Abstract

Houston, Texas
September 19-22, 2024
Oral presentations
Poster No. 80
Abstract No. 1785523
Imposter syndrome: embryonic pulmonary rhabdomyosarcoma mimicking pulmonary embolism
1Vanderbilt University Medical Center
Background: A 38-year-old man with hypertension and varicose veins presented with hemoptysis and dyspnea following bilateral vein ablation.
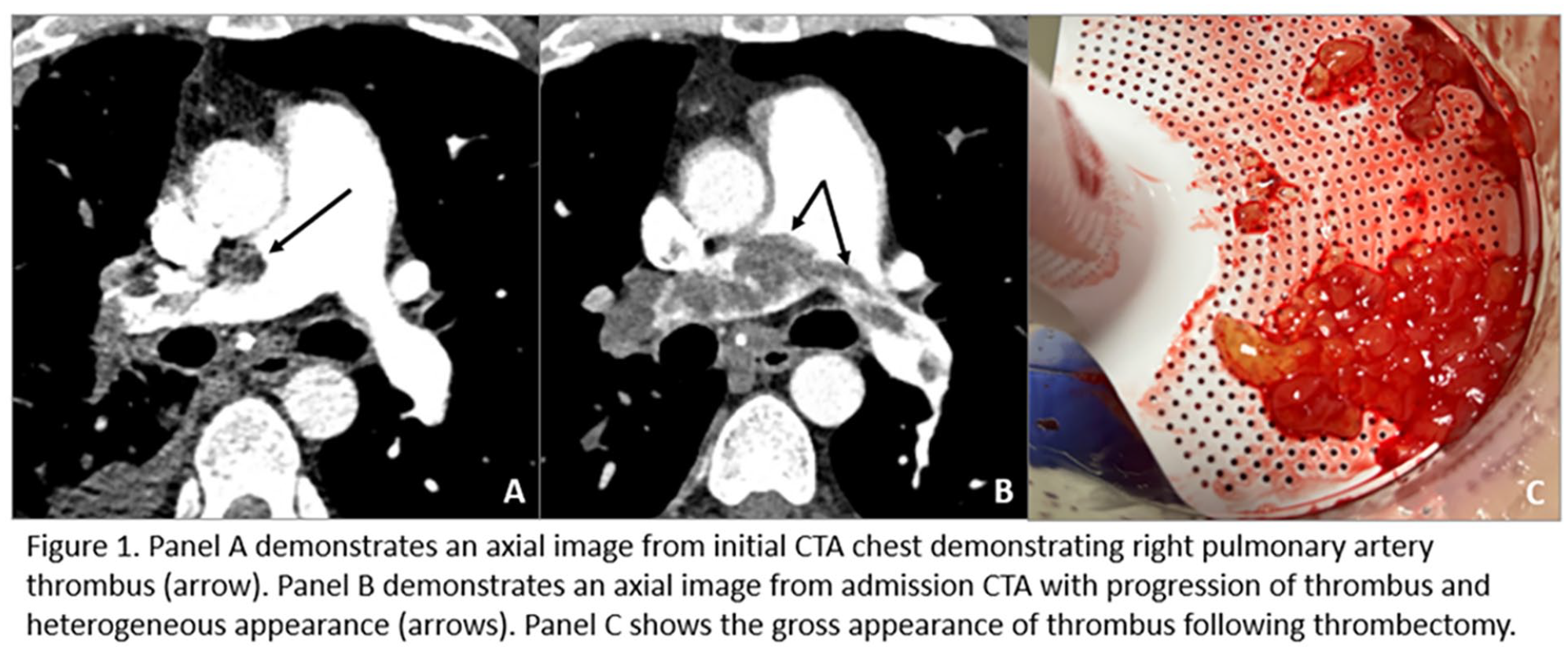
Case presentation: He was diagnosed with a pulmonary embolism (PE) and treated with apixaban. He returned one month later with pneumonia-like symptoms. Repeat CT angiography (CTA) demonstrated worsening PE burden, and he was transitioned to warfarin with an enoxaparin bridge. Hypercoagulability testing was unremarkable. Therapy was complicated by 2 weeks of subtherapeutic INR while on warfarin. Interval imaging in one month showed worsening of his PE burden, and he was transitioned to therapeutic enoxaparin alone. At follow-up, he complained of progressive dyspnea and recurrent hemoptysis. He was admitted to the hospital, and chest CTA was repeated (Figure). The heterogenous appearance of thrombus on imaging and lack of response to anticoagulation raised concern for malignancy mimicking PE. CT of the chest, abdomen, and pelvis was negative for malignancy. Testicular ultrasound showed an indeterminant lesion of the left epididymis. Transthoracic echocardiography showed right ventricular dysfunction, and V/Q scan showed minimal perfusion of the right lung and multiple perfusion defects in the left lung. He underwent aspiration thrombectomy for tissue sampling.
Conclusions: Pathology was consistent with embryonal rhabdomyosarcoma, found to be stage IV on PET/CT imaging. The primary source of the malignancy was suspected to be testicular. Systemic chemotherapy was initiated shortly after discharge.
Poster No. 81
Abstract No. 1787885
Erdheim-Chester disease presenting with aortitis
1Mayo Clinic
Background: Erdheim–Chester disease (ECD) is a rare multiorgan non-Langerhans cell histiocytosis. Diagnosis relies on radiographic findings and histopathologic features while excluding other mimics such as malignancy and autoimmune disease.
Case presentation: A 53-year-old female presented to the ED with left-sided abdominal pain. A CT scan revealed sigmoid diverticulosis and an incidental finding of a thoracic aorta aneurysm. Further evaluation with CTA showed marked wall thickening of the distal ascending aorta, arch, and descending thoracoabdominal aorta, down to the iliac arteries, as well as periaortic soft tissue thickening suggestive of aortitis (Figure 1-A). Furthermore, the patient had a history of one episode of bilateral orbital swelling about five years ago, with CT findings indicating right rectus muscle thickening which successfully treated with high-dose steroids, prompted by suspicion of IgG4 disease. However, despite the suspicion of IgG4 disease causing aortitis, treatment with glucocorticoids and rituximab yielded no improvement. With regard to normal serum IgG4 levels, this diagnosis was subsequently ruled out. Following further assessment with a PET scan, hypermetabolism was observed in the periaortic and atrial septal areas, accompanied by an enlargement of the atrial septal soft tissue mass. Suspecting a histiocytic disorder, the patient underwent a biopsy of the right atrial mass (Figure 1-B, C). After three attempts, the third biopsy revealed an atypical histiocytic infiltrate positive for CD163, cyclin D1, and Factor XIIIa, with a subset positive for OCT2. S100 was sporadically positive, while BRAF was negative. These findings led to a diagnosis of ECD involving the heart or aorta and possibly previous orbital involvement. Next-generation sequencing identified a MAP2K1 K57N mutation, prompting the initiation of cobimetinib.
Conclusions: ECD, a rare multisystem disorder, should be considered in the differential diagnosis when aortitis is present, particularly in cases demonstrating marked aortic wall thickening with periaortic soft tissue thickening on imaging.

A: Coronal CT Angiography (Mediastinal Window) showing the atrial mass. B: Fluorodeoxyglucose-PET/CT scan demonstrated hypermetabolic activity and thickening along the descending thoracic aorta (white arrow), C: PET-CT demonstrates hypermetabolism of the interatrial mass (white arrow) and metabolic activity in the aortic arch and abdominal aorta.
Poster No. 82
Abstract No. 1785471
Polycythemia vera and vibratory-induced thrombosis
1Beth Israel Deaconess Medical Center
Background: A 73-year-old male with a history of GERD presented to the emergency room with necrotic fingers on his left hand.
Case presentation: Three weeks prior, he had been working outdoors with a chainsaw when he noticed a small dark area of skin on the distal aspect of his left second digit. Over the following days, the affected area spread proximally and extended to the three adjacent fingers with surrounding erythema, pain with finger flexion, and swelling. He did not have a history of Raynaud’s, cardiac arrhythmias, or smoking. The only medication he took consistently was aspirin 325 mg to reduce the risk of colonic polyps. Initial evaluation with non-invasive arterial study demonstrated normal Doppler waveforms of the left brachial, radial, and ulnar arteries with mild abnormalities in the 2nd-5th digits on photoplethysmography. Embolic evaluation was negative. Left upper extremity angiography demonstrated normal arterial flow through the digits with an angiographic blush in distal 2nd-4th digits. Given the patent vasculature, vasodilators and surgical intervention were not indicated, and biopsy was deferred given the concern for possible poor wound healing. Serological workup was notable for an elevated hemoglobin of 17.7 g/dL, platelets of 631 K/uL, negative autoimmune markers, and normal APS labs. The elevated hematocrit was concerning for a myeloproliferative disorder; therefore, the patient underwent therapeutic phlebotomy and was started on hydroxyurea. JAK2 V617F mutation testing returned positive. Ultimately, it was believed the patient had distal thrombosis in the setting of hypercoagulability secondary to polycythemia vera with localized vibratory injury of the digital arteries from frequent recent chainsaw use. His delay in presentation and cessation of handling the power tool may have allowed for thrombus resolution by the time he underwent imaging.
Conclusions: Upon discharge, the patient was started on apixaban for anticoagulation and his necrotic lesions continued to slowly improve. After 20 months, the patient had full recovery of all fingertips and hadn’t experienced any other thrombotic issues.

Patient's fingers on presentation with associated angiogram.
Poster No. 83
Abstract No. 1795650
Approach to adverse events associated with cyanoacrylate closure
1Stanford University School of Medicine; 2Stanford Health Care
Background: Cyanoacrylate closure (CAC) is an effective option for treating saphenous vein reflux. Unlike thermal ablation, it does not require tumescent anesthesia and avoids nerve injury. However, there are adverse events (AEs), such as hypersensitivity and foreign body granuloma (FBG), specific to CAC. We present a case that highlights these AEs and their treatment options.
Case presentation: 68F with interstitial lung disease and frontal fibrosing alopecia on hydroxychloroquine had CAC of her right small saphenous vein at an outside vein clinic. Shortly after, erythema and pain developed along the treated area. This did not improve with antibiotic therapy and eventually led to skin breakdown with continued drainage and extrusion of foreign material. The lesions diminished in size with intralesional triamcinolone injection; however, nodular lesions remained palpable, and the FBG continues to be noted.
Conclusions: A foreign body reaction consisting of giant cells after CAC is a physiologic response seen in all patients who receive this treatment. Most patients have excellent results; however, there are rare cases of excessive hypersensitivity and FBG reaction that present long-term consequences. This persistent immune response can be dampened with systemic and intralesional steroids but reaction at the tissue level may continue for the duration that the material is present. When there are relapsing episodes requiring repeated courses of treatment, complete removal of the offending material can be necessary.

Hypersensitivity and FBG associated with CAC.
Poster No. 84
Abstract No. 1775684
Suspected antiphospholipid syndrome in Interleukin-7 deficiency
1National Heart, Lung, and Blood Institute; 2Hokkaido University; 3National Institute of Allergy and Infectious Diseases
Background: Antiphospholipid syndrome (APS) is an autoimmune thromboinflammatory disorder with unclear pathogenesis. Seronegative APS has been proposed in high-risk individuals with repeatedly negative antiphospholipid antibodies (aPL) and recurrent thrombosis; however, a lack of longitudinal studies and standardization tools for investigating non-criteria antibodies (e.g., anti-phosphatidylserine/prothrombin Ab) has limited incorporation into classification schemata. Interleukin-7 (IL-7) is a cytokine that regulates the development of T-, B-, and natural killer (NK) immune cell progenitors, all of which have been implicated in the pathogenesis of APS. As a result, patients with genetic loss of IL-7 develop an adult onset combined immunodeficiency. Based on IL-7 function, one could surmise correction of IL-7 deficiencies may increase production and survival of immune cells and augments monocyte activity and recruitment; however, the real impact of IL-7 repletion on pathogenic aPL production and the immune system itself remains unknown.
Case presentation: 57-year-old Japanese female with IL-7 deficiency complicated by HPV associated digital verruca vulgaris on warfarin for presumed APS considered for IL-7 repletion. APS was suspected due to multiple early term miscarriages, stroke, and single low titer (< 40 IU/mL) anticardiolipin IgG and beta-2 glycoprotein I IgG positivity. Repeat aPL panels were negative x 2. Vascular Medicine was consulted to evaluate the validity of APS diagnosis and safety of IL-7 therapy.
Conclusions: APS has not been readily reported in IL-7 deficient individuals and considered whether IL-7 deficiency capable of suppressing autoantibody production. In order to ascertain the effects of IL-7 repletion on aPLs, we planned to: 1) monitor aPL and PS/PT antibodies after initiation of IL-7 therapy with repeat testing in 12 weeks if abnormal, 2) if aPLs normal, consider seronegative APS in view of high-risk history, and 3) continue warfarin (vs DOAC). This case illustrates the unique considerations of diagnosing autoimmune disease in patients with immunodeficiency.
Poster presentations
Poster No. 85
Abstract No. 1795726
Unraveling the link: resistant hypertension amidst heavy metal toxicity
1Cleveland Clinic Abu Dhabi
Background: Identifying the etiology of hypertension is crucial. It enables targeted treatments, reduces complications, and ultimately aids in improving prognosis. However, due to the complex interplay of genetics, lifestyle, concurrent medical conditions, and environmental exposures identifying the etiology may be challenging.
Case presentation: Vascular service has been consulted for blood pressure management of a 68-year-old gentleman with medical history significant for CAD s/p PCI, on DAPT, type 2 diabetes, and ESRD on HD in setting of diabetic nephropathy. When seen, the patient was not in pain or distress. Vitals were within normal limits, except for SBP range of 160-170mmHg. Extensive investigations into secondary hypertension have been found insignificant. Patient states that his home SBP ranges between 150-160mmHg. Patient is on 4 antihypertensive medications at home, that are regularly changed due to inadequate BP control. He states that in 2019, his BP was well controlled while on one anti-hypertensive medication. On chart review, patients have been seen by neurology in 2019 for gradual memory deficits and tremors, the patient worked in ceramic and metal factory in 2019. Investigations revealed elevated lead levels. The patient has been asked to decrease exposure to industrial material, and within 6 months, and blood lead level decreased. BP improved, therefore his primary care provider discontinued 3 of his anti-hypertensive medication. Patients have been doing well, until 2021, where have presented to the ED on multiple occasions for generalized abdominal pain, nausea, and emesis. No underlying etiology was identified. Patient also states that he went back to his job at the factory in 2021.Ultimately, heavy metal testing detected high lead levels.
Conclusions: Heavy metal toxicity is often a neglected reason for hypertension, therefore it’s crucial to consider it as a potential cause of hypertension in patients with resistive hypertension, especially those with occupational exposure. In the case hereby, it has been challenging to identify lead toxicity as etiology of hypertension, however with appropriate history taking and investigations, causality has been made.
Poster No. 86
Abstract No. 1787983
Sitting on a tinderbox
1St. Luke's Medical Center-Bonifacio Global City
Background: Supra-clinoid aneurysms are intradural aneurysms that arise from the supra-clinoid segment of internal carotid artery (ICA). They may be asymptomatic or cause headaches and cranial nerve issues. Subarachnoid hemorrhage is the worst outcome. Its management is controversial due to the natural history of these vascular lesions and associated risks of their repair. Treatment options include surgical clipping and endovascular coiling, both preventing rupture.
Case presentation: We present a case of a 67-year-old female, known hypertensive, dyslipidemic, with essential thrombocythemia, who complained of occasional mild occipital headache, throbbing, with no apparent triggers. Until nine months prior to admission, she had 7/10 occipital headache with partial relief with pain reliever. Magnetic resonance imaging/angiography showed right clinoid aneurysm measuring 8.3 mm x 5.9 mm with neck of 4 mm. During the interim, no recurrence of symptoms and neurologic deficits noted. Sought consult and was advised monitoring twice a year. Repeat computed tomography angiography for monitoring showed right clinoid ICA saccular aneurysm with tip pointing inferiorly, medially, and posteriorly measuring 8.3 mm x 6.4 mm with neck of 4.6 mm; Fetal-type right posterior cerebral artery is seen. Progression of aneurysm with formation of outpouching noted, hence advised intervention. Cerebral angiogram with coiling using a microcatheter was done. Five coils were embolized into the aneurysm. Upon attempt to embolize the sixth coil, it was not going in properly hence taken out. Repeat angiogram showed >95% occlusion of the aneurysm hence no further coil was deployed. No thromboembolic complications noted.
Conclusions: In conclusion, the treatment decision depends on the aneurysm’s size, location, and neck geometry. Endovascular management has advanced significantly over the last decades and continues to evolve. Coiling is currently the most common treatment modality and are favored in older patients with poor medical condition and with aneurysm in certain location. Post-procedural surveillance is crucial for complication prevention.
Poster No. 87
Abstract No. 1787985
Internal iliac artery aneurysm presenting as urinary incontinence
1Davao Doctors Hospital
Background: Isolated internal iliac artery aneurysm (IIIAA) is a life-threatening disease and of clinical importance because of its unspecific symptoms, challenging anatomic position and high risk of rupture. Most are incidental findings using imaging modalities. There is no consensus regarding the optimal therapeutic strategy. Minimally invasive endovascular methods are considered to lessen morbidity associated with long hospitalization stay. But because of its rarity, the outcome of these endovascular approaches remained unclear.
Case presentation: A 71-year-old male came in due to urinary incontinence. His comorbidities were hypertension, coronary artery disease, paroxysmal atrial fibrillation and chronic obstructive lung disease with 45 pack-years smoking history. Due to persistent urinary incontinence, abdominal ultrasound was initially requested which revealed right external iliac pseudoaneurysm. However, abdominal CT angiogram instead confirmed a fusiform aneurysm at the right internal iliac artery measuring 11.10 cm x 8.69 cm x 9.51 cm, negative for dissection and no signs suggesting impending rupture. The urinary bladder was compressed inferiorly due to its large size and open surgery was considered for immediate decompression. Given his age and multiple comorbidities, endovascular aneurysm repair (EVAR) was the modality of choice using an Endurant II stent graft. Post-balloon documentation demonstrated a well apposed stent graft, no perforation and dissection. Final aortogram showed complete aneurysmal exclusion, optimal graft expansion and opposition.
Conclusions: We report this case for the following reasons: 1) Under recognized clinical manifestations of large IIIAA with concomitant therapeutic dilemma and 2) consider minimally invasive approach as option for high-risk patients.
Poster No. 88
Abstract No. 1787986
Saddle pulmonary embolism induced syncope
1St. Lukes Medical Center, Dr. HB Calleja Heart and Vascular Institute
Background: Despite the high incidence of pulmonary embolism its diagnosis continues to be difficult, primarily because of the various presentations of symptoms and signs with chest pain and dyspnea as its 2 most common presenting symptoms. Syncope as its initial presentation occurs in about 10% making it even more challenging and offers long list of possible etiologies.
Case presentation: This is a case of a 67-year-old female, married, hypertensive and dyslipidemic who presented with syncope and vaginal bleeding. 1 day before admission she experienced lightheadedness with subsequent loss of consciousness. Upon regaining consciousness, she noted chest heaviness associated with dyspnea. She was rushed to the emergency room and was seen GCS 15 without neurologic deficits however with blood pressure of 70/40 and tachycardia at 110. Fluid resuscitation was done with improvement of vital signs. Her ECG demonstrated sinus tachycardia, nonspecific ST-T wave changes and S1Q3T3 pattern with elevated troponin I. 2D echo showed McConnell’s sign. CTPA was then done showing saddle embolus. Venous compression revealed deep venous thrombosis. She was given 100 mg alteplase as IV infusion and was noted to have massive vaginal bleeding post-infusion. Blood transfusion of 2 units packed RBCs as well as vaginal packing was done with resolution of bleeding. She was then started with heparin drip and anticoagulation thereafter and was discharged stable.
Conclusions: Pulmonary embolism is an important differential in patients presenting with syncope, with many of these having saddle embolus. Despite our patient having massive vaginal bleeding post alteplase infusion, the benefits of giving thrombolytics and heparin outweighed its risks and were managed accordingly by the multidisciplinary team approach. Early identification is vital to avoid hemodynamic compromise and to optimize survival.

Acute saddle pulmonary emboli with extension to the bilateral lobar, segmental, and distal branches of both pulmonary arteries.
Poster No. 89
Abstract No. 1787995
Case of acute pulmonary embolism with head trauma
1St. Luke's Medical Center - Global City
Background: Pulmonary embolism (PE) in patients presenting with syncope is relatively uncommon. These subset of patients are prone to sustain injury from fall. The management of PE is largely anticoagulation and/or thrombolysis, and as the guidelines will recommend, thrombolysis is contraindicated in patients with recent head trauma.
Case presentation: A previously well 55-year-old male, with a recent short-haul flight presented in the emergency room with loss of consciousness after sudden onset difficulty of breathing. On physical examination, he was alert and coherent with a blood pressure of 120/80, heart rate 105, respiratory rate 32, afebrile and an oxygen saturation of 85% at room air. Breath sounds was clear and cardiac rhythm was regular. Laceration on the nasal bridge with epistaxis was sustained during the fall. Cranial computed tomography (CT) scan revealed comminuted fracture of the nasal bone with hematoma formation but no acute intracranial infarct or bleed. CT of pulmonary artery (CTPA) conveyed extensive filling defects in the bilateral pulmonary arteries. 2D echocardiogram showed dilated right ventricle with systolic dysfunction. He was managed as a case of pulmonary embolism, intermediate-high risk. He was started on Enoxaparin 100 mg twice daily. He then underwent catheter-directed thrombolysis with 8mg Alteplase given as bolus followed by drip at 1.5mg per hour. On the 12th hour of Alteplase drip, there was profuse epistaxis, hence drip was placed on hold and eventually discontinued. Repeat CTPA showed near complete resolution of the extensive pulmonary emboli in both pulmonary arteries. Patient was weaned off oxygen support. He was discharged stable after 8 days with apixaban 5 mg twice a day and a plan for repair of nasal bone fracture after 3 months.
Conclusions: Catheter-directed therapy (CDT) has emerged as a viable treatment option for acute sub-massive PE, supplementing existing approaches such as systemic thrombolysis or anticoagulation. CDT holds promise in providing the benefits of systemic thrombolysis while potentially reducing the risk of bleeding. Further studies are recommended to address the gap in knowledge.
Poster No. 90
Abstract No. 1787996
Successful streptokinase infusion in high-risk pulmonary embolism
1Makati Medical Center
Background: Venous Thromboembolism is a worldwide crisis. Deep vein thrombosis (DVT) and pulmonary embolism (PE) are interconnected conditions within the spectrum of venous thromboembolism (VTE). The severity of PE is influenced by several factors, including the embolus size, its location within the pulmonary arteries, and the overall cardiopulmonary health of the individual. The acute increase in pulmonary artery pressure due to the obstruction of blood flow by the embolus can lead to increased right ventricle strain which can result in severe dysfunction and can lead to potentially life-threatening complications. PE therefore poses a serious mortality threat which warrants a timely treatment course.
Case presentation: This is a case of a 40-year-old female, diabetic, obese and smoker who presented with sudden onset dyspnea, chest pain and syncope. She was eventually diagnosed and managed as a case of high-risk pulmonary embolism with documentation of central and peripheral pulmonary thromboembolism with widespread peripheral thrombus burden in both lungs on CTPA. Significant findings would include multiple emboli on both right and left main pulmonary arteries and filling defects in the left popliteal vein extending to the left external iliac vein. Patient was initially treated with Streptokinase infusion continued over 24 hours due to initial refusal for thrombectomy. Over the course of the admission, patient deteriorated with increasing oxygen requirement and inotrope support and ultimately underwent thrombectomy with catheter directed thrombolysis with Alteplase and was given Low molecular weight heparin and DOACs thereafter. Thrombectomy findings revealed no filling defects in the left pulmonary artery in contrast to CTPA findings which would support the assumption that Streptokinase reduced the thrombus burden in the said patient. Patient was eventually discharged well with a satisfactory 6-minute walk test.
Conclusions: Thrombolysis is widely accepted as the treatment of choice for acute massive life-threatening pulmonary embolism. Although newer thrombolytics such as Alteplase are more commonly used in clinical practice, Streptokinase is still a noninferior treatment regimen in the management of pulmonary embolism.
Poster No. 91
Abstract No. 1788003
Acute on top of chronic pulmonary embolism
1St. Luke's Medical Center - Global City; 2Makati Medical Center
Background: Chronic thromboembolic pulmonary hypertension (CTEPH) is the most severe long-term complication of acute pulmonary embolism (PE). Diagnosing CTEPH is difficult as algorithms for predicting or ruling it out are limited.
Case presentation: A 60-year-old male presented with a 3-month history of unilateral right leg pain and swelling associated with shortness of breath that was progressive. Baseline vital signs were stable. He had clear breath sounds and regular cardiac rhythm. Right leg was bigger than the left. Revised Geneva rule score was 10. Chest HRCT showed extensive PE with signs of acute and chronic thrombus formation (Fig 1). 2D echocardiogram showed dilated RV with adequate systolic function and moderate pulmonary hypertension. He was managed as a case of PE intermediate-low risk. The patient was given Enoxaparin 100 mg twice daily. He underwent aspiration thrombectomy with thrombolysis of right pulmonary artery, aspiration thrombectomy of right femoral vein thrombus and IVC filter placement. Prior to discharge, repeat 6-minute walk test showed improvement from Borg scale of 5 to 0. Repeat echocardiogram showed normal RV dimension with adequate systolic function and moderate pulmonary hypertension. Patient was sent home stable and advised follow up after 3 months.
Conclusions: There is subset of patients, who will present with clinical picture consistent with acute PE but with signs of CTEPH on index HRCT. These patients are in the gray zone of acute on chronic PE and management should be tailored-fit to patient’s clinical profile.
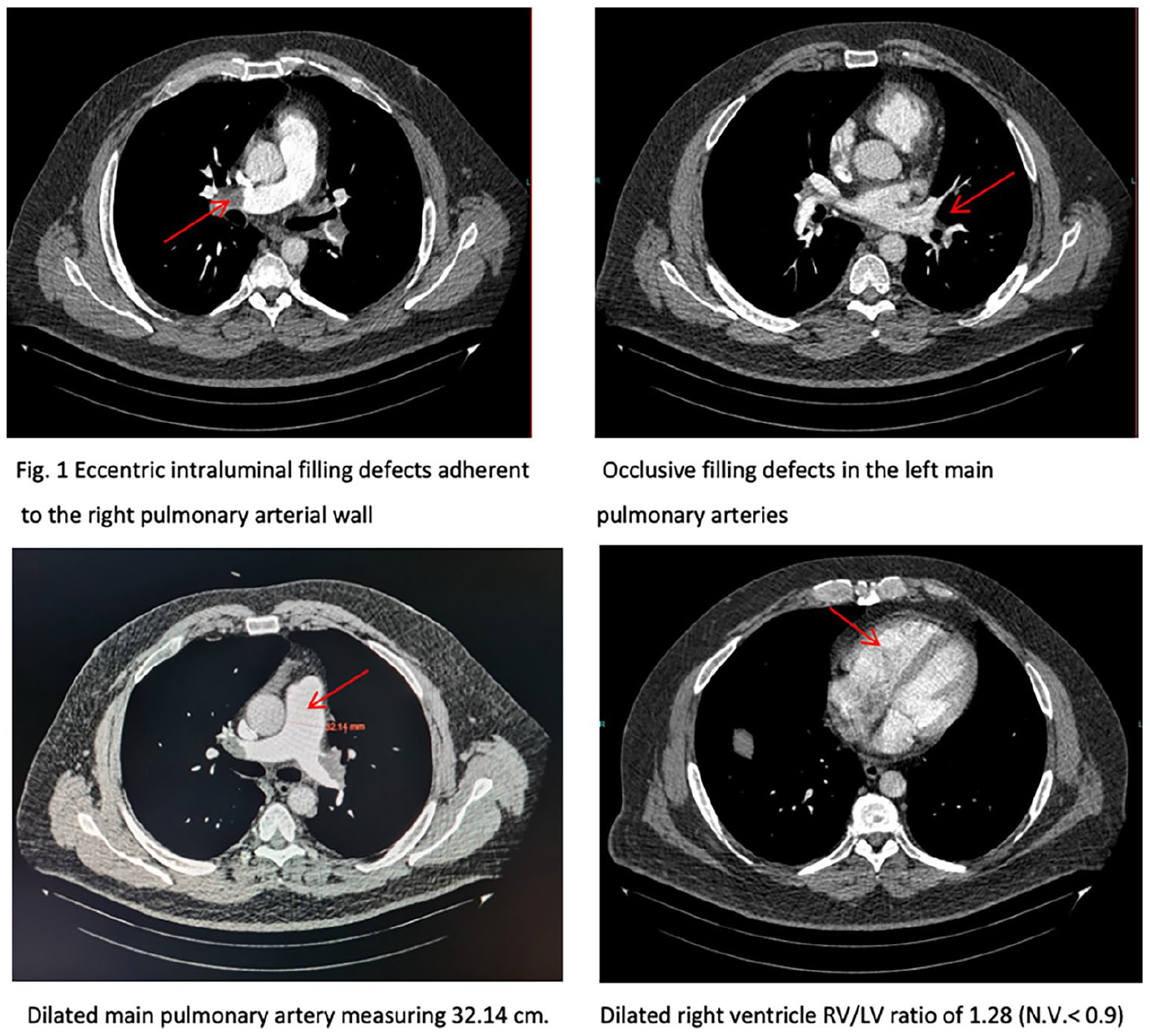
Signs of CTEPH on index high resolution computed tomography (HRCT) of a patient presenting with acute PE.
Poster No. 92
Abstract No. 1787966
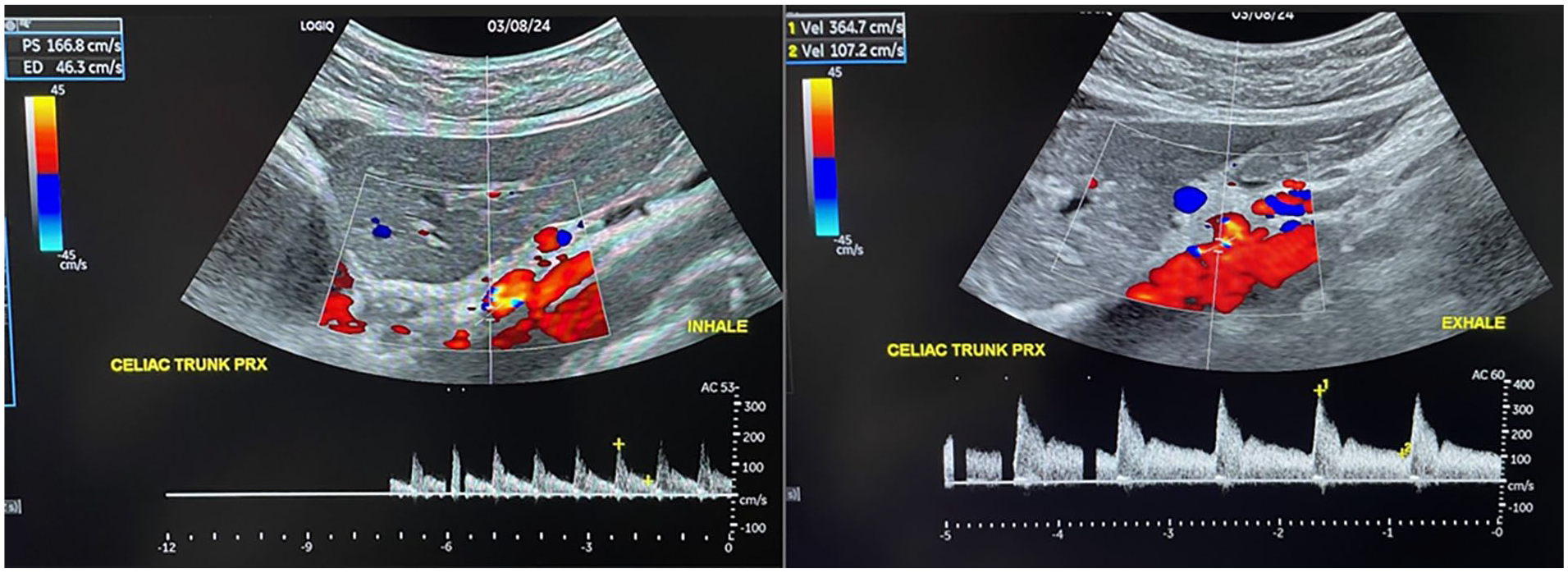
Stubborn emboli in acute mesenteric ischemia
1St. Luke's Medical Center; 2H.B. Calleja Heart & Vascular Institute, St. Luke's Medical Center
Background: Acute mesenteric ischemia has an estimated incidence of 1% in patients with acute abdomen. Regardless of etiology, it may ultimately lead to intestinal infarction. It also has a high mortality rate at 70% or more.
