
Abstract
Background
Young transgender or gender nonconforming (TGNC) children and adolescents or those with a gender dysphoria (GD) diagnosis show an increased risk of suicidal and nonsuicidal self-harming thoughts and behaviors (STBs). Data from German-speaking regions on this topic and studies comparing self- and parent-reported STBs have been scarce. The study aims were therefore to examine: (a) frequencies of self- and parent-reported STBs in a German clinical sample of children and adolescents with GD and (b) differences between age and gender groups, as well as between self- and parent-reports.
Methods
Two items from the Child Behavior Checklist (CBCL) and the Youth Self-Report (YSR) were used to assess self- and parent-reported STBs in a sample of 343 adolescents and 49 children who presented to the Hamburg Gender Identity Service (Hamburg GIS) between 2013 and 2019. Seventy-eight percent of the analysis sample was assigned female at birth (AFAB), and 22% were assigned male at birth (AMAB).
Results
Parents reported STBs on the CBCL for 16% and 6% of the cases in childhood and for 20% and 29% of the adolescent cases, respectively. STBs were self-reported by 38% and 45% of the adolescents who could report on the YSR. STBs were higher among adolescents than among children and in self-reports (YSR) compared to parent reports (CBCL). AFAB adolescents reported higher degrees of STBs than AMAB adolescents.
Conclusions
Children and adolescents with GD are a high-risk population for STBs, especially pubescent and AFAB individuals. Mental health professionals should screen early for STBs to prevent possible suicidal ideation-to-action transitions.
Introduction
Young transgender or gender nonconforming (TGNC) populations are faced with different challenges early in life. Youth with a gender dysphoria (GD) diagnosis (according to the DSM-5) often wish to undergo a social and medical gender transition to alleviate the experienced distress resulting from gender incongruence or a persistent identification with a gender other than the sex assigned at birth (American Psychiatric Association, 2013; Becker et al., 2017; Coleman et al., 2012). According to two population-based studies, between 1.8% and 2.7% of high school students from the US were identified as transgender (Johns et al., 2019; Rider et al., 2018), and in a survey from middle schools, 1.3% of students (grades 6–8) self-identified as transgender (Shields et al., 2013). For Germany, Becker et al. (2017) reported gender incongruence among 0.9% of adolescents aged 10–16 years old in a school-based population. Individuals assigned male at birth (AMAB) and identifying as female are often addressed as transfemale and those assigned female at birth (AFAB) and identifying as male as transmale (Newcomb et al., 2020). Gender experiences of TGNC individuals, however, can include a variety of gender identifications. Beyond the binary understanding of gender, TGNC individuals sometimes do not (entirely) identify as either female or male (i.e., nonbinary and genderqueer).
Children and adolescents with GD or who identify as TGNC report increased mental health problems (Becerra-Culqui et al., 2018; Connolly et al., 2016; de Graaf et al., 2018; Levitan et al., 2019; Newcomb et al., 2020; Su et al., 2016), including suicidal and nonsuicidal self-harming thoughts and behaviors (STBs) (Aitken et al., 2016; Arcelus et al., 2016; de Graaf et al., 2020; Grossman & D’Augelli, 2007; Heino et al., 2021; Skagerberg et al., 2013; Taliaferro et al., 2019; Thoma et al., 2019).
Suicide was defined as the second most common cause of death in youths in the general population in 2016 by the World Health Organization (World Health Organization, 2019). STBs are even more common in adolescents than actual suicides (Nock et al., 2013; Voss et al., 2019, 2020) and are associated with a broad range of negative (long-term health) outcomes (Brière et al., 2015; Resch et al., 2008; Steinhausen & Metzke, 2004). Suicidal thoughts or behaviors include suicidal ideation, plans and attempts with the intention to die (O’Connor & Nock, 2014). Nonsuicidal self-injury (NSSI) means self-harming without any intention to kill oneself and can function as a form of self-punishment or regulation of feelings and emotions (Claes & Vandereycken, 2007).
In the 1991 version of the Child Behavior Checklist (CBCL) or Youth Self-Report (YSR), two items can be used to assess STBs in children and adolescents from different (parental and youth) perspectives referring to the previous 6 months; however, these do not distinguish between suicidal and nonsuicidal behaviors (Achenbach, 1991a, 1991b). In a random general population sample from Germany, suicidal ideation/thoughts were reported by 3.8%, and self-harming behavior and suicide attempts by 2.9% of adolescents (aged 11–17 years old), with comparably lower parent-reported rates: 2.2% and 1.4%, respectively (Resch et al., 2008).
