
Abstract

Houston, Texas
September 19-22, 2024
Jay D. Coffman Young Investigator Award Presentations
In honor of Dr. Jay D. Coffman (1928–2006), distinguished internist and researcher of vascular medicine and clinical cardiology, SVM sponsors an annual award in vascular medicine and biology research.
Poster No. 1
Abstract No. 1787335
The interdependence between cancer and atherosclerosis
1Stanford University; 2University of California San Francisco; 3Massachusetts General Hospital; 4University of Texas MD Anderson Cancer Center; 5Technical University
Background: Emerging epidemiologic and animal studies suggest cardiovascular disease and cancer may directly influence one another. Multiple population studies indicate atherosclerosis is associated with the risk of a range of malignancies. We hypothesize that cancer promotes atherogenesis.
Methods: RNA sequencing was performed on the aortic arches of mice being subcutaneously injected with colorectal cancer cells or control buffer, from various background (diet, genetic, age, etc.). Similar experiments were carried out on atheroprone apolipoprotein E (Apoe)-deficient mice that were implanted with different types of tumors. A carotid ligation model was introduced to Apoe-deficient mice fed a high-fat diet. Colorectal cancer cells were inoculated subcutaneously into mice 4 weeks prior to harvesting carotid arteries. The arteries were subjected to Oil Red O, CD31 (an endothelial cell marker), and TER-119 (a red blood cell marker). O-link proteomics and ELISA were conducted on serum collected from tumor-bearing and tumor-free mice. RT-qPCR and tube formation assays were performed on cultured human aortic endothelial cells being treated with conditional media from primary cells and cancer cell lines.
Results: LRG1 was consistently upregulated in the aortic arches of mice regardless of the background or types of tumor cells being implanted. Tumor-bearing mice tended to have larger plaques and significantly more intraplaque neovascularization and hemorrhage. Mice implanted tumors had a higher level of circulating TNF. In vitro, conditional media from tumor cells stimulated LRG1 expression and tube formation. Blocking TNF in conditional media suppressed tube formation.
Conclusion: Our data provided evidence that cancer might promote atherogenesis through TNF-LRG1-stimulated intraplaque neovascularization and plaque instability.
Poster No. 2
Abstract No. 1788110
Clinical trajectory before and after ankle-brachial index testing
1Vanderbilt University Medical Center
Background: Many patients with peripheral artery disease (PAD) develop signs, symptoms, and high-risk comorbidities of PAD long before diagnostic testing is obtained. We sought to characterize the clinical trajectories of patients before and after ankle-brachial index (ABI) testing in a large healthcare system.
Methods: From more than 3 million individuals in a deidentified electronic medical record database, we used a validated natural language processing tool to identify patients without prior PAD who underwent first-time ABI testing. Clinical data, including comorbidities and medical therapy, were abstracted from the two years preceding and five years following ABI testing. The primary outcome was clinical trajectory before and after ABI testing using validated phenome-wide association study (PheWAS) codes. Secondary outcomes included medical therapy and endovascular/surgical revascularization before and after an abnormal ABI.
Results: A total of 13,015 patients, including 5,287 women and 1,728 Black patients, underwent initial ABI testing. This yielded 5,837 normal (ABI=1.0-1.4), 5,685 abnormal (ABI < 0.9), 873 borderline (ABI 0.91-0.99), and 620 noncompressible (ABI > 1.4) results. Diabetes, chronic kidney disease, and tobacco use were observed in 29.6%, 14.9%, and 46.9% of the total population, respectively. In PheWAS analysis, pre-existing atherosclerosis was associated with an abnormal ABI. Following ABI testing, abnormal ABI was associated with claudication and foot wounds, whereas normal ABI was associated with osteoarthritis. Prescription of PAD-related medical therapy modestly increased after an abnormal ABI. For instance, 51.1% were on a statin prior to abnormal ABI, and this increased to 61.5% in the subsequent 5 years (P< 0.001). Among patients with an abnormal ABI, most revascularizations occurred following first-time ABI testing (endovascular: 2.6% vs 9.5%, P< 0.0001; and surgical: 1.3% vs 7.1%, P< 0.0001).
Conclusion: ABI testing is an important inflection point in the clinical trajectory of patients with pre-existing atherosclerosis and an opportunity to optimize medical therapy prior to PAD-related complications. More attention should be devoted to medical optimization following an abnormal ABI.
Poster No. 3
Abstract No. 1782235
HIV association with incident venous thromboembolism among veterans
1Vanderbilt University; 2Vanderbilt University Medical Center; 3University of Pittsburgh School of Public Health; 4Veterans Affairs Connecticut Healthcare System & Yale University Schools of Medicine and Public Health; 5Vanderbilt University Medical Center & Veterans Affairs Tennessee Valley Healthcare System
Background: Data from early in the antiretroviral therapy (ART) era suggest people with human immunodeficiency virus (PWH) are at increased risk of superficial thrombophlebitis and other forms of venous thrombosis. We hypothesized that this risk would be attenuated in a contemporary cohort with sustained viral suppression and a focus on pulmonary embolism and deep vein thrombosis.
Methods: We analyzed data from the Veterans Aging Cohort Study, a longitudinal, observational, prospective study of PWH matched 1:2 with people without HIV on age, sex, and race/ethnicity. The primary outcome was incident venous thromboembolism (VTE), defined as pulmonary embolism or lower extremity deep vein thrombosis, identified using administrative codes. After excluding individuals with prevalent VTE, we calculated VTE incidence rates by HIV status using Poisson regression. We performed Cox proportional hazards regression to estimate risk of incident VTE based on HIV status and either CD4+ T cell count or HIV viral load. Models were adjusted for demographics, VTE risk factors (including malignancy and central venous catheters), and time-updated measures of viral suppression.
Results: Among 143,461 total individuals (43,444 PWH), mean age was approximately 50 years, and 47% were Black. There were 8,502 incident VTE events (2,764 among PWH) over a mean follow-up period of 10.8 years. Rates of incident VTE per 1000 person-years were higher for PWH (6.41; 95% CI, 6.17-6.65) than those without HIV (5.09; 95% CI, 4.96-5.23). PWH were at increased risk of VTE (HRadj, 1.45; 95% CI, 1.38-1.53) compared to those without HIV. The risk was highest among those with time-updated CD4+ T cell counts < 200 cells/mm3 (HRadj, 2.67; 95% CI, 2.41-2.95) or HIV viral loads >500 copies/mL (HRadj, 1.84; 95% CI, 1.69-2.01) compared to those without HIV.
Conclusion: In a large, racially diverse cohort with access to contemporary ART, HIV infection was associated with an increased risk of incident VTE. This risk was greatest in those with low CD4+ T cell counts or elevated HIV viral loads. If confirmed in additional settings, these findings may help risk stratify patients and potentially guide prophylactic interventions in the future.
Poster No. 4
Abstract No. 1787142
Beneficial venous endothelium response to local mTOR inhibition
1University of Michigan; 2Surmodics, Inc
Background: mTOR inhibitors impact thrombotic, inflammatory, and fibrotic pathways in vitro. Drug-coated balloons (DCB) deliver mTOR inhibitors that effectively reduce arterial intimal hyperplasia, but their utility in the venous system is unknown. We develop a novel microsurgical balloon venoplasty (BV) survival technique for DCBs testing characterizing deep vein endothelium changes.
Methods: Using adult anesthetized (isoflurane) Sprague Dawley rats (500g), IVC infrarenal side branches were ligated, and back branches cauterized. A sharpened guidewire with a 3x10 mm sirolimus DCB backloaded (dose: 3.0 μg/mm²) was inserted using a novel retrograde cannulation technique (RCT) and inflated for 3 minutes with 15% overstretch (IVC diameter measured by ultrasound). IVC thrombosis was created by placing a microclip in the IVC for 24 hours before DCB in the thrombotic cohort. IVCs were harvested after 15 days measuring sirolimus concentration (liquid chromatography-LC), protein inflammation, cell adhesion molecules, and active/phosphorylated-AKT (pAKT) levels, and histology analysis.
Results: Our microsurgical RCT model for DCB testing had a 99.96% survival rate (58/60) in non- and thrombotic cohorts. LC confirmed sirolimus vein wall uptake. Coated balloon venoplasty (CBV) compared to no treatment (Sham) and uncoated venoplasty (UB) resulted in significantly decreased local protein levels of E- and P-selectin, IL-6, and pAKT confirming mTOR inhibition, and decreased vein wall thickness. Figure 1. A-F.
Conclusion: Sirolimus CBV treatment inhibits venous endothelial cellular adhesive properties and inflammatory profile up to 15 days post-procedurally. Such modulation deserves further study in post-thrombotic veins as a potential measure to prevent sequelae such as recurrent venous thrombosis and fibrosis.
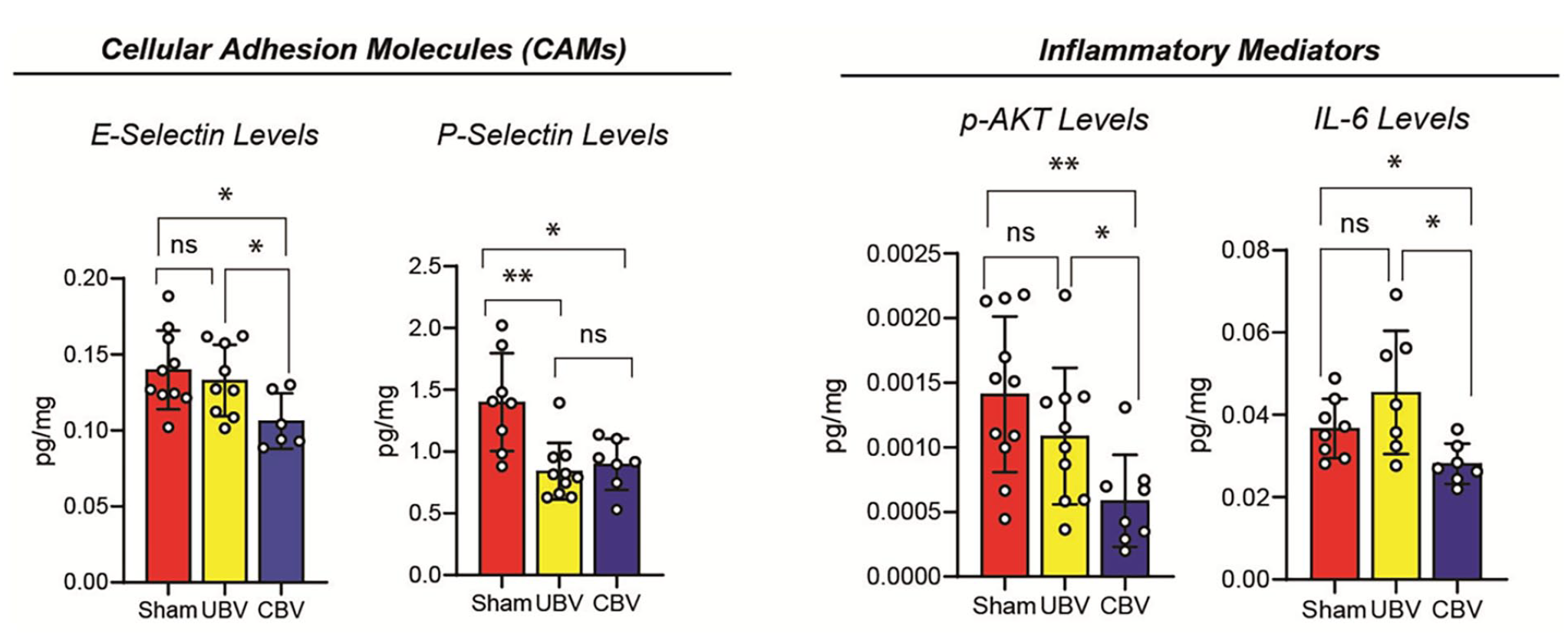
IVC protein levels after 15 days of sirolimus DCB.
Oral poster presentations
Poster No. 5 – Withdrawn
Poster No. 6
Abstract No. 1796224
Sex- and age-based trends in Loeys-Dietz syndrome
1Mayo Clinic Arizona; 2Mayo Clinic
Background: Connective tissue disorders can have variable vascular manifestations across different groups. Marfan’s syndrome, for instance, is associated with higher rates of aortic dissections in males compared to females. The impact of age and sex on the vascular presentations of patients with and Loeys-Dietz Syndrome (LDS) has not been examined in the literature, especially in younger cohorts ⩽ 60-years-old.
Methods: Patients with LDS ⩽ 60-years-old were selected from a database of 84,496 patients who were enrolled in the Mayo Clinic Tapestry DNA Sequencing Research Study. Patients were categorized by sex and grouped into 4 age groups: 18-30, 31-40, 41-50, and 51-60. Outcomes, defined as revascularization, stroke, dissection, surgical intervention (for aneurysm repair), or death, were compared using chi-squared analysis and Fisher’s Exact Test.
Results: A total of 33 LDS patients (11 males, 22 females; x̄ age= 42.36 ± 11.05) were included. The most common aneurysm sites were the thoracic aorta (21.21%) followed by the carotid (15.15%) and splanchnic arteries (12.12%). When comparing overall differences between sexes, there was no significant difference in outcomes. When comparing across age groups, males had a higher prevalence of revascularization (40%), dissection (40%), stroke (40%), and death (20%) across the 31-40 age range compared to females, who had 0% prevalence of all outcomes in that age. Interestingly, this was reversed in the 41-50 and 51-60 ranges, where males had 0% prevalence of all outcomes. Compared to the other age groups, patients in the 41-50 age range had the highest prevalence of stroke (18.18%), surgery (27.27%), and dissection (27.27%). Those in the 31-40 range had the highest prevalence of revascularization (22.22%) and death (11.11%). The differences in prevalence were however not statistically significant.
Conclusion: Despite the lack of statistical significance, the trend suggests that younger males experience more severe outcomes compared to females in the same age group, whereas older females tend to have a higher prevalence of adverse outcomes. These findings call for further analysis with larger, multi-institutional cohorts to create more definitive risk assessment tools for LDS patients.
Poster No. 7
Abstract No. 1781599
Acetyl-CoA metabolism enhances vascular recovery through angiogenic transdifferentiation
1Houston Methodist; 2Houston Methodist Research Institute
Background: We have exciting new evidence for metabolic control of cell fate in the vascular response to limb ischemia in our murine model of Peripheral Arterial Disease (PAD). Our prior work indicates that a glycolytic shift increases nuclear concentrations of citrate during transdifferentiation. Citrate is then converted by ATP Citrate Lyase (ACL) to acetyl-CoA for histone acetylation to increase DNA accessibility.
Methods: In mice, pharmacological inhibitors and a fibroblast conditional knockout approach were used to abrogate ACL expression. Fsp1-Cre: R26R-EYFP and inducible Col1A2-iCre: R26R-tdTomato mice served as fibroblast lineage-tracing models. We utilized the murine model of hindlimb ischemia, along with an in vivo Matrigel plug assay and lineage tracing studies, to examine the function of ACL-mediated acetyl-CoA in fibroblasts responding to ischemia. Isotope tracing assays were conducted to identify the primary carbon sources of acetyl-CoA.
Results: We observed a significant upregulation of ACL in mouse ischemic muscle following femoral artery ligation, primarily occurring in fibroblasts. Pharmacological inhibition of ACL; or genetic knockdown as in fibroblast conditional ACL-deficient mice; were each associated with impaired perfusion recovery as assessed by Laser Doppler; with decreased capillary density in gastrocnemius muscle; and with greater ischemic injury. Ablation of ACL reduced the population of fibroblast-derived endothelial cells, as indicated by lineage-tracing studies. This suggests that ACL regulation of vascular recovery may occur through the modulation of angiogenic transdifferentiation. Additionally, subcutaneous Matrigel administration in mice revealed that ACL knockdown in fibroblasts diminished plug vascularity and the number of fibroblast-derived endothelial cells. We also demonstrated that glucose and glutamine were the primary carbon sources for accumulated acetyl-CoA, and inhibition of glucose transporter (Glut1) or glutamine transporter (Slc1a5) significantly impaired transdifferentiation.
Conclusion: ACL-mediated acetyl-CoA is a regulator of vascular recovery in limb ischemia and may act through the modulation of angiogenic transdifferentiation.
Poster No. 8
Abstract No. 1788275
Endothelial mRNA-sequencing in combustible and electronic cigarette users
1Boston Medical Center; 2Boston University; 3Boston University
Background: Young adults increasingly use electronic cigarettes (e-cigs) rather than traditional combustible cigarettes. We performed mRNA sequencing to explore the mechanisms of endothelial cell (EC) dysfunction in cigarette and e-cig users.
Methods: Endothelial biopsy was performed on 64 healthy adults aged 18-45 who were combustible or e-cig users, or tobacco non-users. Ecs were purified using CD144 magnetic immunobeads. EC total RNA was isolated with Qiagen RNA Easy Micro Kits. Profiling was done on a NextSeq sequencer. Samples with transcript integrity number (TIN) < 10 were removed, genes were filtered with edgeR::filterByExpr, and differential expression analysis was done with DESeq2. Pathway analysis was done via Gene Ontology database.
Results: The cohort was 34% female with a mean age 26±7 years. 49/64 samples meeting TIN-quality standards were analyzed to yield the final cohort of combustible (n=16), e-cig (n=17), and non-users (n=16). Compared to non-users, there were 28 up- and 1 downregulated gene in combustible cigarette users, and 26 up- and 0 downregulated genes in e-cig users (Log2 fold change>1, FDR p-adj< 0.01). 14 genes were upregulated in both combustible and e-cig users. Pathways involving inflammation and adaptive immunity were highly upregulated (FDR p-adj< 0.05).
Conclusion: Combustible and e-cig use leads to upregulation of pathways related to inflammation and adaptive immune responses. Differences in EC gene expression between combustible and e-cig users suggest unique mechanisms of EC dysfunction.

Poster No. 9
Abstract No. 1786971
LATS1/2 -CD38 axis role in disturbed-flow induced atherothrombosis
1University of Texas MD Anderson Cancer Center; 2Escuela de Medicina y Ciencias de la Salud, Tecnológico de Monterrey; 3Houston Methodist Research Institute; 4Baylor College of Medicine
Background: Atherosclerotic and high-risk plaques are often found in areas of the vessel wall subjected to disturbed blood flow (d-flow), which suggests that d-flow-induced endothelial cell (EC) dysfunction may contribute to plaque formation, unlike the regions experiencing laminar flow (l-flow). While the involvement of the Hippo pathway (LATS1/2-YAP) in mechano-transduction has been proposed, the specific role of LATS1/2 in response to d-flow is not fully understood.
Methods: We utilized endothelial cell (EC)-specific Lats1 and Lats2 knockout (EKO) mice in a partial left carotid ligation (PLCL) model to recapitulate the d-flow conditions. Plaque phenotyping was performed by integrating imaging mass cytometry and sequential immunofluorescence of COMETTM.
Results: Although both l-flow and d-flow activate YAP activity, only d-flow decreases LATS1/2 expression. Within 14 days after inducing Lats1/2 deletion with tamoxifen in tamoxifen-inducible Lats1homo(-/-) /Lats2 homo(-/-) EKO mice, all the mice (27/27) had died of severe systemic edema with increasing vascular permeability. In Lats1het(+/-)/Lats2 homo(-/-) EKO mice, we observed the development of atherothrombotic lesions characterized by increased EC proliferation, a senescence-associated secretory phenotype (SASP), and upregulation of thrombosis-related molecules in ECs at the single-cell level in the atherothrombosis lesion in vivo. Mechanistically, the reduction of LATS1/2 caused by d-flow stimulated CD38 expression, which is a strong inducer of SASP via provoking NAD+ depletion, in a manner dependent on Lamin A, but independent of YAP. Furthermore, the inhibition of CD38 mitigated both d-flow-induced EC proliferation and SASP, as well as the formation of atherothrombosis in conditions where LATS1/2 was depleted.
Conclusion: These findings indicate that downregulation of LATS1/2-mediated CD38 induction in response to d-flow triggers a dual endothelial response characterized by increased proliferation and SASP, ultimately contributing to the development of atherothrombosis, which is commonly seen in the advanced stages of coronary atherosclerosis in humans, but not in mouse models of atherosclerosis.
Poster No. 10
Abstract No. 1787956
Role of d-beta-hydroxybutyrate dehydrogenase in endothelial senescence
1Houston Methodist Research Institute; 2The University of Texas MD Anderson Cancer Center
Background: Senescence resulting from replicative aging as well as chronic stress, alters cell metabolism and triggers the senescence associated secretory phenotype (SASP), generating a pro-inflammatory environment that promotes cardiovascular disease (CVD). SASP-manifesting cells release a mix of pro-inflammatory cytokines, chemokines, growth factors, pro-angiogenic factors, and reactive oxygen species (ROS). Vascular aging accelerates with SASP, evident after exposure to ionizing radiation (IR) or accumulation of progerin in Hutchinson-Gilford progeria syndrome (HGPS). Therefore, regulatory mechanisms governing SASP may be shared by endothelial cells (Ecs) exposed to IR and those affected by progerin.
Methods: We utilized ion chromatography-mass spectrometry (IC-MS) to identify critical metabolite changes common between IR-exposed and HGPS Ecs. Ecs derived from induced pluripotent stem cells were obtained from HGPS patients and non-HGPS controls. Advanced analytical methods, including Random Forest and Support Vector Machines (SVM), were employed to analyze integrated datasets for identifying key protein and metabolite networks affected by these conditions.
Results: Significant pathways were initially identified using MetaboAnalyst5.0, followed by selection of relevant metabolites using statistical or machine-learning methods to train predictive models with Random Forest and SVM using HGPS metabolite data. Predictive accuracies with 15 features from this analysis were 75%, with CDP-Ethanolamine (CDP-E) and 3-Hydroxybutyric acid (3-HB) emerging as the top hits. A similar approach was applied to RNA-seq data, revealing Atg9b and Pou5f1 as the top genes. Notably, CDP-E-mediated phosphatidylcholine serves as an allosteric activator of BDH1, leading to upregulation of 3-HB, which subsequently induces Pou5f1 mRNA. Upregulation of BDH1 and Pou5f1 was observed in Ecs exposed to IR and HGPS Ecs, regulating 3-HB induction and senescence.
Conclusion: This study represents the first report demonstrating the potential role of CDP-E-mediated BDH1 activation and subsequent 3-HB induction in regulating senescence, and potentially SASP, in Ecs.
Poster No. 11
Abstract No. 1794905
Hepatocyte growth factor for pad: a clinical trial
1Northwestern University Feinberg School of Medicine; 2National Institute on Aging; 3University of Virginia; 4Northwestern University; 5Augusta University; 6Stanford University; 7The University of Chicago; 8University of Maryland School of Medicine; 9University of Kentucky; 10University of California San Diego
Background: VM202 is a plasmid that encodes isoforms of hepatocyte growth factor (HGF). HGF stimulates angiogenesis and promotes muscle regeneration. We hypothesized that VM202 injections in gastrocnemius muscle of people with lower extremity peripheral artery disease (PAD) would improve walking performance.
Methods: In a double-blind randomized clinical trial, people with PAD were randomized to gastrocnemius muscle injections of either four doses of 4 mgs of VM202 or placebo every 14 days. The primary outcome was 6-month change in 6-minute walk distance. Secondary outcomes included 3-month change in treadmill walking time, hyperemic calf perfusion by MRI arterial spin labeling, and gastrocnemius muscle biopsy measures. In this Phase II Trial, statistical significance was pre-specified as a one-sided P value < 0.10.
Results: 39 participants with PAD (25 (64.1%) Black, 11 (29.1%) female) were randomized. Adjusting for age, race, smoking, and baseline performance, VM202 did not improve 6-minute walk at 6-month follow-up, compared to placebo (-13.5 meters, -38.5, +∞). At 3-month follow-up, VM202 significantly increased maximum treadmill walking time and gastrocnemius abundance of central nuclei, compared to placebo (Table).
Conclusion: These data do not support gastrocnemius injections of VM202 to improve 6-minute walk in PAD. Secondary outcomes suggested the potential for benefit on skeletal muscle measures and treadmill walking.
Effects of VM202, compared to placebo, on study outcomes in people with peripheral artery disease.

