
Abstract
Keywords
Introduction
Body dissatisfaction, defined as “a person’s negative thoughts and feelings about his/her body” (Grogan, 1999, p. 2), is prevalent among adolescents (ranging between 15-62%) (Al Sabbah et al., 2009) and is a leading cause of eating disorders, disordered eating and poor psychological wellbeing (Cruz-Sáez et al., 2018; Stice & Shaw, 2002). Social media use, especially engaging in appearance-related behaviours such as viewing or posting appearance-related content, is associated with increased body dissatisfaction (Saiphoo & Vahedi, 2019). This is problematic given that 96% of adolescents aged 13–17 years use appearance-focused social media platforms (e.g., Instagram, Snapchat) for an average 2–2.5 hours per day (Dooley et al., 2019; Ofcom, 2020).
According to the Tripartite Model of Body Image (Thompson et al., 1999), body dissatisfaction arises when individuals internalise, or cognitively endorse, societal body ideals as a personal body standard and engage in “upward” comparisons with these ideals, that highlight discrepancies between one’s own body and the ideal. Social media may amplify appearance comparison and body ideal internalisation processes because it contains a profusion of idealised content largely endorsing “muscular” or “lean athletic” body ideals for men and “fit”, “thin” or “curvy” ideals for women. Upward comparisons with these largely unattainable body ideals are cited as a primary source of body dissatisfaction in adolescents especially among those who internalise these ideals (Rodgers et al., 2015). Social media also facilitates comparisons with carefully curated, edited images shared by peers and the likes/comments received on posts. These distorted comparisons can lead individuals to hold low social rank perceptions (i.e., that one’s body is flawed and negatively evaluated by others) which result in feelings of inferiority, inadequacy and body shame (Ferreira et al., 2013).
Self-compassion has received research attention as a promising way of addressing body dissatisfaction (Braun et al., 2016). Self-compassion is an emotion-regulation strategy that involves a sensitivity to one’s suffering and a motivation to alleviate it (Gilbert, 2014). Self-compassion is suited to address self-criticism and shame, which are strongly associated with the onset and maintenance of body dissatisfaction (Albertson et al., 2015; Goss et al., 2010). Self-compassion is thought to counter body dissatisfaction and foster body appreciation by helping critical comparisons to be interpreted in more balanced/empathetic ways and by providing individuals with alternative ways to value themselves rather than focusing on the attainment of societal body ideals (Berry et al., 2010).
Higher levels of self-compassion are associated with lower body image concerns and more positive body image in adults and adolescents (Rodgers et al., 2017; Turk & Waller, 2020). Self-compassion interventions are also effective in reducing eating pathology and body image concerns in adults, with medium effect sizes (g = 0.58, g = 0.39). However, self-compassion interventions have not been extensively investigated among adolescents. Adolescence is a vulnerable time for body image concerns and has been identified as a key period for intervention. One randomized control trial of a self-compassion app for adolescent body image yielded improvements in self-compassion and body esteem that were maintained at 3-month follow up (Donovan et al., 2016; Rodgers et al., 2018). Further research is required to build on these findings and ascertain if self-compassion interventions can address unique body image concerns experienced by adolescents on social media.
The present study extends the literature by evaluating a self-compassion intervention adapted to address social media-related body image concern as indicated by the literature, including pressures associated with attaining body ideals and comparing one’s appearance to peers (Rodgers & Melioli, 2016). The intervention was grounded in Compassionate Mind Training (CMT) (Gilbert, 2014) an approach which has been widely investigated in the context of eating and body image disturbance (CFT-E: Goss et al., 2010; Steindl et al., 2017). Compassionate mind training seeks to build self-compassion by increasing activation in “self-compassionate/soothing” affect regulation systems to reduce activation in “threat” and “drive” affect regulation systems responsible for self-criticism and shame. Compassionate mind training teaches mindfulness exercises to help modulate activity in these affect regulation systems. Compassionate mind training also provides psychoeducation about the evolved nature of the human brain to help individuals develop an awareness and understanding of the thoughts, feelings and behaviours they experience. For example, CMT explains that because social hierarchies emerged as significant in the mammalian brain, our human minds have evolved to engage in social comparisons as a safety strategy to gauge what position we are in the group (hierarchy) and to behave in ways that ensure we don’t jeopardise our position within the group (by trying to maintain certain body standards for example). Compassionate mind training emphasises that it is not our fault that we as humans, are concerned about rejection and negative evaluations from others – our minds have evolved to care about this. This insight into functional brain processes and dissolution of self-blame/shame is proposed to help foster compassion (Gilbert, 2014).
Digital SMART (Social Media Adolescent Resilience Training) is a 5-week, schools-based CMT body image intervention for adolescents aged 15–17 years. The feasibility, acceptability, and effectiveness of this intervention on main outcomes of body dissatisfaction, self-criticism, self-compassion, body appreciation and secondary outcomes of social media appearance comparisons and body ideal internalisation were evaluated. It was hypothesised that Digital SMART would improve self-compassion and body appreciation and reduce self-criticism and body dissatisfaction, as well as reducing appearance comparisons and body ideal internalisation, from pre- to post-intervention, and that these changes would be maintained at 3-month follow up.