Among transgender populations, suicide rates are nearly four times higher than in the general population; for example, Wiepjes et al. (2020) reported 40 per 100.000 compared to 11 per 100.000 deaths in the Dutch general population. Existing studies have indicated an elevated risk for committing suicide in both transgender children and adolescents, as well as a high prevalence of STBs independent of the respective sample selection (general population, community-based or clinical samples; Surace et al., 2021). For example, in a recent meta-analysis, Surace et al. (2021) summarized the overall risk of suicidal behavior and NSSI for young TGNC clinical populations (age up to 25 years old) and found a mean prevalence of 28.2% for NSSI, 28.0% for suicidal ideation and 14.8% for suicide attempts. Aitken et al. (2016) conducted a study to examine the prevalence of suicidality and behavioral problems among children aged 3–12 years old referred to a gender clinic and compared these measures with three control groups: siblings, children referred to a clinic for other reasons, and nonreferred children. The group of gender-referred children was 15 times more likely to talk or think about suicide and 32 times more likely to engage in suicide attempts/self-harm than the nonreferred group. Among pubescent adolescent populations with GD, the prevalence of STBs is higher than that in prepubescent children, and there seem to be gender differences (Becker et al., 2014; Holt et al., 2016; Skagerberg et al., 2013). When examining transgender adolescents aged 10–17 years old, AFAB people were 144 times more likely to self-harm than a reference group of male youth. Similarly, suicidal ideation seemed to be 45 times more frequent in AFAB people than in reference males, and AMAB people were 31 times more likely to think about suicide than reference females (Becerra-Culqui et al., 2018). De Graaf et al., (2020) found that STBs were more frequently reported by AFAB adolescents than by AMAB adolescents. Additionally, some studies have found evidence for more suicidal and nonsuicidal actions in AFAB individuals and more suicidal ideation in AMAB individuals (Holt et al., 2016; Ream, 2019; Skagerberg et al., 2013; Toomey et al., 2018). In contrast, the results of Fisher et al. (2017) and Newcomb et al. (2020) showed that young AFAB individuals were more likely to think about suicide, while young AMAB individuals, in contrast, were more likely to carry out self-harming actions.
Aims of the study
Multiple studies from around the world have shown that clinical populations of TGNC youth or youth with GD present higher prevalence rates of different types of STBs. However, studies in this population remain scarce (Cha et al., 2018), and there have only been a limited number of clinical studies from the German-speaking part of Europe focusing on children and adolescents with GD (e.g., Becker et al., 2014; Levitan et al., 2019). The present clinical descriptive study aims to explore STBs in a German clinical population of children and adolescents aged 5–18 years old who received a GD diagnosis at the Hamburg Gender Identity Service (GIS) from different perspectives.
The following research questions are addressed in the present study: a) How often do parents of children and adolescents, as well as adolescents with a GD diagnosis, report different aspects of STB (self-harming behavior/suicide attempts vs. suicidal ideation/thoughts)? b) Do children (5–10 years old) and adolescents (11–18 years old) differ with regard to STBs (as reported by parents on the CBCL)? c) Do AMAB and AFAB children and adolescents differ regarding their STBs (as reported by either parent- or self-reports)? and d) Do parent- and self-reported degrees in suicidality scores (on the CBCL and YSR) reported for the adolescent population differ from each other?
Methods
Study design and sampling
The present study was part of a clinical research project addressing TGNC youth and those with a GD diagnosis in childhood (aged 5–10 years old) and adolescence (aged 11–18 years old), as well as their caregivers/parents, in a specialized clinical unit for GD at the University Medical Center Hamburg-Eppendorf (Hamburg GIS). The department provides specialized care to children and youths with questions around their gender identity when they self-identify as transgender or experience GD and related distress. A multidisciplinary team consisting of specialized psychiatrists, psychologists and endocrinologists provides assessment, diagnostic, psychotherapeutic and medical treatment for TGNC youth and their families. After several sessions with the child/adolescent and their caregivers, the corresponding clinicians complete a therapeutics-based questionnaire, including a DSM-5 checklist on GD criteria.
Data collection occurred during the first visit to the Hamburg GIS before receiving any treatment. All individuals who visited the Hamburg GIS between September 2013 and December 2019 (N = 859 families; 74% AFAB) were invited to voluntarily participate in a questionnaire-based research project. Written informed consent was obtained from all of the participants (including caregivers and adolescents themselves) according to guidelines from the local ethical institution.
