (T1) and follow-up (T2). At both times, caregivers reported children’s age and sex, and parents’ educational level. At T1, caregivers reported children’s home language and history of living in/outside Finland. Information on children’s family structure, daycare, and medication was collected from medical records. At T2, questions regarding children’s school form, living situation, health care contact, medication, and family’s support from social services were included in the background questionnaire.
Sleep
Sleep Disturbance Scale for Children (SDSC) (Bruni et al., 1996)was used to comprehensively assess children’s sleep problems at T1 and T2. Caregivers filled out the questionnaires consisting of 26 items on sleep over the last 6 months. The first two questions were about sleep duration and latency, and the remaining questions were answered on a 5-point Likert scale (1, never; 2, occasionally (1–2 times a month); 3, sometimes (1–2 times a week); 4, often (3–5 times a week); 5, always (daily)). The total score reflects general sleep problems and is the sum of 6 subscales: (1) Disorders of Initiating and Maintaining Sleep, (2) Sleep Breathing Disorders, (3) Disorders of Arousal, Nightmares, (4) Sleep–Wake Transition Disorders, (5) Disorders of Excessive Somnolence, and (6) Sleep Hyperhidrosis. A total score of 46 points or more was used as a cut-off point for clinical sleep problems in the present study, similarly to the studies by Simola et al. (2012) and Huhdanpää et al. (2018).
Psychiatric symptoms
Caregivers filled out the standardized ASEBA Child Behavior Checklist (CBCL) form. Versions for preschool (CBCL/1½-5) and school-aged children (CBCL/6–18) were used at T1 and T2, respectively. The questionnaires comprise 100 and 113 items, respectively, scored on a 3-point Likert scale (0, not true; 1, somewhat or sometimes true; 2, very true or often true). Both CBCL versions include narrowband symptom scales that combine into externalizing and internalizing problem broadband scales and a total problem score (Achenbach & Rescorla, 2000). ASEBA-web system was used to score the CBCL and to obtain standardized T-scores based on ASEBAs multicultural population norms. The T-scores describe the severity of the psychiatric symptoms and include cut-off points for subclinical (score 60–62) and clinical (score >= 63) ranges for total, internalizing, and externalizing scales.
Data analysis
Software
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 25 (IBM Corp., Armonk, NY, USA). For drawing graphs, R version 3.6.1 (R Core Team, 2019), RStudio version 1.2.1578 (RStudio Team, 2019), and the packages ggplot2 (Wickham, 2016) and cowplot (Claus O, 2020) were used.
Variables
Summary variables were formed for analyses. A variable describing both parents’ educational level was formed from the highest educational level reported. Education level was classified in the following categories: high (‘higher academic degree’ or ‘licentiate/doctor’), intermediate (‘lower academic degree’ or ‘some college’), and low (‘less than some college’ or ‘no further education’).
Categories from the background questionnaire’s living situation were partially combined to form a new variable with categories ‘living with both biological parents’, ‘living with only mother or father’, ‘living in turn with both parents’, and ‘living in placement’ (e.g. foster care or children’s home).
To examine associations between persistency of sleep problems and psychiatric symptoms, children were divided into three groups according to the clinical cut-off point for SDSC total score: (1) ‘no sleep problems’, no sleep problems at either time point; (2) ‘temporary sleep problems’, sleep problems at either T1 or T2; and (3) ‘persistent sleep problems’, sleep problems at both time points.
Covariates
For covariates, we selected variables that have been associated with sleep difficulties or psychiatric symptoms in previous studies (Bai et al., 2020; Calhoun et al., 2014; Kahn et al., 1989; Kronholm et al., 2015; Quach et al., 2009; Rubens et al., 2016; Simola et al., 2012), along with the background variables correlating significantly with sleep and/or psychiatric variables in this sample. The chosen covariates were child’s age (at T2), sex (0 = female, 1 = male), parents’ educational level (at T2), and baseline CBCL psychiatric symptoms.
Statistical analysis
To investigate the continuity of sleep problems, SDSC total scores and subscale scores at T1 and T2 were compared using paired samples Student’s t-test. Analysis of Variance and Tukey’s Honestly Significant Difference (HSD) were used to compare the levels of psychiatric symptoms between the three sleep problem groups. Whether sleep problems at preschool predict sleep problems at school age was investigated with multiple linear regression, where T1 SDSC total score predicted T2 SDSC total score. To investigate associations between sleep problems and psychiatric symptoms, separate multiple regression analyses were conducted. In each model, T1 SDSC total score predicted either CBCL total score, CBCL internalizing score, or CBCL externalizing score at T2. Three separate regression models were created for each. The non-adjusted models included only the two variables of interest. The partially adjusted models included child’s age, sex, and T1 CBCL total score, and the fully adjusted models further included parents’ educational level.
Results
Descriptive data
Demographic information of children, family, school, service use, and medication at Time 2 (n = 68).