Case presentation: Patient is a 68-year female, hypertensive, diabetic with permanent atrial fibrillation. She is maintained on Rivaroxaban, however, was temporarily on hold due to scheduled thyroidectomy. She presented with sudden onset of persistent abdominal pain with vomiting and diarrhea. Abdominal CT scan showed pneumatosis intestinalis in the mid to distal jejunum. She became hypotensive and immediately underwent surgical abdominal exploration. There were noted necrotic segments spanning segments 60 cm from ligament of Treitz to 200 cm proximal to the ileocecal valve; eventually resected. Mesenteric angiogram showed non-opacification of the right colic and ileocecal branches of the superior mesenteric artery even after nitroglycerin injection. This was followed by 10 mg of Alteplase injection which showed prominence of the middle colic and jejunoileal arteries, however, the rest of the superior mesenteric branches were not opacified. She was immediately started on heparin drip, thereafter. Postoperatively, patient still has abdominal pain with dusky jejunostomy. CT angiogram showed no opacification of the right colic and ileocecal branches of the superior mesenteric artery. On repeat laparotomy, remaining necrotic segments were resected. Embolectomy was done and was able to extract 3.5 cm of thrombus. Noted brisk backflow from affected artery. Post-operative repeat CT angiogram showed opacification of the previously attenuated segment of the SMA and distal right colic branches. On subsequent hospital days, meticulous postoperative care, infection treatment and nutrition support were provided. Subsequently, she was discharged stable.
Conclusions: Diagnosis of acute mesenteric ischemia can be difficult due to non-specific nature of its symptoms, which contribute to high mortality rate. If not treated promptly, the condition progresses rapidly. By maintaining a high index of suspicion for this condition, early diagnosis and treatment with multidisciplinary approach can help to improve survival.
Poster No. 93
Abstract No. 1787972
Insidous threat: a case of mycotic aortic aneurysm
1St. Luke's Medical Center-Bonifacio Global City
Background: Mycotic aortic aneurysms, rare but serious infections of vessel walls, necessitate timely diagnosis and treatment to avert catastrophic outcomes. Tuberculous aneurysms, though infrequent, pose a life-threatening risk of rupture, often presenting as pseudoaneurysms. Treatment focuses on preventing rupture and eradicating the tuberculous infection. Surgical intervention carries a heightened risk of postoperative complications, increasing mortality rates. Recently, emerging endovascular interventions have shown improved outcomes for aortic aneurysms.
Case presentation: A 65-year-old male, a smoker with hypertension and prediabetes, was admitted due to recurrent fever, chills, cough, weakness, and weight loss. Hypotension was noted in the ER, leading to a diagnosis of sepsis secondary to pneumonia, with consideration of pulmonary tuberculosis. Antibacterial and antimycobacterial medications were initiated. During treatment, jaundice developed, and a CT scan revealed incidental finding of fusiform dilatation of infrarenal abdominal aorta (4.2 cm) with thick circumferential thrombus around the lumen and focal active extravasation of contrast into the thrombosed portion of aneurysm near the level of faintly visualized inferior mesenteric artery. Advised surgical versus endovascular treatment. A 4-phased dynamic liver scan identified penetrating atherosclerotic ulcers along the infrarenal abdominal aorta up to the inferior mesenteric artery. Endovascular repair utilized aorto-uni-iliac stent graft as aortic bifurcation size was not suitable for bifurcated graft with vascular plug occlusion of the left common iliac artery followed by femorofemoral bypass. Final imaging confirmed a well-expanded, well-opposed graft with no dissection, fracture, or perforation, fully excluding the abdominal aortic aneurysm and ensuring a patent internal iliac artery on the left.
Conclusions: In conclusion, early recognition and prompt intervention, whether surgical or endovascular, coupled with anti-TB medication, are crucial in preventing the fatal outcomes associated with tuberculous mycotic aneurysms.
Poster No. 94
Abstract No. 1788022
Arteriovenous graft pseudoaneurysm in a kidney transplant candidate
1St Luke's Medical City, Bonifacio Global Cityy
Background: Pseudoaneurysm of grafts is a complication that occurs in 2 to 10% of patients undergoing hemodialysis. The goal of treatment is to maintain patency and prevent thrombosis. In a patient for kidney transplant, a working access is crucial prior to operation. Any complication that needs intervention that can cause transfusion-requiring blood loss can be detrimental to a transplant candidate.
Case presentation: A 52-year-old male with diabetic kidney disease on dialysis presented with left upper arm swelling of 2 weeks. The patient is a candidate for kidney transplant. Duplex scan of showed left brachio-axillary graft pseudoaneurysm measuring 4.28 cm x 5.53 cm with a neck diameter of 0.305 cm that is connected to the inflow segment of the graft with thrombus formation. Intervention to remove the pseudoaneurysm with minimal blood loss was planned. The goal is to minimize blood transfusion that can potentially initiate immune response against renal allograft. Coil embolization of the graft was done followed by evacuation of hematoma and removal of pseudoaneurysm capsule. A temporary dialysis access was inserted. The patient will undergo planned kidney transplantation.
Conclusions: Pseudoaneurysms of vascular accesses should be suspected when dialysis patients present with swelling of their limb. Vascular imaging is crucial for timely management. A team approach in managing pseudoaneurysm in transplant candidates is needed to find the best strategy which will decrease risk of inducing immune responses that can cause allograft rejection.
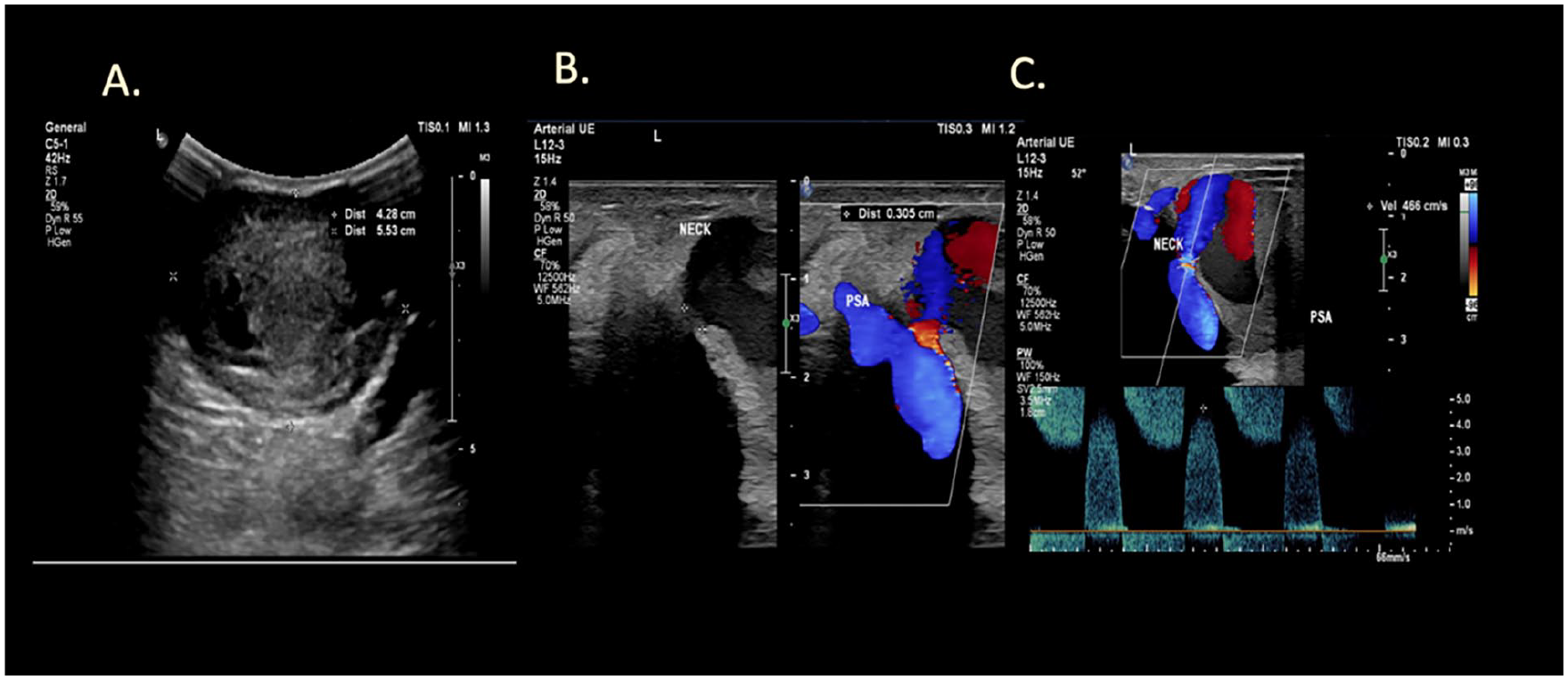
Duplex ultrasound of pseudoaneurysm.
Poster No. 95
Abstract No. 1788106
An adventure into aortitis
1Dartmouth-Hitchcock
Background: Aortitis can occur with large vessel vasculitides or infections. Incidence of giant cell arteritis (GCA) is estimated to be around 19 /100,000 individuals a year over the age of 50. GCA can present with headache, visual changes, and polymyalgia rheumatica. Aortitis screening is crucial in GCA due to the risk of dissection and rupture. Prompt multimodal imaging is crucial for diagnosis and treatment.
Case presentation: An 82-year-old woman with history of ascending aortic aneurysm (4.5 cm), coronary artery disease, diabetes, and hypertension presented with chest pain. She was normotensive with heart rate in the 70s. EKG showed non-specific ST changes. Computed tomography (CTA) showed severe mid-ascending aortic aneurysm of 7.7 cm in diameter without dissection (Fig 1). An emergent echocardiogram showed dilated left ventricle, left ventricular ejection fraction of 65%, aortic root dilated to 5.1 cm, ascending aorta of 7 cm, and severe central aortic insufficiency (Fig 2). Coronary angiography showed multivessel disease. She subsequently underwent successful coronary artery bypass grafting, aortic valve replacement, and tube graft. Aortic tissue pathology (Fig 3) showed medial necrosis with giant cells, confirming GCA, and patient was treated with prednisone.
Conclusions: This case demonstrates guidance of multimodal imaging and angiography to diagnose GCA with isolated aortitis and massive ascending aneurysm. Subsequent surgery and rheumatology multidisciplinary involvement finalized the treatment plan.
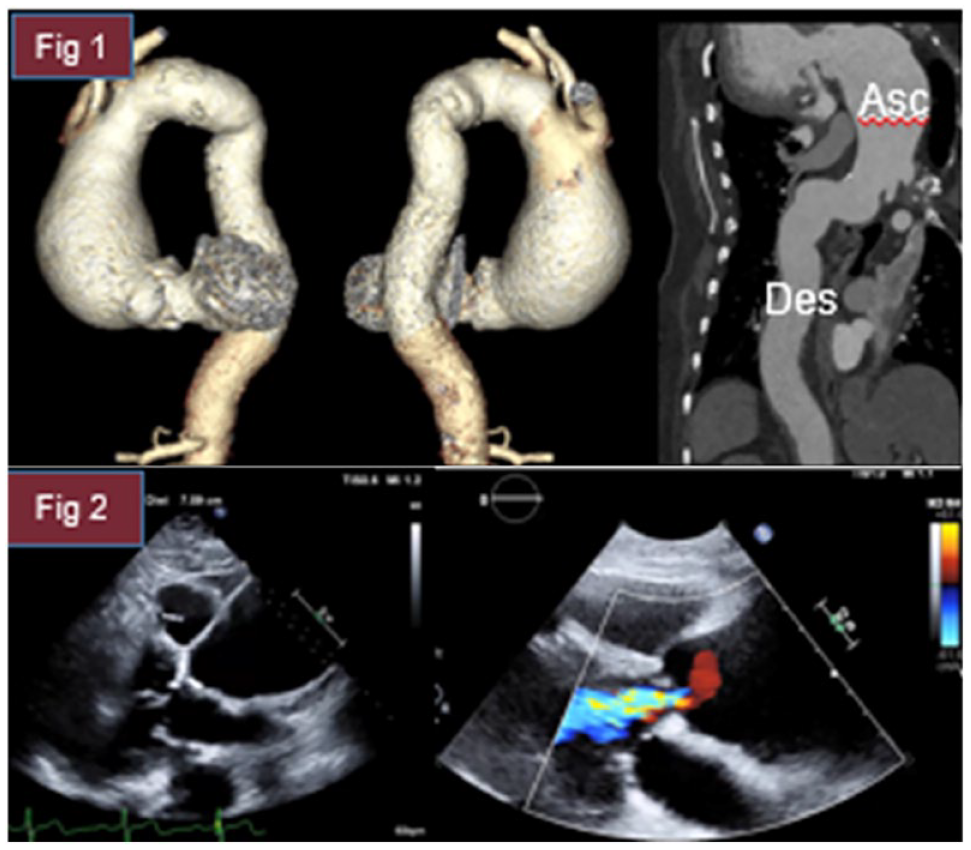
1: CTA chest with contrast showing 3D reconstruction of the thoracic aortia in LAD 90, RAD 115 views, and curvilinear reformation of thoracic aorta. 2: Echocardiogram in parasternal long view showing dilated left ventricle, dilated aortic root, and ascending aorta, severe aortic regurgitation.
Poster No. 96
Abstract No. 1788252
Leg variant angina? A case of vasospastic claudication
1Cleveland Clinic
Background: Spontaneous vasospastic limb ischemia is an uncommon entity. Increased awareness of the condition is crucial in preventing complications and avoiding unnecessary interventions.
Case presentation: A 44-year-old woman with Raynaud’s phenomenon, coronary arterial vasospastic disease status post balloon angioplasty of the 1st diagonal branch, carotid arterial disease status post left internal carotid endarterectomy, seronegative rheumatoid arthritis, and former tobacco use presented with three years of progressive lower extremity claudication. She denied the use of illicit drugs. Physical exam showed dusky digits and decreased femoral, popliteal, and pedal pulses. Ankle brachial index with exercise was significantly reduced. Computed tomography angiography demonstrated no significant atherosclerosis. Autoimmune/inflammatory work up was unremarkable. Magnetic resonance angiography excluded popliteal artery entrapment, iliac endofibrosis, and cystic adventitial disease. Peripheral angiography revealed severe vasospasm of the peroneal trunk that responded to nitroglycerin infusion. Her home tadalafil was up-titrated and prazosin was initiated with improved symptoms during hospitalization.
Conclusions: While rare, arterial vasospastic disease should remain on the differential for claudication. Diagnosis relies on exclusion of underlying conditions and demonstration of vasospasm on angiography. Pharmacologic vasodilation is the mainstay of treatment.
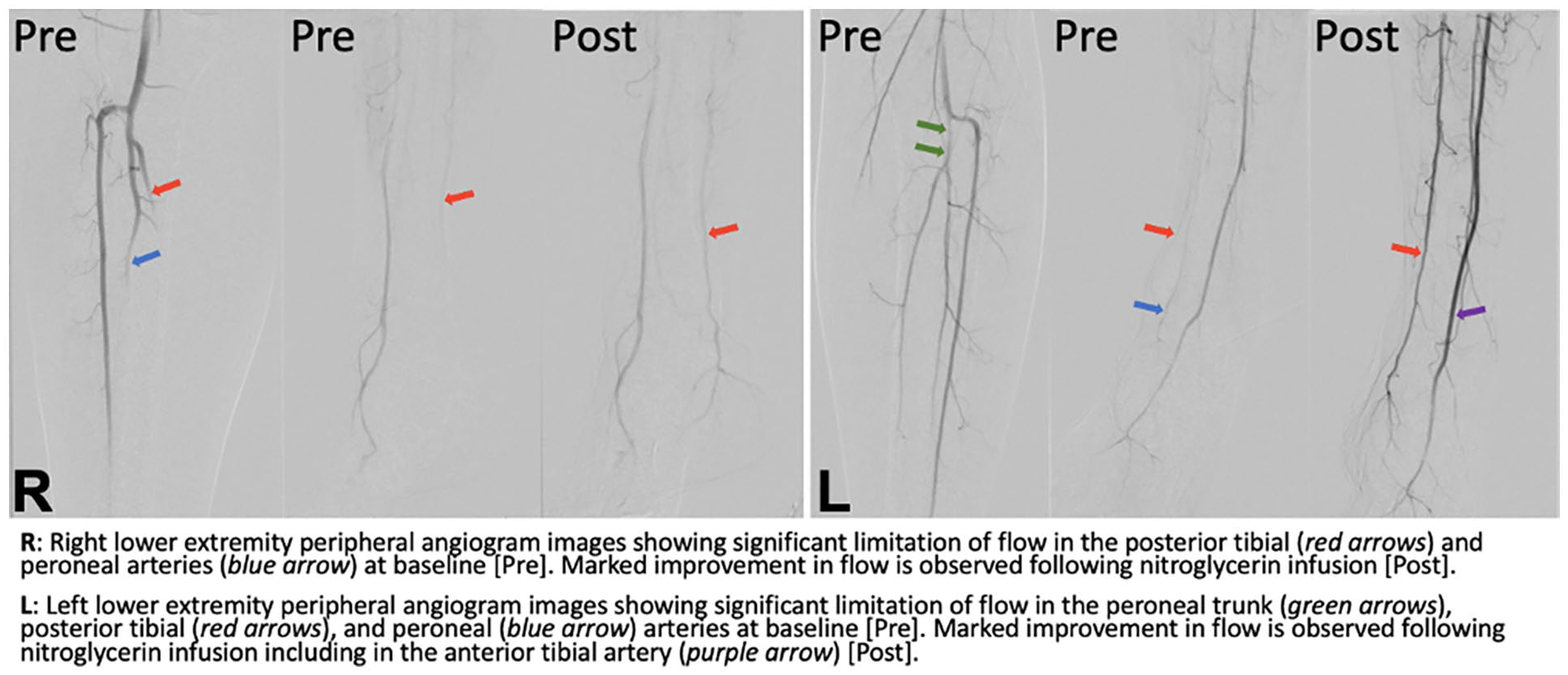
Peripheral angiogram images showing baseline vasospasm that improved with nitroglycerin infusion.
Poster No. 97
Abstract No. 1788278
Pudendal angioplasty optimizes perfusion in penile glans ischemia
1Cleveland Clinic; 2Cleveland Clinic Fairview Hospital; 3Cleveland Clinic Akron General; 4University of Rome Tor Vergata
Background: Internal Pudendal Artery (IPA) Percutaneous Transluminal Angioplasty (PTA) is a promising intervention for erectile dysfunction. Its utilization for wound healing after penectomy has been sparsely reported.
Case presentation: A 55-year-old man with type II diabetes mellitus, congestive heart failure, hypertension, hyperlipidemia, peripheral arterial disease, tobacco abuse, and refractory erectile dysfunction due to severe Peyronie's disease, underwent inflatable penile prosthesis implantation with complex penile reconstruction complicated by distal penile ischemia and dry gangrene, leading to device explantation and partial glansectomy. His ischemia progressed despite sildenafil with eventual surgical site infection. Intravenous antibiotics were initiated. Aortic and selective internal iliac angiography revealed subtotal occlusion of the IPAs. PTA was performed resulting in a significant reduction of stenosis in both vessels (< 30%). He received a loading dose of ticagrelor with a transition to clopidogrel and long-term aspirin. He underwent incision and drainage of an intracavernosal abscess, debridement of subcutaneous tissues, partial penectomy, and penoscrotal urethrostomy. Remaining tissue appeared well perfused, and the penile stump showed good healing.
Conclusions: Pre-operative assessment of IPA flow is of paramount importance in preventing devastating ischemic outcomes following penile surgeries. IPA PTA could be a useful therapeutic modality for improved wound healing after penectomy.
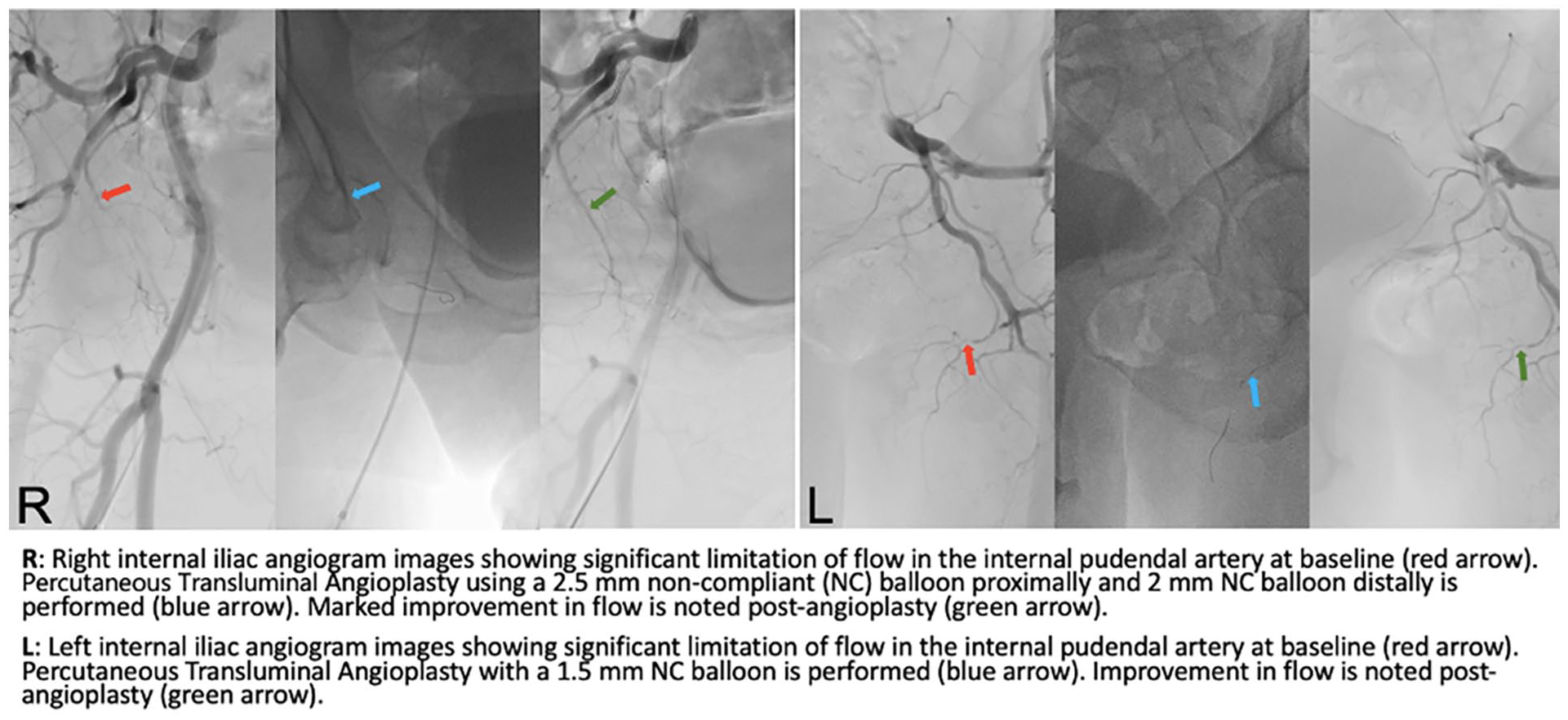
Angiogram images showing improved flow through bilateral internal pudendal arteries following percutaneous transluminal angioplasty.
Poster No. 98
Abstract No. 1788282
Anticoagulation failure and invasive management of recurrent strokes
1Mayo Clinic
Background: A 59-year-old male with metastatic pancreatic cancer was treated with FOLFIRINOX in July 2023. In August, he was found to have bilateral pulmonary emboli (PE) and was treated with apixaban. In September, he suffered a stroke and anticoagulation was switched to enoxaparin twice daily. Cancer progression with new SMV tumor encasement and occlusion prompted treatment with Gemcitabine and nab-Paclitaxel.
Case presentation: In January 2024, he suffered an acute left M2 stroke, new PE (Image 1A), and new mitral valve mass (Image 1B). This occurred despite weight-based enoxaparin (80 mg twice daily; weight 63.9kg) with therapeutic levels (anti-Xa trough 0.32 IU/mL and peak 0.65 IU/mL). Transesophageal echocardiography (TEE) revealed a thickened mitral valve with a large (Image 1C; 12 x 5.5 mm) echogenic mass with tiny mobile components attached to the A2 scallop of the anterior leaflet. The patient was managed successfully with AngioVac thrombectomy under TEE guidance. Pathology revealed bland fibrin thrombus without inflammation or microorganisms, consistent with non-bacterial thrombotic endocarditis (NBTE). Enoxaparin dosing was increased to 100 mg twice daily. Despite remaining asymptomatic following the procedure, he was discharged to hospice.
Conclusions: Anticoagulation failure is 2-3 times higher among cancer patients with NBTE compared to cancer associated venous thromboembolism. Options to lower the risk of recurrent embolism, particularly stroke, would be clinically useful irrespective of palliative care.
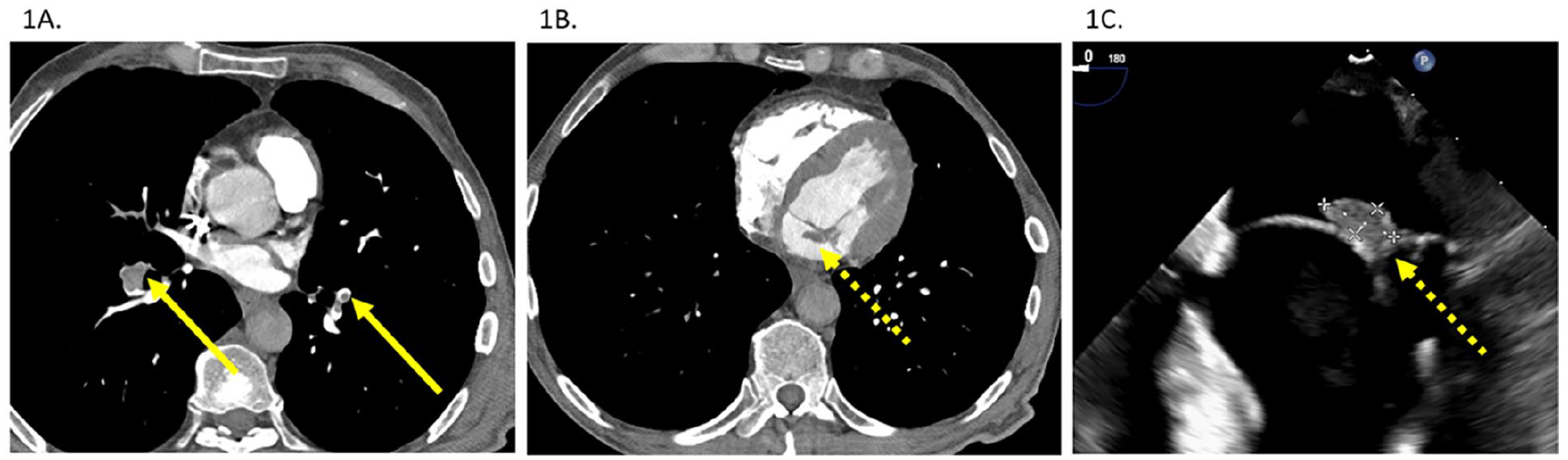
CT angiogram of chest and pulmonary arteries, showing bilateral pulmonary embolism progression (1A), mitral valve mass on said CT angiogram (1B), and transesophageal echocardiogram showing a 12.3 x 5.5-millimeter echogenic mass with tiny mobile components fixed to the A2 scallop of the anterior leaflet (1C).
Poster No. 99
Abstract No. 1788171
Pneumococcal bacteremia leading to Austrian syndrome, mycotic aneurysms
1OhioHealth Doctor's Hospital
Background: Austrian syndrome is a rare clinical triad of disseminated Streptococcal infection characterized by pneumonia, meningitis, and endocarditis, and is associated with a mortality rate up to 32%. Endocarditis caused by Streptococcal infection accounts for less than 3% of all cases, and fewer still, less than 1% of these cases will present with Austrian Syndrome. Additionally, mycotic aneurysms are also rare, making up only 1-2.6% of all aortic aneurysms. They have a high risk for expansion and death, requiring aggressive management.
Case presentation: Here is a case of Streptococcal bacteremia with mycotic aneurysm and endocarditis, progressing to bilateral embolic strokes and associated CNS infection. A 55-year-old male presented with 2 weeks of worsening body aches, fever, and cough. Initial workup revealed a S. pneumoniae bacteremia with imaging and tagged WBC scan consistent with pneumonia and mycotic aneurysm formation of the aortic arch. Although stable on admission, he acutely worsened on day 7 while awaiting transfer to tertiary care center. Repeat imaging revealed enlargement of existing aneurysm, new formation of a second aneurysm in the distal thoracic aorta, as well as new aortic valve vegetation. Brain imaging revealed diffuse bilateral embolic frontal lobe infarcts, with associated abscess conversion, as well as cerebritis and ventriculitis. Patient ultimately underwent aortic valve replacement, tricuspid valve repair, as well as closure of PFO and VSD seen in perioperative echocardiogram. Days later, open repair of the thoracic aorta with graft reconstruction was performed. Hospital course showed marked clinical improvement.
Conclusions: Although S. pneumoniae endocarditis rates have fallen, mortality rates remain high; up to 60% without early surgical intervention. Similarly, even with surgical intervention, mortality rates for mycotic aneurysms have been reported as high as 43%. In this case we highlight two rare and potentially fatal processes occurring simultaneously as a result of disseminated Streptococcal infection, progressing to the equally deadly triad known as Austrian Syndrome. Appropriate diagnosis requires high clinical acuity, coupled with swift intervention to prevent patient mortality.
Poster No. 100
Abstract No. 1788349
Refractory shock in PE requiring VA-ECMO despite thrombectomy
1University of Connecticut
Background: Pulmonary embolism (PE) is the third leading cause of death in the US after MI and stroke. High-risk PE has many treatment strategies including systemic or catheter thrombolysis, and surgical or catheter thrombectomy. The role of VA-ECMO in high-risk PE is increasingly recognized.