Calf muscle perfusion was measured with MRI arterial spin labeling.
Poster No. 12
Abstract No. 1771272
Home-based gamification to increase physical activity in PAD
1University of Pennsylvania; 2Lehigh Valley Heart and Vascular Institute; 3Ascension Health
Background: Supervised exercise improves walking performance and quality of life in patients with peripheral artery disease (PAD), but few are able to participate. A home-based walking program could extend these benefits to more patients.
Methods: We conducted a randomized controlled trial of gamification and automated coaching to increase daily physical activity in patients with PAD. Patients were mailed a wearable fitness tracker, established a baseline daily step count, set a goal to increase daily step count, and were randomized to control (n = 52) or gamification plus automated coaching (n = 50). The control group wore the device but received no other intervention for 24 weeks. The gamification plus automated coaching group participated in a game based on meeting daily step goals and received educational text messages. The 16-week intervention was followed by an 8-week follow-up period.
Results: 102 patients (mean age, 70 years; 52% male, 71% with exertional lower extremity symptoms) were enrolled. Compared with controls, gamification plus automated coaching led to a greater increase in mean daily steps from baseline during the intervention period (adjusted difference, 922; 95% CI, -44 to 1888; P = 0.06) and follow-up period (adjusted difference, 1085; 95% CI, 118 to 2052; P = 0.03)
Conclusion: Gamification plus automated coaching increased daily physical activity compared with control in patients with PAD and may represent an attractive option for patients who are not able to participate in supervised exercise therapy.

Mean daily steps for gamification + automated coaching versus control over the study period.
Poster No. 13
Abstract No. 1787070
Colchicine mitigates radiation-induced senescence-associated secretory phenotype and atherosclerosis
1University of Texas MD Anderson Cancer Center; 2Houston Methodist Research Institute
Background: Colchicine’s (microtubule disruptor) effectiveness in suppressing inflammasome activation, which is prompted by the deactivation of SIRT2 due to NAD+ depletion, through the inhibition of α-tubulin acetylation is reported. But its impact on the depletion of NAD+ itself, as well as the consequent induction of senescence-associated secretory phenotype (SASP), remains unclear. Our hypothesis posits that colchicine may reduce NAD+ depletion and subsequent SASP induction, thereby diminishing the occurrence of RICVD in mouse models used for preclinical studies.
Methods: C57Bl6 mice were subjected to both AAV-PCSK9 and a high-fat diet for 14 days, culminating in exposure to 3 Gy of IR to the neck and thoracic areas. Subsequently, they received a daily regimen of colchicine at 0.01 mg/kg or a placebo for 15 days, timed to end with the partial left carotid ligation (PLCL) surgery. Carotid arteries were collected for histological analysis 3 weeks after PLCL. Additionally, in a separate assay to evaluate the post-irradiation effects and SASP development, colchicine treatment commenced 2 weeks post-IR and continued for another 2 weeks. SASP was then assessed in bone marrow-derived macrophages (BMDMs).
Results: Our findings demonstrate that colchicine, at an in vitro concentration of 10 µM, effectively halted NAD+ depletion, mtROS production, and SASP, which are commonly induced by 2 Gy of IR in BMDMs. In vivo, we administered colchicine at a dosage of 0.01 mg/kg/day, or a placebo to the mice 14 days after IR exposure and analyzed BMDMs after a subsequent 14-day treatment period. The results showed that colchicine curbed the prolonged depletion of ATP/NAD+ and reduced cytokine production in BMDMs, even with treatment commencement 14 days post-IR. These results collectively suggest that colchicine’s ability to prevent IR-induced SASP is likely due to its action on NAD+ levels. Lastly, we found that colchicine significantly attenuated the progression of carotid atherosclerosis instigated by IR in C57Bl6 mice.
Conclusion: The results underscore colchicine’s potential efficacy in lessening the detrimental impact of radiation on atherogenesis, offering important perspectives for its prospective therapeutic use in the treatment of RICVD.
Poster No. 14
Abstract No. 1787258
TERF2IP sumoylation drives endothelial senescence and stemness
1University of Texas MD Anderson Cancer Center; 2Houston Methodist Research Institute; 3Escuela de Medicina y Ciencias de la Salud, Tecnológico de Monterrey
Background: TERF2IP shields telomeres (TLs) by associating with TRF2 and promotes senescence by interacting with p90RSK. This interaction occurs in endothelial cells (Ecs) under disturbed flow (d-flow). Although TERF2IP K240 can be SUMOylated, its role in senescence and atherogenesis remains unclear.
Methods: Ecs were exposed to d-flow and treated with TRF2 (a critical protector of TLs) siRNA, (siTRF2) or control siRNA to detect the specific effects of TERF2IP SUMOylation in TL damage-mediated senescence, proliferation, and inflammation. We also generated TERF2IP K237R knock-in (KI) mice (mouse K237 is equivalent to human K240) and assessed the role of TERF2IP SUMOylation in atherosclerosis.
Results: TERF2IP K240 SUMOylation increased in Ecs under d-flow, but not by laminar flow. D-flow and siTRF2-induced senescence and DNA damage response were abolished by overexpressed TERF2IP K240R (KR) mutant compared to TERF2IP wild type (WT), suggesting the crucial role of TERF2IP SUMOylation on TL damage-mediated senescence. Although TERF2IP KR did not inhibit d-flow-induced NF-κB activation, TERF2IP KR inhibited inflammasome activation via activating NAD+-Sirtuin 2 (SIRT2) and reducing α-tubulin acetylation, suggesting that TERF2IP SUMOylation regulates EC inflammation via NAD+-SIRT2 dependent and NF-κB independent mechanism. RNA-seq analysis has shown that SUMOylation of TERF2IP concurrently enhances the expression of genes associated with proliferation (Hoxb5), apoptosis (Anxa1), and inflammation (Tnsf18). This modification of TERF2IP also leads to increased proliferation, apoptosis, and inflammation in Ecs following d-flow. The findings indicate that TERF2IP SUMOylation plays a role in the SASP and SAS triggered by d-flow and TL damage. The transfer of WT bone marrow into TERF2IP KI mice reduced the atherosclerosis caused by hypercholesterolemia, highlighting the contribution of vascular TERF2IP SUMOylation to the progression of atherosclerosis.
Conclusion: TERF2IP SUMOylation drives TL DNA damage-related NAD+ depletion, while also elevating the expression of genes associated with SASP and SAS and contributing to the development of atherosclerosis induced by d-flow.
Poster No. 15
Abstract No. 1773749
Effect of optimal medical therapy: Best-Cli trial
1Frederik Meijer Heart and Vascular Institute; 2Brigham’s and Women; 3Boston University; 4UT, Southwestern; 5Mass General; 6Dartmouth; 7UNC; 8Harvard University
Background: The use of guideline-directed optimal medical therapy (OMT) is considered a cornerstone of treatment in patients with chronic limb threatening ischemia (CLTI). The Best Endovascular vs Best Surgical Therapy in Patients with CLTI (BEST-CLI) compared revascularization strategies in patients with CLTI. In this pre-specified post hoc analysis, we studied the effect of OMT intensity on the outcomes of patients with CLTI.
Methods: A multispecialty committee defined OMT criteria during the trial design. OMT included metrics that each received 1 point: hypertension management, lipid-lowering and anti-platelet medication use, and tobacco cessation. Patients were stratified by OMT scores from 0 to 4. OMT scores were assessed for the duration of the trial. The association of Major Adverse Limb Events (MALE), Major Adverse Cardiovascular Events (MACE), and death were examined.
Results: A total of 1830 patients were enrolled between August 2014 and October 2019. At baseline, patients had OMT 0=2%, OMT 1=11%, OMT 2= 24%, OMT 3=38%, and OMT 4= 25%. Significant differences were present at baseline for patients with OMT 0/1 vs. OMT 4 including age (OMT Score 0/1, 64.1±9.8 years vs. OMT Score 4, 69.6±9 years, P < .001), current smoking (74.4% vs. 0%, P<.001) and ankle-brachial indices (0.49±0.23 vs. 0.65±0.39, P < .001). Approximately, 30% of patients in aggregate had an OMT score of 4 and 40% of patients had an OMT score of 3 during 60 months of followup. The use of statins (73.9% vs. 80.6%, p <.0001), any antiplatelet (74.5 vs. 88.7%, p <.0001), dual antiplatelet therapy (18.1 vs. 39.5%, p <.0001) and direct oral anticoagulant (4.4 vs. 7.8%, p <.0001) increased from baseline to 30 days. Patients with OMT ¾ at baseline were independently associated with a significant decrease in MALE (HR 0.74, 95% CI 0.57,0.96; p=0.023) and CEC confirmed major intervention (HR 0.73, 95%CI 0.54, 1.00; p=0.051). Increased OMT score did not influence MACE or survival in patients undergoing either endovascular or open revascularization.
Conclusion: OMT remains highly variable in patients with CLTI but improves early in a trial environment. Higher levels of OMT reduces the risk of MALE and major reintervention in patients undergoing revascularization.

Multivariable Cox regression Models.
Poster No. 16
Abstract No. 1788118
Livedoid vasculopathy evaluation in hemoglobinopathy-associated chronic leg ulcers
1University of North Carolina Chapel Hill School of Medicine
Background: Hemoglobinopathy associated chronic leg ulcers (HACLU) are poorly understood and difficult to treat. Livedoid vasculopathy (LV), a non-inflammatory thrombotic vasculopathy, has been reported in HACLU. We assessed the frequency and outcomes of workup for secondary causes of HACLU such as LV.
Methods: UNC Health System electronic medical record data were queried for patients with HACLU. Hemoglobinopathy diagnosis, chronic leg ulcers, and comorbidities were confirmed by manual chart review.
Results: 89 patients with sickle cell disease-HACLU were identified. Ten (11%) had undergone skin biopsy compared with 19% of those with trait. Seven biopsies were non-specific, two showed venous stasis, and one showed LV. Also, 19 patients with thalassemia-HACLU were identified. Two of these patients (12%) underwent skin biopsy and both biopsies showed venous stasis. DVT history was present in up to 36% of HACLU patients compared to 19% of those with sickle cell trait.
Conclusion: Skin biopsy is rarely performed in HACLU and most findings are non-specific. However, reports of LV in HACLU and the high prevalence of deep vein thrombosis (DVT) may suggest that thrombosis plays a role in HACLU. The role of anticoagulation in HACLU treatment remains unclear but needs to be investigated.
Secondary workup for hemoglobinopathy associated chronic leg ulceration.

US, ultrasonographic; CVI, chronic venous insufficiency; PAD, peripheral artery disease; DVT, deep vein thrombosis.
Poster No. 17
Abstract No. 1795659
Retinal microvascular changes in fibromuscular dysplasia
1Cleveland Clinic; 2Loyola University
Background: Fibromuscular dysplasia (FMD) is a condition that predominantly affects women, resulting in stenosis, aneurysms, and dissections in small to medium sized arteries. While it is most commonly described in the renal and carotid arteries, more than 50% of patients have multi-vessel involvement. Our understanding of the extent of involvement and association with outcomes is limited by number of vascular beds screened. In this study, we perform retinal imaging in FMD patients to assess the retinal microvasculature.
Methods: We prospectively performed retinal optical coherence tomography (OCT) and OCT angiography imaging using the Optovue Avanti XR on patients with FMD and controls with no known arterial disease. Both 3mm x 3mm and 6mm x 6mm images were captured. Retinal thickness and vascular density maps were compared. Categorical and continuous variables were compared using a Chi-square and Student’s T-test respectively.
Results: A total of 62 eyes of 31 female patients with FMD and 110 eyes of 55 control subjects were included. Average age (60y vs. 62y, p=0.46), prevalence of hypertension (45% vs. 52%, p=0.50) and hyperlipidemia (45% vs. 51%, p=0.61) were similar in the two groups. In patients with FMD, 71% had carotid involvement, 61% had multivessel FMD, 48% had a prior dissection, aneurysm or stenosis requiring intervention and 16% had a history of stroke. Overall retinal superficial vascular density was not statistically different between the two groups. However, central subfield superficial vascular densities were lower in the FMD group vs controls (3x3 17.7 vs 20.4, p=.017; 6x6 20.49 vs 23.63, p=.013). Central subfield retinal thickness measurements were smaller in the FMD group vs controls (3x3 253.82um vs 262.52um; 6x6 253.00um vs 261.94um). Relative thinning was especially seen in the inner retina of FMD patients (3x3 47.98um vs 53.01um p =.016; 6x6 52.85um vs 58.91um, p=.001). Finally, the foveal avascular zones were statistically larger in the FMD group vs control (3x3 0.287mm2 vs 0.232mm2, p <.001; 6x6 0.282mm2 vs 0.226mm2, p<.001).
Conclusion: Patients with FMD have subclinical retinal changes with smaller superficial vascular densities in the central subfield area, thinner inner retinas, and larger foveal avascular zones.
Poster No. 18
Abstract No. 1795719
Prospective evaluation of novel dynamic compression for phlebolymphedema
1Stanford University School of Medicine; 2NYU Langone Medical Center; 3University Surgical Associates; 4Weill Cornell Medicine
Background: Chronic edema is a pervasive medical problem impacts outcomes and quality-of-life and poses significant financial burden. The most common adjunctive treatment options include compression devices. Existing pneumatic devices require a power outlet, obligating patient immobility during treatment, and treatment adherence is poor. A novel non-pneumatic compression device (NPCD or Koya Dayspring®), with a portable battery, enables patient ambulation and mobility, thereby potentiating synergism with the extrinsic muscle pump. The NPCD utilizes a smart metal that dynamically stimulates the superficial lymphatics in conjunction with the applied, active compression. The NPCD has been developed to address the current unmet needs of this disease in a multimodal approach. This study aims to understand methodology that optimizes responses and adherence to dynamic compression therapy in phlebolymphedema.
Methods: This prospective, single crossover, multi-center study enrolled subjects with phlebolymphedema to receive, in a randomized order, either the Non-Pneumatic Compression Device (NPCD) or the Advanced Pneumatic Compression Device (APCD). After12 weeks of daily self-treatment and a 4-week wash-out period, there was crossover to the alternate device with an identical protocol.
Results: Seventy-one (71) subjects completed the study, of which 35 had phlebolymphedema and are presented here. Mean limb volume reduction was 424.4.9 ± 100.9 mL in the NPCD cohort and 50.8 ± 112.1 mL in the APCD cohort. Improvement in overall Quality of Life (LYMQOL) was 1.39 ± 0.39 points (NPCD) and 0.18 ± 0.29 ( APCD), respectively. Treatment adherence was 81 ± 6.5% ( NPCD) versus 49 ± 4.0% (APCD). Overall, 85% of participants preferred the NPCD. No AE/SAEs occurred with either device.
Conclusion: The inherent challenges in the effective management of chronic edema/lymphedema warrant innovation for usability, outcomes, and patient satisfaction. Incorporation of this novel NPCD in the management of chronic edema due to CVI, lymphedema (primary or secondary), or phlebolymphedema has demonstrated improved outcomes, greater adherence to use due to its design for mobility, and enhanced patient preference compared to traditional management strategies.
Poster No. 19
Abstract No. 1795385
Machine learning classification of carotid plaque using ultrasound
1Cleveland Clinic
Background: Carotid plaque tissue was classified by machine learning using ultrasound (US) intensity and spectral information. We aim to non-invasively classify carotid plaque tissue.
Methods: Backscattered US radiofrequency (RF) data from carotid plaque were acquired in vivo prior to carotid endarterectomy for 134 subjects. Excised plaques were histologically processed. A balanced data set of 1200 fibrous, calcium and hemorrhagic and/or necrotic core (HNC) regions of interest (ROIs) were selected from the RF data corresponding to homogenous regions within the histology. US parameters extracted from each ROI were provided as inputs into a random forest that was trained using the matched histology. Three random forest algorithms were produced: IB from the fundamental spectrum, IB and spectral parameters from the fundamental spectrum, and IB and spectral parameters from both the fundamental and second harmonic bandwidths. Areas under the receiver operating curves (AUCs) were computed.
Results: A combination of IB and spectral parameters using both the fundamental and harmonic bandwidths provided the greatest AUC (see Figure) when classifying all plaque types and a statistically significant improvement in the HNC AUC: 0.63 (95% CI 0.57 – 0.69) vs 0.56 (95% CI 0.48 – 0.62). The HNC AUC for the fundamental IB and spectral parameters fell in between: 0.59 (95% CI 0.53 – 0.65).
Conclusion: The addition of spectral information and use of the second harmonic bandwidth improves the performance of the machine learning classification of carotid plaque based on ultrasound backscatter compared to using IB alone.

ROC curves of random forest machine learning classifiers.
Poster No. 20
Abstract No. 1777911
Obesity paradox in acute DVT outcomes: national analysis
1Aurora Cardiovascular and Thoracic Services, Aurora Sinai/Aurora St. Luke’s Medical Centers, Aurora Health Care
Background: Obesity is a well-established risk factor for cerebrovascular disease. However, some studies reported paradoxical survival benefits associated with obesity. A large-scale analysis of the effect of obesity on inpatient outcomes of acute deep vein thrombosis (DVT) is unknown.
Methods: The 2020 National Inpatient Sample (NIS) was used to identify all admissions with a primary discharge diagnosis of Acute DVT using International Classification of Disease, tenth revision, Clinical Modification. Similarly, the presence of obesity was identified as the group of interest. The primary outcome of interest was in-hospital mortality, and secondary outcomes included length of stay (LOS) and total hospital charges.
Results: Among 478,399 acute DVT-related admissions, 112,814 (23.5%) had a secondary diagnosis of obesity. The group with obesity was younger than non-obese (mean of 60.5 vs 63.3 years, P< 0.001) and had a lesser percentage of females (13% vs 35%, P< 0.001). The in-hospital mortality rate in the entire cohort was 6%. The odds of mortality were lower in the obesity group on both unadjusted (0.70, P< 0.001) and risk-adjusted (0.52, P< 0.001) analyses. The mean LOS and total charges were also less in the obesity group (Table 1).
Conclusion: Obesity is associated with a better short-term prognosis in patients with acute DVT. Future studies are needed to examine the long-term outcomes and pathophysiology behind this phenomenon.
Univariate and multivariate regression of outcomes of acute DVT.

Poster presentations
Poster No. 21
Abstract No. 1788327
Endothelial JAK/STAT, mixed-lineage-leukemia-1, IRAK1/4 axis mediates SARS-CoV-2 coagulopathy
1University of Michigan
Background: Endotheliitis and immunothrombosis are hallmarks of severe SARS-CoV-2 (CoV2) infection. Endothelial-leukocyte interactions, cellular adhesion molecules (CAM), and procoagulant mediators (PCM) augment immunothrombotic risk. We hypothesize chromatin modifying enzymes (CME) associated with NF-kB signaling drive transcriptional changes leading to a prothrombotic phenotype.
Methods: Public human scRNA sequencing evaluated pulmonary endothelial epigenetic transcriptome (PMID34876692). Murine venous Ecs (mVEC), EOMA cells, and human venous Ecs (HUVECs) were treated with murine beta-coronavirus (MHV-A59) or CoV2 spike protein. Pharmacologic and/or siRNA inhibition was used to accomplish MLL1, JAK/STAT, and IRAK silencing.
Results: Human pulmonary Ecs in fatal CoV2 had increased KMT2/MLL histone methyltransferases. mVEC infection increased transcription of CME kmt2a, CAMs, and PCMs. H3K4 methylation and MLL1 were enriched on promotors of identified genes. MLL1 inhibition reduced CAM and PCM transcripts and monocyte-EC adhesion. JAK/STAT inhibition abrogated the induction of CAMs and IRAK inhibition exacerbated the induction of CAMs.
Conclusion: Kmt2a/MLL1 positively regulates CoV-2 induction of CAMs and PCMs, endothelial inflammation, and resultant EC-IC interactions. JAK/STAT promotion and IRAK1/4 degradation appear to regulate MLL1 levels. MLL1 may represent a novel target to ameliorate immunothrombosis in CoV-2 infection.

Induction of endothelial MLL1 and downstream cellular adhesion molecules in coronavirus infection.
Poster No. 22
Abstract No. 1787980
10-year clinical outcomes of in-hospital cancer-associated thrombosis
1Davao Doctors Hospital
Background: Cancer remains a major risk factor to develop cancer-associated thrombosis (CAT). Epidemiological data support the role of race and ethnicity in thrombogenicity of malignancy. CAT is less studied in Asia, wherein Philippines has no registry of cancer patients admitted due to venous thromboembolism (VTE). This study aims to determine demographic profile, clinical outcomes, and risk factors for unfavorable outcomes in patients admitted due to VTE.
Methods: Patient data from January 2013 to December 2023 were retrieved from electronic hospital registry coded using the International Classification of Disease, Tenth Revision-Clinical Modification (ICD 10-CM). Demographic profile, clinical outcomes and risk factors for unfavorable outcomes were determined using inferential statistical analysis and logistic regression.
Results: Our study identified 3558 patients with both solid and hematologic malignancy, where 55 patients had VTE. The prevalence rate was 2.9% with incidence rate of 15 per 1000-person years-the latter being higher than established Asian studies. Age (p< 0.05, Cramer’s V of 035) and symptoms of dyspnea, shortness of breath, leg pain and chest heaviness (p< 0.001, Cramer’s V of 0.43-0.64) were statistically significant risk factors and had moderate to strong association for admission due to VTE. Meanwhile, those who do not report dyspnea and chest heaviness had higher odds (B=2.91, p< 0.01, r2=0.15) of developing VTE. VTE-related unfavorable outcomes developed in 60% of patients while 30-day all-cause mortality was 14.5%. Furthermore, SBP < 90mmHg (p=0.0, X² = 7.88, Cramer’s V of 0.38) and respiratory rate ⩾24/min (p=0.01, X² = 7.84, Cramer’s V of 0.37) were both statistically significant and had moderate association for unfavorable outcomes. Those who do not disclose dyspnea and chest heaviness had higher likelihood (B=2.22, SE=1.12) of unfavorable outcomes but p-value was 0.05 only marginally significant. This imply further studies are needed to confirm the role of clinical manifestations in risk assessment.
Conclusion: Presence of symptoms along with hemodynamic instability warrant aggressive intervention to improve unfavorable outcomes in-hospital. These findings may help identify gaps in implementation of risk stratifications and role of thromboprophylaxis to prevent in-hospital admissions and consequently improve clinical outcomes.
Poster No. 23
Abstract No. 1795759
Reversal of heart failure: role of vascular recovery
1Houston Methodist Research Institute; 2Boston Children’s Hospital; 3Houston Methodist
Background: Clinically, unloading of the LV in heart failure (HF) using a left ventricular assist device (LVAD) can lead to the increased endothelial density, reduced fibrosis, and improved cardiac function. However, the mechanisms of these processes are not understood. We hypothesize that reversal of heart failure after LVAD is a vascular recovery driven by cell fate plasticity and mesenchymal to endothelial transition (MendoT).
Methods: We compared histologic and cellular properties along with sequencing studies of pre-LVAD (HF) and post-LVAD cardiac tissues. In parallel, we utilized our murine model of non-ischemic heart failure and recovery (HFR) which emulates the recovery observed after LVAD unloading. We leveraged tamoxifen inducible fibroblast lineage-tracing mice (Col1a2-creERT2:R26RtdTomato), to track potential cell fate transitions.
Results: We observed decreased cardiac fibrosis and increased capillary density in post-LVAD compared to pre-LVAD hearts. The snRNAseq revealed a fibroblast subtype capable of MendoT. Isolated non-myocytes from postLVAD were more proliferative with an angiogenic phenotype. Murine model of HFR replicated the increase in capillary density and reduced fibrosis via bead perfusion study. Lineage tracing studies confirmed that MendoT contributed significantly to the increased vascular volume during HFR.
Conclusion: Thus, recovery from HF is associated with, and possibly driven by a microvascular recovery. This new paradigm for HFR may provide a novel therapeutic approach for HF treatment.