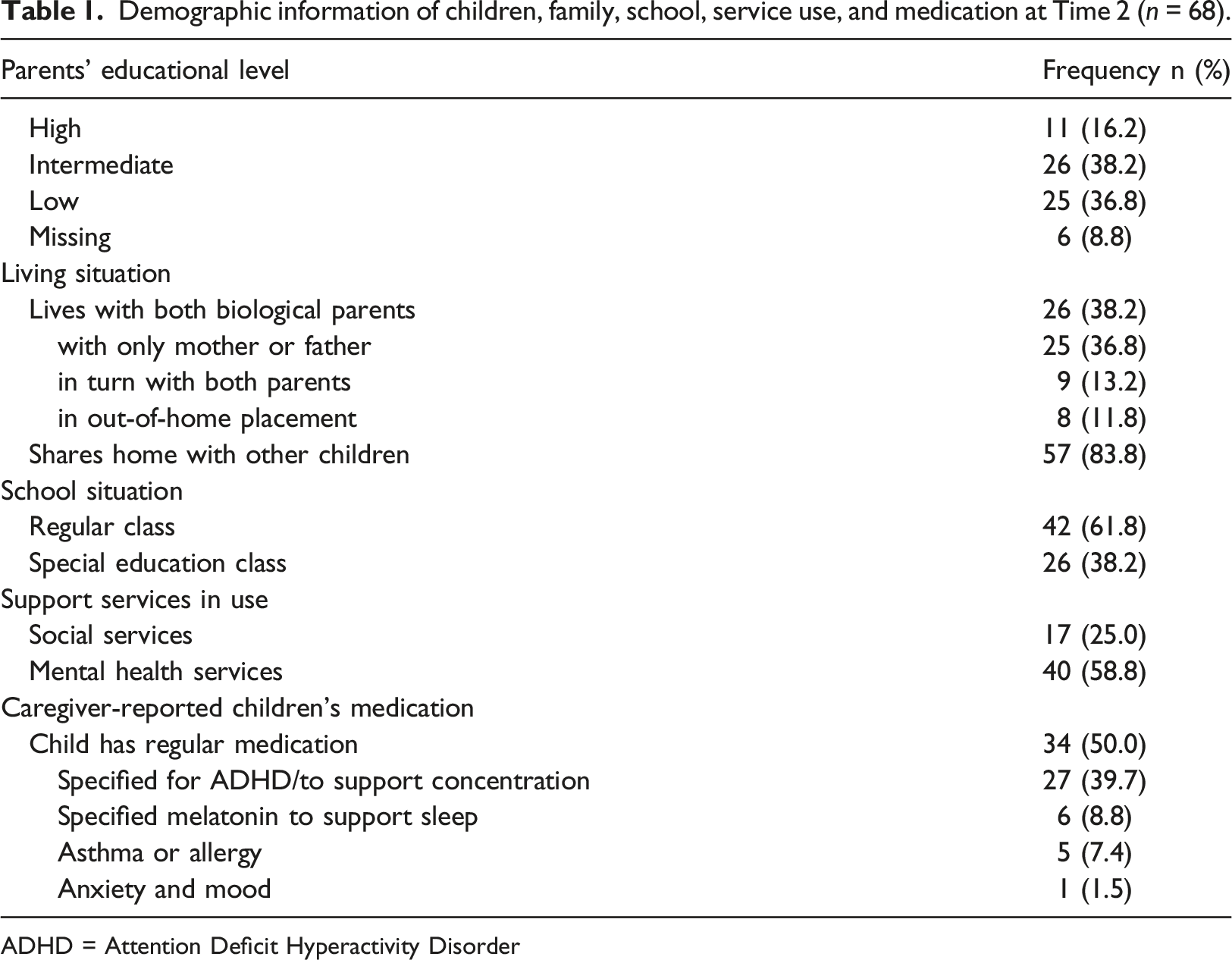
ADHD = Attention Deficit Hyperactivity Disorder
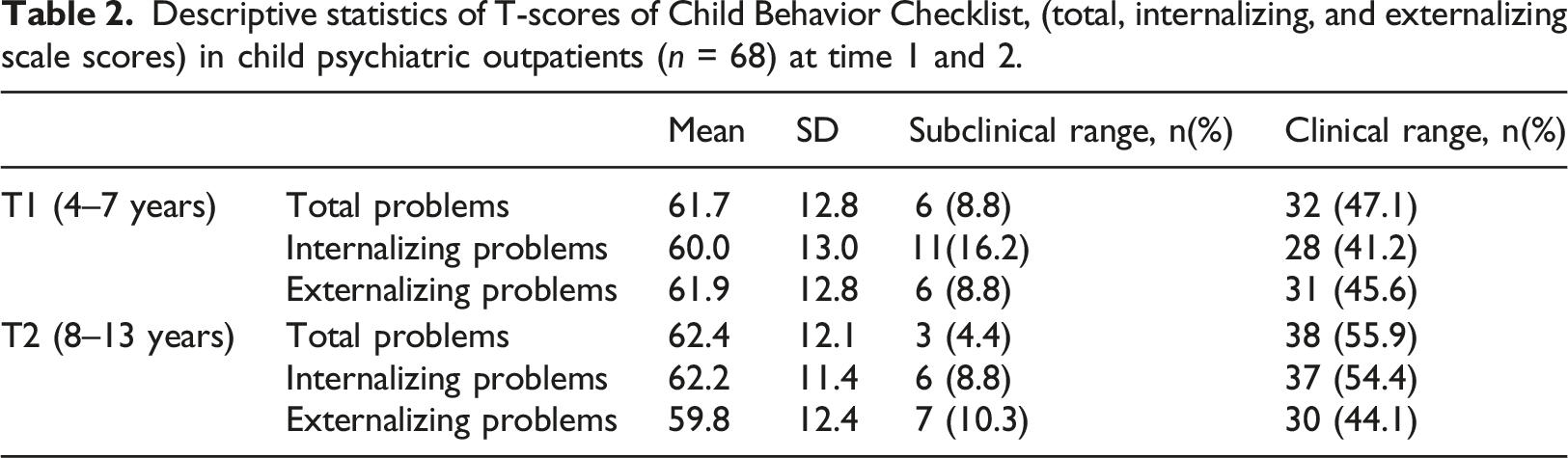
Descriptive statistics of T-scores of Child Behavior Checklist, (total, internalizing, and externalizing scale scores) in child psychiatric outpatients (n = 68) at time 1 and 2.
Sleep
Characteristics of sleep and frequency of sleep problems at Time 2
According to SDSC, 22 (32.4%) of the children had sleep problems at T2 (clinical cut-off point total score ≥ 46). Caregiver-reported average sleep duration