
Abstract
Introduction:
Carotid body tumors are rare neoplasms with malignant potential. We aim to follow up on our initial experience published in 2015 and compare the occurrence of complications and postoperative outcomes with the use of retrocarotid dissection (RCD) against the standard caudocranial (SCCD) technique.
Methods:
This was an observational, case–control study in which we analyzed all of the carotid body tumor resections performed from 1986 to 2022. Parametric and nonparametric tests were used accordingly. Statistical analysis was performed on Stata 17.
Results:
A total of 181 surgical procedures were included, mean age was 56 years (± 13.63), and 168 (93%) were performed in women. The mean medio-lateral diameter was larger in the RCD group (2.85 ± 1.57 cm vs 1.93 ±1.85 cm; p = 0.002) and presurgical embolization was more frequently performed in the SCCD group (27.5% vs 0.7%; p < 0.001). A total of 40 (22.09%) resections were performed using the SCCD technique. In contrast, in 141 (77.91%) procedures the RCD technique was used. The mean surgical time in the RCD group was lower (197.37 ± 70.56 min vs 232 ± 98.34 min; p = 0.01). No statistically significant difference was found between SCCD and RCD in terms of vascular lesions (n = 20 [11.04%], 15% vs 9%, respectively; p = 0.36), transient or permanent nerve injuries (25% vs 33%, respectively; p = 0.31), or mean intraoperative bleeding (SCCD: 689.95 ± 680.05 mL vs RCD: 619.64 ± 837.94 mL; p > 0.05).
Conclusions:
RCD appears to be a safe and equivalent alternative to the standard caudocranial approach in terms of intraoperative bleeding or vascular lesions, with a sustained, significant decrease in surgical time.
Introduction
Carotid body tumors (CBTs) are rare neuroendocrine neoplasms that originate from the carotid body, a highly vascularized chemoreceptor situated at the bifurcation of the common carotid artery. These tumors play a crucial role in maintaining the balance between oxygen (O2) and carbon dioxide (CO2) concentrations in the bloodstream. Although CBTs have a reported incidence of 1 in 30,000, 1 they represent the most common type of head and neck paragangliomas. 2
CBTs have variable etiologies, classifying them into three types: sporadic, familial, and hyperplastic. Hyperplastic CBTs are the most prevalent subtype and are commonly associated with chronic hypoxia, prevalent in populations residing at high altitudes and patients suffering from chronic obstructive pulmonary disease (COPD).1,3
The Shamblin classification, which describes the relationship between these paragangliomas and the carotid vessels, 4 is widely favored due to its ability to predict intraoperative technical challenges. 5 This classification aids surgical teams in decision-making processes. Vascular surgeons predominantly employ the standard caudocranial dissection (SCCD) technique to treat CBTs. 6 However, due to the complex surgical field in which these tumors are enclosed, complications such as nerve injury, hemorrhage, and stroke remain common.1,6
Furthermore, the occurrence of postoperative stroke appears to be directly associated with the Shamblin classification. 1 Given the limited experience that many surgeons have in treating CBTs, there is a pressing need for a more comprehensive understanding of the condition and safer surgical options to enhance patient outcomes.
This study aims to follow up on our initial experience published in 2015. 6 We present our 15-year experience (2008-2022) with the retrocarotid dissection (RCD) technique for CBT treatment and compare it to the SCCD technique in terms of intraoperative and postoperative complications.
Methods
This was an observational, retrospective, case–control study in which we analyzed all of the CBT resections that have been performed from 1986 to 2022. Data were obtained from medical records provided by our statistics department. We then divided the data by groups, depending on the surgical technique that was used; hence, retrocarotid dissection or standard caudocranial dissection. Furthermore, surgical outcomes were compared between techniques.
Continuous data were presented using central tendency measures. Parametric data were presented as means along their SD and nonparametric data were presented as medians along their IQR. Categorical data were reported as percentages.
For the statistical analysis, parametric and nonparametric tests were used accordingly. Finally, a Poisson regression model was performed. Data were analyzed on Stata 17 software (StataCorp LLC, College Station, TX, USA). For all tests, p < 0.05 was considered statistically significant.
Ethical approval of this study was granted by the local institutional ethic committee. All patients’ data were anonymized and de-identified before analysis to commit to the ethical principles of the Declaration of Helsinki.
Results
A total of 181 surgical procedures had been performed in our institution by the time we started our analysis. In terms of demographics, 168 (93%) were performed in women, the mean age was 56.12 years (± 13.63), and mean body mass index (BMI) was 27.87 kg/m2. Regarding comorbidities and demographics, no statistically significant differences were found between groups (Table 1).
Comparison of demographics and comorbidities between surgical techniques.