Methods
Participants
A G-power analysis indicated that a sample size of 76 was required; allowing for a 35% attrition rate, we aimed to recruit 100 participants. Convenience sampling was used; the primary researcher had established links with four mixed gender Irish secondary schools who agreed to host the study. Students in year 4 were invited to participate. The sample contained 102 adolescents, 54 girls (53%), 48 boys (47%), aged 15–17 years (M = 15.6, SD = .46).
Procedure
Mixed methods were used to evaluate the programme. Initially, a quasi-experimental waitlist control design was employed; approximately half of the participants in each school were assigned to either the immediate commencing group or the waitlist control. Class groups were divided by gender to facilitate participant engagement with the programme. Immediate commencers and waitlist controls completed assessments at Time 1 (pre-intervention), Time 2 (post-intervention for immediate commencers, baseline 2 for controls), Time 3 (post-intervention for controls) and Time 4 (3-month follow up). As depicted in Figure 1 and described below, the study design was altered to account for data loss because of study cessation due to Covid-19. Following completion, a subset of students partook in focus groups to share their experiences of the programme. Flowchart depicting participant recruitment, allocation, intervention, assessment and analysis for Digital SMART Programme.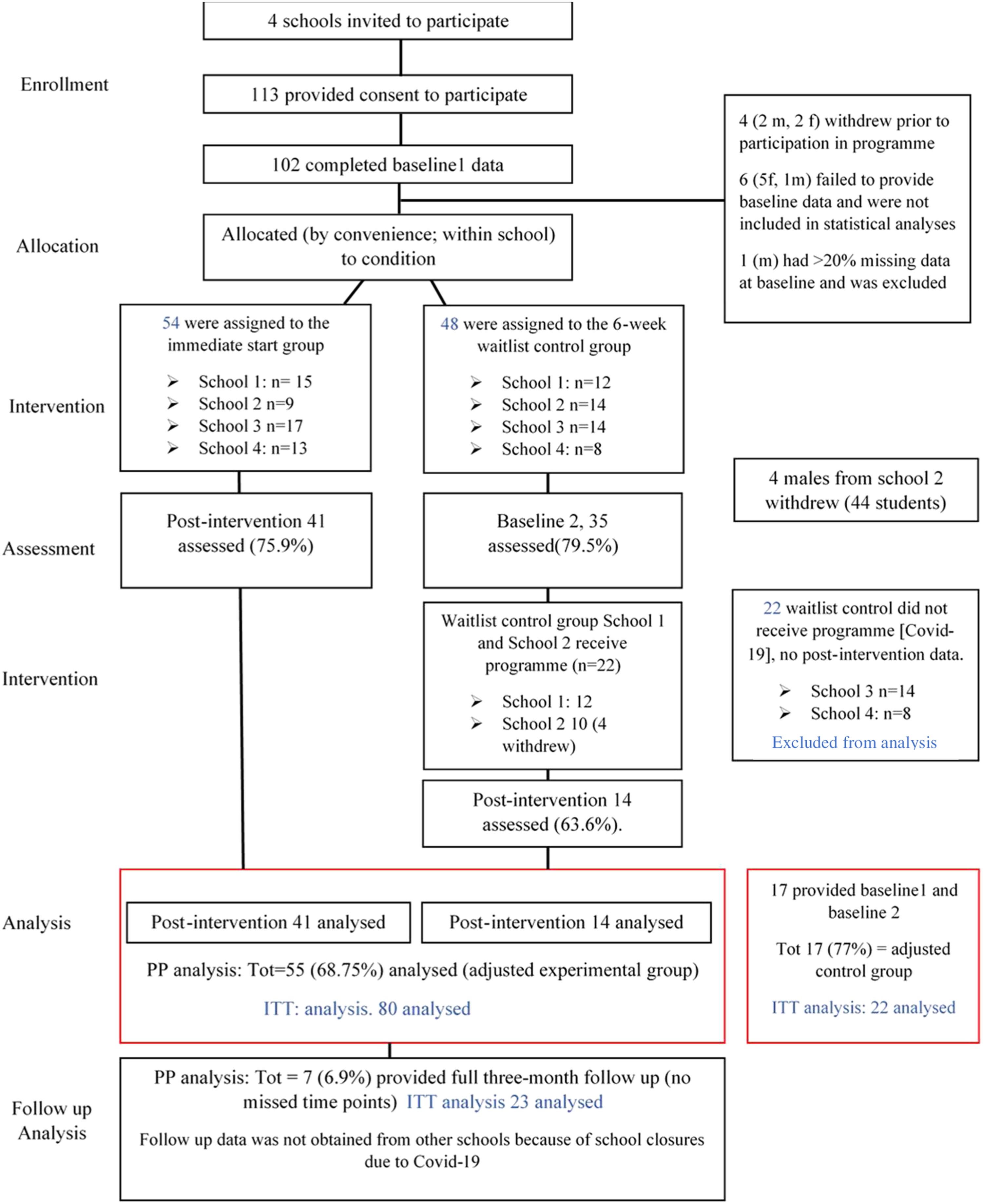
Ethical approval was received from the university’s ethics committee and school principals consented to host the study. Parental consent and participant assent were obtained prior to participation. The programme was delivered by the primary researcher CM (certified in CMT) to six class groups, four girls-only and two boys-only groups. Six 30–45-minute focus groups containing 6-8 participants from each group were conducted by an independent female researcher to facilitate an objective evaluation of the programme. Participants’ weekly feedback in reflection booklets were also evaluated.