per night was 9–11 hours for 37.7%, 8–9 hours for 47.1%, 7–8 hours for 13.2%, and 5–7 hours for 1.5% of the children.
Persistence of sleep problems from preschool to school age
Of the children (n = 68), 37 (54.4%) did not have sleep problems at either time point, 15 (22.1%) had sleep problems at either T1 or T2, and 16 (23.5%) had sleep problems at both time points. Thus, 64% of the children who had sleep problems at T1 still had them at T2.
Figure 1 shows the continuity of sleep problems in our sample. In total, 23.5% (n = 16) of the children had persistent sleep problems. Occurrence and course of sleep problems from preschool to school age (Sleep problems defined as SDSC Total score ≥ 46).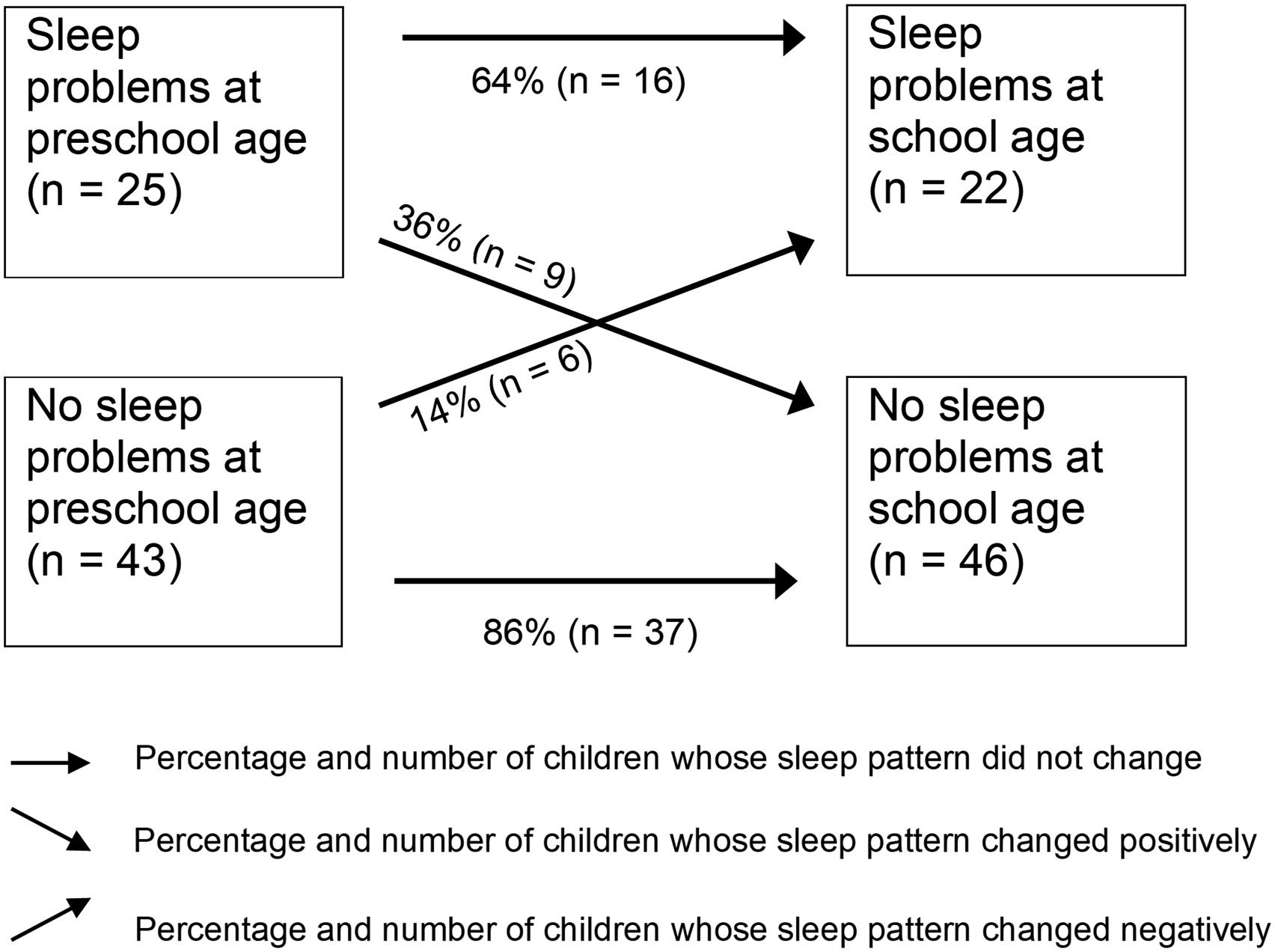
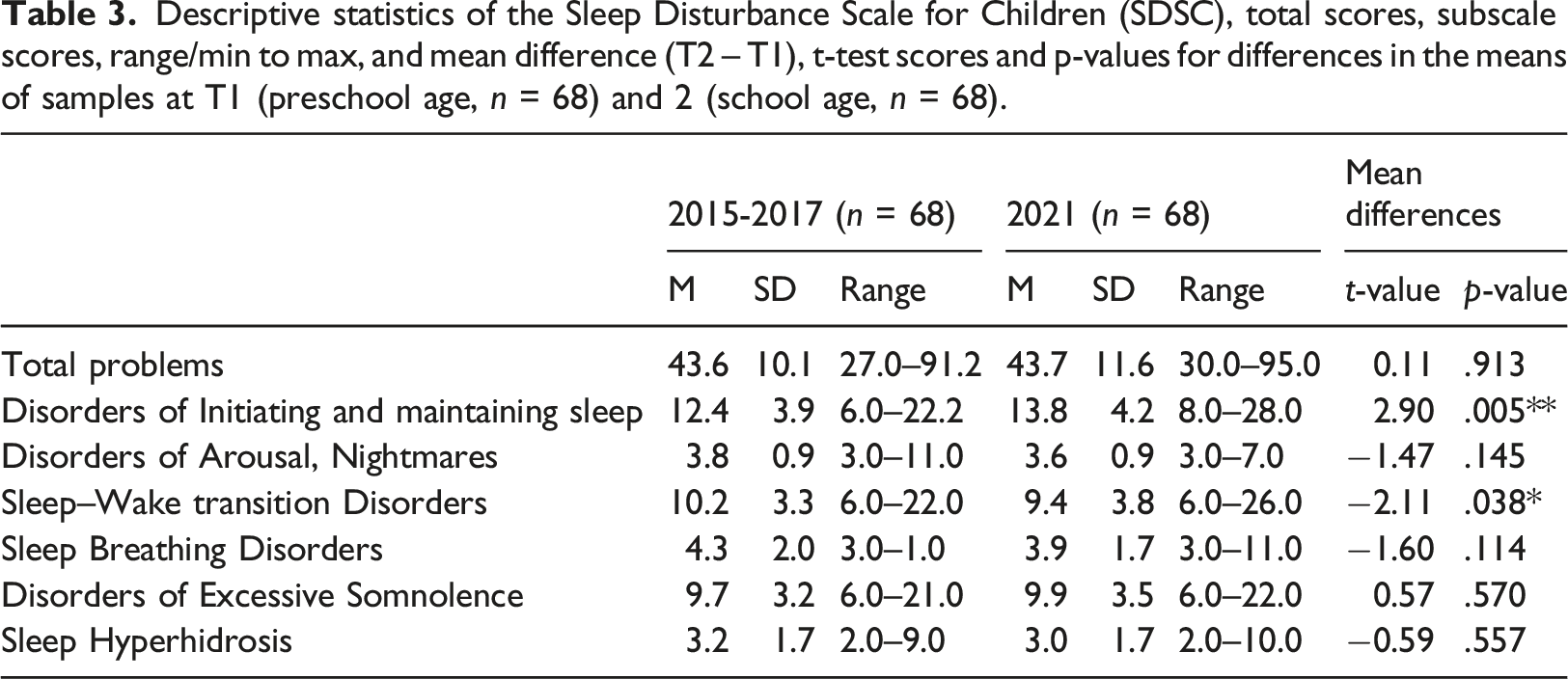
Descriptive statistics of the Sleep Disturbance Scale for Children (SDSC), total scores, subscale scores, range/min to max, and mean difference (T2 – T1), t-test scores and p-values for differences in the means of samples at T1 (preschool age, n = 68) and 2 (school age, n = 68).