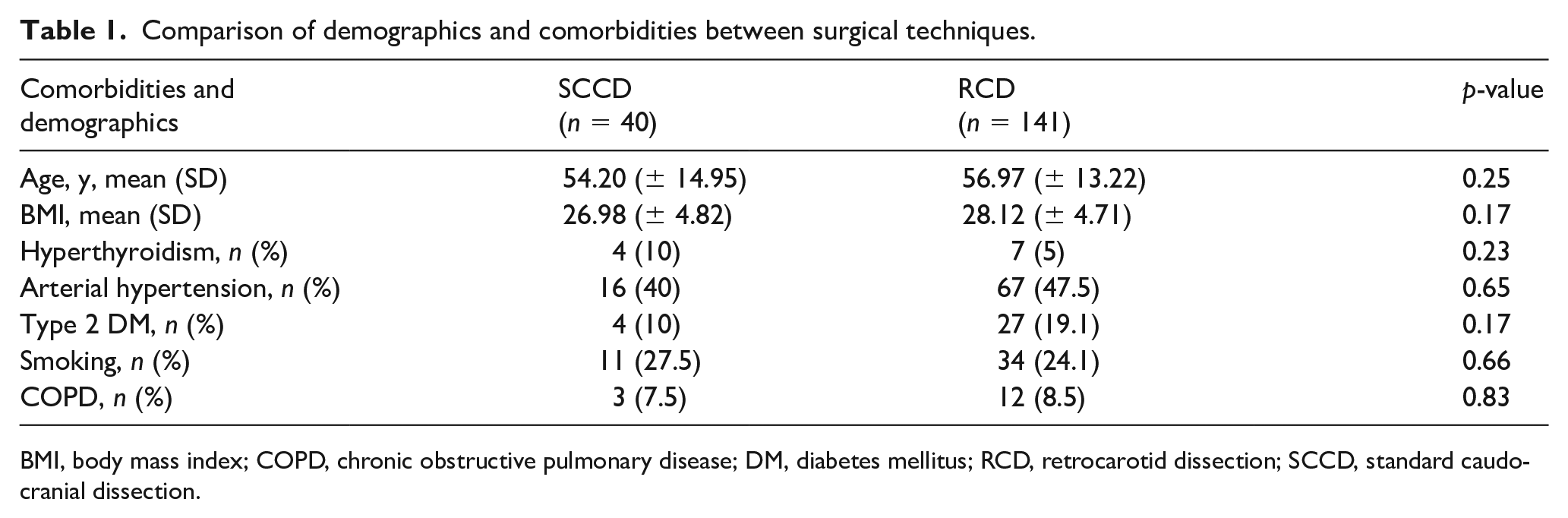
BMI, body mass index; COPD, chronic obstructive pulmonary disease; DM, diabetes mellitus; RCD, retrocarotid dissection; SCCD, standard caudocranial dissection.
In terms of clinical findings at presentation, 107 (59.11%) patients were symptomatic. The most common symptoms reported were pain (33.7%), any degree of dysphagia (17.67%), and headache (22.09%). Additionally, a neck mass was reported in 126 (69.61%) cases and patients presented more frequently with a left CBT (47.51%), with the incidence of right and bilateral CBT being 37.56% and 14.93%, respectively. Regarding time-to-diagnosis, a mean of 18 months (± 28.46) was evidenced.
Concerning surgical procedures, 40 (22.09%) were performed using the SCCD technique and the remaining 141 (77.90%) were executed using the RCD technique. In terms of Shamblin classification, 55 (39%) CBTs were classified as Shamblin II and 50 (34.46%) as Shamblin III in the RCD group; similarly, the majority of CBTs in the SCCD group were classified as Shamblin II (n = 10) or III (n = 21).
With respect to size of CBT (cephalo-caudal × medio-lateral × antero-posterior), the mean diameters were 3.57 × 2.65 × 2.64 cm in our sample. When divided by surgical technique, the medio-lateral size was significantly larger in the RCD group (2.85 ± 1.57 cm vs 1.93 ± 1.85 cm; p = 0.002). Additionally, the mean tumor distance to base of skull (DTBOS) was 2.07 ± 2.15 cm, and mean tumor volume was 9.36 ± 14.81ml. Furthermore, the SCCD group had a larger proportion of cases subjected to preoperative embolization (27.5% vs 0.7%; p < 0.001).
As for intraoperative observations, surgical time was significantly lower in the RCD group (197.37 ± 70.56 min vs 232 ± 98.34 min; p = 0.01). Regarding preoperative embolization (PE), no statistically significant differences were found in terms of bleeding (no PE: 675.77 ± 834.37 mL vs PE: 547.5 ± 642.53 mL; p > 0.05) or in surgical time (no PE: 212.32 ± 74.22 min vs PE: 188.58 ± 56.41 min; p > 0.05).