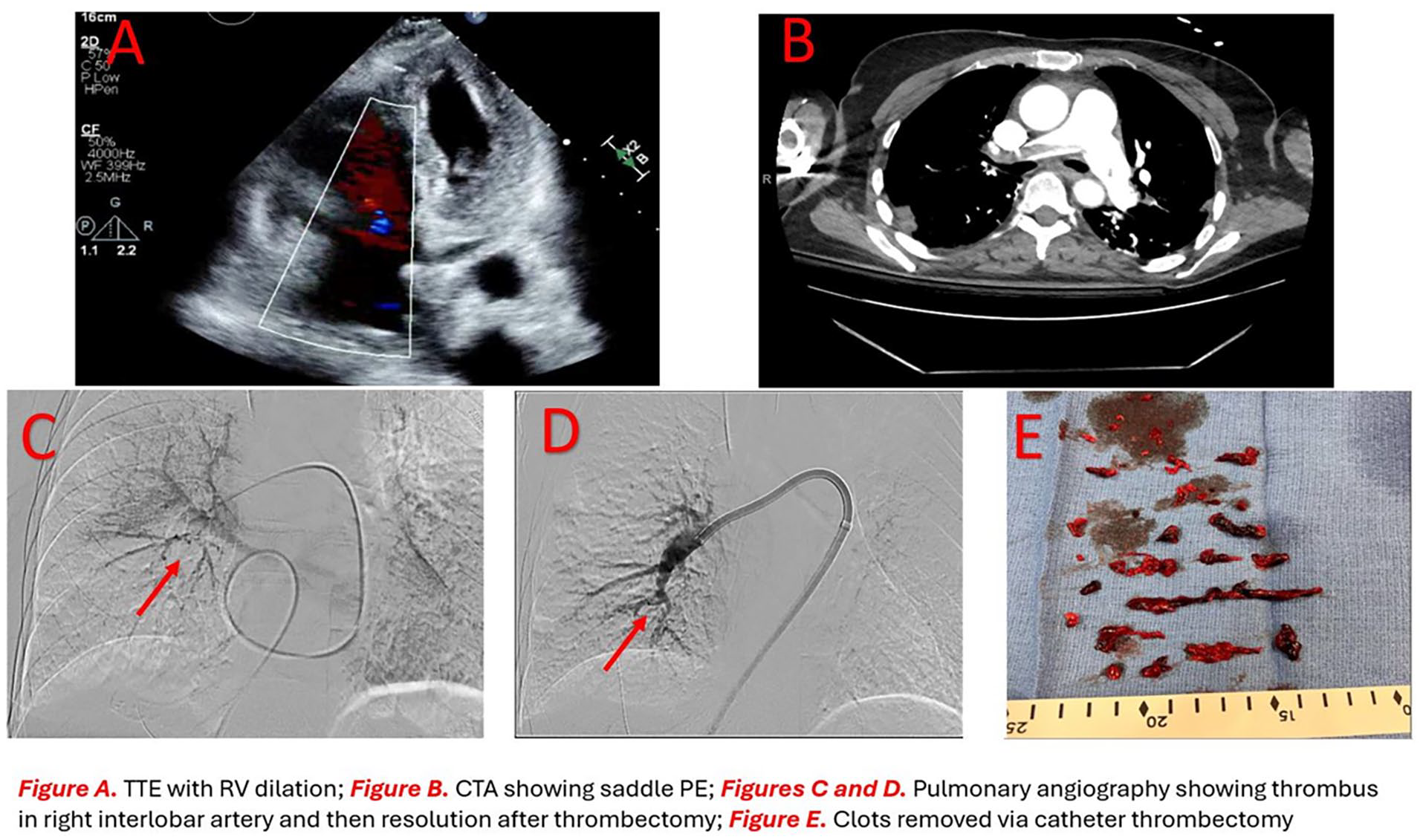
Case presentation: A 65-year-old female presented with PEA arrest. CPR was performed and ROSC was achieved in 5 minutes. EKG had an S1Q3T3 pattern. Laboratory results revealed creatinine 1.6 (baseline 0.8), troponin 1400 (normal < 30), and lactate 4 mmol/L. An echocardiogram showed a dilated right ventricle (RV) (Figure A). CT angiogram showed saddle PE (Figure B). A full dose of tPA was administered. Due to increasing pressor requirements thrombectomy was pursued. Pulmonary angiography was done before and after (Figures C and D). A large clot burden was aspirated (Figure E). The patient's lactic acidosis persisted, necessitating transfer to another hospital for VA-ECMO. She was decannulated in 48 hours. She has continued to do well in follow-up.
Conclusions: Acute RV failure plays an essential role in obstructive shock. An acute increase in RV afterload causes RV dilation. This reduces RV contractility and decreases RV coronary perfusion causing ischemia. This results in an "RV death spiral", which is not reversible with thrombus resolution. Most expert consensuses recommend early initiation of MCS in patients with high-risk PE. Not all centers have MCS capability. We describe a patient with persistent shock after thrombectomy needing VA-ECMO to allow RV recovery.
Poster No. 101
Abstract No. 1788359
Pelvic mass unmasking a functional adrenal adenoma
1Beth Israel Deaconess Medical Center
Background: Primary aldosteronism is an important cause of secondary hypertension but is underdiagnosed.
Case presentation: We report the case of a 35-year-old woman with hypertension diagnosed at age 27 who originally presented to acute care for evaluation of inability to urinate and was found to have profound electrolyte derangements including a potassium of 2.0, sodium of 121 and creatinine of 10. A computed tomographic (CT) abdomen/pelvis showed a 10.0 x 9.6 x 9.0 cm necrotic mass arising from the posterior cervix, extending into the vaginal canal and causing mass effect on the urinary bladder. A 3.0 x 2.6cm left adrenal mass was also present which was initially concerning for metastatic disease. During her index hospitalization, she was noted to have severe systemic hypertension with blood pressures ranging 150/100-170/110 mmHg. She started lisinopril and nifedipine but had persistent hypertension and hypokalemia requiring 80 mEq of potassium supplementation daily. As part of a pre-operative evaluation, a renin/aldosterone ratio was obtained which showed an aldosterone level of 39 ng/dL, renin of 0.10 ng/mL/h for an aldosterone/renin ratio of 390. Catecholamine screening for pheochromocytoma was unremarkable as was cortisol testing for Cushing syndrome. A repeat adrenal protocol CT abdomen/pelvis showed a 56% washout of contrast and thus was indeterminate. She started spironolactone with considerable improvement in her blood pressure to 130/90mmHg. As surgical intervention for her the gynecologic mass was already planned, adrenal vein sampling was not pursued, and she underwent a combined laparoscopic total hysterectomy and left adrenalectomy. Subsequent pathology showed that the uterine mass was a uterine fibroid and that the adrenal gland mass was well-circumscribed without evidence of malignancy. After adrenal adenoma resection, her aldosterone/renin ratio and hypokalemia normalized and her hypertension improved markedly.
Conclusions: We encourage clinicians to have a low threshold to test for hyperaldosterone states, particularly in young patients with severe hypertension or evidence of hypokalemia.
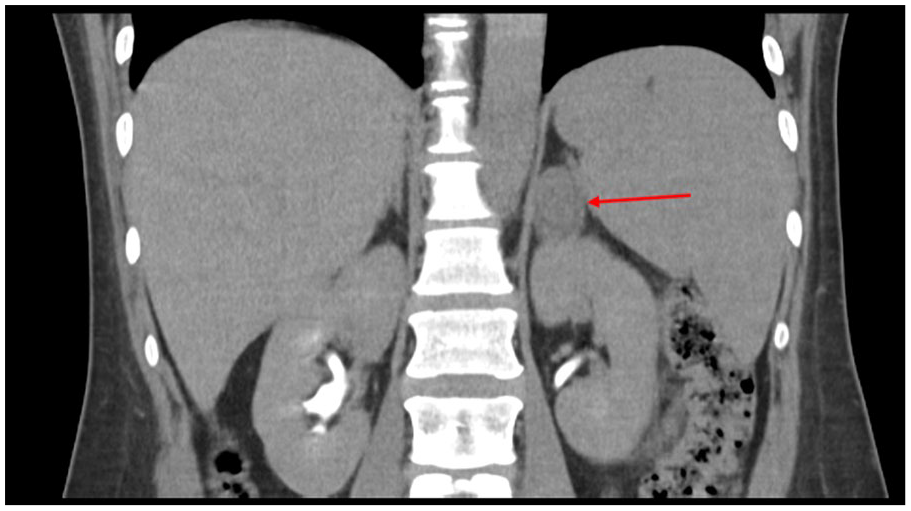
Left adrenal mass.
Poster No. 102
Abstract No. 1788409
Fat embolism: prolonging life with extracorporeal membrane oxygenation
1Makati Medical Center
Background: Fat embolism syndrome (FES) causes a systemic inflammatory cascade affecting multiple organ systems and is due to the presence of fat globules in the bloodstream following a long bone fracture caused by trauma. It has a reported mortality of 5-20% hence timely management of FES is imperative and ultimately life-saving.
Case presentation: We present a case of a 47 year-old man, otherwise healthy individual who came in at the ED after suffering multiple injuries following a cycling accident. His right tibia, fibula, and femur had comminuted fractures, necessitating external fixator application and stat wound debridement investigation. 12 hours post-surgery, he went into ventricular fibrillation and eventually arrested with a total downtime of 15 minutes before return of spontaneous circulation was achieved. Unfortunately, due to persistent hemodynamic instability necessitating use of multiple vasopressors and intractable acidosis, patient eventually underwent venous-arterial extracorporeal membrane oxygenation (ECMO) cannulation. 2d echocardiogram showed dilated right ventricle and mild pulmonary hypertension and a consideration of fat embolism was made. On the 2nd hospital day, there was gradual improvement in hemodynamics hence vasopressors were slowly tapered down. CT Pulmonary angiography was done revealing that pulmonary arteries are well opacified with no evidence of filling defects. Patient eventually weaned off of ECMO and decannulated on the 5th hospital day and was fortunately discharged well after undergoing multiple debridement.
Conclusions: Fat embolism syndrome is a potentially fatal condition from acute right ventricular failure and hypoxia. The backbone of the management of FES is supportive care and early fixation. VV-ECMO is more commonly utilized than VA-ECMO as respiratory support in FES. In this report, VA-ECMO was used to as a bridge to recovery from cardiogenic shock. After 5 days on ECMO, inotropes were eventually discontinued due to improving vital signs and patient had successful ECMO decannulation.
Poster No. 103
Abstract No. 1788420
Acute limb ischemia in a 41-year-old female
1Mayo Clinic
Background: Exogenous hormone therapy is a described risk factor for the development of thrombosis, though the causative mechanism is incompletely understood. Estrogen therapy is associated with higher risk of both arterial and venous thrombosis. However, an association between testosterone therapy and arterial thrombosis is less described. Here, we present a unique case of acute limb-threatening ischemia (ALI) requiring urgent revascularization related to exogenous hormone therapy.
Case presentation: A 41-year-old female, former smoker, on combined oral contraception, presented with severe pain and loss of sensation in the right foot, compatible with ALI. Cross-sectional imaging demonstrated occlusion of the anterior tibial, peroneal artery, and posterior tibial arteries requiring lytic therapy followed by aspiration thrombectomy; significant amount of thrombus was aspirated. There was no evidence of atherosclerosis. Despite therapeutic levels of intravenous heparin, she developed recurrent thromboses in the subsequent 48 hours, requiring additional surgical interventions with arteriotomy and thromboembolectomy. Each time, a significant amount of thrombus was removed. She was eventually discharged on aspirin and warfarin. Extensive work-up was pursued to evaluate for causes of arterial thrombosis including antiphospholipid antibodies, myeloproliferative neoplasm, heparin-induced thrombocytopenia, etc. along with imaging to exclude intracardiac or other proximal source of embolism. This work-up was unremarkable. In further discussion, the patient revealed she underwent an injection of testosterone and estrogen ‘pellets’ for “hormone balance” six weeks before presentation. Testosterone levels drawn approximately 8 weeks after thrombosis were markedly elevated with total testosterone of 89 ng/dL (upper limit of normal 55 ng/dL). Recheck of testosterone levels 4 months later were normal.
Conclusions: ALI is a rare consequence of exogenous hormone use. While the mechanism of thrombogenesis from hormone therapy is incompletely understood, our case highlights the critical importance of obtaining a thorough clinical history when evaluating for atypical causes of arterial thrombosis.
Poster No. 104
Abstract No. 1794450
Lipus for no-option CLTI patient with Buerger disease
1Hiroshima University
Background: Thromboangiitis obliterans (TAO), or Buerger disease, is a non-specific inflammation of small and medium-sized arteries with thrombus obliteration and without atherosclerotic changes. Despite conservative treatment methods, patients with TAO can develop chronic limb-threatening ischemia (CLTI) and are at risk of limb amputation.
Case presentation: A 72-year-old man presented with rest pain, discolored toes, and renal impairment. He was a chronic recurrent smoker and was previously diagnosed with Buerger disease and presented with recurrent ulcers since 2011. Despite the conventional therapy measures of standard wound dressings, stopped smoking and was prescribed with medications of sarpogrelate hydrochloride and clopidogrel tablets, there was worsening of the limbs condition. He was later diagnosed with Rutherford classification stage 6 CLTI (Figure A) with IgA nephropathy. He refused limb amputation. The noninvasive treatment option of low-intensity pulsed ultrasound (LIPUS) was initiated and the patient’s symptoms in the bilateral lower limbs, ulcers and the blue-colored toes gradually recovered (Figure B). After one year of treatment with LIPUS, he had achieved better walking independence with improved quality of life.
Conclusions: LIPUS can be a noninvasive option for therapeutic angiogenesis to improve ischemic limb conditions in patients with peripheral arterial disease and to avoid limb amputation.

Poster No. 105
Abstract No. 1795403
Spontaneous arterial dissections and external iliac artery agenesis
1Franciscan Health; 2Kent Hospital; 3Rhode Island Medical Imaging; 4Harvard Medical School
Background: Spontaneous coronary artery dissection (SCAD) is an important cause of acute coronary syndrome, particularly in women. The pathogenesis of SCAD is unknown but may be linked to extra-coronary vascular abnormalities.
Case presentation: A 69-year-old female presented with abrupt onset of chest pain. Electrocardiogram demonstrated ST-segment elevation in inferior leads. At the time of coronary angiography (CA), femoral angiogram revealed focal dissection of the right external iliac artery. CA revealed acute subtotal occlusion of the right posterolateral branch (consistent with type-2 SCAD), and normal appearance of the remainder of the epicardial coronary arteries. Coronary intervention was not performed. Transthoracic echocardiography demonstrated low-normal left ventricular systolic function and mitral valve prolapse with moderate regurgitation. Outpatient computed tomography angiogram confirmed chronic focal dissection of the right EIA (Fig. B, C). The left EIA was absent, and there was a persistent common iliac artery coursing posteriorly, giving rise to superior and inferior gluteal arteries before turning anteriorly toward the inguinal ligament (Fig. A-D). Infra-inguinal arterial anatomy of the left lower extremity was normal. No aneurysm or stenosis was identified. No evidence of fibromuscular dysplasia was identified based on carotid and renal arterial duplex ultrasound. Finally, genetic testing using Invitae arrhythmia/cardiomyopathy/hereditary hemorrhagic telangiectasia/vascular malformations panels (194 total genes) revealed variants of uncertain significance in HCN4 (c.697A>T) and KCNK3 (c.1054C>T).
Conclusions: During management of acute coronary syndrome due to SCAD, our patient was found to have two unusual abnormalities of the arterial system, i.e. chronic focal dissection of the right EIA and agenesis of the left EIA. Congenital anomalies of the iliac arteries are uncommon, with the most recognized form being persistent sciatic artery and having a prevalence of 0.03-0.06%. Agenesis of the EIA with persistence of the CIA appears to be a distinct and extremely rare entity. Whether these cardiovascular abnormalities share a common genetic and/or epigenetic thread warrants further study.

Cardiovascular abnormalities of the case.
Poster No. 106
Abstract No. 1795448
Recurrent subclavian steal syndrome causing global coronary insufficiency
1Kent Hospital; 2Lifespan Cardiovascular Institute; 3Harvard Medical School
Background: Subclavian artery stenosis is an uncommon but important cause of ischemic events in patients with ipsilateral mammary artery bypass. As more patients enjoy longevity following coronary artery bypass graft (CABG), surveillance for subclavian stenosis becomes an important part of cardiovascular evaluation.
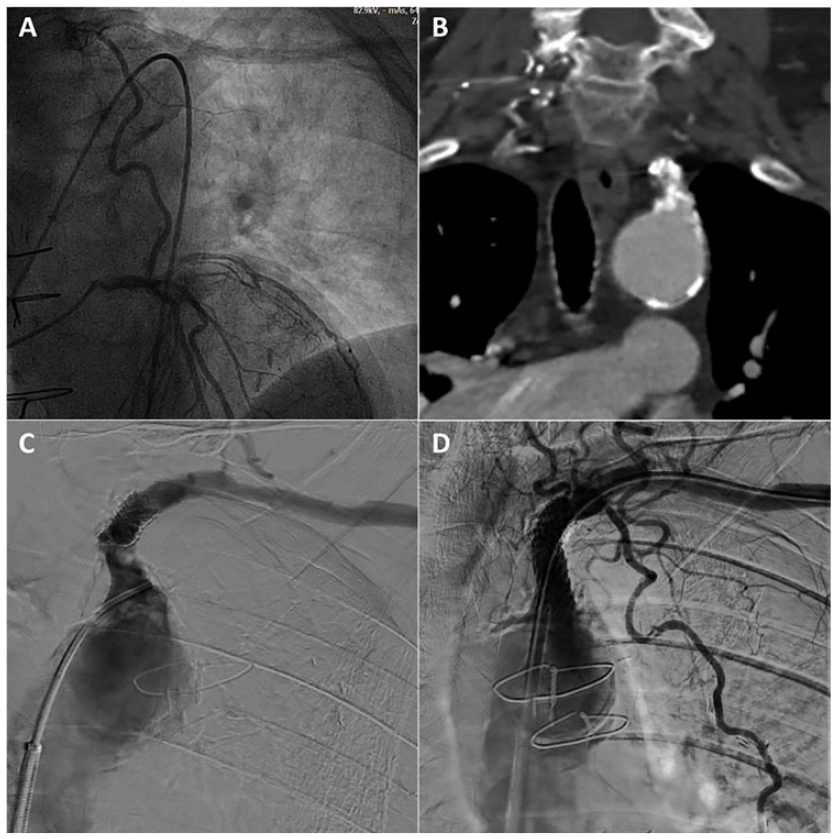
Case presentation: A 76-year-old male with atherosclerotic cardiovascular disease who underwent CABG at age 53, including left internal mammary artery (LIMA) to left anterior descending artery, was admitted after developing severe chest pain after washing car with left hand. At age 66 he developed angina and was found to have left subclavian artery stenosis proximal to the LIMA graft. He underwent left subclavian artery (LSA) stenting but did not follow up. On current presentation, he was hypotensive with diffuse ST-segment depression and ST elevation in lead aVR on ECG. Exam was notable for a non-palpable left radial pulse. He underwent urgent coronary angiography, which revealed severe native coronary artery stenosis with a patent LIMA graft. However, there was focal severe and calcified stenosis in the LSA at stent edge, causing subtotal occlusion (C), with flow reversal in the LIMA (A). The lesion was confirmed by CT angiogram (B). The patient underwent successful LSA stenting, requiring retrograde wiring to cross the severely calcified stenosis. Intravascular lithotripsy was employed to fully dilate the lesion before a balloon-expandable covered stent was deployed (D). The patient remained asymptomatic and remained asymptomatic.
Conclusions: Significant subclavian artery stenosis is present in 2.7 to 5% of patients at time of CABG surgery. Following CABG, onset of subclavian artery stenosis may lead to coronary ischemia, called coronary-subclavian steal syndrome (CSSS). Our case demonstrates the importance of long-term surveillance in patients with known CSSS. Furthermore, calcified subclavian lesions may benefit from IVL before stenting to allow adequate stent expansion and minimize complications. This promising technology may indeed lead to improved long-term procedural success/stent patency.
Poster No. 107
Abstract No. 1795547
Multiple coronary aneurysms after COVID-19 multisystem inflammatory syndrome
1University Hospitals Cleveland Medical Center; 2Case Western Reserve University
Background: Multisystem inflammatory syndrome in adults (MIS-A) has been described as a complication of COVID-19 infection. It has been associated with multiple vascular conditions including coronary complications.
Case presentation: A 25-year-old woman with no significant past medical history presented with fatigue, back pain, and cervical adenopathy along with inflammatory marker elevation. She was initially treated for retropharyngeal abscess but ultimately diagnosed with MIS-A as a result of mild COVID-19 infection one month before presentation. She then developed acute substernal chest pain. Electrocardiogram showed diffuse ST segment elevations and hs-troponin level was elevated with peak 10,912 ng/L leading to a diagnosis of myopericarditis. A coronary CT angiogram also showed long segment aneurysmal dilation of the left anterior descending coronary artery (LAD) with a maximum diameter of 1.0 cm, along with diffuse ectasia of the entire right coronary artery (RCA) with a maximum diameter of 0.9 cm. There was also a focal area of aneurysmal dilatation within the left circumflex artery (LCX) between the first and second obtuse marginal branch origins. There was no calcification and there was no involvement of the left main coronary artery. MRA of the thoracic aorta revealed no evidence of aortitis. She was treated with Intravenous Immunoglobulin, (IVIG), corticosteroids, aspirin, and oral anticoagulation. Repeat imaging 2 months later with slight regression of the dilatation within the LAD and RCA.
Conclusions: MIS-A associated with COVID-19 is a rare entity that if unrecognized can lead to serious complications. Due to the increased recognition of the role of IVIG for aneurysm regression, vigilance is necessary for diagnosing coronary aneurysm among patients with MIS-A with potential cardiac symptoms.

Top: (LEFT) RCA aneurysm measuring 8.6 cm (RIGHT) RCA aneurysm regression to 7.9 cm 2 months later. Bottom: (LEFT) LAD aneurysm measuring 8.2 cm (RIGHT) LAD aneurysm regression to 7.3 cm 2 months later.
Poster No. 108
Abstract No. 1795599
Isolated right internal iliac artery aneurysm rupture
1Philippine Heart Center
Background: We present the case of a 73-year-old, male who came in for right lower quadrant pain, initially managed as a case of acute appendicitis. Diagnostic laparoscopy found a cystic lobulated hematoma in the right lower quadrant. A CT aortogram confirmed a saccular right internal iliac artery aneurysm. He underwent surgical repair and was discharged stable.
Case presentation: A 73-year-old male hypertensive diabetic was admitted for 3-week history of intermittent dull ache in the hypogastric area, not related to defecation and urination, accompanied by development of a movable, tender lymph node in the right inguinal area with pain that radiated to both testicles. Two weeks prior, progression of pain now radiating to the right lower quadrant and back, accompanied by dysuria and numbness over the right thigh prompted consult at a local hospital. Urinalysis was normal. Workup for appendicitis was done at another hospital. Diagnostic laparoscopy showed cystic lobulated hematoma adherent to the terminal ileum and cecum. The appendix was normal. A JP drain was left in place. A CT aortogram was done which confirmed a saccular iliac artery aneurysm. He was then transferred to our institution for surgery. An ABI of 1 was obtained bilaterally. Examination revealed Grey Turner sign right, no palpable mass, direct tenderness but no rebound tenderness on the right lower quadrant. No testicular swelling. CT aortogram done at the previous hospital showed aneurysmal dilatation of the right internal iliac artery 5.1 x 6.0 x 7.4 cm. Hematoma formation seen within the right retroperitoneum and paracolic region with anterior displacement of the bowels 7.7 x 11.2 x 18.3 cm. Estimated volume of 825cc. He underwent Emergency Repair with evacuation of hematoma. There were no intraprocedural complications. He was discharged stable home on the 10th postoperative day.
Conclusions: Iliac artery aneurysms are rare. Symptoms can mimic other abdominal diseases; hence, a thorough clinical examination and a high index of suspicion is needed. CT scan is the preferred imaging. Retroperitoneal bleeding, testicular swelling and thigh/ back pain are telling of a ruptured iliac artery aneurysm. Endovascular repair is the first line therapy for internal iliac artery aneurysms.
Intraoperative image of the retroperitoneal hematoma.
Poster No. 109
Abstract No. 1757034
Post-Bentall procedure cardiac tamponade: a case report
1Makati Medical Center
Background: Cardiac tamponade is a rare but potentially fatal complication of cardiac surgery. Regional tamponade may result from localized pericardial effusion following open-heart surgery. Coagulopathy as an adverse effect of cardiopulmonary bypass has been established, and this plays a role in the pathogenesis of post-surgical effusions. Early recognition is critical for optimal management and favorable outcome.
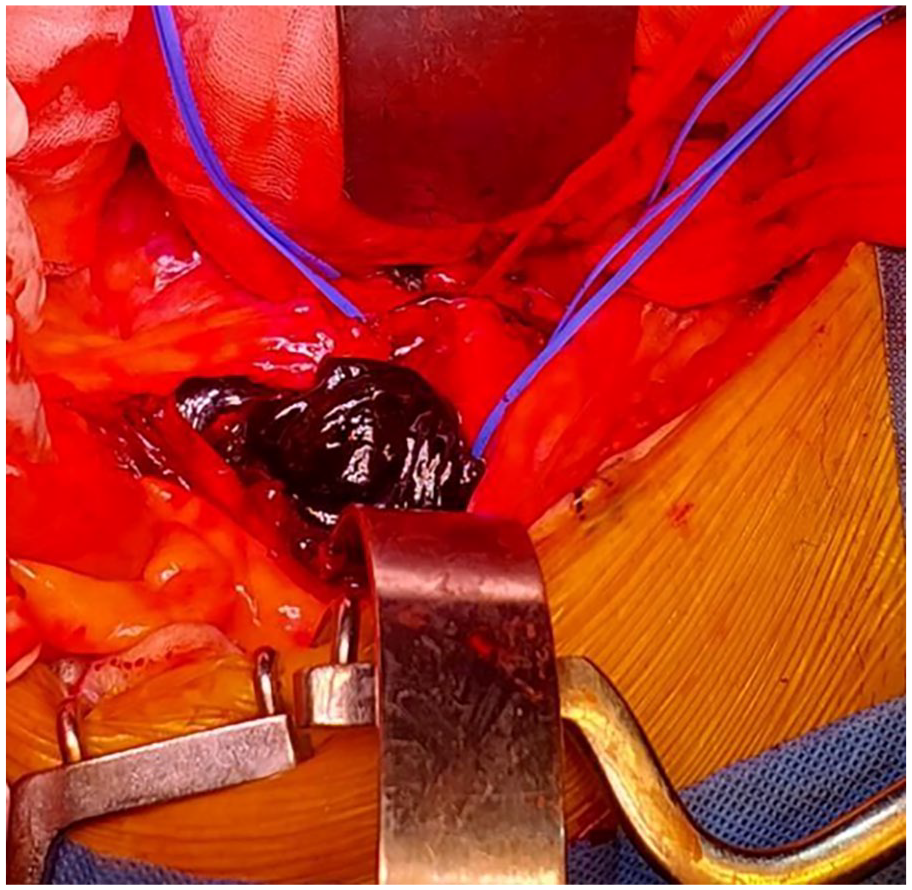
Case presentation: A 57-year-old male with bicuspid aortic valve, severe aortic stenosis, and aortic root aneurysm, complaining of intermittent episodes of angina during exertion for the past year, underwent an uneventful Bentall procedure. In the recovery room, chest tube drain was bloody. Monitoring recorded more than 300 ml per hour on the second and third hour post-surgery, hence tranexamic acid was administered intravenously. On the fourth hour post-surgery, the patient presented with sudden decrease in blood pressure (51/40 mmHg), tachycardia (125 bpm), and decreased sensorium. Further physical examination revealed weak pulses and cold extremities. Heart sounds were not distinct due to the very rapid rate. Prothrombin time was elevated at 15 second while platelet count was decreased at 109x10^9/L. Despite fresh frozen plasma and platelet transfusions, aggressive fluid administration and vasoactive medications, he remained unresponsive. Immediate point-of-care ultrasound of the heart noted a pericardial effusion and a collapsed right atrium. Emergency re-exploration for bleeding was performed which revealed no active bleeding from the surgical site but noted 500 ml of blood and blood clots pressing against the right atrium. After the procedure, the patient's hemodynamics returned to normal and was eventually discharged. Two weeks post-procedure, he was asymptomatic with improved exercise tolerance. Echocardiography revealed no signs of periaortic leakage from the repaired aorta.
Conclusions: Cardiac tamponade after an open-heart surgery may occur immediately or within days. Surgical intervention is necessary for cardiac tamponade that occurred within 24 hours post-surgery to identify and address the source of bleeding.

Blood clots evacuated from the pericardium on re-exploration.
Poster No. 110
Abstract No. 1758162
Alport syndrome: catheter woes, access failures, thrombosis troubles
1The Medical City
Background: According to a study conducted by the National Center for Biotechnology Information (NCBI), the overall incidence of primary arteriovenous fistula (AVF) failure is 23.9%. In this regard, Alport syndrome is a rare but significant cause of renal failure, distinguished by genetic mutations in type IV collagen. A study by Field et al. found that pseudoaneurysms occur at a rate of 2-10% in this population. Central line complications include catheter thrombosis, which accounts for 10% of all deep venous thrombosis (DVT) in adults. This rare case describes the critical decision points involved in managing a complex patient with catheter-related thrombosis, Alport syndrome, and multiple access site failure.
Case presentation: A 24- year-old female with Alport Syndrome and multiple access site failure who was undergoing hemodialysis developed swelling and pain in her right thigh. Compression ultrasonography revealed an acute deep vein thrombosis. A bruit was noted on the left arteriovenous (AV) graft. The right lower extremity exhibited grade 2 edema, warmth, and tenderness. An AV graft ultrasound was performed for monitoring which revealed a pseudoaneurysm but no significant stenosis. She had a left AV graft repair which revealed a 4-cm pseudoaneurysm and a 0.5-cm graft defect. Heparin was resumed. On the second day, no bruit or thrill was detected, necessitating a thrombectomy and the implantation of a new AV graft in her left arm. The initial success was followed by graft thrombosis, and heparin was continued. Serial ultrasounds revealed a mild improvement in flow, and she was discharged with apixaban. Two weeks later she was seen more comfortable with regression of right thigh swelling. A repeat ultrasound revealed normal flow and she was cleared to use the AV graft, with the goal of eventually removing the femoral catheter.
Conclusions: The interaction of catheter-directed thrombosis in a patient with Alport Syndrome and multiple access site failure poses a challenge that necessitates a multidisciplinary approach to management. In this situation, careful planning is required to ensure that the risks and benefits of each approach for maximizing access are balanced against their advantages and disadvantages.
Poster No. 111
Abstract No. 1766184
Symptomatic extrahepatic portal vein aneurysm in a non-cirrhotic patient
1Philippine Heart Center
Background: Venous aneurysms are less common than arterial aneurysms; those of the portal vein are relatively rare, in some series accounting for only 3% of all venous aneurysms. Majority of portal vein aneurysms in adulthood are associated with portal hypertension or liver cirrhosis. Small aneurysms are asymptomatic, whereas large aneurysms may cause compressive symptoms, obstruction of the biliary tree, thrombosis, or even rupture.
Case presentation: We present the case of a 49-year-old male, non-alcoholic, with no known comorbidities, with a 5-year history of epigastric and right upper quadrant pain. Abdominal CT scan done last 2019 showed a portal vein aneurysm measuring 5.2 x 8.1 x 5.6 cm. He was started on losartan and amlodipine, taken with good compliance. Gradual enlargement and increasing frequency of symptoms were noted hence he was admitted. Physical examination was negative for signs of chronic liver disease or portal hypertension. Repeat scan an aneurysmally dilated extrahepatic portal vein measuring 5.5 x 8.9 x 8.8 cm, dilated right portal vein, with no signs of portosystemic collateral formation, and no cirrhotic changes in the liver. Doppler ultrasound of the portal vein likewise showed an aneurysmally dilated main portal vein with hepatofugal flow and generalized decrease in portal flow velocity and increased portal vein diameter, with no evidence of portal vein thrombosis, and normal bilateral hepatic vein flow pattern. He underwent portal vein aneurysm repair via polytetrafluoroethylene (PTFE) graft interposition (16 mm x 5.16 mm x 6 cm x 19 mm x 5 mm), cholecystectomy, and ligation of splenic vein. Post-operatively, no complications were noted, and repeat scan showed PTFE graft seen near the hepatic hilum anastomosed to the superior mesenteric vein with a length of 6.8 cm and a caliber of 2.2 cm, patent, with no evidence of thrombus formation or anastomotic leak. Aspirin and antihypertensive medications were given post-operatively and the patient was subsequently discharged improved.
Conclusions: This case presents a successful management of a non-portal hypertensive, non-cirrhotic adult male with portal vein aneurysm and highlights the need for further studies in order to properly define the management of such patients.
Poster No. 112
Abstract No. 1767412
Aortic dissection: the covert actor behind neck swelling
1The Medical City
Background: A right-sided arch is a congenital anomaly of the aortic arch with an estimated prevalence of 0.05-0.1%. This can result from a disordered embryogenesis of the branchial arches with either abnormal persistence or involution of embryonic vascular segments. This is a case showing the decision points involving an uncommon presentation of this rare disease entity in the context of concomitant COVID-19 infection.
Case presentation: An 80-year-old woman with hypertension, a thoracic descending aortic aneurysm, and a right-sided aortic arch with Kommerell diverticulum presented with a four-day history of cough and chest tightness, which was initially diagnosed as COVID-19 pneumonia. Her condition deteriorated, necessitating intubation and ICU admission. In the ICU, a non-erythematous submandibular mass developed. A subsequent neck CT revealed a significant retropharyngeal hematoma, most likely caused by Kommerell diverticulum rupture, along with diffuse neck edema. Chest CT revealed an aortic dissection with rupture, as well as mediastinal and retropharyngeal hematomas. Anemia and hypotension necessitated further investigation. A 2D- echo revealed a large pericardial effusion with early tamponade signs. A pericardiostomy removed 200 mL of serosanguinous fluid, and thoracic endovascular aortic repair (TEVAR) was performed concurrently. Intraoperatively, an abnormal central arterial system was discovered, with the right common carotid and right subclavian arteries serving as the first and second branches of the aortic arch, respectively. The left common carotid emerged as the third branch, with the descending thoracic aorta located in the right thoracic cavity. Graft deployment from the distal descending thoracic aorta, landing proximally in zone 2, resulted in a successful post-deployment angiogram with no endoleak. However, the post-operative course was marked by acidosis and an increasing pressor requirement, which resulted in the patient's unfortunate death.
