
Abstract

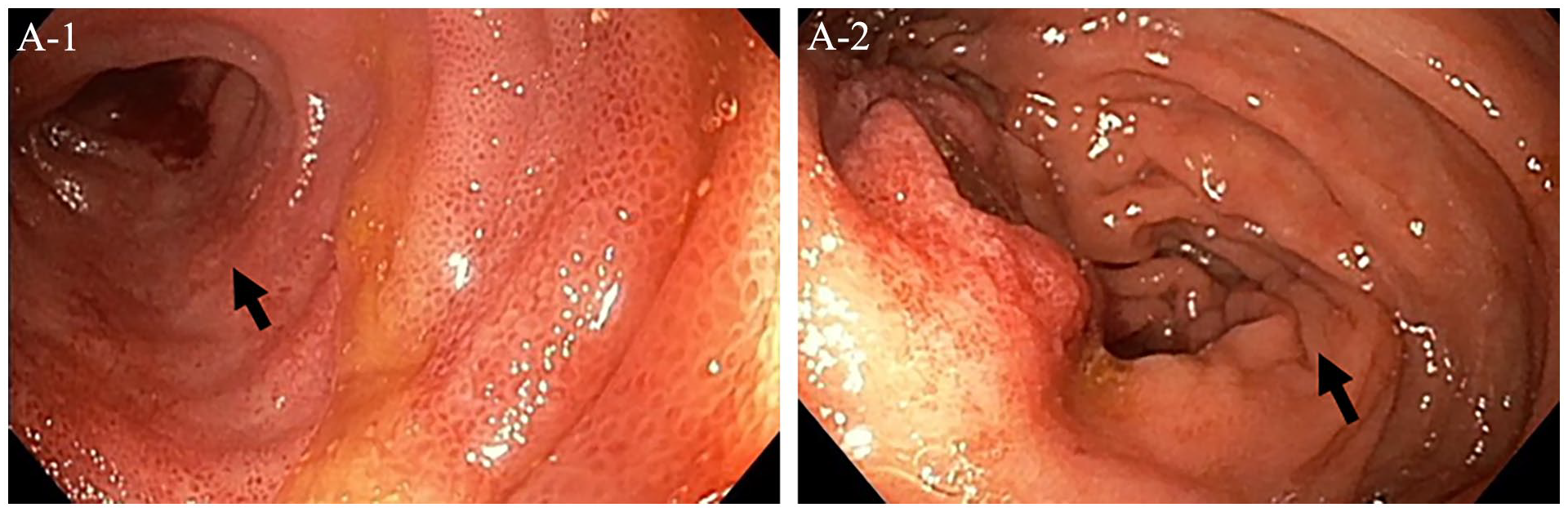
A 67-year-old man with a history of hypertension presented with a chief complaint of chronic, postprandial abdominal pain. Two years earlier he had similar symptoms at which time an extensive work-up led to a diagnosis of biopsy-proven sclerosing mesenteritis that was managed with tamoxifen therapy, ultimately resulting in clinical improvement. However, 3 months prior to the current presentation, the pain returned and was now associated with significant sitophobia, resulting in over a 20-pound (9 kg) weight loss. Colonoscopy showed edematous, erythematous, and cyanotic discoloration of the terminal ileum villi and ileocecal valve (Panel A, arrows). Magnetic resonance imaging of the abdomen and pelvis revealed irregularity of several distal left mesenteric branches with extensive mesenteric venous collaterals (Panel B, arrows) and thickening and mural edema of the terminal ileum, cecum, and descending colon (Panel B, arrows). Owing to concern for ileocolonic vein thrombosis, he was started on therapeutic dose apixaban. Additionally, tamoxifen was discontinued in favor of high-dose steroids. An extensive autoimmune work-up was negative for systemic vasculitides.