A: Isolated cardiac non-myocytes from post-LVAD hearts proliferate faster compared to pre-LVAD. B: Pseudo-time trajectory analysis shows an endothelial cell (EC) to fibroplast (FB) and a FB to EC path in pre- and post-LVAD cells, respectively. C: Increased vascular density in HFR mice compared to HF. D: Angiogenic transdifferentiation during HFR visualized by confocal imaging. E: Angiogenic transdifferentiation during HFR quantified by flow cytometry.
Poster No. 24
Abstract No. 1795782
Clinical outcomes of isolated calf vein thrombosis
1St. Luke’s Medical Center Global City; 2St. Luke’s Medical Center
Background: The significance of isolated calf deep vein thrombosis (ICDVT) remains unclear with the current guidelines not being based on strong level of evidence. Given the uncertainties, the therapeutic approaches vary among institutions; hence, it is prudent to look at the existing experience of an institution where examination of the calf veins is routinely done during venous duplex ultrasound of the lower extremities. We aim to determine the clinical features of patients with isolated calf deep vein thrombosis on venous duplex scan and identify which factors are associated with clinical outcomes.
Methods: Using a retrospective cohort design, this study investigated the clinical outcomes of patients with ICDVT at a single tertiary center in a span of five years. The association of certain factors with the clinical outcomes was determined using logistic regression analysis.
Results: One hundred fifty-one subjects were included in the study. Most of the subjects (36.42%, 95% CI: 28.75-44.64%) had stabilization of ICDVT. Resolution was noted in 35.76% (95%: CI: 28.14-43.96%). Recurrence occurred in 15.89% (95% CI: 10.46-22.72%) while proximal DVT extension only occurred in 10.60% (95% CI: 6.18-16.64%) of the subjects. Only two subjects developed pulmonary embolism. None of the factors studied (recent surgery, leg varicosities, in-patient status, active cancer, and therapeutic management) were significantly associated with proximal DVT extension, recurrence, pulmonary embolism and ICDVT stabilization. When it comes to resolution, only therapeutic management was found to have a significant association. Those who were anticoagulated had about four times higher odds of resolution than those managed conservatively.
Conclusion: This study demonstrated that previously cited risk factors do not play a role in the development of ICDVT complications in this population. While anticoagulation contributes significantly to the resolution of ICDVT, this study suggests that it can safely be managed conservatively with no significant effect on proximal DVT extension, recurrence, or pulmonary embolism.
Poster No. 25
Abstract No. 1788088
Circular telomerase messenger RNA reverses endothelial senescence
1Houston Methodist Research Institute; 2Houston Methodist
Background: Hutchinson-Gilford Progeria Syndrome (HGPS) is caused by a mutation in LaminA (Progerin), and is characterized by accelerated aging, and death from coronary or carotid disease in the mid-teens. Vascular smooth muscle cells (VSMCs) and endothelial cells (Ecs) derived from HGPS children manifest many of the hallmarks of aging including telomere erosion, reduced proliferation, impaired function, DNA damage and senescence markers, altered cellular and nuclear morphology, and an aberrant transcriptional profile. These hallmarks of aging are substantially reversed by treatment with linear mRNA telomerase (TERT), with greater benefit in HGPS cells than the current therapy, lonafarnib. However, linear mRNA has a short half-life, which necessitates frequent administration. By contrast, circular (circ) RNA with an internal ribosome entry site can be translated into protein and is more stable than linear mRNA. We hypothesized the circ RNA hTERT would provide for longer duration of telomerase expression and would have a greater benefit for HGPS.
Methods: By comparison to Ecs from their unaffected parents, Ecs derived from HGPS patients manifested advanced senescence. HGPS Ecs were treated with linear or circ hTERT mRNAs.
Results: We found that at day 28 after treatment, the benefit of circ hTERT exceeded that of linear hTERT in all measured variables. Circ RNA TERT provided for greater telomere length as determined by quantitative fluorescence in situ hybridization; induced a three-fold greater reduction in beta-gal positive cells, and in cells with morphologically aberrant nuclei. In HGPS Ecs, circ RNA hTERT provided for a three-fold greater reduction of senescent markers, inflammatory markers, and DNA damage markers, including Progerin, p16, p21, IL-1B, IL-6, IL-8 MCP-1, gH2A.X and 53bp1. In addition, circ hTERT mRNA restored NO production, promoted cell proliferation as assessed by Ki-67, enhanced angiogenesis in tube formation assay and LDL uptake to a greater degree. Circ hTERT RNA was also more effective in reducing mitochondrial ROS as assessed by MitoSOX and normalizing mitochondrial membrane potential as assessed by JC-1 staining.
Conclusion: Circular RNA hTERT is more effective than linear hTERT, possibly because of its longer half-life. Circular RNA hTERT is a promising therapy for HGPS and other disorders associated with accelerated vascular aging.
Poster No. 26
Abstract No. 1787974
10-year single-center descriptive cross-sectional study on renal artery stenosis (RAS)
1St. Luke’s Medical Center Global City; 2St. Luke’s Medical Center
Background: Atherosclerosis is the most common cause of renal artery disease. In population-based studies in the United States, up to 6.8% of healthy people, 65 years and older were diagnosed with renal artery stenosis (RAS). Currently there is a paucity of local data regarding the prevalence, clinical profiles, and sonographic patterns of patients with RAS.
Methods: This is a 10-year single-center, descriptive, cross-sectional study on the clinical profiles and renal duplex sonographic findings of patients with renal artery stenosis (RAS) at St. Luke’s Medical Center Global City, Philippines. This study involves patients with RAS who underwent renal duplex scan at St. Luke’s Medical Center – Global City from June 2012 to June 2022.
Results: A total of 963 patients were included. There were 875 (90.86%) patients who had normal renal duplex scan and 67 (6.96%) were found to have RAS. This was seen in female patients, with increasing age, hypertension, and renal impairment. Among the risk factors studied, hypertension and diabetes appeared mostly in this study population. Furthermore, a decreased in eGFR was found in the majority of patients with RAS. Majority had stenosis in the proximal to mid segments of the renal artery. This suggested a pattern of atherosclerotic renal artery involvement which typically involves the ostium and/or proximal one-third of the renal artery.
Conclusion: The overall prevalence of RAS over a period of 10 years was 6.96%. Hypertension is closely associated with RAS, appearing both as a risk factor and a possible clinical manifestation of the disease. Atherosclerotic RAS as a cause of kidney dysfunction and end-stage kidney disease is being increasingly recognized and a decreased eGFR as an independent risk factor for RAS should be considered. The best Doppler criterion for diagnosis of RAS seen in post renal transplant patients is a stenotic renal artery PSV that is 13 times higher than that of an interlobar artery. This was likewise observed in this study involving native kidneys in patients with renal duplex scan findings that are highly suggestive of >60% RAS.
Poster No. 27
Abstract No. 1788019
Histological analysis of severe Marfan mouse model
1Johns Hopkins School of Medicine
Background: Map2k6 and Mmp17 have been identified as modifier genes that are linked to severe aortic disease in the Fbn1C1039G/+ mouse model of Marfan Syndrome (MFS) on a 129S6/SvEvTac background (129 MFS). This study aims to localize expression of these modifier genes in the aortic root of 129 MFS mice and identify changes in MAPK and Smad2/3 signaling that could be driving progression of a severe aortic phenotype.
Methods: Hematoxylin and eosin staining was used to assess gross morphological changes within the aortic root. Mason’s trichrome staining enabled visualization of collagen deposition and extracellular matrix (ECM) composition in the aortic root. Immunofluorescence (IF) and RNAscope in situ hybridization (ISH) were performed in combination with confocal microscopy to localize expression of the modifier genes, MAPK, and Smad2/3 signaling pathways within aortic root cell populations.
Results: 129 MFS mice display marked thickening of the aortic root wall and striking accumulation of both cellular and ECM components by 2 months of age relative to both BL6 MFS mice and WT littermates on both backgrounds. Notably, these histological features are normalized in 12-month 129 MFS mice that are homozygous for a null allele of either one or both modifier genes. Smad2/3 and pp38 activation are increased throughout the aortic root in 129 MFS mice. In contrast, Erk1/2 and Pkc activation are elevated in distinct, mutually exclusive cell populations that are selectively present in the aortic root of 129 MFS animals. Map2k6 expression colocalizes predominantly with pErk1/2-positive cells, while Mmp17 expression colocalizes with a subset of pPkc-positive cells.
Conclusion: Histological analyses reveal early accumulation of a novel population of cells that is selectively present in the aortic root of 129 MFS mice. We herein show that both modifier genes Map2k6 and Mmp17 are expressed in this disease-specific cell population and confirm their colocalization with activated MAPK signaling. Knockout of each modifier gene rescues both aortic root aneurysm growth and the aforementioned histological changes, indicating a causal role for each gene in aortic root aneurysm pathogenesis in 129 MFS mice.
Poster No. 28
Abstract No. 1788220
Immunocheckpoint inhibitor specifically accelerates coronary atherosclerosis not aorta
1University of Texas MD Anderson Cancer Center; 2Escuela de Medicina y Ciencias de la Salud, Tecnológico de Monterrey; 3Houston Methodist Research Institute
Background: ICIs are a cornerstone in cancer immunotherapy. Unfortunately, ICI-associated coronary artery disease (IACAD) poses a significant challenge.
Methods: C57BL/6 mice were treated with AAV-PCSK9 and fed a high-fat diet (HFD) for 8 weeks. At 4 weeks of HFD feeding, transverse aortic constriction (TAC) was performed. Anti-PD-1, and a control IgG were administered by IP. All mice were assigned into three groups: IgG control (n = 8), low-dose anti-PD-1 (low-PD1, n = 9), and high-dose anti-PD-1 (hi-PD1, n = 7). The low-PD1 was treated with 250 µg of anti-PD-1 twice, two days before and after TAC surgery, for a total of 500 µg. In addition to 500 µg of anti-PD-1, the hi-PD1 was treated with biweekly 100 µg for three weeks, totaling 1,100 µg. Echocardiography and histological analysis were performed. We aimed to establish a mouse model to investigate the underlying mechanisms of IACAD.
Results: The fractional shortening (FS) was lower (11.80 ± 7.8 vs. 28.06 ± 8.95 %, p = 0.0009), but the left ventricular mass was bigger in hi-PD1 than those in IgG control (125.8 ± 21.68 vs. 207.5 ± 49.05, p = 0.0004), suggesting that hi-PD1 accelerated both heart failure and hypertrophy after TAC. The clear pericarditis (2/7) and myocarditis (1/7) were observed in hi-PD1 group only. The left anterior descending artery (LAD) stenosis with atherosclerosis (0.0117 ± 0.04 vs. 0.2275 ± 0.19, p = 0.0001) and wall thickness (0.1117 ± 0.01 vs. 0.1450 ± 0.02, p = 0.0053) were significantly increased in hi-PD1. Enhanced perivascular fibrosis with infiltrating cells was observed in the hi-PD1 group, whereas interstitial fibrosis did not show a comparable rise. Lastly, atherosclerosis was found at the proximal section of the TAC site affecting the ascending aorta and right carotid artery in both the IgG and hi-PD1 groups. However, there was no observed difference in the size of the lesions between the two groups.
Conclusion: Administration of ICIs has been correlated with an increase in CAD risk by more than four times, although their impact on peripheral artery disease remains indistinct. According to our model, anti-PD-1 treatment was found to exert more detrimental effects on the coronary arteries compared to the aorta and carotid arteries, attributable to the higher cardiac tissue affinity of anti-PD-1.
Poster No. 29
Abstract No. 1795616
RNA-based therapy for familial hypercholesterolemia
1Houston Methodist Research Institute; 2Houston Methodist
Background: Familial hypercholesterolemia (FH) is the most prevalent genetic disease often caused by defective low-density lipoprotein (LDL) receptor (LDLR). LDLR is responsible for hepatic uptake of LDL cholesterol and its clearing from the circulation. Lack of functional LDLR elevates LDL cholesterol in serum and increases the risk of cardiovascular diseases. The pharmacotherapy of the available treatments to reduce cholesterol, such as statins and PCSK9 inhibitors, is not always effective in FH patients, especially in homozygous FH variants. We aim to develop a novel mRNA-based gene therapy to overcome limitations and potentiate the therapeutic efficacy of currently available treatments.
Methods: LDLR mRNA and GFP (reporter gene) constructs – designed and manufactured by RNAcore to replace defective LDL receptor. Cell line: HepG2 human hepatocytes. mRNA expression/functionality: Western Blot- LDLR expression Flow cytometry – cellular LDL uptake Delivery systems: Two lipid nanoparticles (LNP), namely LNP#1 and LNP#2, with different lipid composition were designed and tested to assess their efficacy in delivering GFP mRNA to hepatic cells lacking LDLR. LNP were fluorescently labeled (red). mRNA LNP uptake and mRNA expression: Fluorescent intensity of red (LNP) and green (mRNA expression) signals was assessed hourly for 24 h by Incucyte. A set of lovastatin (LOV)-treated cells was also transfected with GFP mRNA-LNPs to determine the dependency of LNP uptake on LDLR-mediated endocytosis.
Results: Western blot analysis confirmed the expression of LDLR protein from LDLR mRNA constructs 24 h after transfection. Moreover, LDLR mRNA-treated cells demonstrated a significantly higher uptake of LDL. Ionizable lipids formulation was much more effective in delivering RNA to the hepatic cells than cationic lipids formulation. However, we found higher GFP expression with stimulated cells to express LDLR.
Conclusion: Our data provide proof of concept for further development and translation of the proposed highly required mRNA therapy to the clinic. The next step will be to assess proposed therapy’s effectiveness and short-term safety in the FH animal model.
Poster No. 30
Abstract No. 1775484
Prevalence of PAD in chronic kidney disease (CKD) using post-6MWT ABI
1Perpetual Help Medical Center Binan Laguna; 2Philippine Heart Center
Background: This study aims to determine the prevalence of lower extremity arterial disease (LEAD) among patients with no symptoms of intermittent claudication using ankle-brachial (ABI) at rest and ABI after 6-minute walk test (6MWT) in the out-patient department of hospitals in Binan, Laguna
Methods: This is a cross-sectional study that determined the prevalence of LEAD diagnosed by measurement of the resting ABI and ABI after 6MWT among CKD patients with no symptoms of intermittent claudication in the out-patient department in the hospitals in Binan Laguna. The patients’ demographics, co-morbidities, laboratory results and the prevalence of LEAD were noted. Descriptive statistics was used to summarize the demographic and clinical characteristics of the patients. Frequency and proportion were used for categorical variables, median and inter quartile range for non-normally distributed continuous variables, and mean and SD for normally distributed continuous variables. STATA 13.1 was used for data analysis.
Results: Patients who had LEAD were mostly males, 15-pack year smokers who had hypertension and/or diabetes mellitus type 2. Patients with LEAD were mostly at CKD stage G2 and A2. Among these patients without symptoms of lower extremity intermittent claudication who initially had normal resting ABI, 10.47% were found to have LEAD after a 6MWT. Most of the patients who were found to have LEAD were male.
Conclusion: The prevalence of LEAD with a normal ABI at rest and abnormal ABI after a 6MWT is 10.47%. The ABI after a 6MWT did not increase the detection of LEAD and it did not unmask LEAD in CKD patients.

CKD Stage of participants with normal resting ABI and abnormal ABI after 6MWT.
Poster No. 31
Abstract No. 1787166
Ctsk & Slc25a53 in TLR9-induced endothelial senescene-associated secretory phenotype after ionizing radiation
1University of Texas MD Anderson Cancer Center; 2Houston Methodist Research Institute
Background: Toll-like receptor 9 (TLR9) inhibition has been shown to offer protective effects against endothelial dysfunction triggered by cancer therapy. However, the role of TLR9 in atherosclerosis is contentious. Our research aims to clarify the role and investigate the molecular mechanisms by which inhibiting TLR9 in Ecs may prevent SASP following IR.
Methods: To determine the precise function of TLR in Ecs, we utilized mice engineered with a tamoxifen-inducible, EC-specific TLR9 knockout (TLR9-EKO). We isolated lung endothelial cells from both wild-type (WT) and TLR9-EKO mice after exposing them to a 2 Gy dose of IR and performed RNA-seq.
Results: In an Ingenuity Pathway Analysis to compare Ecs from TLR9-EKO mice and WT mice following IR exposure, as well as comparing irradiated and non-irradiated Ecs from WT mice, we identified 46 significant genes. The analysis revealed three primary pathways affected: there was a downregulation of the ‘Kinetochore Metaphase Signaling Pathway’ and the ‘Cell Cycle Control of Chromosome Replication’ in the comparisons made. Conversely, there was an upregulation observed in the ‘Cell Cycle: G2/M DNA Damage Checkpoint Regulation Pathway”. The findings indicate that TLR9 may play a critical role in modulating the balance between cell proliferation and the DNA damage response following exposure to IR. Cathepsin K (Ctsk) was identified as one of the top five genes significantly upregulated by IR and was notably downregulated following TLR9 depletion, which is essential for moderating IR-induced inflammation. Additionally, Slc25a53, a mitochondrial NAD+ transporter, showed decreased expression due to IR and a subsequent reversal with TLR9 depletion. This IR-specific downregulation, not observed with other cytokine stimuli, attenuates a nuclear-mitochondrial feedback loop that exacerbates SASP in Ecs.
Conclusion: Our research indicates that activation of TLR9 in Ecs increases Ctsk and decreases Slc25a53 expression following IR, an effect not replicated by cytokine stimulation. This concurrent elevation of Ctsk and downregulation of Slc25a53 in Ecs contributes to SASP induced by TLR9 activation.
Poster No. 32
Abstract No. 1785128
Telomerase-mRNA therapy: a protective strategy against radiation-induced cellular-damage
1Houston Methodist Research Institute; 2Houston Methodist
Background: Aging is closely linked to diminished tissue regeneration capabilities, primarily due to an increase in senescent cells, including endothelial cells (Ecs). These cells display shortened telomeres and DNA damage, leading to a loss of proliferative capacity and adverse effects on surrounding cells via cytokines and chemokines. Persistent senescent cell accumulation impedes tissue repair and promotes fibrosis, contrasting with the beneficial role of transient senescence in wound healing. We have previously shown that telomerase (TERT) mRNA therapy not only reduced DNA damage but also mitigated many senescence markers in iPSC-derived Ecs from patients with Hutchinson-Gilford Progeria Syndrome. We hypothesize that TERT mRNA therapy can repair genomic DNA damage, thereby enhancing tissue repair and regeneration post-radiation.
Methods: Adult human skin or various skin cell types are transfected with either GFP or TERT mRNA 24 hours before being exposed to 5 or 10 Grays of radiation. Skin explants are then collected at different time points post-radiation to assess markers of senescence and inflammation, in addition to the Ki67 proliferation marker and telomere length. Genomic DNA repair is quantified using long-range amplification analysis on total DNA from human epidermal keratinocytes, dermal fibroblasts, and dermal microvasculature endothelial cells.
Results: In skin explants, exposure to radiation at levels of both 5 and 10 Gy resulted in increased levels of γH2AX, p21, and p16. However, micro-needling with hTERT mRNA encapsulated in lipid nanoparticles, as opposed to GFP mRNA, led to a reduction in DNA damage and senescence markers while simultaneously enhancing mitochondrial functions. Cultured cells pre-treated with TERT mRNA exhibited similar benefits in DNA damage recovery post-radiation. Notably, no changes in telomere length were observed at 2 and 24 hours post-radiation in any samples, regardless of treatment, which suggests a non-telomeric function of TERT in providing protection against radiation.
Conclusion: Our findings indicate TERT mRNA therapy may reduce genomic DNA damage from aging or radiation, offering a potential avenue for rejuvenating human tissues and enhancing regenerative capacities.
Poster No. 33
Abstract No. 1796183
TLR4 signaling disruption impairs thrombolysis independent of monocytes
1University of Michigan
Background: Absence of TLR4 signaling decreases Venous Thrombosis (VT) resolution. Elevated leukocyte TLR4 expression in the acute/chronic VT transition suggests Mo/Mϕ TLR4 signaling in thrombus clearance.
Methods: Wild type, Tlr4-/-, LysMcre+/-Tlr4fl/fl mice underwent VT via IVC stasis at 4/7/14d, thrombus size assay/flow cytometry analysis of subtypes. Murine blood stimulated with TLR2/4 agonists underwent HALO assay of thrombolytic potential. Immunohistochemistry was performed for cellular infiltrate. Fibrinolytic mediator expression was quantified in splenic/bone marrow Mϕs.
Results: TLR4 cell surface expression was elevated in thrombi CD11b+/Ly6C- Mo/Mϕ. 4d stasis Tlr4-/ mice saw impaired thrombus clearance. Blood thrombolysis increased with TLR4 agonism (MPLA) in Cre- vs Cre+ mice. Efficiency restored upon TLR2/4 agonism (LPS). Circulating Mo/Mϕs in Cre+ mice saw decreased Urokinase/MMP9 expression, and bone marrow Mϕs in Cre+ thrombosed mice saw decreased Urokinase/MMP9 protein levels. No difference in thrombus weight or Mo infiltrate into the thrombus was observed (Fig. 1).
Conclusion: Mo/Mϕ TLR4 signaling loss alters induction of fibrinolytic/matrix remodeling gene expression. TLR4 agonism increased blood thrombolysis in Cre- but not Cre+ mice. Further TLR2 agonism in Cre+ mice restored activity, indicating a TLR2-related compensatory pathway responsible for the static in vivo phenotype in LysMCreTlr4 mice. Further research of this mechanism could provide an alternate pathway for targeting VT resolution.