The exclusion criteria for participation were insufficient understanding of the German language and a current severe psychiatric disease (e.g., psychosis). Figure 1 shows the referral rates, study participants and sex ratios at the Hamburg GIS. A total of N = 859 families were referred between September 2013 and December 2019. Of these families, n = 278 families chose not to participate, and n = 103 dropped out due to missing data. Furthermore, n = 51 families were excluded because they had sought help or treatment prior to attending the Hamburg GIS, and n = 35 did not fulfill the diagnostic criteria for GD (neither criterion A nor B of the DSM-5 definition). This process resulted in a total of n = 392 datasets eligible for study analysis. The final analysis sample consisted of n = 49 children (aged 5–10 years old) and n = 343 adolescents (aged 11–18 years old) with a diagnosis of GD or ongoing diagnostic procedure (TGNC) (see Figure 1). For a detailed description of the sampling and sample, please also refer to Levitan et al. (2019). Referral rates and study participation at the Hamburg gender identity service for children and adolescents.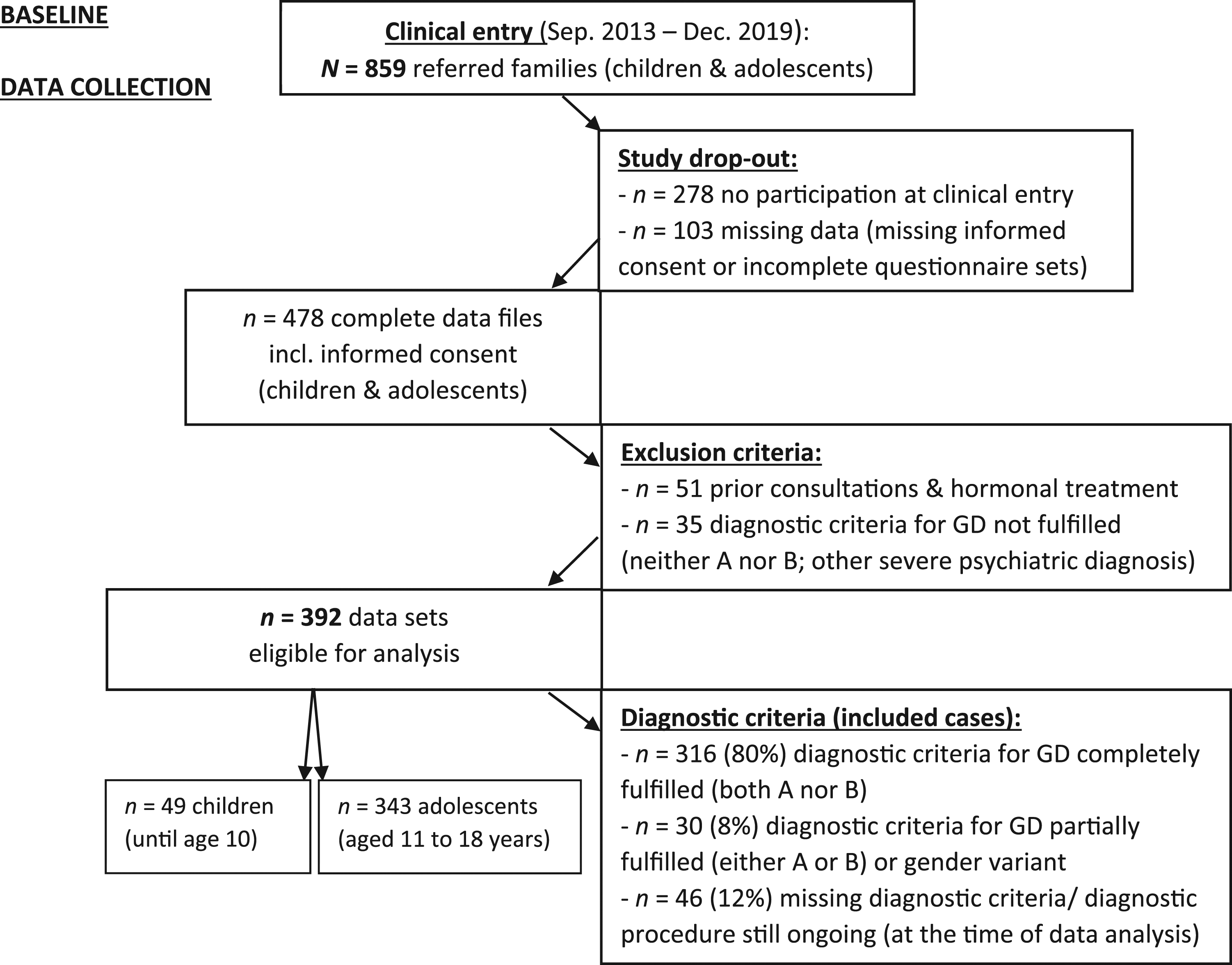
Measures
During their first visit, participating families were invited to complete a set of questionnaires that included, among others, a self-constructed questionnaire on sociodemographic characteristics and the German versions of the Child Behavior Checklist (CBCL; Achenbach, 1991a; Döpfner et al., 1998a) and the Youth Self-Report (YSR; Achenbach, 1991b; Döpfner et al., 1998b).