When describing postoperative outcomes, seven paragangliomas were classified as malignant tumors (3.8%) and one death ⩽ 30 days was documented in the RCD group. Additionally, no statistically significant difference was found between SCCD and RCD in terms of vascular lesions (n = 20 [11.04%]; 15% vs 9%, respectively; p = 0.36), transient or permanent nerve injuries (25% vs 33%, respectively; p = 0.31), or intraoperative bleeding (SCCD: 689.95 ± 680.05 mL vs RCD: 619.64 ± 837.94 mL; p > 0.05).
In terms of neurovascular complications during the perioperative period, four patients suffered from stroke with no statistically significant difference in proportions between techniques (SCCD: 2.5% vs RCD: 2.1%; p = 0.88).
The median hospital length of stay (LOS) in our sample was 4 days (IQR 3–6), and 13 patients were admitted into the intensive care unit (ICU) in the immediate postoperative period.
When performing multivariate analysis in relation to surgical complications, DTBOS and tumor volume were significantly linked to vascular injuries (Table 2). In the Poisson regression model, tumor consistency and Shamblin classification were found to have a greater incidence rate ratio (IRR) for days in the ICU (Table 3).
Clinical characteristics associated with the occurrence of vascular injuries.
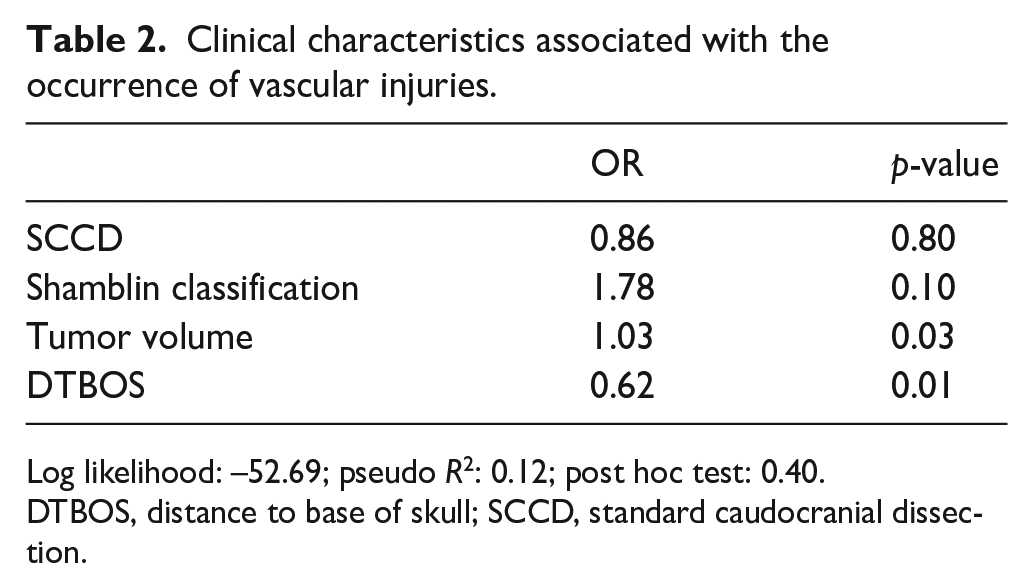
Log likelihood: –52.69; pseudo R2: 0.12; post hoc test: 0.40.
DTBOS, distance to base of skull; SCCD, standard caudocranial dissection.
Clinical characteristics associated with length of stay in the intensive care unit (days) expressed as incidence rate ratios in the Poisson regression model.
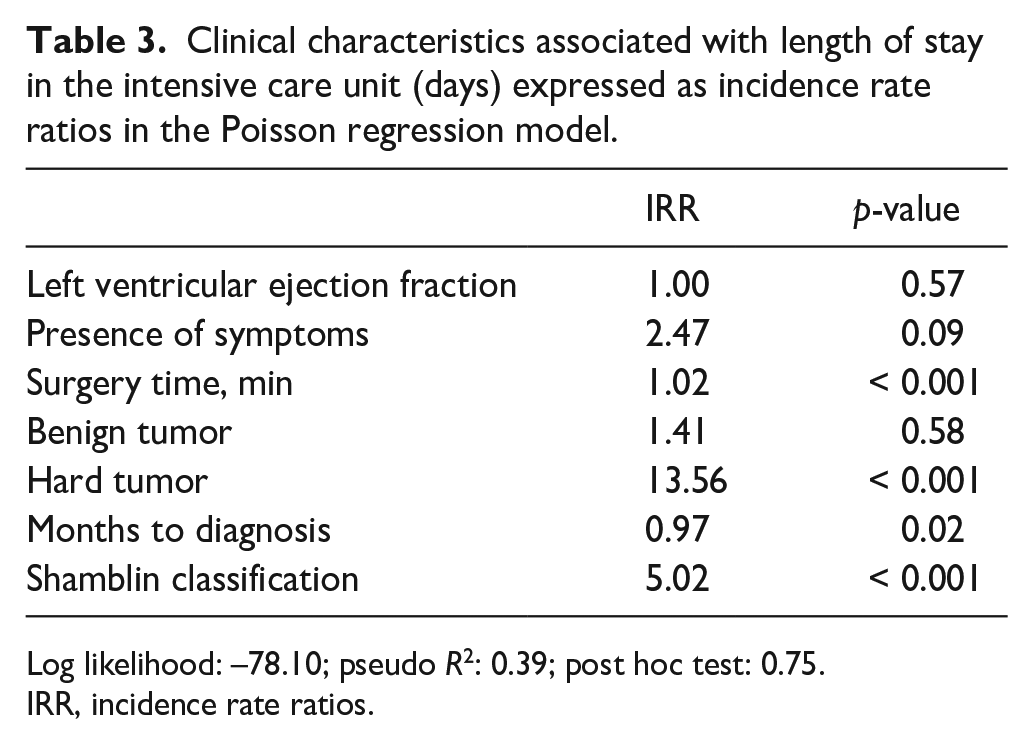
Log likelihood: –78.10; pseudo R2: 0.39; post hoc test: 0.75.
