
Abstract
Background:
An estimated 10% of children and adolescents with chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) experience eating difficulties; however, little is known about why these difficulties develop, what the impact is or how to manage them.
Methods:
Semi-structured interviews were conducted with adolescents (aged 12–17 years) attending a specialist service who have a primary diagnosis of CFS/ME and experience nausea, abdominal pain and/or eating difficulties. A total of 11 adolescents were interviewed (eight female, mean age: 15 years). Transcripts were analysed thematically using techniques of constant comparison which commenced soon after data collection and informed further interview protocols.
Results:
Adolescents perceived their eating difficulties were caused by abdominal symptoms, being too fatigued to eat and changes to their senses of taste and smell. Some of the adolescents recognised how their eating difficulties were exacerbated and maintained by psychological factors of low mood and anxiety. The adolescents eating difficulties had a negative impact on their weight, fatigue, socialising and family life. They perceived helpful interventions to include modifying their diets, families adjusting and also medical interventions (e.g. medication). Adolescents identified that early education and support about diet and eating habits would have been helpful.
Conclusions:
If adolescents diagnosed with CFS/ME develop eating difficulties, this has a significant impact on their quality of life, illness and on their families. Not eating increases fatigue, low mood and anxiety which further exacerbates the eating difficulties. Clinicians should screen for eating difficulties in those with symptoms of nausea and abdominal pain, warn adolescents and their families of the risk of developing eating difficulties and provide interventions and support as early as possible.
Keywords
Introduction
Paediatric chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME) is defined as a disabling fatigue which is not relieved by rest, has lasted for more than 3 months and is not explained by other disorders, with between one and four additional symptoms, including muscle pain, nausea, cognitive dysfunction and sleep disturbance (Fukuda et al., 1994; National Institute for Health and Clinical Excellence (NICE), 2007; Royal College of Paediatrics and Child Health, 2004). The prevalence of paediatric CFS/ME is between 0.5% and 2.4% (Chalder, Goodman, Wessely, Hotopf, & Meltzer, 2003; Crawley et al., 2012; Nijhof et al., 2011; Rimes et al., 2007). CFS/ME is disabling with a negative impact on children’s schooling, mood and families (Crawley, Hunt, & Stallard, 2009; Crawley & Sterne, 2009; Jelbert, Stedmon, & Stephens, 2010; Missen, Hollingworth, Eaton, & Crawley, 2012; Velleman, Collin, Beasant, & Crawley, 2015).
Over 50% of young people with CFS/ME experience nausea and/or abdominal pain (Davies & Crawley, 2008). Nausea and abdominal pain are associated with headaches and dizziness in a ‘migraine phenotype’ of CFS/ME which was associated with worse anxiety, physical function, pain and school attendance in comparison to two other CFS/ME phenotypes (May, Emond, & Crawley, 2010). The presence of abdominal symptoms is associated with eating disorders in other chronic illnesses such as cystic fibrosis and celiac disease (Abbott et al., 2007; Karwautz et al., 2008). Although anecdotally, children with CFS/ME have problems eating, little is known about why problems develop or how clinicians and their families can support them.
The aim of this study was to explore what adolescents felt had caused their problems with eating, whether there were triggers and maintaining factors and what interventions they felt would be helpful.
Method
Sample
The sample was drawn from a CFS/ME specialist hospital service providing regional support for assessment and treatment of over 300 children a year in the Gloucestershire, Bristol, Wiltshire and Somerset areas, covering a population of around 400,000 children aged 5–19 years (Office for National Statistics, 2011).
Adolescents were invited to participate in the study by the CFS/ME clinical team if they had a diagnosis of CFS/ME, were aged between 12 and 18 years and experienced at least one of the following: difficulty with eating, frequent nausea, lack of appetite, weight loss, abdominal pain, bloating, diarrhoea or constipation. Adolescents were not eligible for this study if (1) they were housebound, (2) if they did not speak sufficient English to read and understand the recruitment forms, (3) if they did not have CFS/ME as their primary diagnosis or (4) if they had an additional diagnosis that would otherwise explain any eating difficulties.