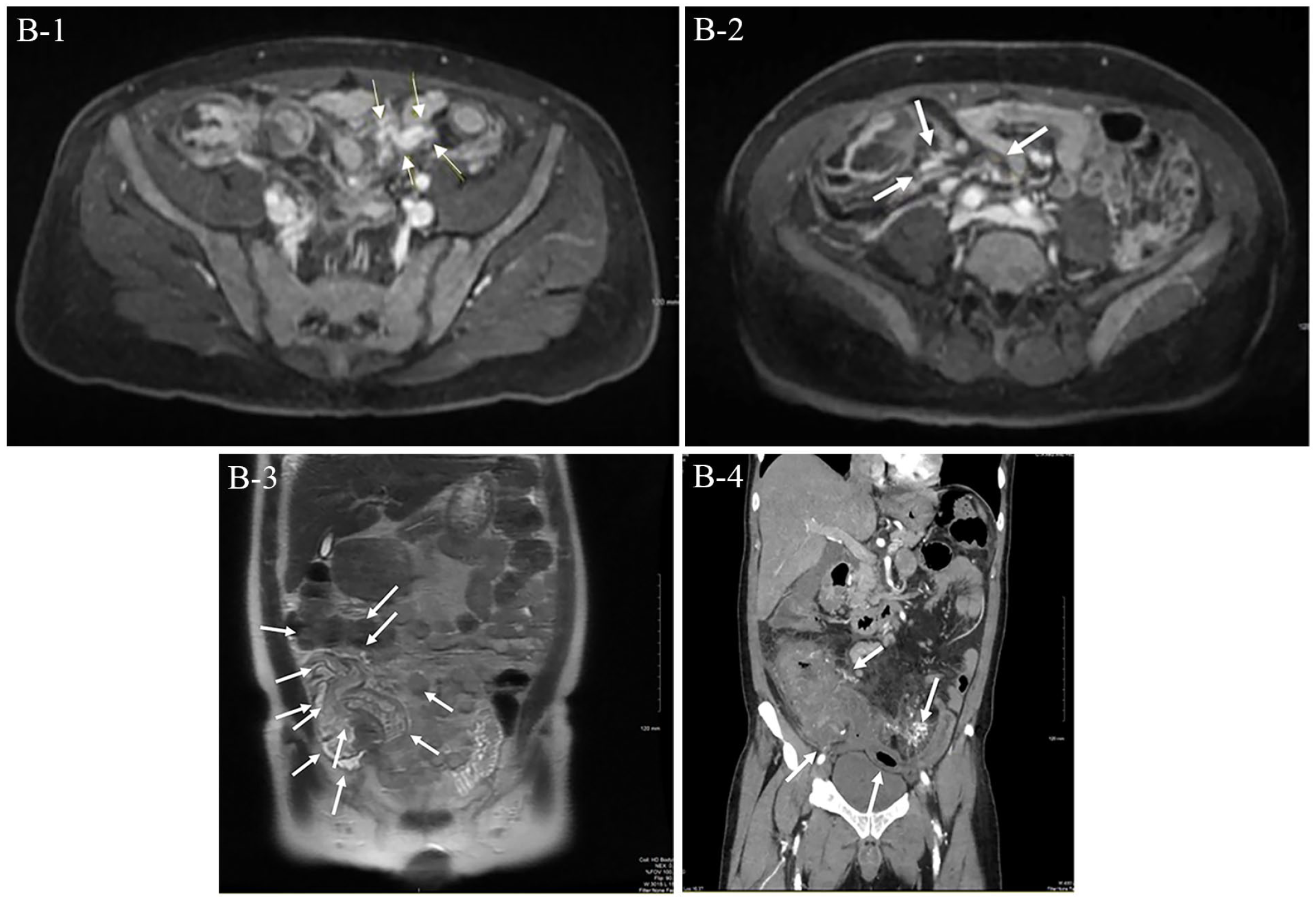
Despite these changes, he represented for severe right lower quadrant pain. He was found to be febrile, tachycardic, and have significant leukocytosis and an elevated serum lactate. Computed tomography angiography of the abdomen and pelvis revealed bowel wall thickening concerning for ischemia (Panel B, arrows). An exploratory laparotomy revealed a markedly thickened, inflamed ileum with ischemia and gangrene of the right colon. Ileocolectomy with primary ileocolonic anastomosis was performed. Surgical pathology of the small bowel specimen (Panel C-1, low power, arrows) showed intimal hyperplasia (Panel C-2, high power, arrows) and lymphocytic phlebitis (Panel C-3, low power, arrows; C-4, high power, arrows). Given the clinical presentation, negative autoimmune evaluation, and findings on histopathology, a diagnosis of enterocolic lymphocytic phlebitis was made after multidisciplinary collaboration.