IRR, incidence rate ratios.
In Figures 1 and 2, we present the progression of relevant intraoperative and postoperative variables over time using the RCD technique.
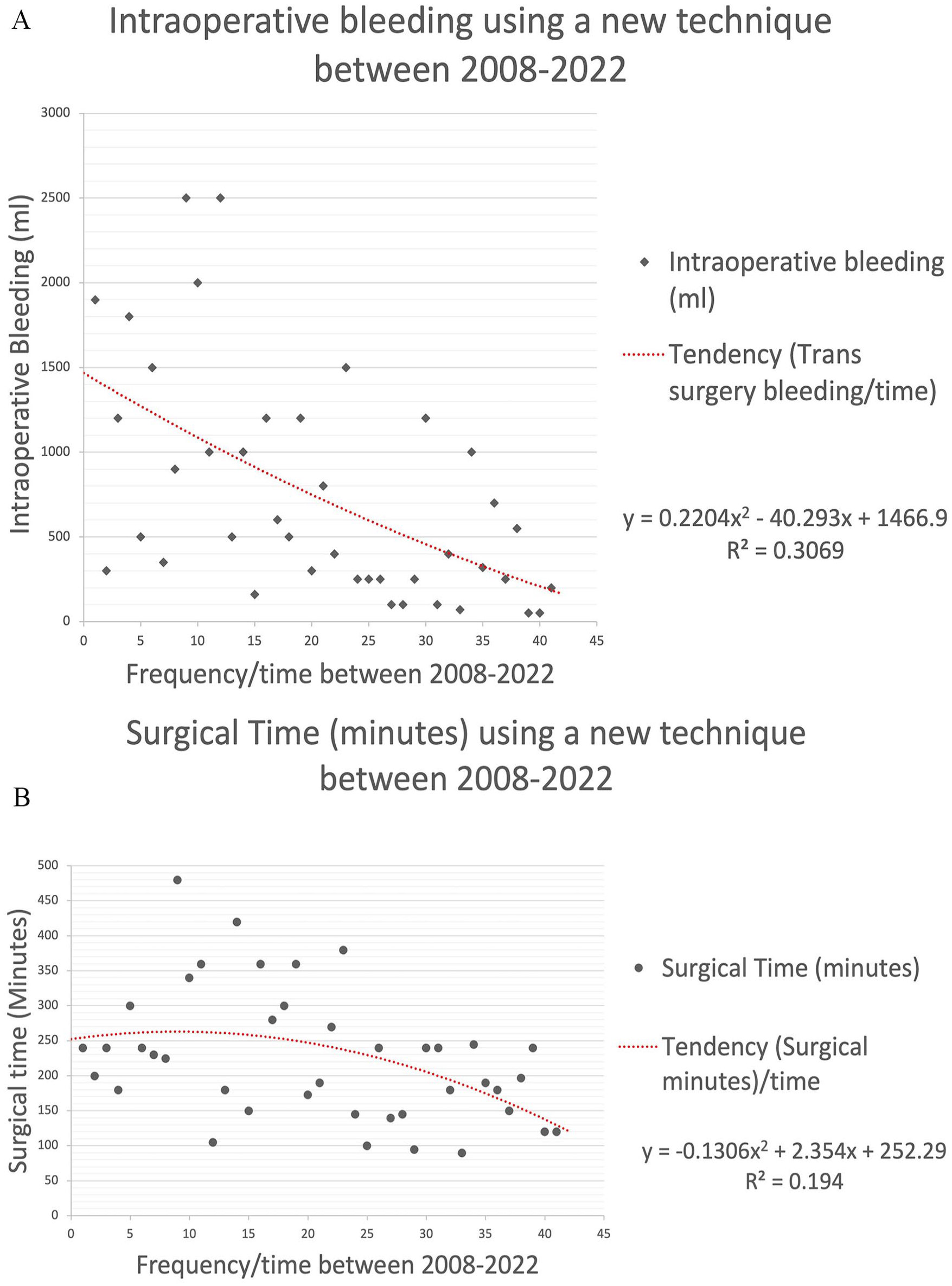
Regression graphic showing dynamic mean trend over time.