Data collection and analysis
Potential participants were identified as being eligible by their clinician, who explained the study. Interested adolescents opted-in to the study by contacting the researcher. If, after further information was given by the researcher, the adolescent continued to be interested, an interview was arranged. Recruitment continued until data saturation was reached, meaning the researcher had gained an adequate understanding of the concepts and themes that have emerged and no new information was emerging from interviews (Watling & Lingard, 2012).
The interview topics included the adolescents’ experience of eating; the factors they felt caused and exacerbate eating difficulties and what they believed were helpful strategies. Interviews lasted approximately 30 minutes and were audio-recorded, transcribed verbatim and analysed thematically (Braun & Clarke, 2006).
We followed the six key steps of thematic analysis outlined by Braun & Clark (2006). We familiarised ourselves with the data by transcribing, reading and rereading the transcripts. The transcripts were coded, and to check coding reliability, they were independently double-coded by one of three different researchers (S.H., L.B. and J.B.) who met regularly throughout the process of analysis to discuss emergent themes. Areas of disagreement were discussed and resolved with reference to the raw data. Codes and themes were regularly discussed with a CFS/ME specialist (E.C.) and a child psychiatrist (M.G.). Interview transcripts were then imported into the NVivo Qualitative Data Analysis Software (2010), where the data were systematically assigned codes, as a result of the double-coding process. Analysis started soon after data collection commenced and was an ongoing and iterative process using methods of constant comparison (Glaser & Strauss, 1967). Themes were then reviewed and refined, with reference to the entire data set. We discarded and merged themes reducing our seven initial themes to four themes. Themes were defined, structured and named to ensure they reflected the raw data as accurately as possible.
The trustworthiness of this research was enhanced using this explicit and pragmatic method of thematic analyses. We were particularly interested in contrasting themes and different views. Constant comparison methods are derived from a grounded theory approach (Glaser & Strauss, 1967). We chose an inductive thematic analysis because of the lack of previous research in this area. We felt it was important that themes emerged from participant accounts (Patton, 1990) as opposed to a theory-driven thematic analysis that could have been used if there had been existing knowledge and theory.
Ethical approval
This study was given a favourable opinion by the Grampian National Health Service ethics committee: Research Ethics Committee (REC) number 14/NS/0062 on 09/05/2014.
Results
Participants
