
Abstract

Carotid artery atherosclerosis, accounts for one-third of ischemic strokes in the population. 1 In patients with carotid artery disease and indication for surgical repair, open carotid endarterectomy (CEA) is the first-line treatment. 2 However, in patients who are unfit for CEA, carotid artery stenting is a possible alternative. Anatomic variations of the extracranial internal carotid artery (ICA), such as high carotid bifurcation or abnormal ICA trunk, may be considered as relative contraindications to open repair.1,2 About 30% of all ICAs have anatomic abnormalities; however, they rarely affect preoperative planning. 3
A 68-year-old man was admitted for elective treatment of an asymptomatic 80% carotid artery stenosis. Preoperative computed tomography angiography (CTA) revealed that the right ICA was positioned posterior to the cricothyroid cartilage, at the level of its origin, just distal to the carotid bifurcation as shown in Panel A (dashed arrows indicate common [CCA], internal, and external [ECA] carotid arteries; solid arrows indicate the cricothyroid cartilage). Panel B displays the digital subtraction angiography images, indicating high-grade stenosis of the ICA.
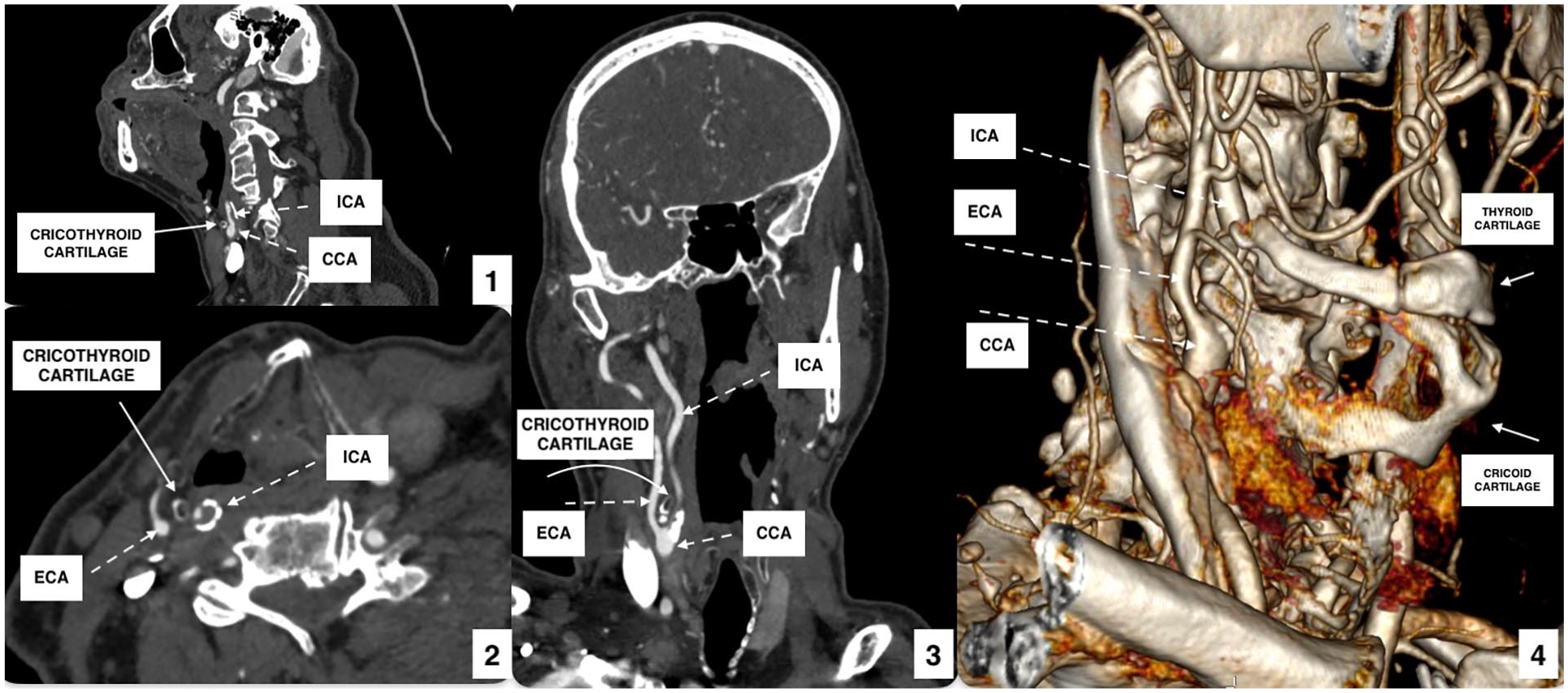
Panel A is in color online.