With regard to sociodemographic characteristics, the present study analyzed the age at assessment and the sex assigned at birth. For more sociodemographic details on a previous sample from the same study, please refer to Levitan et al. (2019).
The CBCL and the YSR are standardized measures for emotional and behavioral problems that are completed by caregivers/parents (for children and adolescents aged 4–18 years old) and adolescents (aged 11–18 years old), respectively. The German versions of the CBCL and YSR were found to be reliable and valid (Döpfner et al., 1994, 1995). For adolescents (aged 11 years old and older), both the YSR and CBCL were used to obtain self- and parent-reported information, whereas for children (5–10 years old), only the CBCL was used to obtain parent-reported information.
Suicidal and nonsuicidal self-harming thoughts and behaviors
STBs comprising either suicidal ideation or NSSI (self-harming behavior) and suicide attempts were assessed using the following two items from the CBCL (Achenbach, 1991a) or YSR (Achenbach, 1991b).
Self-harming behavior and suicide attempt
Intentionally hurting or attempting suicide was assessed using Item 18 from the YSR/11–18 (“I deliberately try to hurt or kill myself”). Item 18 from the CBCL/4–18 (“Deliberately harms self or attempts suicide”) was used to evaluate parent-reported perceptions of self-harm or attempts of their children to kill themselves. Like all of the items from the CBCL or YSR, Item 18 was rated on a scale from 0 to 2 (0 = “not true,” 1 = “somewhat or sometimes true,” 2 = “very true or often true”).
Suicidal ideation/thoughts
