
Abstract

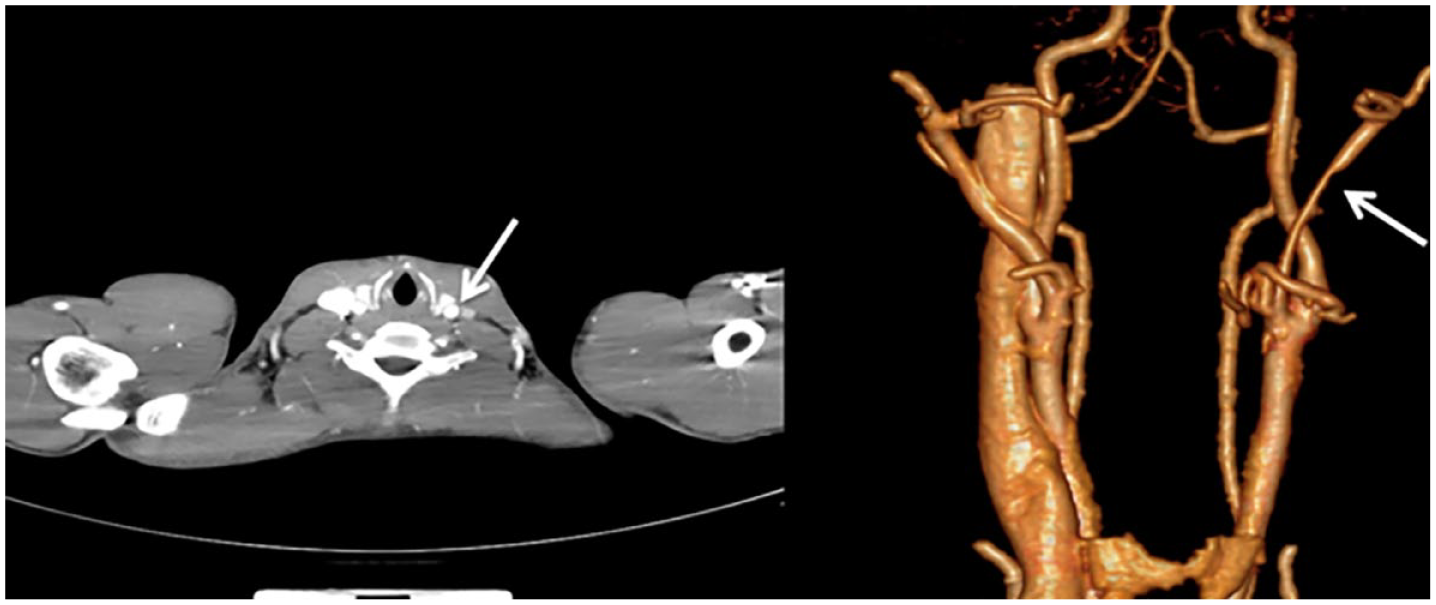
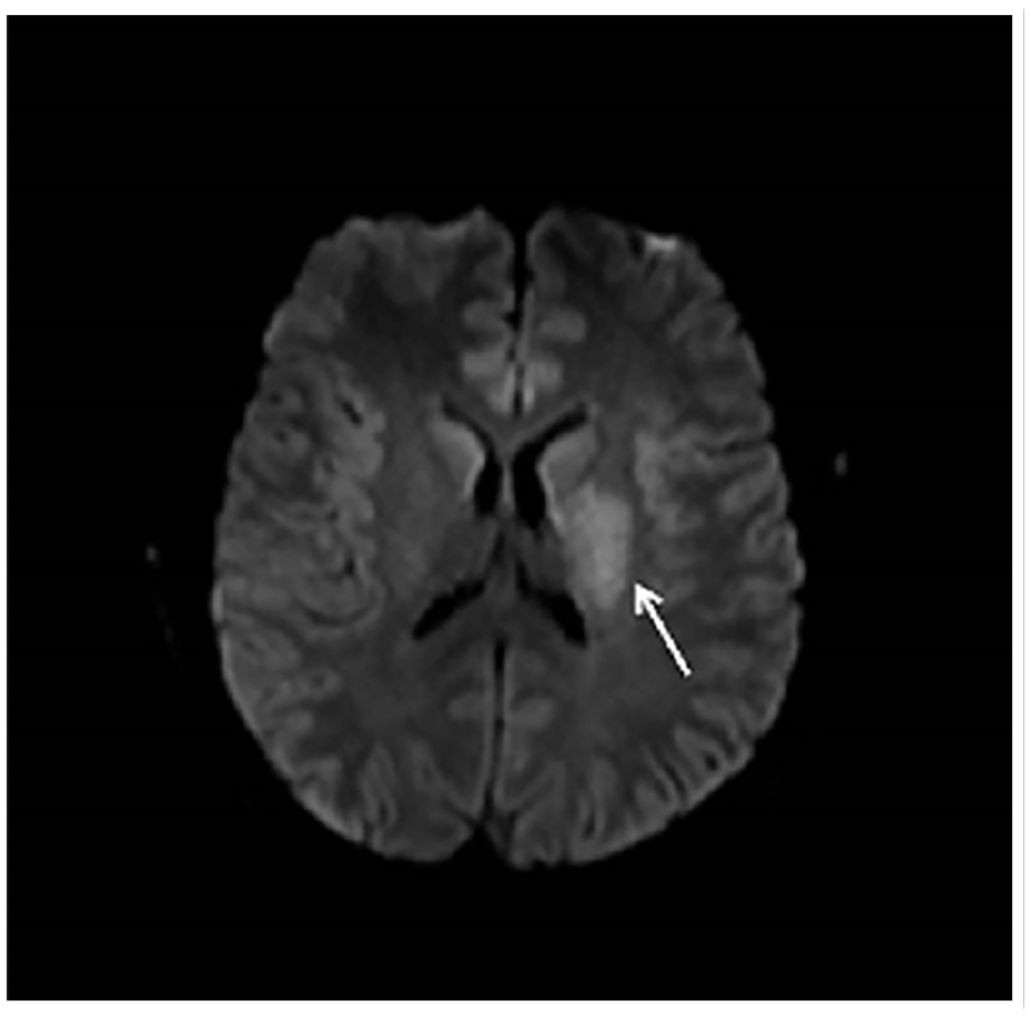
A previously healthy 27-year-old man presented with sudden right limb movement disorder and then fell to the ground. The patient sprained his neck a day earlier and subsequently experienced neck discomfort. He was conscious and verbal on admission. On admission the patient underwent computed tomography (CT) of the brain, and no bleeding or infarct foci were found. The patient walked unsteadily, and neurological examination showed muscle strength of the right upper limb was grade 4 and less than grade 5 in the right lower limb, no dystonia in the right lower limb, and positive Babinski sign and Chaddock sign of the right lower limb. After about 36 hours, the patient presented with flattening of the right nasolabial fold and right deviation of the tongue. Ultrasound (US) revealed a separated intimal flap (Panel A, arrows) and CT angiography (CTA) revealed luminal stenosis of the left external carotid artery (ECA) (Panel B, arrows). Diffusion-weighted imaging demonstrated a cerebral infarction in the left basal ganglia, corona radiata, and parietal lobe (Panel C, arrow). Subsequently, he underwent cerebral angiography and was finally diagnosed with left external carotid artery dissection (ECAD).