Sleep problems at preschool age predict sleep problems at school age
Multiple regression analysis was used to test if sleep problems at T1 significantly predicted sleep problems at T2. T1 SDSC total scores were found to explain a significant amount of the variance in sleep problems at T2 (F(5,61) = 15.6, p < .001, R 2 = .55, R 2 Adjusted = .48), whereas age (β = −.06, t(61) = −.68, p = .50), sex (β = − .06, t(61) = −.65, p = .52), and parent’s lower educational level (β =.04, t(61) = .34, p = .73) did not significantly predict sleep problems at T2.
Sleep and psychiatric symptoms
Sleep problem persistency and psychiatric symptoms at school age
One-way ANOVA revealed a significant difference in CBCL Total (F(2, 67) = 8.19, p = .001), externalizing (F(2, 67) = 5.96, p = .004), and internalizing (F(2, 67) = 6.03, p = .004) scores between the three sleep problem groups (no sleep problems, temporary sleep problems, persistent sleep problems). Tukey’s HSD test showed that CBCL scores in all broadband symptom scales were significantly higher in the ‘persistent sleep problems’ group than in the ‘no sleep problems’ group (Figure 2). Boxplots showing the CBCL total problems, externalizing, and internalizing T-scores (median, quartiles, min and max) in the sleep groups (1 = no sleep problems, 2 = temporary sleep problems, 3 = persistent sleep problems). Means are shown with a dot. The brackets above the boxes show T-score differences between the group means and their significance in Tukey’s HSD (** = significant difference at 0.01 level, *** = significant difference at 0.001 level).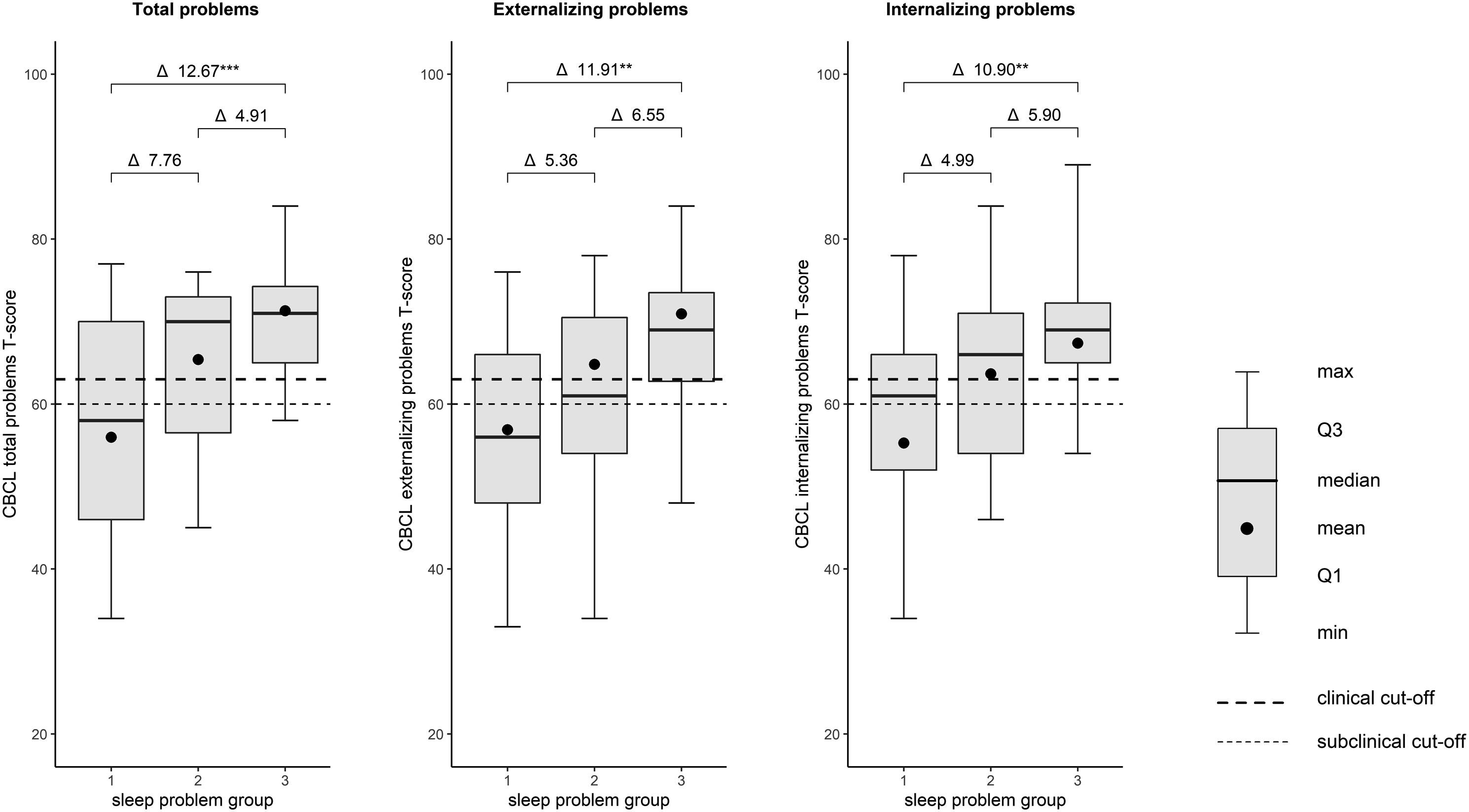
Sleep problems at preschool age predict psychiatric symptoms at school age
Multiple regression analysis of SDSC total score at T1 for predicting CBCL Total score, CBCL Internalizing score, and CBCL Externalizing score at T2.