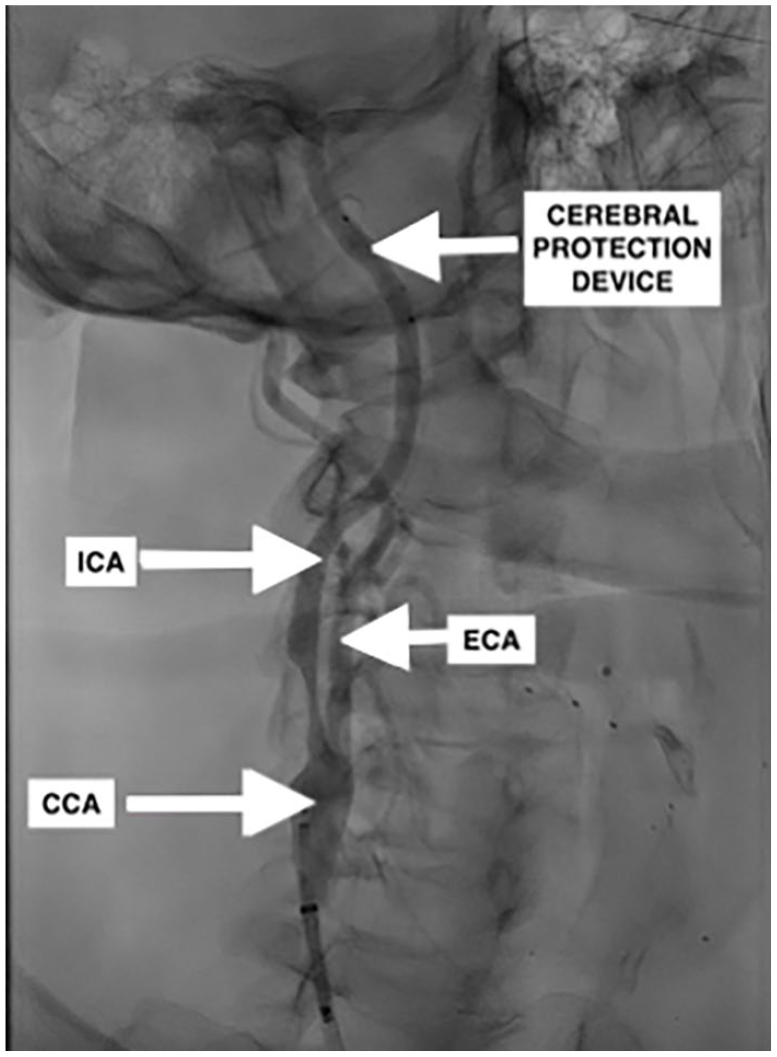
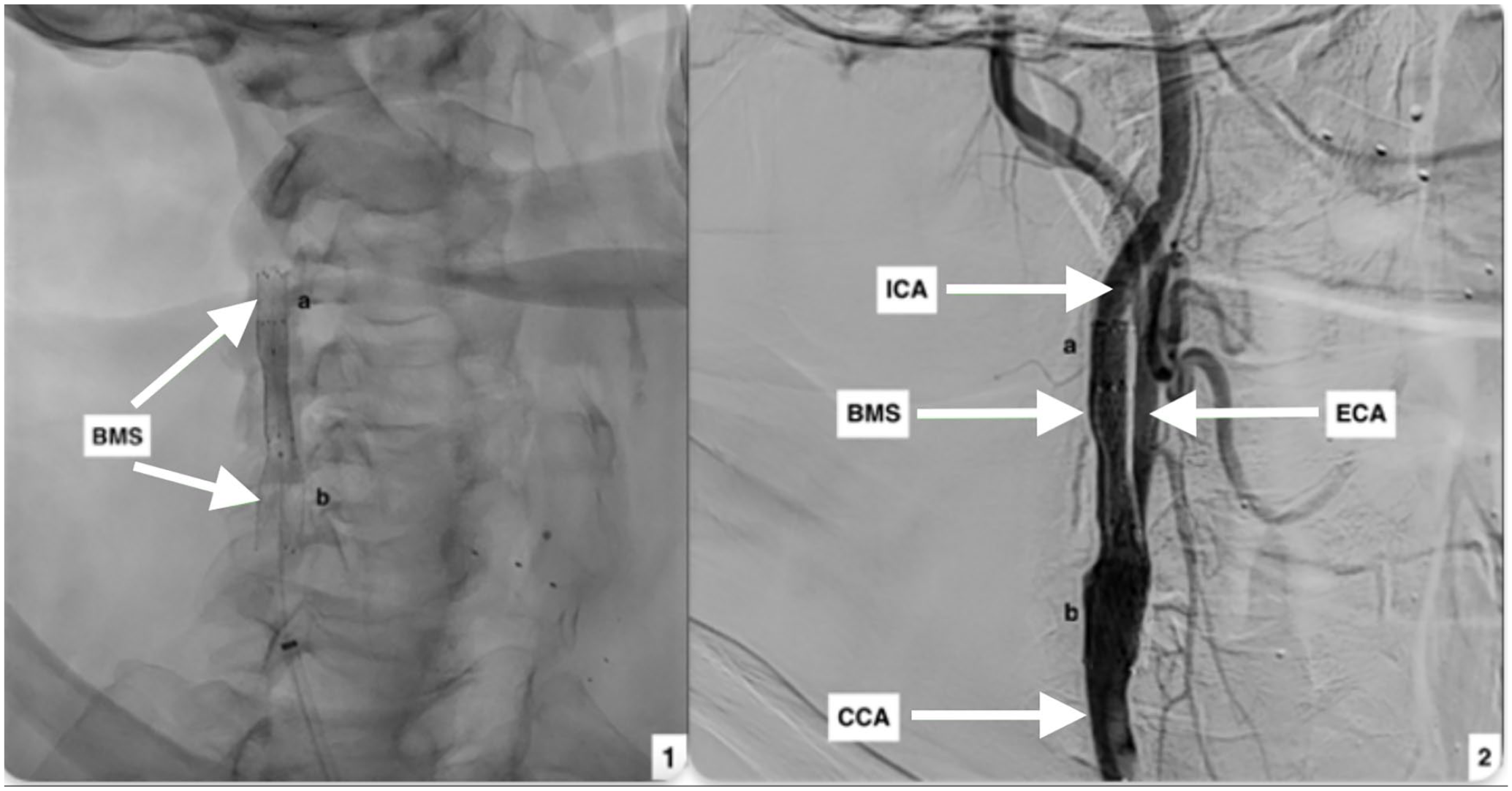
The patient underwent carotid artery stenting under local anasthesia. Stenting of the lesion was performed with the deployment of two self-expandable stents (Protégé 8/6 × 40 mm; Medtronic, Minneapolis, MN, USA) and postdilated with the use of a 5 × 20-mm balloon, under cerebral protection (5-mm SpiderFX; Medtronic), which is presented in Panel C (solid arrows indicate the bare metal stent [BMS], CCA, ICA, and ECA; ‘a’ and ‘b’ indicate the distal and proximal stent, respectively). The procedure was uneventful. Panel C also shows the completion angiography indicating unimpeded patency of the right CCA and ICA without residual stenosis. The 6-month postoperative duplex ultrasound showed good stent patency with no restenosis. The patient consented to publication of this case.
To the best of our knowledge, this particular anatomy has not been previously described. Such anatomic configuration could escape attention during evaluation of standard axial CT images, so meticulous attention is needed to identify the abnormal course of the ICA. Moreover, in the current case, the ICA was located retropharyngeally, which has been previously reported in the literature, although this was not so evident and did not cause any displacement of the tissues of the palate in our patient. 4 It has been reported that developmental anomalies can result in the presence of aberrant carotid arteries in the retropharyngeal space. 5 Such an anomaly mostly needs caution during intubation or treatment modalities via the pharynx, such as otolaryngology manipulations, whereas the abnormal course posterior to the cricothyroid cartilage should signal caution when treating the carotid artery itself.
If anatomic anomalies are not identified preoperatively, the surgeon may not be able to surgically access the lesion. Despite CEA being the first-line surgical treatment for carotid surgery, carotid artery anatomy may impose stenting as a better treatment option.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.