Intervention
Digital SMART: five session intervention content overview.
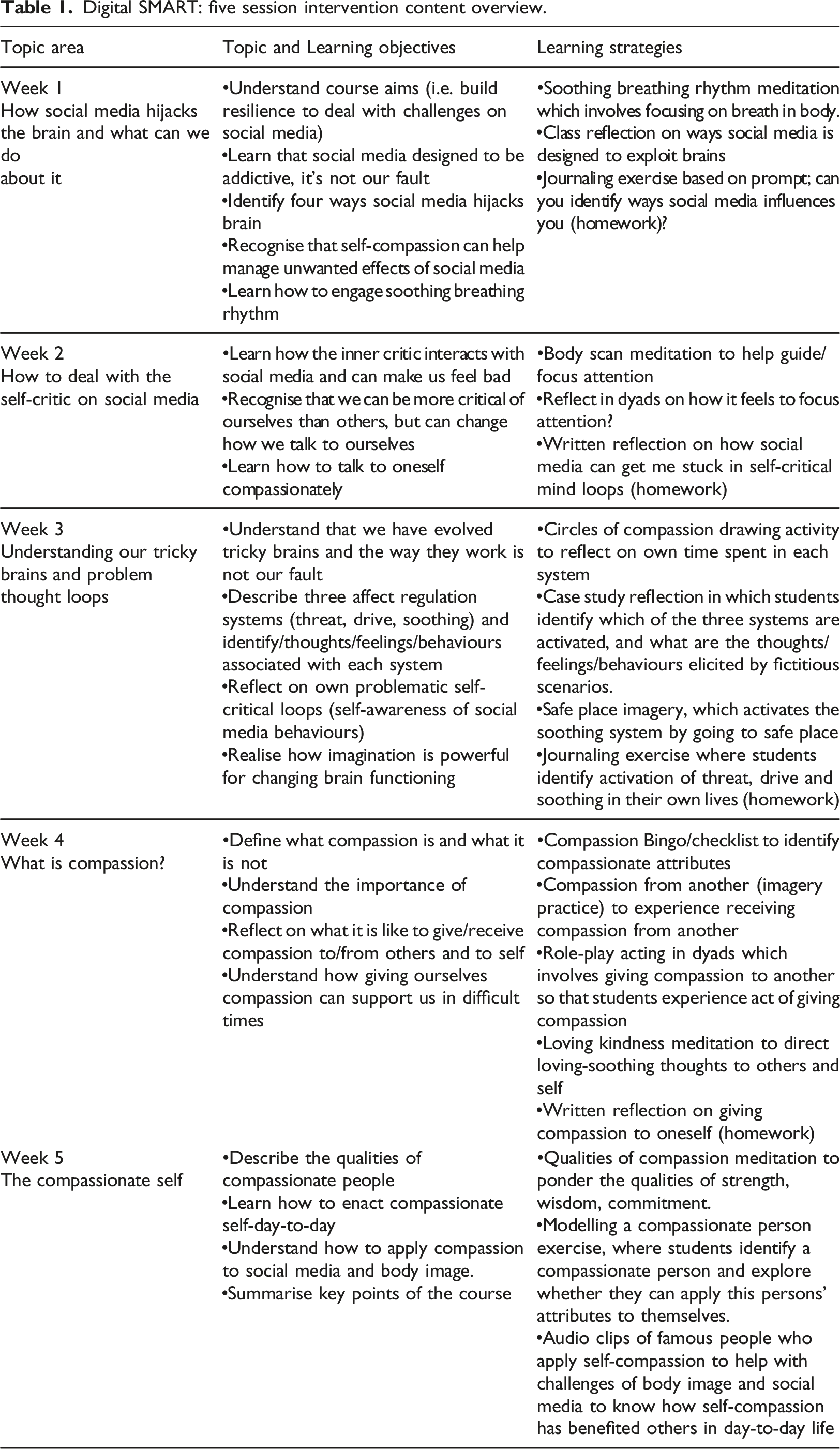
Each session introduced a different theme/topic related to self-compassion, body image and social media; students were invited reflect on topics and engage in interactive activities (writing/role-play/brainstorming exercises). Outside of class, students were invited to practice mind-training skills and answer short prompts in reflective journals to consolidate content encountered in class.
Measures
Acceptability
Assessed by asking participants to rate 1.) How easy/difficult and 2.) How helpful they found the session using a 5-point Likert scale.
Feasibility
Assessed using participant attendance and retention data. Aligning with previous studies (e.g., Bluth et al., 2016), the feasibility criteria were 75% for attendance and 80% for retention. Participants’ self-reported practice of self-compassion exercises (adherence) was evaluated.