A total of 11 adolescents aged between 13–17 years (mean age: 15 years) were interviewed, eight of whom were female. All adolescents were given the option to be interviewed alone or with a parent and seven chose to have their mothers present, all of whom contributed to the interview. Verbatim quotes from participants (P) and mothers (M) are used to illustrate themes. Table 1 describes five themes and subthemes which emerged from the data.
Themes and sub-themes.
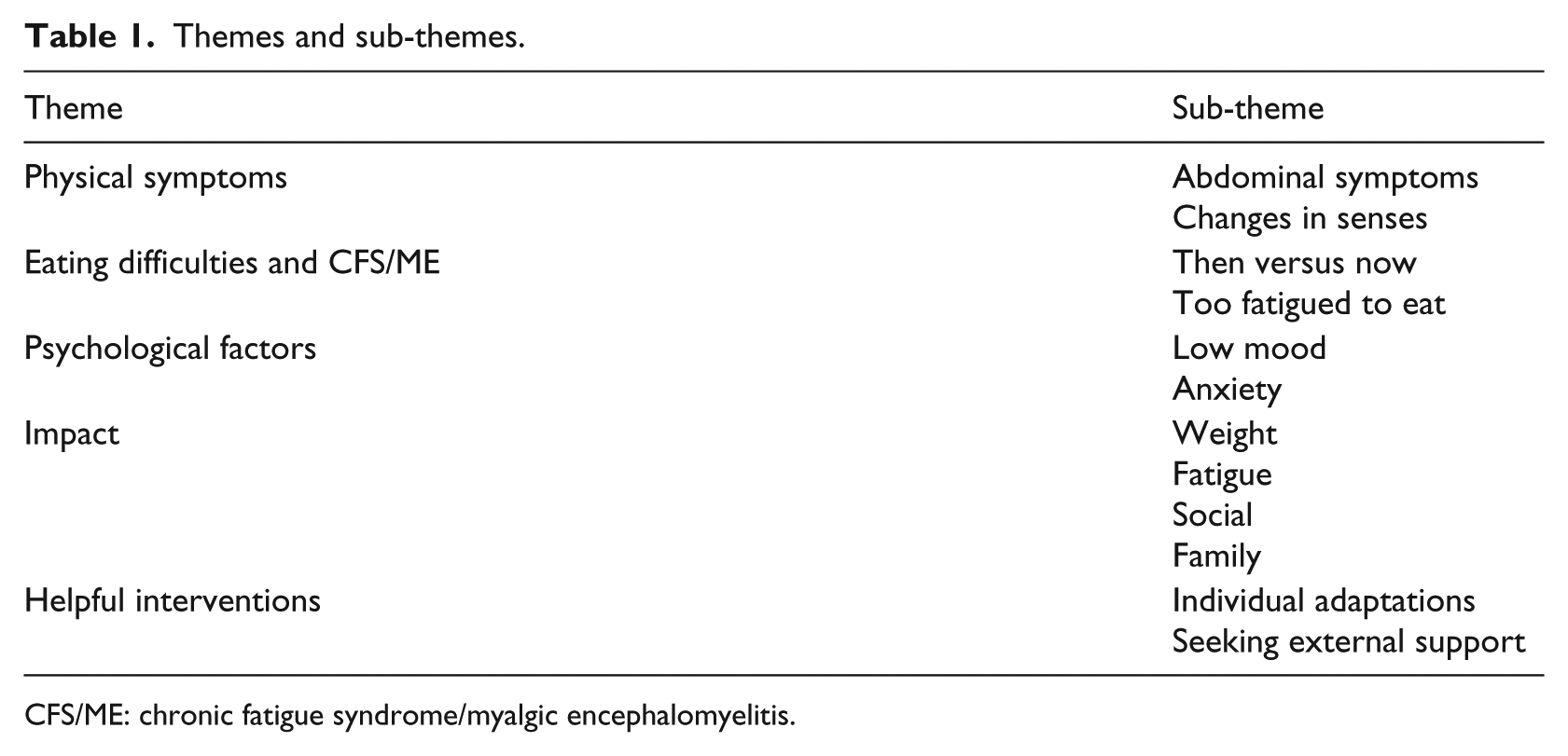
CFS/ME: chronic fatigue syndrome/myalgic encephalomyelitis.
Physical symptoms
Abdominal symptoms
In some cases, adolescents described abdominal symptoms which they perceived were caused by eating such as ‘bloating’ (P2, P4), ‘indigestion’ (P6), ‘stomach cramps’ (P4) and ‘stomach pain’ (P2, P3, P5, P6, P7, P11):
If you have a cut . . . and someone ground their finger against it, it’s like that . . . so it wasn’t nice at all and that’s why it felt so sore, it was like your whole inside was cut. (P2)
Adolescents also experienced symptoms which they thought were unrelated to eating. For example, every adolescent experienced severe nausea which they perceived as a CFS/ME symptom. Seven explicitly stated nausea as a ‘permanent’ (P2, P7) or ‘main symptom’ (P9, P5, P8, P10, P11) of their CFS/ME illness, above fatigue. The adolescents experienced extensive and frequent episodes of nausea alongside sickness-associated symptoms such as ‘burping’ (P2) and a ‘watery mouth’ (P7) which they had not experienced prior to the onset of CFS/ME. Only three adolescents had vomited. Nausea prior to eating often caused the adolescents to perceive that eating would make it worse or induce vomiting. Therefore, they did not want to eat or even feel that they could eat, thus exacerbating eating difficulties:
Feeling sick before you even eat, you don’t wanna eat when you feel sick, it just makes it worse. (P7)
Changes in senses
Seven adolescents noticed a change in smell or taste (or both). This highlighted the major contrast in adolescents’ relationship with food from their pre-CFS/ME selves who had a healthy appetite and ‘loved’ (P2, P7) and ‘enjoyed’ (P9) food. This is in contrast to adolescents who now experienced repulsions to foods that used to be ‘old favourites’ (M9). They also could not stand the smell of certain food cooking because this was associated with nausea:
Smelling certain foods makes me feel like as sick as if I had eaten it. (P9)
Previously loved foods became ‘tasteless’ (P5), ‘disgusting’ (P5, P7) or ‘overly sweet’ (P9). Changes in food textures resulted in the adolescents not being able to swallow foods and often refused to eat them thus reducing the variety and quantity of food eaten. The adolescents perceived these physical changes in their senses were attributed to the onset of CFS/ME. The adolescents explained they had not experienced such severe repulsion to smell or taste previously and parents reported a transformation in the adolescent’s attitudes towards food and meal times.