Poster No. 34
Abstract No. 1796177
Calf pump function versus chronic venous insufficiency severity
1Mayo Clinic
Background: The calf muscle pump is an understudied contributor of venous return from the lower extremity. No large contemporary study has examined calf pump function (CPF) and its independent link to chronic venous insufficiency and ulcers. This study aimed to investigate the correlation between CMP function and the severity of chronic venous disease (CVD) classified by CEAP.
Methods: Patients referred to the Gonda Vascular Laboratory for venous studies between March 2015, and September 2023 were included. Venous air plethysmography was performed by standard technique, measuring obstruction, and hemodynamic incompetence, and CPF. The clinical component of the CEAP score was evaluated at the study of the study in each limb.
Results: A total of 8404 limbs from 3733 patients underwent venous air plethysmography. The mean age was 61.9 ± 14.8 years and 5245 (62.4%) were females. Limbs were categorized based CEAP classification: C0 (no signs or symptoms of CVD), C1: 345 limbs, C2: 1111 limbs, C3: 1107 limbs, C4: 3414 limbs, C5: 1789 limbs, and C6: 263. Venous obstruction was detected in 3.2% of limbs. The severity of venous incompetence was categorized as normal (44.4%), mild (26.4%), moderate (19.0%), and severe (10.2%). A notable trend of reduced CPF was observed with higher CEAP scores (p < 0.001). Specifically, the proportion of individuals with reduced CPF consistently rose from clinical stages 1 to 6 (Figure). To determine if CPF was an independent risk factor for an active/healed ulcer, a multivariable logistic regression model was performed. After adjustment for age, sex, degree of venous incompetence, and obstruction, reduced CPF was a significant predictor (OR:1.9, CI: 1.6 – 2.3) of active/prior ulcer (C5 or 6).
Conclusion: This study demonstrates that in addition to venous obstruction and incompetence, reduced CPF is an independent contributor to the active/healed ulcers of CVD.
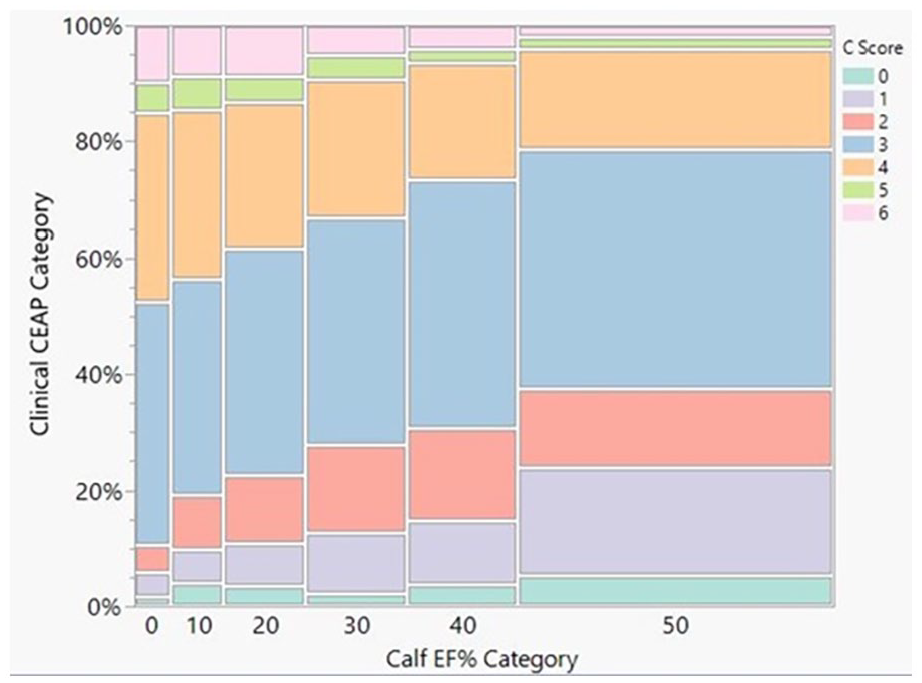
Mosaic plot showing relationship between calf EF% category and clinical CEAP category.
Poster No. 35
Abstract No. 1796220
Secondary prevention improves mortality in high ABI patients
1Harvard Medical School; 2Massachusetts General Hospital
Background: Patients with a high (>1.4) ankle-brachial index (ABI) have mortality comparable to peripheral artery disease (PAD) (ABI < 0.9) and higher than normal ABI (0.9-1.4). It is unknown if the traditional secondary cardiovascular (CV) risk modification is effective in reducing mortality in high-ABI patients.
Methods: Over 400 patients were enrolled in the Limb Evaluation and Preservation Program (LEAPP), a multidisciplinary program at Massachusetts General Hospital focusing on limb salvage. Information on risk factors, coronary artery disease (CAD), cerebrovascular disease (CVD), medication usage, and mortality was obtained via a review of electronic medical records.
Results: 97 patients had high-ABI in at least one limb. Of these, 72% were Men, 74% Caucasian, and 8% African American. The median age was 73 years. The prevalence of hypertension, diabetes, CAD, and CVD was 90%, 72%, 38%, and 35%, respectively. 16% of patients died during the follow-up period of up to 5 years. We found better prescription rates for the CV prevention measures in the LEAPP registry compared to the existing literature. Some individual components did not achieve significance due to low numbers. However, the high-ABI patients with polyvascular disease had higher mortality (OR=3.3, p=0.03), and there was a survival benefit in those on all three cardiovascular medicines (OR=0.3, p=0.02).
Conclusion: The high-ABI patients should also receive aggressive medication therapy for CV risk prevention like PAD patients.
Relationship of cardiovascular disease and secondary prevention measures with mortality.

CAD: Coronary artery disease; CVD: Cerebrovascular disease; ACEI: Angiotensin-converting enzyme inhibitor; Angiotensin receptor blocker;
Poster No. 36
Abstract No. 1797190
Carotid artery web outcomes in asymptomatic patients
1Harvard Medical School; 2Massachusetts General Hospital
Background: Carotid webs are postulated to play a role in patient with cerebrovascular accidents. The significance of carotid web is not fully understood. Although there is no consensus on pathophysiology, stasis, and turbulence in flow along the surface of the web leading to thrombus formation is the suspected culprit in the proposed stroke association. However, this is not widely accepted as there is no robust data available and the relationship is extrapolated from case reports and literature reviews. Similarly, very little, if any, is known about incidental carotid webs noted on imaging and their outcomes in asymptomatic patients. Currently there are no guidelines on surveillance or the optimal management of symptomatic and asymptotic carotid webs. As vascular specialist, it is crucial to attempt understand the implications of these findings to appropriately and safely monitor and/or manage webs.
Methods: We identified adult patients (age >18yrs) with asymptomatic carotid webs on imaging by conducting a retrospective review of data within the Massachusetts General Brigham database.
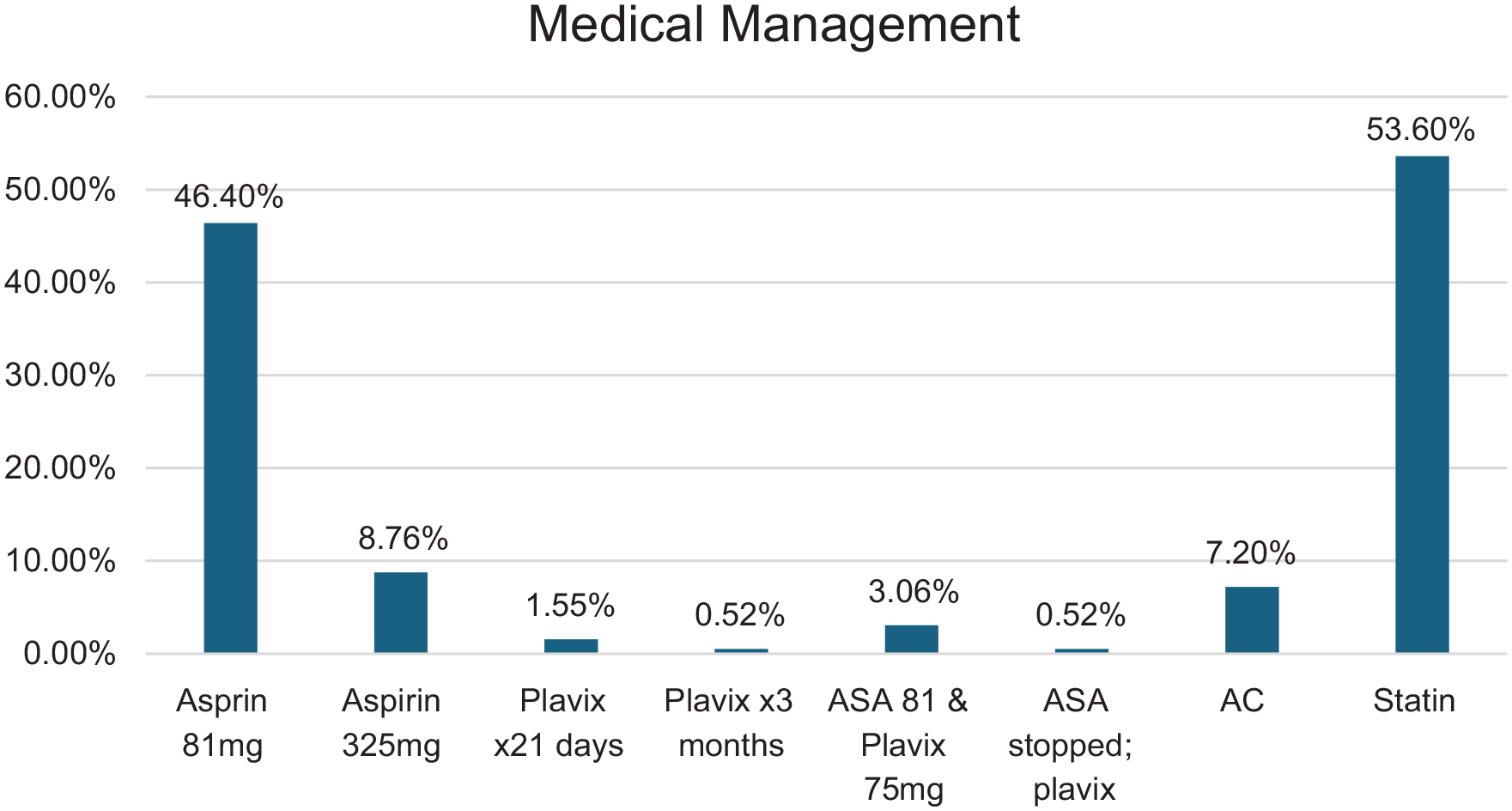
Results: A total of 432 patients were identified from 1990-2023. Forty five percent (194/432) webs were asymptomatic (see Image 1 for demographic data). 77.8% of webs were identified on Computed Tomography Angiography neck. Carotid artery dissections and atheromas were the most common differentials. 180/194 had unilateral web (R 86; L 94) while 14/194 had bilateral webs. Webs measured from 1mm-8mm in size. Vascular occlusion and thrombosis were not common. 9/194 patients had a recurrent TIA or CVA while another 10/194 experienced recurrent or worsening neurologic symptoms. Overall, most patients were medically management although several web findings were ignored without further evaluation. Approximately 47% of patients had some follow up and 33% had repeat imaging ordered. Anti-platelets and lipid lowering therapy were utilized more than other regimens.
Conclusion: Carotid artery webs are underdiagnosed and underestimated findings and has potential to be a nidus for thromboembolic vascular events. Increased awareness and research are needed to fully understand the long-term outcomes and create optimal management/surveillance guidelines.
Poster No. 37
Abstract No. 1795742
A single-center limb salvage quality improvement initiative
1Houston Methodist
Background: This paper aims to outline the process and present initial outcomes of a local quality improvement initiative focusing on length-of-stay (LOS) and 30-day unplanned readmissions in peripheral arterial disease (PAD).
Methods: Clinical informaticists, adept in Epic data mining, were tasked with monthly query of our database for PAD patients managed since May 2021and generate an automated report of required variables, eliminating the need for manual chart review. Referencing the top-decile institutions in the Vizient ranking, we set target goals of 7 days for LOS and 11% for 30-day readmission and studied trends in our cohort. To enhance this initiative, we formed a multidisciplinary Limb Salvage Committee (LSC), that met regularly to review monthly reports, propose improvements, which were then communicated to the vascular surgery faculty for feedback and implementation. Monthly outcomes were continuously monitored by the LSC to assess progress and pinpoint areas necessitating further improvement.
Results: Between May 2021 and March 2023, 985 consecutive procedures were performed. The average postoperative LOS was 7±10 days, with 35% not meeting the goal. Patients not meeting the LOS goal often had a history of coronary artery disease or congestive heart failure, initially admitted for non-vascular reasons. The readmission rate was 15%. Recommendations from the LSC included deferring non-urgent revascularization to outpatient care with prehabilitation for at-risk patients, and early follow-up by a nurse practitioner for wound check and pain management. These recommendations were implemented at the end of March 2023. After implementing recommendations, 272 cases recorded between April and July 2023 saw a decrease in patients not meeting the target LOS to 27%, and unplanned readmissions reduced to 11%.
Conclusion: Our limb salvage QI project has proved efficient in monitoring quality metrics and targeting specific areas in need of improvement. Continuous monitoring is necessary to ensure compliance, track outcomes and identify areas in need of further improvement. Future studies will further assess the effectiveness of this process in improving patient care.
Poster No. 38
Abstract No. 1785565
Mortality risk of severe and critically ill enoxaparin-treated COVID-19
1Philippine heart center; 2Makati Medical Center
Background: COVID-19 with blood clotting issues (coagulopathy) is linked to worse outcomes. International guidelines recommend low-dose blood thinners (LMWH) for severe cases due to their anti-inflammatory and anti-clotting effects. However, local data on using blood thinners for COVID-19 patients is limited. This study evaluated if preventive blood thinners (LMWH) improve outcomes in severe COVID-19 patients at a tertiary hospital.
Methods: We studied 70 patients with severe/critical COVID-19 admitted to a tertiary center (March 1 – April 15, 2020). Patients who received preventive or therapeutic LMWH (enoxaparin) were compared to those who didn’t. We assessed bleeding complications, hospital stay length, and mortality/recovery.
Results: Seventy COVID-19 patients (42 received LMWH, 28 did not) were studied. Both groups had similar average age and gender distribution. Most patients in the LMWH group were critical (76.2%), while most in the non-LMWH group were severe (75%). Common underlying conditions were kidney disease (LMWH group) and asthma (non-LMWH group). Key findings include recovery of 54.8% in LMWH group and 45.2% mortality. The LMWH dose has no significant impact on mortality, but shorter duration (6.5 days) in deceased patients. The hospital stay is longer in LMWH group (33 days). Bleeding has minor complications in 16.7% of LMWH group. The blood tests like white blood cells are elevated in LMWH group and D-dimer are elevated in both (higher in LMWH group). Platelets, PT, and PTT are normal in both groups.
Conclusion: This study suggests LMWH anticoagulation may benefit critically ill COVID-19 patients, with over half recovering. LMWH dose did not impact mortality, but deceased patients received it for a shorter duration. Hospital stays were longer in the LMWH group, which had more critical cases. LMWH appeared safe with only minor bleeding complications.
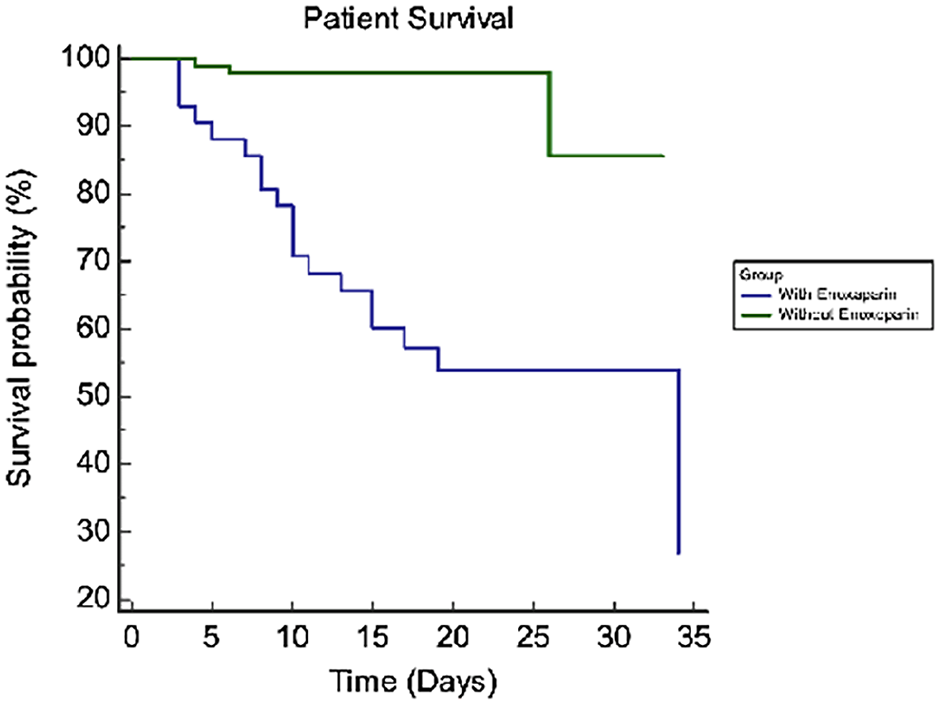
Kaplan-Meier survival curve – all patients.
Poster No. 39
Abstract No. 1786280
The effect of antiplatelet therapy on AAA growth
1Cleveland Clinic; 2Johns Hopkins University; 3University of Cincinnati; 4Washington University
Background: The role of platelet activity in growth and rupture of abdominal aortic aneurysms (AAA) has been described. We previously demonstrated that in our cohort of patients with AAA, aspirin use was associated with reduced rates of AAA growth. However, whether this finding applies to patients on a P2Y12 inhibitor or those on dual antiplatelet therapy is not known.
Methods: In our cohort of patients with at least two abdominal duplex studies between 2010 and 2020, we divided patients into the following categories based on the medications they were prescribed at the time of their first ultrasound: (1) No antiplatelet agent; (2) Aspirin (ASA) only; (3) P2Y12 inhibitor; (4) Aspirin and P2Y12 (DAPT). We built a multivariable model to assess the association between antiplatelet use and fast AAA growth (⩾ 0.5 cm/year). We controlled for age, sex, initial diameter, smoking, hypertension, diabetes, and prior aneurysmal repair.
Results: In our cohort of 2,186 patients, the rates of fast AAA growth were as follows: No antiplatelet: 19.5%; ASA: 15.0%; P2Y12 inhibitor: 23.4%; DAPT: 13.4%. The rates of fast AAA growth were similar between ASA and DAPT (p = 0.614). There was no significant difference between patients not on an antiplatelet agent and those taking a P2Y12 inhibitor (p = 0.305). Patients on aspirin had lower rates of fast AAA growth as compared to those on a P2Y12 inhibitor (p = 0.02). Although there was a signal for reduced rates of fast AAA growth in patients on DAPT, this did not reach statistical significance (p = 0.068).
Conclusion: While aspirin use was associated with reduced rates of fast AAA growth, this perceived antiplatelet effect did not apply to patients taking a P2Y12 inhibitor. While there was a signal for reduced rates of fast AAA growth in patients on DAPT, this is likely because of aspirin use.
Poster No. 40
Abstract No. 1786304
RAAS inhibition and AAA growth in renal atherosclerosis
1Cleveland Clinic; 2Johns Hopkins University; 3Washington University; 4University of Cincinnati
Background: In animal models, activation of the renin angiotensin aldosterone system (RAAS) has been shown to play an essential role in the pathogenesis and progression of abdominal aortic aneurysms (AAA). However, it is not known if inhibiting RAAS in conditions where it would be upregulated, such as with renal artery stenosis (RAS), using angiotensin converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARB) will lead to decreased AAA growth.
Methods: Patients with at least two aortic duplex ultrasounds and one renal artery duplex ultrasound between 2010 and 2020 were identified. Multivariable models were built to assess the association between ACE/ARB use and AAA growth (⩾ 0.5cm/year) in patients with and without RAS. Models adjusted for sex, initial AAA diameter, age, aspirin use, smoking, hypertension, chronic kidney disease and diabetes.
Results: A total of 238 patients were included in this analysis (RAS: N= 74; No RAS: N= 164). The proportion of RAS patients with fast AAA growth was lower in patients taking ACE/ARB (6.5% vs 28.6%; adjusted OR 0.18, p = 0.031). This association remained significant when AAA growth was assessed as a continuous variable (Coefficient: -0.19 cm/year, p = 0.041). There was no difference in the proportion of fast growth in patients without RAS between those taking and not taking ACE/ARB (26.0% vs 27.9%; Adjusted OR 0.99, p = 0.98).
Conclusion: In our cohort of patients with AAA, ACE/ARB use was associated with a lower odds of fast AAA growth and lower annual AAA growth in patients with RAS but not in those without RAS. This may suggest that the benefit of ACE/ARB might only apply in situations of an upregulated RAAS.
Poster No. 41
Abstract No. 1786316
Effect of insulin and metformin on AAA growth
1Cleveland Clinic; 2Johns Hopkins University; 3Washington University; 4University of Cincinnati
Background: Although abdominal aortic aneurysms (AAA) are generally a manifestation of atherosclerosis, diabetes mellitus (DM) is paradoxically negatively associated with AAA. Whether rates of AAA growth are driven by metabolic derangements in DM or from medications given to diabetics is less clear.
Methods: We identified patients with DM and at least two aortic Duplex studies between 2010 and 2020. Patients were divided into the following categories: (1) DM not on medication; (2) DM on metformin; (3) DM on insulin; (4) DM on metformin and insulin. A multivariable model was built to compare the rates of fast AAA growth (⩾ 0.5cm/year) between the categories. The model was adjusted for age, initial diameter, sex, aspirin use, smoking and hypertension.
Results: In our cohort of 529 patients with DM, the rates of fast AAA growth were 12.6%, 9.3%, 24.5% and 5.2% in those without medications, on metformin, on insulin and on both metformin and insulin groups, respectively. Insulin use was associated with an increased risk of fast AAA growth as compared to those not on medication (OR 2.16, p = 0.048) and those on metformin alone (OR 3.1, p = 0.008). Although there was a signal for decreased rate of fast AAA growth in those on metformin and those on metformin and insulin, this did not reach statistical significance.
Conclusion: In our cohort of patients with DM, insulin use was associated with an increased risk of fast AAA growth as compared to those not on medication and those on metformin. Further studies are required to determine if this is a result of progression of atherosclerosis or a mechanism that has yet to be elucidated.
Poster No. 42
Abstract No. 1786349
Readiness for behavior change in peripheral artery disease
1Northwestern University
Background: Peripheral artery disease (PAD) is a chronic and incurable disease that is impacted by adoption of health-promoting behaviors. This study assesses activation (understanding, competence, and willingness to participate in care) and readiness for behavior change (RBCh) in patients with PAD.
Methods: Patients with PAD were recruited from vascular surgery clinic and completed a survey on demographics, PAD-specific knowledge, and RBCh stage (pre-contemplation, contemplation, preparation, action, and maintenance) in domains of smoking cessation, physical exercise, medication compliance, and diet. Health literacy and activation were quantified with the s-TOFHLA and PAM-13, respectively. Activation scores were dichotomized as activated or poorly activated. RBCh scores were compiled into a composite score for all domains. Multivariable logistic and linear regression was used to identify predictors of activation and RBCh, respectively.
Results: Of 105 patients with PAD who completed the survey (mean age 68.5 years, 47.7% female, 30.2% Black, 13.4% active smokers), 77% had undergone leg revascularization and 71.6% scored as activated. Mean composite RBCh score was 17.4/20, indicating a behavior change stage of action. On bivariate analysis, lower PAD knowledge score, non-White race, lower education level, and lower income were associated with poor activation. Lower PAD knowledge score, non-White race, current smoking, and lower education level were associated with lower RBCh stage. In multivariable models controlling for race, income, health literacy, and education level, lower knowledge score was significantly associated with poor activation (OR=1.1, p=.04), while lower knowledge score and history of revascularization were significantly associated with lower RBCh score (b-coefficient 0.13, p=.04 and b-coefficient 1.5, p=.009, respectively).
Conclusion: Patients with PAD demonstrated overall high activation and RBCh. After controlling for demographic variables, lower PAD knowledge was associated with poor activation and low RBCh while history of revascularization was significantly associated with lower RBCh. Behavior interventions in PAD should be tailored to level of PAD knowledge and PAD severity.
Poster No. 43
Abstract No. 1787363
Duplex criteria for hemodynamically significant renal artery FMD
1Emory University School of Medicine; 2University Hospitals Harrington Heart & Vascular Institute; 3Rollins School of Public Health; 4University of Southern California
Background: Fibromuscular dysplasia (FMD) is a non-atherosclerotic vascular disease affecting renal arteries. Duplex ultrasonography (DUS) is non-invasive and commonly used to assess atherosclerosis-related renal artery stenosis (RAS). However, validated criteria for FMD-RAS severity are lacking. We sought to identify DUS parameters for detecting hemodynamically significant RAS in patients with multifocal FMD.
Methods: A retrospective analysis was conducted on multifocal FMD patients from 2 centers who underwent DUS followed by renal angiography within six months, along with hemodynamic assessment using pressure wire. DUS were performed at IAC-accredited facilities by registered vascular technologists. Data, including hemodynamic assessment, were collected and pooled for analysis. Hemodynamically significant RAS was defined as a Pd/Pa ratio < 0.9. Pairwise Pearson’s correlation coefficients between Pd/Pa ratio and maximum renal PSV, maximum EDV, and highest renal-to-aortic ratio (RAR) were calculated. Optimal cutoffs were explored through ROC curve analysis using Youden’s index.
Results: 41 renal arteries from 29 patients with DUS and Pd/Pa data were included in this analysis, 7 of which had Pd/Pa < 0.9. There were moderate negative correlations between Pd/Pa and maximum PSV (R=-0.48, p=0.002) and between Pd/Pa and EDV (R=-0.47, p=0.002). The correlation with RAR was weaker (R=-0.3 p=0.053). The most accurate renal artery PSV threshold for hemodynamically significant FMD-RAS was maximum PSV >/ 300.6 cm/s (57.1% sensitivity, 93.8% specificity, 87.1% accuracy). PSV >/ 273.0 cm/sec provided best combination of sensitivity (71.4%) and specificity (78.1%) with overall accuracy (76.9 %). No RAR cut point provided satisfactory sensitivity or specificity. All 7 renal arteries with Pd/Pa < 0.9 were treated with balloon angioplasty.
Conclusion: No established DUS criteria exist for diagnosing hemodynamically multifocal renal FMD. We suggest velocity parameters to identify patients who may benefit from hemodynamic assessment. PSV thresholds for renal FMD exceed those for atherosclerotic RAS assessment. Further validation through larger independent studies could lead to new criteria for quantifying renal FMD.
Poster No. 44
Abstract No. 1787364
Nicotinamide riboside and walking velocity in PAD
1Northwestern University Feinberg School of Medicine 2University of Delaware; 3University of California at San Diego; 4National Institute on Aging; 5University of Maryland School of Medicine; 6Northwestern University; 7University of Virginia; 8Augusta University; 9University of Florida; 10Stanford University
Background: In the NICE clinical trial, nicotinamide riboside (NR) improved 6-minute walk at 6-month follow-up in PAD, and resveratrol did not enhance benefits from NR. In post-hoc analyses, effects of NR on the short physical performance battery (SPPB) were evaluated.
Methods: PAD participants were randomized to NR 1,000 mgs, NR 1,000 mgs + resveratrol 125 mgs, or placebo for 6 months. The SPPB combines data from three tests (four meter walking velocity, standing balance, and time to stand five times from a seated position). Tests are scored on a 0-4 scale (4-best) and summed to attain the SPPB (range 0-12, 12-best). Clinically meaningful change is 1.0 for the SPPB and 0.1 m/sec for walking velocity. Statistical significance was pre-specified as a one-sided P value < 0.10.
Results: Due to the COVID-19 pandemic, of 90 participants randomized (43 (47.8%) Black), 41 completed the SPPB at 6-month follow-up. Adjusting for age, sex, race, and baseline 4-meter walking velocity, compared to placebo, NR (+0.09 m/sec, P=0.023) and NR + resveratrol (+0.06 m/sec, P=0.097) each improved 4-meter walking velocity. Compared to placebo, NR improved the SPPB and NR and NR+ resveratrol each improved the walking velocity score (Table). Compared to NR, NR + resveratrol did not significantly improve any outcome.
Conclusion: Compared to placebo, NR and NR + resveratrol each significantly and meaningfully improved lower extremity performance unrelated to walking endurance in PAD. Results require confirmation in a large randomized clinical trial.
Effects of nicotinamide riboside and nicotinamide riboside + resveratrol on the short physical performance battery in PAD.