Item 91 from the YSR/11–18 (“I think about killing myself”) was used to measure suicidal ideation/thoughts directly via adolescents’ self-reports. Information was also obtained from a parent or other guardian asking whether their children ever talked about killing themselves using Item 91 from the CBCL/4–18 (“Talks about killing self”). Like all of the items from the CBCL or YSR, Item 91 was rated on a scale from 0 to 2 (0 = “not true,” 1 = “somewhat or sometimes true,” 2 = “very true or often true”).
Statistical analysis
Data were analyzed using SPSS software, version 22.0. Prevalence rates including 95% confidence intervals (95% CIs) were determined for self- and parent-reports and for self-harming behavior/suicide attempts and suicidal ideation, separately. An overall sum score out of Items 18 and 91 from the CBCL/YSR was created, resulting in the Sum Suicidality Index (SSI) with a range of 0–4 to compare degrees of different aspects of suicidality/STBs among children and adolescents and to evaluate gender differences and differences between the self-reported and parent-reported data. Group comparison was conducted using the t test. Tests were performed with a 2-sided alpha level of .05.
Results
Sociodemographic features
Sex ratio and age distribution in the total sample, in children (aged 5–10), and adolescents (aged 11–18).
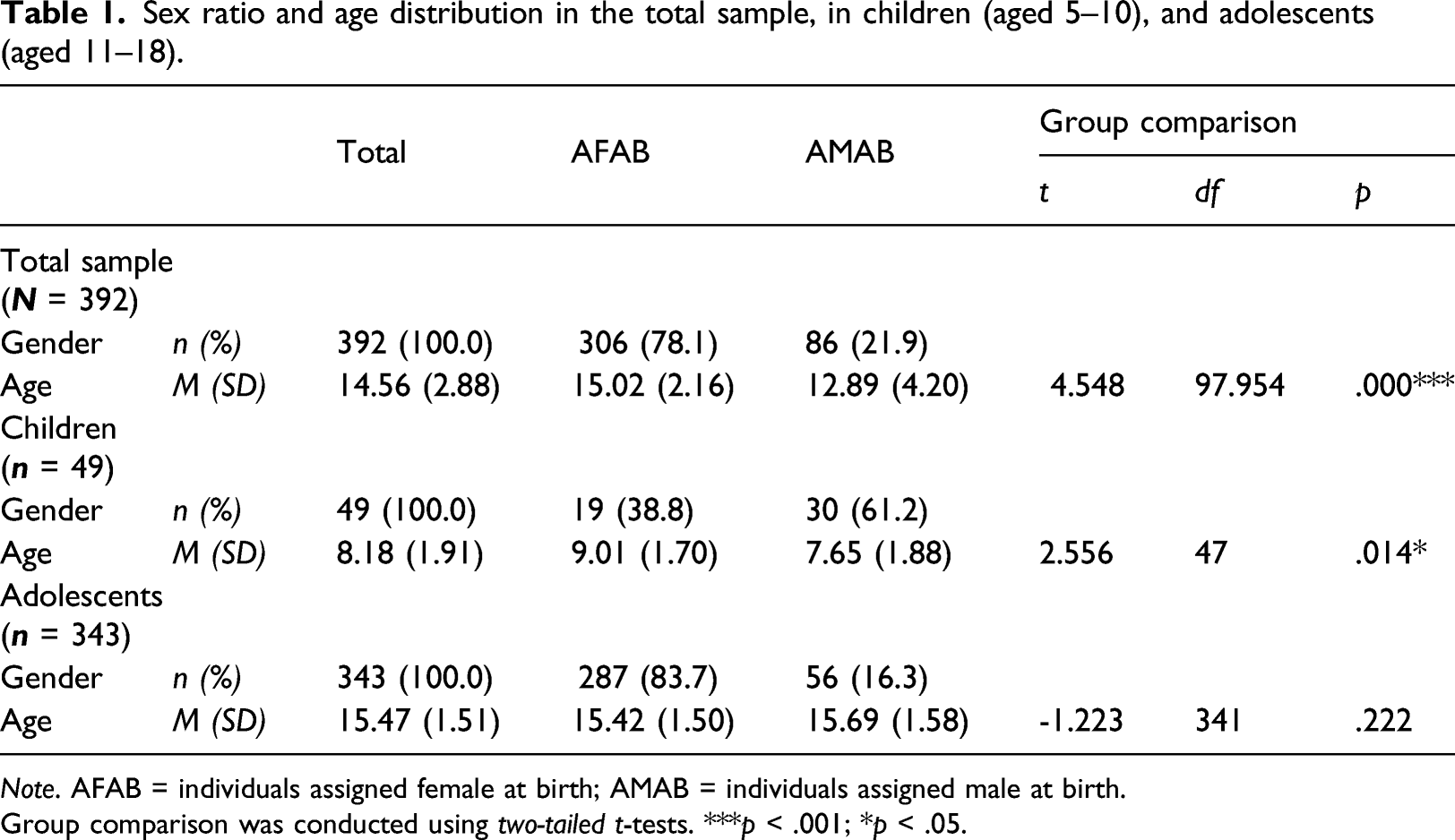
Note. AFAB = individuals assigned female at birth; AMAB = individuals assigned male at birth.
Group comparison was conducted using two-tailed t-tests. ***p < .001; *p < .05.
Suicidal and nonsuicidal self-harming thoughts and behaviors
Parent- and self-reported aspects of STBs in children (aged 5–10) and adolescents (aged 11–18) according to both CBCL and YSR
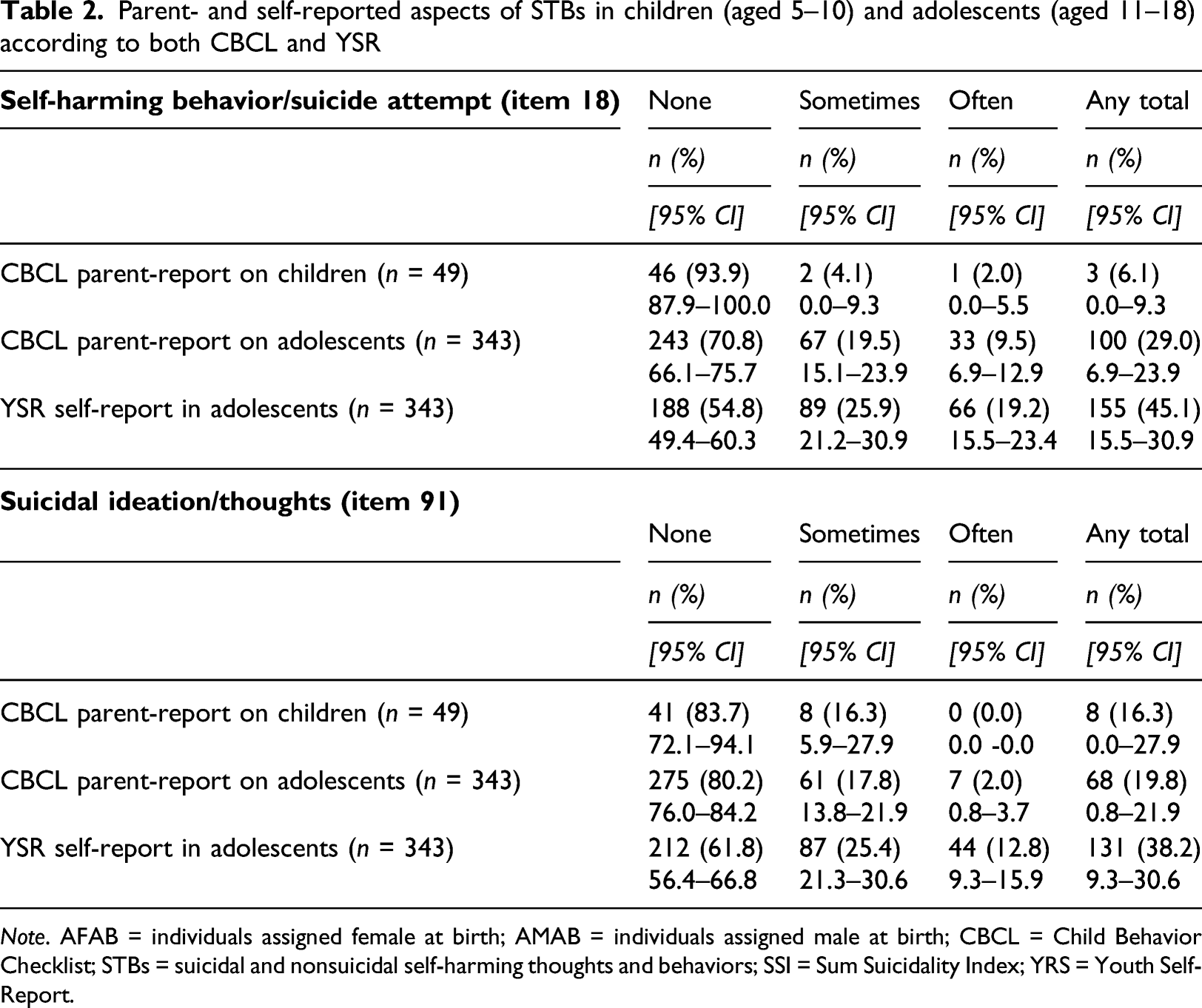
Note. AFAB = individuals assigned female at birth; AMAB = individuals assigned male at birth; CBCL = Child Behavior Checklist; STBs = suicidal and nonsuicidal self-harming thoughts and behaviors; SSI = Sum Suicidality Index; YRS = Youth Self-Report.
Frequencies of self-harming behavior and suicide attempts