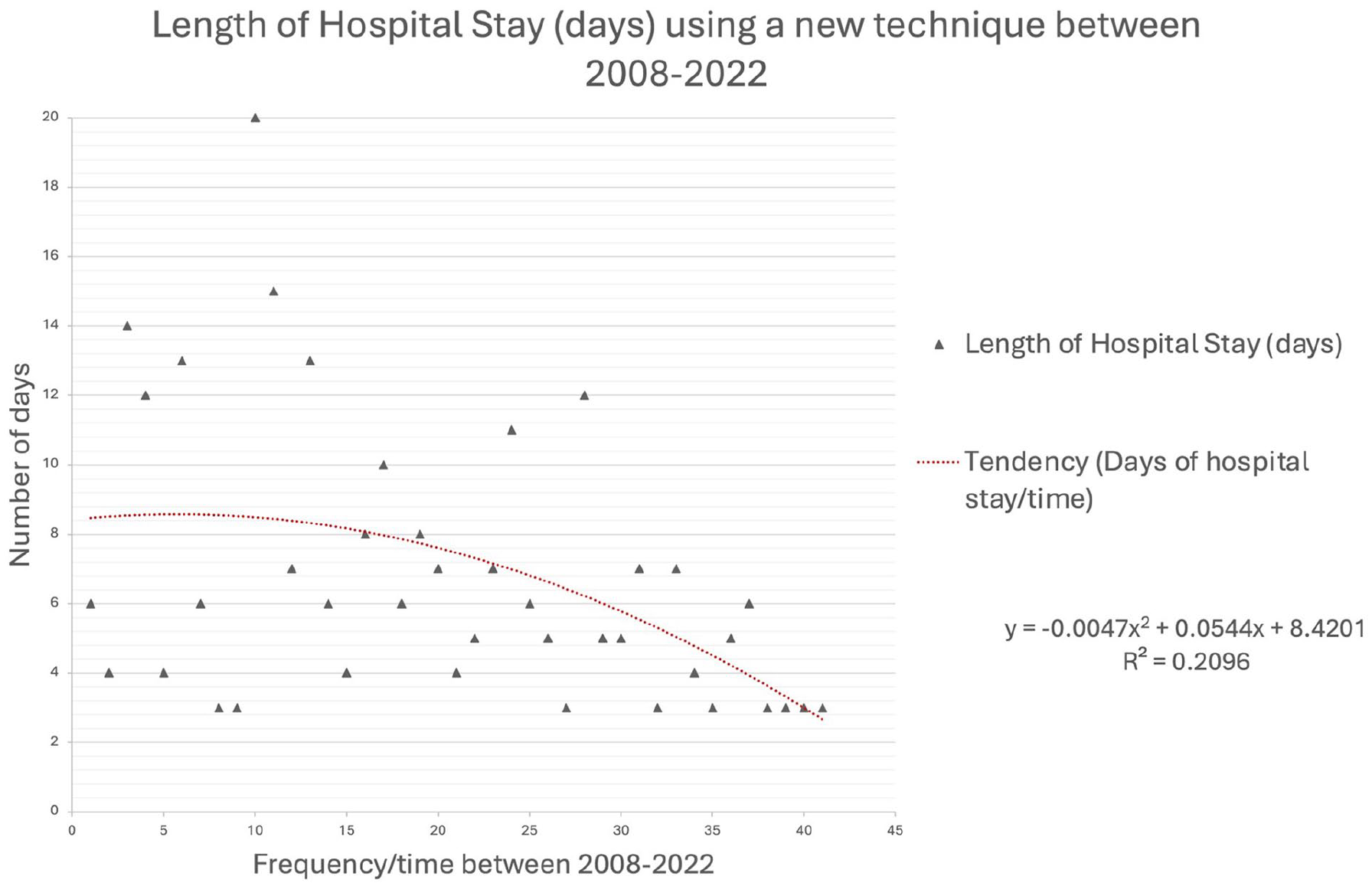
Regression graphic showing dynamic mean trend over time (2008–2022) in regard to length of stay using the RCD technique.
Discussion
CBTs continue to be an intriguing focus of research, captivating vascular surgeons globally due to their distinctive anatomical location and intriguing physiological characteristics. Notably, Latin American institutions, as exemplified by our colleagues in the CAPACITY group, 3 have played a leading role in the ongoing efforts to enhance our understanding of this complex field.