Poster No. 45
Abstract No. 1787944
Variations in antiplatelet therapy following peripheral vascular interventions
1Henry Ford Hospital
Background: Antithrombotic therapy following endovascular peripheral vascular intervention (PVI) remains understudied. While many believe there is advantage for dual antiplatelet therapy (DAPT) and dual pathway inhibition (DPI) over single antiplatelet therapy (SAPT), much of this practice has been extrapolated from current coronary experience. This study aims to assess the varying prescribing patterns of antithrombotic therapy following PVI among Vascular Surgeons in Michigan.
Methods: A survey on the utilization of antithrombotic therapy following PVI was distributed to members of the Michigan Vascular Society in February 2024. DAPT was defined as the combination of aspirin with another antiplatelet, whereas DPI was defined as the combination of aspirin with an anticoagulant.
Results: A total of 32 vascular surgeons responded to the survey. 47% and 56% of respondents believe that there is clinical uncertainty around the safety/efficacy of DAPT and DPI, respectively, following PVI. In terms of prescribing patterns following PVI, 3% use SAPT, 53% use DAPT, 3% use DPI, while the rest expressed that their choice is dependent on the clinical situation. Preference for duration of therapy were as follows: 4 weeks (3%), 6 weeks (10%), 3 months (27%), 6 months (17%), 1 year (3%), and lifelong (33%). Prescribing patterns and durations varied between plain balloon angioplasty, drug-coated balloon angioplasty, drug-eluting stenting, bare metal stenting and covered stenting. In situations when patients were already on anticoagulation for an unrelated medical issue, 93% expressed that they would prescribe SAPT, whereas only 4% prescribe additional DAPT and 4% do not prescribe any antiplatelet therapy. Up to 89% of respondents expressed interest in a trial evaluating DAPT and DPI post-PVI. Specifically, 78% expressed interest in studying the duration of DAPT (6 weeks vs 6 months), and 85% in studying DAPT vs DPI (6 months each).
Conclusion: There is very high variation in the antiplatelet and antithrombotic prescribing patterns both in drug selection and duration following PVI among members of the Michigan Vascular Society. A prospective, multicenter, randomized controlled trial is needed to determine the safest and most effective treatment.
Poster No. 46
Abstract No. 1787961
Venous thromboembolic events in hospitalized cancer patients
1St. Luke’s Medical Center-Global City; 2St. Luke’s Medical Center
Background: This study aimed to determine the frequency and proportion of VTE events in hospitalized cancer patients, the frequency and proportion of the primary malignancy among hospitalized cancer patients with VTE, And the proportion of patients given VTE prophylaxis prior to diagnosis of VTE.
Methods: A descriptive cross-sectional study of the prevalence of VTE among cancer patients admitted in the Oncology Unit of St. Luke’s Medical Center – Global City was performed from January 2020 to January 2023.
Results: Acute VTE events were observed in 41.57%. The most occurring acute VTE event was DVT with the remainder having PE. Majority was observed in solid malignancies, followed by double-triple primary malignancies and least in hematologic malignancies. The cancer with the most evidence of VTE in their type was musculoskeletal malignancy with 83.33% of their type having evidence of VTE upon work up and 16.67% having no evidence of VTE. This is followed by pancreatic cancer with 81.25% of this cancer having evidence of VTE and 18.75% having none. Gastroesophageal cancer had 60.00% documented VTE in their population and 40.00% without VTE. The malignancy with the least occurrence of VTE in their type was colorectal with 79.25% of them having no evidence of VTE and 20.75% having evidence of VTE. This is followed by hematologic malignancy with majority oof them having no evidence of VTE with 22.45% having evidence of VTE. Hepatobiliary cancer had mostly no evidence of VTE in 65.38% with 34.63% of this cancer having evidence of VTE. Majority were on anticoagulation prior to evaluation for VTE as VTE prophylaxis followed by those who did not receive any anticoagulation prior to being evaluated for acute VTE. . Of the subjects with evidence of acute VTE events during this admission, majority did not receive anticoagulation prior to the event.
Conclusion: The real rate of VTE at various sites remain unclear given the paucity of Asian data and diverse population regarding VTE in hospitalized cancer patients. Nevertheless, there is consistent evidence that a trend of increased documented VTE in hospitalized cancer patients. Whether due to increased awareness, utilization of diagnostic imaging, or other risk factors needs is undetermined. Although breast, lung and gynecologic malignancies had the most recorded VTE events, the malignancy with most occurrence of VTE in their population are the musculoskeletal, pancreatic, and gastroesophageal. There is predominantly no utilization of anticoagulation prior to VTE event.
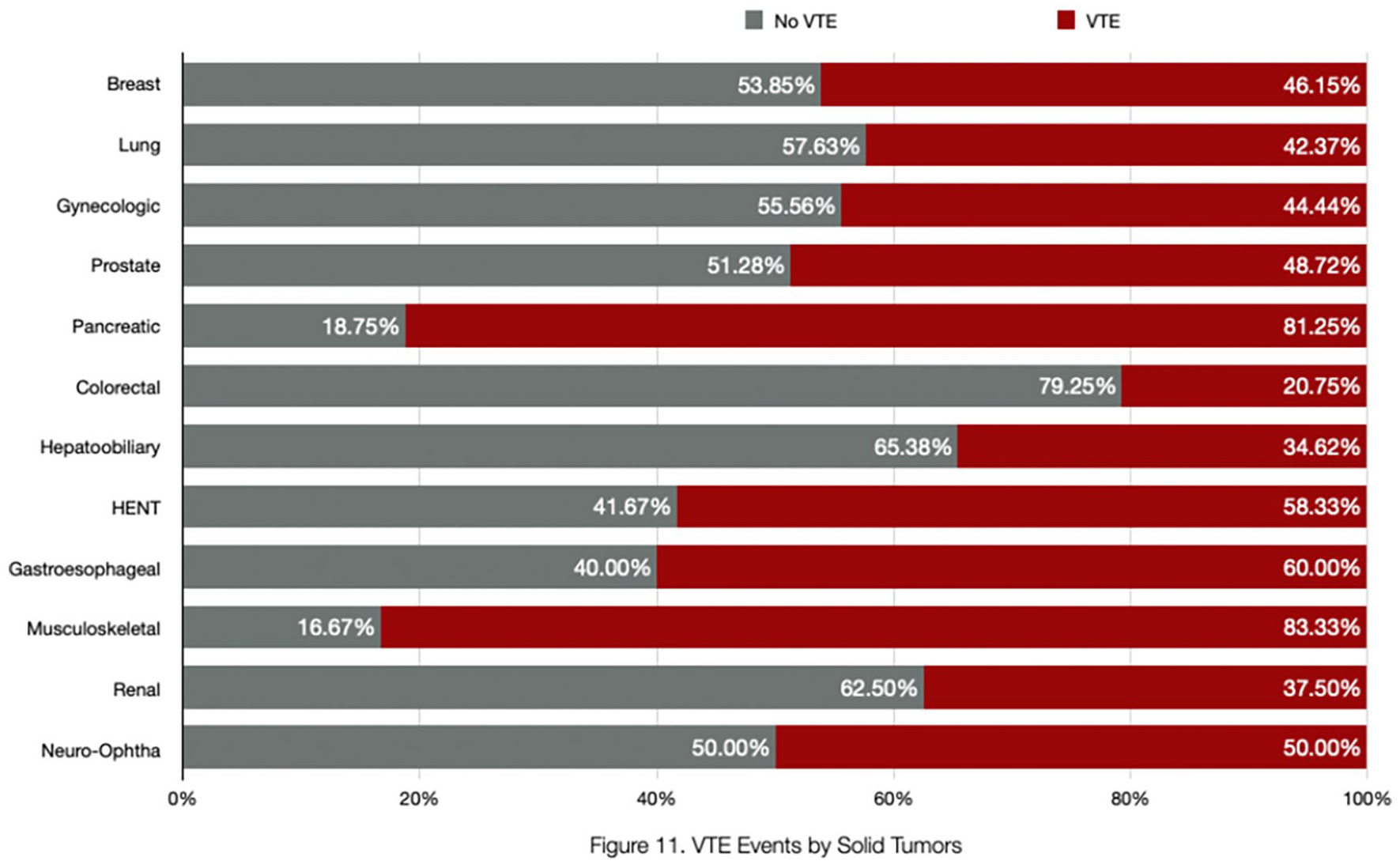
VTE events by solid malignancy.
Poster No. 47
Abstract No. 1754444
Utilizing pediatric mechanical pump for fluoroscopic lymphangiography
1Mayo Clinic
Background: Lymphangiography is a reliable diagnostic tool to assess and treat multiple pathologies including lymphatic flow abnormalities, malformations, and iatrogenic complications. However, the techniques behind achieving images can often be resource and time-intensive. Although slow manual dye injection is currently the standard of delivery, greater efficiency as a result of mechanical infusion would be desirable. In this case, we examined the efficacy of utilizing pediatric pumps to replace manual injection of lipiodol in intranodal fluoroscopic lymphangiography.
Methods: We replaced the process of slow standard manual injection with the use of a Medfusion 4000 pediatric syringe pump on an adult patient undergoing fluoroscopic lymphangiogram for chylothorax after lung resection. Using ultrasound-guidance, bilateral inguinal nodes were accessed successfully with 25-gauge needles and standard primed infusion tubing was connected with Luer-lock connectors. We used sterile 30 mL glass infusion syringes (each filled to 6 mL) to withstand the volume and duration for the infusion. Each syringe was attached to pediatric pumps with both pumps’ infusion rates set at 6 mL/hr.
Results: Within ten minutes into the procedure, contrast leaking was noted from the needle connector end of the tubing. The infusion was immediately aborted, and the disintegrated tubing discarded. The integrity of the needle connectors remained intact and successfully attached to new primed small bore extension tubing to resume manual injection. The remainder of the study was successfully completed without any compromise.
Conclusion: In this particular case, we were unable to successfully utilize a pediatric pump for lipiodol infusion as a substitute for manual injection. A 2004 study conducted by Kudo et. Al suggested that materials made from polycarbonate are susceptible to degradation from lipiodol, specifically the three-way stopcock, while other plastic materials made from polypropylene, polyamide, and polysulfone remained damage-free from lipiodol soaks and injections. These findings suggest that our method for mechanical infusion of lipiodol is feasible but may be better achieved by substituting for a compatible connector.
Poster No. 48
Abstract No. 1787529
Hydromorphone impact on antiplatelet efficacy in PAD patients
1Massachusetts General Hospital
Background: Narcotics are common pain medications given to peripheral artery disease (PAD) patients post revascularization. Antiplatelet medications are provided to PAD patients to decrease thrombotic risk; however, morphine has been shown to delay clopidogrel absorption which may lead to treatment failure. The impact of narcotics on antiplatelet efficacy has not been quantified. This study aims to evaluate the impact of hydromorphone on the platelet-inhibiting effects of anti-platelet medications in PAD patients post revascularization.
Methods: This prospective observational study was conducted from December 2020 to July 2023 and included PAD patients undergoing revascularization. Thromboelastography with platelet mapping (TEG-PM) was used to assess coagulation parameters in patients who received IV hydromorphone 0.4 mg within 6 hours of the surgery and those who did not receive narcotics. Platelet reactivity (ADP/AA Aggregation) was measured in the presence of clopidogrel and aspirin. A Mann-Whitney-U test was used to compare the medians of TEG parameters between groups. Multivariate linear regression was utilized to assess independent variables.
Results: Of the 230 patients analyzed, hydromorphone was administered to 42 patients (18%) intravenously. Patients on hydromorphone exhibited increased median percent ADP aggregation [HM: median 71.9 (39.6, 88.3); no HM: median 58.7 (37.2, 79.5), p < 0.05]. The univariate analysis showed ADP % aggregation was significantly associated with hydromorphone use, type of intervention (open vs. endo), smoking status, and hypertension. The multivariate analysis showed hydromorphone use, tobacco use, and hypertension (all: p < 0.05) independently increased post operative ADP % aggregation indicating that patients with these risk factors may not glean complete therapeutic effect of antiplatelet medications.
Conclusion: The study provides insights into the impact of hydromorphone use on the effectiveness of antiplatelet therapy and coagulation parameters in PAD patient’s post-revascularization. Our findings suggest that the administration of hydromorphone post-operatively can influence clot dynamics, potentially affecting the adequacy of the antiplatelet therapy.
Poster No. 49
Abstract No. 1787591
Vessel arteriopathies – the silent threat of stroke
1Mayo Clinic Arizona; 2Scripps Health
Background: Arteriopathies, which include a broad spectrum of vascular abnormalities, are recognized as significant risk factors for stroke. However, the prevalence of stroke in patients across various diagnoses and vascular conditions have not been extensively studied.
Methods: A cohort of individuals ⩽ 60 years old (n = 2117), diagnosed with any form of arteriopathy were identified using ICD and billing codes, with manual verification of charts to ensure accuracy. We assessed the odds ratios (OR) of stroke among individuals with aneurysms/dissections in different vascular beds and those with syndromic conditions such as fibromuscular dysplasia (FMD), all types of Ehler-Danlos (EDS), Marfan’s syndrome, and Loeys-Dietz syndrome.
Results: Distinct variations in incident stroke frequency were observed among individuals who had previously been diagnosed with aneurysms or dissections involving the abdominal aorta (OR 2.93 [CI 1.57 – 5.49], p-value 0.0016), carotid or cerebral vessels (OR 3.85 [CI 2.92 – 5.08], p-value < 0.00001), mesenteric vessels (OR 2.219 [CI 1.54 – 3.20], p-value < 0.0001), and the peripheral extremity vessels (OR 3.08 [CI 1.67 – 5.66], p-value 0.0007). There was a statistically significant overlap between the diagnosis of these conditions and the diagnosis of FMD. However, there was not an increased odds of stroke associat–d with spontaneous coronary artery dissection, thoracic aortic aneurysm or dissection, FMD, EDS, Marfan’s, or Loeys-Deitz syndrome.
Conclusion: The study finds that in a relatively younger population, aneurysms or dissections affecting various vascular beds were associated with increased odds of stroke. There was a significant overlap between these conditions and the diagnosis of FMD; however, syndromic conditions in general did not demonstrate the same increased odds of stroke. The timing of vascular pathology relative to any clinical diagnosis of a syndromic condition remains unclear, necessitating cautious interpretation of these results. Further evaluating the risk of stroke in patients with vascular aneurysms or strokes may be a focus of further research.
Poster No. 50 – Withdrawn
Poster No. 51 – Withdrawn
Poster No. 52
Abstract No. 1787614
Beyond the echocardiogram – is vascular investigation justified?
1Mayo Clinic Arizona; 2Scripps Health
Background: Clinical uncertainty exists regarding whether a complete vascular investigation for concomitant aortopathy should be conducted in individuals with thoracic aortic aneurysms/dissections or bicuspid aortic valves, particularly in cases where syndromic causes are not suspected.
Methods: A cohort of individuals ⩽ 60 years old (n = 2117), diagnosed with any form of arteriopathy were identified using ICD and billing codes, with manual verification of charts to ensure accuracy. Patients with syndromic vascular conditions (Marfan syndrome, Loeys-Dietz syndrome, or Ehlers-Danlos syndrome) were excluded. Of the remaining (n = 1438), we identified the prevalence of thoracic aortic aneurysm/dissection or bicuspid aortic valves, along with the odds ratios (OR) of having other concomitant vascular conditions.
Results: Of the filtered cohort, 44.64% (n = 642) were diagnosed with thoracic aortic aneurysm/dissection or a bicuspid aortic valve. Notably, FMD had a prevalence of 12.8%, yielding an OR of 0.08 [95% CI 0.05 – 0.14] with a p-value < 0.01; SCAD had a prevalence of 11.96%, corresponding to an OR of 0.123 [95% CI 0.07 – 0.20] with a p-value of < 0.01. Similarly, the prevalence of concomitant carotid or cerebral extremity aneurysm/dissection was 33.31%, with an OR of 0.03 [95% CI 0.02 – 0.04] and a p-value of < 0.01; abdominal aortic aneurysm/dissection was 3.27%, with an OR of 1.34 [95% CI 0.75 – 2.40] and a p-value of 0.32; mesenteric aneurysm/dissection had a prevalence of 13.42%, resulting in an OR of 0.13 [95% CI 0.08 – 0.21] and a p-value of < 0.01; peripheral extremity aneurysm/dissection had a prevalence of 3.40%, with an OR of 0.59 [95% CI 0.32 – 1.08] and a p-value of 0.09.
Conclusion: In individuals with thoracic aortic aneurysm/dissection or bicuspid aortic valves, the prevalence of concomitant arteriopathies were lower than anticipated. These findings support existing guidelines, which do not recommend comprehensive vascular investigations in this population. However, the timing of aortic pathology relative to other arteriopathies remains unclear, necessitating cautious interpretation of these results. This study contributes valuable data to the literature by providing insights into a relatively understudied population.
Poster No. 53
Abstract No. 1787894
DVT impact on PE outcomes among non-cancer patients
1Mayo Clinic Alix School of Medicine; 2Mayo Clinic
Background: Venous thromboembolism (VTE) affects over one million patients every year in the United States, with nearly 400,000 cases of pulmonary embolism (PE). Yet, it remains unclear whether co-incident deep vein thrombosis (DVT) adversely impacts the risk of mortality or VTE recurrence.
Methods: Consecutive patients with confirmed acute PE (March 1, 2013 – June 30, 2021) who underwent ultrasound (US) imaging were divided into two groups based on the presence or absence of leg DVT. PE severity was classified by AHA criteria. Patients were followed prospectively for symptomatic VTE recurrence, major and clinically relevant non-major bleeding (CRNMB) and all-cause mortality.
Results: Over the study interval, 872 patients with PE and without cancer were enrolled. 545 (62.5%) had leg DVT confirmed by US. Patients with leg DVT were slightly older (by 2.5 yr, p=0.022) and less often female (39.8% vs 52.3%, p=0.022). Clinical risk factors were similar between groups. Patients with leg DVT more often had symptomatic PE (79.6% vs 67.6%, p< 0.001) PE, with more often massive PE (6.6% vs 2.9%, p=0.033) PE, and submassive PE (39.5% vs 23.1%, p< 0.001). All patients were treated with anticoagulation. Patients with leg DVT more often received unfractionated heparin (55.2% vs 50.1%, p < 0.001) and low molecular weight heparin (22.7% vs. 22.0%, p < 0.001), whereas those without DVT were more frequently treated with apixaban (18.9% vs. 12.7%, p=0.012). There were no differences in anticoagulant duration. There were 56 deaths in the group with leg DVT and 32 deaths in the patients without leg DVT (2-year rates 20.4% vs 25.9%, p=0.046). VTE recurrence, major bleeding and CRNMB were similar between groups.
Conclusion: Among a large cohort of PE patients without cancer, the presence of leg DVT at the time of PE does not appear to carry increased risk of mortality compared to the absence of leg DVT. In fact, patients with leg DVT died less often in our cohort than patients without leg DVT. While there is a theoretical risk of recurrent embolization, the presence of leg DVT does not appear to affect VTE recurrence or bleeding outcomes when adequately treated with anticoagulation.
Poster No. 54
Abstract No. 1775526
Limb risk after LER in PAD and chronic kidney disease (CKD)
1University of Colorado School of Medicine; 2CPC Clinical Research, University of Colorado; 3University of Hamburg-Eppendorf; 4Duke University; 5Hamilton Health Sciences and McMaster University; 6Bayer AG Research & Development, Pharmaceuticals; 7Janssen Research and Development; 8University of Mainz
Background: Patients with chronic peripheral artery disease (PAD) and comorbid chronic kidney disease (CKD) have higher rates of major adverse cardiovascular (MACE) and limb (MALE) events than those with normal renal function. The impact of comorbid CKD on the risk of MACE and MALE and the efficacy and safety of rivaroxaban in the acute lower extremity revascularization (LER) setting is not well described.
Methods: VOYAGER-PAD randomized patients with PAD after LER to rivaroxaban 2.5 mg twice daily or placebo. CKD was defined as eGFR < 60 mL/min/1.73m2 at baseline. Patients with eGFR < 15 were excluded. The risk of MACE and MALE (n/N%) in those with and without CKD was evaluated as well as the consistency of efficacy and safety of rivaroxaban.
Results: Of 6564 randomized, baseline eGFR was available in 96.2% with 1327 (21%) having CKD. At a median follow up of 28 months, patients with vs without CKD had a higher risk of MACE (15.8% vs 9.1%, Panel A). This pattern of increased risk was consistent across MACE components. In contrast, risk of MALE (8.6% vs. 8.9%, Panel A) and its components (Panel B) did not differ by CKD. TIMI major bleeding was higher in those with CKD vs. without (1.83% vs. 1.21%). The efficacy for MALE and safety of rivaroxaban was consistent in those with and without CKD (Panel B).
Conclusion: In patients with symptomatic PAD following LER, those with CKD are at higher risk of MACE. The risk of MALE did not differ by CKD. The efficacy for MALE and safety of rivaroxaban was consistent in those with and without CKD.
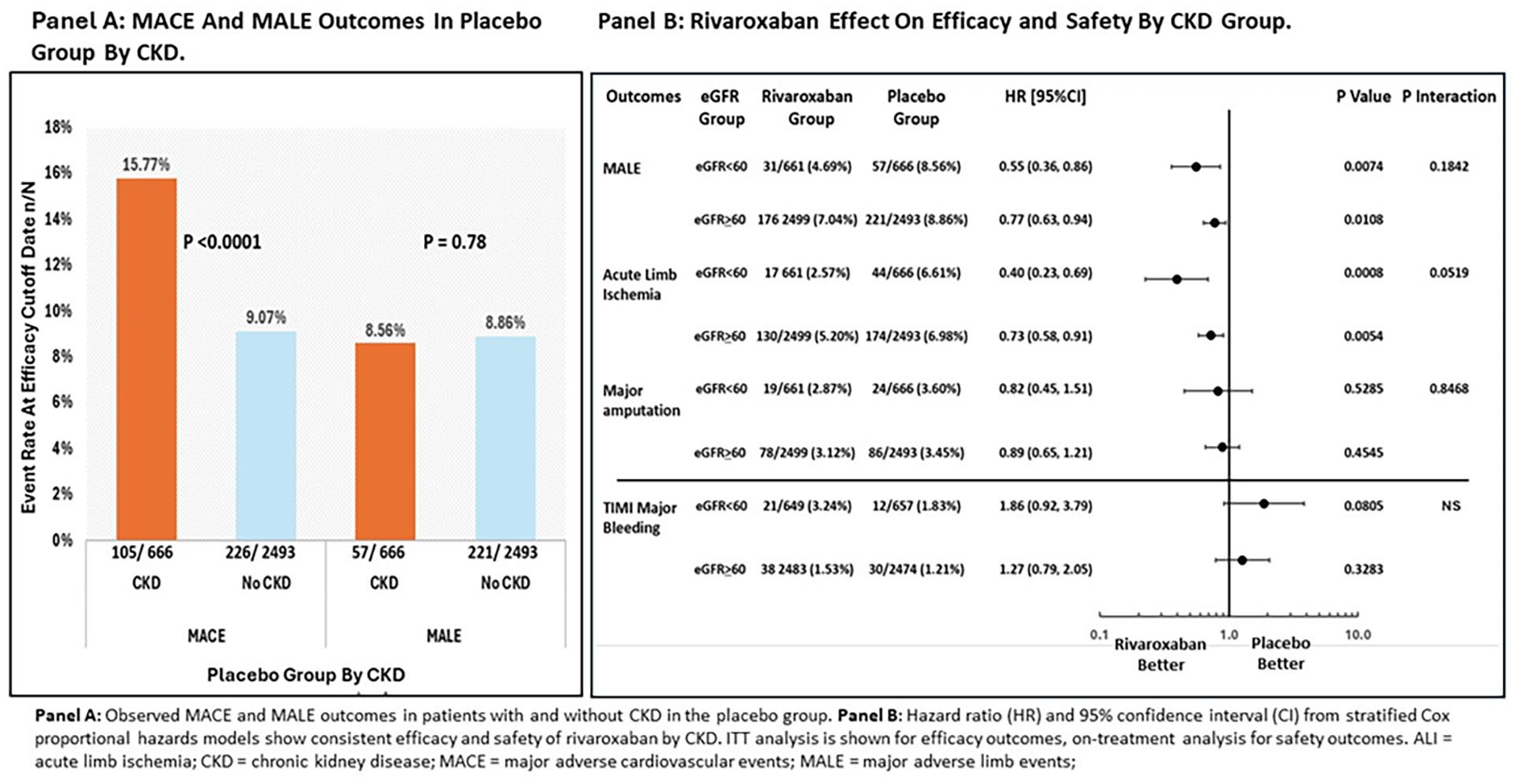
Risk of MACE and MALE and Effects of Rivaroxaban after Revascularization in Patients with PAD and CKD.
Poster No. 55
Abstract No. 1775791
Variability in response to CMS-reimbursed supervised exercise therapy
1University of Minnesota School of Nursing; 2M Health Fairview; 3University of Minnesota
Background: Variability in response to supervised exercise therapy (SET) for symptomatic peripheral artery disease (PAD) is a poorly understood phenomenon that affects approximately one third of patients. In this study, we evaluated the prevalence and characteristics of variability in response among patients who completed SET during the first five years of CMS reimbursement.
Methods: Using data from a SET Registry established at a large, Midwest hospital system with a well-established SET program, we conducted a retrospective chart review of patients with PAD who completed SET between 10/1/2017-12/31/2022. Patient demographic and medical characteristics, details of SET participation, and outcomes (6-minute walk test [6MWT], timed up and go test, and the Vascular Quality of Life Questionnaire [VascuQOL-6]) were abstracted. Descriptive statistics, data visualizations, and multiple linear regression were used to examine the sample and poor response (lack of a clinically meaningful improvement) and nonresponse (no improvement) to SET.
Results: A total of N=207 patients completed SET. Two thirds were male, with a mean (SD) age of 71.7 (8.5) years, ABI of 0.67 (0.23), and baseline 6MWT distance of 298.4 (99.1) meters. The mean (95% CI) increase in 6MWT was 53.6 (44.8, 62.4) meters. Of the 207 patients, n=29 (14.2%) had no improvement or a decline in their 6MWT total distance; and additional n=15 (7.4%) did not meet the threshold for at least a small, clinically meaningful difference (10 meters). For the VascuQOL-6, n=29 (25.9%) had no improvement. Nonresponse varied from 3.3% (treadmill workload) to 58.9% (timed up and go). There were no differences in demographic or medical characteristics between responders and nonresponders.
Conclusion: The prevalence of nonresponse observed in this program is less than half of what has been reported in randomized controlled trials. This may be due, in part, to increased ability to tailor exercise prescriptions in clinical settings or differences in characteristics of patients enrolling in clinical vs. research programs. Additional research should examine modifiable predictors of poor and nonresponse to maximize an individual’s potential benefit from SET.
Poster No. 56
Abstract No. 1782384
Subclavian vein occlusion due to pacemaker leads
1Arizona Cardiovascular Consultants & Vein Clinic; 2Fountain Hills Medical Center
Background: Unilateral upper extremity, breast and chest edema and congestive symptoms are underreported complications of pacemaker (or defibrillator) implantations. They occur due to venous occlusion or stenosis of the subclavian vein secondary to the implanted leads. They are frequently misdiagnosed as cellulitis, mastitis and are unnecessarily treated with antibiotics.
Methods: We treated 35 patients with unilateral upper extremity and breast congestive symptoms with percutaneous balloon venoplasty (PBV) with or without catheter directed thrombolysis (CDT) with tPA. There were 20 patients with acute deep vein thrombosis ( DVT). All underwent PBV and those with DVT received tPA at 1 mg/hr for 18-24 hours. Access was through the brachial or axillary vein. All received 81 mg of aspirin and maintenance dose of apixaban or rivaroxaban. For those with DVT the duration of anticoagulation was 6-12 months and for those without it, 4-6 weeks.
Results: There were 28 women. The patients’ mean age was 68±3 years. Symptom onset was at 8± 3 days after device implantation. Venographic evidence of previous venous insults ( stenosis, compression, old DVT) was noted in 30 patients. Substantial improvement in symptoms occurred at around 5 days following intervention. There were no procedural complications. At a mean follow-up of 32± 4 months no recurrence of DVT or congestive symptoms had occurred.
Conclusion: We conclude that pacemaker leads can obstruct the subclavian vein leading to congestive symptoms and DVT which often get misdiagnosed as an infectious process. They usually occur in patients with previous venous insults. PBV and if necessary CDT is an effective and safe tool in the management of this condition.