Qualitative Data Collection
Focus groups further explored the acceptability of the programme by asking participants whether they understood the content, found the programme helpful/informative and were able to apply these practices and principles to their daily lives. See Appendix A for the full questionnaire schedule.
Demographics
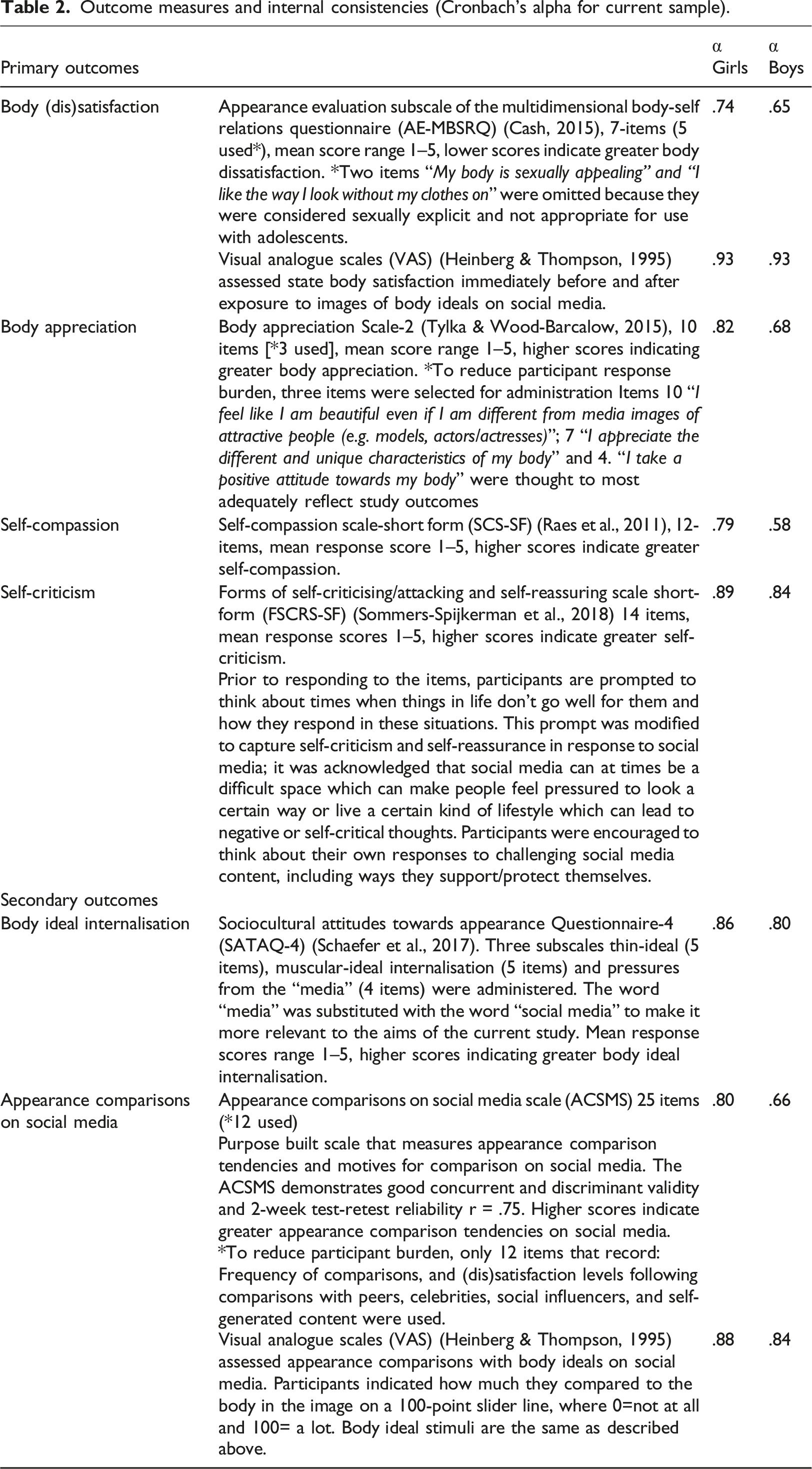
Outcome measures and internal consistencies (Cronbach’s alpha for current sample).
Data analysis
Qualitative data analysis
Qualitative data was transcribed verbatim by the independent researcher and analysed by the primary researcher using MAXQDA software. Data was subjected to an iterative, recursive thematic analysis, guided by Clarke and Braun’s (2017) thematic analysis procedure, which involves; familiarisation with the data, division of data into codes, grouping codes into themes and subthemes, refining and defining themes. Participant reflection booklets were analysed using content analysis, where data were categorised into codes and codes were grouped into themes in an iterative, recursive fashion. Inter-rater reliability was established by having a second independent researcher review the coding-frame for focus groups and reflection booklets and indicate their (dis)agreement with proposed codes. Discrepancies were resolved through discussion with the lead author (DH). Kappa Coefficient values were high (K = .92), indicating a high level of inter-coder agreement. The researcher adopted a reflexive approach and acknowledged that their own biases and background (white, Irish, educated woman in her mid-twenties) shaped the data obtained and the way it was interpreted.