Conclusions: Managing dissections of a right-sided aortic arch is challenging due to its rarity. This requires a comprehensive approach that considers patient anatomy, existing health conditions, and the available specialized knowledge.
Poster No. 113
Abstract No. 1772349
Case-report of bilateral subclavian and axillary artery stenosis
1Staten Island University Hospital
Background: Large vessel vasculitis (LVV) manifests as the inflammation of large blood vessels, such as the aorta and its main branches. The leading cause of mortality in patients with LVV is cardiovascular disease.
Case presentation: A 63-year-old white woman with no PMH was hospitalized for shortness of breath. She was diagnosed and treated for acute intermediate-risk PE and new onset HFrEF (EF 17%). Hypercoagulable workup was negative and cardiac catheterization negative for significant CAD. The patient was discharged on DOACs, with a life vest, and started on goal-directed medical therapy (GDMT). A repeat TTE 3 months post-discharge showed improvement of EF to 42% and the life vest was discontinued. As her activity improved, she started to complain of claudication symptoms in the bilateral (B/L) (L > R) upper extremities (UE) and intermittent tinnitus. Her outpatient course was complicated with low B/L UE BP readings interfering with GDMT and she was referred to vascular cardiology for evaluation. The referring physician ordered a repeat CTA Chest that revealed resolution of PE and short segment stenosis within the proximal portion of the right subclavian artery and a repeat ESR which increased from hospital values of 78 to 130 and CRP from 36 to 72.8. In the vascular clinic, US duplex UEs revealed diffuse wall thickening and severe (>75% stenosis) B/L subclavian and axillary artery stenosis. (Figure 1) US duplex carotid revealed R and L ICA < 50% stenosis and R and L ECA elevated velocities. CTA Head/Neck was performed and confirmed smooth circumferential mural thickening involving the visualized aortic arch, great vessel origins, and B/L subclavian arteries and revealed severe long segment B/L subclavian artery stenoses. It also showed severe craniocervical stenosis/occlusion of the right and left vertebral arteries. She was diagnosed with LVV and advised to switch to life-long Coumadin. She started prednisone, 40 daily tapered slowly down to 10 daily over 6 months, with resolution of UE claudication.
Conclusions: Despite advances in our understanding and ability to manage LVV, morbidity remains high. Future advances should include an improved understanding of pathogenesis, earlier diagnosis, and more targeted therapeutic approaches to LVV.
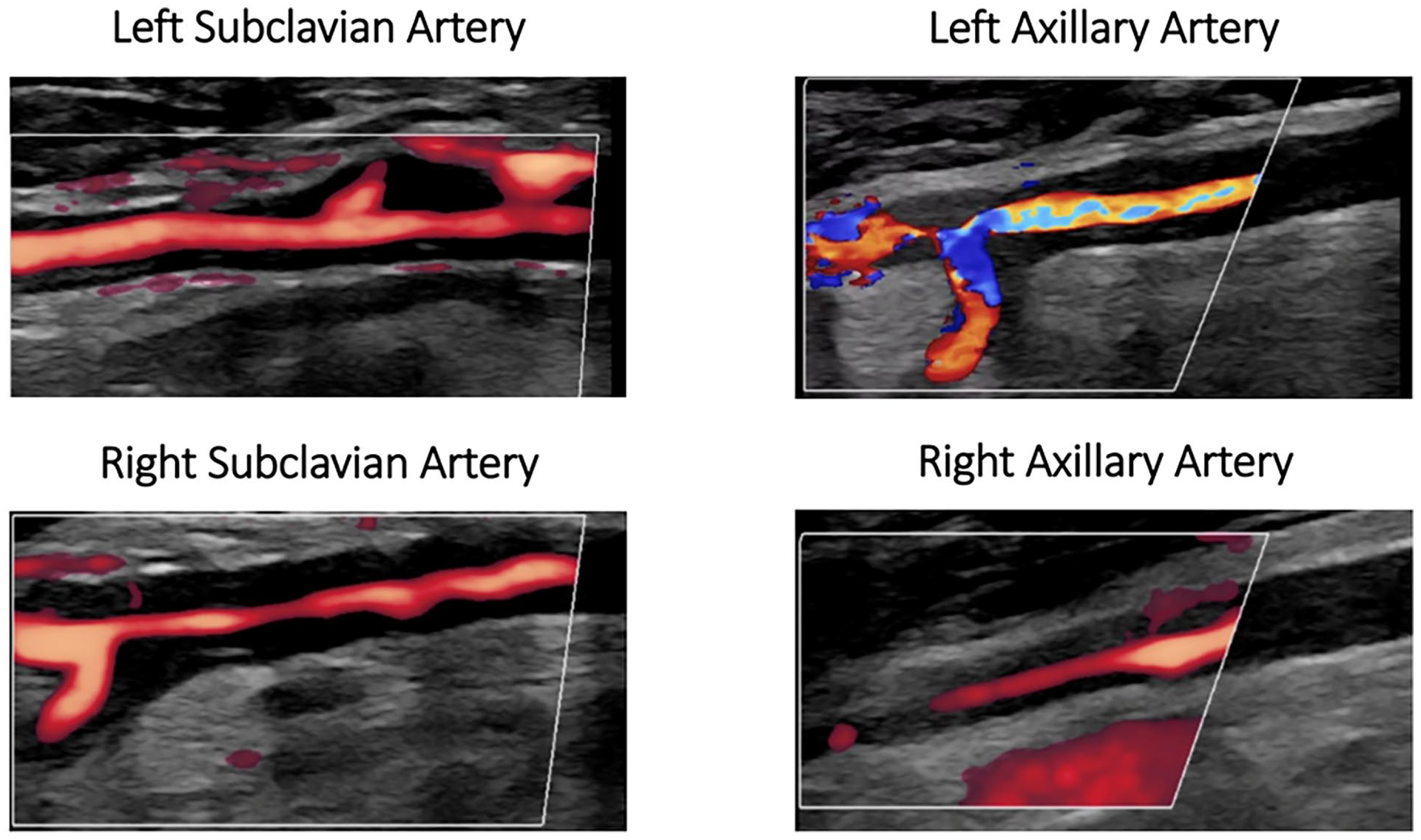
Power Doppler of bilateral subclavian and axillary arteries.
Poster No. 114
Abstract No. 1772822
Monoclonal gammopathy of thrombotic /thrombocytopenic significance (MGTS): hit-like pathology
1Mayo Clinic
Background: Monoclonal gammopathy of thrombotic/thrombocytopenic significance (MGTS) is a recently described heparin-independent, persistent thrombotic condition that is mediated by monoclonal anti-platelet factor 4 (PF4) antibodies.
Case presentation: An 80-year-old patient with a complex medical history was hospitalized due to a sub-massive bilateral pulmonary embolism (PE, DVT). During the hospitalization, the patient was found to have multiple acute ischemic strokes, and further developed transient ischemic attack events even during transient cessation of anticoagulation for planned procedures. His history was significant for prior thrombotic events: Twelve months prior to admission (unprovoked PE), one month prior to admission (acute limb ischemia, ALI that required emergent thrombectomy) as well as ST-elevation MI and small vessel ischemic stroke a few years prior. Platelets were below 50,000/uL when symptoms started. The patient tested weakly positive for anti-platelet factor-4 (PF4) antibodies by HIT ELISA and was negative in the serotonin release assay (SRA). Thrombocytopenia during the thrombotic episodes (e.g., critical limb ischemia, PE, DVT) raised suspicion for a HIT-like platelet factor 4 (PF4)-dependent platelet activating antibody which was confirmed by the PF4-dependent P-Selectin expression assay (PEA). Furthermore, due to multiple thrombotic episodes over months-years, MGTS was suspected. Standard immunofixation did not detect a monoclonal gammopathy. Anti-PF4 antibodies were isolated from patient serum and characterized by mass spectrometry, that confirmed the presence of a monoclonal anti-PF4 antibody (Figure).
Conclusions: MGTS, a recently described heparin-independent entity characterized by persistent anti-PF4 antibodies was the cause of thrombotic thrombocytopenia in our patient. This case highlights the possibility of unusual HIT serology in MGTS (e.g. negative SRA and negative M-spike on standard testing). This case highlights the need for diagnostic testing using PF4-treated platelets (e.g., PEA, PF4-enhanced SRA) and evaluation of anti-PF4 antibody clonality when MGTS is suspected.
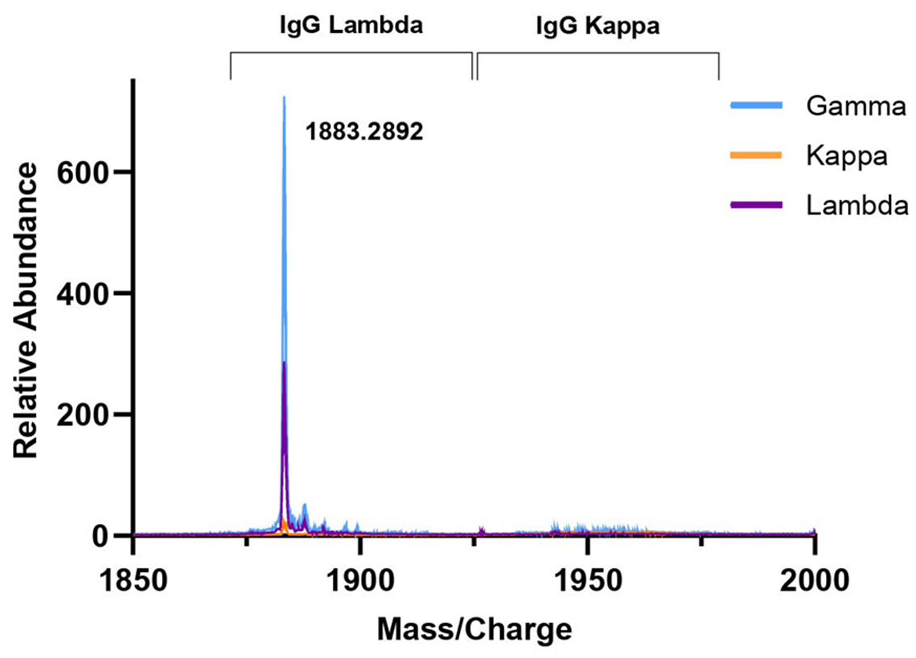
Characterization of monoclonal anti-PF4 antibodies from patient serum using mass spectrometry.
Poster No. 115
Abstract No. 1772911
Catastrophic vascular manifestations of infective endocarditis
1Makati Medical Center
Background: Infective endocarditis, a condition marked by microbial infection of the heart's inner lining and valves, still carries high mortality rates despite medical progress. It is complicated by systemic embolism which is a frequent occurrence with infective endocarditis. We present a case of infective endocarditis with multiple vascular complications.
Case presentation: A 26-year-old man presented to the emergency department with shortness of breath, initially managed as a COVID-19 infection based on symptoms and a positive RT-PCR result. His blood cultures were positive for Staphylococcus aureus. Despite initial stability, subsequent days revealed complications including thrombocytopenia, gastrointestinal complaints and splinter hemorrhages in the fingers of both hands, On the 9th hospital day, the patient experienced an episode of unresponsiveness and seizure and patient developed complete heart block developed, acute pulmonary embolism involving the segmental arterial branch in the left lower lobe, renal and splenic infarcts and acute limb ischemia of the bilateral lower extremities. The patient also developed an acute onset right-sided motor deficit. Cranial CT scan revealed a massive infarct involving the left insula, left temporal and occipital lobes. The patient eventually underwent thrombectomy of the right lower extremity where thrombi were extracted along the right distal popliteal artery, tibio-peroneal trunk, and distal posterior tibial artery. 3D echocardiogram was performed, revealing vegetation along the posterior leaflet of the bicuspid aortic valve and suspicious abscess formation. On the 17th hospital day, the patient underwent on-pump aortic valve replacement. Post-operatively, the patient experienced significant hemodynamic instability and multi-organ dysfunction, requiring V-A Extracorporeal Membrane Oxygenation. The patient ultimately expired on the 19th hospital day.
Conclusions: Vascular complications associated with infective endocarditis significantly increase morbidity and mortality. This case underscores the vital importance of collaborative teamwork among various specialties in addressing the complexities of infective endocarditis management.
Poster No. 116
Abstract No. 1772964
Systemic sclerosis presenting with isolated right ventricular dysfunction
1Makati Medical Center
Background: Systemic sclerosis is a multisystem disease and can lead to multitude of vascular dysfunction and a wide variety of cardiac abnormalities. The associated pulmonary artery hypertension has a poorer prognosis than idiopathic cases. We present a case of systemic sclerosis initially presenting as right ventricular dysfunction diagnosed by nailfold capillaroscopy.
Case presentation: A 73-year-old female presented to the Emergency Department with cyanosis and hypotensive episodes. Transthoracic echocardiography revealed a dilated and akinetic right ventricle with apical sparing and severe pulmonary hypertension. Initially managed for suspected acute pulmonary embolism, prompting increase in Enoxaparin to therapeutic dose. On the 1st hospital day, there was still hemodynamic instability prompting initiation of inotropes and referral to interventional cardiology for an emergency coronary angiogram due to a suspicion of right ventricular infarct secondary to acute coronary syndrome. However, no lesion in the right coronary artery was found. Subsequently, stabilization of vital signs, renal function improvement, and normalization of potassium levels were observed. CT pulmonary angiography eventually ruled out acute pulmonary embolism. By the fifth hospital day, cautious diuresis led to a significant decrease in pulmonary artery pressure from severe to mild. Despite this improvement, bluish discoloration on all fingernails and difficulty in obtaining finger oxygen saturation were noted, leading to the initiation of calcium channel blockers for Reynaud’s phenomenon. Nailfold capillaroscopy was performed showing presence of multiple anomalies (ramifications, giant capillary loop, and low capillary densities) suggestive of late-stage scleroderma pattern.
Conclusions: Systemic sclerosis presents complex challenges due to its diverse cardiovascular manifestations, including pulmonary artery hypertension. Timely recognition and management are essential to mitigate cardiovascular compromise and prevent adverse outcomes. This case underscores the significance of a comprehensive approach to diagnosis, highlighting the role of nailfold capillaroscopy in diagnosing systemic sclerosis.
Poster No. 117
Abstract No. 1773641
Giant aneurysmal iliac artery causing deep venous thrombosis
1Cleveland Clinic
Background: The occurrence of deep venous thrombosis (DVT) is more common in left lower extremity compared with the right, and this disparity could partly be attributed to extrinsic compression of the left common iliac vein. In the majority of cases, compression is caused by the right common iliac artery, called May-Thurner syndrome. Our case is unique because the mechanical compression of the left common iliac vein is caused by ipsilateral aneurysmal common iliac artery.
Case presentation: 66-year-old man with active tobacco use and stable coronary artery disease, who presented to the primary care provider’s office with redness and swelling in his left lower extremity. He denied any trauma, recent hospitalization, surgery, long distance travel or malignancy. His vital signs were normal. He underwent venous duplex ultrasound that revealed incompressible left-sided popliteal, femoral and calf veins, consistent with an acute DVT. He subsequently underwent computed tomography (CT) of the abdomen and pelvis to rule out May-Thurner syndrome. CT scan, instead, showed a large aneurysm of the left common iliac artery measuring 5.1 x 5.3 x 7.8 cm, causing extrinsic compression of the left common iliac vein against the vertebral body (Figure A-C). Additional findings included right common iliac artery aneurysm measuring 2.6 x 3.1 x 4.4 cm, and short segment ectasia of the infrarenal abdominal aorta with mural thrombus. The patient was started on anticoagulation with rivaroxaban. After completion of 3 months of anticoagulation, he underwent transperitoneal infrarenal abdominal aorta and bilateral common iliac artery aneurysm repair with Gelsoft graft. Given provoked nature of the DVT due to extrinsic compression, anticoagulation was eventually stopped after surgery. He did not experience any recurrent events at the 6-month outpatient follow up.
Conclusions: Left-sided DVT can rarely be caused by mechanical compression of the left common iliac vein by ipsilateral aneurysmal common iliac artery. While anticoagulation is initially warranted for DVT, aneurysmal repair is the ultimate treatment.

Axial view (A), sagittal view (B) and coronal view (C) – red arrows showing large left common iliac artery compressing left common iliac vein against the vertebra.
Poster No. 118
Abstract No. 1775354
Case report: recurrent PE with an unusual path
1University of Michigan
Background: Recurrent pulmonary emboli (PE) despite anticoagulation may have multiple causes, including malignancy. Reports of recurrent tumor emboli developing into chronic thromboembolic pulmonary hypertension (CTEPH) are rare.
Case presentation: A 57-year-old male presented with dyspnea – workup found small segmental acute PE and he was discharged on direct oral anticoagulant (DOAC). He re-presented with worsened symptoms, increased thrombus burden, and was diagnosed with intermediate-high risk PE. Catheter thrombectomy reduced thrombus burden but hemodynamics and symptoms were unchanged. Formal right heart catheterization and pulmonary angiogram indicated surgically accessible CTEPH. Surgical pulmonary thromboendarterectomy removed significant mixed acute-on-chronic appearing thrombi, yielding normalization of pulmonary hemodynamics and symptom resolution. Operative pathology unexpectedly found a malignancy, subsequently identified as urothelial origin on further testing. Despite oncologic therapies and enoxaparin, the patient had more recurrent PE and malignancy progression.
Conclusions: Recurrent PE despite anticoagulation should prompt comprehensive investigation for subtherapeutic anticoagulation and underlying disease states such as malignancy or hematologic disorders. In patients with malignancy-related PE, DOAC or enoxaparin therapy are recommended, but guidance for breakthrough cases is sparse. The management of tumor emboli and chronic presentations can prove further challenging.
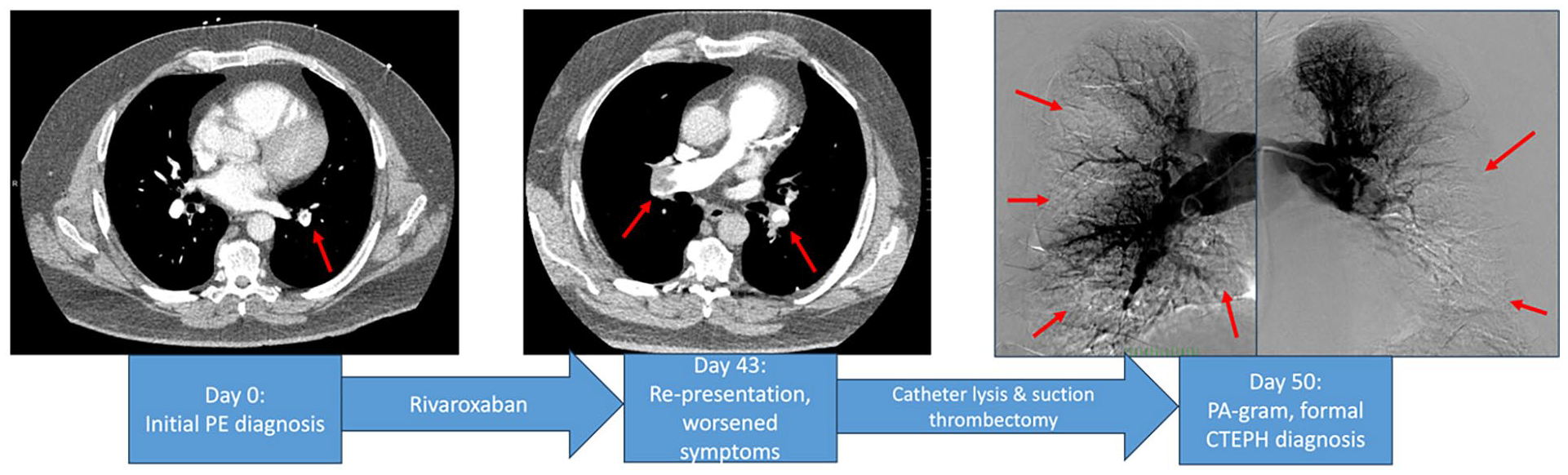
Progression from initial CT imaging to CTEPH diagnosis on pulmonary angiogram.
Poster No. 119
Abstract No. 1775434
Retrograde-transpedal intervention among patients with chronic limb-threatening ischemia
1Chong Hua Hospital
Background: Chronic limb-threatening ischemia (CLTI) is the most severe end of the disease spectrum of Peripheral Arterial disease (PAD). It affects 11% of patients with PAD and is associated with high rates of limb loss and mortality as well as high costs of care. Antegrade recanalization is associated with a high failure rate and retrograde transpedal approach has been used to overcome this limitation.
Case presentation: We are presented with four cases of patients with CLTI with varying symptomatology of PAD. All patients exhibit complex atherosclerotic occlusion in the arterial bed which poses a challenge in traditional cannulation. Retrograde transpedal approach was performed on all four patients. Three patients had successful revascularization while the last patient encountered difficulty in cannulation. Optimal medical management was implemented post-procedure.
Conclusions: Among patients with CLTI, the peripheral transpedal approach is a safe option for revascularization for complex lower extremities lesions. This approach has its advantages compared to the traditional antegrade approach. This case series discussed the first few patients in our country in which this technique was used wherein vascular medicine played a part in the patients' interventions.
Poster No. 120
Abstract No. 1775610
A case of multiple arterial dissections and beading
1University of Colorado School of Medicine; 2CPC Clinical Research, University of Colorado
Background: Arteriopathies can have overlapping clinical presentations which lead to diagnostic dilemmas.
Case presentation: A 45-year-old female presents with acute flank pain and found to have left renal infarct with left renal infarct with left renal segmental artery (LRA) occlusion on imaging. Catheter-based angiography and stenting of the LRA was performed. Bilateral renal artery beading was noted. During her hospitalization, a celiac artery dissection was diagnosed following evaluation of new abdominal pain and left vertebral dissection with right vertebral beading were found by surveillance CTA. Medical history: Raynaud's, Sjogren disease, hypothyroidism, miscarriages, migraines, abdominal hernia. Family history: Factor 5 Leiden (mother). Social history: No smoking or drug use. Recent husband death. Physical examination: Height and weight: 180 cm, 65 kg. Pectus excavatum. No hyperlaxity. The differential diagnosis following presentation included fibromuscular dysplasia, genetic arteriopathy, segmental arterial mediolysis, and less likely vasculitis. Thorough rheumatologic evaluation and hematologic hypercoagulability workup were unrevealing, and genetic testing revealed a variant of undetermined significance in the COL3A1 gene. No arterial biopsy was performed.
Conclusions: Conclusion: This case exemplifies the challenges in diagnosis of rare, non-atherosclerotic arteriopathies. This patient’s imaging was consistent with FMD, but she may have an additional arteriopathy as well.

Arterial dissections and beading.
Poster No. 121
Abstract No. 1775667
Treatment of total radial artery occlusion using rivaroxaban
1The Medical City
Background: Radial artery occlusion is one of the most common but significant complication of transradial catheterization procedures. It affects 3 to 5 % of patients undergoing cardiac catheterization and is typically asymptomatic due to the presence of dual arterial supply to the hand.
Case presentation: A 52-year-old female known case of type 2 diabetes mellitus, dyslipidemia, obesity, and bronchial asthma came in due to right forearm pain. About two and a half weeks prior, she underwent transradial cardiac catheterization due to anginal symptoms and easy fatigability in the background of a family history of cardiovascular diseases. A 5F introducer sheath was inserted with one attempt and a total of 5000IU heparin was given. Post procedure, radial pulse was good, and no immediate complications were noted. Five days after the procedure, she started having intermittent tearing right forearm pain and difficulty in sustaining hand grip but no paresthesia nor cyanosis of the digits or hand. She self-medicated with oral and topical pain relievers, which provided slight relief. Persistence of symptoms prompted follow up. Physical examination was notable for swollen right forearm, faint pulse over the right radial artery, capillary refill time of more than 2 seconds, pale and cold right hand with 10% sensory deficit over the right thenar area as well as inability to sustain hand grip. On Doppler, there was faint biphasic signal over the distal radial artery. Arterial duplex scan of the upper extremities revealed totally occluded right radial artery, hence, admission. She was given Heparin bolus of 80 IU/kg and continuous infusion at 18 IU/kg/hour adjusted accordingly. Heparin was shifted to Enoxaparin 180 mg daily in divided doses. She subsequently had decreased right forearm pain; weak pulse was noted over the right radial artery. Due to financial constraints, she opted to continue treatment with Rivaroxaban 15 mg twice daily as outpatient instead of Enoxaparin. After 3 months of treatment, repeat arterial duplex scan showed recanalization of radial artery occlusion.
Conclusions: Currently, treatment regimens for radial artery occlusion are scarce. This case shows that Rivaroxaban may be a promising treatment for patients with radial artery occlusion.
Poster No. 122
Abstract No. 1775718
Pelvic congestion syndrome in postmenopausal female
1St. Luke’s Medical Center, Dr. HB Calleja Heart and Vascular Institute
Background: Pelvic Congestion Syndrome is a medical condition that can cause a variety of symptoms in the abdomen, pelvis, and legs, and is most commonly found in women of reproductive age with multiple pregnancies. The most prevalent symptom is chronic pelvic pain that persists for at least 6 months. Non-specific symptoms may include pelvic heaviness, painful intercourse, painful periods, lower back pain, frequent urination, and signs of varicose veins in the vulva, perineum, buttocks, or lower limbs. Unfortunately, despite its prevalence, only 30% of cases are referred to specialists for evaluation, leading to misdiagnosis.
Case presentation: An 84-year-old postmenopausal female presented with recurrent low back pain associated with urinary retention, recurrent urinary tract infection, intermittent left leg heaviness, and edema. The physical exam was unremarkable. Significant surgical history was only for exploratory laparotomy with graham patching for duodenal ulcer. Abdominal ultrasound and CT scans did not demonstrate any pathological findings. The above symptoms were attributed to findings of disc desiccation in the lumbar spine MRI. Surface DUS finding of flow reversal within the superficial epigastric vein (SEV). Considering PCS, abdominal MRV was done demonstrating dilated and tortuous right parametrial veins and left ovarian vein measuring up to 0.7 cm as a unique finding. She underwent coil embolization of the left ovarian and right internal iliac veins, and sclerotherapy of the left ovarian vein. The patient was symptom-free during the follow-up visit.
Conclusions: This case is particularly unique, as there have been limited reports of postmenopausal women experiencing pelvic congestion syndrome, with a prevalence rate of just 0.5%. Additionally, our patient is presenting with atypical urological symptoms not associated with pelvic pain. This case underscores the significance of considering pelvic venous congestion syndrome as a potential diagnostic option for postmenopausal women experiencing low back pain and urinary frequency, even when other tests fail to yield positive results. It's worth noting that previous literature may suggest PCS is limited to premenopausal patients, but that's not the case.

Dilated left ovarian vein measuring 0.7 cm (yellow arrow) and parametrian vein (green arrow) and post-embolization venogram showing complete devascularization of the left ovarian and the tributary of the right internal iliac veins (orange arrow).
Poster No. 123
Abstract No. 1776085
When tumor thrombus is benign
1Mayo Clinic
Background: Tumor thrombus (TT) is solid tumor mass in a vascular lumen; cancer complicated by TT is associated with decreased survival. Not all TT originates from underlying malignancy; intravascular leiomyoma (IVL) is a form of benign TT of smooth muscle cells that may originate from and/or extend into local veins, the inferior vena cava (IVC), and even right heart and pulmonary arteries.
Case presentation: A 50-year-old woman was referred for evaluation of inferior vena cava (IVC) thrombosis and right adnexal mass. After previous laparoscopic cholecystectomy she developed abdominal pain; CT showed partial intestinal obstruction, IVC thrombosis (extending into the right internal but not external iliac vein), and a 2.3 cm solid right adnexal mass. After failed attempt at thrombectomy she was started on apixaban but had persistent dyspnea and leg swelling. Past medical history: PE, HTN, hysterectomy and BSO (due to uterine fibroids). Medications: apixaban, desvenlafaxine, gabapentin, metoprolol, vitamin D, and aripiprazole. Examination: BP 116/82 mm Hg; HR 92/minute; lungs clear; no cardiac murmurs; arterial exam was normal; pitting bilateral ankle edema was present. Testing: lower extremity DUS showed no thrombus from the level of the common femoral veins through the calf bilaterally. She had no identifiable molecular thrombophilia. TTE was normal except for low filling pressure; V/Q scan showed no chronic PE. Due to the expansile appearance of the IVC thrombus, TT was suspected and MRA showed continuity between thrombus and mass; post contrast MR images demonstrated heterogeneous enhancement of the TT. F-18 FDG PET-CT scan showed no abnormal uptake in the right adnexal mass or TT. Provisional diagnosis of IVL was made and she underwent resection of the right adnexal mass and the vena cava mass; pathology confirmed leiomyoma.
Conclusions: IVL is a type of TT which is considered a benign neoplasm but can behave in an infiltrative and obstructive manner, with vena cava and intracardiac extension possible. Negative PET-CT in the setting of apparent TT should increase suspicion for IVL. Although complex surgery may be required, prognosis is excellent with low incidence of recurrence with complete resection.
Poster No. 124
Abstract No. 1776329
A vexing case of VEXAS
1Stanford University School of Medicine
Background: VEXAS (vacuoles, E1 enzyme, X-linked, autoinflammatory, somatic) is an adult-onset syndrome that links disparate multi-organ auto-immune and hematological symptoms. It is a monogenic disease caused by acquired somatic mutations in UBA1, an X-linked gene that encodes for the master enzyme of cellular ubiquitylation.
Case presentation: 80 M was referred to hematology for evaluation of leukopenia and thrombocytopenia. He was then hospitalized for hematemesis and melena. While hospitalized, he was diagnosed with a right superficial femoral DVT, and Apixaban was started. However, he developed right calf and thigh swelling about 3 months later and was found to have a right femoral to popliteal DVT. Warfarin was started due to concern for DOAC failure. A hypercoagulable workup was negative. Due to persistent bicytopenia, he underwent a bone marrow biopsy, which revealed hypercellular marrow (80-90%) with multilineage dysplasia and 1-2% blasts. Neogenomics panel reported DNM3TA and UBA1 M41T mutations. He was diagnosed with low-risk MDS with multilineage dysplasia (MDS-MLD). Pathologists noted an increase in cytoplasmic vacuoles in a subset of myeloid and erythroid precursors, which, in the context of recurrent thromboses, despite anti-coagulation, raised the possibility of VEXAS syndrome. He soon developed erythematous and violaceous papules and plaques on the forehead, cheeks, chest, forearms, arms, and back associated with night sweats and intermittent fevers. A skin biopsy showed neutrophilic dermatoses with admixed CD163-positive, MPO-positive cells and concurrent vasculitic changes- features commonly reported in association with VEXAS syndrome. He was treated intravenous solumedrol and was discharged on a prednisone taper. However, any attempts to decrease prednisone dose below 50 mg daily, would lead to the development of skin ulcerations (VEXAS flare). It is unknown whether wounds related to VEXAS also demonstrate pathergy like other neutrophilic dermatoses such as pyoderma gangrenosum.
Conclusions: VEXAS syndrome is challenging to diagnose and manage. It should be considered in the differential diagnosis of individuals presenting with unexplained hematological and pro-inflammatory abnormalities.
Poster No. 125
Abstract No. 1777822
Gangrene of the digits: a case of calciphylaxis
1Texas Tech University Health Sciences Center, El Paso; 2Paul L. Foster School of Medicine; 3Lahey Clinic
Background: Deposition of calcium in small and medium-sized vessels leading to tissue ischemia and necrosis, known as calciphylaxis, is a rare but painful and potentially life-threatening condition. It is predominantly seen in patients with end-stage renal disease (ESRD) on renal replacement therapy. The diagnosis may be supported by a bone scan or a skin biopsy, but negative results do not exclude it. Due to its high morbidity and mortality, prompt identification of calciphylaxis is crucial for the appropriate treatment of these patients.