Significant edema and congestive symptoms post pacemaker implantation using the left subclavian vein.
Poster No. 57
Abstract No. 1782488
Experience with limb revascularization at safety net hospital
1University of Texas at Southwestern Medical Center; 2UT Southwestern; 3Parkland Memorial Hospital
Background: Peripheral artery disease (PAD) is a common disease associated with major adverse atherosclerotic events, both cardiac and limb-related. Despite this, screening, diagnosis, and optimization of medical therapy remains a significant unmet need.
Methods: The cohort included patients who have undergone their index limb revascularization for severe symptomatic peripheral artery disease between 01/01/2021 and 12/31/2022 at a major urban safety net hospital. Exclusion criteria include popliteal aneurysm, vasculitis/Buerger’s disease, prior chemotherapy, and prior radiation therapy. Data was obtained using ICD-10 and CPT codes.
Results: The final cohort included 311 patients, was 36% female, ~50% Hispanic, 36% Black, and was 63 +/- 10 years old. Furthermore, 58% were either on Medicaid or a hospital-specific subsidized health plan. History of hypertension, hyperlipidemia, and type 2 diabetes were seen in 98%, 93%, and 79% of patients, respectively. Nearly 2/3rd of patients was either current or former smoker. When looking at patients with labs prior to revascularization, 57% had HA1c ⩾ 7%, and 64% had LDL ⩾ 70 mg/dL. More than 6 in 10 patients had revascularization within 1 year of PAD diagnosis. Half of the patient received initial PAD diagnosis at time of revascularization. Most revascularizations were endovascular (88%). Nearly a quarter of patients in our cohort required repeat revascularization within median of 127 days from index procedure.
Conclusion: In a diverse patient population of a safety net hospital, we found that approximately 50% of patients were diagnosed with PAD during admission for the index revascularization and nearly a quarter required repeating revascularization suggesting need to improve both our screening and management of this high-risk population. We are implementing a quality improvement initiative to tackle this problem.
Poster No. 58
Abstract No. 1756684
Offline deep reinforcement learning model estimates warfarin dosing
1Yale; 2Mayo Clinic
Background: Safe and effective warfarin dose management remains challenging. Despite efforts and resources time in therapeutic range (TTR) typically remains low (40-50%) in community practices. Specialized clinics achieve higher TTR but are not widely available and are resource intensive. The aim of this study was to compare the dosing recommendation for warfarin maintenance given by a Deep Reinforcement Learning (DRL) model with those of pharmacists and physicians staffing an anticoagulation clinic.
Methods: A previously developed offline reinforcement learning model to estimate warfarin dosing (prediction accuracy of 91-96%) was compared with clinician recommendations in 17 real clinical scenarios. Clinicians were presented with past warfarin doses and 5 prior INR values then asked to recommend dosing for a specified interval. The mean dose for the interval of all clinicians was compared with the dose estimated by the model. The survey was sent to experienced physicians, pharmacists, and advanced practice providers (APP) working in all anticoagulation clinics within the Mayo Enterprise.
Results: Twenty-eight clinicians responded to the survey (61% pharmacists and 32% physicians, 7% APP; mean time in practice 14±9 years). The mean interval dose was 26.8±14.8 mg for the clinicians and 26.5±14.8 mg for the model. The mean difference between clinicians and model dosing for all cases was not statistically different p=0.12 (1.1 ± 0.5mg) The comparison with the model by clinician is depicted in figure 1.
Conclusion: No significant difference was found between the warfarin dosing recommendation given by specialized clinicians compared to the DLR model. This DLR model has potential for assisting anticoagulation management in the clinical setting.
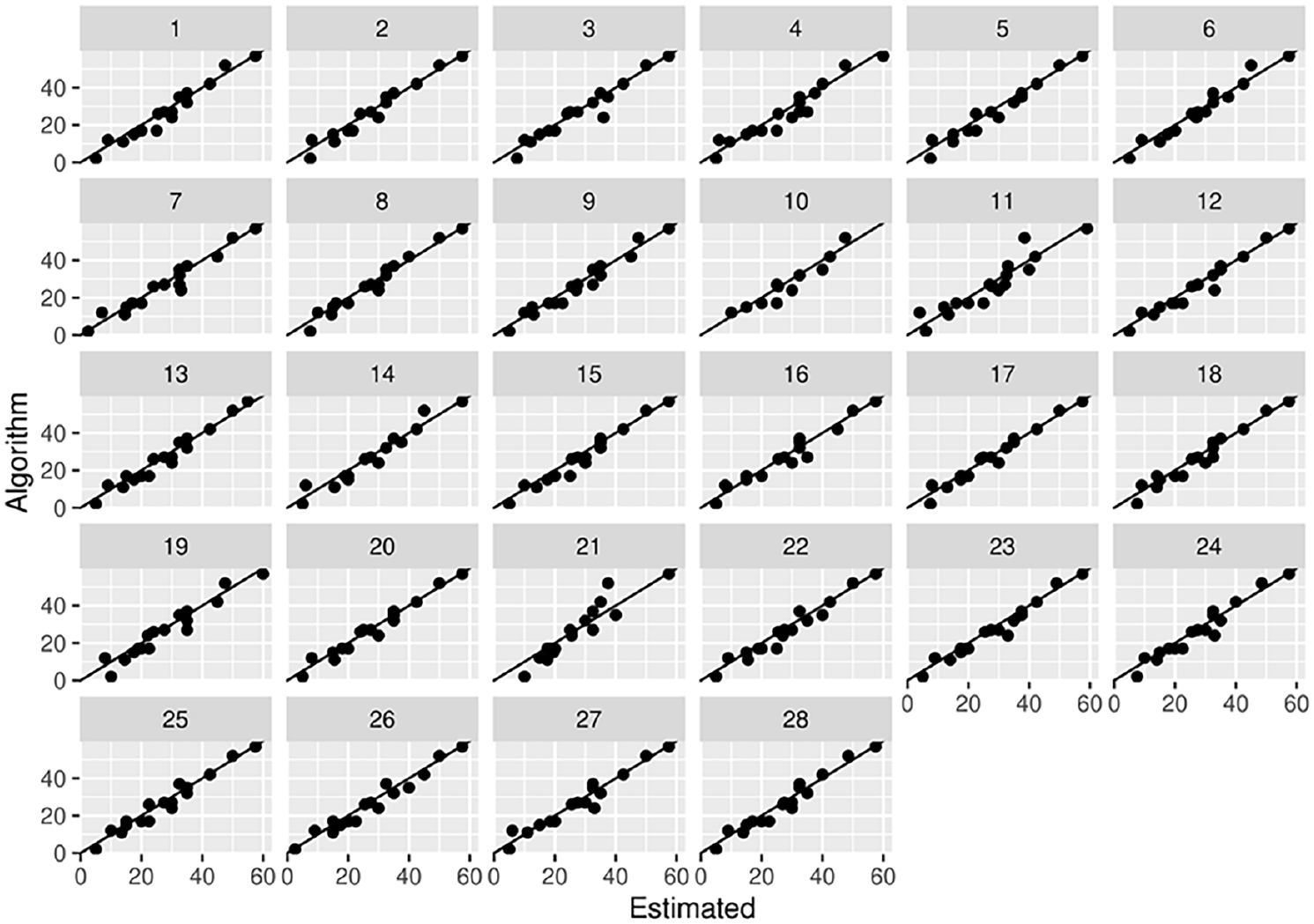
Comparison of clinician interval dose vs. model interval dose. Numbers 1 to 28 represent the different clinicians.
Poster No. 59
Abstract No. 1751146
Agreement between pedal acceleration time (PAT) and ABI in diagnosing pad
1St. Luke’s Medical Center, Quezon City, Philippines; 2St. Luke’s Medical Center, Dr. HB Calleja Heart and Vascular Institute
Background: Pedal acceleration time (PAT) is an additional diagnostic tool to identify peripheral artery disease-afflicted patients. This is especially useful in local institutions that lack the machines in acquiring the ankle-branchial index (ABI) / toe-brachial index (TBI). We aim to discuss the importance of pedal acceleration time in diagnosing significant PAD in centers without ABI machine and present the cut-off values for ABI and TBI in diagnosing significant PAD in Filipinos.
Methods: This was a cross-sectional analytical study of adult Filipinos with ABI done at the Vascular Laboratory of St Luke’s Medical Center, Quezon City. For patients with compressible arteries, the agreement between PAT (arcuate, mid-plantar, lateral plantar and deep plantar arteries) and ABIs were analyzed. However, for patients with non-compressible arteries, the agreement between PAT and TBIs were analyzed instead.
Results: A total of 399 limbs were included. In classifying patients’ PAD severity, this study demonstrated a moderate agreement between PAT and ABI (kappa value of 0.519, p < 0.001) among patients with compressible arteries, and a fair agreement between PAT and TBI (kappa value of 0.244, p < 0.001) among patients with non-compressible arteries. The diagnostic PAT cut-off value was determined to be more than 124 milliseconds, with a sensitivity of 78.4% (95% CI 69.2-86.0) and specificity of 82.4% (95% CI 77.6-86.6), in patients with significant PAD. A PAT cut-off value of 124 milliseconds is also correlated with a TBI of less than or equal to 0.7, with a sensitivity of 85.5% (95%CI 75.96-92.5) and specificity of 82.4% (95%CI 77.6-86.5).
Conclusion: Pedal acceleration time has a moderate agreement with the ankle-brachial index among patients with compressible arteries and has a fair agreement with the toe-brachial index among patients with non-compressible arteries. This study has shown that a PAT value of more than 124 milliseconds is enough evidence for the diagnosis of significant peripheral artery disease. This may be used as a surrogate diagnostic test in machine-lacking institutions.
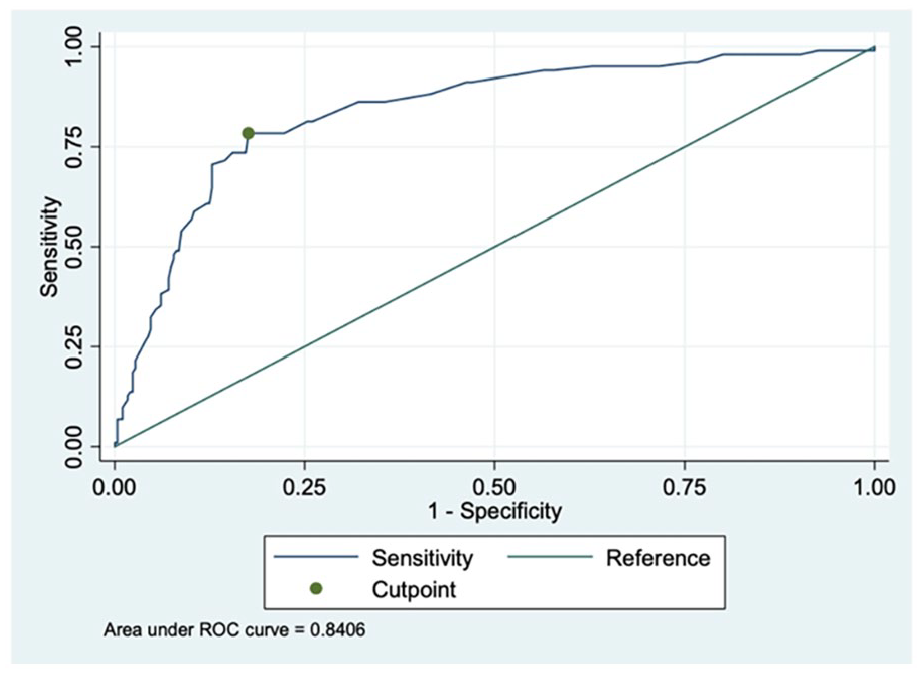
Receiver operator characteristic (ROC) curve of PAT in predicting significant PAD. The optimal cutoff point for PAT in predicting significant PAD in this dataset is 124.
Poster No. 60
Abstract No. 1772307
Walking distance with venous and arterial disease
1Mayo Clinic
Background: Peripheral arterial disease of the lower extremities can cause claudication leading to reduced walking distance. The influence of venous disease on arterial claudication has not been well described. Objective: Determine if concurrent venous disease is associated with reduced walking distance in patients with peripheral arterial disease (PAD).
Methods: The Mayo Clinic Vascular Laboratory database was searched for ambulatory adults age > 18 years who underwent venous plethysmography and standard protocol lower arterial treadmill exercise study within 1 year of each other were identified. Venous plethysmography per standard techniques assessed the severity of venous incompetence (categorized as none, mild, moderate, or severe) and calf pump function (CPF) measured as ejection fraction (EF) per leg.
Results: A total of 219 patients underwent venous plethysmography and lower extremity arterial treadmill exercise testing and met the study criteria. The median ABI was 1.04 (SD 0.18; IQR 0.93– 1.13), median CPF EF was 39.8% (SD 22.5, IQR 25.2-56.7), and median CEAP score was C3 (IQR 2-4). No clear relationship was observed between CPF, ABI, and CEAP scores overall. Mean walking distance decreased with increasing severity of PAD as categorized by worst leg {No PAD: 206yds, Mild: 181yds, Moderate: 165yds, Severe: 128yds, Non-compressible (ABI >1.4): 192yds}. Decreased walking distance appeared to be most pronounced in patients with EF < 20% (EF < 20% vs >=20% 161yds vs 206yds, p=0.003). Walking distance was reduced by approximately 60yds (110 vs 169yds, p=0.1) in patients with EF < 20% and moderate or severe PAD and 44yds (169 vs 213yds, p=0.006) in patients with mild or no PAD (Figure). In a multivariable linear regression model adjusting for age, sex, PAD, venous incompetence, CEAP score, and CPF, PAD (p=0.07), CPF (p=0.004), and CEAP score (p=0.03) were associated with walking distance but not venous incompetence (p=0.70).
Conclusion: In this hypothesis-generating study, we found that chronic venous disease (driven by reduced CPF) reduced walking distance overall and with a severity that appeared to be increased in patients with PAD.
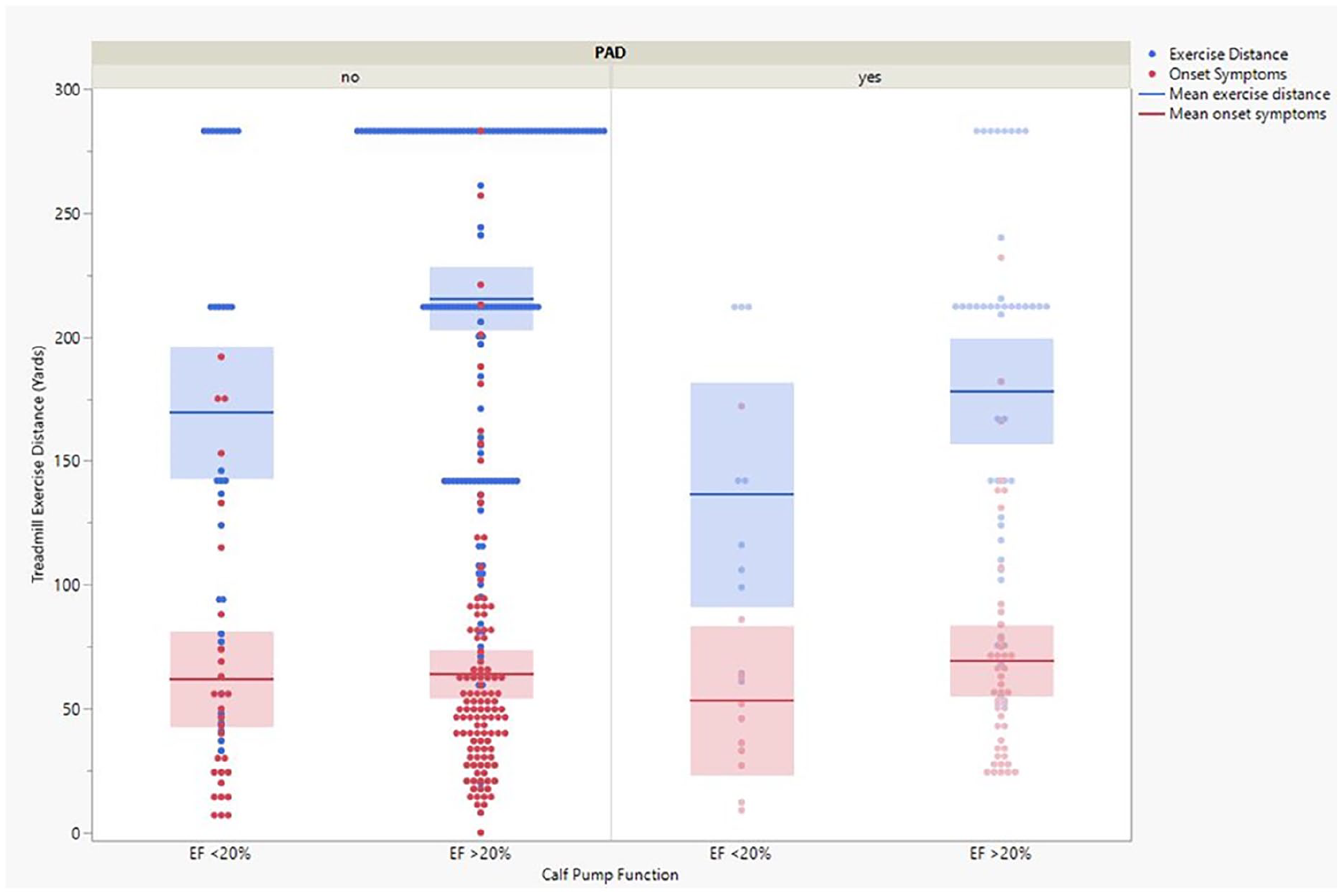
Calf pump function and treadmill walking distance.
Poster No. 61
Abstract No. 1774337
A case series of failed percutaneous pulmonary thrombectomy
1University of Michigan; 2Henry Ford Health System
Background: Occult chronic thromboembolic pulmonary hypertension (CTEPH) may initially be inappropriately diagnosed as acute pulmonary embolism (PE), leading to use of mechanical aspiration thrombectomy (MAT) devices unsuited for removal of chronic thrombi. The mechanisms, predictors, and outcomes of failed MAT are poorly understood.
Methods: Retrospective case series at a high-volume CTEPH center with low volume of MAT. In-house and outside MAT cases (12/2018 - 7/2023) were identified by electronic medical records search engine. Manual abstraction identified demographic, clinical, laboratory, imaging, procedural and outcome data. MAT was considered “failed” if no acute thrombus was obtained or symptoms didn’t improve.
Results: 14 failed and 18 successful MAT cases were identified. Failed cases were due to underlying chronic thrombus (n=11), hemodynamic intolerance (n=2), and right ventricle dilation limiting catheter support (n=1). In contrast to successful cases, failed MAT cases presented with more prolonged symptoms, less tachycardia, less hypotension, lower biomarkers, and had greater in-hospital PE mortality.
Conclusion: Failed MAT cases often presented with decompensated CTEPH physiology, less severe vital sign changes, and underlying chronic embolic material. A high index of suspicion is needed to avoid subjecting chronic pathology to unsuitable interventions, and to enact appropriate treatment in this high-mortality group. Clinical factors to improve differentiation of acute and chronic PE require further study.
Presenting clinical features and outcomes among successful and failed MAT cases.