Quantitative data analysis
Participants who failed to provide baseline scores (n = 6), who withdrew from the study (n = 4) and whose responses contained >20% missing data (n = 1), were excluded from analyses. Missing values (<1% across participant scores) were treated with person missing substitution (proration). Intention to treat was used; all participants who were randomly assigned to a condition were included in the analysis. Missing data were imputed using the “Last observation carried forward” technique, whereby missing data points were replaced with the last data point provided by the participant prior to withdrawal.
Because of premature study cessation due to the outbreak of Covid-19, we were unable to collect post-intervention data from two waitlist-control groups, and 3-month follow up data from three schools. Additionally, due to timetabling constraints imposed by schools, we were not able to randomise immediate start and waitlist control groups appropriately (i.e., all immediate start groups contained girls only). We adjusted our analyses to account for these changes to study design. We removed participants who did not receive the intervention because of study cessation from the analysis (n = 22). To maximise statistical power and address issues of inappropriate randomisation, we assigned all individuals who received treatment (i.e., completed the intervention and post-intervention measures) to an experimental group, regardless of whether they were initially assigned to experimental or waitlist control groups (n = 80). We conducted a repeated measures ANOVA for the full experimental group, as well as for boys and girls separately to determine main effects of time. We also conducted repeated measures ANOVAs on pre-, post- and 3-month follow up data provided by participants in one school (n = 23) to establish maintenance effects. Bonferroni post-hoc analyses assessed change across time. Partial eta squared (ηp2) measured effect sizes for ANOVAs; effects were considered small 0.01, medium 0.06, and large 0.14. Hedge’s gave established the magnitude of within-subjects pre-post change; effects were considered, 0.2 small, 0.5 medium and 0.8 large.
Results
Feasibility
Participants’ average attendance rate was good (75%), absences were due to illness or participation in other school activities. Overall, 42.9% of reflective booklets were returned by participants but girls’ return rates (55.6% returned) were greater than boys’ (13% returned). On average, participants practiced meditation sessions one time between sessions.
Acceptability
In reflective booklets, participants’ median ratings of “ease” of sessions was 3 (alright), indicating that content was pitched at an appropriate level. The median rating of “helpfulness” was 2 (helpful) indicating the utility of the programme.
Qualitative Data
Content analysis of participants’ reflective booklets and thematic analysis of focus group discussions identified five themes relating to programme acceptability including; satisfaction, comprehension, engagement, relevance, utility/impact.
Satisfaction
Participants who completed reflective booklets reported that the programme was interesting/informative (5 mentions) and enjoyable/relaxing (3 mentions). Psychoeducation about the evolved brain and about how social media hijacks the brain was favoured by boys, while girls responded more to learning about compassionate self-talk, appearance comparisons and body ideals on social media. As noted by one boy, “It was useful to understand why sometimes you might feel a certain way, like oh that’s just a part of my brain that does that kind of thing that was needed thousands of years ago and it’s still with us today”. The breathing and meditative practices were popular among many students who reported that they “enjoyed the mindfulness exercises we did at the end of each session because they were nice and relaxing, and you could use them at home by yourself if you wanted”. However, others felt that the content was not interesting, the delivery was slow, or the mindfulness practices were unhelpful; “It was just a bit boring; I suppose I wouldn’t be that bothered about how it [the brain] works really”. Participants reported that increased active participation, pair work, real-life examples, and more time to explore concepts in class would enhance programme satisfaction.
Comprehension
Participants felt the course was easy to understand (3 mentions) and largely demonstrated good comprehension of course content. They were able to identify that appearance comparisons with body ideals activated “threat”, viewing fitness-content activated “drive” and chatting with friends activated “soothing” on social media. They could also recognise self-critical thoughts arising from social media use, with one participant noting that “Social comparison affected [her] by making [her] focus on others’ “perfect” lives and made [her] feel bad about [her]self”. Participants also demonstrated a comprehensive understanding of compassion and how to relate it to themselves by “Accept[ing] that [they’ve] made a mistake, don’t beat [themselves] up, live and learn”. Participants also mentioned “try[ing] to talk to [themselves] in the same way [they] would talk to [their] friends” and “cutting down negative thoughts about self”. Participants reported “conscious[ly]” bringing “a balance between the three systems” by “practic[ing] more soothing techniques to cancel out threat or drive feelings”. However, some struggled to apply it to their lives with one girl remarking that “Like nobody, if they get a bad comment or something, is going to sit there breathing closing their eyes, nobody’s going to do that”.
Relevance
Boys conceded that the programme would be helpful for those who did struggle with body image and social media but felt that because they did not have these issues, the programme was less relevant for them. Boys felt it would have been more helpful if it targeted broader wellbeing and mental health issues. However, other groups reported that the programme addressed pertinent topics, such as self-criticism and body dissatisfaction, that were not covered in school curricula. Discussing these topics helped normalise their issues. One girl noted “Today really helped because I realised I wasn’t alone in the self-critique which made me feel much better”.
