
Abstract

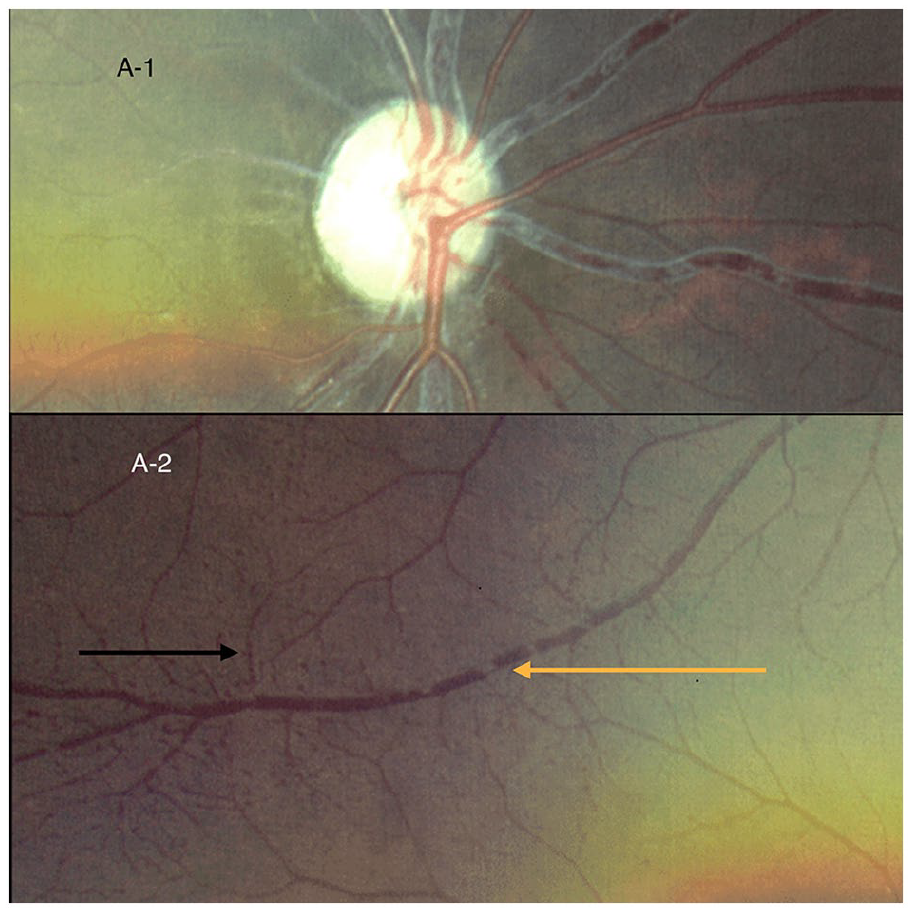
A young woman in her 20s presented to our tertiary eye care center in southern India with defective vision in the right eye. Upon examination, there was a relative afferent pupillary defect in the right eye and both eyes had sluggish blood flow in the conjunctival microvasculature, optic disc pallor (Panel A), segmented flow in the retinal vasculature (termed as ‘cattle trucking’ or ‘box carring’ – typically described in retinal arterial occlusions), and multiple peripheral microaneurysms in the retina (Panel A-2: black arrow: microaneurysms; yellow arrow: ‘box carring’).
A basic examination of the systems revealed a bilaterally nonpalpable radial arterial pulse, prompting a strong suspicion for a systemic cardiovascular cause for the same, most notably Takayasu arteritis – also known as the pulseless disease.
A heightened erythrocyte sedimentation rate in the blood workup strengthened this suspicion. The diagnosis was subsequently confirmed with ultrasound and computed tomography angiography studies, which showed circumferential wall thickening in the aortic arch, bilateral common, external, and internal carotid arteries, and vertebral arteries having up to 50% narrowing of the lumen, consistent with acute active phase Takayasu arteritis type I (Panel B: arrows). 1

The therapeutic approach involved systemic steroids, anticoagulant therapy, and dual antiplatelet medication. Upon stabilization and review at our clinic after 1 month, normal flow patterns in the retinal vasculature were res-tored. However, optical coherence tomography findings indicated permanent ischemic thinning and loss of normal retinal architecture (Panel C-1) in the right eye; the left eye retinal architecture was relatively well preserved (Panel C-2). To assess the extent of ischemia, fundus fluorescein an-giography was performed (Panel D), revealing multiple retinal capillary nonperfusion areas (white boxes) and microaneurysms (red [or gray] boxes), consistent with stage 2 Tak-ayasu retinopathy. 2 Pan-retinal laser photocoagulation was conducted to prevent neovascular complications due to chronic ischemia.


Interestingly, Mikito Takayasu, who described this gra-nulomatous vasculitis in 1908, was an ophthalmologist. 3 Although ocular manifestations in Takayasu arteritis typica-lly range from retinal arterial occlusion to ischemic optic neuropathy, this case represents a unique presentation of eponymous Takayasu retinopathy described and staged by Uyama and Asayama in 1976 4 as the primary manifestati-on. Mirouse et al. have also noted that the existence of retinopathy indicates a poorer prognosis. 5 Systemic involvement in Takayasu arteritis can also lead to hypertension and subsequently hypertensive retinopathy, which is characterized by arteriolar attenuation, arteriovenous crossing changes, soft exudates (‘cotton wool spots’), and even edema of the optic disc, whereas Takayasu retinopathy is characterized by ischemic changes, such as segmented flow in vasculature and microaneurysms followed by arteriovenous shunts and neovascular complications. This case underscores the critical importance of interdisciplinary collaboration for comprehensive patient care in Takayasu arteritis, especially given the nuanced ocular presentations that may serve as early indicators of this systemic condition.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Note – figures are in color online.