
Abstract
Guided self-help has become an important treatment option in the field of eating disorders as access to in person evidence-based treatments is limited. Given the scant amount of literature published on guided self-help for the treatment of eating disorders in the child and adolescent population, our aim was to describe online GSH-FBT sessions in detail as conducted as part of a larger feasibility study, examining quotations from therapists that illustrate the GSH-FBT stance and also describing how online GSH-FBT differs from FBT delivered by videoconferencing within a descriptive case report.
Introduction
Guided self-help has become an important treatment option in the field of eating disorders as access to evidence-based treatments has become more challenging. New cases of eating disorders as well as hospitalizations have increased significantly during the COVID-19 pandemic, suggesting a need for expansion in eating disorder services (Agostino et al., 2021; Haripersad et al., 2021). Guided self-help implies the presence of a therapist or coach (in contrast to pure self-help) and can be more efficient compared to standard therapy as sessions are generally shorter and material is provided to watch or read in between sessions (Lock et al., 2021; Lock et al., 2017). To date, guided self-help in the field of eating disorders has mostly focused on the adult population and has largely focused on binge eating disorder (BED) (Traviss-Turner et al., 2017). Guided self-help in children, adolescents, and emerging adults with eating disorders has recently been recommended in virtual care guidelines for the COVID-19 context and beyond, as a treatment of importance (Couturier et al., 2021), however it is not widely available and evidence is just emerging (Lock et al., 2017, 2021).
Similarly, challenges to delivering evidence-based treatments with fidelity (meaning the treatment is delivered as true to the treatment model) are numerous. This has also been seen in the delivery of Family-Based Treatment (FBT) where there can be issues with therapist drift (Couturier et al., 2013; Kosmerly et al., 2015). A model in which essential material is delivered by text or video could standardize the treatment, ensuring that key components are delivered. This is a potential advantage of GSH where the role of the therapist is to act as a “coach” directing patients, or families, to text or video material that is standardized. In this role, the coach remains true to the model by providing standardized information; theoretically there should be less deviation from the key components. In addition, “coaches” may not need extensive training in models and theory of family therapy, as they are to focus on directing families to the information that has been pre-recorded. This could enhance dissemination as training requirements are not as intensive. In summary, the potential benefits of a GSH model include greater therapist efficiency, increased fidelity, and a positive impact on dissemination (Lock et al., 2021).
The effectiveness of parental guided self-help FBT (GSH-FBT) for adolescents with Anorexia Nervosa (AN) has recently been reported within an open feasibility study (Lock et al., 2017) and a feasibility randomized controlled trial (Lock et al., 2021). The open trial involved 19 families receiving 12 parent-only sessions lasting 20–30 minutes each over a 6-month period conducted over the phone or computer (Lock et al., 2017). Median BMI increased from 85% at baseline to 97% at end of treatment. Eating related psychopathology also improved. Dropout rate during treatment was 21%. These outcomes indicate that GSH-FBT is feasible and acceptable to families (Lock et al., 2017). In addition, a feasibility study of a randomized trial has recently been completed comparing GSH-FBT to FBT delivered by videoconferencing (FBT-V) (Lock et al., 2021). This feasibility study involved 40 adolescents aged 12–18 years with AN and their parents. Both treatments were rated similarly in terms of acceptability. Improvements in weight, Eating Disorder Examination Scores and parental self-efficacy were similar between the groups, although GSH-FBT was more efficient (outcome/therapist time) (Lock et al., 2021).
Given the limited amount of literature published on guided self-help for eating disorders in the child and adolescent population, our aim was to review transcripts of online GSH-FBT sessions conducted as part of the larger feasibility randomized controlled trial mentioned above (Lock et al., 2021), examining quotations from therapists that illustrate the GSH-FBT stance and how it differs from FBT-V (Matheson et al., 2020). We present case material concurrently to illustrate the application of this treatment model. Ethics approval was obtained through Stanford University and the Hamilton Integrated Research Ethics Board, with informed written consent provided by parents and therapists involved in the study.