Engagement
Many felt that the classroom environment was not conducive to sharing and discussing sensitive issues. Concerns about peer judgement and fears that their contributions “would get out of the room and people would be talking about [them]”, limited participation, particularly in male groups. Participation issues were not evinced in all groups; some groups engaged in open conversations where participants “could relate to other people’s problems … even people from different friend groups”. Small group size, friendliness between classmates and a non-judgemental classroom atmosphere facilitated this disclosure. Engagement with reflective prompts and meditative exercises outside of class was poor and limited by distractions at home, competing activities or forgetfulness.
Utility/Impact
“Helpful/useful” was one of the most common codes observed across reflective booklets. The programme encouraged participants to be more compassionate towards themselves and equipped them with the skills “Not to think about myself so negatively as I did”. Some participants were able to extend compassion to their bodies and reported developing greater body acceptance and appreciation. Many girls reported that they were less negatively affected by body-related content they encountered on social media. One girl remarked “Like before I’d look at my pictures I’d have say on Instagram and I’d say ‘No, that’s disgusting, take it down’ but now I just leave it and I’m like ‘well that’s me… that’s it… deal with it’. Body acceptance was facilitated by the recognition that uniqueness/difference is a good thing and an understanding that there are biological and genetic factors that limit body change. Some felt the programme had little or no impact and failed to change the ways they related to themselves, their bodies or social media.
Quantitative Data
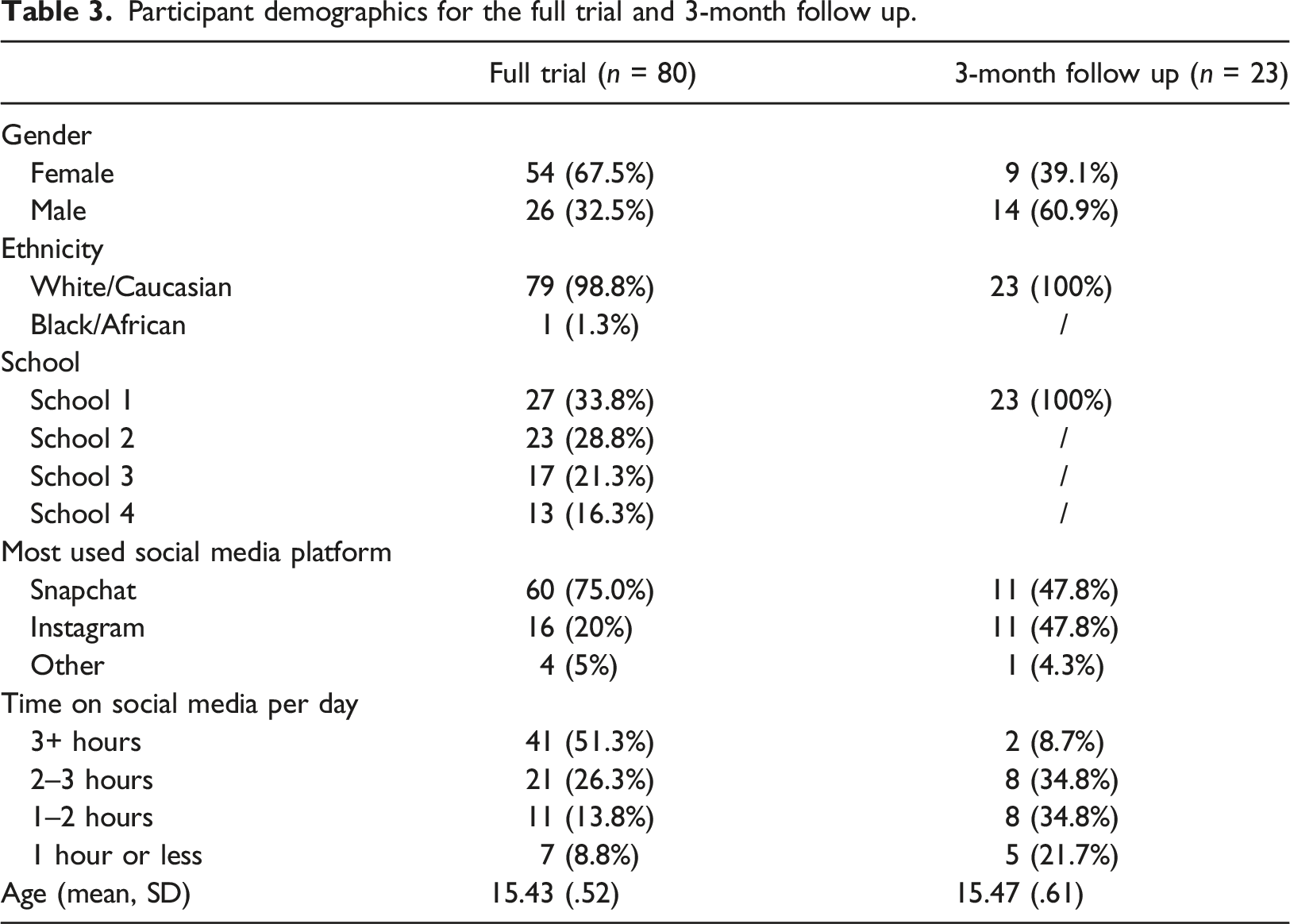
Participant demographics for the full trial and 3-month follow up.