My eating difficulties
In all, 9 of 11 adolescents experienced eating difficulties and illustrated these problems through highlighting comparisons with their past eating behaviours.
Then versus now
Those who had problems eating compared their current eating difficulties with a time prior to CFS/ME. They said they ‘loved’ (P2, P7) and ‘enjoyed’ (P9) eating and were ‘foodies’ (P5, P2), with ‘good’ (P1, M10), ‘healthy’ (P9) appetites. The time prior to CFS/ME was used as a reference point for normality emphasising the adolescent had not always had these difficulties. This was consistent with parental views who had seen a ‘real change’ (M5) in their child’s eating. Not only had the adolescent previously enjoyed food but they ate vast quantities suggesting the adolescents’ eating had not caused concern for their families prior to CFS/ME:
Before I had the chronic fatigue I used to eats loads and I used to just never stop eating. (P4)
In comparison to this ‘normal’ time, the current eating behaviours are very different. Adolescents described being fuller quicker, often blaming a ‘smaller appetite’ (P1, P4, P6, P9) or a ‘shrunken stomach’ (P1, P2, P5) and, therefore, portion sizes of meals had considerably reduced. In addition, some adolescents spoke of frequently skipping meals altogether (P1, P5, P2, P7, P11) causing a reduction in food intake.
Too fatigued to eat
Eating was described as an activity that used up ‘too much energy’ (M8) and on the occasions they felt they had limited energy, eating was significantly reduced:
I’m thinking ‘I could make food or I could go to bed and go to sleep and eat in the morning’ and just going to bed usually wins. (P1)
This often happened during periods of ‘pay-back’, a term used to describe when someone with CFS/ME has overdone activity and experiences an increase in symptoms. During these periods, eating was minimised as the adolescents said they did not feel hungry and that eating was ‘not a priority’ (P4) as they were ‘too tired’ (P2, P11) or ‘sick’ (P6) to eat:
When you’re so tired, you can’t be bothered to pick up a knife and fork and just eat. (P7)
Psychological factors
Although explanations of eating difficulties were physical in nature, adolescents described how emotions, such as low mood and anxiety, exacerbated and maintained their eating difficulties.
Low mood
Comorbid low mood was experienced by four adolescents who described a complicated relationship between low mood, fatigue and eating. Feeling low meant that adolescents were sometimes ‘not being bothered to eat’ (P1, P5, P7):
I’d rather just do nothing than go get food because it’s easier because my health is the last thing I am thinking about when I am in a low mood. (P1)
Furthermore, their mood lowered when others ate foods they felt they should be able to eat or wished that they still could eat which resulted in them feeling ‘lonely’ (P5), ‘envy’ (P5) and ‘annoyed’ (P2, P3, P5, P6). Eating difficulties fuelled negative emotions of ‘frustration’ (P2, M7), ‘anger’ (P7), ‘scared’ (P2, P5, P7), ‘embarrassment’ (P7) and ‘worry’ (P2, P3, P4, P6, P7, P8, P9, P11) which increased the adolescents’ negative relationship with food. Some recognised that not eating made their CFS/ME symptoms worse, which then had a negative impact on their mood, meaning that low mood could be both a cause and a consequence of eating difficulties:
If you don’t eat, you’ll get worse and if you get worse your attitude towards a lot of things will go down a lot. (P5)
Anxiety
Nine adolescents experienced anxiety and worry which they attributed to their eating problems and the associated symptoms. Some adolescents recognised that anxiety increased the nausea reducing their ability to eat:
If I feel more anxious, I feel more sick and then I probably won’t want to eat. (P9)
Adolescents interpreted nausea as a sign that they would vomit imminently, even though most had never vomited. This contributed to anxiety prior to meal times, and they described feeling ‘worried’ (P2, P3, P4, P6, P7, P8, P9) and ‘afraid’ (P2) before eating, enhancing the negative association with food:
It’s like a feeling of perceived danger of being sick so I am assuming I will be sick if I eat something. (P4)
Impact
Eating difficulties impacted the adolescents’ health affecting their weight, fatigue and their broader social and family circumstances.