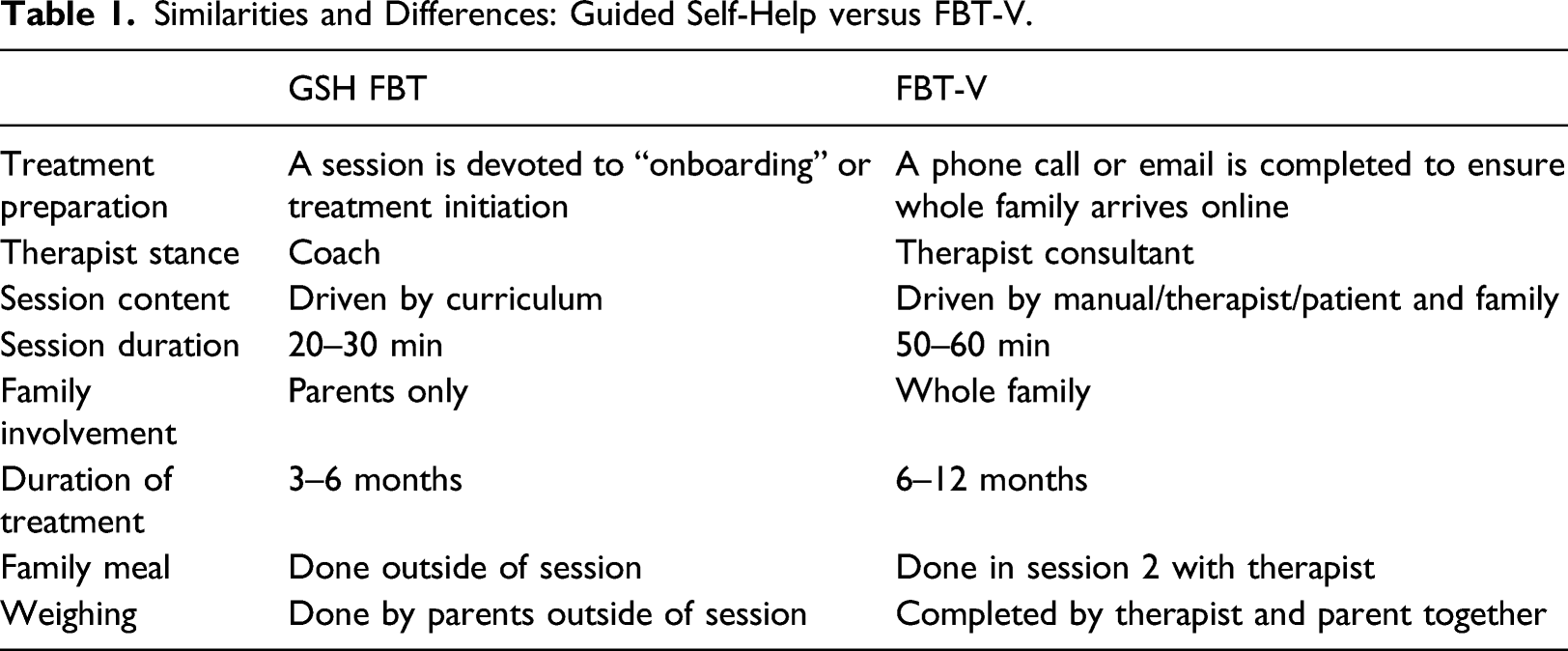
GSH-FBT: Overview
Similarities and Differences: Guided Self-Help versus FBT-V.
Phase 1
Onboarding
In the onboarding session, the GSH-FBT coach discusses the general treatment parameters, introduces the online platform, and ensures that the technology is working. Homework is given to review prior to the first session. The process of weighing is also discussed. This is an example of how the treatment is explained to the parents by the coach, “So, the other part about guided self-help is that it’s really… more of the onus is on you guys to do the treatment at home. As the therapist, I’ll be available to you and answering questions and guiding you, but the duration of our meetings is a bit shorter than it would be in regular family therapy. So, our sessions are 20–30 minutes, whereas in regular family therapy, it’s an hour. I’ll be more like guiding you to watch the videos and help you apply it, but, really, it’s more self-directed. Does that make sense?”
The process of weighing at home is also explained by the coach as follows, “….Want to talk a little bit about weighing her because every week, we’re going to be discussing whether her weight is going up or down or staying the same. So, in guided self-help, you guys would be the ones to weigh her at home and then report it to me.”
Session 1
The stance of the GSH-FBT coach is to redirect and keep parents focused on the educational material provided. For example, the GSH-FBT coach would initiate a session by asking if parents had done the homework and whether they had any questions about what they had reviewed. The coach continually brings back the discussion to the educational material. For example, “What did you notice, after watching the video, that you paid attention to?....You probably read in the book too that we don’t spend a lot of time in this treatment trying to figure out why this happened. We can hypothesize, and we can guess, but a lot of the time we can’t figure out why exactly this occurred.”
And, “what else did you take away about the medical complications?”