Hedge’s g effect size and 95% confidence intervals for change scores between pre- and post-intervention.
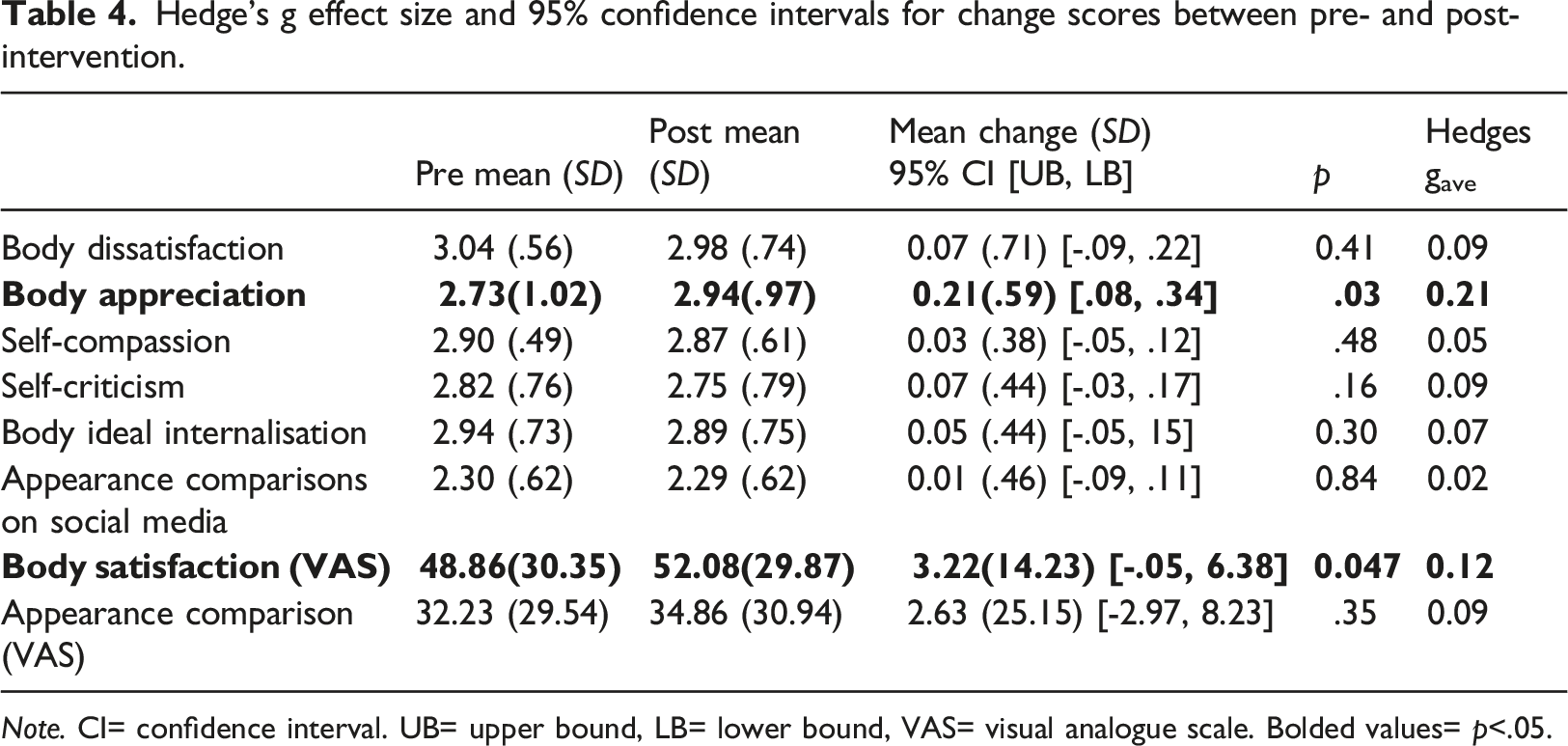
Note. CI= confidence interval. UB= upper bound, LB= lower bound, VAS= visual analogue scale. Bolded values= p<.05.
Boys reported significant increases in body satisfaction F (1, 25)=6.34, p =.019, ηp2 =.20 from pre-to-post intervention, while girls demonstrated significant improvements in body appreciation F (1, 51)=7.63, p =.008, ηp2 =.13 and significant reductions in self-criticism F (1, 53)=5, p = .03, ηp2 =.09 from pre-to-post intervention (Table B2, Appendix B).
Three-month follow up analyses found no significant effects across time, except for body satisfaction F (3,20)=3.65, p =.03, ηp2 =.14, which increased across pre-, post-intervention and 3-month follow up, but only became significant from time 2 to 3 (Table B3, Appendix B).
Discussion
This research represents a novel contribution to the field of body dissatisfaction prevention programs, and is, to our knowledge, the first to evaluate a self-compassion intervention to address adolescents’ social media-related body image concerns.