Weight
Seven adolescents lost weight since the onset of CFS/ME which families thought was because of their eating difficulties. One adolescent lost five stone over a year and another was referred to an eating disorders team. Weight loss was one of the most ‘scary and dramatic’ (M2) consequences for the parents. Weight loss was also most common at the beginning of the illness, often before an official CFS/ME diagnosis was given, and before eating became ‘stable’ (P9) as they understood and managed their CFS/ME more effectively and discovered the factors which relieved their eating difficulties (see ‘helpful interventions’).
Fatigue
All adolescents understood the important link between eating and fatigue. They appreciated that their restricted diets had reduced their ‘nutritional’ (P2) and ‘vitamin’ (P7) intake therefore impacting overall health. Eating difficulties had been linked to feeling ‘weaker’ (M5) and ‘worse’ (P2, P3, P5) while improved eating was related to ‘improved energy’ (P2, P5, P6, P7) and ‘making me better’ (P5, P7, P8, P11):
If like my eating is bad it’ll makes me more tired and everything else worse and if everything else is worse that will make my eating worse. (P3)
Social
Eating difficulties had a negative impact on socialising as when their peers invited them to restaurants; the adolescents would commonly ‘cancel’ (M7) or ‘be reluctant’ (P9) to accept the invitation and therefore miss opportunities to socialise and spend time with peers. The adolescents said they might not find anything to eat at the restaurant, they would not be able to eat very much or they would feel too sick because of the intense smells.
For the younger adolescents who would typically visit each other’s houses, the social impact differed. Although the adolescents felt they knew their friends’ parents well enough, they believed these parents could not accommodate their nausea and specific food requests as well as their own parent. Therefore, social events were limited and reliant on their friends coming over to their own house to stay close to ‘safety’ (P9):
Obviously their parents don’t really know what would happen or what they’d need to do, I mean they understand but they don’t. I’d just prefer to be here [home]. (P8)
Several of the adolescents felt their friends and family were ‘monitoring’ (P2) what they ate, particularly those who had previously lost weight due to their eating difficulties. This created feelings of ‘pressure’ (P2) and ‘tension’ (M7) at meal times adding to the negative experience of social eating.
Family
Mothers reported feeling ‘scared’ (M2), ‘awful’ (M8), ‘angry’ (M7), ‘stressed’ (M1, P7) and ‘terrified’ (M2) by the dramatic weight loss and ‘real change’ (M5) in their child’s health as a consequence of poor eating. Families adapted by helping the adolescents to eat whatever they could, when they could, meaning extra, specific food was purchased, and meal preparations took longer as separate meals were required: one for the adolescent and one for the rest of the family. These logistical and emotional impacts were made worse if the adolescent struggled with the smell of their families’ food cooking, to sit at the dining table with the rest of the family or refused to eat altogether. Impact on siblings was seldom mentioned, and the adolescents did not always have full insight into how their eating difficulties affected their parents:
If I’m cooking for other people I gotta do hers first . . . cause if she smells me cooking theirs, it puts her off before she has her meal. (M7)
Helpful interventions
Adolescents and their mothers described a variety of interventions that they thought were helpful. These were a mixture of individual adaptations (change to diets, distraction and relaxation techniques and family adjustments) and those suggested from clinicians (medication, alternative therapies and future interventions).
Individual adaptations
Adolescents frequently excluded various dietary items such as diary, gluten and sugar, claiming these created greater digestive disturbances, although they had not been given a medical explanation for this. Other food types such as ginger, carbohydrates and protein had been increased due to perceptions they ‘ease’ nausea (P3), ‘settle my stomach’ (P6) and minimised the effect of food to the digestive system. Diet was also adjusted because food offered by parents had to be what the adolescent ‘fancied’ (P1, P5, P6, P8, P9) or ‘craved’ (P5) as other food made them feel sick and they were usually unable to eat it. The four adolescents who had not lost weight appeared to adapt to their nausea more effectively as they had continued to eat, even when feeling sick, as long as they were given food they wanted:
We’ve noticed that you suddenly get feeling very sick quite quickly and you need to eat quickly and it has to be what you fancy. (M8)
Chicken was a favourite food that was regularly requested by most adolescents; however, there were few similarities amongst other food choices. Adolescents appeared very vocal and knowledgeable about the foods they felt able to eat.