Regarding self-harming behaviors and suicide attempts (Item 18), 2% of the caregivers/parents reported often and 4% sometimes such behaviors in their children (total: 6%). For adolescents, 9.5% of the parents reported often, and 20% sometimes reported such behaviors (total: 29%). Examining adolescents’ self-reports, 19% reported often and 26% sometimes such behaviors (any in total: 45%).
Frequencies of suicidal ideation/thoughts
Regarding suicidal ideation/thoughts (Item 91), none of the caregivers/parents reported often, and 16% reported sometimes suicidal ideation/thoughts for their children (total: 16%). For adolescents, 2% of the parents reported often, and 18% reported sometimes such thoughts (total: 20%). Examining adolescents’ self-reports, 13% reported often and 25% sometimes suicidal thoughts (total: 38%).
Sum suicidality index: Differences between age and gender groups
Comparison of degrees of suicidality/STBs between children (aged 5–10) and adolescents (aged 11–18) as well as self- and parent-reports according to the sum suicidality index (SSI)A.
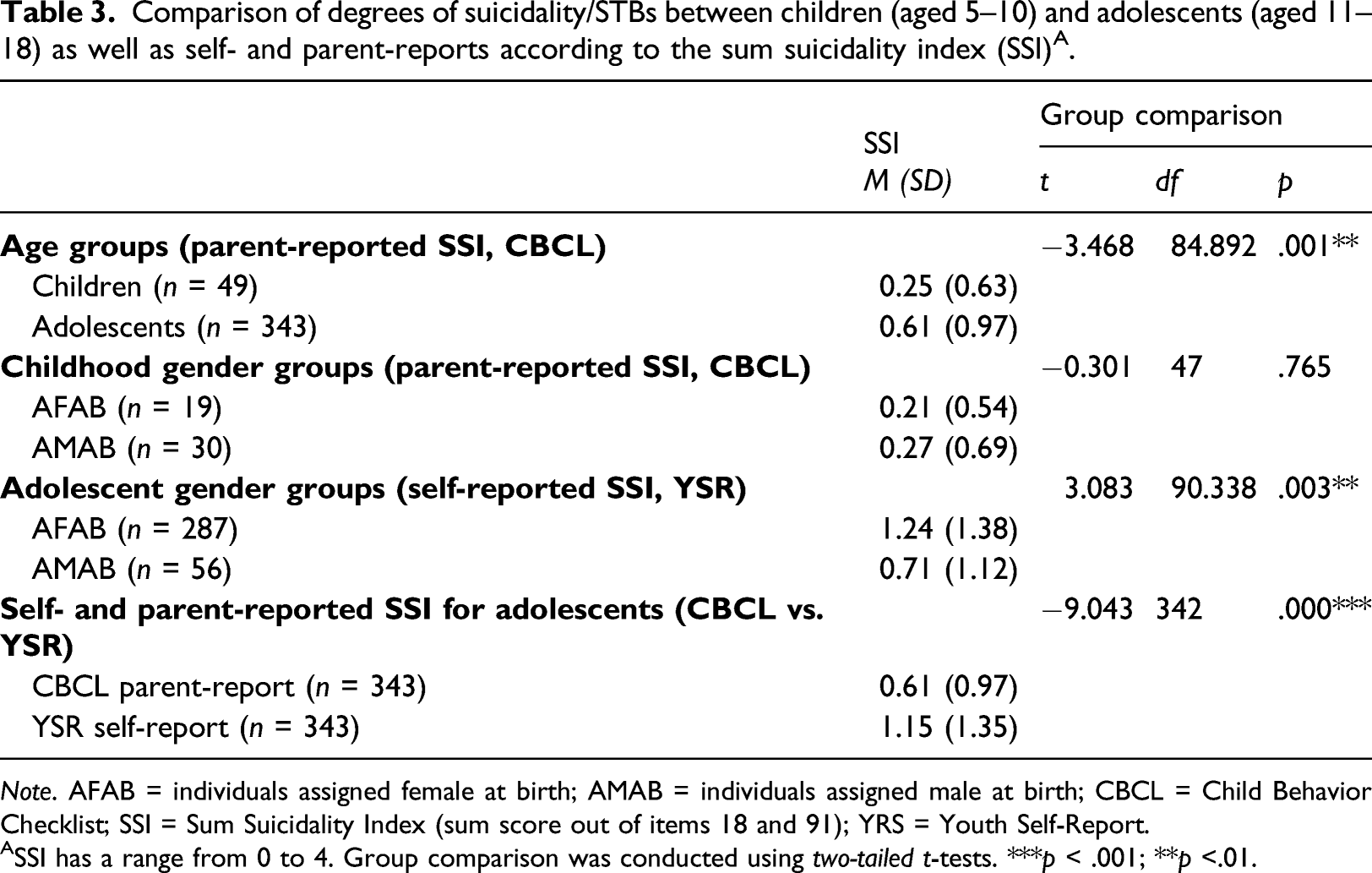
Note. AFAB = individuals assigned female at birth; AMAB = individuals assigned male at birth; CBCL = Child Behavior Checklist; SSI = Sum Suicidality Index (sum score out of items 18 and 91); YRS = Youth Self-Report.
ASSI has a range from 0 to 4. Group comparison was conducted using two-tailed t-tests. ***p < .001; **p <.01.
According to the evaluation of parent reports, the SSI reported by caregivers/parents for adolescents was M = 0.61 and M = 0.25 for children. The scores differed significantly from each other, implying that parents reported significantly less STBs for children than adolescents.
Comparing parent-reported outcomes of STBs between AFAB and AMAB children revealed similar SSI scores for both gender groups. The SSI was M = 0.21 for AFAB children and M = 0.27 for AMAB children, showing no significant differences.