Setting up for Session 2. There is no observed family meal in GSH-FBT, however, parents are asked to complete a challenging meal at home that will re-nourish their child. “Okay, well, the next set of videos is going to cover some strategies around mealtimes and how to help her more during meals. There’s also a bit of a reflection—it’s for homework—to write down how a meal went when you really tried to increase the amount for her and perhaps, I don’t know, if you’ll face some resistance….”
Session 2–7
These sessions proceed similarly to FBT-V in which the focus is maintained on weight restoration and parental efforts at feeding their child. However, the GSH-FBT coach stays focused on the curriculum
And the GSH-FBT coach assigns homework for the upcoming week, “Yeah, that’s part of it. All right, well, let’s talk about the homework for this week. I don’t know if you guys have gone ahead with the videos, but it says the homework for this week is Lecture 4 videos—so, ‘Staying on Course’ and then some reading. Oh, and this is appropriate because we talked about being united. So, the reading is about harnessing the power of unity—so, staying together as a couple and being firm on the expectations of what she eats. Yeah, so that’s the homework.”
Transition to Phase 2. The curriculum of GSH-FBT moves forward into phase 2, although some families may not be ready to apply the concepts in real life. The criteria for applying concepts learned in Phase 2 videos and reading material are the same as in FBT-V (ie. Weight of their child should be at least 90% of a treatment goal weight (TGW), and there should be little resistance to refeeding efforts). This is explained to the parents as follows, “I know that we’re supposed to be talking about moving into Phase 2 and whether your child is ready for moving into Phase 2. I think we can probably agree that she is not, because we haven’t met the criteria, which is usually someone has to be above 90%. And she’s being pretty compliant with you, so that is another criteria. But we’re not quite at the weight point. However, the curriculum of the guided self-help keeps moving on, and it’s going into Phase 2 stuff now. Which I know you watched already, right?”
Phase 1: case summary
Sam is a 17 year old female with a four-month history of a 30 lbs weight loss. She is currently about 85% of a TGW. She lives in an intact family. Dad works in the field of computers and Mom has a house cleaning business. She has an older brother aged 21 years who attends university. Sam had been seeing her family doctor and dietician before enrolling in this treatment. At the onboarding session, parents voiced concern that she would not have any therapy herself. They mentioned they wished they were receiving FBT-V as at least she would be involved in the treatment. Parents were encouraged by the GSH-FBT coach to give GSH-FBT a chance and that it had similar outcomes to FBT-V when studied to date, and that Parent-Focused Therapy (Le Grange et al., 2016) (where the adolescent is not involved) works just as well. Then, later during Phase 1, Sam started asking her parents for body image therapy. This made parents question the treatment modality even more. It was explained to parents that body image therapy is typically not effective at this stage of treatment and that they needed to focus on getting her physically healthy first. In FBT-V, the therapist would review the effects of starvation and why it is important to act right away. Instead, the GSH-FBT coach explained that weight restoration is the key as a first step and that parents are in the best position to do this. The coach then asked the parents to re-watch videos on the “the effects of starvation” and “it’s not your fault, but you are the solution” to help increase a sense of urgency and to empower parents by use of the course material. The parents were asked to reread sections of the book on cognitive distortions associated with eating disorders (Chapter 5 “Get Into Your Child’s Head”). They were also encouraged to read sections of the book on agnosticism, for example, Chapter 3 “Don’t waste time on Why?”
At times, in Phase 1, parents were not aligned in their approach and Mom often felt she was the one setting all the limits. The coach directed parents to re-watch videos on parental unity, “remaining aligned” and reread the sections from the book, Chapter 2 “Get Together” on parental alignment. Dad was particularly encouraged to watch videos on externalization “How Anorexia is like Cancer” and medical complications “the effects of starvation”, so that he would feel heightened urgency to support mom’s efforts at refeeding. Mom mentioned she would become frustrated and angry at times. She was encouraged to review the video “try, keep trying, and know when to walk away” as well as videos on “Understanding externalization”. In FBT-V, the therapist might spend significant time during each session by attempting to develop parental alignment and have parents come up with solutions as to how they could be on the same page. In GSH-FBT, parents are directed to read and watch material that is pertinent to the issue of parental alignment.
Phase 2
Session 8–10
These sessions, similar to FBT-V, focus on Phase 2 material such as gaining independence with eating in a gradual fashion. “Yeah. So that’s good though that she’s still making progress and obviously you’ve been feeding her well. And I was thinking as you were talking that even though the curriculum moves ahead and is talking about independence, it’s always up to you guys how much independence to give her. You don’t have to follow the curriculum if she’s not ready for it.”