Distraction and relaxation techniques were useful for six adolescents when they were struggling to eat. Two of these adolescents had compromised with their parents to adjust meal routines, so they could be distracted by television or relax through eating alone, away from the dining table and the rest of their families. After meals, when the digestive disturbances were at their worst, playing with pets or focusing on their breath and lying down was also used to relax and distract:
Mum does let me eat on the sofa watching telly so I am relaxed when I eat, and then that makes me eat more because like I’m not tense and I am not even thinking about it. (P7)
Many parents developed protective strategies such as pre-empting when their child would feel nauseous and offer them food to ‘curb’ (M5) it, eating slowly as a whole family so the adolescent with CFS/ME can ‘keep up’ (P4), ordering a child’s portions when eating out and relaxing family meal structures.
Seeking external support
Some of the families described seeking external, professional support for the adolescents eating difficulties. Five adolescents took prescribed sickness or stomach acid relief medication which they found helpful. However, it was not common to have been offered medication to relieve their symptoms which frustrated some adolescents:
be less reluctant to let us try things [medication], because they were so reluctant and you thought well if it doesn’t work then fine but can we at least try it. (P2)
Most of the families did not explicitly discuss consideration of medication or alternative therapies. Some families sought diverse treatments such as acupuncture, dietician input, sickness bands and the emotional freedom technique, while others spoke to their CFS/ME clinician for advice. External support varied greatly in perceived accessibility and helpfulness; therefore, outcomes across participants were inconsistent.
Families felt education about CFS/ME, and its associated eating difficulties should be routinely offered by healthcare professionals. Parents felt it would help to know eating problems are ‘normal’ (M1) in this population and may help them to understand the illness further. Practical advice such as ‘recipe booklets’ (M5), ‘cooking classes’ (M5) and ‘guidelines on what I should and shouldn’t eat’ (P4) were also suggested as possible helpful interventions.
Discussion
This study gains an important insight into how eating difficulties can impact the quality of life for adolescents with CFS/ME and their families, as eating difficulties were found to have a negative impact on the adolescents’ weight, fatigue, socialising and family life. The adolescent’s perceptions suggest the possibility that their eating difficulties were caused by abdominal symptoms, their fatigue hindering an ability to eat and sensory changes (taste and smell). Furthermore, some of the adolescents interviewed felt that their eating difficulties were exacerbated and maintained by psychological factors (low mood and anxiety). Potential interventions were described by the adolescents and their families, including a mixture of individual adaptations (such as dietary changes, relaxation and distraction techniques and family adjustments) as well as clinician suggestions (including medications, alternative therapies and future interventions).
Results in context of previous literature
Families in this study used the time prior to CFS/ME when there were few problems with eating to contrast with their current problems. We are unaware that this has been described previously. Historically, CFS/ME has been an illness surrounded by controversy and adolescents with CFS/ME experienced disbelief from others and feared judgement regarding their illness (Jelbert et al., 2010; Webb et al., 2011) The diagnosis can be stigmatising partly due to the poor understanding of the aetiology (Asbring & Narvanen, 2002), and families may develop strategies to protect themselves from judgement, blame or disbelief and to portray the severity of CFS/ME (Guise, Widdicombe, & McKinlay, 2007). Alternatively, comparisons to pre-CFS/ME may be triggered by a grief process, whereby families reflect on how simple and enjoyable eating used to be. Previous research suggests that adolescents with CFS/ME experienced a sense of loss as a consequence of their illness (H. Fisher & Crawley, 2013). In particular, adolescents miss the activities they used to enjoy (Jelbert et al., 2010), which may explain why the families in this study put such importance on eating being a previously loved and enjoyable activity.