Poster No. 62
Abstract No. 1774370
Pulmonary embolism profiles in a Philippine tertiary hospital
1University of the Philippines - Philippine General Hospital
Background: Pulmonary embolism (PE) continues to be the leading preventable cause of death and the third most common vascular cause of death among hospitalized patients. Literature however is significantly lacking on the incidence and clinical profiles of venous thromboembolism among Filipinos.
Methods: A retrospective single-center cohort study was conducted including all adult PE patients admitted in a tertiary government hospital from May 2022 to April 2023. Baseline clinical profile, IMPROVE bleeding risk, European Society of Cardiology (ESC) risk stratification, simplified pulmonary embolism severity index (sPESI), interventions, and outcomes (mortality, length of hospitalization, major bleeding, acute kidney injury) were investigated.
Results: Among the 102 patients included, the mean age was 53 years with 62.7% being females. The most common risk factors identified were immobilization >/= 5 days (81.4%), malignancy (72.5%), infection (77.4%) and prior deep venous thrombosis (38.2%). ESC risk stratification was as follows: 16.7% low, 57% intermediate-low, 17.6% intermediate-high, and 8.8% high risk. Low molecular weight heparin was given to 99% of patients. Oral anticoagulation was given in 77% of patients upon discharge with apixaban being the most commonly prescribed. No catheter-based thrombolysis and surgical embolectomies were recorded. Development of outcomes such as acute kidney injury including need for dialysis (42.2%), major bleeding (25.5%), stroke (7.8%), myocardial infarction (6.9%), were also investigated. Overall, in-hospital mortality rate was 30.3% and mean length of hospitalization was 30 days. Furthermore, an exploratory analysis using multivariable logistic regression revealed that elevated serum troponin levels above age-specific cut-offs (OR 7.74; 95% CI 1.53-39.0; p=0.01) could potentially increase the risk for mortality.
Conclusion: Patients with acute PE were younger but shared similar risk factor profiles when compared to those reported in Western literature. Subsequent studies with larger populations are recommended to investigate predictors for mortality and prolonged hospitalization.
Poster No. 63
Abstract No. 1789688
Carotid stenosis is associated with slower AAA growth
1Cleveland Clinic; 2Johns Hopkins University; 3Washington University; 4University of Cincinnati
Background: Atherosclerosis is a systemic condition that can affect multiple arterial territories. Although abdominal aortic aneurysms (AAA) are generally considered a consequence of atherosclerosis, it is not known if multi-vessel atherosclerosis is associated with increased AAA growth.
Methods: We identified patients with DM and at least two aortic Duplex studies and one carotid artery duplex between 2010 and 2020. A multivariable model was built to compare the rates of fast AAA growth between those with and without internal carotid artery (ICA) stenosis (defined as stenosis ⩾60%). The model was adjusted for age, initial diameter, sex, aspirin use, statin use, smoking, and hypertension. We also looked at the difference in rates of fast AAA growth in those with one and two vessel stenosis.
Results: In our cohort of 830 patients with AAA and a carotid duplex, the rate of fast AAA growth was 17.6% in patients without ICA stenosis and 10.8% in those with ICA stenosis (10.6% with one stenosed ICA, 11.4% with stenosis of both ICA). ICA stenosis was associated with a lower rate of fast AAA growth (OR 0.60, p = 0.03). There was no significant difference in rates of fast AAA growth between those with one or both ICAs affected.
Conclusion: In our cohort of patients with AAA, ICA stenosis was associated with slower AAA growth. There was no difference in rates of fast AAA growth between patients who had one or two ICA disease. Further studies are warranted to replicate and explore the findings of this study.
Poster No. 64
Abstract No. 1788251
Symptom concordance analysis in relapsing giant cell arteritis
1Mayo Clinic; 2Parkview Medical Center; 3Clinica Alemana
Background: Relapse is common in patients with giant cell arteritis (GCA). A relevant question for patients and providers is whether the initial symptoms at GCA diagnosis will be present at the time of relapse or whether other symptoms may manifest.
Methods: A 510-patient aggregate of 3 GCA cohorts was analyzed. Clinical symptoms at initial presentation, first relapse and second relapse were grouped into 5 categories: constitutional, musculoskeletal (MSK), cranial (non-visual), visual, and large vessel (LV). Patients could have more than 1 category at each time point. Conditional probabilities were calculated.
Results: 303/510 (59%) patients had at least 1 relapse and 160/510 had at least 2 relapses. 20% of patients presented with a symptom category on first relapse that was not present at baseline. Conditional probabilities of symptoms at a later stage according to presence or absence of symptoms of an earlier stage are shown in the Table. No patient without cranial symptoms at baseline developed visual symptoms at first or second relapse. The probabilities of specific symptom categories repeating themselves on first relapse if present at baseline were: 27% for constitutional, 57% for MSK, 56% for cranial, 13% for visual, and 44% for LV.
Conclusion: 1 in 5 patients reported a symptom discordance between baseline and first relapse. Visual relapse probability was higher if visual symptoms were present at a previous stage. Providers should educate patients on the entire spectrum of GCA symptoms to be aware of.
Conditional probabilities of given symptom category at first relapse according to presence or absence of baseline symptom category (A), conditional probabilities of given symptom category at second relapse according to presence or absence of baseline symptom category (B), and conditional probabilities of given symptom category at second relapse according to presence or absence of first relapse symptom category (C).