Case presentation: A 53-year-old male with a history of ESRD on peritoneal dialysis, former smoker, diabetes mellitus, blind right eye, and hypertension was evaluated for progressive, painful black discoloration of the fingers. The lesion was initially seen on the right 4th digit but gradually progressed over 5 months to involve multiple digits with small ulcers. Laboratory testing showed normal platelet count and hyperparathyroidism with a Calcium-phosphate product of 67. Autoimmune and hypercoagulability work-up was negative. Ultrasound of the upper extremities revealed calcified arteries with no occlusive large or medium vessel disease; X-rays of the hands and feet showed calcified arches; and CT angiography of the upper extremities demonstrated diffuse multifocal calcified atherosclerotic disease with mild multifocal stenoses of the brachial, radial, and ulnar arteries. Bone scan showed features of calciphylaxis in the distal segments of the involved digits. A skin biopsy showed skin ulceration, superficial necrosis, intravascular fibrin thrombi, and calcifications suggestive of calciphylaxis. Pharmacological therapy included low-dose rivaroxaban, clopidogrel, and supportive care of the digital gangrene.
Conclusions: With the improved survival of patients with ESRD, the incidence of calciphylaxis appears to be on the rise. Early diagnosis and interdisciplinary management aimed at symptom control, wound care, correction of electrolytes, and adequate hemodialysis can reduce morbidity in patients with calciphylaxis. Heightened clinical awareness and recognition of calciphylaxis are essential to improve clinical outcomes.
Poster No. 126
Abstract No. 1777836
Deep vein arterialization in acute limb ischemia
1The Medical City
Background: Deep venous arterialization involves creating a connection between an arterial proximal inflow and a distal deep venous target at the ankle with the intent of arterializing the veins of the foot thereby providing adequate blood flow to resolve rest pain. The typical candidate for DVA is a patient with chronic limb-threatening ischemia who is not a candidate for open or endovascular arterial revascularization because of lack of a distal outflow target for bypass intervention. In this paper, we aim to present a case of an acute limb ischemia successfully revascularized by deep vein arterialization.
Case presentation: We present a case of a 77 year-old female with history of hypertension, diabetes and peripheral arterial disease who presented with one week history of claudication. There was diminished pulse in the right popliteal artery with absent pulses in the right posterior tibial and dorsalis pedis arteries. Doppler signals distal arteries were not appreciated. There were intact venous Doppler signals on both lower extremities. Imaging done with AV duplex scan showed severe stenosis of the distal segment of the right Superficial Femoral Artery progressing to near total occlusion with possible thrombus formation extending to the proximal right Popliteal artery. There was a near totally occluded posterior tibial, peroneal and anterior tibial arteries of the right leg. These findings were consistent with the CT angiogram of the lower extremities. Heparin drip was started immediately upon establishing the diagnosis of Acute Limb Ischemia. Since bypass was not feasible, the team recommended to do a Deep Vein arterialization using the greater saphenous vein as conduit. Intra-op, a subacute thrombus was noted in the distal superficial femoral artery and thrombectomy was done. The team then proceeded with harvesting the great saphenous vein and created a conduit to the dorsal venous arch of the right foot. Procedure was successful, patient discharged on the 5th post operative day with no complications.
Conclusions: Given the successful outcome of this case, Deep Vein Arterialization can be a technically feasible option for patients presenting with an acute limb ischemia and can prevent major amputation in no-option patients presenting with ALI.

Poster No. 127
Abstract No. 1778914
A rare case of aortitis in relapsing polychondritis
1Emory University
Background: Relapsing polychondritis (RP) is a rare autoimmune disorder that affects cartilaginous structures— most commonly the tracheal, nasal, and auricular cartilage. Autoantibodies against collagen target these tissues, resulting in inflammation. Cardiac manifestations of RP include aortic valve (AV) regurgitation, aortic root disease, and rarely aortitis.
Case presentation: A 29-year-old female with RP, on immunosuppressive therapy, was referred to cardiology after her rheumatologist noted a murmur on exam. Echocardiography revealed a normal ejection fraction and severe AV regurgitation. Due to angina, she underwent computed tomography angiography, which showed a 4.1 cm ascending aortic aneurysm with circumferential thickening of the aorta up to 7 mm, extending from the aortic root to the abdominal aorta suggestive of aortitis (Figure). There were no metabolically active foci on position emission tomography (PET) within the aorta. She underwent bioprosthetic AV replacement and graft replacement of the ascending aorta. The patient is now doing well on immunosuppressive therapy.
Conclusions: This case demonstrates a rare presentation of extensive aortitis and aortic aneurysm in a patient with RP. The lack of active foci on PET suggests changes in the aorta and AV were sequelae of RP, not active disease. Aortitis associated with RP has a high mortality rate. Up to 20% of patients may be asymptomatic. Therefore, it may be reasonable for clinicians to screen for cardiac manifestations of RP.
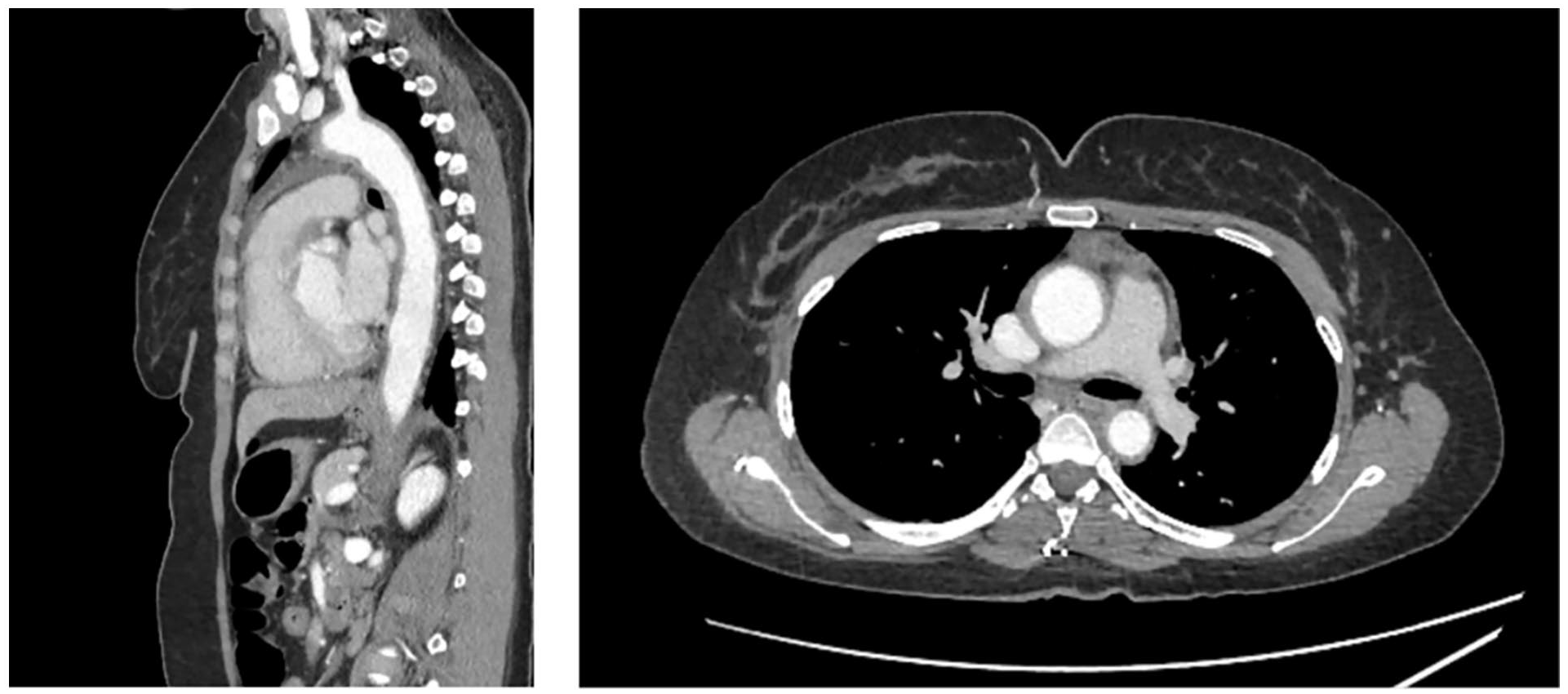
Computed tomography angiography (CTA) images demonstrating circumferential thickening of the thoracic aorta.
Poster No. 128
Abstract No. 1756155
Carotid artery thrombosis, stroke, and rheumatic heart disease
1Philippine General Hospital
Background: Internal carotid artery (ICA) thrombosis and atrial fibrillation are established risk factors for stroke. However, data on incidence, diagnostic and management are lacking when these disease entities are combined.
Case presentation: A 40-year-old male known hypertensive with exertional dyspnea but no angina. He has no vices. 1 day prior to admission, patient had sudden loss of consciousness associated with right sided weakness. Pertinent physical examination revealing no carotid bruit, irregularly irregular rhythm, with grade 2/6 diastolic murmur at the apex and grade 2/6 systolic murmur at the right upper parasternal border, right central facial palsy and hypotonic right extremities. Cranial CT scan showed an acute infarct on the left middle cerebral artery territory with secondary subfalcine and descending transtentorial herniation and cerebral edema, hence patient underwent stat decompressive hemicraniectomy. Patient tolerated the procedure well. On further work up, 2D-echocardiography revealed rheumatic heart disease with moderate aortic regurgitation, moderate aortic stenosis, severe mitral stenosis, dilated left heart chambers, global left ventricle hypokinesia with mildly depressed LVEF (47%), no intracardiac thrombus. Craniocervical angiogram CT scan showing a totally occluded long-segment left internal carotid artery (ICA) thrombosis. Bilateral carotid artery Doppler ultrasound revealed a left internal and common carotid artery thrombus with bilateral increase in the resistive indices. Since this patient has total occlusion of the left ICA, he was only given the best medical therapy. Patient was discharged hemodynamically stable with occasional regard, incomprehensible verbal output, occasionally follows commands and with right sided residual. He was maintained on warfarin, atorvastatin and phenoxymethylpenicillin.
Conclusions: To the best of my knowledge, there are no case reports of stroke in the young from a combined internal carotid artery thrombosis and atrial fibrillation. Management of such case should be individualized, and teamwork of both skilled medical and surgical team is recommended to achieve the best outcome.
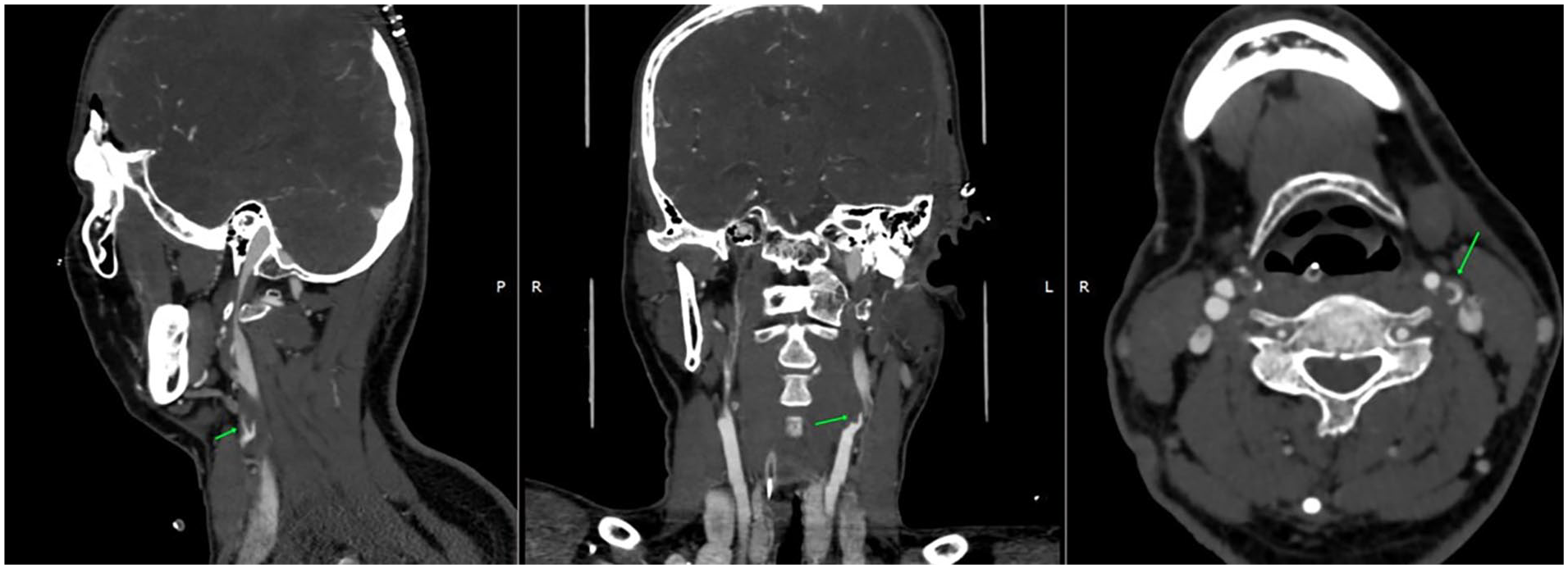
Left internal carotid artery thrombosis.
Poster No. 129
Abstract No. 1781786
Pulmonary artery osteosarcoma masquerading as pulmonary embolism
1Dell Seton Medical School; 2Dell Medical School
Background: Contrasted CT pulmonary angiography (CTPA) is the gold standard for identification and characterization of Pulmonary Embolism (PE). However, atypical pathologies including invasive malignancies can cause obstructive pulmonary artery (PA) masses which mimic both the CTPA and clinical traits of an elevated risk PE.
Case presentation: A critically ill 19-year-old male, with osteosarcoma and PE diagnosed 2 years prior, presented to an outside facility requiring vasopressors and intubation. CTPA demonstrated obstructive mass in the main and bilateral PAs. The patient was treated with 100mg tissue type plasminogen activator followed by mechanical PA thrombectomy (MT) with the Penumbra system with minimal thrombus extraction. Veno-arterial ECMO (VA-ECMO) was initiated prior to transfer to a quaternary care facility. A repeat MT with the larger bore Inari thrombectomy system removed a small amount of mucoid material. Due to persistent hemodynamic compromise, the patient underwent surgical pulmonary thrombo-endarterectomy which produced a mass from the bilateral PA resembling the original mucoid mass. Frozen section analysis revealed invasive high-grade sarcoma. The patient partially improved but remained VA-ECMO dependent. Given the poor prognosis of the patient’s recurrent malignancy, the family pursued palliative care measures and the patient expired.
Conclusions: Though a pulmonary arterial mass in a high-risk patient is often pathognomonic for a PE, alternate etiologies, including invasive malignancy must be considered.
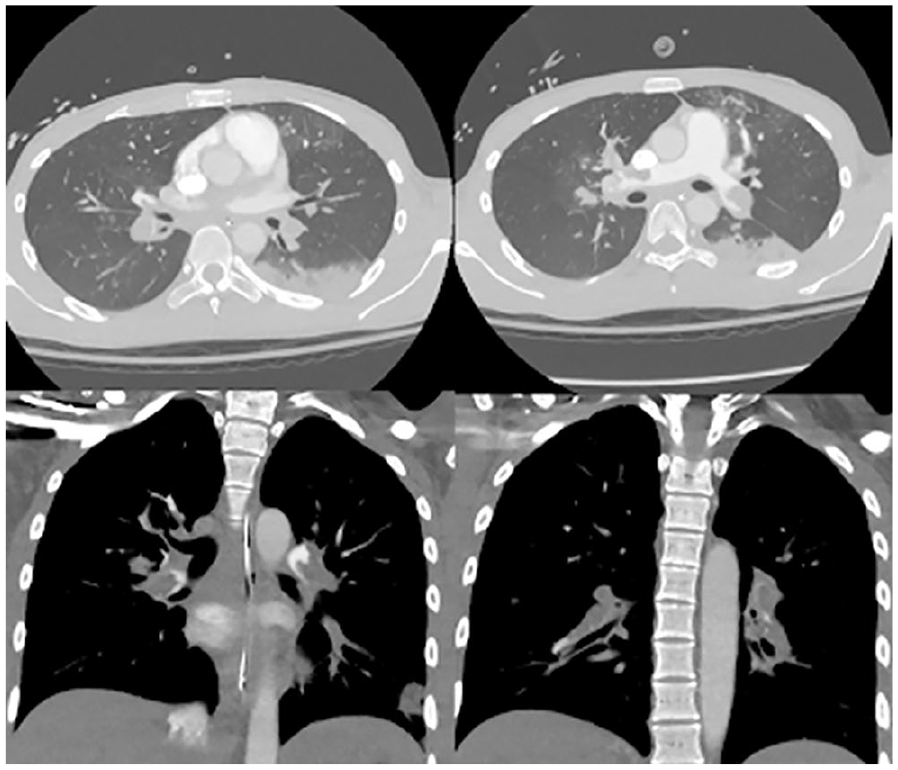
CTPA demonstrates pulmonary arterial mass mimicking PE, en bloc surgical resection of sarcoma from bilateral PA.
Poster No. 130
Abstract No. 1783479
Diagnosis of large vessel vasculitis on duplex ultrasound
1Stanford Health Care; 2Stanford University School of Medicine
Background: Large vessel vasculitis (LVV) is an inflammatory vasculopathy affecting the aorta and its major branches, and unchecked flares can lead to significant morbidity. Diagnosis is based on clinical presentation and imaging. Computed tomography angiography (CTA) and magnetic resonance imaging (MRI) have been the modes of choice; however, target noninvasive duplex ultrasound examinations (US) can also be utilized. We present 2 cases to highlight this use.
Case presentation: Case 1: 77F with polymyalgia rheumatica and non-Hodgkin’s lymphoma. US with a high-frequency transducer of the carotid arteries, the temporal arteries, and its branches showed concentric wall thickening (halo sign) with the absence of vessel compressibility (Figure) and an increased intimal medial thickness (IMT), indicating LVV. Case 2: 30F with Crohn’s Disease, PCOS and pulmonary embolism presented with bilateral weakness and arm claudication. Inflammatory markers were elevated with ESR 116, CRP 6.6. Vessel narrowing with elevated velocities, and the halo sign of the subclavian arteries seen on ultrasound, indicated LVV.
Conclusions: The sonographic findings (halo sign, non-compressibility, and increased IMT) combined with clinical symptoms can support a diagnosis of LVV. The value of utilizing US in LVV care may be in its ability to (1) provide rapid diagnosis based on vessel wall characteristics, (2) obtain flow and velocities to exclude occlusion or vascular malformation, (3) perform repeated imaging to evaluate response to treatment, (4) easy availability at low cost, and (5) minimize radiation exposure.
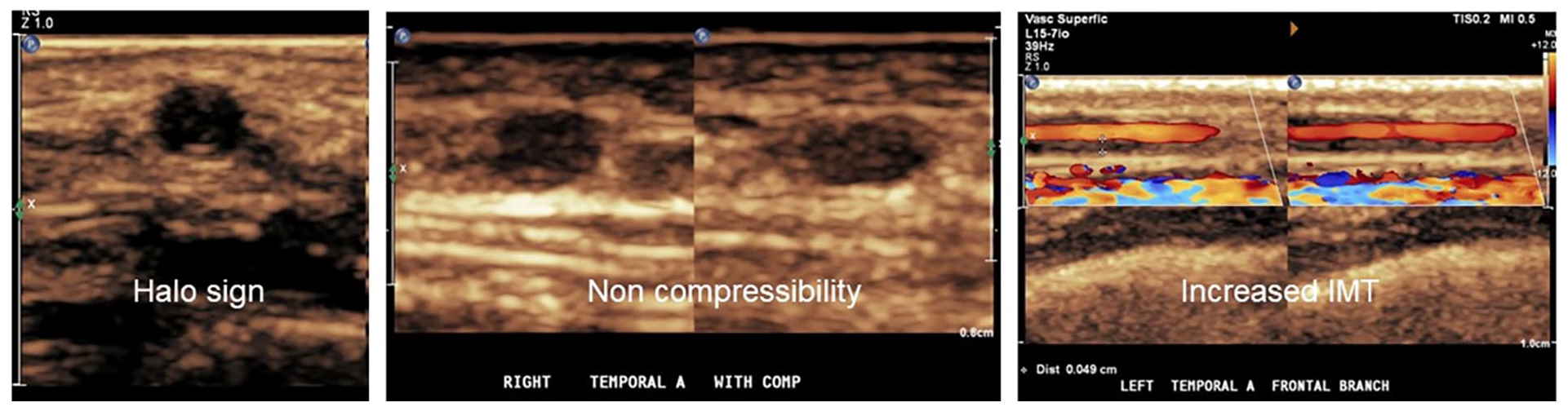
Concentric wall thickening of the artery wall as evident by the Halo sign (A), non-compressibility (B), and increased IMT (C).
Poster No. 131
Abstract No. 1783694
Congenital LIMA-LAD-pulmonary artery vascular malformation in young patient
1University of Michigan
Background: Coronary artery vascular malformations are rare congenital anomalies. We report a case of LIMA-LAD-pulmonary artery arteriovenous malformation in a young patient without previous coronary intervention.
Case presentation: A 22-year-old man presented to primary care clinic with mild chest pain for 6 weeks after a viral infection. He was diagnosed with costochondritis but given symptom duration, was referred for a CT chest- which demonstrated soft tissue thickening and a vascular lesion with concern for LIMA and LAD connection. Follow-up CT coronary showed angiomatous lesion with vessels converging overlying the pericardium of the anterior LV wall with branches fed by left upper lobe segmental pulmonary artery, LIMA, and diagonal branch of LAD. Further history revealed that his chest pain was not exertional. He was subsequently seen in cardiology clinic and follow up echo was requested.
Conclusions: To our knowledge, no previous cases have been reported for congenital LIMA-LAD anastomosis. LIMA to pulmonary artery fistulas are also rare findings after a CABG and are typically discovered due to coronary steal phenomenon. Consideration for right to left shunt from PA to LAD could only exist with elevated PASP and pulmonary hypertension to overcome the diastolic coronary filling pressure. He was not recommended any intervention since symptoms were unrelated. If intervention were necessary, coiling of the small branch PA could be offered. No routine surveillance was recommended for CT or echo unless angina was suspected.
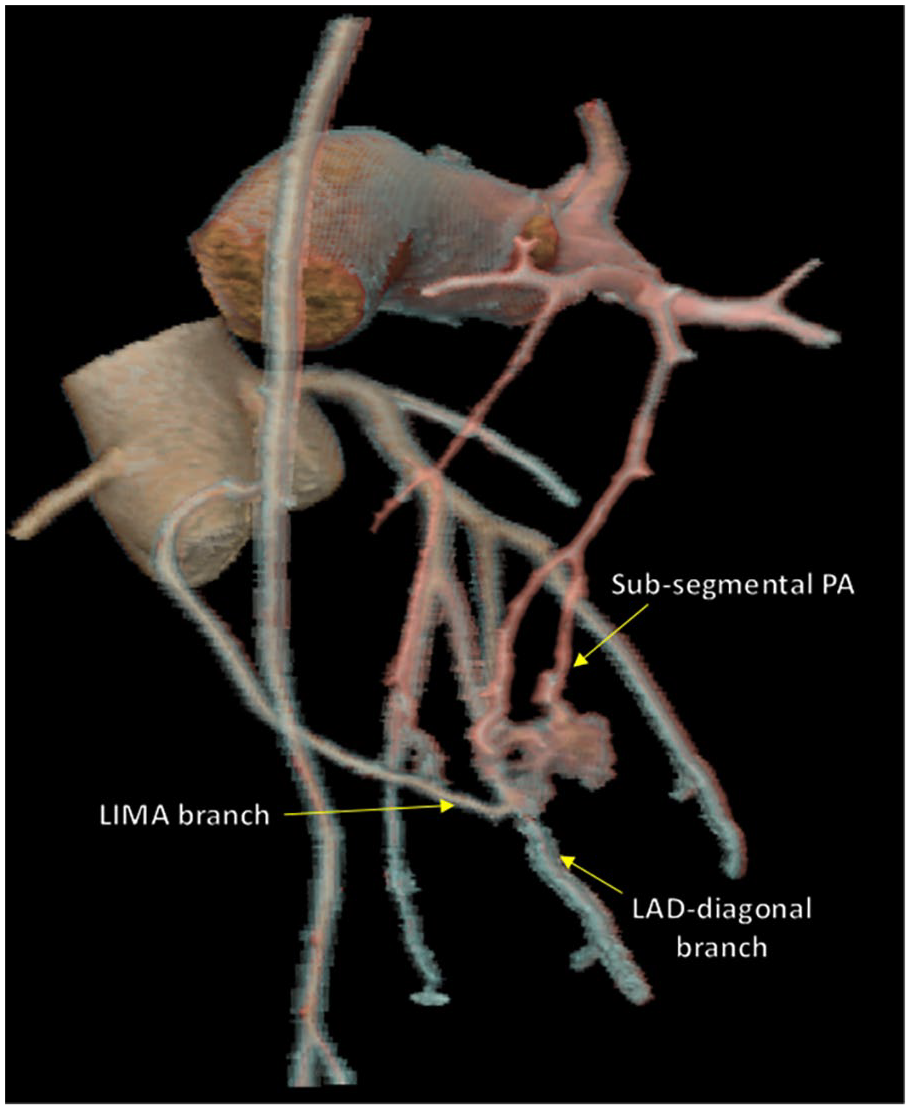
3D reconstruction of a congenital LIMA-LAD-PA complex vascular malformation in a 23-year-old patient.
Poster No. 132
Abstract No. 1783919
Aortic thrombus after multiple sternotomies: a case report
1Texas Tech University Health Sciences Center, El Paso; 2Mayo Clinic
Background: Median sternotomy is the most common incision for cardiac surgeries. Recovery from this procedure can be associated with infectious, osseous, or hardware-related complications and are potentially fatal. Deep sternal wound infections can extend into the aorta leading to the formation of vegetation with systemic embolization.
Case presentation: A 74-year-old male with prior CABG and aortic arch replacement complicated by cardiac arrest, chronic sternal osteomyelitis (OM) and aortic graft infection (completely treated 4 years back with antibiotics, wound VAC, and sternal reconstruction), diabetes, COPD, and prostate cancer presented with complaints of discharge from the base of the scar. Denied other symptoms. Vitals unremarkable. Examination revealed a purulent material draining from the base of the chest scar. CTA thorax showed recurrent osteomyelitis; a 6 cm, mobile, intravascular thrombus in the ascending aorta adherent to sternal OM; and severely diseased CABG grafts. Eventually, the patient developed numbness in the right upper limb and was found to have thromboembolism of the brachial, radial, and ulnar arteries. The patient underwent an embolectomy and was started on anticoagulation. A redo sternotomy with ascending aorta and total arch replacement and CABGx1 was performed. The cultures grew candida albicans and the patient was treated with long-term Fluconazole.
Conclusions: Prompt identification and treatment of complications can prevent extension into deeper tissues and improve clinical outcomes.
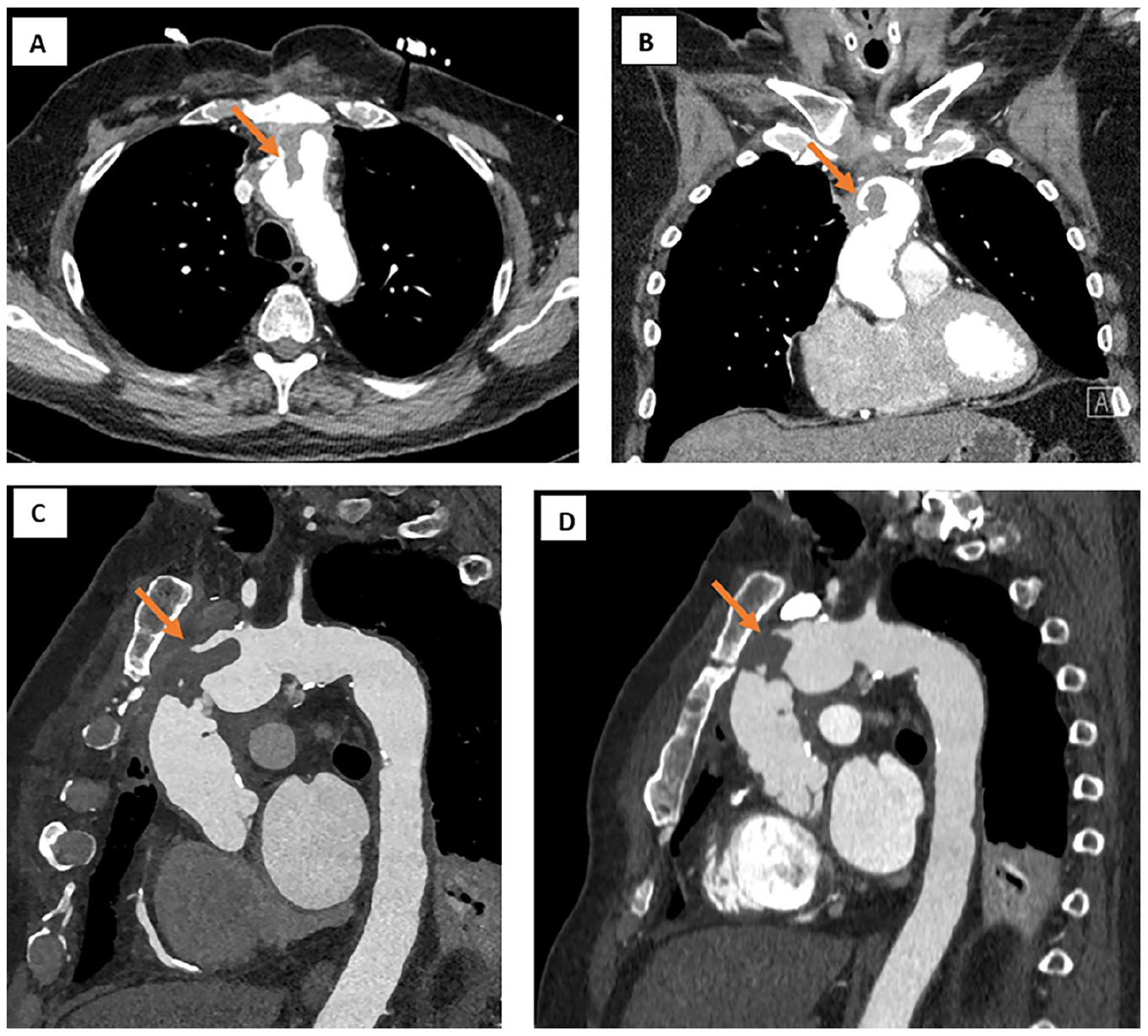
Images A–C show the large mobile intravascular aortic thrombus and osteomyelitis of the sternum. Image D shows a decrease in the size of the thrombus after embolization to the right upper extremity.
Poster No. 133
Abstract No. 1785592
Ruptured aortic abdominal aneurysm presenting with syncope
1St. Luke’s Medical Center, Dr. HB Calleja Heart and Vascular Institute
Background: Ruptured abdominal aortic aneurysm (AAA) is a catastrophic event with mortality rate of 80- 90%. 30-50% of individuals die before reaching the hospital and 30-40% die after reaching a hospital without intervention. Its operative mortality rate is 40% to 50%. Less than 50% of ruptured AAA presents with the triad of back pain, hypotension, and pulsatile mass. Survival of these patients depends on prompt diagnosis which includes the utility of point-of-care ultrasound (POCUS) with immediate intervention.
Case presentation: A 60-year-old, Filipino, male with uncontrolled hypertension, dyslipidemia, and is a 30-pack year smoker developed sudden severe low back pain, diaphoresis, and syncope. He was rushed to the ER and was seen GCS 15, tachycardic with blood pressure of 160/90 on both arms. Abdomen had a palpable, tender, and pulsatile mass. POCUS revealed a large 9cm AAA. He was given esmolol and morphine. He underwent CT aortogram confirming a large ruptured infrarenal AAA measuring 9.3 cm x 16 cm with mural interruption and retroperitoneal hematoma. Open surgical repair was done using an aortobifemoral graft. Postoperatively, the right leg was noted to have pallor and poikilothermia with absent Doppler signals in the infrapopliteal arteries. Repeat aortogram showed filling defect in the right distal external iliac artery. Emergency embolectomy with femoral-femoral artery bypass was done. Completion angiography showed good flow on the bilateral femoral down to the infrapopliteal arteries. During admission, he also developed upper gastrointestinal bleeding from peptic ulcer disease. He was maintained on Cilostazol and Clopidogrel, discharged stable and underwent vascular rehabilitation.
Conclusions: Ruptured AAA is a medical emergency that requires immediate diagnosis and treatment. POCUS can aid in the diagnosis and increase the survival rate. We present a unique case of ruptured AAA in a patient who experienced syncope. Although the patient developed lower extremity ischemia as an early complication of an open AAA repair and gastrointestinal bleeding, he was successfully treated with Cilostazol and Clopidogrel with good patency of stent graft during follow-up.