AFAB adolescents self-reported the highest SSI of all groups (M = 1.24) and showed significantly higher SSI than AMAB individuals (M = 0.71).
Comparing adolescents’ self- and parent-reported SSI scores showed significant differences, revealing a significantly higher degree of STBs on the SSI for adolescents (M = 1.15) than in reports made by their respective caregivers/parents (M = 0.61).
Discussion
The current study addressed a gap in the existing literature considering STBs in clinically referred children and adolescents with GD from the German-speaking part of Europe. The aim was to examine prevalence rates of STBs or degrees of suicidality and differences between children and adolescents, gender groups and self-reported versus parent-reported outcomes in a large clinical sample of children and adolescents with GD. Our findings emphasize the high risk of STBs in both children and adolescents with GD, reported via both self- and parent-reports. Since information from both caregivers/parents and the clinically referred youth themselves was obtained for adolescents, this comparison of self-reported and parent-reported outcomes (YSR vs. CBCL) is a considerable strength of the study.
The present results on STBs reported by caregivers/parents of children aged 5–11 years old (6% reported self-harming or suicide attempts, and 16% reported suicidal ideation/thoughts on the CBCL) are in line with a similar study assessing children with GD conducted by Aitken et al. (2016), who reported approximately 7% and 19%, respectively, for Canadian children aged 6–12 years old. Holt et al. (2016) underscored these outcomes in another clinical study from the UK by showing that approximately 15% of their assessed children aged 5–11 years old engaged in suicidal thoughts, 2.5% in suicide attempts and 15% in self-harm.