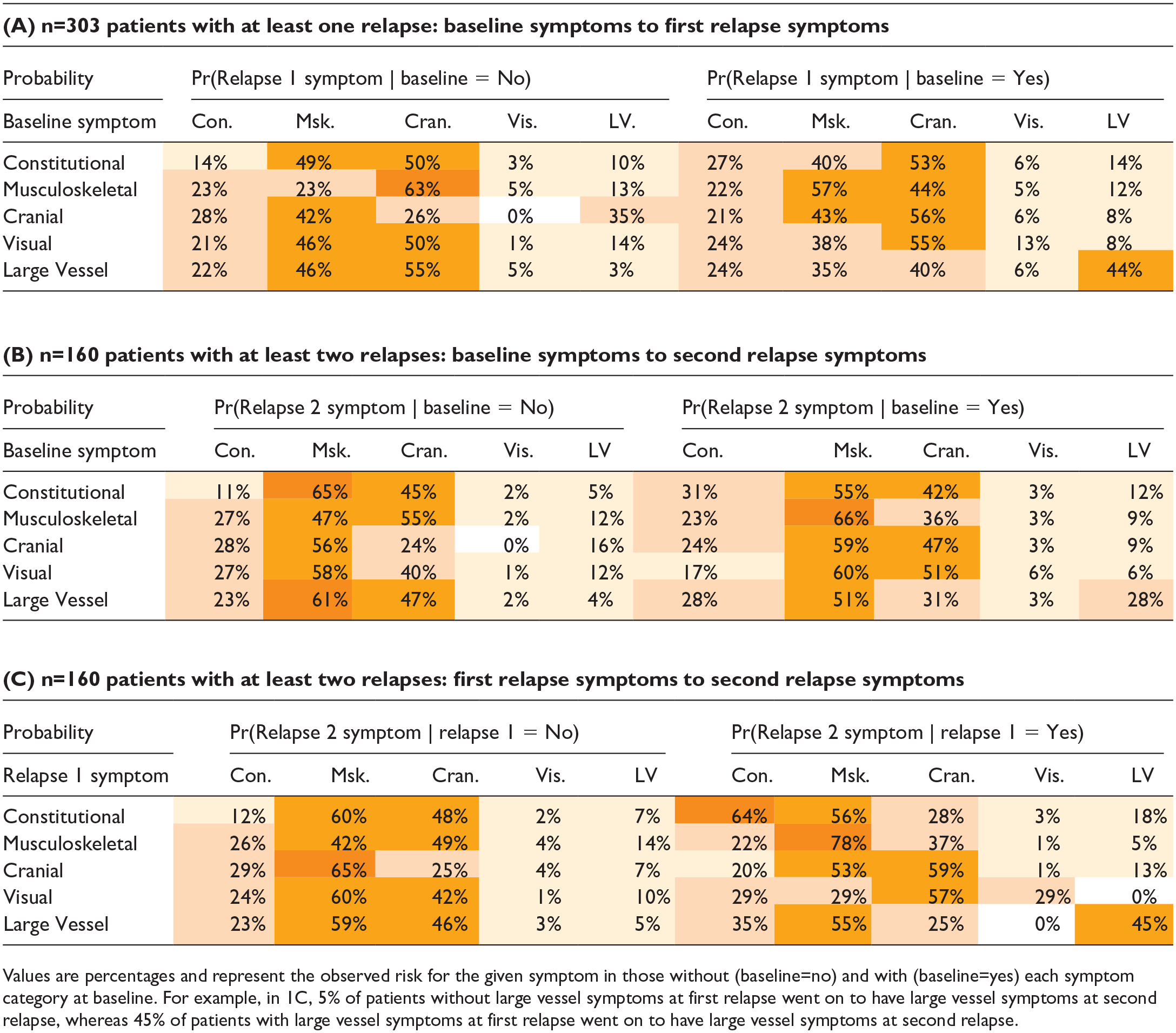
Poster No. 65
Abstract No. 1788324
Qualitative experiences with implementing an outpatient PE pathway
1University of Michigan
Background: Many low-risk pulmonary embolism (PE) patients can be safely managed from the emergency department (ED) with outpatient oral anticoagulation, yet this practice is rare in the United States. Barriers and facilitators to outpatient PE pathways have been previously described, but the qualitative implementation experience with such pathways is not understood.
Methods: An institution-approved ED low-risk PE outpatient management pathway was developed. Pre- and post-implementation semi-structured interviews were conducted with ED clinicians to understand barriers, facilitators, and practical challenges to the pathway while simultaneously guiding iterative modifications.
Results: 10 pre-implementation and 10 post-implementation interviews were conducted with ED clinicians including physicians, residents, and advanced practitioners. Outpatient management barriers included patient selection issues, care-coordination, PE diagnosis stigma, health literacy, social support, concomitant illness, and unfamiliarity with discharge options. Facilitators included institutional support, short-interval follow-up, ancillary support, and departmental education. Post-implementation interviews revealed challenges with patient identification, care-coordination, follow-up, and anticoagulant prescription, all corrected by iterative pathway modifications.
Conclusion: Iterative clinician interviews streamlined the experience of implementing an ED low-risk PE outpatient management pathway.
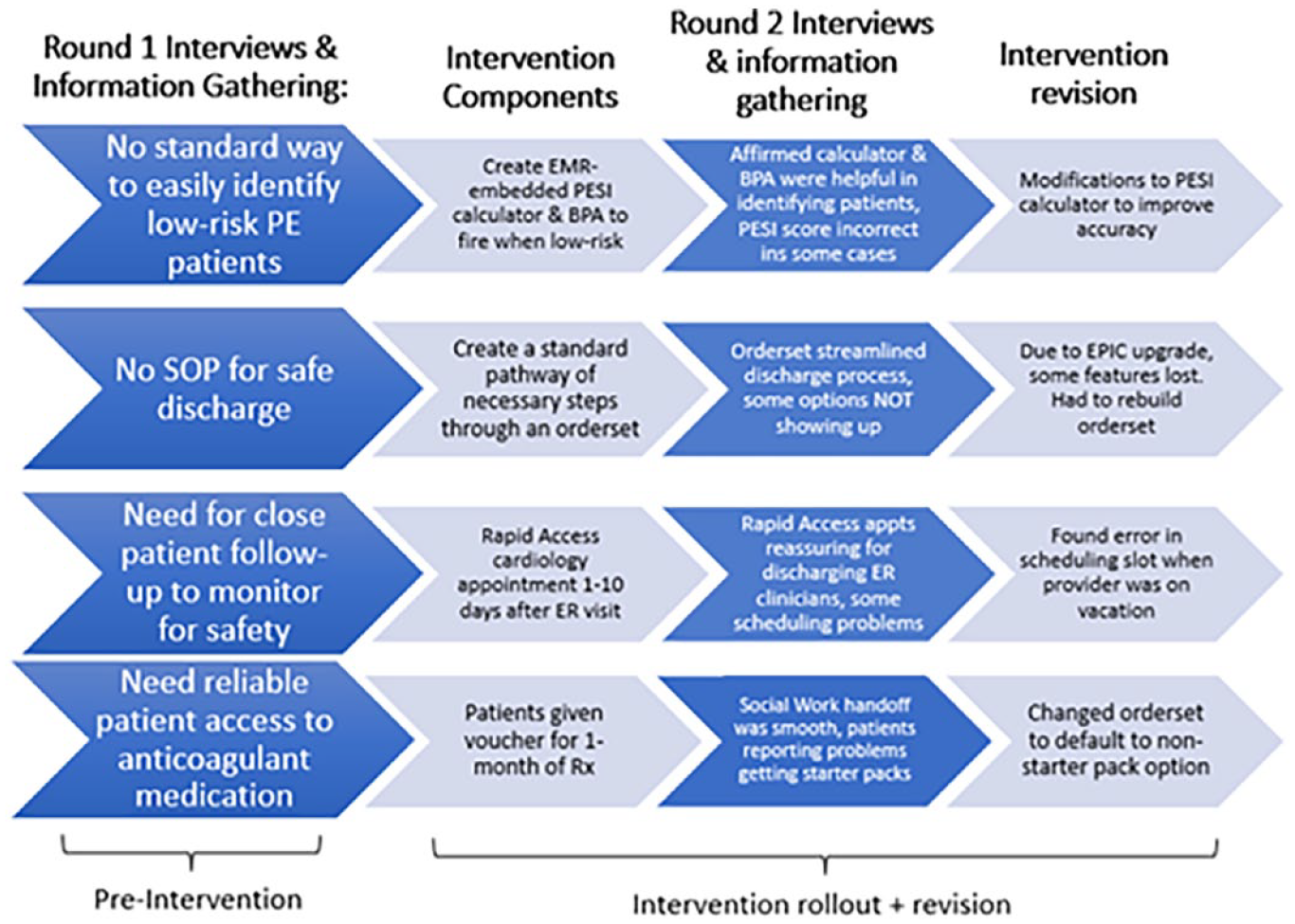
Challenges identified during pathway rollout, and process modifications implemented to improve clinician and patient experience with ED-based low-risk PE outpatient management pathway.
Poster No. 66
Abstract No. 1788402
Community exercise impact on functional outcomes in PAD
1University of Minnesota; 2University of Minnesota School of Nursing; 3University of Colorado School of Medicine
Background: PAD is an atherosclerotic disorder affecting 8-12 million people that can significantly limit walking ability and health-related quality of life (HRQoL). Community exercise training (CET) using supervised exercise training (SET) components and experiential knowledge of patients has been demonstrated to improve walking performance outcomes in patients with PAD. This study determined the impact of a CET program using SET elements and input from patients with PAD on functional outcomes and HRQoL.
Methods: A randomized controlled trial of CET for 12 weeks was conducted in patients with PAD (intervention: n=22; control: n=22). The current CET program included elements of training, monitoring, and coaching with additional program design modifications using formal feedback from a separate group of patients with PAD (barriers and facilitators to exercise). Control patients received upfront advice to increase their volume of walking. Functional outcomes were assessed using the Short Physical Performance Battery (SPPB) which included: 1) balance, 2) 4 m gait speed at normal and fast pace, and 3) a repeated stand chair test. HRQoL was evaluated using the Medical Outcomes Study Short Form 36-item (SF-36) questionnaire mental and physical component subsections.
Results: Time to complete the fast pace 4 m gait speed test improved significantly from baseline to 12 weeks for intervention vs. control patients (mean±SD: -0.27±1.11 vs. +0.24±0.34 s, p=0.046). However, no differences in change scores were found for other SPPB functional outcomes. Change in SF-36 mental and physical component scores were greater for intervention vs. controls (mental component: +2.5±6.8 vs. -1.6±5.7%; p=0.03; physical component: +2.2±3.7 vs. -1.1±5.8%; p=0.03).
Conclusion: CET programs that incorporate SET elements in addition to designing the program through the lens of patients with PAD, may be beneficial for improving functional and HRQoL outcomes. Prescribing exercise programs that occur in home and community settings, informed by patient feedback, may bypass barriers to SET programs and thereby improve the health of patients with PAD.
Poster No. 67
Abstract No. 1788354
Single versus dual antiplatelet therapy following PVI
1Henry Ford Hospital; 2Maine Medical Center; 3Spectrum Health; 4Frederik Meijer Heart and Vascular Institute; 5Yale University School of Medicine
Background: The best antiplatelet therapy following endovascular peripheral vascular intervention (PVI) remains understudied. While proponents of dual antiplatelet therapy (DAPT) believe that it offers an advantage over single antiplatelet therapy (SAPT), there is a paucity of data to support this contention. This study aims to compare the outcomes of SAPT and DAPT following PVI.
Methods: Patients receiving PVI for lower extremity peripheral arterial disease between 2004-2019 were identified in the Vascular Quality Initiative (VQI). Patients were divided based on the antiplatelet regimen used post-PVI. Exclusion criteria included arrhythmia, preoperative or discharge anticoagulation, and cases involving concomitant arterial procedures. Multivariate Cox-regression analysis was done to evaluate the independent association of antiplatelet therapy with the primary outcomes of amputation, reintervention, major adverse limb events (MALE), and mortality.
Results: Of 108,896 patients included, 31,225 (29%) received SAPT whereas 77,671 (71%) received DAPT. Patients treated with DAPT were more likely to have coronary artery disease (34.7% vs 24.9%, p< 0.001), prior PVI (26.1% vs 19.3%, p< 0.001), prior PCI (28.3% vs 17.0%, p< 0.001), and prior CABG (21.6% vs 15.6%, p< 0.001) compared to those treated with SAPT. At one year, the rate of reintervention was similar between the two groups (SAPT 14.7% vs DAPT 14.5%, p=0.549). Patients treated with DAPT had a lower rate of amputation (4.2% vs 5.2%, p< 0.001) and MALE (17.5% vs 18.7%, p=0.010) at 1-year compared to those on SAPT. 1-year mortality was also lower for patients on DAPT (6.2% vs 7.1%, p< 0.001). On Cox-regression analysis, patients on DAPT had a 14% lower hazard of amputation (HR 0.86, 95% CI 0.77-0.97) and 8% lower hazard of MALE (HR 0.92, 95% CI 0.87-0.97) compared to those on SAPT. No differences were observed regarding reintervention and mortality.
Conclusion: Patients placed on DAPT post-PVI demonstrated lower incidence of amputation and MALE than those on SAPT. This study provides evidence favoring DAPT as a more effective antiplatelet regimen following PVI. A randomized controlled trial is needed to better characterize this relationship.
Poster No. 68 – Withdrawn
Poster No. 69
Abstract No. 1788161
Outcomes using a dedicated ivc filter tracking system
1Baptist Health; 21. William Carey University College of Osteopathic Medicine
Background: IVC filter retrieval rates remain low despite national efforts to increase the rates of removal. The purpose of this study was to report 12-month outcomes from the usage of a dedicated IVC filter software (Filter Tracker (FT) VIR systems, Little Rock, AR, USA).
Methods: This study is a multi-site retrospective evaluation of 112 removable IVC filters that were placed between January 2021 and December 2021.
Results: 100% of filters had documented outcomes. The average first patient contact date was 70.8+/-35.2 days after filter placement. The average filter dwell time was 195.9+/-109.9 days. 48%(n=54) of the patients were candidates for filter removal. Of these, 53%(n=29) had their filters removed at the time of analysis. Overall, 26%(n=29) of all filters were removed. 19%(n=21) filters were made permanent. 11%(n=12) of patients were pending reassessment at time of analysis. 10%(n=11) of patients required registered letters to be sent due to recurrent non-response. 33%(n=37) of patients were deceased at the time of analysis. 2%(n=2) of patients were scheduled to have their filter removed in the near interim.
Conclusion: A dedicated filter tracking software can play a pivotal role in managing the highly co-morbid IVC filter patient population.
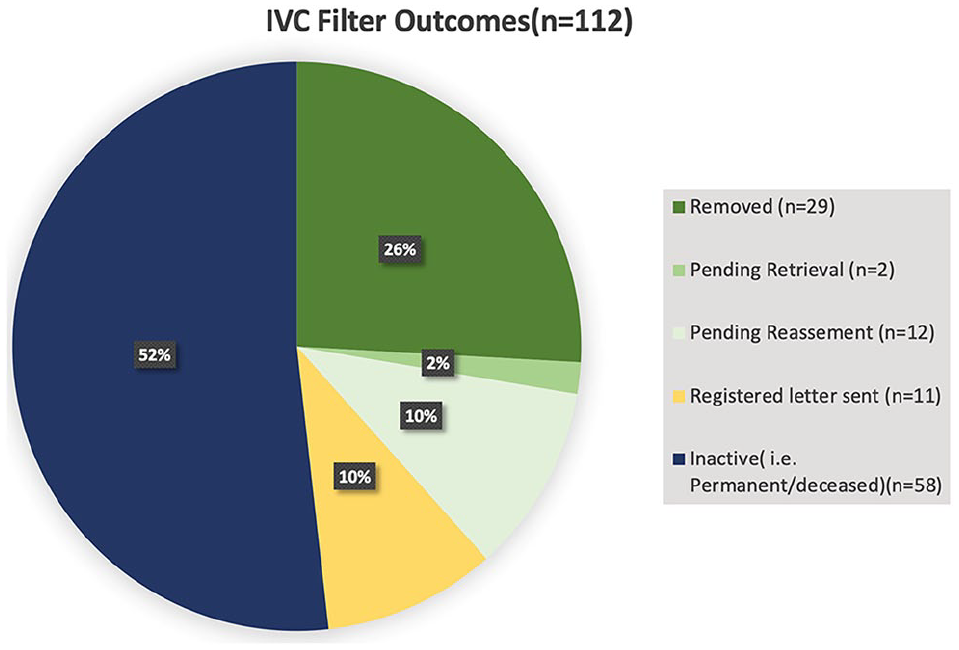
Poster No. 70
Abstract No. 1795652
Use of thermographic imaging in superficial venous disease
1Jobst Vascular Institute
Background: Thermographic imaging allows visualization of superficial veins that have influx of higher temperature blood from deep veins. This phenomenon can result from perforator reflux, or junctional reflux in saphenous veins. The place of this modality in the toolbox of the venous surgeon remains to be determined. The aim of this case series is to demonstrate five clinical scenarios when the use of thermographic imaging resulted in changes in the treatment plans or facilitated physician-patient interaction.
Methods: This is a case series of five patients with superficial venous reflux.
Results: These five cases demonstrate different clinical scenarios when thermal imaging changed the treatment plan for patients with superficial venous disease or facilitated physician-patient interaction, thereby improving patient compliance and modifying treatment recommendations.
Conclusion: Thermographic imaging is a useful practical tool for managing patients with superficial venous disease.
Poster No. 71
Abstract No. 1788297
Prescription of dual pathway inhibition (DPI) in PAD patients underwent lower extremity revascularization (LER)
1CPC Clinical Research, University of Colorado; 2CPC Clinical Research, University of Colorado, Denver Health and Hospital Authority
Background: VOYAGER PAD demonstrated the favorable benefit/risk of dual pathway inhibition (DPI) after lower extremity revascularization (LER) and was approved by the FDA in 2021. Despite benefits, the real-world prescription of DPI, including aspirin and low-dose rivaroxaban, may be suboptimal.
Methods: Encounters with a diagnosis of PAD undergoing LER were selected from TriNetX from Jan 2022 to Dec 2023 in the University of Colorado health system. The key inclusion and exclusion criteria were age ⩾ 50 and successful LER, without known exclusions (atrial fibrillation, venous thromboembolism, CKD stage V or dialysis, recent acute coronary syndrome, intracranial hemorrhage, transient ischemic attack, or history of malignancy).
Results: There were 780 encounters for PAD undergoing LER in 2022 and 2023 of which 420 (54%) qualified for VOYAGER PAD. Overall, dual antiplatelet therapy (DAPT) with aspirin and clopidogrel was most frequent (figure), followed by DPI (with or without clopidogrel), aspirin monotherapy, and no recorded antithrombotic. Use of DPI increased 8% in absolute terms (57% relative) from 2022 to 2023 with the majority in 2023 without clopidogrel. Use of DAPT and aspirin monotherapy both decreased.
Conclusion: In one health system DPI remains underutilized and DAPT remains the most frequent regimen after LER; however, the use of DPI is increasing. These data highlight opportunities for implementation science and optimization of antithrombotic therapies after LER.
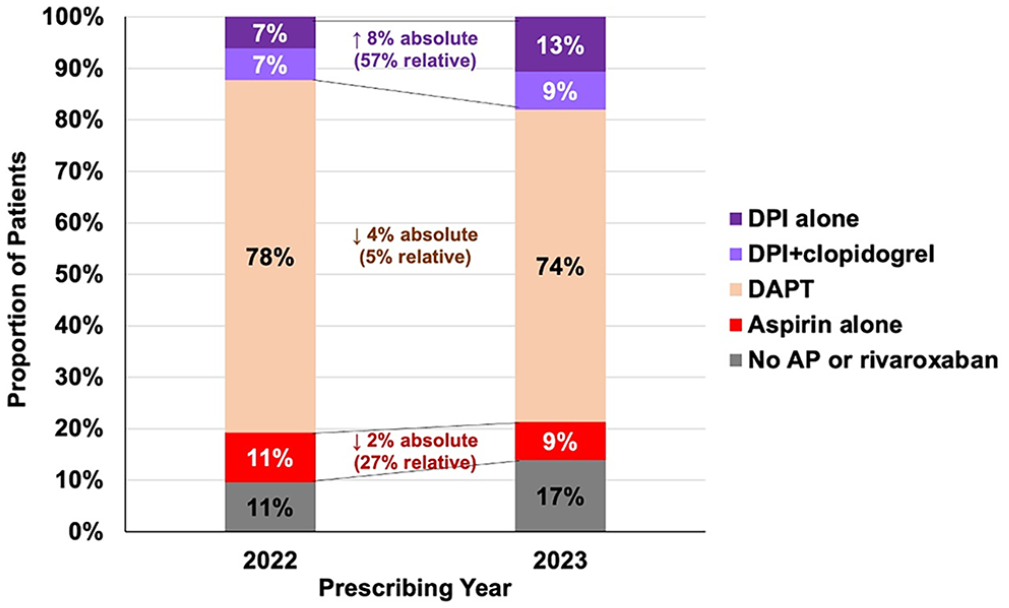
Poster No. 72
Abstract No. 1795240
The association between epilepsy and venous thromboembolism
1University of Virginia School of Medicine; 2University of Virginia
Background: Epilepsy has been shown to be associated with risk factors including obesity, reduced mobility, and frequent hospitalizations, of which are also predisposing factors for venous thromboembolism (VTE). Despite similar risk factors, the association between epilepsy and VTEs has not been well-established.
Methods: This retrospective cohort study investigated the relationship between epilepsy and VTE in patients seen at the UVA Health System using the TriNetX Live Network which provided access to de-identified, aggregated electronic medical records. All patients were over the age of 18 years, had an encounter at a UVA Health facility between September 28, 2010 and March 14, 2024, and did not have any diagnosis for malignancy, hypercoagulability states, Dravet disease, or absence epilepsy as identified by International Classification of Disease, tenth revision codes.
Results: A total of approximately 1,306,000 patients were screened, of which roughly 12,305 (0.94%) of patients had a diagnosis of epilepsy and 14,773 (1.14%) of patients had a VTE event. The odds ratios of an individual having a diagnosis of epilepsy to have any VTE occurrence after the initial diagnosis was 2.9 (95% Confidence Interval [CI]: 2.6, 3.3) when adjusting for both age and sex. Adjusting for only sex, patients between 35 and 54 years had the highest odds of VTE at 3.4 (95% CI: 2.9-4.2). Adjusting for age, female patients had higher odds of VTE at 3.0 (95% CI: 2.6 - 3.5), while men had lower odds at 2.8 (95% CI: 2.4 - 3.3).
Conclusion: A diagnosis of epilepsy is associated with a statistically significant increased odds for VTE regardless of age or sex. Further investigation into the correlation of epilepsy and VTE, as well as use of prophylactic anticoagulation in patients with epilepsy is warranted.
Poster No. 73
Abstract No. 1795624
Copay impact on elderly vascular patients’ medical compliance
1College of Medicine, University of Arizona; 2Xavier College; 3Midwestern University
Background: Patient compliance with medications and clinic visits may influence outcomes of cardiovascular disease management. Copay can influence compliance particularly in elderly patients with limited financial resources.
Methods: We surveyed 90 patients attending a vascular clinic in a retiree community in Maricopa County, Arizona. Demographics, socioeconomic status, type of insurance and copay, impact of later on compliance with prescription medication, clinic visits, diagnostic and interventions was recorded.
Results: (M/F 55/45%), (average age 75.3), (married 56%/widow-single-divorced 44%)(White 85%/ Latino 11%/ AfriAm 4%). 65/88 (74%) patients had copay with 52% stating it affects compliance with medications or clinic visits/testing, while only 9% of 23 no copay patients expressed non-compliance. Personal financial reserve/month(<$500), calculated as money remaining to patient after all expenses paid had no effect on compliance overall, however significantly affected copay patients’ compliance (p<.05).
Conclusion: We conclude that current models of copay significantly impact compliance with medications and clinic visits in elderly patients with vascular disease and consequently may affect outcomes of their disease management.
Poster No. 74
Abstract No. 1774476
Utilization of endovascular thrombectomy in ESKD and stroke
1University of Kansas Medical Center; 2University of Missouri at Kansas City; 3Khyber Medical University
Background: Patients with end-stage kidney disease (ESKD) have a higher risk of stroke compared to the general population. There is limited data on the use of endovascular thrombectomy (EVT) in these patients. This study aimed to investigate the use of EVT in patients with ESKD and acute ischemic stroke (AIS) using data from the National Readmission Database (NRD) from 2016 to 2020.
Methods: We identified patients with ESKD and AIS using relevant ICD-10-CM codes from the NRD from 2016 to 2020. We then identified patients who underwent tissue plasminogen activator (TPA) or EVT. We compared the rates of EVT and TPA use in ESKD patients and non-ESKD patients. We also looked for trends in EVT use over time.
Results: A total of 2,535,777 patients with AIS were identified, of whom 37,799 had ESKD. The median age was 71 years old in the ESKD group and 67 years old in the non-ESKD group (p < 0.001). Female distribution was 50% in both groups. Comorbidities such as coronary artery disease (45% vs 28%), hypertension (94% vs 27%), atrial fibrillation (29% vs 26%), peripheral arterial disease (14% vs 9.8%), and hyperlipidemia and diabetes (67% vs 22%) were more common in the ESKD group compared to non-ESKD ( p < 0.001) Patients with ESKD were less likely to receive EVT or TPA compared to non-ESKD patients (2.5% vs. 3.6% for EVT, 8.1% vs. 9.2% for TPA; p < 0.001). Inpatient mortality was higher in the ESKD group (9.3% vs. 4.3%; p < 0.001). From 2016 to 2020, there was an increasing trend in EVT use in the non-ESKD population (p < 0.001), but no such trend was observed in the ESKD group (p = 0.46). Similarly, ESKD patients with AIS who has received TPA were more likely to have hemorrhagic stroke in the same hospitalization compared to non-ESKD 5.3% vs 4.7%, p< 0.001.
Conclusion: Patients with ESKD and acute ischemic stroke have very high mortality rate, yet the utilization of the EVT in these patients is lower compared to general population. Further research is needed to address this disparity in these high-risk patients.
Outcomes and interventions among patients with acute ischemic stroke in ESKD and Non-ESKD populations.

LOS: Length of Stay, EVT: Endovascular Thrombectomy, TPA: Tissue Plasminogen Activator.
Poster No. 75
Abstract No. 1774648
VTE joust: tech versus script in cancer screening
1The Medical City
Background: Venous thromboembolism (VTE) poses a significant health threat with notable morbidity, mortality, and healthcare costs. Our institution has implemented a VTE risk stratification tool integrated in our institution's electronic health records (EHRs). Our study aims to assess the efficacy of this tool in terms of improving compliance with VTE prophylaxis among cancer patients.
Methods: The study was a retrospective cohort study, comparing those screened electronically to those who used a written tool. The study included cancer patients from January 2021 to December 2022, aged 18 years old and above, were not on any form of anticoagulation and did not have any contraindication to mechanical and chemoprophylaxis for VTE.
Results: Our study of 261 hospitalized cancer patients screened 130 electronically using the VTE screening tool integrated into hospital EHRs and 131 through a written form. Although both groups had similar baseline characteristics and laboratory parameters, VTE prophylaxis use was low—3.08% in the electronic group and 3.82% in the written form group. This concurred with the literature that VTE prophylaxis is underused. Failure modes in VTE prophylaxis systems should be considered. The lack of order sets and prompts are failure modes among VTE prophylaxis systems, according to the Agency for Healthcare Research and Quality. Our electronic screening tool lacked this, hindering users' ability to translate risk assessments into thromboprophylaxis, resulting in low utilization despite high VTE risk, improved screening accuracy and acceptable bleeding risk. Furthermore, our system, which was designed for resident screening and coordination with attending physicians (APs), received low utilization from APs (1.54%), potentially contributing to its failure to achieve desired outcomes in improving VTE prophylaxis adherence.
Conclusion: The study revealed that screening electronically did not impact the utilization of guideline-directed prophylaxis. Addressing potential system failure modes is crucial for maximizing adherence to VTE risk screening and appropriate prophylaxis, ensuring optimal use of guideline-directed measures, and providing adequate care for cancer patients.
Poster No. 76
Abstract No. 1753721
Characterizing fibromuscular dysplasia and spontaneous coronary artery dissection
1University of Michigan
Background: Fibromuscular dysplasia (FMD) and spontaneous coronary artery dissection (SCAD) are two female sex-biased arteriopathies for which epidemiological patterns remain poorly defined. We sought to leverage an electronic health record (EHR) system to investigate the prevalence and clinical manifestations of both diseases.
Methods: Individuals within the Michigan Medicine (MM) EHR system, MiChart, were queried for ICD-10 codes I77.3 and I25.42 to identify cases of FMD and SCAD, respectively. EHRs were manually reviewed and FMD was confirmed if radiographic evidence was available while SCAD was confirmed if high clinical suspicion or catheterization reports documenting SCAD were available. In those confirmed to have FMD, data on vascular bed involvement and vascular complications was also abstracted.
Results: Among 5,148,455 patients within MiChart between 2000-2023, 753 had an ICD code for FMD and 349 for SCAD. Of these initial cohorts, 77.3% and 50.9% were confirmed to have FMD and SCAD, respectively. Iatrogenic dissections and coronary atherosclerosis were the most common diagnoses in disqualified SCAD cases while inconclusive radiographic evidence was the most common reason for FMD case disqualification. Based upon the final confirmed case counts, the estimated prevalence for FMD and SCAD were 11.3 and 6.9 cases per 100,000 individuals, respectively. The final confirmed FMD cohort was 89% female and 86% white while the final SCAD cohort was 88% female and 86% white. In the FMD cohort, 34% had renal artery FMD, 45% had cervical artery FMD, and 21% had FMD involvement of both arterial beds. Among those with FMD, 53% had a vascular complication, with the most common being intracranial aneurysms, which occurred in 14.4% of the cohort.
Conclusion: In the current study’s EHR-based query, the prevalence of FMD and SCAD within a tertiary referral care center, the MM Health System, appears consistent with results from prior studies. Further, vascular complication rates were high among patients with confirmed FMD. Additional large-scale EHR- and population-based studies are ideally needed to better ascertain the true prevalence of both arteriopathies and to this aim, we report a pipeline which can be implemented within other EHR systems.
Poster No. 77
Abstract No. 1787467
Claudication prevalence in Filipinos with peripheral artery disease
1St. Luke’s Medical Center, Dr. HB Calleja Heart and Vascular Institute; 2St. Luke's Medical Center, Quezon City
Background: Peripheral Artery disease (PAD) affects over 200 million adults worldwide. There has been disproportionate prevalence and outcomes of PAD as most patients do not present with stereotypical claudication symptoms which further underestimates the disease burden. Despite its huge impact on adverse clinical outcomes and the long-term socioeconomic burden, PAD is still under-recognized and understudied, especially in most developing countries. In this study, we aimed to provide epidemiological data on symptomatology and clinical variables related to peripheral artery disease in the Filipino population.
Methods: A single-center, retrospective study was conducted and included all adult patients who underwent arterial duplex scans at the vascular laboratory from 2020 to 2022. Electronic health records on clinicodemographic characteristics were identified and thoroughly reviewed.
Results: Between 2020-2022, a total of 169 patients had peripheral artery disease with hemodynamically significant (>50%) stenosis. The prevalence of claudication in those with hemodynamically significant stenosis was 17.2%. The presence of chronic kidney disease was the only factor that significantly affected the prevalence of claudication in both the univariate and multivariate analyses (OR 2.708, 0.850-8.626, p=0.082 and OR 5.091, 1.169-22.169, p=0.030, respectively). In contrast, claudication was not statistically affected by sex, smoking history, body mass index, hypertension, and diabetes mellitus.
Conclusion: The prevalence of claudication in Filipino patients with hemodynamically significant stenosis was 17.2% in this retrospective study. Larger sample sizes and studies across multiple local centers are recommended to better view the association of clinical characteristics with claudication and hemodynamically significant peripheral artery disease that will contribute to the existing symptomatology landscape in literature.
Poster No. 78
Abstract No. 1795810
Analysis high-risk Jordanian women with vascular risk factors
1The University of Jordan; 2University of Jordan; 3Istishari Hospital; 4Muath University
Background: The exact burden of vascular disease in the Middle East (ME) remains unknown, however, high prevalence of vascular disease risk factors has been reported. Moreover, high burden of atherosclerotic cardiovascular disease (ASCVD) in females has been reported. Therefore, the key to reducing the vascular disease burden is risk factor modification. Higher prevalence of vascular risk factors (RFs) specifically hypertension (HTN) and hypertensive disease of pregnancy (HDP) has been identified among female patients in ME with ASCVD.
Methods: Our Study included females, age (18-50 years) with ASCVD and age-matched control group. We enrolled subjects from 12 centers (August 2021 to October 2023) in Jordan and Gaza.
Results: 618 women enrolled (mean age 44.0±4.5 years), 305 (48.6%) were found to have HTN and/or HDP, and 322 (51.4%) did not . Compared with women with no HTN/HDP, the HTN/HDP group had prevalence of ASCVD (44.9% vs. 22.4%), diabetes (33.1% vs. 9.6%), and obesity (52.1% vs. 35.7%), consecutively. All P values< 0.05. Within subjects with reported RF, in addition to the higher prevalence of HDP, there was a higher prevalence of preterm delivery, however gestational diabetes, persistent weight gain, premature menopause, and polycystic ovary syndrome were of no significant difference. Regarding the psychosocial factors, lower socioeconomic class, less educational degree, obesity, sedentary lifestyle has been observed in the HTN/HDP group. On multivariate analysis, HTN was found to be an independent predictor of ASCVD (Odds ratio 2.15, 95% CI 1.41-3.30, p< 0.001).
Conclusion: Based on our findings, HTN/HDP in females are more likely to have a worse clinical and psychosocial profile compared with those who do not. Therefore, early screening and management is crucial to improve overall prognosis of this patient’s group.
Poster No. 79
Abstract No. 1795831
Epidemiology of chronic thromboembolic pulmonary hypertension
1University Hospitals Cleveland Medical Center
Background: Chronic Thromboembolic Pulmonary Hypertension (CTEPH) is an important clinical entity that is often underdiagnosed, necessitating a comprehensive understanding of its epidemiological characteristics. This study explores the prevalence, demographic patterns, and incidence rates of CTEPH within a large patient cohort.
Methods: A retrospective analysis was conducted on 85,204,225 patients available in the TriNetX database between October, 2017 and March, 2023. Chi-squared tests were used to assess the significance of demographic disparities in CTEPH prevalence across gender, race, and ethnicity categories. T-test was used to compare the mean ages in both groups.
Results: Among the cohort of 85,204,225 patients, 8,711 individuals were identified with CTEPH, resulting in a prevalence of 10.2 per 100,000 persons. Females accounted for 53.03% of CTEPH cases. Notably, the prevalence of CTEPH was significantly higher among patients who are black (18.7 per 100,000) as compared to patients of all other races (p< 0.05) and similar between patients who are white, Asian and Native Hawaiian or Other Pacific Islander. The mean age of CTEPH patients was 65 years (SD= 16), significantly higher than the general population (mean: 46, SD = 25) (p< 0.0001). The highest incidence rate occurred in the 75-79 age group (29 per 100,000).
Conclusion: This study highlights the demographic patterns and incidence rates for CTEPH, with elevated prevalence among individuals who are of older age, are female or are black. The findings emphasize the importance of heightened clinical vigilance and targeted interventions in these high-risk demographic groups to mitigate the burden of CTEPH effectively.