Diagnosing CBTs remains a classic challenge, as many of these tumors can be mistaken for enlarged lymph nodes or an enlarged thyroid. 2 Our series underscored this difficulty, revealing an average time-to-diagnosis of 18 months. Consequently, a painless neck mass emerged as the most frequently reported symptom in our series, aligning with existing literature.1,3,7
Given the often-protracted diagnostic journey, CBTs are seldom categorized as Shamblin I. Instead, they more commonly fall into the categories of Shamblin II or III, presenting surgeons with formidable excision challenges during preoperative planning (Figure 3).1–3,6,7 In relation to this, some authors 8 have posited nonoperative management as a potential option for patients without somatic mutations. However, as highlighted by Bozzani et al. 9 in their commentary on our work, 2 a reliable screening mechanism for tracking the cytologic progression of CBTs is currently lacking, reaffirming surgical excision as the gold standard for an accurate diagnosis.10,11 Moreover, our group’s quality of life assessment revealed a diminished health-related quality of life (HRQoL) in CBT patients, 12 emphasizing the significance of surgical intervention.
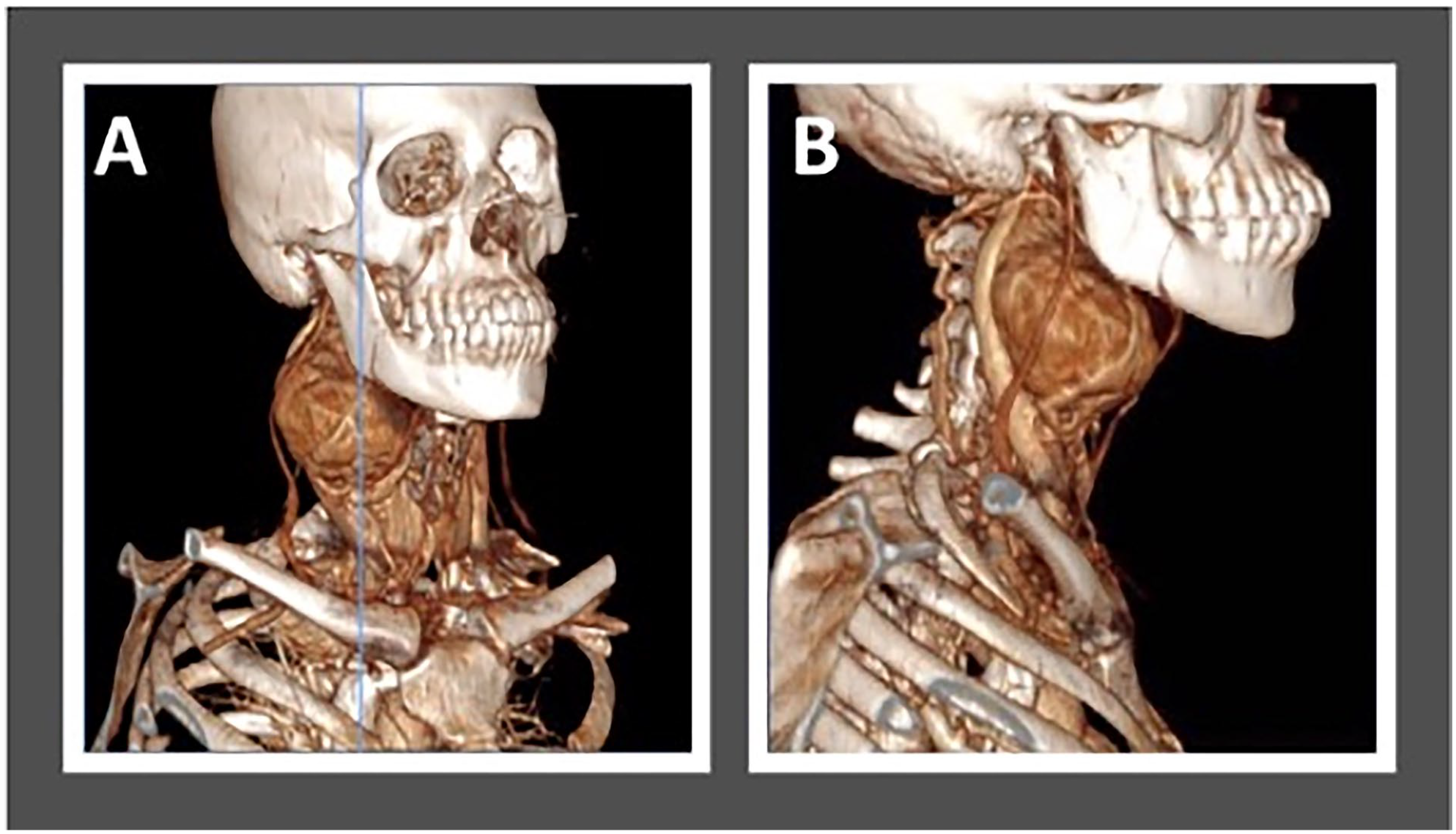
Contrast tomographic angiography of a 40-year-old female patient in two different views
Complex surgical procedures, such as CBT resection, inherently carry the risk of complications.13,14 Recent evidence, as reported by Kim and colleagues, 15 has introduced innovative predictive approaches. Factors such as DTBOS, tumor volume, and Shamblin classification were found to anticipate bleeding and cranial nerve injury. 15 Our analysis similarly identified associations between DTBOS and tumor volume with vascular lesions, underscoring their potential in predicting surgical outcomes.