Phase 2: case summary
When the curriculum moved on to Phase 2, parents did not quite feel comfortable transitioning control back to Sam as she still had quite a bit of weight left to gain. There was a discussion about waiting until parents felt more comfortable and that although the curriculum moved forward, parents still needed to decide when they felt comfortable with the progression to Phase 2. With more time in between sessions, Sam was eventually able to gain appropriate weight and began to transition into Phase 2 by having meals at her boyfriend’s house. She also started playing volleyball again. At times, parents voiced anxiety about giving more control to their daughter and they worried about her having a relapse. Whereas an FBT-V therapist would process this material and have parents come to a united decision about how to proceed for the next couple of weeks, they were instead directed to watch video material on “expecting an uneven transition”, “dealing with setbacks”, and “Phase 2—remaining aligned”. They were encouraged to come to their own decisions independently on how they wanted to proceed, outside of the session.
Phase 3
Session 11 and 12
In Phase 3 of GSH-FBT the focus is on returning to life as it was before the eating disorder and planning to mitigate relapses. The curriculum ends, assuming weight restoration will continue as parents have learned all of the principles that they need. “We don’t expect her to be fully recovered by 12 weeks—that would be too much to ask - but that the progress continues even after the treatment ends.” “Just want to congratulate you. But you’ve done the hard work. You guys followed the curriculum. Even when you doubted it, you did it, and I think you’re really seeing the results of all your hard work, but you really stuck to your guns and helped her to eat, and she deserves a lot of the credit too, that she cooperated.”
Phase 3: case summary
Parents were diligent in watching videos and completing reading assignments. As in FBT-V, development was discussed in this phase and parents recalled their adolescent challenges. They watched “Healthy Development for 17–18 year olds”. Sam had broken up with her boyfriend, and parents were confident she would be able to handle this stressor. They were referred to the videos “How to think about stress during this process” and “Dealing with setbacks”. Throughout the treatment, Sam continued to see her medical practitioner as he deemed necessary and she occasionally saw the dietician (about once a month for a weight check). Sam gained from 121.6 lbs (86.1% TGW) to 134.4 lbs (95.3% TGW) over 4.5 months. Global EDE score decreased from 4.50 at baseline to 0.26 at end of treatment. At the end of the treatment, parents stated that they were pleased with Sam’s progress and they no longer felt that she needed further treatment. The treatment ended just before COVID-19 was declared a pandemic. This is relevant as Sam was able to gain independence with eating in various settings that would not have been possible during the pandemic.
Discussion
There is a dearth of literature examining self-help and guided self-help in the field of eating disorders in the child and adolescent population. Thus, this paper adds an important discussion of the application of GSH-FBT. We have described how the treatment differs in therapeutic stance with the therapist acting as a coach in GSH-FBT. Sessions are shorter in duration, and the GSH-FBT coach continues to keep bringing the focus back to the homework at hand (videos and written material) rather than orchestrating behavioral change directly.
Advantages of this approach are numerous. The videos and reading material ensure that parents receive standardized and consistent therapeutic content. This lessens the onus on the therapist and can enhance dissemination of content that is standardized and maintains fidelity to FBT principles. In addition, the virtual nature of the treatment allows families in hard to serve areas to access treatment. Parents might even be in separate locations while they access sessions with their therapist. As siblings, and the patient themselves, are not required to attend, this might reduce the burden placed on young people. Furthermore, the material can be reviewed as many times as parents wish to do so.
Disadvantages of the treatment are also apparent. Parents often feel that their affected child should be involved in the treatment sessions, and should perhaps watch the videos or read the material. Although this is not prohibited, GSH-FBT coaches must communicate to parents that they are the key agents of change, and that it is not necessary for the child to be involved directly in sessions, as demonstrated by previous research on parent-focused FBT (Le Grange et al., 2016). Therapist coaches must remain efficient in directing parents back to video and reading material so as not to proceed into a full therapeutic session of FBT-V. In addition, the family meal session is not held within the session in GSH-FBT. This might prove to be a missed learning opportunity for FBT-V therapists as they cannot directly observe familial interactions during the meal and coach parents through a challenging moment. However, families may view the meal as awkward in FBT-V, particularly in a virtual sense, and may not be disappointed that there is no family meal in session in GSH-FBT. Of note, there is no family meal in parent-focused FBT (Le Grange et al., 2016), and effectiveness remains high.