GD can be exacerbated by puberty, thus leading to more mental health problems. This is in accordance with the current study, which indicated that adolescents reported even higher degrees of overall STBs than children. When the percentages of answers rated (1) or (2) were combined, a total of 45% of the adolescent sample self-reported self-harming or suicide attempts, and 38% reported suicidal ideation/thoughts (on the YSR) - nearly half of the sample. These numbers are similar to a recent cross-national study by de Graaf et al. (2020), who found that between 15% and 45% of their adolescent samples across different clinics in Canada, the Netherlands and the UK self-reported self-harming or suicide attempts, and 27%–55% reported suicidal thoughts. The results are also in line with previously reported numbers from a German chart review from the same clinic: Becker et al. (2014) reported that 40% of their clinical sample had experienced suicidal thoughts, 30% self-harmed, and 12% had attempted suicide in the past. Similarly, Holt et al. (2016) reported that approximately 40% of their adolescent sample had thoughts of killing themselves, 44% self-harmed, and 16% had attempted suicide.
Unfortunately, a distinction between self-harm and suicide attempts was not obtained in the current study due to assessment method limitations of the CBCL/YSR; therefore, a direct comparison with some of the previous studies could not be achieved. When comparing the present results to findings from a general population sample aged 11–17 years old from Germany; however (suicidal ideation/thoughts in approximately 4% and self-harming behavior in approximately 3% of the population; Resch et al., 2008), individuals with a diagnosis of GD showed an increased risk for STBs compared to the German normal population.
AFAB adolescents presented a higher mean value on the SSI and thus a significantly higher degree of STBs/suicidality than AMAB adolescents. This finding is in line with previous studies highlighting possible gender differences between AFAB and AMAB youth and possible consequences for their mental health (Arcelus et al., 2016; de Graaf et al., 2020; Fisher et al., 2017; Holt et al., 2016; Newcomb et al., 2020; Ream, 2019; Skagerberg et al., 2013; Thoma et al., 2019; Toomey et al., 2018). Arcelus et al. (2016) specifically observed NSSI among trans youth from the UK. The authors concluded that, although AMAB individuals might experience more stigmatization and preconceptions, AFAB youth might seem to cope differently with distress, apparently self-harming without any intention of killing themselves. Therefore, identifying the risks for the respective gender group and developing distinctive treatment concepts appear to be crucial in order to support each individual properly.
Furthermore, the present study underscores that caregivers/parents of adolescents with GD are often aware of the degree of suicidality or distress in their children, but differently than when addressing adolescents themselves. Since young TGNC individuals likely know best how they are feeling but might not constantly discuss their worries, family members might not always have correct insight into what is truly going on and might fail to predict risky behaviors, a result that has also been reported for the general population of youth in Germany (Resch et al., 2008). On the one hand, this result is therefore nothing “TGNC specific” but rather is “typical” for the sensitive period of adolescence. On the other hand, it highlights the need to include caregivers/parents or families in the treatment progress of youth with GD to facilitate support and mutual understanding (Levitan et al., 2019).
Limitations
The current study examined clinically referred individuals and so might have underestimated the true numbers of STBs in the German TGNC population since young individuals not seeking help because of their GD-related distress were not included. Furthermore, the significant difference in the sample size of AFAB (78%) and AMAB individuals (22%) tends to limit the conclusions of the study. We did not differentiate between possible transgender or nonbinary identities. In addition, the sample of children was relatively small compared to the adolescent sample, which might reduce the generalizability of the results.
The evaluation of STBs was based on only two items from the CBCL/YSR questionnaires, leading to another methodological limitation. Regarding Item 18 from both the CBCL and YSR, no distinction between a definitive indicator of suicidality, as in “attempting to kill oneself,” and a “self-harming behavior,” perhaps without any relation to suicidality, could be determined. These two terms were combined into one item, which did not allow for a differentiation between NSSI and actual suicide attempts.
Conclusions
As one of the first studies in the German-speaking parts of Europe assessing a large clinical sample of young individuals with a GD diagnosis, this study adds considerable value to the current state of the literature. The findings particularly emphasize the need to screen for signs of STBs in TGNC populations and to provide adequate care that tends toward possible mental health problems and suicidality in TGNC youth or those with a GD diagnosis. Different prevention approaches exist, although not specifically for this population (Zalsman et al., 2016). In this age group, the development of new technologies using real-life approaches might be a useful target. The present study does not draw conclusions about the source of suicidality in TGNC youth. However, external stressors, such as one’s own family and peers, have been identified as key factors in previous studies. Furthermore, enabling and improving access to care and treatment options for individuals with GD are essential. Future research is needed to help this population at risk to attend to STBs more adequately and to prevent suicide attempts. Identification of difficulties from the beginning and intervening at an early stage are key to the protection of TGNC individuals or those with a GD diagnosis.
Footnotes
Acknowledgments
We thank all the families who contributed to the study by participating in the first place and providing their personal information. We also thank all the clinicians and colleagues for their effort they put in the data collection and their contributions within the interdisciplinary team in Hamburg.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.