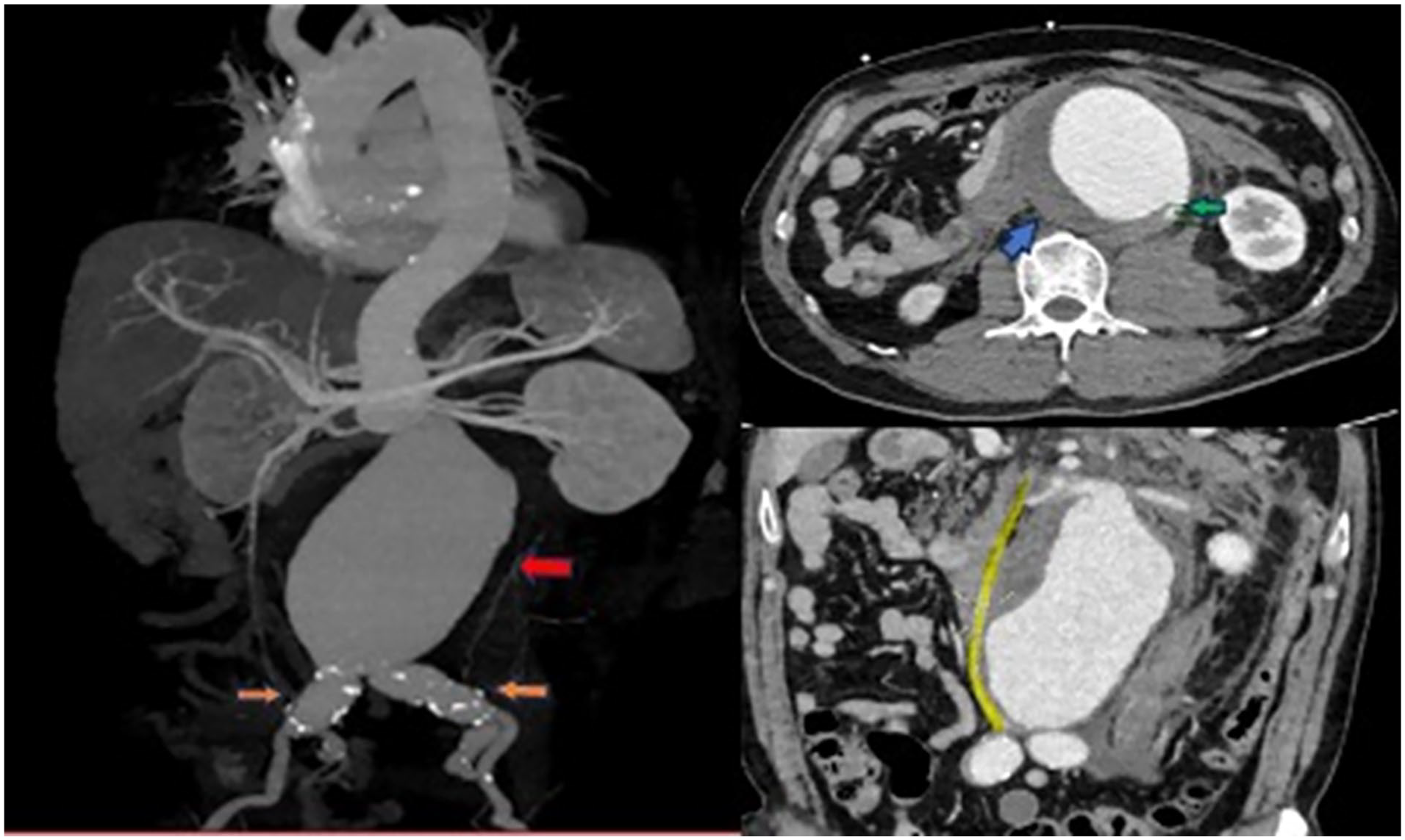
CT aortogram showing large ruptured infra-renal abdominal aortic aneurysm (red arrow) seen measuring 9.3 cm x 16 cm with mural interruption (green arrow) in the left posterolateral aspect and large periaortic hematoma (blue arrow) extending to the retroperitoneal spaces and fusiform dilatation of both common iliac arteries (orange arrow). Associated compression and luminal narrowing of the inferior vena cava (yellow line).
Poster No. 134
Abstract No. 1785735
Secondary antiphospholipid syndrome (APS) in idiopathic CD4 lymphopenia
1National Heart, Lung, and Blood Institute; 2National Institute of Allergy and Infectious Diseases; 3Mayo Clinic
Background: Idiopathic CD4 lymphopenia (ICL) is a rare disease defined by a persistently low CD4+ count (< 300 cells/mm3 on two or more occasions) most often characterized by opportunistic infection, though it may also be asymptomatic. A complex relationship between immunodeficiency and autoimmunity exists with ICL patients marked by a high frequency of autoimmune disease and presence of autoantibodies which may be related to CD4 cell turnover. The superior mesenteric artery (SMA) is vulnerable to thrombosis from atherosclerosis (>85% of cases) or embolic occlusion. Renal artery stenosis (RAS), commonly caused by atherosclerosis or fibromuscular dysplasia (FMD), is suspected in patients with refractory hypertension +/- loss of renal function.
Case presentation: 36-year-old male with ICL and history of disseminated histoplasmosis, epidermodysplasia verruciformis, multidermatomal shingles, admitted for worsening dyspnea and hypertensive urgency. Non-invasive imaging revealed new cardiomyopathy (LVEF 28%), acute SMA thrombosis, and new left renal atrophy (7.6 cm) with chronic ischemic changes and 22% function by scintigraphy in the setting of ipsilateral high-grade ostial RAS (peak systolic velocity 254 cm/sec). Magnetic Resonance Angiography demonstrated mural aortic thrombus through the origin of the SMA without evidence of atherosclerosis, FMD, or dissection. Serology revealed abnormal ANA, dsDNA Ab, and lupus anticoagulant (LA) raising suspicion for antiphospholipid syndrome (APS) with lupus-like phenotype. LA positivity was corroborated by positive antiphosphatidylserine/prothrombin antibodies (anti-PS/PT Ab; >100 U). Anticardiolipin and beta-2 glycoprotein I antibodies were negative.
Conclusions: He underwent successful revascularization via 6 x 21 mm balloon expandable covered stent to the left renal artery with subsequent improvement in labile blood pressures. Aspirin, carvedilol, amlodipine, and serial duplex ultrasound surveillance were initiated. A diagnosis of secondary APS was made based on comorbid autoimmune disease, positive LA and anti-PS/PT Ab, and arterial thrombosis. Life-long anticoagulation with vitamin-K antagonist was initiated.
Poster No. 135
Abstract No. 1786437
VA-ECMO-assisted aspiration thrombectomy of a massive pulmonary embolism
1Loyola University Medical Center
Background: Postoperative massive pulmonary embolism (PE) poses a significant challenge as recent surgery is often an absolute contraindication to systemic tissue plasminogen activator (tPA) due to bleeding risks. In this report, we describe a complex clinical scenario where a postoperative neurosurgical patient suffered from cardiopulmonary arrest secondary to obstructive shock from massive PE, requiring hemodynamic support with VA-ECMO followed by aspiration thrombectomy.
Case presentation: A 63-year-old male with a history of meningioma, status post resection 1 month prior to presentation, was transferred to our medical center with suspected meningitis. The patient underwent endoscopic endonasal repair of the cerebrospinal fluid leak and lumbar drain placement. On postoperative day 5, the patient became acutely unresponsive secondary to a PEA cardiac arrest. Return of spontaneous circulation was obtained, however, the patient remained in severe cardiogenic shock. CT scan identified a large burden of acute bilateral, proximal emboli in the right and left main pulmonary arteries with a marked increase in the right ventricle to left ventricle ratio to 2.7. Due to recent surgery, the patient had an absolute contraindication to systemic tPA and catheter-directed thrombolysis. After Pulmonary Embolism Response Team activation, it was decided to pursue aspiration thrombectomy with VA-ECMO. The patient had emergent initiation of peripheral VA-ECMO. With the guidance of pulmonary angiography, aspiration thrombectomy was performed via the Inari FlowTriever Suction Device (Inari Medical) with significant thrombus removal and immediate improvement in hemodynamics. Given the improvement of invasive hemodynamics and right ventricular systolic function, the patient was decannulated from the ECMO circuit approximately 14 h from initial cardiac arrest.
Conclusions: In patients with contraindications to systemic tPA, endovascular interventions are now increasingly favored over traditional surgical thrombectomy due to decreased rates of morbidity and mortality. Furthermore, VA-ECMO has been described in previous reports as a bridge to therapy in hemodynamically unstable patients with massive PE.
Poster No. 136
Abstract No. 1786516
Catheter induced venous spasm during treatment of DVT
1HCA Northside Hospital; 2HCA Florida Northside Hospital; 3University of Alabama Birmingham
Background: Debulking procedures using mechanical thrombectomy for the management of deep vein thrombosis (DVT) has been well established. A rare event that can occur and should be recognized includes venous spasm (vs). Vs has been previously described in few case reports and was described during the implantation of intracardiac devices. Herein, we describe our experience of vs that occurred during the treatment of femoral dvt using a wide bore thrombectomy catheter system.
Case presentation: A 48-year-old male with a past medical history of remote provoked upper extremity DVT and hypertension who developed left lower extremity DVT one week after left ankle surgery. He was diagnosed after presenting with pain and edema. A venous ultrasound was performed demonstrating a nonocclusive thrombus in the left posterior tibial vein. He was on rivaroxaban and a follow up 3 months later showed persistent left lower extremity DVT. Hence, he was referred for evaluation of invasive options. He was still complaining of pain and swelling in his left leg; otherwise, he had no additional complaints.
Conclusions: The use of a wide bore thrombectomy catheter can lead to venous spasm, a transient rare phenomenon that needs to be recognized to avoid unnecessary intervention.
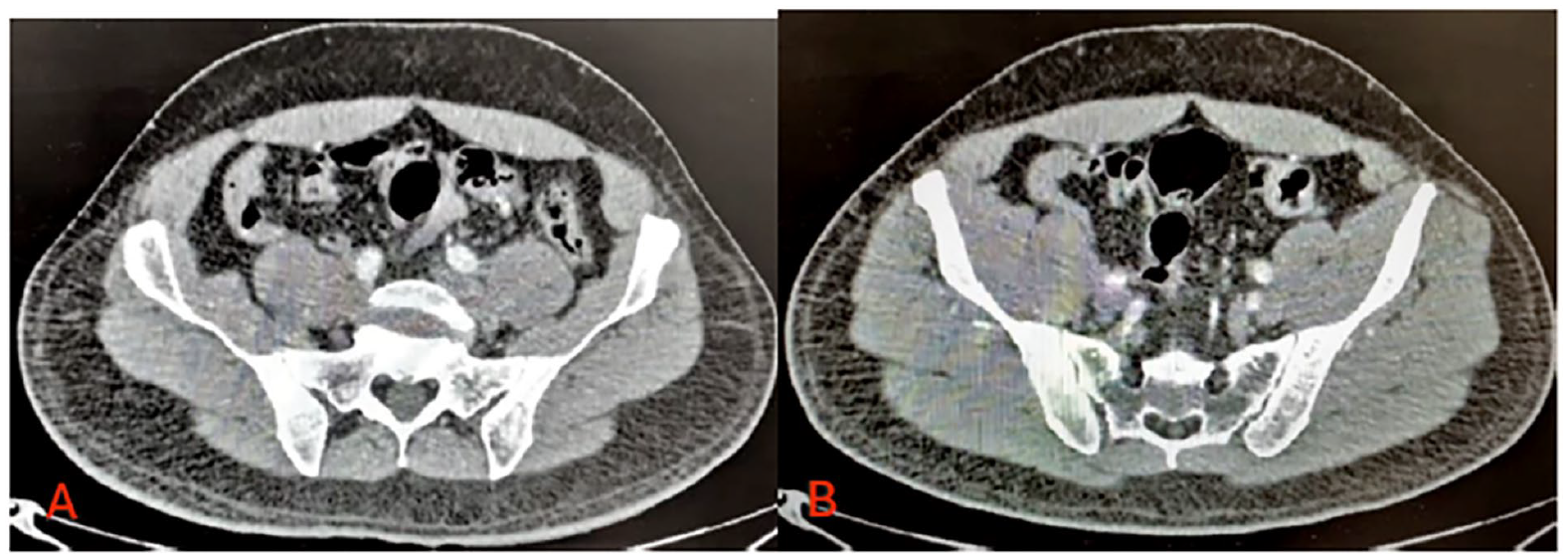
Demonstrating patent left common, left external iliac vein and absence of left external iliac vein compression by the right external iliac artery.
Poster No. 137
Abstract No. 1786535
Acute aortic dissection secondary to salmonella bacteremia
1Makati Medical Center
Background: Aortic dissection secondary to aortic infection is an infrequent occurrence. Infections affecting the endothelium, particularly those caused by non-typhoidal species, are more prevalent in the aorta than in peripheral arteries, often affecting the abdominal aorta rather than the thoracic region. Here, we describe an uncommon case of aortic infection leading to aortic dissection that encompasses both the thoracic and abdominal segments.
Case presentation: This case involves a 44-year-old male, hypertensive for the past decade with consistent adherence to losartan. He remained in apparent good health until a few days before admission when he experienced abdominal pain without fever or diarrhea. No medications taken or consult done until few hours prior to admission, he suddenly experienced intense, squeezing back pain rated at 8/10, radiating to the chest area. Admitted to the Emergency Department, the patient exhibited an isolated fever of 38°C. The physical examination, chest x-ray, CBC, troponin I, and 12-lead ECG yielded unremarkable results. However, chest and abdominal CT scans revealed an extensive dissection starting from the aortic root and extending just before the origins of the renal arteries, reaching the celiac and superior mesenteric arteries. The patient underwent urgent repair for acute thoracoabdominal dissection, involving aortic dissection repair and ascending arch aneurysmorrhaphy. The surgery, performed under hypothermic arrest, revealed a well-functioning left ventricle and an intimal tear at the ascending aorta. In the ICU, the patient experienced febrile episodes, and blood culture confirmed Salmonella enteritides. Aortic wall histopathology displayed inflammatory infiltrates and additional work up with abdominal CT scan revealed findings of fat stranding representing acute inflammation. Patient was then treated with 2 weeks of intravenous ceftriaxone, followed by oral ciprofloxacin. The patient was discharged in good health, free from fever episodes.
Conclusions: Timely diagnosis and intervention are crucial for aortic dissection to prevent mortality. Considering a broad range of differentials is essential for effective management.
Poster No. 138
Abstract No. 1786584
Urticarial vasculitis presenting as edema, neuropathy and hypereosinophilia
1Makati Medical Center
Background: Urticarial vasculitis usually presents as prolonged urticarial lesions and is linked with diverse triggers like infections and autoimmune disorders, but most are idiopathic. Systemic involvement can occur such as hematuria, pleuritis, and diarrhea, more frequently in hypocomplementic patients. Other rare presentations include pericardial effusion, pericarditis, and neuropathy. Lesional biopsy shows leukocytoclastic vasculitis.
Case presentation: A 30-year-old female with Chronic Autoimmune Urticaria, comes in with bilateral leg edema associated with heaviness and paresthesia for 1 week. Symptoms progressed now with joint pains, skin tightness and difficulty ambulation. Initial work-up showed normal Lupus panel, ANA, RF, C3, C4, and ESR but D-dimer, CRP and WBC were elevated with eosinophilia (33%; AEC 5148 c/uL). She then had multiple hyperpigmented patches on both ankles and feet. Anti-TPO, Anti-TG, Crea and urinalysis were normal. Hydrocortisone and diphenhydramine IV were given. Venous duplex showed chronic venous insufficiency. Skin punch biopsy noted immune-complex vasculitis with C3 and Fibrinogen deposits. IgE, cryglobulin, allergen panel, hepatitis profile, C- and P-anca were negative. CXR noted minimal pleural effusion. 2D Echo was normal except for trace pericardial effusion. After 3 days, CBC was normal but still with leg edema and neuropathy. Manual lymphatic drainage was done which markedly lessened the edema, decreased skin tightness, and improved paresthesia. Ambulation also improved. She was sent home with tapering doses of oral steroid, bilastine, diosmin/hesperidin, and pregabalin. She continued manual lymphatic drainage as out-patient. On follow-up, there was edema but with minimal neuropathy and persistent eosinophilia, hence Azathioprine was started.
Conclusions: We present an unusual presentation of urticarial vasculitis with the patient developing edema and neuropathy due to compressive symptoms before manifesting skin lesions. It is a complex condition with variable outcomes, often benign in those with normal complement levels. Treatment can be as equally challenging as diagnosis. Close monitoring is important as well as re-evaluation when new symptoms arise or treatment fails.
Poster No. 139
Abstract No. 1787272
Direct sac puncture embolization of type II endoleak
1University of Virginia; 2MedStar Health
Background: Type II endoleak (EL) is the most common type of EL after endovascular abdominal aortic aneurysm repair (EVAR) and increases the risk of aneurysm sac rupture. Management options include transarterial or direct sac puncture embolization.
Case presentation: An 88-year-old woman presented to the clinic for evaluation of abdominal discomfort and back pain (worse with standing). Her medical history was significant for renal artery stenosis (status post left renal stent) and an abdominal aortic aneurysm (status post EVAR 3 years prior to presentation). Postoperative follow-up CT scans had revealed an enlarging aneurysm sac with a type II EL. Her most recent abdominopelvic CTA revealed a patent aortic endograft and left renal artery stent, with a continued EL and increased aneurysm sac size of 5.7 cm (Figure 1 A and B). She was referred to interventional radiology and was planned for direct aortic aneurysm sac puncture, aneurysm angiography and embolization. The aneurysm sac was directly accessed using fluoroscopic guidance (Figure 1 C). Initial cone beam imaging demonstrated absence of embolic in the posterior aspect of the aneurysm sac. Embolization agents included Onyx and Nester coils. After embolization, the posterior area of leak contained embolic. Follow-up 1-month interval abdominopelvic CTA revealed stable aneurysm size with no residual EL (Figure 1 D and E).
Conclusions: Direct sac puncture embolization of type II EL following EVAR can be a safe and effective option for achieving aneurysm sac stability and resolution of the leak.
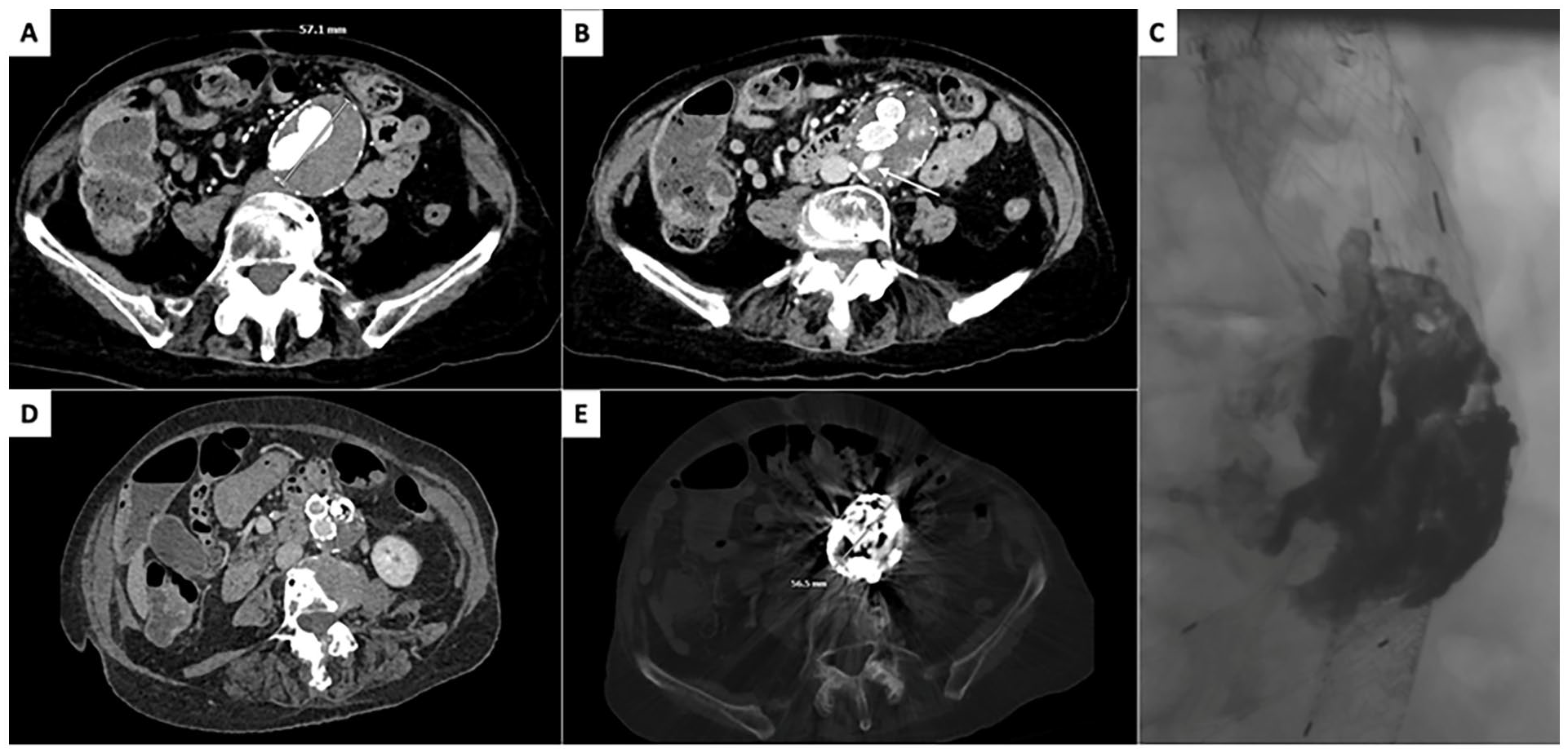
(A) Pre-embolization abdominopelvic CT angiography revealing a bilobed infrarenal abdominal aortic aneurysm (AAA) measuring 5.7 cm, and a patent endograft. (B) Pre-embolization abdominopelvic CT angiography delayed images demonstrating extensive type II endoleak (white arrow) involving the 4th lumbar arteries, with a second component in the left anterior aneurysm sac at approximately the origin of the iliac limbs. (C) Fluoroscopic images demonstrating extensive posterior endoleak. (D,E) Post-embolization abdominopelvic CT angiography demonstrating stable size of AAA and no evidence of residual endoleak, although evaluation was limited by significant streak and beam hardening artifact from the embolization material.
Poster No. 140
Abstract No. 1787348
Non-dominant thoracic outlet syndrome: before your very eyes
1Mayo Clinic
Background: We present a case of non-dominant thoracic outlet syndrome.
Case presentation: A 38-year-old left-hand dominant female presented to the ER with acute right upper extremity deep venous thrombosis (DVT), preceded by bluish discoloration and swelling of extremity. Venous ultrasound showed acute DVT of left axillosubclavian vein. She was dismissed on apixaban. She denied repetitive/strenuous activity of right arm. History revealed right arm abduction above head while asleep. Family history was negative. Pertinent exam findings: loss of radial pulse and bruit in sub-clavicular region with costoclavicular maneuvers. Adson's maneuver was negative. Prominent superficial veins (neck and upper chest) i.e. Urschel's sign. Thrombophilia survey was negative for heritable and acquired thrombophilia markers. Post-thrombotic changes in subclavian vein and axillary artery occlusion on ultrasound in Adson's position. Subclavian vein occlusion with hyperabduction on venogram.
Conclusions: The patient presented with non-dominant axillosubclavian vein thrombosis with an acute Paget-Schroetter pattern of thoracic outlet syndrome (TOS). High index of suspicion should be maintained in the most unlikely situation. Clues to diagnosis are careful history, clinical exam (Urschel's sign and thoracic outlet maneuvers), and imaging. Management includes anticoagulation, thoracic outlet decompression (1st rib resection and venoplasty), activity modification with PM&R consultation.
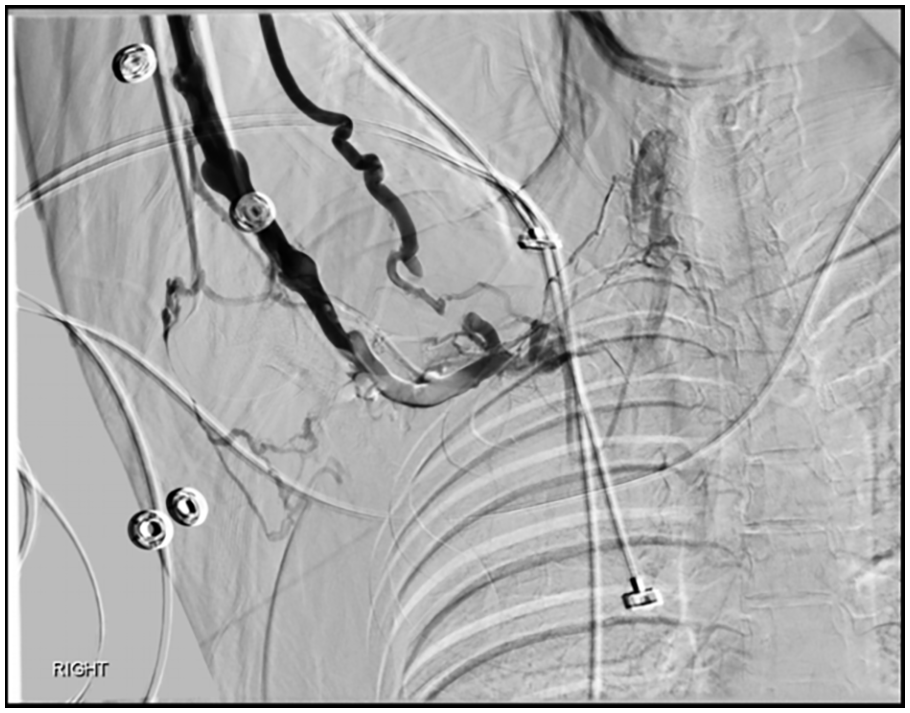
Upper extremity venogram demonstrates right-sided TOS with collateralization of flow around subclavian, jugular, and thyrocervical veins and subclavian vein occlusion with hyperabduction.
Poster No. 141
Abstract No. 1787664
Young man with vascular neck pain
1Instituto Cardiovascular de Buenos Aires; 2Hospital Rivadaia
Background: Usually, doctors think of coronary or muscular pain like diagnosis when they assess neck pain, however we must think about vascular (carotid) differential diagnoses especially in young people.
Case presentation: A 44-year-old male presented left neck pain for 1 month irradiating into the ipsilateral mandibular and tinnitus. The neck pain was intense, continuous, and localized over the left carotid bifurcation. It increased with neck movements and palpation. Physical and neurological examination was normal. No trauma, infection, or chiropractic neck manipulation was reported. Laboratory tests was normal. Doppler US, the thickened arterial wall was isoechoic to muscle (Figure) The MRI showed eccentric soft tissue thickening of the left carotid bifurcation with hypointense signal on the T1-weighted sequence and hyperintense signal on the T2-weighted sequence. After IV administration of contrast, intense enhancement of the carotid bifurcation was present suggesting an inflammatory etiology. presence of structure lymph node measuring 10.7 mm on that left side. After negative immunological laboratory tests, the diagnosis of carotidynia was established and the patient was treated with NSAIDs, due to persistence of the pain a corticotherapy was prescribes with mild improvement. Given the rare diseases, and the partial response to the medical treatment a PET CT was carried out, which showed a diffuse thickening of the left carotid wall with a maximum standardized uptake value (SUVmax) of 6,1. After that we increase the dose of meprednisona and started colchicine. This Treatment with colchicine resulted in disappearance of neck pain and tinnitus in a few weeks. Follow-up Doppler US obtained 4 months later revealed disappearance of the abnormal soft tissue lesion surrounding the carotid bifurcation. The patient continued to be asymptomatic.
Conclusions: We presented an inflammatory vascular and perivascular, despite the carotidynia is a rare entity, we should the exercise to think in vascular (carotid) compromise (first carotid dissection) in young patient with neck pain. The images have a main role in carotidynia diagnosis joint with the clinical suspicion The colchicine could be an attractive treatment in carotidynia.
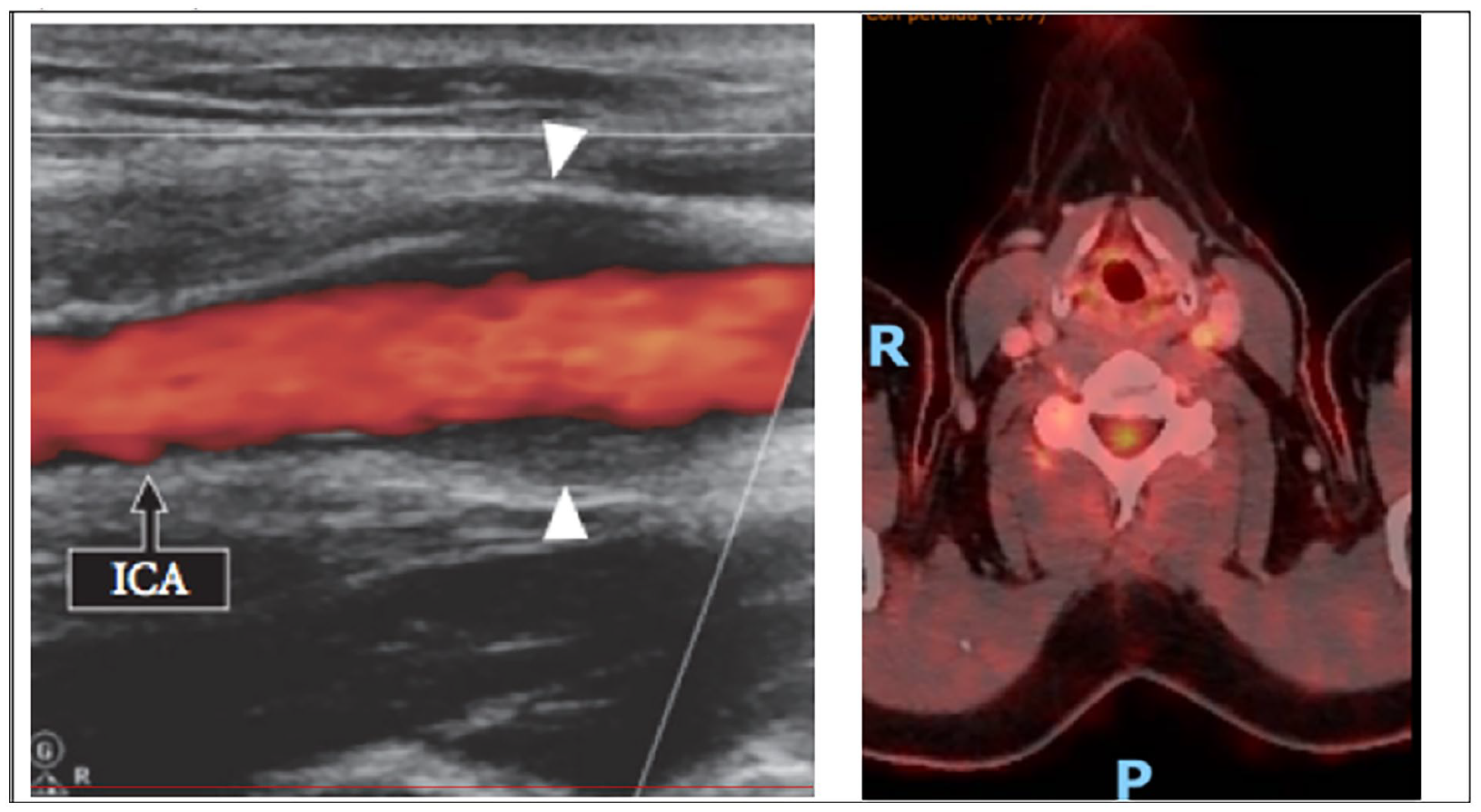
Left: Ultrasound shows the thickened arterial wall was isoechoic to muscle. Right: shows a diffuse thickening of the left carotid wall with a maximum standardized uptake value (SUVmax) of 6.1.
Poster No. 142
Abstract No. 1787667
Rare adrenal leiomyosarcoma with extensive deep venous thrombosis
1St. Luke’s Medical Center, Dr. HB Calleja Heart and Vascular Institute; 2St. Luke's Medical Center
Background: Primary adrenal leiomyosarcoma (PAL) with inferior vena cava invasion is exceptionally rare with only around 50 cases reported. Typically, the diagnosis is based on imaging and histopathology and is often made late in the disease course. The prognosis is poor, with the longest reported survival being two years.