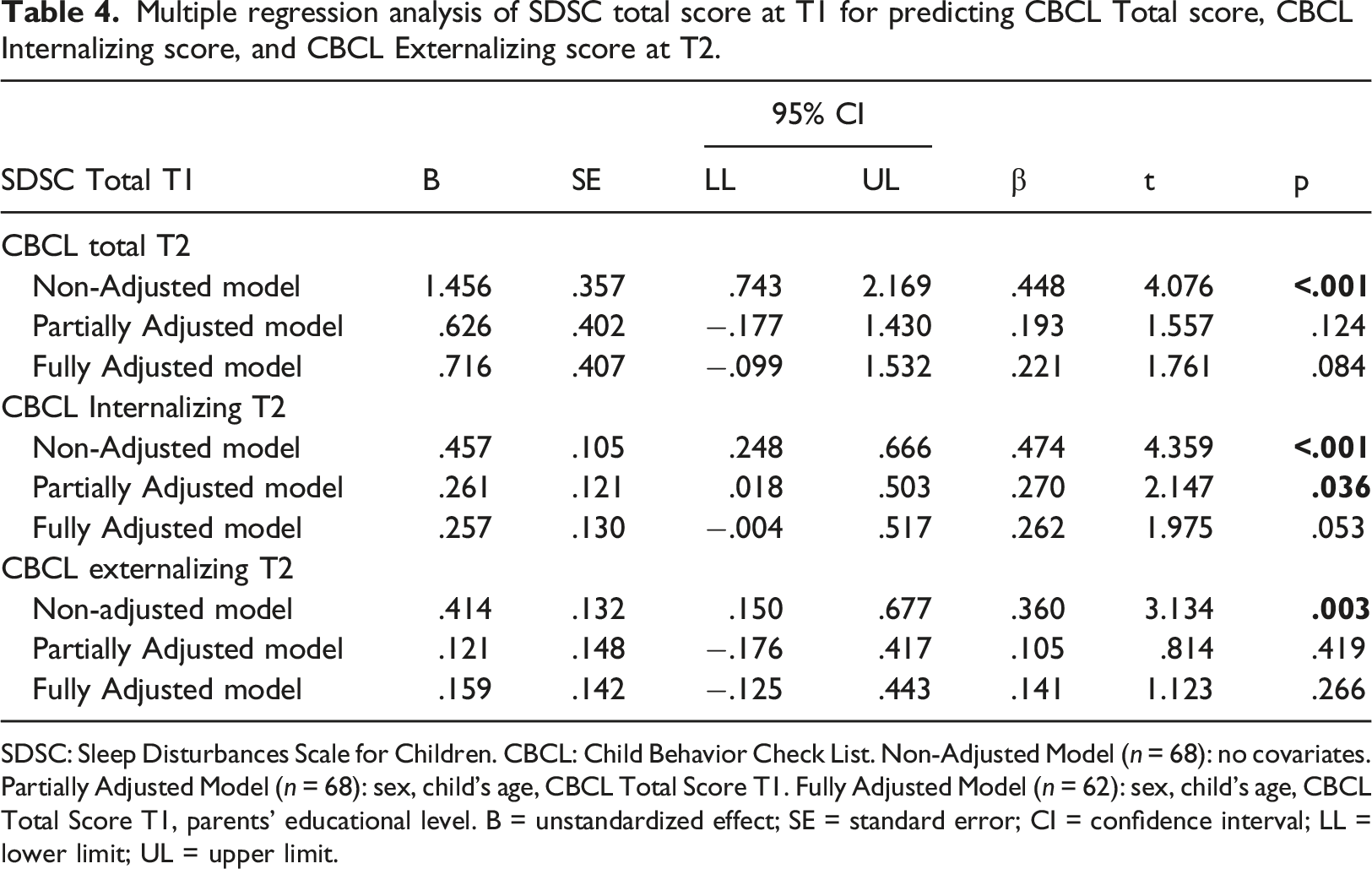
SDSC: Sleep Disturbances Scale for Children. CBCL: Child Behavior Check List. Non-Adjusted Model (n = 68): no covariates. Partially Adjusted Model (n = 68): sex, child’s age, CBCL Total Score T1. Fully Adjusted Model (n = 62): sex, child’s age, CBCL Total Score T1, parents’ educational level. B = unstandardized effect; SE = standard error; CI = confidence interval; LL = lower limit; UL = upper limit.