Possible future applications of GSH-FBT might include its adaptation to a stand-alone treatment for those awaiting services or on a waitlist (ie. Self-help, without therapist coach involvement). Alternatively, GSH-FBT could be studied for those stepping up or down from more intensive services such as hospitalization. GSH-FBT could be an important element of a full continuum of treatment services for children and adolescents with AN. We do not know which factors determine who does well with less intensive treatment and who needs more intensive service. This could be a direction for future research. It is possible that GSH-FBT could become one tool in an armamentarium of a full complement of treatment options for early onset EDs in children and adolescents. Generalizing GSH-FBT to other ED populations in a transdiagnostic approach, such as those with Avoidant/Restrictive Food Intake Disorder (ARFID) or Bulimia Nervosa might be possible as there is some evidence that all eating disorders can be treated using FBT principles (Le Grange et al., 2003, 2015; Lock et al., 2019; Spettigue et al., 2018).
Although this paper describes the application of GSH-FBT in a single case, the descriptive detail of therapist dialogue may help others to apply the treatment themselves. To date, the content of videos is not widely disseminated, however, reading material is widely available in terms of the parent manual (Lock & Le Grange, 2015), and could be used in a guided fashion by therapist coaches to ensure that the therapeutic principles of FBT are communicated to parents in a standardized fashion. In summary, this paper is the first to illustrate the application of GSH-FBT in a practical and detailed manner, and differentiates GSH-FBT from FBT-V.
Footnotes
Acknowledgements
The authors would like to acknowledge the seminal contributions by Alison Darcy, PhD and Katherine Kara Fitzpatrick, PhD in creating the initial platform of materials for the online delivery of family-based treatment.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: JL receives royalties from Guilford Press and Routledge for books related to family-based treatment and is co-owner of the Training Institute for Child and Adolescent Eating Disorders that trains professionals in family-based treatment.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Davis Foundation.
Curriculum content for GSH-FBT.
Lecture 1: Act Now 1. Observing changes in your child 2. Get on the same page 3. The effects of starvation 4. Bradycardia 5. Other physical symptoms 6. How anorexia hijacks your child 7. It's not your fault but you are the solution 8. But how?
Lecture 2: Strategies 1. Expect & develop strategies for time 2. Expect and develop strategies for tantrums 3. Expect and develop strategies for threats 4. Expect & develop strategies for tricks 5. Strategies: Move closer & flank you child 6. Strategies: Mantras 7. Strategies: Don't try to reason 8. Strategies: Selective ignoring 9. One bite more
Lecture 3: More on Strategies 1. It's going to harder before it gets easier 2. Trial & error 3. Setting up an environment conducive to success 4. Try, keep trying, & know when to walk away 5. Strategies: Patience 6. How to talk to your child about what’s happening 7. Why you should be honest about the food you’re serving 8. Weight goals
Lecture 4: Staying the course 1. If it's hard, you are right where you should be 2. How anorexia is like cancer 3. Getting support & self care 4. Internet use in anorexia 5. Understanding ideal weight as a moving target 6. Remaining aligned 7. Understanding “externalization” 8. Externalizing analogies
Lecture 5: Reflection 1. Interview with a Recovery Role Model Part 1
Lecture 6: Phase 2 1. Transitioning to Phase 2 2. How do you know when you are ready? 3. How do you know when your child is ready? 4. Transition to phase 2 should be slow 5. Behavior matters 6. Expect uneven transition 7. Engaging the healthy part of your child 8. What is “healthy” in the context of anorexia? 9. Understanding "externalization"
Lecture 7: Phase 2 Strategies 1. Plating meals in phase 2 2. Dealing with setbacks 3. Behaviors to look for 4. Target maintenance, not causation 5. Remaining aligned
Lecture 8: Figuring it out in Phase 2 1. What to do when you don't know what to do 2. How to stay aligned 3. FILO: First in, last out 4. What it means to have an "ego syntonic" disorder 5. Continuing to separate your child from the illness
Lecture 9: Emerging from Phase 2 1. Developmental stage in phase 2 2. Healthy adolescent development 3. Healthy development: 9–13 yr olds 4. Healthy development: 14–16 yr olds 5. Healthy development: 17 & 18 yr olds 6. Interview with a Recovery Role Model II
Lecture 10: Getting Life Back on Track 1. Moving on from Phase 2 2. Dealing with setbacks 3. Tips for dealing with exercise and other behaviors 4. How to think about stress during this process 5. Schedule changes, summertime & sleep 6. Interview with a recovery role model III