Case presentation: A 55-year-old man came in with bilateral leg swelling for 5 days. He had no significant familial, medical, or surgical history. Physical examination was normal except for grade 2 bipedal edema. Routine tests did not reveal relevant findings except for the venous compression ultrasound which showed acute extensive bilateral deep venous thrombosis. Enoxaparin was started. CT scan revealed an irregular soft tissue density mass in the right renal/suprarenal region which measures 4.4 x 3.1 x 4.1 cm. A PET scan showed an irregular hypermetabolic lesion in the same area. Filling defects were seen in the inferior vena cava, bilateral iliac, renal, and femoral veins. A CT-guided biopsy confirmed the presence of a smooth muscle neoplasm. The immunohistochemical stain yielded positive for SMA, Caldesmon, and Desmin. This patient was started on Doxorubicin and Dacarbazine and was counseled on the guarded prognosis and limited effective later-line therapies.
Conclusions: PAL with inferior vena cava invasion is a rare condition that often goes undiagnosed until late in the course due to lack of symptoms. A multidisciplinary approach is essential. Early recognition and optimal treatment strategies are yet to be determined.
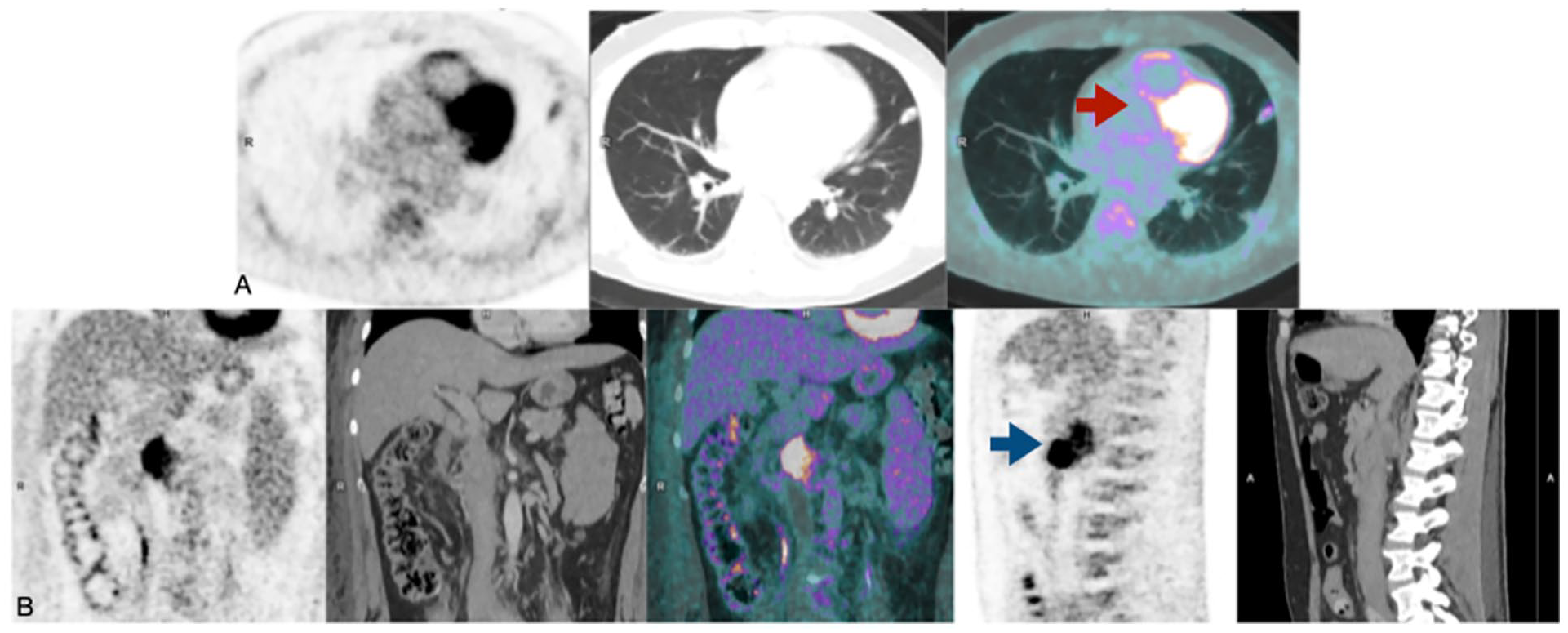
A. PET scan showing multiple varied-sized non-calcified parenchymal and sub-pleural nodules (red arrow) B. PET scan showing irregular hyper-metabolic mass lesion in the area of the inferior vena cava at the right renal/suprarenal level (blue arrow).
Poster No. 143
Abstract No. 1787678
Descending aortic dissection during elective ascending aneurysm repair
1St. Luke’s Medical Center, Dr. HB Calleja Heart and Vascular Institute; 2St. Luke's Medical Center
Background: Intraoperative aortic dissection (IAD) is a rare but potentially fatal complication that can occur during an aortic intervention. It has a reported frequency of 0.06% to 0.35%. Immediate recognition and repair are crucial to prevent high operative mortality rates ranging from 14.8% to 43%.
Case presentation: A 71-year-old hypertensive male presented with intermittent 1/10 retrosternal pain over the past year. The physical examination was unremarkable. 2D echo revealed an aneurysmally dilated aortic root. Further imaging with CT angiogram showed a fusiform ascending aortic aneurysm (5 x 7 cm) with no dissection. He was admitted for an elective aneurysm repair. Mid-procedure transesophageal echocardiography (TEE) showed dissection at the descending aorta extending to the aortic arch and common carotid arteries. Replacement of the aortic hemiarch and total arch debranching was done. A repeat scan post-op showed an extension of dissection at the ostium to the proximal segment of the left renal artery. Dissection was also seen from the graft site of the distal brachiocephalic artery extending to the proximal right common carotid, subclavian and axillary arteries. The patient remained stable with no neurologic deficits. No repeat intervention was done. He was discharged improved after 5 weeks.
Conclusions: IAD is a rare but serious complication during aortic surgery. Concrete risk factors for IAD occurrence have not been established. The utility of intraoperative TEE and expertise for immediate surgical repair is indispensable.
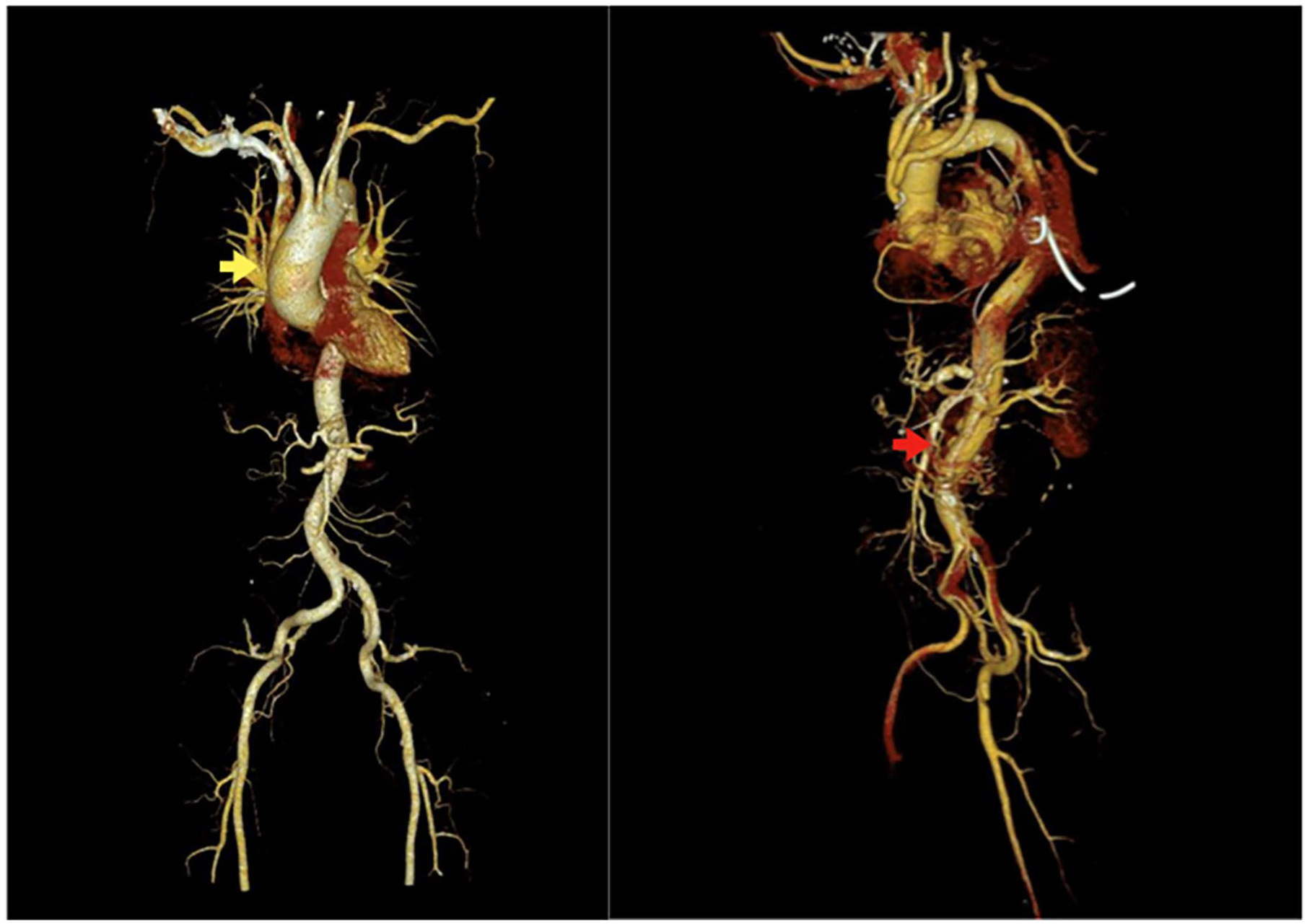
CT aortogram images of pre-operative ascending aortic aneurysm (yellow arrow) and post-operative descending aortic dissection (red arrow).
Poster No. 144
Abstract No. 1787686
Breaking boundaries: navigating thromboembolic risk in a transgender woman
1Odessa National Medical University; 2Kannur Medical College; 3Massachusetts General Hospital
Background: Individuals with gender dysphoria often encounter discrimination and experience higher rates of depression compared to cisgender peers. Challenges in accessing affirmative healthcare for gender identity alignment and providers who understand their needs are common. Estrogen offers favorable physical changes but raises risks of venous thromboembolism (VTE). This case explores role of personalized care in navigating challenges in transgender health including vascular complications and hormonal therapy.
Case presentation: A 41-year-old patient presented with right calf/ankle pain post-ankle twist with limited mobility. She has gender dysphoria since a teenager and underwent male-to-female gender-affirming surgery a decade ago, followed by 3-months oral estrogen. Estrogen therapy was halted for years due to relocation/inaccessible care. She resumed oral estradiol recently and shifted to IM estradiol valerate 2 months ago. Denies new medications, travel, surgeries, smoking, clotting disorders, cancer, or family history of VTE. Vitals stable, BMI- 25. Exam showed 1+ pitting edema at the right ankle, trace edema below knee, and right calf tenderness. Labs WNL except D-dimer at 2800. RLE venous duplex showed posterior tibial and peroneal vein thrombus (Figure). Therapeutic anticoagulation was initiated. Given VTE, oral/IM estrogen was switched to transdermal patch, as patient preferred ongoing estrogen therapy. After 3 months of therapeutic anticoagulation, questions about long-term anticoagulation arose. Considering initial low-risk VTE event and provoking factors like immobility, decision made to repeat D-dimer and hold long-term anticoagulation, if negative. She declined low-dose aspirin prophylaxis and was closely monitored off anticoagulation. No further VTE episodes reported.
Conclusions: Transgender healthcare requires joint decision-making, emotional considerations, and patient preference. VTE is common in initial months of treatment, especially with formulations like ethinylestradiol, conjugated equine-estrogen and high dosages. Transdermal estrogen is advised for women aged 40 and above. Currently, no widely accepted guidelines exist to manage/treat or monitor these patients.
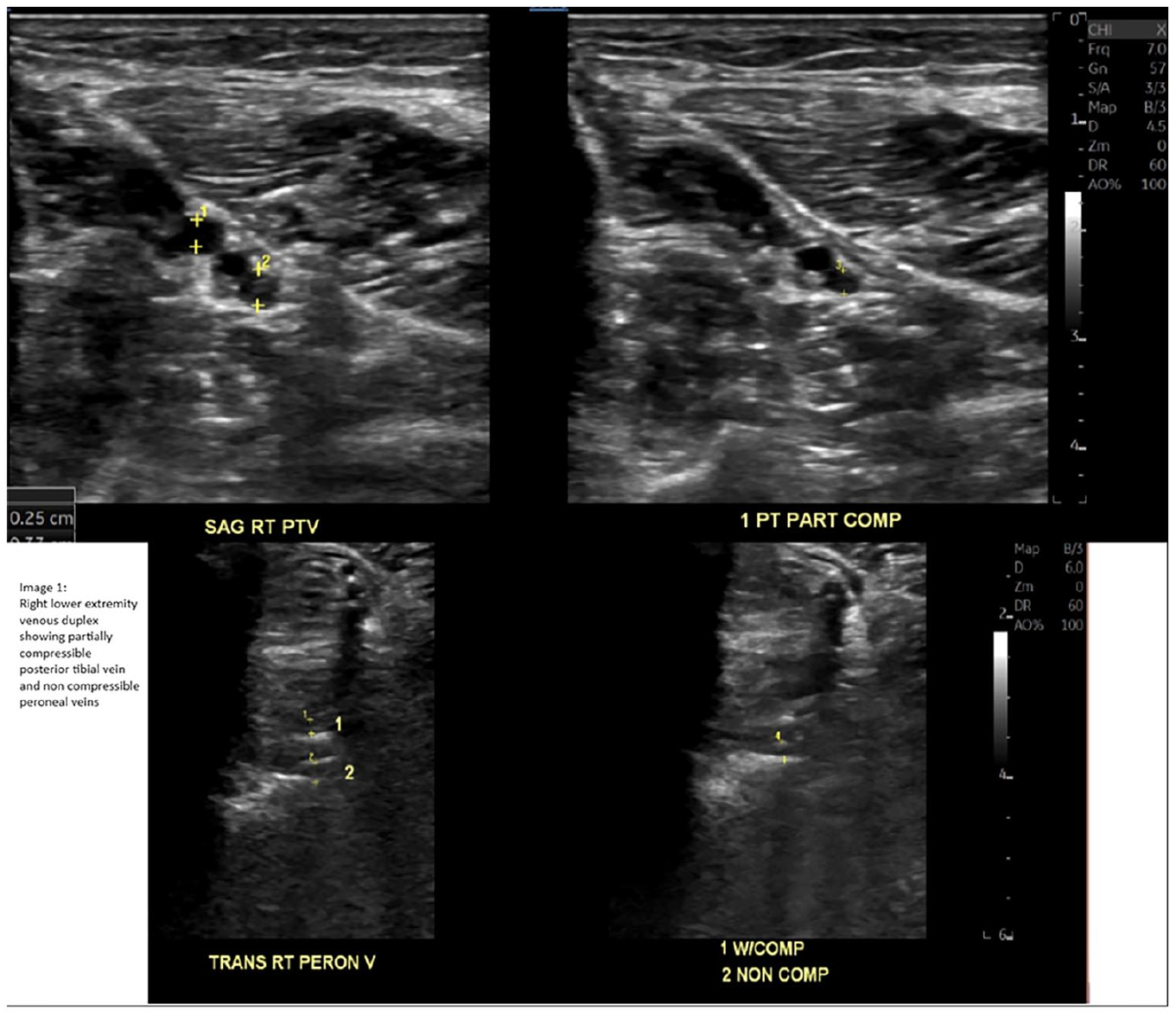
Venous duplex scan of right lower extremity.
Poster No. 145
Abstract No. 1787780
A giant miss! Challenges in diagnosing aortitis
1University of Kansas Medical Center; 2UCLA Medical Center
Background: Giant cell arteritis (GCA) is a vasculitis that affects large to medium-sized vessels. Aortitis involvement in the form of aneurysm, stenosis, dissection, or rupture can present in 40-65% of GCA cases. Surgical outcomes improve significantly when the active inflammation is better controlled, hence, the importance of delaying surgical intervention if clinically possible. In current practice, disease activity is ascertained based on laboratory markers of inflammation and cross-sectional imaging such as FDG-PET or MRA. The following case illustrates the limitations of currently available methods in detecting disease activity.
Case presentation: A 72-year-old Caucasian female was referred to cardiac surgery clinic for an ascending aortic aneurysm (5.3 cm). She was diagnosed with GCA 7 years ago when she presented with temporal headaches, scalp tenderness, jaw claudication, and elevated erythrocyte sedimentation rate (ESR) and c-reactive protein (CRP) without biopsy confirmation. Three years ago, CTA revealed a minimally calcified 4.3 cm ascending aorta without dissection, mild right subclavian ectasia, and mild irregularity of arch vessels consistent with GCA. She was unable to taper off the prednisone monotherapy due to scalp tenderness. When evaluated in our center, the inflammatory markers were normal. Insurance declined a vasculitis protocol MRA. An FDG-PET CT showed no signs of active arteritis. She agreed to increase her prednisone dose from 5 mg to 30 mg daily for 3 weeks before her successful aneurysm resection with valve-sparing aortic grafting. The surgeon reported the aorta as leathery and irregular with a focal intimal medial disruption not detected on CT. Pathology showed active aortitis with vessel wall infiltration of CD3-positive lymphocytes, CD-68 histiocytes, scattered CD-20 lymphocytes, and medial degeneration. Chest CTA was stable 1 month post-surgery. Tocilizumab was initiated while prednisone was gradually tapered down. She remained asymptomatic.
Conclusions: This case highlights the limitations of currently available tests for detecting GCA disease activity and the importance of high clinical suspicion for occult or smoldering active disease when managing these patients perioperatively.
Poster No. 146
Abstract No. 1787801
Case of cancer-related venous thrombosis and obstructive uropathy
1St Luke's Medical City, Bonifacio Global City
Background: Cancer-related venous thrombosis can be a clinical dilemma. The nature of solid tumors and its treatment are factors that may complicate its management. Acute kidney injury secondary to obstruction by tumors can increase the complexity treatment.
Case presentation: A 52-year-old female known case of spindle cell sarcoma of the abdomen presents with bilateral leg swelling. She has a history of deep venous thrombosis of her left leg 5 months prior to current consult, for which she received Enoxaparin 60mg twice daily. On duplex scan, there was venous thrombosis in the left proximal external iliac, bilateral distal external iliac, and femoral veins despite being on anticoagulation. Her creatinine level was 6.18 mg/dL and her serum potassium 5.6mEq/L. CT scan showed a pelvoabdominal mass measuring 12.2 x 13.1x 20 cm which compresses the urinary bladder and ureters. The mass abuts the bilateral psoas muscle compressing the sigmoid colon. The mass extends to the left ischio-anal fossa and inguinal region. Anticoagulation was shifted to Heparin 5000 units twice daily. A retrievable inferior vena cava filter was inserted. Hemodialysis was initiated. Her creatinine and serum potassium decreased. She was discharged on Apixaban 2.5mg twice daily. Her symptoms improved and she regularly follows up with her physicians.
Conclusions: Knowing appropriate anticoagulation in patients with multiple co-morbidities is needed to achieve a balance of treatment of cancer-related venous thrombosis and maintaining safety of patients.
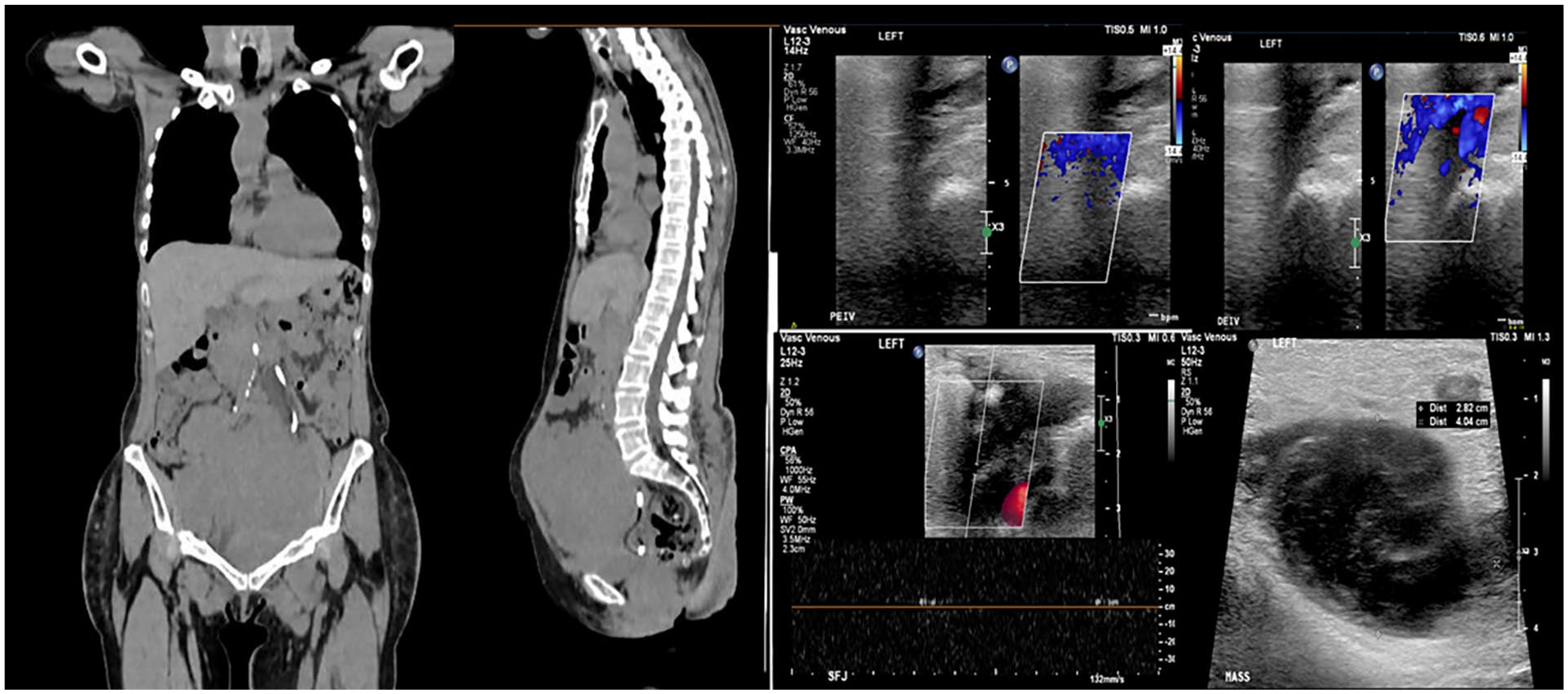
Abdominopelvic CT scan showing pelvoadominal mass; Vascular imaging showing venous thrombosis of the left proximal venous segments and pelvoabdominal mass.
Poster No. 147
Abstract No. 1787889
Puzzling leg discomfort relieved by sclerotherapy
1Makati Medical Center
Background: Patients might report ongoing leg discomfort despite addressing peripheral arterial disease through endarterectomy with patch angioplasty. It is crucial to accurately identify leg pain symptoms, as chronic venous insufficiency could be the underlying cause, and improvement may be observed following sclerotherapy of the affected leg vein.
Case presentation: This is a case of a 71-year-old male, known to be hypertensive, with peripheral arterial occlusive disease. He initially presented with claudication symptoms a year ago and underwent a successful left common femoral and profunda endarterectomy, with patch angioplasty. He now reports recurrent leg discomfort, more pronounced on the left, characterized by crampy pain and weakness. The initial impression was chronic venous insufficiency. A venous duplex study revealed no deep vein thrombosis but indicated superficial vein valve incompetence in the great saphenous vein. The patient also underwent a 6-minute walk test without reporting claudication. Post 6-minute walk test, the ankle-brachial index showed improved ankle pressures by more than 10mmHg and toe pressures by more than 10mmHg. There was also an improvement in bilateral ankle-brachial and toe-brachial index results, changing from mildly abnormal to normal. The patient was maintained on diosmin + hesperidin, sulodexide, clopidogrel, losartan, rosuvastatin, and as-needed pain medications. He underwent ultrasound-guided sclerotherapy of the left great saphenous vein under local anesthesia. A follow-up 10 days after sclerotherapy demonstrated clinical improvement with the complete resolution of crampy leg pain.
Conclusions: It is essential to distinguish between various leg pain symptoms. Recognizing signs of chronic venous insufficiency in the presence of peripheral arterial disease can pose a challenge, yet it is crucial for effective symptom management. Diligent and timely intervention can significantly enhance the quality of life for our patients. Ultimately, in cases like this one, performing sclerotherapy on superficial veins, such as the great saphenous veins, results in noticeable clinical improvement within a short timeframe.
Poster No. 148
Abstract No. 1787558
Acute limb ischemia after abdominal aortic aneurysm repair
1St. Luke’s Medical Center, Dr. HB Calleja Heart and Vascular Institute
Background: Acute limb ischemia is an unusual and potential complication that can arise within the first 24 hours after open surgical or endovascular repair of abdominal aortic aneurysms (AAA). It can occur shortly after the surgery or during the follow-up period and can be caused by various factors, including patient-related, technical, or graft-related factors. It is worth noting that the incidence of lower extremity ischemia is higher in endovascular surgery as compared to open surgery, at a rate of about 2–5%.
Case presentation: A 70-year-old Filipino male, diabetic, dyslipidemic, and 30-pack year smoker coming in for pulsating mass in the abdomen associated with constipation. Abdominal ultrasound showed dilated abdominal aorta measuring 9.5 cm hence CT aortogram was done and confirmed a large infrarenal abdominal aortic aneurysm with circumferential mural thrombosis measuring 11.3 cm x 10.1 cm. Duplex scan of both lower extremities were also done showing right superficial femoral and bilateral popliteal aneurysms. He was not suitable for endovascular stent grafting due to absence of landing zone; hence, he underwent open surgical repair. Postoperatively, his left leg was pale, cold to touch, with absent pulses. Extraction of emboli was prohibitive with failure to reestablish adequate aortoiliac inflow hence an expeditious femorofemoral bypass was most appropriate. He was maintained on heparinization post-operatively and was discharged improved. On follow-up, he was stable with a decrease in aneurysm size in the abdomen, right femoral and bilateral popliteal arteries.
Conclusions: The incidence of femoral and popliteal aneurysm in AAA is 6-9 % which carries a risk for ischemia. Because of the high co-existence of AAA with other peripheral aneurysms, screening using ultrasound among these patients could be of benefit as seen in this case. Lower extremity ischemia can be an early complication of open AAA repair. Acute limb ischemia affecting just one leg only usually results from a technical problem with the distal anastomosis, thromboembolism, atheroembolism, or in situ thrombosis of the ipsilateral graft limb. Treatment of lower extremity ischemia after open AAA repair involves immediate heparinization and surgical exploration.
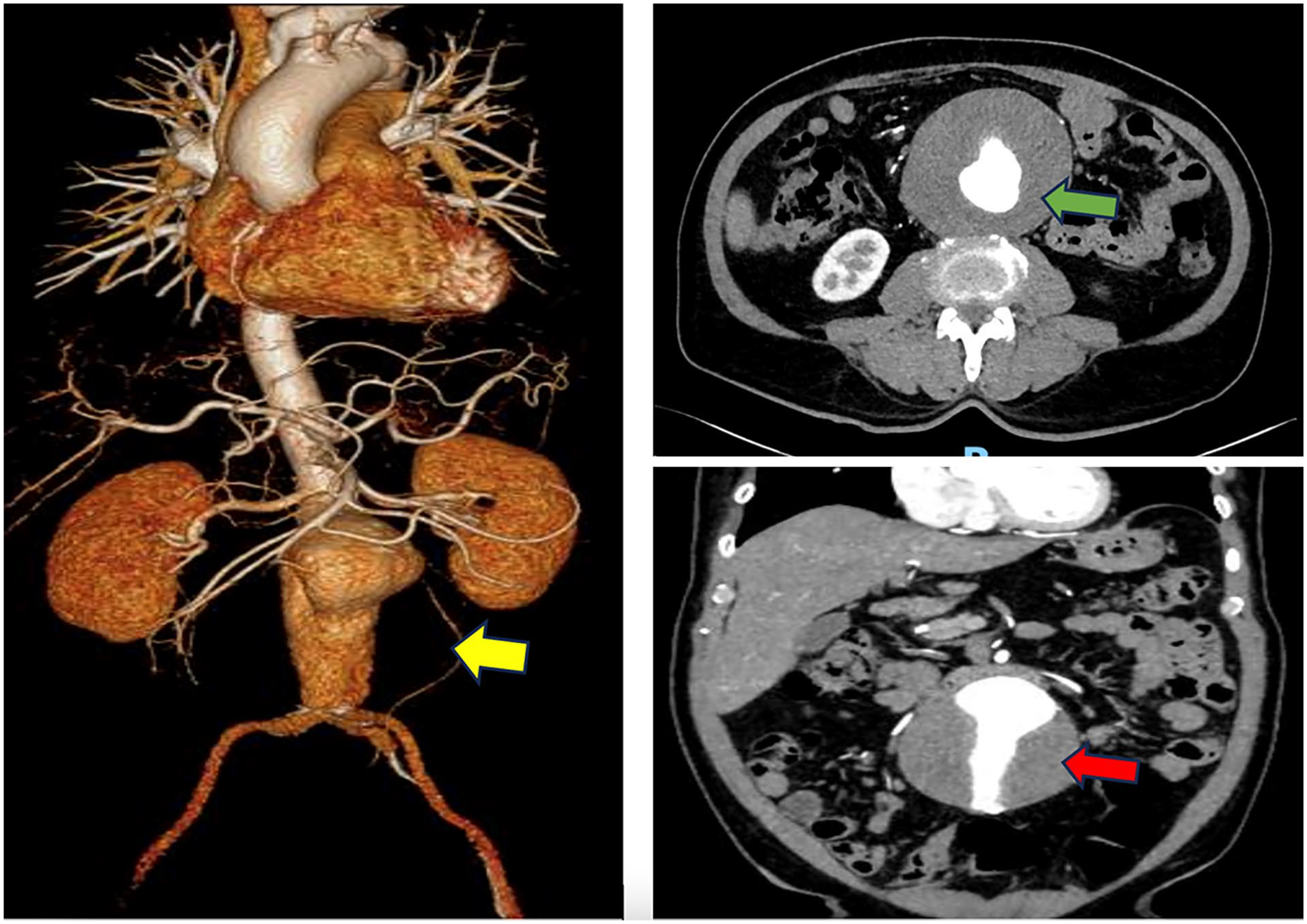
3D reconstruction (yellow arrow) showing dilatation of the abdominal aorta just below the origin of the renal arteries down to the prebifurcation, with maximum diameter of 10.1 cm and length of 11.3 cm (red arrow) with circumferential mural thrombosis (green arrow) with widest lumen diameter of 5.6 cm.
Poster No. 149
Abstract No. 1787910
Renal denervation cutting through resistant hypertension
1Beth Israel Deaconess Medical Center
Background: A 70-year-old female with history of chronic, resistant hypertension initially diagnosed at age 8 had cycled through various antihypertensives for decades.
Case presentation: Blood pressures were moderately controlled until 2013 when she developed recurrent symptomatic hypertensive episodes with systolic blood pressures over 200 mmHg characterized by pulsating headaches. Her situation was further complicated by significant lability in her blood pressures that resulted in lightheadedness – she reduced her time driving due to the unpredictable nature of her symptoms. She had normal renal function, adhered to a strict low sodium diet, did not use any illicit drugs, and had excellent medication adherence. Given the complicated nature of her hypertension, she was referred to the Beth Israel Deaconess Medical Center complex hypertension clinic. Initial ambulatory blood pressures excluded white coat hypertension and identified higher blood pressures in the evenings. Then, underlying causes were evaluated with blood work which revealed an aldosterone of 21 ng/dL, renin of 0.21 ng/mL/h, and a ratio of 105. Follow up adrenal CT demonstrated an 8 mm left adrenal nodule but had effective saline suppression testing suggestive of adrenal hyperplasia. She otherwise had an unremarkable renal artery duplex ultrasound and appropriate serum metanephrines. Over the following years, her antihypertensive requirements continued to escalate but efforts were made to introduce as many long-acting agents as possible. Systolic blood pressures were finally below 140 mmHg on a regimen including transdermal clonidine 0.6 mg weekly, felodipine 5 mg daily, hydrochlorothiazide 12.5 mg daily, olmesartan 40 mg daily, and spironolactone 50 mg twice daily. However, the pill burden was overburdensome for the patient so interventional options were presented. After multiple discussions in clinic, she was the first patient at our institution to undergo renal denervation after FDA approval for hypertension.