Discussion
The results of this follow-up study of young child psychiatric outpatients showed sleep problems at preschool age to significantly predict sleep problems at school age. In our sample, 64% of the children with sleep problems at preschool continued to have these problems at school age. Thus, 23.5% of the children in the whole sample had persistent sleep problems. Even though population-based studies have reported sleep problems to be prevalent through childhood, persistent sleep problems are not as common among normative children (e.g. Quach et al., 2009; Simola et al., 2012). The proportion of persistent sleep problems was higher in our psychiatric sample than in population-based samples in which 33.3% to 35% of children who had sleep problems at younger ages (3–8 years) continued to suffer from them 4 years later, with the prevalence of persistent sleep problems being 9% to 12% in Finnish school-aged children (Paavonen et al., 2003; Simola et al., 2012).
Longitudinal studies of child psychiatric patients’ sleep, other than sleep of children with autism spectrum disorders (ASDs) (Fletcher et al., 2017; May et al., 2015; Mazurek et al., 2019) or attention deficit hyperactivity disorder (ADHD) (Becker et al., 2015; Mulraney et al., 2016), are rare. Indeed, we found only one prospective study also including children with disorders other than primarily neurodevelopmental disorders. The study by Hansen and colleagues (2013) evaluated sleep of 7–13-year-old children (n = 76) with ADHD and/or anxiety disorder and found that up to 55% of the total sample experienced persistent sleep problems in an 18-month follow-up. In our study, 23.5% of the total sample had persistent sleep problems. Of the children who had sleep problems at T1 in the study by Hansen and colleagues, 72.4% still had them at T2, whereas in our study the corresponding frequency was 64%. Our results are consistent with those of Hansen et al. (2013), the minor differences likely arising from the sample ages and follow-up periods being different.
Results from our study are in line with the suggestion by Simola et al. (2012) that only relatively few children without sleep problems in preschool develop them at school age, although the incidence in our sample (14%) was again higher than in the community sample (7%). Longitudinal studies from the general population have reported slight decreases in sleep problems with age (Simola et al., 2012) along with improvements in sleep quality (Pesonen et al., 2014). However, no difference emerged between the means of SDSC Total Scores at preschool and school age in our sample. Furthermore, the only decrease with age was found in Sleep–Wake Transition Disorders, and an increase was observed in the Disorders of Initiating and Maintaining Sleep. This is contrary to the findings of Simola et al. (2012) in a community children’s follow-up, in which none of the subscale scores increased from preschool to school age, and decreases emerged in the scales Disorders of Initiating and Maintaining Sleep, Sleep–Wake Transition Disorders, and Disorders of Excessive Somnolence.
Our results suggest that preschool sleep problems associate with psychiatric symptoms at school age in children who attended mental health services at preschool age. Internalizing problems at school age were predicted by preschool sleep problems after controlling for age, sex, and T1 psychiatric symptoms. After further controlling for parents’ educational level, the result still approached significance (p = .053). Previous studies have found especially high levels of anxiety and depressive symptoms to be associated with sleep problems in children and youth (Alfano et al., 2007; Iwadare et al., 2015; Whalen et al., 2017) and have suggested a bidirectional link between internalizing problems and sleep (Alvaro et al., 2013; Bai et al., 2020; Steinsbekk & Wichstrøm, 2015). Only few earlier studies (Mulraney et al., 2016; Bai et al., 2020) have examined the prospective links between sleep-related problems and severity of psychiatric symptoms among child psychiatric patients. The study by Bai et al., (2020) found that having higher levels of dysregulated sleep and more severe internalizing symptoms during a 4-year follow-up entailed a greater risk for poor mental health among youth treated for paediatric anxiety disorders. However, their sample was on average older (11–26 years, median age 17.7 years) than ours. A bidirectional link was observed in adolescence and young adulthood despite treatment for anxiety/depression (Bai et al., 2020).