High retention (87%) and attendance rates (75%) and self-reported practice of mindfulness between sessions indicated that Digital SMART was feasible. Acceptability as indicated by levels of comprehension, engagement, satisfaction, perceived relevance and usefulness of the programme varied. Comprehension of content was good, but participant engagement in classroom discussions was mixed; some groups felt comfortable openly discussing issues/concerns while others did not. Those who completed reflective booklets and groups who readily engaged in classroom discussions held more favourable opinions of the programme, indicating that level of engagement may have influenced perceptions of programme acceptability.
Some felt that the programme was relatable and addressed pertinent issues, such as self-criticism and body dissatisfaction that were avoided in school curricula. However, boys didn’t find the programme very relatable because they felt they did not struggle with body image, social media or self-criticism; they did acknowledge that the programme would be helpful for individuals who did have such concerns.
Some perceived the programme to have little/no impact, but others reported that the programme was successful in changing how they related to themselves, their bodies and social media. Participants reported heightened awareness of their inner dialogues and an ability to relate to themselves more compassionately. Breathing and mindfulness exercises reportedly helped participants self-soothe in challenging times. Self-compassion enabled some girls to reappraise critical evaluations of their bodies and mitigated the impact of problematic appearance-related content on social media (Albertson et al., 2015). Learning about the biological limits of body change, recognising the universal nature of body dissatisfaction and imperfection helped some girls foster body appreciation (Goss et al., 2010). Similar changes in body perceptions or social media use were not reported by boys. Given that the programme drew from a relatively sparse literature on male body image, further research is required to tailor the programme to address their needs.
Digital SMART yielded significant improvements in body appreciation and body satisfaction from pre- to post-intervention. Although effect sizes were small, these positive findings are consistent with literature that highlights the usefulness of self-compassion interventions for body image (Rodgers et al., 2018; Turk & Waller, 2020).
Interestingly, participant outcomes differed by gender: boys’ body satisfaction significantly increased, while girls’ body appreciation increased, and self-criticism reduced from pre- to post-intervention. Findings may be attributable to differences in how body image and/or self-compassion is experienced by boys and girls (Bluth et al., 2017); further research is required to understand these gender differences.
As hypothesised, girls experienced reductions in self-criticism concurrent with improvements in body appreciation. However, no improvements in self-compassion were observed. It may be that girls’ body image can be improved by reducing self-criticism without necessarily improving self-compassion; however, this warrants further exploration. There were no changes in boys’ self-criticism or participants’ appearance comparisons and body ideal internalisation, therefore the mechanisms through which change occurred remain unclear – further research is required to explore this.
Body satisfaction increased significantly from post-intervention to follow up; while findings may reflect lagged benefits for body satisfaction, follow up data should be interpreted cautiously given the small sample size.
Limitations
The sample size was small and data loss incurred by the premature cessation of the study due to Covid-19 may have reduced statistical power to detect significant effects. Inferences on maintenance effects are particularly limited as follow up data was only obtained from one school. Because of data loss and the inability to appropriately randomise ‘immediate start’ and ‘waitlist control’ groups because of school timetabling constraints, we adjusted our analyses to evaluate outcomes in an intervention arm only. Subsequently there was no control group and so findings should be interpreted cautiously. Future research should evaluate self-compassion interventions using large, gender balanced samples over a sustained time period.
Additionally, while outcomes were evaluated using validated measures, the reliability of the self-compassion scale in boys was low and changes were made to some scales to reduce response burden and to increase their relevance/appropriateness. This may have altered reliability/validity scores and/or limited our ability to capture nuances/changes in these constructs (Kruyen et al., 2013). Finally, this study relied on self-reported data to evaluate intervention outcomes, therefore it is difficult to determine the extent to which participants over or under report behaviours, especially for behaviours perceived as being socially undesirable (Jaycox et al., 2006). Boys’ reported lack of body image concerns, contrasts with literature suggesting that boys and girls experience similar levels of social media-related body dissatisfaction (Saiphoo & Vahedi, 2019); the stigma surrounding male body image may have impeded boys’ willingness to admit to these concerns (Hargreaves & Tiggemann, 2006). The return rate of boys’ reflective booklets was low, which limits insights into private perceptions of the programme. Finally, although we adopted a reflective approach and attempted to verify the credibility of responses by triangulating them with responses provided to questionnaires and reflective booklets, it is also plausible that we missed trends or misreported on them.
Conclusion
Findings provide preliminary support for the feasibility, acceptability and effectiveness of a CMT intervention to improve adolescent body image, but further research is required.
Supplemental Material
Supplemental Material - Pilot trial of a self-compassion intervention to address adolescents’ social media-related body image concerns
Supplemental Material for Pilot trial of a self-compassion intervention to address adolescents’ social media-related body image concerns by Ciara Mahon and David Hevey in Clinical Child Psychology and Psychiatry
Footnotes
Acknowledgements
Thanks to Ms. Aoife Fennelly for assisting with focus groups and Dr. Chris Irons for kindly sharing CMT resources.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.