Both adolescents and their mothers had a physical and medical focus when describing the cause of the eating difficulties, possibly due to the presence of dominant physical symptoms. The three perceived causes (abdominal symptoms, being too fatigued to eat and changes to senses) were understood by families to be triggered by the CFS/ME. Furthermore, adolescents talked about experiencing cravings and having to eat what they fancied; therefore, it is possible there could be biological underpinnings of their food choices. Hyper-sensitivity to noise and light are recognised symptoms associated with CFS/ME and loaded onto the same CFS/ME phenotype (called ‘migraine’; phenotype 2) as nausea and abdominal pain (May et al., 2010). It is possible smell and taste are affected by CFS/ME in a similar way to that of sound and sight. These biological symptoms could be explained by chronic stress. Chronically stressed mice exhibited increased signs of anxiety and developed ‘sickness behaviours’ (Kent, Bluthé, Kelley, & Dantzer, 1992) with associated symptoms such as general malaise, fatigue, fever and sleep changes (Dantzer & Kelley, 1989). Sickness behaviour is also related to a reduction in food intake and a lack of weight gain due to the physiological response to chronic stress (Tannenbaum, Tannenbaum, Sudom, & Anisman, 2002). This theory may explain why the adolescents in this study developed aversion to food smells and tastes as eating priorities may be physiologically reorganised when sickness behaviours intensify to facilitate recovery from an illness (Dantzer & Kelley, 2007).
Previous studies have found that the presence of abdominal symptoms is associated with eating pathology in cystic fibrosis and coeliac disease (Abbott et al., 2007; Karwautz et al., 2008). However, there is very little identifiable literature on co-morbidity between CFS/ME and eating disorders (M. Fisher, Krilov, & Ovadia, 2002; Griffiths, Beumont, Moore, & Touyz, 1996). This study did not identify eating disorder behaviour or cognitions such as fear of weight gain as contributing to the eating difficulties, in contrast to reports in other chronic conditions (i.e. Karwautz et al., 2008). The lack of eating disorder behaviours and cognitions lends support to the hypotheses that eating disorder behaviours are an unusual occurrence in CFS/ME and should prompt diagnostic review (Griffiths et al., 1996).
Many of the adolescents discussed experiencing anxiety, in particular, catastrophising thoughts in relation to their nausea, which they perceived impacted on their eating. Previous research suggests that catastrophising can increase symptom perception in patients with fibromyalgia (Hassett, Cone, Patella, & Sigal, 2000). The adolescents in this study worried that nausea meant imminent vomiting even though most had never vomited as a result of their CFS/ME. Therefore, these catastrophised cognitions often caused the adolescents to avoid certain foods they believed would cause or make the nausea worse. The selective attention and vigilance for vomiting is likely to exaggerate the feelings of nausea in a ‘vicious circle’ (Veale & Lambrou, 2006). This is especially true when coupled with anticipated negative consequences. In relation to this study, although nausea is a recognised symptom of CFS/ME, there is a possibility that anxiety about vomiting could exacerbate the adolescent’s experiences of the eating difficulties. As explained by an adolescent, ‘It’s like a feeling perceived danger of being sick so I am assuming I will be sick if I eat something’ (P4).
Implication for clinical practice
Adolescents with CFS/ME attending medical appointments and receiving treatment should be routinely screened for eating difficulties. If eating difficulties are found, adolescents should be reassessed regarding their perception of the cause as well as for anxiety and depression, and treatment should be tailored appropriately. Information should also be provided to warn of the risk of developing eating difficulties and provide interventions and support as early as possible for the adolescent and their family. Further research needs to investigate the relationship between eating, CFS/ME and family interactions.
Strengths and limitations
Qualitative methods were used for this study, as we are not aware of other studies exploring eating difficulties in paediatric CFS/ME and we wanted to understand more about adolescent’s experience of eating problems and the relationship with fatigue in this complex disorder. We recruited adolescents with abdominal symptoms which may explain why all the children had nausea. Therefore, these results may not be generalisable to those without abdominal symptoms. As adolescents were recruited from a specialist CFS/ME clinic, study findings are not generalisable to primary, secondary or adult services. We continued recruiting until data saturation was reached as during the last three interviews; no new themes emerged. As seven adolescents choose to have their mother present in the interviews, this may have changed the information obtained. However, adolescents who were interviewed with their mother present appeared to provide more information and greater insight regarding their difficulties and their parents contributed interesting perspectives. As no fathers were interviewed, their perceptions and experiences of their child’s eating difficulties were not identified and they could have provided a different perspective to that of the mother and adolescent.
Footnotes
Acknowledgements
We are extremely grateful to the families who took part in this study and to the staff at the chronic fatigue syndrome (CFS/ME) specialist hospital service. Thank you for your contributions, time and support. We would like to thank Professor Julie Barnett, University of Bath, for her support and guidance.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.