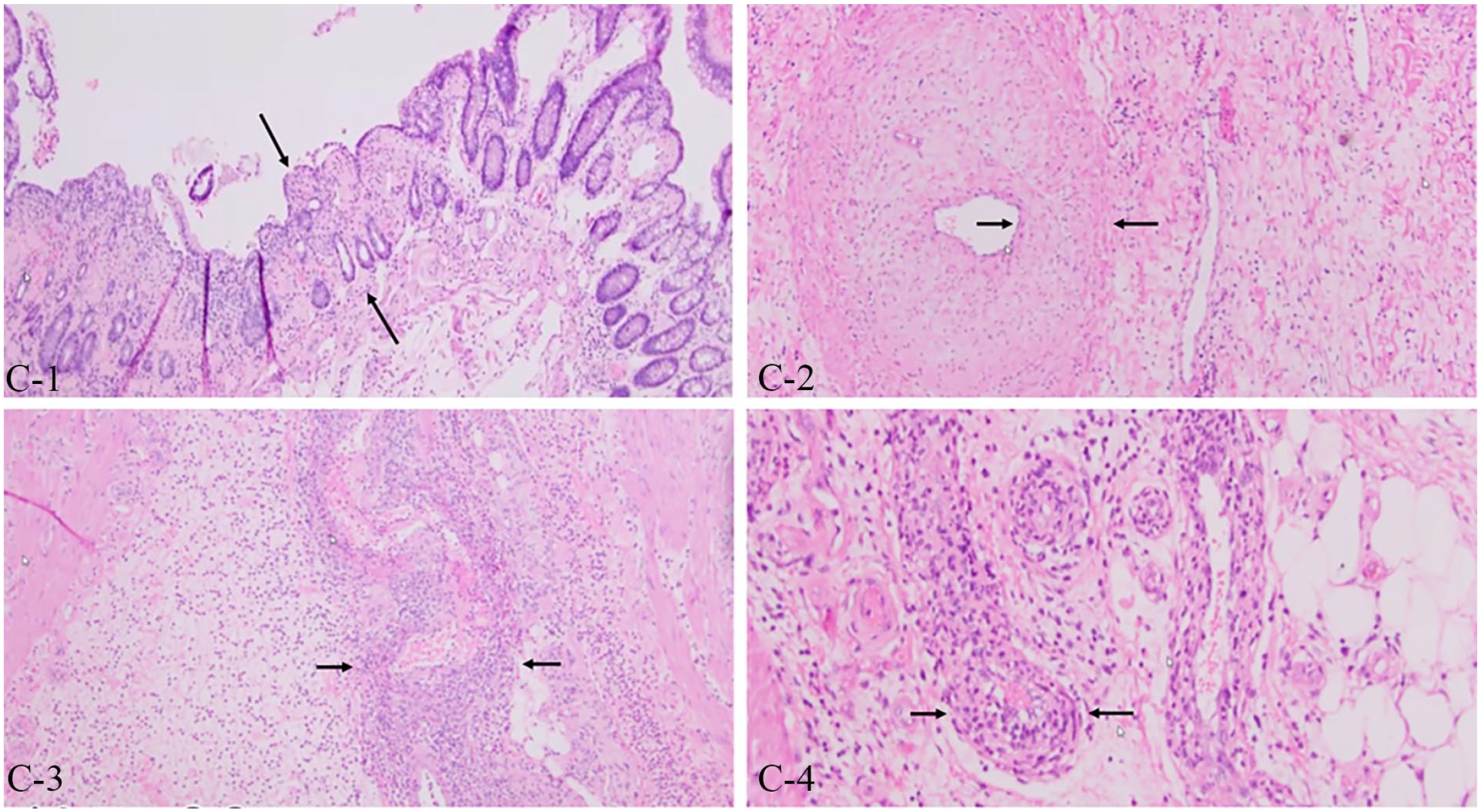
Enterocolic lymphocytic phlebitis is a rare, nonneoplastic, inflammatory enteropathy in which there is lymphocytic infiltration of mesenteric veins and venules without arterial involvement. The characteristic histologic feature is prominent lymphocytic inflammation affecting mesenteric veins of any size in the large or small bowel. 1 The congregation of lymphocytes leads to localized venular hyperplasia which heightens the risk for developing bowel ischemia and thrombosis. The condition is notably not associated with systemic vasculitides. 2 As in this case, definitive diagnosis is with bowel pathology, which may reveal venous vascular changes distinct from areas of ischemic mucosal injury, favoring a primary venous process. Definitive management involves surgical resection of the affected bowel, after which clinical improvement was achieved.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.