Interestingly, our results suggest the longitudinal association between sleep and externalizing symptoms to be weaker than that between sleep and internalizing symptoms. These results are in line with Mulraney et al. (2016) who found evidence for a bidirectional relationship between sleep problems and emotional problems but not for a longitudinal relationship between sleep and behavioural problems among 5–13-year-olds with ADHD in a 12-month follow-up. Becker et al. (2015) reported sleep problems to predict externalizing and depressive symptoms in their one-year follow-up of children with ADHD. The results of the associations between sleep problems and externalizing symptoms as well as symptoms of ADHD from community-based longitudinal studies have also been partly conflicting (Armstrong et al., 2014; Whalen et al., 2017; Williamson et al., 2021). It would not be surprising if these associations differed among typically developing children and children with psychiatric or neuropsychiatric disorders (e.g. depression, anxiety, ADHD, ASD), as psychiatric and neuropsychiatric disorders are suggested to share neurological aetiology with sleep disorders (Baglioni et al., 2016; Harvey et al., 2011). The biology of sleep has been reciprocally connected to emotion regulation and suggested to share or interact through the same neurobiological substrates (Harvey et al., 2011). The genes that are important in cultivation and regulation of circadian rhythms are associated with several psychiatric disorders, and disturbances in dopaminergic and serotonergic systems have been widely linked to a range of psychiatric and medical disorders’ aetiology (Harvey et al., 2011). Both systems are suggested to closely be involved and interact also with sleep and circadian systems (Harvey et al., 2011). For example, Bai et al. (2020) hypothesized that among youth treated for paediatric anxiety disorders, age was possibly a less marked correlate for changes in the levels of internalizing and sleep problems than among relatively healthy youth. Thus, maturation might affect typically developing children’s sleep differently than the sleep of children with internalizing problems.
Furthermore, previous research has suggested sleep problems to contribute to facilitating and maintaining mental disorders. The role of sleep problems as a predictor of anxiety later in life has been particularly investigated (Alfano et al., 2007; Gregory et al., 2005; Whalen et al., 2017) . Sleep problems may act as an early risk factor for developing later mental health problems (Armstrong et al., 2014; Quach et al., 2009; Whalen et al., 2017; Williamson et al., 2021). There are some findings of psychiatric symptoms not predicting later sleep problems, suggesting the direction to be from sleep problems to later psychopathology but less strongly vice versa (Alvaro et al., 2013; Gregory et al., 2009; Gregory & Sadeh, 2016). Directional relations between internalizing problems and sleep are further complicated by the presence of sleep problems as one of the diagnostic criteria in depression and anxiety disorders.
Our results suggest that child psychiatric patients with persistent sleep problems have more psychiatric symptoms at school age than those who do not have sleep problems. This is in line with findings from the Finnish community sample reporting children with persistent sleep problems to have, for example, more anxious/depressed mood, aggressive behaviour, and social and attentional problems than children without sleep problems (Simola et al., 2014). In community samples, persistent sleep problems have been found to predict poorer health-related quality of life, behavioural problems, and language and learning difficulties (Quach et al., 2009; Simola et al., 2014). Persistent sleep problems have also been associated with poorer treatment response among depressed adolescents (Manglick et al., 2013).
Limitations, Future Work
Even though the families were reminded up to three times, the non-response to the follow-up was high. Families with child psychiatric issues may be more burdened than families on average, which could be one of the reasons for the low response rate, and even explaining the lack of longitudinal studies in this patient group. The response rate may limit the generalizability of our results to all young child psychiatric patients. The follow-up sample, however, represents well the baseline sample (n = 176), as there were no statistically significant differences in symptom or demographic level. Our sample consisted mostly of boys (75%), which may restrict the generalizability of these results to girls. Although sex was not associated with the relations between sleep problems and psychiatric symptoms in our sample, some previous studies have proposed preliminary evidence of sex-specific associations between sleep and psychiatric problems (Ranum et al., 2019; Rubens et al., 2016). Due to only moderate sample size, it was not possible to determine whether specific sleep problems were related to specific psychiatric symptoms, for which there are some suggestions at the population level (Armstrong et al., 2014). Further, relying solely on caregiver report may limit reliability since caregivers may be unaware of school-aged children’s sleep problems, resulting in biased reports (Paavonen et al., 2003; Rubens et al., 2016). We tried to collect information from patients themselves, but due to a very low response rate and incomplete answers, we could not quantitatively analyse the data. In future studies, for more comprehensive assessment, both child and caregiver report and such objective measurements as actigraphy should be used.
Conclusions
This study highlights the importance of recognizing and treating sleep problems in young child psychiatric patients since sleep problems may contribute to or complicate psychiatric symptoms. Especially persistent sleep problems are associated with severe psychiatric problems. Developing sleep problem treatments specifically for child psychiatric patients is important, as their treatment requirements may differ from those of their normative peers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:Lastentautien Tutkimussäätiö, Helsinki University Hospital Research Funds; TYH 2018203, Helsinki University Hospital Research Funds; TYH2021301