Conclusions: She had a tremendous response resulting on in sustained blood pressures in the 90 to 100s on spironolactone 50 mg twice daily, olmesartan 20 mg, and hydrochlorothiazide 12.5 mg daily and completely eliminating felodipine and clonidine.
Poster No. 150
Abstract No. 1795733
From herbal remedy to unforseen risk
1Cleveland Clinic Abu Dhabi
Background: Understanding the underlying factors contributing to the DVT is essential for effective management and prevention of recurrence. However, in some cases this may be a challenging process. We hereby present a case of deep vein thrombosis while using milk thistle.
Case presentation: A 41-year-old gentleman with no significant past medical history presented to the vascular medicine clinic with complain of left lower extremity swelling and pain that started 24 hours prior to presentation. A duplex ultrasound has been done that revealed DVT in the posterior tibial and popliteal veins of the left lower extremity. Patient denied history of hypercoagulable disease, blood clots, prolonged immobilization, travel, flu-like symptoms, contact with sick persons, positive COVID testing, injuries, or trauma prior to presentation. Hypercoagulable workup has found normal, including lupus anticoagulant, anticardiolipin antibodies, beta 2 glycoprotein, protein S, protein C, antithrombin, prothrombin, homocysteine, and factor V. In addition, age-appropriate malignancy screening has been found insignificant. On further questioning, the patient stated that seven months ago he started using supplements including vitamin D, milk thistle, and vitamin B complex.
Conclusions: We are hereby presenting a case of DVT, where a patient’s medical history, including the duration and dosage of milk thistle usage, as well as other relevant factors, were thoroughly examined. Although there is no currently established direct relationship between milk thistle and DVT, there has been emerging case reports suggesting the use of milk thistle as potential risk factor for DVT. Milk thistle is a widely used herbal supplement known for its purported hepatoprotective properties has been found to induce hormonal changes through estrogen-like effects, which may explain associated risk of DVT. In conclusion, the aim of this case is to shed light on the unexpected association between milk thistle and DVT, providing valuable insights into the potential risks and implications of herbal supplement use in patients with thrombotic disorders.
Poster No. 151
Abstract No. 1795765
A rare cause of a'q'ute limb ischemia
1Mayo Clinic
Background: Acute limb ischemia (ALI) is a limb-threatening and potential life-threatening process that must be quickly assessed and intervened upon. Determining the etiology of ALI is essential to prevent recurrent events. Here, we present a unique case of ALI from a popliteal artery embolism secondary to Q-fever endocarditis of a transcatheter aortic valve replacement (TAVR).
Case presentation: A 57-year-old female with medical history of bicuspid aortic valve status post TAVR (2019) presented to the ED with Rutherford IIA ALI. CT angiogram with run-off was notable for right popliteal artery occlusion. Heparin nomogram was initiated. She underwent right popliteal artery thromboembolectomy. For evaluation of her ALI, echocardiogram demonstrated multiple mobile masses on the TAVR valve. Blood cultures were drawn, and broad-spectrum antibiotics initiated. PET-CT showed increased FDG uptake at the TAVR. Culture-negative infective endocarditis (IE) workup was positive for Coxiella burnetii IgG and IgM antibodies. The patient proceeded to the OR for mechanical aortic valve replacement plus CABG x 1 (LIMA-LAD) for obstructive CAD as seen on a preoperative coronary angiogram. She was then discharged on doxycycline and hydroxychloroquine.
Conclusions: The workup for ALI should focus on finding the proximal source, as seen in this Q fever endocarditis case.
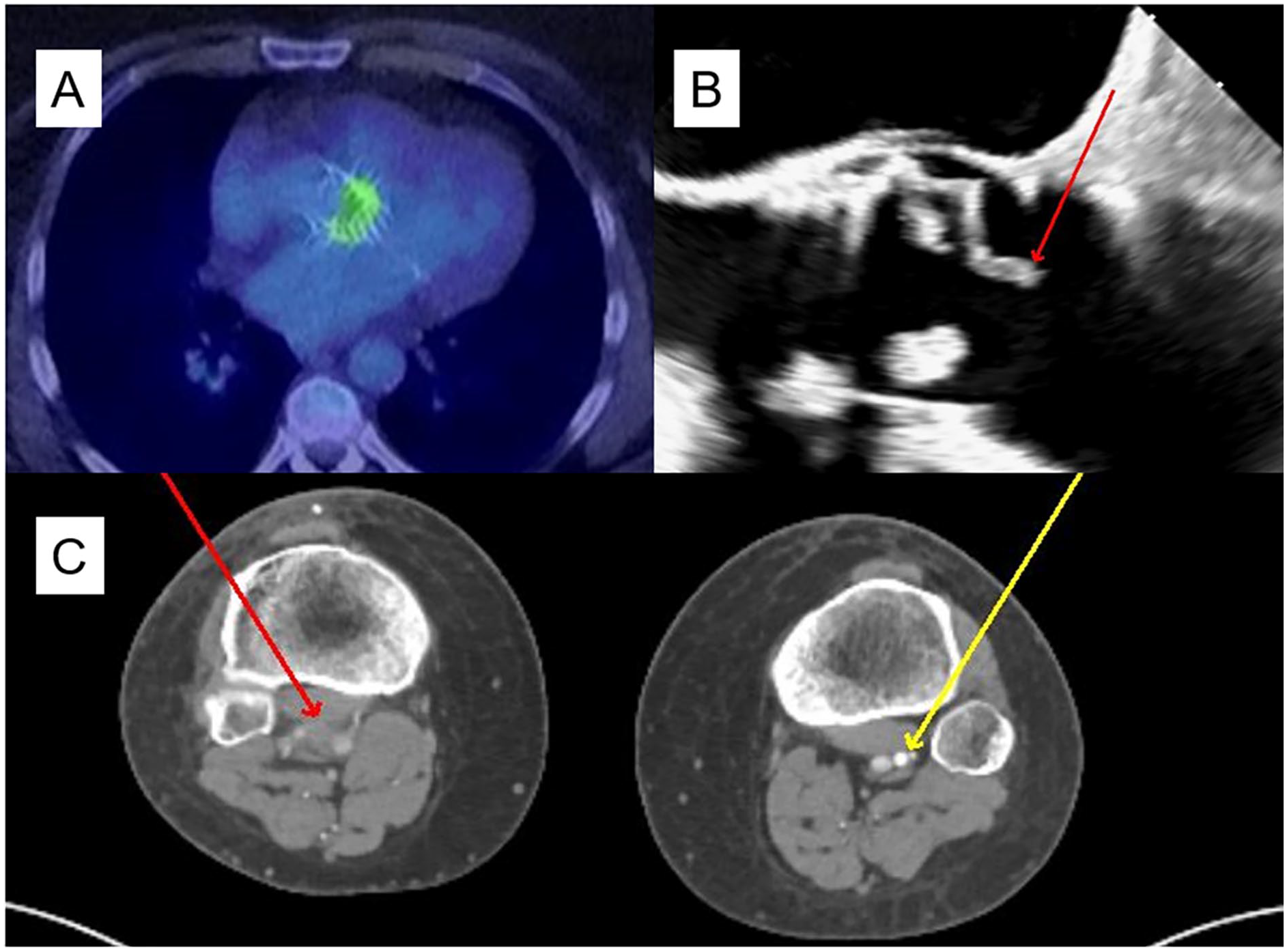
A: PET CT (transverse view) with avid FDG uptake at the aortic valve (bright green enhancement). B: transesophageal echocardiogram with vegetation prolapsing out of the valve plane (red arrow). C: CT Angiogram with runoff (transverse view) with acute occlusion of the right popliteal artery (red arrow) and patency of the left popliteal artery (yellow arrow).
Poster No. 152
Abstract No. 1796002
Takayasu's arteritis in the postpartum period
1Mount Auburn Hospital; 2Brigham and Women's Hospital
Background: Takayasu's arteritis is a rare, inflammatory vasculitis that primarily affects the large arteries, predominantly the aorta and its major branches. Pregnancy-associated Takayasu's arteritis is rare and presents an interesting association.
Case presentation: A 32-year-old female with a history of pre-eclampsia presented to the emergency room with sudden onset back pain and was found to have on a CT angiography of the chest, abdomen, and pelvis: 1. Circumferential wall thickening of the aortic arch and infrarenal abdominal aorta extending to the arch vessels. 2. Occluded left common carotid artery, left subclavian artery, and left vertebral artery. 3. Focal dissection of the infrarenal abdominal aorta with associated aneurysmal dilatation. 4. Focal wall thickening of the mid right subclavian artery with moderate luminal stenosis and possible focal dissection. She underwent a work-up for autoimmune and infectious etiologies with PET CT of the chest, abdomen, and pelvis, temporal artery duplex ultrasound, blood cultures, RPR/VDRL test, QuantiFERON test, HIV testing, CRP, ESR, ANA antibodies, c-ANCA antibodies, p-ANCA antibodies, and complement levels. The work-up was negative except for ESR at 39 mm/h, CRP at 33.4 mg/L, and PET CT of the chest, abdomen, and pelvis positive for: 1. Circumferential mural uptake in the aneurysmal aortic arch. 2. Uptake in the periphery of the abdominal aortic dissection. 3. Uptake at the proximal segments of the right subclavian, left common carotid, and left subclavian arteries. After a multidisciplinary discussion between rheumatology, infectious disease, and vascular medicine, the patient was diagnosed with Takayasu's arteritis and was started on intravenous Methylprednisolone. Subsequently, she underwent endovascular aortic aneurysm repair of the infrarenal aortic aneurysm. She remains on steroid therapy together with Azathioprine and Adalimumab.
Conclusions: We have described a peculiar case of Takayasu's arteritis diagnosed in the postpartum period. We hypothesize that pregnancy may have played a role in triggering the Takayasu's arteritis flare. Further research is needed to understand the complex relationship underlying pregnancy and autoimmunity.
Poster No. 153
Abstract No. 1796064
An atypical case of vasopressor induced peripheral ischemia
1Ohio University College of Osteopathic Medicine; 2Kettering Health Cardiology
Background: Surviving Sepsis guidelines endorse early use of Norepinephrine in the treatment of septic shock. Vasopressor-induced peripheral ischemia, though not routinely considered, has been reported with prolonged infusion of multiple vasopressors. Our case highlights IV norepinephrine used < 24 hours implicated with severe digital ischemia. We identify a lack of dosage thresholds in current literature for prevention of peripheral ischemia.
Case presentation: A 69-year-old female with type II diabetes mellitus and coronary artery disease presented with septic shock. IV fluids, broad-spectrum antibiotics and IV norepinephrine were given. The next day oral midodrine TID was favored the setting of improved hemodynamic stability. Pain and dusky discoloration developed in her fingertips. Vascular Doppler ultrasound and CTA abdomen with distal runoff revealed absent arterial flow in the hands and feet. Progressing dry gangrene presented a diagnostic challenge. Underlying anemia, thrombocytopenia, and PT/PTT occurred in the absence of palpable purpura or livedo reticularis. Vasopressor induced peripheral ischemia was diagnosed resulting in limb preserving amputation.
Conclusions: This case underscores severe consequences of peripheral ischemia in the management of septic patients. There is currently no literature consensus for risk averse dosing and duration of norepinephrine. Future consideration is needed so that risk factors and best practices can be identified to prevent development of this debilitating condition.

Dry gangrene with bullous changes in the setting of vasopressor administration. CT angiography demonstrating abrupt occlusion of the left anterior tibial artery above the ankle.
Poster No. 154
Abstract No. 1795801
Unusual digital vasculopathy in a young patient
1Harvard Medical School; 2Massachusetts General Hospital; 3Brigham and Women's Hospital; 4Boston Children's Hospital
Background: Discoloration of fingers and hands, with or without cold exposure, is often considered a benign phenomenon. However, when pain and ulcerations emerge, it is often a sign of serious systemic illness.
Case presentation: : A 17-year-old female with history of Raynaud’s phenomenon (RP) reports 6 months of progressive painful ulcerations and paronychia involving index fingers of both hands (A, B). Although symptoms are worsened by cold exposure, white to purple fingers discoloration did not improve with warming. Rheumatological work up was notable for positive anti-nuclear antibody (>1:2560, centromere pattern), positive anti-centromere antibody and weakly-positive antipolymerase III antibody. Anti-dsDNA, anti-extractable nuclear antigens, anti-Smith, anti-scl-70 and anti-RNP antibodies were negative. Inflammatory markers, complements, and thrombophilia panel were negative. The patient received botulinum injection to bilateral index fingers but reported worsening pain, prompting presentation to emergency department. Bilateral upper extremity MR angiogram (MRA) revealed multifocal severe stenoses and occlusions of multiple arteries of the distal forearms and hands (C, D). Lower extremity MRA was normal. PET/CTA demonstrated no evidence of medium-large vessel vasculitis. Based on serological and imaging data, she was diagnosed with pediatric systemic sclerosis (SSc) and started on vasodilators (calcium channel blocker and nitroglycerin paste, later changed to sildenafil and fluoxetine). She began immunosuppression using hydroxychloroquine and mycophenolate mofetil. The patient reported resolution of pain and the digital ulcers healed over several months.
Conclusions: RP is a digital vasculopathy affecting up to 11% of women and 8% of men. While primary RP is not associated with tissue destruction or systemic illness, secondary RP is marked by prolonged tissue ischemia and necrosis, and commonly occurs in autoimmune connective tissue disease such as SSc. Due to divergent prognosis in primary versus secondary RP, timely serological and angiographic workup is key. In our patient, MRA was particularly helpful in confirming diagnosis and expediting treatment, which led to healing of her digital ulcerations.
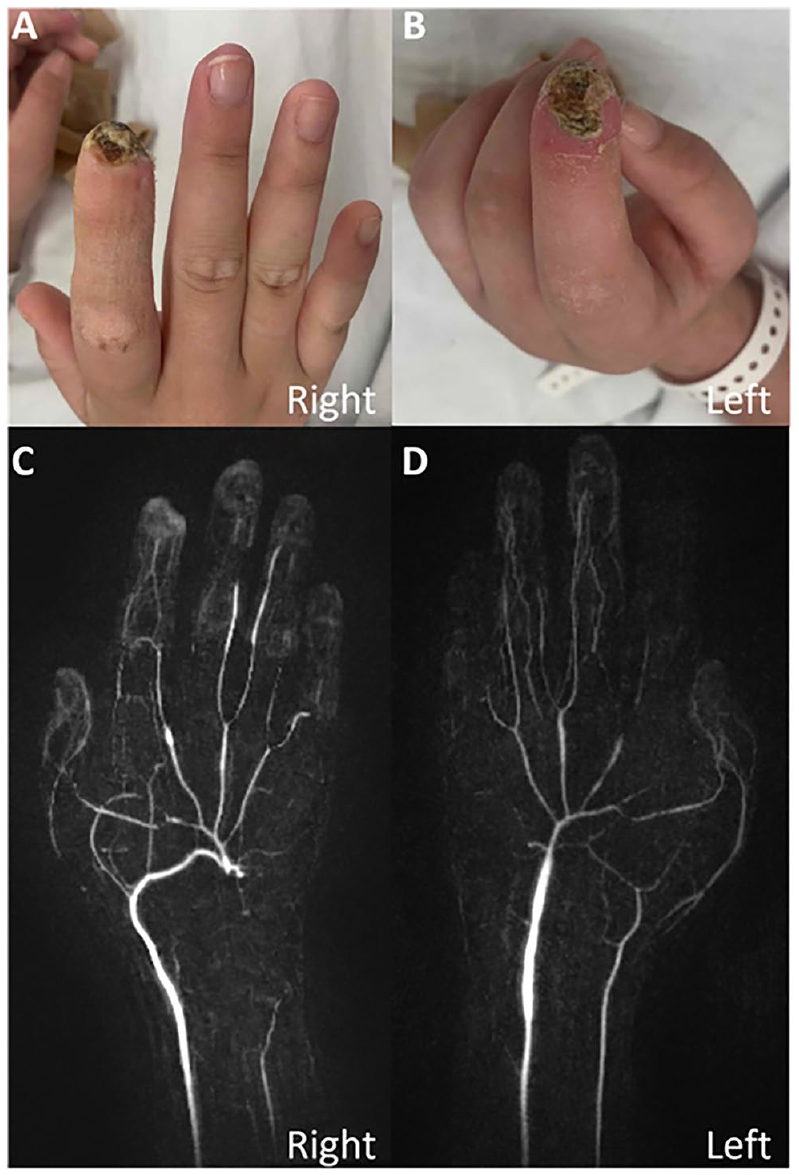
Poster No. 155
Abstract No. 1795906
"Unprovoked" venous-thromboembolism leading to diagnosis of polycythemia vera
1University of Virginia
Background: Polycythemia vera (PV) and other myeloproliferative neoplasms confer an increased risk for thromboembolic events. These thromboembolic events most commonly occur shortly before diagnosis with PV and may actually be what leads to the diagnosis of PV.
Case presentation: A 56-year-old female with a history of obstructive sleep apnea presented to an outside hospital with dyspnea and was diagnosed with acute submassive pulmonary embolism and bilateral lower extremity deep vein thrombosis. She was initially managed with anticoagulation alone but was taken for thrombectomy due to “worsening respiratory status”. The procedure was complicated by worsening hemodynamics requiring cannulation for veno-arterial extracorporeal membrane oxygenation (VA-ECMO) and melena (hemoglobin drop from 14.2 to 6.0 g/dL) requiring transfusion and transfer to our institution. The patient was stabilized, decannulated, and discharged on apixaban. Initially this index venous thromboembolic event was felt to have occurred in absence of identifiable risk factors. At her three month follow up, she was doing well and her hemoglobin had normalized. However, at patient’s six month follow up she reported an episode concerning for a transient ischemic attack and was complaining of significant dyspnea on exertion. A complete blood count checked at that time returned with polycythemia. Ultimately the patient was found to have low erythropoietin level and a JAK2 mutation, conferring a diagnosis of polycythemia vera.
Conclusions: Patients with myeloproliferative neoplasms are at increased risk for thromboembolic events, both venous and arterial.
Poster No. 156
Abstract No. 1796089
Dysautonomia due to aortic and carotid dissection
1Mount Auburn Hospital; 2Brigham and Women's Hospital
Background: Autonomic dysfunction has numerous recognized causes in clinical practice, such as diabetes mellitus and paraneoplastic syndrome. However, aortic dissection is rarely a cause.
Case presentation: A 56-year-old female with a history of hypertension presented after an episode of sudden chest pain followed by seizures. Blood pressure at presentation was 207/88 mm Hg. A CT angiography of chest, abdomen and pelvis showed Stanford type A/DeBakey type I aortic dissection with a flap extending from the aortic root to the left carotid sinus and right common iliac artery. Subsequently, the patient underwent ascending aortic aneurysm and dissection repair with hemi-arch reconstruction. About a month later, the patient was reporting symptomatic and highly variable blood pressures with values between 70/40 and 140/90 mm Hg. CT angiography showed stable aortic anatomy without further complications. The patient denied any history of dysautonomia or other conditions associated with autonomic neuropathy and was diagnosed with dysautonomia secondary to left carotid sinus damage from the previous aortic dissection. She has been responding well to her therapy with compression pantyhose, abdominal compression wrap, Pyridostigmine, and antihypertensives.
Conclusions: This case highlights an exceedingly rare cause of autonomic dysfunction resulting from mechanical damage to the carotid baroreceptors and highlights the intriguing physiology and pathophysiology of the carotid sinus and its repercussions on the patient’s hemodynamics.
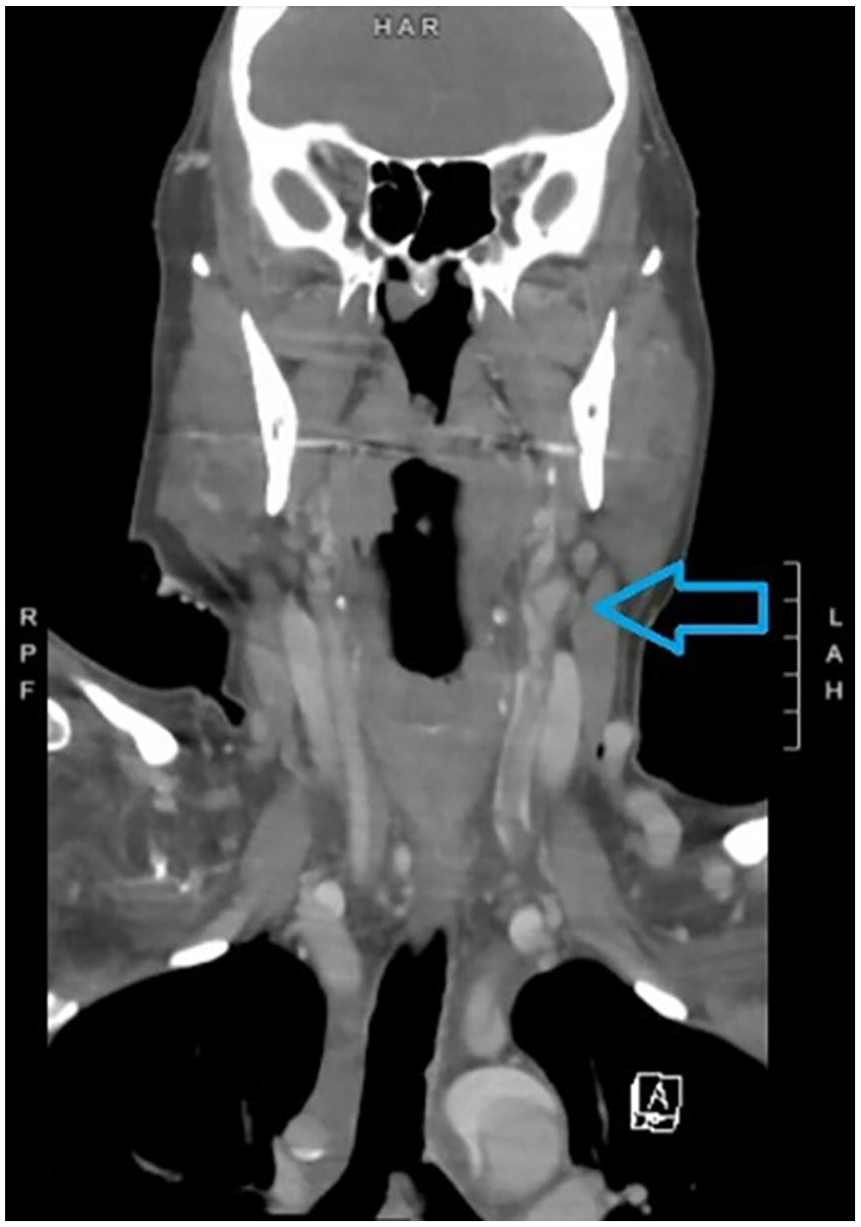
Dissection flap extending to the left carotid sinus.
Poster No. 157
Abstract No. 1796118
Multiple thromboemboli in a patient with dilated cardiomyopathy
1H.B. Calleja Heart & Vascular Institute, St. Luke's Medical Center; 2St. Luke's Medical Center-Quezon City
Background: Systemic thromboembolism is a serious complication of left ventricular thrombus in patients with heart failure. The incidence of LV thrombus in dilated cardiomyopathy ranges at 2-36%. It has an estimated 22% risk of embolization and 37% risk of developing adverse cardiovascular events.
Case presentation: Patient is a 23-year-old, male, came in for shortness of breath and bipedal edema. No co-morbidities and denies illicit substance use. On physical examination, he had bluish discoloration of the bilateral lower extremities with absent pulses and Doppler signals in the bilateral dorsalis pedis arteries; no motor and sensory deficits. Echocardiogram showed ejection fraction of 12.7%, global hypokinesia with multiple thrombi in the left ventricle. Arterial duplex scan showed thrombi in the right posterior tibial, peroneal, anterior tibial; and bilateral dorsalis pedis arteries. He was started on Heparin bolus followed by infusion; given for 4 days, eventually shifted to Enoxaparin; with improved discoloration and restoration of pulses. On further work up, HIV, ANA, anti-Sm, anti-dsDNA, Factor V leiden, Jak2 mutation were negative. Anti-thrombin III and protein C were low. Cardiac MRI findings are compatible with dilated cardiomyopathy with multiple thrombi at the mid and apical LV segments. On 14th hospital day, he had sudden onset of left-sided body weakness and drowsiness. Cranial MRI showed multifocal areas of acute to subacute infarct in the right cerebral hemisphere, with occluded right internal carotid artery. Factor Xa was within target. Emergency mechanical thrombectomy was done; achieved complete recanalization. Post procedure CT scan showed hemorrhagic conversion of the infarcts; hence, anticoagulant was held. A week after, repeat CT scan showed only petechial hemorrhages. Enoxaparin was resumed. Repeat echocardiogram showed improved EF at 26.7%; previously noted multiple LV thrombi were not appreciated. He eventually was discharged, stable.
Conclusions: Systemic thromboembolic events leading to both acute limb ischemia and ischemic stroke from left ventricular thrombus is rare. Due to high morbidity, management is critical. Therapeutic options include anticoagulation and thrombectomy.
Poster No. 158
Abstract No. 1796197
Endometriosis causing inferior vena cava thrombosis
1Mayo Clinic
Background: Endometriosis, an estrogen-dependent inflammatory condition, can lead to significant pelvic pain and infertility. Symptoms vary widely depending on the location of extra-pelvic endometriosis. It is not known to increase risk for venous thromboembolism (VTE). Here, we describe a unique case resulting in invasion of the inferior vena cava (IVC) leading to venous thromboembolism.
Case presentation: A 51-year-old woman with history of endometriosis, status post hysterectomy, presented for progressive abdominal pain with nausea and vomiting. CT showed a nonocclusive ‘tumor’ thrombus in the IVC adjacent to a large left retroperitoneal mass with encasement of the aorta, iliac vessels, and inferior mesenteric artery (Figure A and B). Biopsy revealed endometriosis. Anticoagulation was initiated for IVC thrombus. After three days, she developed severe flank pain due to a retroperitoneal hemorrhage into the mass. Incidentally, multiple segmental pulmonary emboli were identified (Figure C), leading to IVC filter placement. After multidisciplinary collaboration, she underwent surgical excision of mass with infrarenal aortoiliac resection, aorto bi-iliac bypass, and IVC thrombectomy with patch venoplasty. Pathology demonstrated endometriosis with bland thrombus in the IVC and a low grade mullerian adenosarcoma arising from the deeply infiltrating endometriosis.
Conclusions: Endometriosis is a heterogenous disease which is not associated with VTE, however, complications such as mass effect and transformation to adenosarcoma can increase these risks.
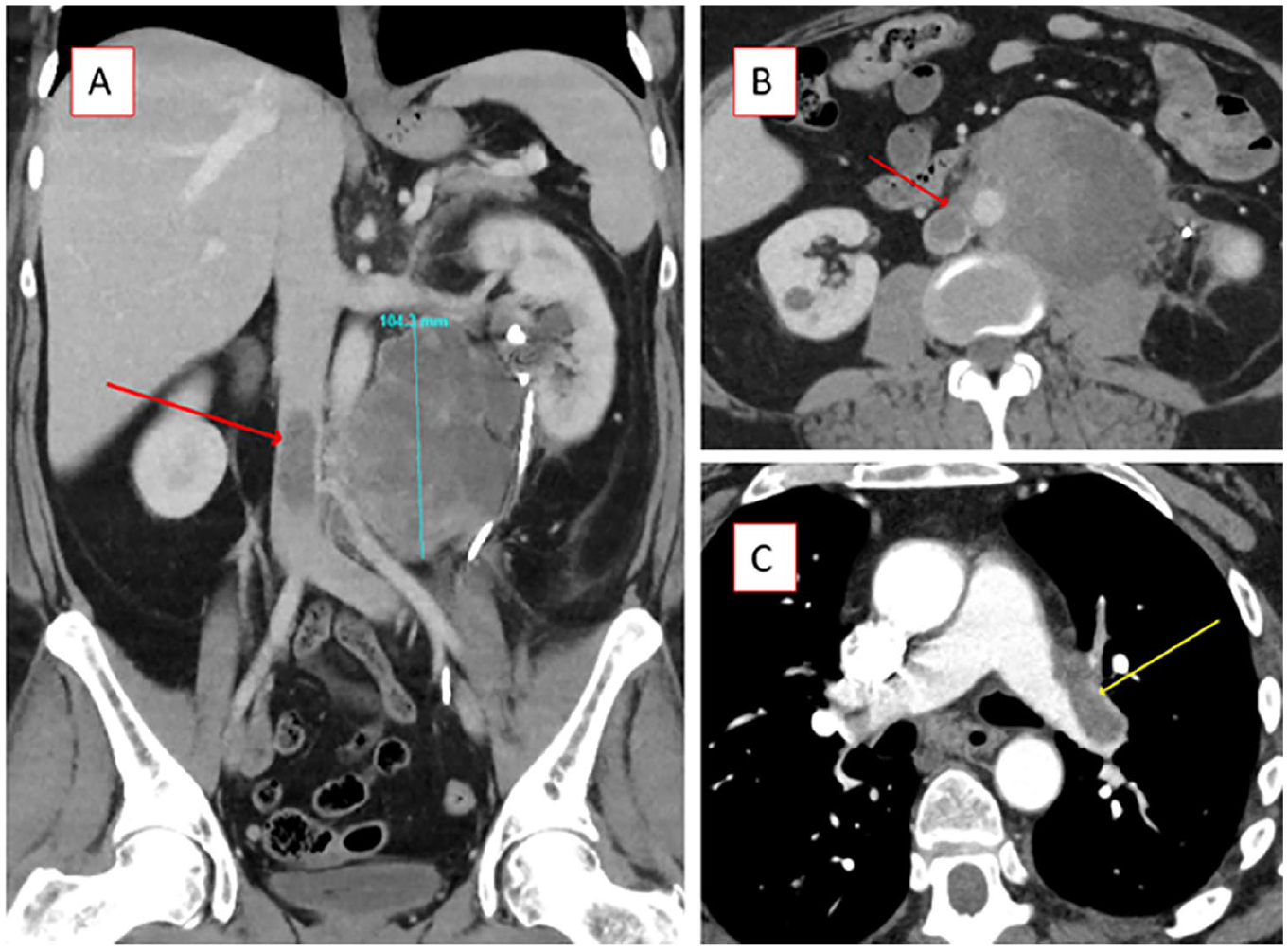
A: CT Abdomen/Pelvic (coronal view) with large retroperitoneal mass (blue line, measuring 104 mm) and associated tumor thrombus (red arrow); B: CT Abdomen/Pelvic (transverse view) with large retroperitoneal mass and associated tumor thrombus (red arrow); C: CT Angiogram of Chest (transverse view) with left main pulmonary artery embolism (yellow arrow).
Poster No. 159
Abstract No. 1796519
An incidental vascular finding during chest pain evaluation
1Eastern Vascular Associates
Background: Chest pain radiating to the back is concerning for acute cardiovascular syndromes. Imaging studies are used for evaluation and incidental findings are common. This case illustrates an incidental vascular abnormality during chest pain evaluation.
Case presentation: A 56-year-old woman presented with central chest pain radiating to the back. Bilateral brachial blood pressures were equal. ECG was unremarkable. Exam revealed tenderness of the sternum and epigastrium. A CBC, CMP, and troponin were normal. A CTA of the chest, abdomen, and pelvis was non-acute, but noted a high-grade stenosis of the celiac artery. The patient was treated with pantoprazole. A mesenteric arterial duplex ultrasound was then performed. Respiratory maneuvers of the celiac artery revealed: PSV 167 cm/s (inspiration) and 365 cm/s (expiration), EDV 46 cm/s (inspiration) and 107 cm/s (expiration), consistent with celiac artery compression physiology (Figure). The patient's symptoms self-resolved with pantoprazole; conservative management was pursued.
Conclusions: Incidental imaging findings are common and can cause emotional distress, leading to costly interventions. It is also important to distinguish between physical findings and a syndrome when evaluating physiologic celiac artery compression versus MALS.