
Abstract

A 42-year-old woman had a rather exceptional condition, which had been manifesting since her adolescence with right hemifacial erythrosis following physical exertion, and a contralateral coldness in the hemiface, without involvement of other territories. These symptoms presented without associated pain; there was no history of erythromelalgia or other pain disorders. The erythema occurs only after physical activity, typically after a 5- to 10-minute run or brisk uphill walking. This is most likely a rare case of Harlequin syndrome, which was first reported by Lance et al., 1 and corresponds to a unilateral dysfunction of the sympathetic nervous system. She is a nonsmoker with regular physical activity and a balanced dietary intake (height: 1.65 m, weight: 60 kg, body mass index: 22.0 kg/m2). She was not on any medication or contraceptive, and did not use any other substances. The patient provided permission to share her case and photographs.
Further etiological investigations were pursued. There was no associated hyperhidrosis, Claude Bernard–Horner syndrome, abnormalities of the cranial nerves, or other abnormalities on the affected side of the face. Laboratory tests showed normal thyroid-stimulating hormone, glycemia, and cholesterol levels. The electrocardiogram was normal. Imaging with Doppler ultrasound of the supra-aortic trunks and a coronary computed tomography (CT) scan were without identifiable stenosis. Therefore, we concluded this was a case of idiopathic Harlequin syndrome. Of note, genetic mutations in SCN9A have not been studied, but mutations appear to be associated with Harlequin syndrome and paroxysmal extreme pain disorder. 2
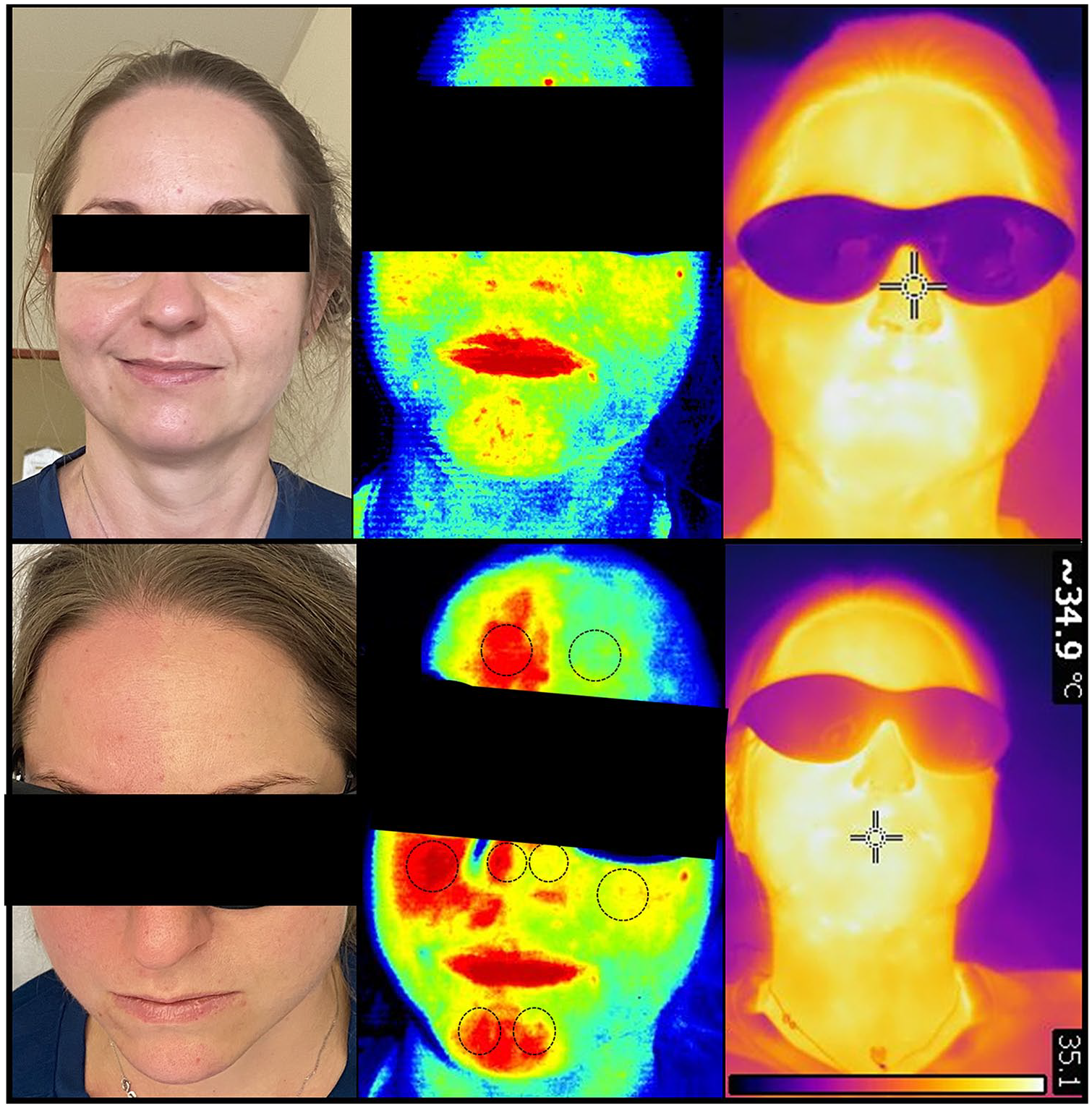
To characterize this syndrome, we carried out dynamic tests. We used laser speckle contrast imaging, which has a high spatial and temporal resolution, 3 and infrared thermography (IT), two noninvasive tools as indexes of cutaneous perfusion before and after a standard treadmill test (Panel A). Eight regions of interest were selected to analyze the vasoreactivity of the skin microcirculation (circles, Panel A). The results of the treadmill test (10% incline, 5.5 km/h speed) were normal. Facial erythema appeared after running 250 meters. We observed a visual persistence of erythema up to 45 minutes after effort, although the patient was no longer feeling any symptoms. There was spatial heterogeneity in cutaneous perfusion, measured with laser speckle contrast imaging. On the right hemiface, a maximum vasodilatation was seen 10 minutes after the end of effort (+125% on the forehead, 72% on the cheek, 62% on the nose, and 49.5% on the chin). On the left, there was no significant modification except for the chin. Variations in facial skin temperature did not significantly differ between the hemifaces.
The findings suggest a neurovascular mechanism. We recommend the laser speckle contrast imaging to assess differences in skin perfusion between hemifaces in Harlequin syndrome.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.