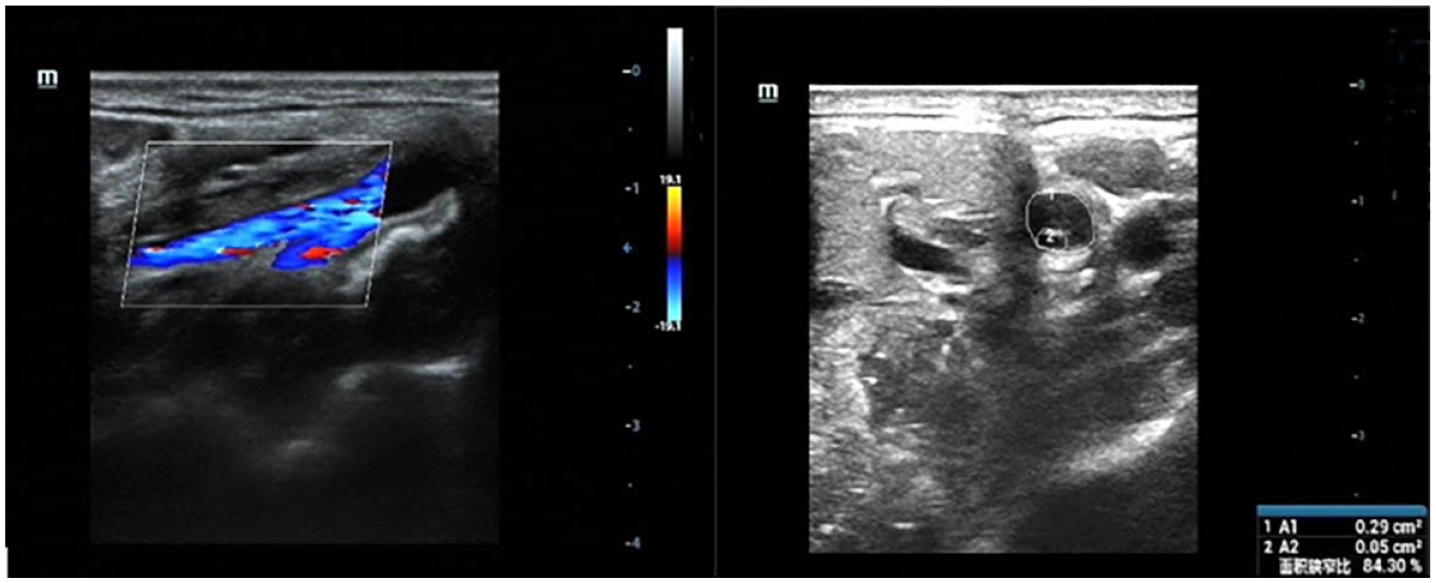
Carotid artery dissection (CAD) is a rare complication of head and neck trauma. Extracranial CAD occurs most frequently in the internal carotid artery (ICA). 1 The prevalence of ECAD is estimated to be less than 1% of all CAD, probably due to the special ultrastructure of the vascular wall of the ECA. 2 The imaging features of CAD can manifest as double-lumen sign, intramural hematoma, etc. Previous studies have reported that the double-lumen sign can increase the sensitivity of CAD diagnosis to 100%. However, isolated stenosis due to intramural hematoma decreases sensitivity to 80%. 3
The ECA delivers blood to the neck and face and is an important component of the cerebral collateral circulation. On the one hand, the ECA can make a meaningful contribution in up to 80% of patients with ICA stenosis or occlusion. 4 On the other hand, in the presence of a normal ICA, clinical symptoms rarely occur, even if the ECA is ligated. 5 Despite no significant abnormalities in the bilateral and other intra- and extracranial arteries, our patient still presented with cerebral infarction. We speculate that the patient’s stroke may have been caused by hemodynamic changes at the bifurcation of the common carotid artery and thromboembolization from the site of dissection in the ECAD through collateral flow to the brain versus via the patent ICA.
Footnotes
Note – the panels are in color online.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.