Regarding PE, recent debates have arisen, with some authors16–18 advocating for its use due to reported reductions in blood loss and postoperative hematomas. Conversely, others19 –22 have highlighted a potential association with longer hospital stays. However, most PE studies exhibit retrospective designs, limiting their ability to account for confounding factors, such as tumor characteristics.16 –22 In our center, PE is not performed in any cases since adopting the RCD technique in 2007. Hence, only one patient (0.7%) underwent PE for a Shamblin III CBT prior to referral to our center and a cerebellar stroke occurred afterwards; however, the tumor remained unchanged. In addition, at the time of surgery, the paraganglioma had a DTBOS of 1.8 cm yet the tumor was safely resected using the RCD technique without postoperative complications. As such, our current work demonstrates acceptable surgical outcomes associated with the RCD approach, even without the routine use of PE.
Since 2007, our department has embraced a modified approach to CBT resection. We initially reported our experiences in 2015, 5 with encouraging results. The RCD technique stands apart from the SCCD approach in that it initiates CBT dissection below the common carotid artery bifurcation to gain control of feeding vessels. Subsequently, the external carotid artery (ECA) is gently rotated laterally, facilitating posterior luxation of the proximal end of the paraganglioma and enhancing visualization of the subadventitial plane of Gordon-Taylor 5 (Figures 4 and 5). In our experience, the RCD technique has been paramount in the improvement of surgical care in these patients; moreover, as it should be expected with any new approach, a learning curve is necessary. In Figures 1 and 2 we show a clear tendency for improvement in bleeding, intraoperative time, and length of stay.
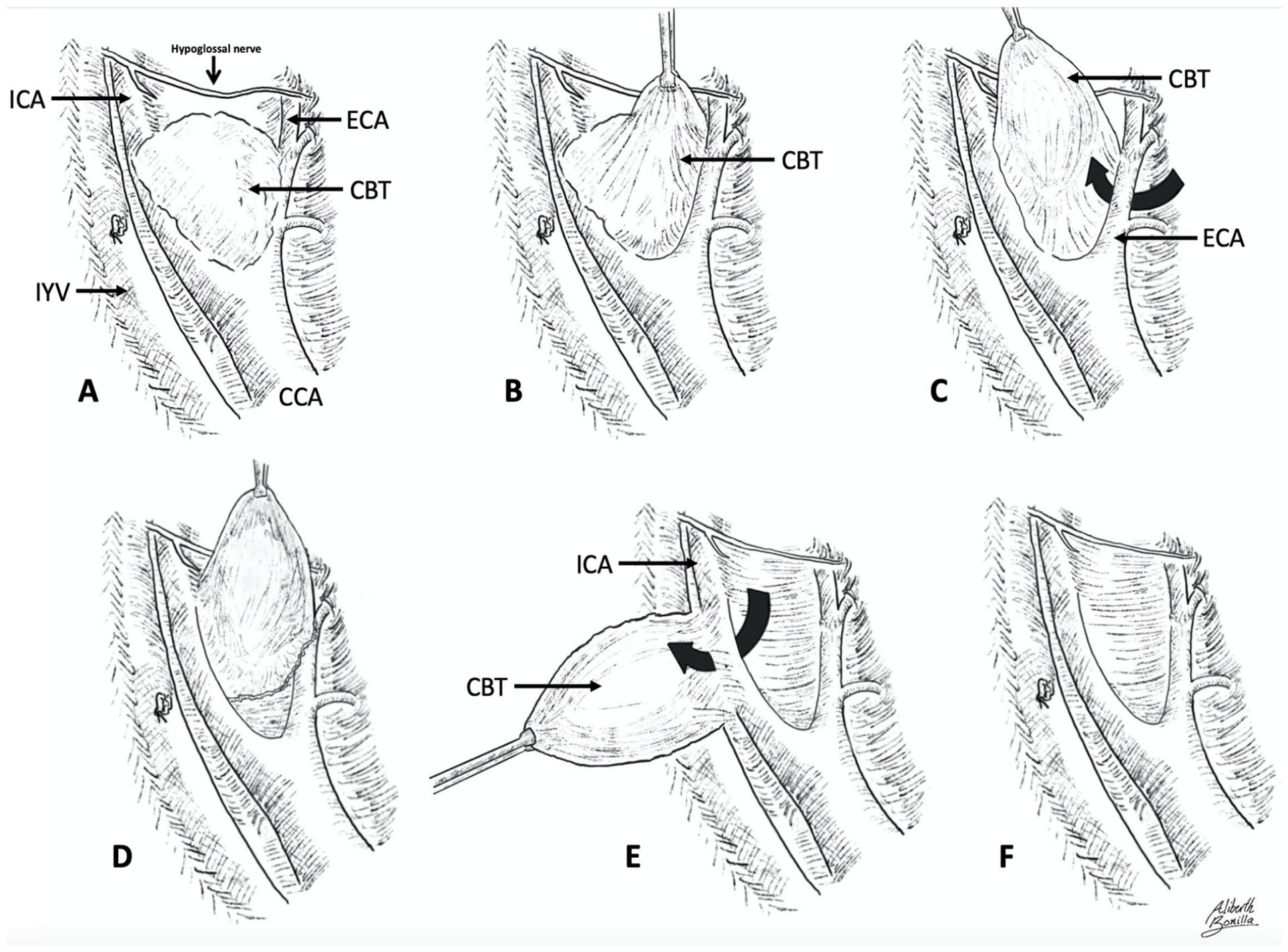
Retrocarotid dissection.
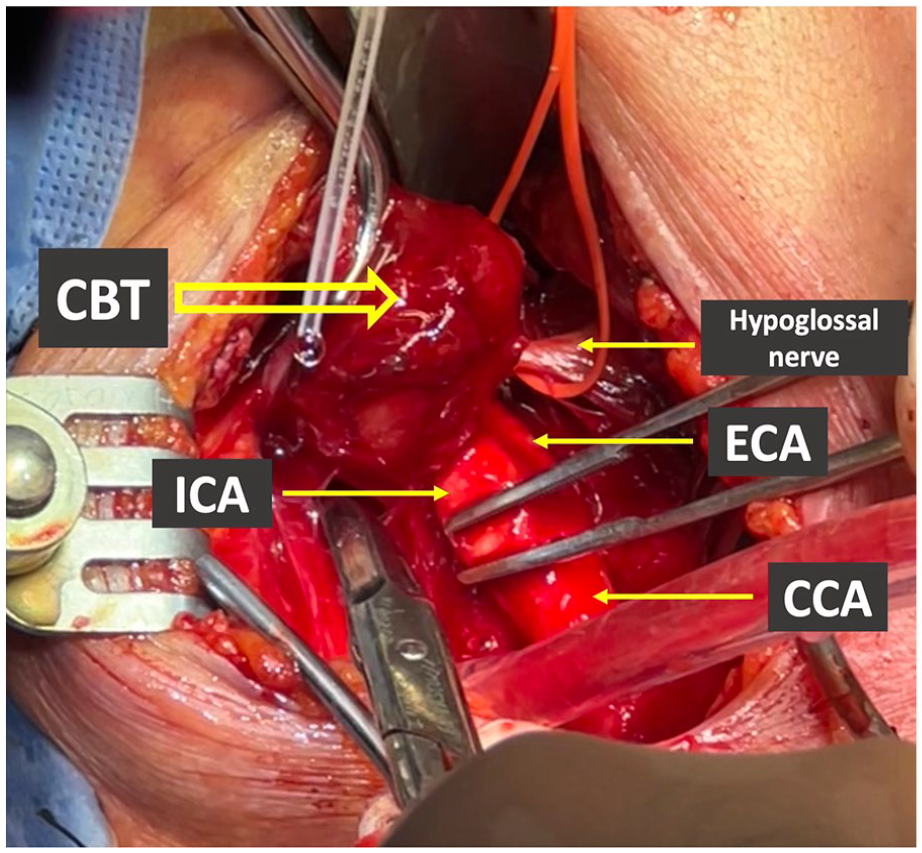
Posterior luxation of a CBT.
Study limitations
As our study is of a retrospective nature, we acknowledge the limitations inherent to the latter. The potential for historical bias cannot be ruled out as we performed a comparison through time.
Conclusion
CBT treatment continues to spark discussion, emphasizing the need for a deeper understanding of the physiological changes occurring in affected patients. Additionally, given the intricacies of surgical excision, techniques should prioritize safety and cost-effectiveness, qualities exemplified by the RCD technique. Our current analysis reaffirms the multiple advantages associated with the RCD technique, even without the use of PE; moreover, DTBOS and tumor volume were confirmed to be correlated with the occurrence of vascular injuries. Furthermore, our department has shown an adequate learning curve underscoring our approach as a safe and equivalent alternative to the standard caudocranial technique.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.